Embed Size (px)
Citation preview

TREATMENT OF SEVER FH: LDL APERESIS
Dr. Hind AlHumaidan, MD,FRCPA
Consultant Hematopathologiest
Director, Blood Bank, Donor,
Transfusion Services, APHERESIS & Stem Cell Cord Blood Bank
Saudi Arabia chairperson of AATM
INTRODUCTION
• Familial hypercholesterolemia (FH) characterized by:
- Hypercholesterolemia
- Cutaneous & tendon xanthomas
- Premature atherosclerotic cardiovascular disease
• FH genetic disorder caused mutation gene related (LDL) receptor pathway:
- LDL receptor
- Proprotein convertase subtilisin/kexin type 9 (PCSK9)
- Apolipoprotein B
- LDLRAP1 gene mutations2
INTRODUCTION
• HoFH pts harbor:
- Homozygous mutations
- Compound heterozygous mutations
- Double-heterozygous mutations of these genes
INTRODUCTION
• HoFH Pts show sever symptoms:
- Severe hypercholesterolemia (600–1,000 mg/dL)
- Cutaneous and tendon xanthomas
- Aortic valvular stenosis
- Supra-aortic valvular stenosis from childhood
• HeFH Pts show milder symptoms
INTRODUCTION
• Development statins enabled the effective treatment of HeFH
• PCSK9 inhibitors made it possible to control LDL-C levels more intensively
• HoFH pts resistant to most lipid-lowering drugs (statins, ezetimibe, resins, and PCSK9 inhibitors)
INTRODUCTION
• Recently, inhibitor of microsome triglyceride transfer protein (MTP) developed shown to reduce LDL-C levels in HoFH (independent LDL receptor pathway)
• Lipoprotein apheresis still one of the major strategies to control LDL-C levels in HoFH, severe hypercholesterolemia
INTRODUCTION
• first trial of lipoprotein apheresis in HoFH patients was performed as plasma exchange by
de Gennes et al 1967
• This therapeutic approach led to the improvement of coronary artery stenosis and regression of xanthoma accompanied by LDL-C reduction
• TPE to eliminate lipoprotein started 1975
• Disadvantage that various important substances, such as immunoglobulin, are removed along with LDL
• Development selective LA systems to avoid loss beneficial plasma components 1980
HISTORY OF LIPOPROTEIN APHERESIS
• HoFH rare life- threatening condition
• Markedly elevated circulating levels of low-density lipoprotein cholesterol (LDL-C)
• Extensive Xanthomas
• Accelerated ,premature atherosclerotic cardiovascular disease before age 20 years
HOMOZYGOUS FAMILIAL HCH
• Prognoses poor ,no treatment, they die at the age of 20 years
• With extracorporeal therapy, life span can be prolonged
• lipid-lowering drugs (statins, ezetimibe, even PCSK9 inhibitors) Not effective.
• these pts. develop cardiovascular complications (e.g., coronary heart disease, stenosis aortic valve), even with LA tx.
HOMOZYGOUS FAMILIAL HCH

• LDL apheresis established therapy for HoFH
• Benefits clearly outweigh the risks and burden
HOMOZYGOUS FAMILIAL HCH
• Extracorporeal removal LDL-C , important adjunctive treatment HoFH
• Expensive , time consuming
• Unselective plasma exchange replaced by Selective elimination atherogenicplasma proteins
• Single treatment decrease LDL-C ,55-70%
• Once weekly exchange achieve close to normal level of LDL-C
HOMOZYGOUS FAMILIAL HCH
• LDL-C concentration follows sawtooth like pattern during regular LA tx.
• Countries screening programs for familial HCH carried out on a large
scale, only few pt effectively treated with LA
• Accumulating data suggest that the earlier the therapy initiated the better the prognoses
France et al 2016
HOMOZYGOUS FAMILIAL HCH
LDL-C LEVELS DECREASE AND THEN REBOUND FOLLOWING APHERESIS
Pre-treatment
LDL level
2-week
interval
LD
L C
HO
LE
ST
ER
OL
Start of LDL apheresis
Baseline LDL
TIME
Post-treatment
LDL level
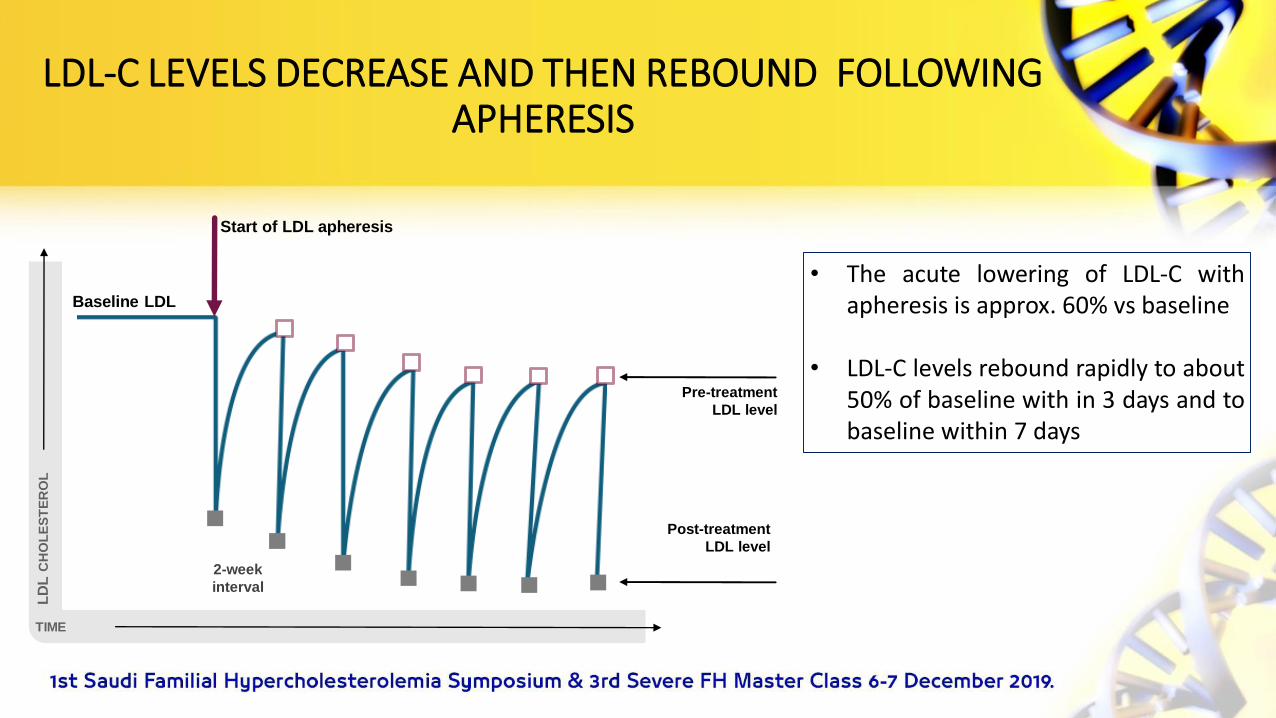
• The acute lowering of LDL-C withapheresis is approx. 60% vs baseline
• LDL-C levels rebound rapidly to about50% of baseline with in 3 days and tobaseline within 7 days
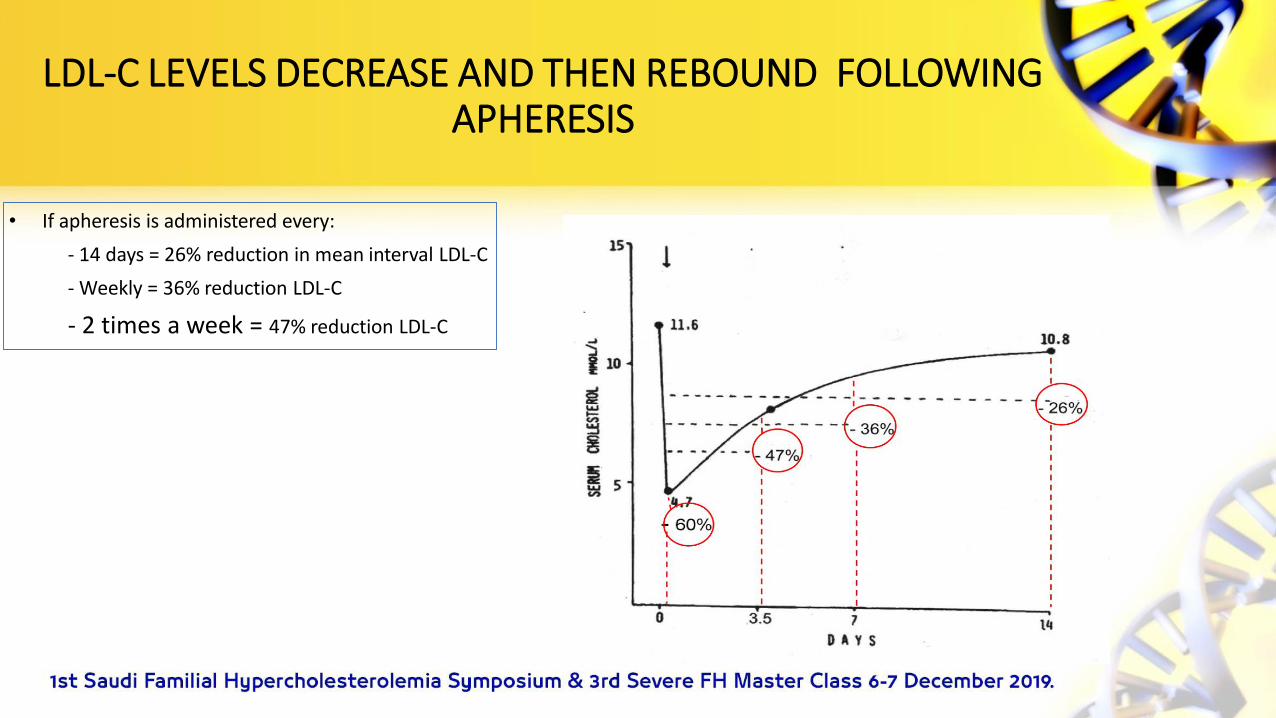
• If apheresis is administered every:
- 14 days = 26% reduction in mean interval LDL-C
- Weekly = 36% reduction LDL-C
- 2 times a week = 47% reduction LDL-C
LDL-C LEVELS DECREASE AND THEN REBOUND FOLLOWING APHERESIS

• Although the earlier the apheresis is initiated the better theprognosis
• In practice age of onset & frequency of treatment representcompromise between practical feasibility
HOMOZYGOUS FAMILIAL HCH

• Severe HCH defined by increased LDL-C levels which have induced atherosclerotic lesions in different vessels.
• An optimal diet should be adhered
• Drug therapy needed.
• LA indication accepted within secondary prevention, in order to prevent new cardiovascular events
• Recommendation LA weekly
SEVERE HYPERCHOLESTEROLEMIA (HCH)

• Since 2000, an elevation of Lp(a) was increasingly recognized as an atherogenic risk factor
• 2008 isolated elevation of Lp(a) was accepted as an indication for LA
• At present, LA is the only available effective therapeutic approach to lower Lp(a).
ISOLATED ELEVATION OF LP(A)
• Pts who develop cardiovascular events due to high Lp(a) concentrations typically have the following peculiarities:
▪ Lp(a) levels are extremely high.
▪ A positive family history with early cardiovascular events in first-degreerelatives.
▪ Patients suffer from first severe cardiovascular event at young age (before50).
ISOLATED ELEVATION OF LP(A)

• Pts who develop cardiovascular events due to high Lp(a) concentrations typically have the following peculiarities:
▪ Many pts. underwent several interventions (PTCA, PCI) before the diagnosisof an elevation of Lp(a) is made.
▪ Very often they were heavy smokers the combination of smoking & highLp(a) is especially atherogenic.
▪ Pts. have a concomitant hypertension.
ISOLATED ELEVATION OF LP(A)

• Two criteria for the initiation of LA in Pts:
1- Lp(a) level higher than 60 mg/dL (or higher than 120 nmol/L )
2- progress of atherosclerotic disease, either clinically or documented with an imaging technique
ISOLATED ELEVATION OF LP(A)
• Lipid concentrations & development atherosclerosis major criteria for evaluation efficiency of LA therapy
• LDL-C and Lp(a) levels are regularly measured before and after the LA session's
• LDL-C reduction 60%-80%
LIPOPROTEIN APHERESISWHAT IS THE EVIDENCE
• Over the years, pre-apheresis LDL-C levels may be decreased.
• In patients with familial HCH xanthomas disappear
• No randomized controlled long-term study had been performed.
LIPOPROTEIN APHERESISWHAT IS THE EVIDENCE
• Study incidence of coronary events apheresis pts, compared with pts being treating with statins alone (all patients had HCH), the rate was found to be reduced by 72% over 6 years.
Mabuchi et al,1998
• Several observational studies saw reduction of cardiovascular events in HCH pts. between 33% & 74%,comparing situation before start LA therapy & during treatment.
Emmrich et al 2015
Heigl et al 2015
Schatz et al 2017
LIPOPROTEIN APHERESISWHAT IS THE EVIDENCE

• A single-blind randomized controlled trial conducted in 20 Pts. with refractory angina and raised lipoprotein(a) >50 mg/dL, with 3 months of blind weekly LA or sham, followed by crossover
• The LA sessions increased myocardial perfusion, improvements with apheresis compared with sham also occurred in atherosclerotic burden, as assessed by total carotid wall volume, exercise capacity by the 6 min walk test, 4 of 5 domains of the Seattle angina questionnaire, and quality of life physical component.
Khan,2017,2018
LIPOPROTEIN APHERESISWHAT IS THE EVIDENCE
• Underlying principles of LA methods are filtration, adsorption, &precipitation
• Two methods process whole blood (DALI, Liposorber D), othermethods need plasma separation as a first step
DIFFERENT LA METHODS


• In filtration methods, plasma is separated from the blood cells by a filter
• A second filter retains macromolecules like lipoproteins.
• Antibodies fixed on sepharose against apolipoprotein B (TheraSorbTM LDL) and against Lp(a) particles (Pocard Lp(a) columns) specifically bind the corresponding lipoproteins.
COMPARISON OF DIFFERENT LA METHODS
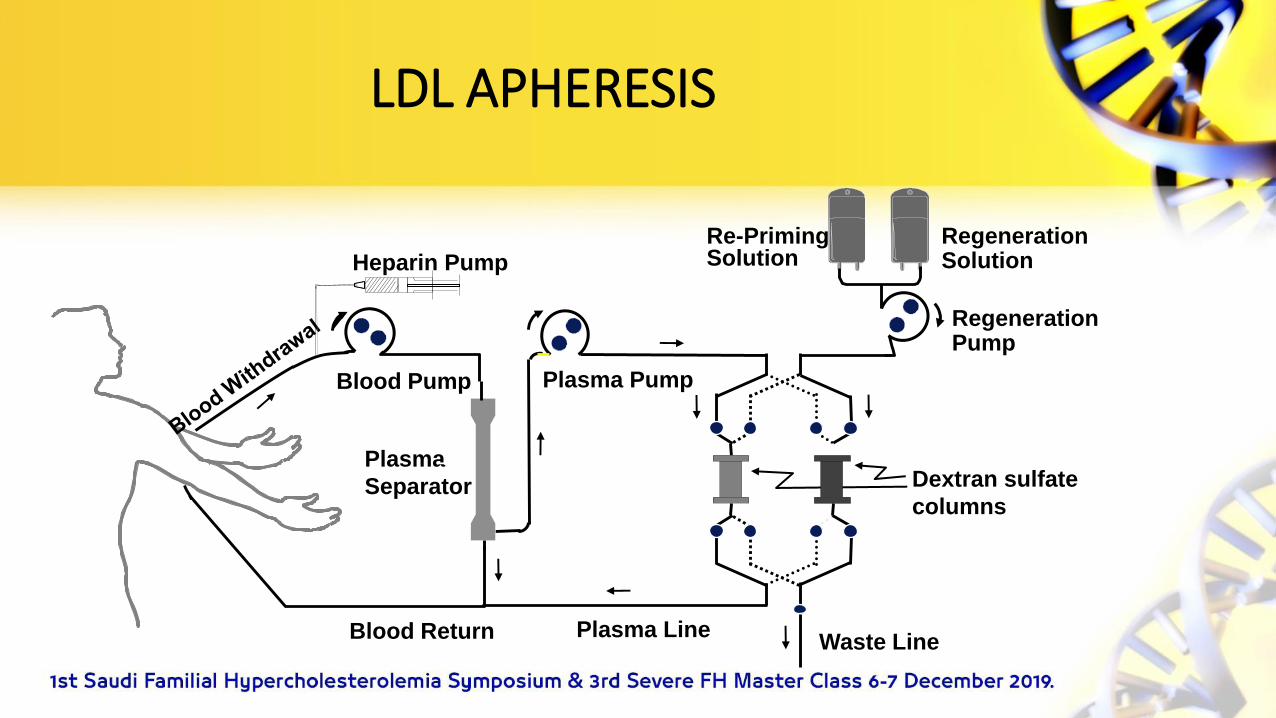
LDL APHERESIS
Plasma Line
Dextran sulfate
columns
Plasma PumpBlood Pump
Heparin Pump
Blood Return
Plasma
Separator
RegenerationPump
Re-PrimingSolution
RegenerationSolution
Waste Line
• An adsorption of apolipoprotein B-containing lipoproteins on a negatively charged surface takes place in the DALI and Liposorber D systems.
• Precipitation of lipoproteins occurs in an acidic milieu (acetate buffer) with an excess of heparin (HELP method).
COMPARISON OF DIFFERENT LA METHODS
• Anticoagulation always has to be performed—with heparin and/or citrate.
• Comparing available LA methods with respect to their lipid-lowering capacity, only minor differences observed.
• Treated vol. blood/plasma established by treating physician, based on recommendations from the manufacturer(1.5 plasma vol)
COMPARISON OF DIFFERENT LA METHODS

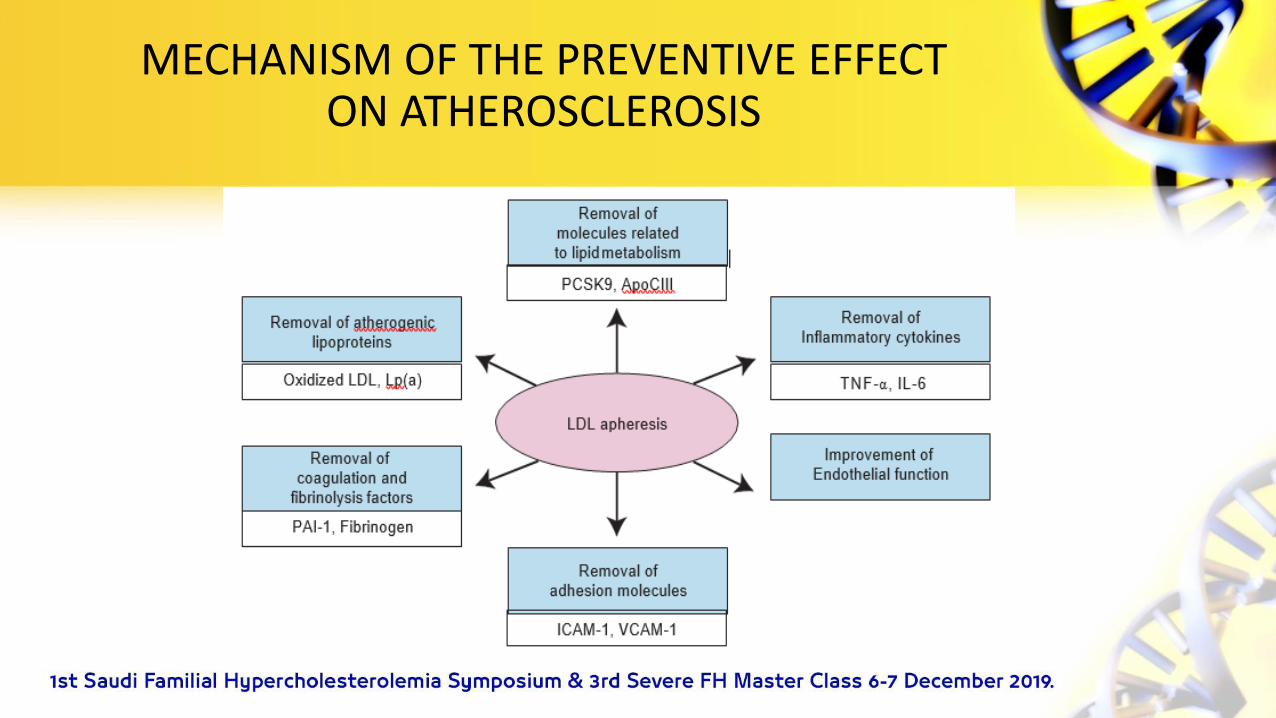
• Selective LDL adsorption therapy can remove not only LDL, but also cell adhesion molecules such as:
- Intracellular adhesion molecule-1
- Vascular cell adhesion molecule
• Selective LDL adsorption can also remove inflammatory cytokines, such as:
-Tumor necrosis factor
-Interleukin-1
MECHANISM OF THE PREVENTIVE EFFECT ON ATHEROSCLEROSIS
• Reduce reactive oxygen species production via NADPH oxidase.
• Thus, LDL adsorption therapy can prevent atherosclerosis as a result of & independent of LDL removal.
MECHANISM OF THE PREVENTIVE EFFECT ON ATHEROSCLEROSIS
• LDL adsorption therapy was also reported to improve vascular endothelial function via the induction of bradykinin and nitric oxide production
• LA improves atherogenic lipoprotein metabolism in addition to direct removal of LDL.
• LDL adsorption therapy could also remove PCSK9, which plays a pivotal role in lipid metabolism by enhancing endosomal & lysosomal degradation of LDL receptor in the liver
MECHANISM OF THE PREVENTIVE EFFECT ON ATHEROSCLEROSIS
• PCSK9 is known to be involved in inflammatory processes by upregulating proinflamatory gene expression
• Elevated plasma Conc. Lp(a) is decreased by LA
MECHANISM OF THE PREVENTIVE EFFECT ON ATHEROSCLEROSIS
MECHANISM OF THE PREVENTIVE EFFECT ON ATHEROSCLEROSIS
• LA methods are well tolerated
• Major problems may occur with the venous access
• Acute hypotension
• Heparin allergy
ADVERSE EFFECTS OF LA

• Some patients need a calcium substitution
• Iron replacement
• ACE inhibitors should be avoided in patients on LA therapy may aggravate bradykinine syndrome
ADVERSE EFFECTS OF LA

• Venous access can be an issue
• Optimal frequency once per week
• Most centers treat every two weeks
• Ideal age to start 5yr not later than 8yr
ADVERSE EFFECTS OF LA
KFSH&RC APHERESIS CENTER
• Both Donor & Therapeutic Center
• 11 Trima Machine
• 11 Optia Machine
• Staff consist of 13 nurse
• Procedures 9000 platelets collection /6000 therapeutic procedures
LDL APHERESIS PROGRAM – KFSH&RC
• Started 2008 LA
• 33 patients on the program
• 23 still on active treatment
• 7 Pts deceased , 2 post liver transplant
• 2 Pts drop out , 1 successful liver transplant in China
• The youngest pt started 9 year old
• 18 pt done with peripheral IV access
• 5 pt have Fistula
• Average clearance 1.5 plasma vol is 70 -85 %
LDL APHERESIS PROGRAM – KFSH&RC

• Sessions done every two weeks
• Most patients achieve < 2.5 mmol/l
• Cost per session around 5000 SR
LDL APHERESIS PROGRAM – KFSH&RC
CHALLENGES PATIENT FACE
• Personal
• Familial
• Social
• Psychological
• Impact of the disease
• Considerable burden for patients
• Physical signs & limitations
• Psychosocial factors
• Treatment related issues
• Impact on education and employment
CHALLENGES PATIENT FACE
• Requires commitment from Pt & family
• Time needed to travel to hospital
• Time for procedure
• Interruption of normal activities
• Financial burden for pt
CHALLENGES PATIENT FACE



THANK YOU