Embed Size (px)
DESCRIPTION
Epilepsi adalah suatu kejang yang berhubungan dengan sistem saraf tubuh kita
Citation preview

Treatment Strategies in Epilepsy: Sequential Monotherapy or Add-on Therapy
Bagian Ilmu Penyakit SarafRS Bayukarta
Karawang
bambanghartono

Marshall 2004
The UK National Institute of Clinical Excellence (NICE) has recommended that doctors in England and Wales should use the newer epilepsy drugs gabapentin, lamotrigine, levetiracetam, oxcarbazepine, tiagabine, topiramate, and vigabatrin to treat epilepsy in adults who have not benefited from treatment with older drugs, such as carbamazepine or sodium valproate.
bambanghartono

Marshall 2004
NICE also recommends that patients should be treated with monotherapy wherever possible. If initial treatment is unsuccessful, monotherapy with an alternative drug should be tried. Combination therapy should only be an option when treatment with monotherapy has failed to prevent seizures. Lamotrigine, oxcarbazepine, and topiramate are licensed in the UK for use as monotherapy; all the drugs are licensed for use in combination therapy.
bambanghartono

Epilepsi (ILAE 1981)Bangkitan Parsial Bangkitan Umum T
IDAK
TERKLASIFIKASI
Bangkitan ParsialSederhana
Bangkitan ParsialKompleks
Bangkitan umum Sekunder (tonik, klonik,tonik-klonik)
(konvulsif & non-konvulsif)
Bangkitan mioklonik
Bangkitan lena (absence seizures)
Bangkitan klonik
Bangkitan tonik
Bangkitan atonik / astatik
Bangkitan tonik – klonik
Manifestasi motorikManifestasi sensorikManifestasi autonomikManifestasi psikik
Gambaran parsial sederhana diikuti serangan lena
Dg serangan lena pada awalnya

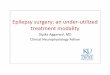
Etiologi Epilepsi
77%
5% 4% 4% 4%3%
2%1%
Primary - Idiopathic
Cerebrovascular
CNS Neoplasma
Congenital CNSMalformation
Trauma
CNS Infection
Other known
Birth asphyxia
Symptomatic or Cryptogenic (23%)
Primary – Idiopathic (77%)

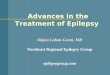
Etiologi Epilepsi
10
20
30
40
50
60
Idiopathic
VascularTumor
TraumaTrauma lahirHerediter
Fre
ku
en
si re
lati
f
USIA
Perkiraan frekuensi macam-macam etiologi epilepsi berdasarkan usia

Algoritma Diagnosis EpilepsiSpells
Seizure Other
Non-epileptic Epileptic
Psychogenicpseudoseizures
Syncope with anoxic seizure
Recurent seizures Febrile seizure
Acute seizure (s)Single seizure(unprovoked)
Epilepsy Recurent febrileseizures
Seizure type(s) Etiology
Generalized,Partial, partial secondary generalization,Unclassified.
No syndromeSyndrome
Localization related Not localization related
Syncope, panic attack,migraine,TIA,movement disorder,Sleep disorder,etc
Metabolic, head trauma,stroke, drugs,
alcohol withdrawal,etc .
Seizure types,etiology,etc
All clinical and laboratory data, neuroimagingSeizure description and
EEG

TUJUAN PENGOBATAN PADA EPILEPSI Mengontrol gejala atau tanda (bangkitan) secara adekuat dengan
penggunaan obat yang minimal
PRINSIP PENGOBATAN1. Diberikan bila terdapat minimum 2 kali bangkitan dalam setahun2. Pengobatan mulai diberikan bila diagnosis telah ditegakkan dan
setelah penyandang dan atau keluarganya menerima penjelasan tujuan pengobatan dan kemungkinan efek samping
3. Pemilihan jenis obat sesuai dengan jenis bangkitan4. Seyogyanya pengobatan dengan monoterapi5. Pemberian obat dimulai dari dosis rendah dan dinaikkan bertahap
sampai dosis efektif tercapai6. Pada prinsipnya pengobatan dimulai dengan OAE lini pertama. Bila
diperlukan penggantian obat, obat pertama diturunkan bertahap dan obat kedua dinaikkan secara bertahap
7. Bila monoterapi gagal, dapat dipertimbangkan kombinasi OAE8. Bila memungkinkan dilakukan pemantauan kadar obat sesuai indikasi
Pedoman Tatalaksana Epilepsi, 2003
bambanghartono

AED Options for Specific Seizure Types
SEIZURE TYPE MONOTHERAPY ADJUNCTIVE 1st CHOICE 2nd CHOISE
Partial onset Carbamazepine Valproic acid GabapentinPhenytoin Phenobarbital LamotrigineOxcarbazepine Primidone Topiramate
TiagabineLevetiracetamZonisamideFelbamate
GeneralizedTonic-clonic Valproic acid Phenytoin Lamotrigine
Carbamazepine TopiramatePhenobarbital FelbamatePrimidone Zonisamide
Tonic, clonic, Valproic acid Phenobarbital Lamotrigineatonic Clonazepam Topiramate
FelbamateZonisamide
Absence Ethosuximide LamotrigineValproic acid Felbamate
AcetazolamideMyoclonic Valproic acid Phenobarbital Lamotrigine
Clonazepam TopiramateFelbamateZonisamide Blum, 2002
bambanghartono

DRUGS USED AS MONOTHERAPY
Partial and secondary generalized seizuresCarbamazepineSodium valproateOxcarbazepine Lamotrigine Levetiracetam Topiramate Phenytoin
Primary generalized seizures Sodium valproateLamotriginePhenytoinTopiramate Levetiracetam
Uncertain seizure typesSodium valproateLamotrigine
Faught, 2004
Newer drug proposedFewer long term side effectsRecommended with cautions
bambanghartono

AEDs should be offered after a first tonic-clonic seizure if :
The patient has had previous myoclonic, absence or partial seizures The EEG shows unequivocal epileptic discharges The patient has a congenital neurological deficit The patient considers the risk of recurrence unacceptable
bambanghartono

PHARMACOKINETICS OF COMMON AEDs
AED HALF-LIFE EFFECT UPON DOSING FREQUENCY (hours) HEPATIC ENZYMES (per day)
Phenytoin 7-42 Inducer 1-3Carbamazepine 12-17 Inducer 2-4Oxcarbazepine 9 Mild 2Phenobarbital 55-140 Inducer 1-3Valproic acid 6-16 Inhibitor 2-3Gabapentin 5-7 None 3Lamotrigine 25 Min Inducer 2-3Topiramate 18-30 Mild 2-3Levetiracetam 6-8 None 2
Adapted from Blum, 2002
bambanghartono

INITIATION SCHEDULE FOR COMMON AEDs
Phenytoin IV / oral load Carbamazepine Gradual initiation / 1-2 weeksOxcarbazepine Gradual initiation / 4-6 weeksValproic acid Immediate therapeutic doseGabapentin Immediate therapeutic doseLamotrigine Gradual initiation / 4-6 weeksTopiramate Gradual initiation / 4-6 weeksLevetiracetam Immediate therapeutic dose
Adapted from AAN, 2003
bambanghartono

SITE OF CLEARANCE FOR COMMON AEDs
Phenytoin > 90% hepaticCarbamazepine > 95% hepaticOxcarbazepine 45% renal; 45% hepaticValproic acid > 95% hepaticGabapentin 100%renalLamotrigine 85% hepaticTopiramate 30-50% hepatic; 50-70% renalLevetiracetam body water
Adapted from AAN, 2003
bambanghartono

SAFETY ISSUES ASSOCIATED WITH NEW ANDOLD AEDs
Phenytoin Aplastic anemia, hepatic failure, Steven-Johnson syndrome
Carbamazepine Aplastic anemia, hepatic failure, Steven-Johnson syndrome
Oxcarbazepine RashValproic acid Hepatic failure, pancreatitis, thrombocytopeniaGabapentin None knownLamotrigine Rash, Steven-Johnson syndrome, hypersensitivityTopiramate Renal calculi, hepatic failure, open-angle glaucoma,
hypohydrosisLevetiracetam None known
Adapted from AAN, 2003
bambanghartono

EFFECT OF NEWER AEDs ON OLDER AEDs
Adapted from AAN, 2003
Phenytoin Carbamazepine Valproic acid Phenobarbital
GabapentinTiagabineZonisamide none none none noneLevetiracetam
Lamotrigine none none ↓25% none
Topiramate may ↑ none none none
Oxcarbazepine may ↑ none slight ↑ none
bambanghartono

For most patients, antiepileptic monotherapy is both less likely to cause unwanted side effects and more likely to control seizure
Other advantages of monotherapy include lower costs, ease of compliance, and less chance for drug interactions.
Roughly 80% of patient with epilepsy are optimally treated with monotherapy
Use of the older generation of antiepileptic drugs is fraught with many pitfalls related to strong pharmacokinetic interactions, both among anticonvulsants and with other therapeutic classes
MONOTHERAPY vs POLYTHERAPY ???
bambanghartono

Partial Seizures First Choice: Carbamazepine
Not toleratedSodium valproateLamotriginePhenytoin
Continued seizure
If already taking: Add:Carbamazepine Sodium valproateSodium valproate LamotrigineLamotrigine Sodium valproatePhenytoin Sodium valproate
Controlled Improved but No improvement not controlled
Withdraw First drug Add one of
LamotrigineTopiramateGabapentinVigabatrin
Withdraw Second drug
SIGN 1999
bambanghartono

Primary GeneralizedSeizures
First Choice: Sodium valproate
Not toleratedEthosuximide / Lamotrigine(Absence)Lamotrigine / Clonazepam(Myoclonic/akinetic)Lamotrigine(Tonic clonic)
Continued seizure
If already taking: Add:Sodium valproate ABSENCE Ethosuximide / LamotrigineSodium valproate MYOCLONIC / AKINETIC Lamotrigine / ClonazepamSodium valproate TONIC-CLONIC Lamotrigine
If Sodium valproate not tolerated, and seizure control not achieved on second choice drug
Substitute: For:Lamotrigine / Clonazepam EthosuximideClonazepam LamotrigineLamotrigine Clonazepam
SIGN 1999
bambanghartono

Partial and secondary generalized seizures
First Line:CarbamazepineSodium valproateLamotrigineOxcarbazepine
Continued seizure
Withdraw First drug
Add one ofLevetiracetam/ Tiagabine/ LamotrigineTopiramate/ Gabapentin / VigabatrinOxcarbazepine
Withdraw Second drug
SIGN 2003
Controlled Improved but not
controlled
No improvement
Consider replace seconddrug or add third drug
bambanghartono

Marshall 2004
The majority of patients with newly-diagnosed epilepsy respond well to AEDs. Failure to do so may be due to:
An incorrect diagnosis of epilepsy An inappropriate choice of AED for the epilepsy syndrome Failure to take the prescribed AED An underlying cerebral neoplasm Covert drug or alcohol abuse
bambanghartono

ANTIEPILEPTIC DRUG BLOOD LEVELS
Routine monitoring of AED concentration is not indicated. Measurement can sometimes be useful in the following circumstances:
Adjustment of phenytoin doseAssessment of adherence and toxicity
Assay of lamotrigine, vigabatrine, gabapentin, topiramate, tiagabine, oxcarbazepine and levetiracetam concentrations should not be undertaken routinely
SIGN 2003
bambanghartono

DRUG-RESISTANT EPILEPSY
First Line AEDs
First Line AEDs
Improve seizure control but fails
to produce seizure freedom
at max dose
Failed
Failed
COMBINATION THERAPY
CONSIDER:• Patients seizure type (s)• Should be limited to two / at most three AEDs• Different mechanism of action• Side effect profile• Drug interaction
SIGN 2003
bambanghartono

ANTIEPILEPTIC DRUG WITHDRAWL
Prognostic index indicators can be used to give an estimate of the risks of seizure recurrence following AED withdrawal
The question of continued treatment or AED withdrawal should be discussed with people with epilepsy, who are at least two years seizure free, so that they can make an informed choice. Factors to be discussed should include driving, employment, fear and risks of further seizures and concerns about prolonged AED treatment.
The rate of withdrawal of AEDs should be slow, usually over few months, and longer with barbiturates and benzodiazepins.One drug should be withdrawn at a time
bambanghartono

Prognostic Index
bambanghartono

Prognostic Index
bambanghartono

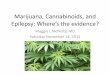
Drug Failure
Generalizedseizure
Unclassifiable Partial seizures
TreatmentMonotherapyLamotrigineValproic acid
TreatmentChoicesTreat as generalizedinitially
TreatmentMonotherapyCarbamazepineLamotrigineValproate
Monotherapy Failure
Add-on:LevetiracetamTopiramate
Add-on:LevetiracetamGabapentinTopiramateTiagabine
Therapy Choices for People with Learning Disability
Trimble, 2003
bambanghartono

Treating patients with epilepsy need a therapuetic options. One of the most important consideration is drug selection, besides of type of epilepsy, age, gender, and special considerations like patient with learning disability. All of these must be placed in the context of treatment strategy.
When patients do not become seizure free on the first or second antiepileptic drug, there are several strategies for continued treatment. One very reasonable options is to convert the patient to another monotherapy. However, removing a drug may involve risk of worsening, and physicians and patiens opt to add a second drug. The concept of polytherapy was frowned upon in the past, but with the advent of new drugs with novel mechanism, and fewer drug interactions, “rational polytherapy” is becoming more appealing.
Clearly, this is where the newer drugs are at a substantial advantage as compared to older drugs. One of the new drugs is levetiracetam which has specific characteristics that make it an optimal choice for many patient populations.
SUMMARY
bambanghartono

THANK YOUTHANK YOU