-
8/13/2019 treatment of sclerosis systemic
1/7
Treatment of Scleroderma
Allen N. Sapadin, MD; Raul Fleischmajer, MD
The treatment of systemic sclerosis (scleroderma) is difficult
and remains a great chal-
lenge to the clinician. Because the cause is unknown, therapies
are directed to improve
peripheral blood circulation with vasodilators and antiplatelet
aggregation drugs, to pre-
vent the synthesis and release of harmful cytokines with
immunosuppressant drugs, and
to inhibit or reduce fibrosis with agents that reduce collagen
synthesis or enhance collagenase pro-
duction. The purpose of this review is to critically analyze
conventional and new treatments of sys-
temic sclerosis and localized scleroderma. The therapeutic
options discussed for the treatment of sys-temic sclerosis include
the use of (1) vasodilators (calciumchannel blockers[nifedipine],
angiotensin-
converting enzyme inhibitors [captopril, losartan potassium],
and prostaglandins [iloprost,
epoprostenol]), (2) immunosuppressant drugs (methotrexate,
cyclosporine, cyclophosphamide, and
extracorporeal photopheresis), and (3) antifibrotic agents
(D-penicillamine, colchicine, interferon
gamma, and relaxin). The treatment options reviewed for
localized scleroderma include the use of
corticosteroids, vitamin D analogues (calcitriol,
calcipotriene), UV-A, and methotrexate. Prelimi-
nary reports on new therapies for systemic sclerosis are also
considered. These include the use of
minocycline, psoralenUV-A, lung transplantation, autologous stem
cell transplantation, etaner-
cept, and thalidomide. Arch Dermatol. 2002;138:99-105
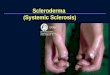
Scleroderma or systemic sclerosis (SSc) isa connective
tissuedisease that affects vari-ous organ systems, including skin,
gastro-intestinal tract, lungs, kidney, andheart. Theseverity of
skin andinternal organ involve-mentmaycorrelate withthe clinical
courseof the disease. Based on the degree of skininvolvement, SSc
can be divided into lim-ited cutaneousSSc or diffuse
cutaneousSSc.Limited cutaneous SSc is characterized
bysclerodactylyor acrosclerosis, withdistal in-volvement of the
extremities (distal to theelbows andknees) with or without face
in-
volvement. This clinical picture comprisesRaynaud
phenomenon,dysphagia,calcino-sis cutis, and telangiectasis; it is
slowlyprogressiveandis frequently associatedwithanticentromere
antibodies. The most se-vere complications are pulmonary
hyper-tension and biliary cirrhosis. Diffuse cuta-neous SSc is more
severe and showsproximal involvement of the extremities
(proximal to the elbows andknees), trunk,or both.1 Diffuse
cutaneous SSc is often as-sociated with pulmonary interstitial
fibro-sis,renal crises,andgastrointestinalinvolve-ment (dysphagia,
hypomotility, and otherdisorders). Diffuse cutaneous SSc is
fre-quently associated with Scl-70 (antitopo-isomerase) and
nucleolar autoantibodies(polymerase I and III, fibrillarin).
The cause of SSc is unknown and isregarded as an autoimmune
disease in-volving cellular and humoral immunity.Cellular
infiltrates, perivascular or dif-
fuse, have been demonstrated in skin,lungs (alveolitis), smooth
muscle cells,esophagus, ileum and jejunum, syno-vium, and liver.2
These cells consist of Tlymphocytes (CD4+, CD8+), B lympho-cytes,
and other nonspecific inflamma-tory cells,such as macrophages,mast
cells,and eosinophils. Adhesion molecules areinvolved in homing and
retention of lym-phocytes and other inflammatory cells inthe
tissues and may play a role in the for-From the Department of
Dermatology, Mount Sinai School of Medicine, New York, NY.
REVIEW
(REPRINTED) ARCH DERMATOL/ VOL 138, JAN 2002
WWW.ARCHDERMATOL.COM99
2002 American Medical Association. All rights reserved.
wnloaded From: http://archderm.jamanetwork.com/ on
01/30/2014
-
8/13/2019 treatment of sclerosis systemic
2/7
mation of cellular infiltrates in SSc.1-6 Vascular involve-ment
in SSc affects mainly capillaries, arterioles. andsmallarteries.
The vascular pathology consists of absence orreduction in
capillaries and ectasia of capillaries (telan-giectases), often
accompanied by an increase in endo-thelialcell proliferation.7
Soluble mediators, adhesion mol-ecules, and cytotoxic factors have
been incriminated inthe mechanism of endothelial cell damage,
includingplasma factor VIII (von Willebrand factor), transform-ing
growth factor, platelet-derived growth factor, gran-
zyme A, vascular cell adhesion molecule-1, intercellularadhesion
molecule-1, and endothelin-1.8
The mechanism of fibrosis in SSc is not fully un-derstood,
although it is known that soluble mediators(transforming growth
factor, platelet-derived growthfactor, interleukin [IL] 4, IL-6,
tumor necrosis factor[TNF]) can affect the behavior of fibroblast
growth,proliferation, collagen synthesis, and chemotaxis.9-11
Therole of humoral immunity in SSc is unknown, althoughabout 90% of
patients with SSc show circulating anti-nuclear antibodies.12
The treatment of SSc is difficult and remains a chal-lenge to
the clinician. The purpose of this review is tocritically analyze
conventional and new treatments of SSc
and localized scleroderma and briefly review new thera-peutic
approaches under current investigation.
TREATMENT OF SYSTEMIC SCLEROSIS
Skin Involvement
Vasodilators. Vasodilators are used in SSc to reducevaso-spasm
(Raynaud phenomenon) and to improve periph-eral circulation
(ischemia, gangrene) secondary to arte-rial blood vessel damage
(Table 1).
Calciumchannel blockers inhibit smooth muscle cellcontraction by
reducing the uptake of calcium, which isneeded for muscle
contraction. There are 2 groups of cal-cium channel blockers: (1)
the pyridine dicarboxylic ac-ids (nifedipine, nicardipine
hydrochloride) and (2) thedimethoxyphenyls (verapamil
hydrochloride, diltiazem).Nifedipine, in dosages ranging from 30 to
60 mg daily,reduces the severity of Raynaud phenomenon.13 More
re-cently, it was shown that nifedipine was superior to bio-
feedback techniques in reducing the frequency of
Raynaudphenomenon episodes.14 Nifedipine is well tolerated, andthe
most common adverse effects are headaches, flush-ing, and edema of
the feet and ankles. Nifedipine therapycan also be combined with
antiplatelet aggregation drugs(low-dose aspirin) and
dipyridamole(up to 400 mg daily,in slow increments).8
Pentoxifylline (400 mg, 3 timesdaily), alone or in combination with
nifedipine, reducesblood viscosity by increasing red blood cell
deformabil-ity and can be used to improve capillary function.
More recently, losartan potassium, an antagonist ofangiotensin
II receptor type I, was found effective in thetreatmentof Raynaud
phenomenon.15 In this study, a regi-men of losartan potassium, 50
mg daily, was compared
with nifedipine, 40 mg daily. After 2 weeks, both drugsreduced
the severity of Raynaud phenomenon, but onlylosartan reduced the
frequency of episodes. Losartan waswell tolerated, and the most
commonadverse effects weredry cough, muscle cramps, back pain,
dizziness, and in-somnia.
Prostaglandins are potent vasodilators. Iloprost is achemically
stable prostacyclin antagonist that wasfound effective in the
treatment of Raynaud phenome-non secondary to SSc. Iloprost induces
prolonged vaso-dilation, reduces platelet aggregation, and
promotesendothelial cell lining. The drug was administered
bycontinuous intravenous infusion (2 ng/kg per minute)for 8 hours
daily for 3 days.16 More recently, an oral
preparation of iloprost was used for the treatment ofRaynaud
phenomenon.17 A study comparing iloprost,50 to 150 g daily, vs
placebo noted a decrease in dura-tion and severity of Raynaud
phenomenon episodes,although the difference was not statistically
significant.Another study18 involving 103 patients showed
signifi-cant improvement in duration and severity of attacksbut not
in frequency, compared with the placebo. How-ever, a third
multicenter study19 involving 308 patientsshowed that oral
iloprost, 50 g twice daily, was no bet-ter than the placebo.
Immunosuppressant Drugs.Because there is evidencefor activation
of cellular and humoral immunity in SSc,
several immunosuppressant drugs have been previ-ously used, with
questionable benefits, including pu-rine antimetabolites
(6-thioguanine, azathioprine) andalkylating agents (chlorambucil,
cyclophosphamide).20
More recently, investigations have been carried out
withmethotrexate, cyclosporine, cyclophosphamide, and
ex-tracorporeal photopheresis.
A controlled, parallel randomized, double-blind trialwith
chlorambucil vs placebo was carried out involving64 patients with
SSc. After a 3-year follow-up, chloram-bucil had obtained no better
results than the placebo.21
Table 1. Treatment of Systemic Sclerosis
Vasodilators
Raynaud phenomenon
Nifedipine, verapamil hydrochloride
Losartan potassium
Iloprost
Pulmonary hypertension
Epoprostenol
Iloprost (carboprostacyclin)
Captopril
Renal crises
Captopril
Enalapril maleate (Vasotec)
Kidney dialysis
Kidney transplantation
Immunosuppressants
Skin induration
Methotrexate
Cyclosporine
Interstitial lung disease
Cyclophosphamide
Antifibrotics
Skin induration
D-Penicillamine
Colchicine
Interferon gammaRelaxin
(REPRINTED) ARCH DERMATOL/ VOL 138, JAN 2002
WWW.ARCHDERMATOL.COM100
2002 American Medical Association. All rights reserved.
wnloaded From: http://archderm.jamanetwork.com/ on
01/30/2014
-
8/13/2019 treatment of sclerosis systemic
3/7
Methotrexate was used in a randomized, double-blind trial
involving 29 patients with SSc. Patients re-ceived weekly
injections of 15 mg of methotrexate or pla-cebo, and the dosage was
increased to 25 mg per week forpoor responders. After a 24-week
follow-up, significantimprovement was noted in skin induration and
handgripstrength.22 Additional trials involving larger numbers
ofpatients are necessary to confirm these results. Before
ini-tiating methotrexate therapy, a thorough evaluation of the
patient should be completed. Baseline laboratory testsshould
include complete blood cell count, platelet count,liver function
tests, serum urea nitrogen, creatinine, andcreatinine
clearance.
Cyclosporine is an immunosuppressive drug thatselectively
inhibits the release of IL-2 from activated Tlymphocytes. There is
evidence that serum levels of IL-2,its soluble receptors, or both
are frequently elevated inearly SSc.23,24 An open clinical trial
with cyclosporine wasconducted in 10 patients with SSc.25 The
starting dosagewas 1 mg/kg per day, which was increased
progressivelyuntil toxicity appeared or when 5 mg/kg per day
wasreached. After 48 weeks follow-up, there was a de-crease in skin
induration but no improvement in pul-
monary or cardiac involvement. Nephrotoxicity was fre-quent but
usually transient and appeared mainly inpatients receiving more
than 3 to 4 mg/kg per day.25
Because renal involvement in SSc is not uncom-mon, cyclosporine
in thetreatment of SSc should be usedwith great caution. Patients
must be carefully moni-tored for the development of nephrotoxicity,
hyperten-sion, and malignant neoplasm, particularly lymphoma.Many
drug interactions occur, and the patient should bequestioned about
concomitant medications.
Extracorporeal photopheresis has been used to treatSSc. The
principle of this technique is to administer oral6-methoxypsoralen,
followed by extracorporeal activa-tion of lymphocytes by UV-A. The
blood carrying cova-
lently cross-linked DNA-psoralen lymphocytes is thentransferred
into the patient to elicit a specific immuneresponse that may block
proliferation of certain T-lymphocyte clones. An initial
multicenter trial was en-couraging and showed significant
improvement in skininduration but no effect on pulmonary
function.26 How-ever, additional trials questioned the efficacy of
extra-corporeal photopheresis.27 Furthermore, extracorpo-real
photopheresis for SSc is not approved by the Foodand Drug
Administration.
Anotherapproach forimmunosuppression in SScwastheuse of
antithymocyte globulin (3-5 mg/kg for 5 days).After 6 months
follow-up, no improvement in skin scoreor pulmonary function was
noted compared with a pla-
cebo group.28Corticosteroids are not useful in improving or
pre-
venting the progression of skin involvement in SSc. How-ever,
they may be helpful in controlling pain caused byarthralgia or
myalgia. Similar benefits can be achievedwith nonsteroidal
antiinflammatory agents.
Antifibrotic Agents.Fibrosis consists of massive depo-sition of
newly synthesized connective tissue, mostly col-lagens, which is
frequently responsible for the develop-ment of organ insufficiency.
Fibrosis is a prominentfeature
in SSc and can develop in other disorders, such
asatherosclerosis, cirrhosis of the liver, and idiopathic
orsecondary pulmonary fibrosis. Pharmacodynamics of an-tifibrotic
agents are geared (1) to reduce synthesis, ex-cretion, or
polymerization of collagen fibrils, (2) to en-hance collagenase
activity, and(3)to neutralize cytokinescapable of stimulating
collagen synthesis, such as trans-forming growth factor, IL-4, and
IL-6.
D-Penicillamine is a copper chelating agent that also
blocks aldehyde groups involved in intermolecular
andintramolecular cross-linkages of collagen. Early clinicaltrials
showed that D-penicillamine was beneficial in thetreatment of SSc,
resulting in skin softening, slower pro-gression of internal
involvement, fewer renal crises, andincreased survival time.29 The
usual dosage was 250 mg,3 times daily. Several adverse effects may
occur, includ-ing bone marrow depression, nephrotic syndrome,
gas-trointestinal distress, and skin reactions, such as pem-phigus
vulgaris. A recent multicenter, double-blind,randomized clinical
trial was conducted in 134 patientswith diffuse SSc of early (18
months) duration. Onegroup of patients received 750 to 1000 mg of
D-penicillamine daily, while the other group was treated
with 125 mg every other day. After 24 months follow-up,there
wereno statistical differences between thegroupsin skin score
(induration), incidence of renal crises, orsurvival time.30
Furthermore, 80% of adverse effects oc-curred in the high-dosage
group. This study raises seri-ous questions about the therapeutic
efficacy of D-penicillamine in SSc. However, if patients are
treated withD-penicillamine, there is no advantage in using more
than125 mg every other day.
Colchicine has been suggested for the treatment ofSSc, based on
the rationale that it interferes with colla-gen synthesis by
depolymerizing microtubules, reducesfibroblast proliferation,
enhances collagenase activity,andhas some antiinflammatory
properties.31 An early un-
controlled study32
involved 19 patients with a follow-upof 19 to 57 months. This
study noted improvement inskin elasticity, mouth opening, and
finger motility, anda reductionin dysphagia. Themean dosage is
0.6mg twicedaily. The drug is well tolerated, and the main
adverseeffectis diarrhea.Blood cell countsandliver function
testsshould be performed periodically for patients
receivinglong-termtherapy. It is unfortunate that
double-blindpla-cebo-controlled clinical trials are not
available.
Interferon gamma has been shown in vitro to re-duce collagen
production and interfere with fibroblastproliferation. Interferon
alfa also inhibits collagen pro-duction but to a lesser degree than
interferon gamma.11
Early investigations in the treatment of SSc with inter-
feron gamma or interferon alfa showed a modest im-provement in
skin score.11 Recent multicenter clinical tri-als were carried out
with recombinant interferon gamma(50 g subcutaneously, 3 times
weekly for 1 year)33 orwith recombinant interferon gamma (0.01
mg/m2 per dayfor 18 weeks).34 Both studies showed a modest
improve-ment in skin score. Adverse effects were common,
mostlyconsisting of a flulike syndrome. Another
multicenter,randomized controlledclinical trial withinterferon
gammaconcluded that this drug hasmild beneficial effects in
skinsclerosis and disease-associated symptoms.35 A 1-year
(REPRINTED) ARCH DERMATOL/ VOL 138, JAN 2002
WWW.ARCHDERMATOL.COM101
2002 American Medical Association. All rights reserved.
wnloaded From: http://archderm.jamanetwork.com/ on
01/30/2014
-
8/13/2019 treatment of sclerosis systemic
4/7
double-blind placebo-controlledtrial with interferon alfashowed
no benefit in the treatment of scleroderma, andin some patients it
was deleterious.36
Relaxin is a pregnancy polypeptide, cytokine growthfactor that
in vitro decreases the synthesis and secretionof interstitial
collagens, blocks transforming growth fac-tor overexpression of
type I and II procollagens, in-creases overexpression of matrix
metalloproteinases, andreduces the production of tissue inhibitor
of metallopro-
teinases.37
Early investigations using porcine-derived re-laxin in the
treatment of SSc were inconclusive. How-ever, recently, a
multicenter, randomized, double-blindclinical trial was carried out
with human recombinantrelaxin. Sixty-eight patients with moderate
to severe dif-fuse SSc of less than 5 years duration received 25 or
100g/kg per day or a placebo, both administered by con-tinuous
subcutaneous infusion for 24 weeks. Patientsreceiving relaxin
showed improvement in skin indura-tion, oral aperture, hand
extension motion, and pulmo-nary forced vital capacity. Adverse
effects consisted ofmenometrorrhagia, reversible anemia, and
irritation andfocal infections at the site of the subcutaneous drug
de-livery.38 However, additional follow-up observation did
not corroborate the efficacy of relaxin, and the study
wasdiscontinued.
Kidney Involvement
Angiotensin-converting enzyme (ACE) inhibitors, in-cluding
captopril and enalapril maleate, have been shownto be effective in
controlling high blood pressure in SScsecondary to renal crisis.
Furthermore, early treatmentmay prevent the onset of renal
failure.39 In addition, oralcaptopril in dosages of 12.5 to 50 mg
daily may reducepulmonary vascular resistance during pulmonary
hyper-tension.40
A retrospective study41 on renal transplantation in SSc
gave encouraging results. Thedata were obtainedfrom
theUnitedNetwork for Organ Sharing Scientific Renal Trans-plant
Registry. Eighty-six patients with SSc from 1987 to1997 received
renal transplants. After a 5-year follow-up,47% of the patients
were alive, and the 5-year graft sur-vival was similar to that seen
with renal transplantationin patients with systemic lupus
erythematosus. This studysuggests that patients with severe renal
insufficiency whodo not improve after receiving
angiotensin-converting en-zyme inhibitors or kidney dialysis should
be consideredas candidates for renal transplantation.
Lung Involvement
Epoprostenol is an arachidonic acid, naturally occur-ring
prostaglandin with vasodilator activity and inhibi-tory effect on
platelet aggregation.Epoprostenol wasusedby continuous intravenous
infusion in 111 patients withmoderate to severe pulmonary
hypertension secondaryto SSc. After 2 weeks of treatment, there was
improvedexercise capacity and cardiopulmonary hemodynamics.There
was also improvement in the severity of Raynaudphenomenon and
healing of digital ulcers. Adverse ef-fects included jaw pain,
nausea, and anorexia. Local com-plications consisted of sepsis,
cellulitis, hemorrhages, and
pneumothorax (4% incidence for each condition).42 In-travenous
iloprost was also effective in the treatment ofpulmonary
hypertension.43
Cyclophosphamide alone or in combination withlow-dose prednisone
was found effective in the treat-ment of severe interstitial lung
disease in SSc.44,45 Morerecently, cyclophosphamide was used in a
retrospectivecohort study46 involving 103 patients with SSc
associ-ated with lung inflammation (alveolitis) proved by bron-
choalveolar lavage or by lung biopsy. The dosage con-sisted of 1
to 1.5 mg/kg per day orally to up to 2 mg/kgper day. In addition,
they received intravenous cyclo-phosphamide, 800 to 1400 mg
monthly, for 6 to 9 months.The patientstreated with
cyclophosphamide showed sta-bilization of forced vital capacity and
carbon monoxidediffusing capacity. Improvementin survival wasalso
dem-onstrated. Myelosuppression, bladder toxicity (hemor-rhagic
cystitis, bladder carcinoma), and carcinogenicityare complications
of cyclophosphamide therapy. Base-line monitoring includes complete
blood cell count withdifferential and platelets, serum chemistry
profile, andurinalysis.
NEW THERAPIESPRELIMINARY REPORTS
Minocyline
Eleven patients with early SSc were treated with mino-cycline
(100 mg daily for 4 weeks; 200 mg daily for 11months). Complete
resolution of skin involvement wasnotedin 4 patients following 9
and 12 months of therapy.The mechanism of action of minocycline in
SSc remainsunknown.47 This is an unexpected result and should
bepursued further with controlled trials.
PsoralenUV-A
A small uncontrolled study48
treated 4 patients with SScwith psoralenUV-A (total dosage,
3.5-9.6 J/cm2). All pa-tients showed significant improvement in
skin indura-tion, hand closure, and flexion range of fingers and
kneejoints. Because UV-A was also shown to improve local-ized
scleroderma (see thePsoralenUV-AandUV-A sub-section of the
Treatment of Localized Scleroderma sec-tion), further controlled
clinical trials are warranted.
Lung Transplantation
In a recent study,49 6 patients with limited cutaneous SScand 1
with diffuse SSc underwent lung transplantation.Five
patientswerealive after a follow-up of2 to 15 months.
These results compare favorably with the overall sur-vival
reported for lung transplantation. Furthermore, 3patients
maintained satisfactory forced vital capacity(53%-71%). This study
suggests that lung transplanta-tion is a feasible procedure and may
prolong survival ofpatients with both SSc and severe lung
involvement.
Oral Etretinate
Thirty-two patientswithchronic graft-vs-host diseasewhodidnot
respond to previous therapieswere treated with oral
(REPRINTED) ARCH DERMATOL/ VOL 138, JAN 2002
WWW.ARCHDERMATOL.COM102
2002 American Medical Association. All rights reserved.
wnloaded From: http://archderm.jamanetwork.com/ on
01/30/2014
-
8/13/2019 treatment of sclerosis systemic
5/7
etretinate in an open clinical trial. Among 27 patients
whocompleted 3 months of therapy, 24 showed improvementin skin
induration, flattening of cutaneous lesions, in-creased range of
motion, and improvement in perfor-mance status.50
Becausesclerodermalike lesions in chronicgraft-versus-host disease
closely resemble SSc, a con-trolledclinical trial investigating the
useof etretinate in thetreatment of SSc may be desirable.
Autologous Stem Cell Transplantation
Autologous stem cell transplantation has been suggestedfor the
treatment of autoimmune disease. Such a proce-dure was carried out
in a 10-year-old patient with SSc of6 years duration who did not
respond to various forms oftherapy. This patient was conditioned
with CD34+ selec-tion, cyclophosphamide, and infusionof a
CAMPATH-1Gmonoclonal antibody. After 2 yearsfollow-up, there wasa
50% improvement in skin score, disappearance of exer-tional dyspnea
and alveolitis, andimprovement in growthrate.51 Another study52
included 8 patients with severe SSctreated with high-dose
immunosuppressive therapy andradiation, followed by autologous stem
cell transplanta-
tion. After a 1-year follow-up, 5 patients were alive andshowed
improvement in skin score and in results on amodified Health
Assessment Questionnaire, while pul-monary function remained
stable. Two patients diedfrom interstitial pneumonitis, probably
related to radia-tion toxicity.
Etanercept
Tumor necrosis factor is a proinflammatory cytokineproduced by
activated T cells and macrophages. Tumornecrosis factor stimulates
the synthesis of other pro-inflammatory cytokines (IL-1, IL-8,
IL-6, and granulocyte-macrophage colony-stimulating factor),
promotes fibro-
blast proliferation, and enhancesmatrix
metalloproteinaseactivity. Specificblocking agents against
TNF-havebeendeveloped, including monoclonal antibodies
(inflix-imab)53 and a fusion protein of soluble TNF receptorlinked
to human immunoglobulin (etanercept).54 Etaner-cept has been shown
to be effective in various forms ofarthritis. In a preliminary
pilot study,55 10 patients withdiffuse SSc were treated with
etanercept, 25 mg subcu-taneously, twice weekly. After 6 months of
therapy, therewas improvement in skin score (4 patients) and
healingin digital ulcers, while pulmonary function remainedstable.
The patientssense of well-being improved, andtolerance was
good.
Thalidomide
Because thalidomide may be effective in treating
chronicgraft-versus-host disease, it was also used in an open
trialinvolving 10 patients with SSc. There was improvementin skin
repigmentation, healing of digital ulcers, re-growth of hair, and a
decrease in gastrointestinal re-flux.56 Histopathological
examination of skin suggesteda reduction in fibrosis. Immunologic
studies revealed up-regulation of CD4+ ligand in T cells and
increased ex-pression of IL-2 and IL-8.
TREATMENT OF LOCALIZED SCLERODERMA
Localized scleroderma is a connective tissue disorder
thataffects the skin and subcutaneous tissue. The disease oc-
curs in children and adults and, clinically, can be di-vided
into morphea, localized or diffuse, deep morphea,and a linear form
that usually affects arms and legs. His-topathological examination
reveals an early inflamma-tory stage consisting mostly of
mononuclear cell infil-trates and a late stage of severe
fibrosis.57 Although thecause of localized scleroderma remains
unknown, an au-toimmune mechanism is suspected because of its
fre-quent association with antinuclear antibodies, rheuma-toid
factor, antisingle-stranded DNA, and antihistoneantibodies.58
Although spontaneous resolution is pos-sible, the disease may cause
severe functional (muscleatrophy) and cosmetic (severe scarring)
disability, par-ticularly in children during the growing stage. The
treat-
ment is difficult, although new therapeutic approachesappear
encouraging (Table 2).
Topical Corticosteroids
Topical corticosteroids (fluorinated,medium potency,
andhydrocortisone) may be of some help during the earlyinflammatory
stage, although controlled clinical trials arenot available.
Intralesional triamcinolone, 5 mg/mL, oncea month for 3 months, may
improve or stop the progres-sion of morphea andlinear scleroderma
affecting thescalpand forehead (coup de sabre).
Calcitriol and Calcipotriene
Calcitriol (1,25-dihydroxyvitamin D3) and calcipo-triene are
analogues of vitamin D and have been used forthe treatment of
psoriasis. Both compounds have a simi-lar receptor binding and
affinity, although calcipotrieneis less potent and has minimal
effects on calcium me-tabolism. Besidesaffecting keratinocyte
differentiationandproliferation, calcitriol also inhibits
fibroblast prolifera-tion, collagen synthesis, and, possibly,
T-lymphocyte ac-tivation.59 Oral calcitriol, in dosages of 0.50 to
0.75 gdaily, improved joint mobility and skin extensibility in
Table 2. Treatment of Localized Scleroderma
Morphea
Corticosteroids (topical and intralesional)
Topical calcipotriene
Linear scleroderma
Corticosteroids (intralesional for coup de sabre)
PsoralenUV-A baths
UV-A alone (340-400 nm)
Oral calcitriol
Topical calcipotriene
Widespread morphea
PsoralenUV-A baths
UV-A alone (340-400 nm)
Oral calcitriol
Methotrexate
Methotrexate plus corticosteroids
(REPRINTED) ARCH DERMATOL/ VOL 138, JAN 2002
WWW.ARCHDERMATOL.COM103
2002 American Medical Association. All rights reserved.
wnloaded From: http://archderm.jamanetwork.com/ on
01/30/2014
-
8/13/2019 treatment of sclerosis systemic
6/7
adult patients with generalized morphea, following 3 to 7months
of therapy.60 In a more recent study,59 7 childrenwith linear
scleroderma were treated with this agent, and5 showedan excellent
response.Because oral calcitriol mayhavea dose-dependent effect on
calciummetabolism,moni-toring of serum and urine calcium, inorganic
phosphate,creatinine, and urea is advised, particularly when
treat-ing children.59
Topical calcipotriene ointment (0.005%) was usedin
12 patients aged 12 to 38 years with biopsy-documentedactive
morphea or linear scleroderma. After 3 months oftherapy, all
patients showed improvement, including de-creases in erythema,
telangiectases, and depigmenta-tion.61 The ointment was well
tolerated, and there wereno adverse effects. Furthermore, there
were no alter-ations in calcium metabolism as measured by serum
lev-els of ionized calcium, parathyroid hormone,
1,25-dihydroxyvitamin D3, andurinary calcium excretion.
Theseresults are encouraging but will have to be confirmed bya
controlled clinical trial.
PsoralenUV-A and UV-A
PsoralenUV-A bath phototherapy has been shown to beeffective in
the treatment of widespread morphea and lin-ear scleroderma.62 In
this study, 17 patients were evalu-ated clinically and by
ultrasound before and after treat-ment. The patients were immersed
for 20 minutes in awarm water bath containing 1 mg/L of
methoxsalen, fol-lowed by UV-A exposures, 0.2 to 0.5 J/cm2,
increased ev-ery third day to a maximum tolerable dosage of 1.2 to
3.5J/cm2. After about 15 treatments, clearance or
markedim-provement was noted in 13 of 17 patients. More recently,it
has been reported that marked improvement wasachievedin 18(75%)of
24 patientsbyusing low-doseUV-Aalone in the range of 340 to 400 nm,
20 J/cm2, toa cumu-lativedosageof 600J/cm2.63 Two patients in this
series with
subcutaneous localized scleroderma failed to respond
toUV-Atherapy. Histopathological findings corroboratedtheclinical
results. Although the mechanism of UV-A in lo-calized scleroderma
is unknown, it is noteworthythe UV-Amay activate interstitial
collagenases.64
Methotrexate
It is known that methotrexate is an effective drug for
thetreatment of rheumatoid arthritis and juvenile
rheuma-toidarthritis.65 Adult widespread morphea hasbeen
treatedwith oral methotrexate, 15 mg/wk, and the dosage
wasincreased to 25 mg/wk in resistant cases. After 24 weeksof
therapy, 6 of 9 patients showed significant improve-
ment in skin induration. There were no serious
adversereactions.66 Ten patients with active localized sclero-derma
(mean age, 6.8 years) of 4 yearsmean durationwere treatedwith
methotrexate (0.3-0.6 mg/kg per week)combined withpulse intravenous
methylprednisolone(30mg/kg for 3 days monthly). Following 3 months
of treat-ment, 9 patientsshowedsignificantbenefit, and there wereno
serious adverse effects.67 Although these data appearinteresting,
the use of methotrexate alone or in combi-nation with
corticosteroids will have to be restricted tochildren with severe
active, disabling disease.
CONCLUSIONS
Although research continues to contribute to our under-standing
of the pathogenesis of SSc, its cause is still un-known. Present
therapies are directed (1) to improve pe-ripheral blood
circulationwithvasodilators and antiplateletaggregation drugs, (2)
to prevent the synthesis and re-lease of harmful cytokines
withimmunosuppressants,and(3) to inhibit or reduce fibrosis with
agents that interfere
with collagen synthesis or enhance collagenase produc-tion.
Although some progresshas been achieved, the treat-ment of
scleroderma remains a challenge to the clinician.Further
elucidation of the events that precipitate the ini-tial activation
of theimmune system in this disease is cru-cial for the emergence
of new therapeutic approaches.
Accepted for publication May 2, 2001.Corresponding author: Raul
Fleischmajer, MD, De-
partment of Dermatology, Mount Sinai School of Medi-cine, 1425
Madison Ave, PO Box 1047, New York, NY 10029(e-mail:
[email protected]).
REFERENCES
1. Leroy EC, Black C, Fleischmajer R, et al. Scleroderma
(systemic sclerosis) clas-
sification, subsets and pathogenesis.J Rheumatol.
1988;15:202-205.
2. Fleischmajer R, Perlish JS, Reeves JRT. Cellular infiltrates
in scleroderma skin.
Arthritis Rheum. 1977;20:975-984.
3. NeedlemanBW. Increasedexpression of
intracellularadhesionmolecule I on the
fibroblasts of scleroderma patients.Arthritis Rheum.
1990;33:1847-1851.
4. Gruschwitz M, von Den Driesch P, Kellner P, et al. Expression
of adhesion pro-
teins involved in cell-cell and cell-matrix interactions in the
skin of patients with
progressive systemic sclerosis.J Am Acad Dermatol.
1992;27:169-177.
5. Gruschwitz MS, Hornstein OP, van den Driesch P. Correlation
of soluble adhe-
sion molecules in the peripheral blood of scleroderma patients
with their in situ
expression and with disease activity.Arthritis Rheum.
1995;38:184-189.
6. WhiteB. Immunopathogenesisof systemic sclerosis. Rheum Dis
ClinNorthAm.
1996;22:695-708.
7. Fleischmajer R, Perlish JS. [3H]Thymidine labeling of dermal
endothelial cells in
scleroderma.J Invest Dermatol. 1977;69:379-382.8. Leroy EC.
Systemic sclerosis:a vascular perspective. RheumDis Clin
NorthAm.
1996;22:675-694.
9. Fleischmajer R, Perlish JS, Krieg T, Timpl R. Variability in
collagen and fibro-
nectin synthesis by scleroderma fibroblasts in primary culture.J
Invest Derma-
tol. 1981;76:400-403.
10. Postlethwaitte AE. Early immune events in scleroderma. Rheum
Dis Clin North
Am. 1990;16:125-139.
11. Jimenez SA,Hitraya E, Vargas J. Pathogenesis of scleroderma:
collagen.Rheum
Dis Clin North Am. 1996;22:647-674.
12. Okano Y. Antinuclear antibody in systemic sclerosis
(scleroderma).Rheum Dis
Clin North Am. 1996;22:709-735.
13. Rodeheffer RJ, Rommer JA, Wigley F, Smith CRN. Controlled
double-blind trial
of nifedipine in the treatment of Raynaud s phenomenon.N Engl J
Med. 1983;
308:880-883.
14. Raynauds Treatment Study Investigators. Comparison of
sustained-release ni-
fedipine and temperature biofeedback for treatment of primary
Raynaud phe-
nomenon: results from a randomized clinical trial with 1-year
follow-up. ArchIntern Med. 2000;160:1101-1108.
15. Dziadzio M, DentonCP, Smith R, Blann HK,BowersE, Black
CM.Losartan therapy
for Raynauds phenomenon and scleroderma: clinical and
biochemical findings
in a fifteen-week, randomized, parallel-group, controlled trial.
Arthritis Rheum.
1999;42:2646-2655.
16. Rademaker M, Cooke ED, Almond NE, et al. Comparison of
intravenous infu-
sions of iloprost and oral nifedipine in treatment of Raynaud s
phenomenon in
patients with systemic sclerosis: a double blind randomised
study. BMJ. 1989;
298:561-564.
17. Belch JJ, Capell HA, Cooke ED, et al. Oral iloprost as a
treatment for Raynaud s
syndrome:a double blind multicentreplacebocontrolled study.
AnnRheum Dis.
1995;54:197-200.
(REPRINTED) ARCH DERMATOL/ VOL 138, JAN 2002
WWW.ARCHDERMATOL.COM104
2002 American Medical Association. All rights reserved.
wnloaded From: http://archderm.jamanetwork.com/ on
01/30/2014
-
8/13/2019 treatment of sclerosis systemic
7/7
18. Black CM, Hazkier-Sorensen L, Belch JJ, et al. Oral iloprost
in Raynauds phe-
nomenon secondary to systemic sclerosis: a multicenter,
placebo-controlled
dose-comparison study.Br J Rheumatol. 1998;37:952-960.
19. Wigley FM, Korn JN, Csuka ME, et al. Oral iloprost treatment
in patients with
Raynauds phenomenon secondary to systemicsclerosis:a
multicenter,placebo-
controlled, double-blind study.Arthritis Rheum.
1998;41:670-677.
20. Steigerwald JC. Chlorambucil in the treatment of progressive
systemic sclero-
sis. In: Block CM, Myers AR, eds. Systemic Sclerosis
(Scleroderma). New York,
NY: Gower Medical Publishing Ltd; 1985:423-427.
21. Furst DE, Clements PJ, Hill S, et al. Immunosuppression with
chlorambucil ver-
susplacebofor scleroderma:resultsof a three-year parallel,
randomized,double-
blind study.Arthritis Rheum. 1989;32:584-593.
22. van den Hoogen FH, Boerbooms AM, Swaak AJ, Rasker JJ, van
Lier HJ, van de
Putte LB. Comparison of methotrexate with placebo in the
treatment of sys-
temic sclerosis: a 24 week randomized double-blind trial,
followed by a 24 week
observational trial.Br J Rheumatol. 1996;35:364-372.
23. Degiannis D, Seibold JR, Czarnecki M, Raskova J, Raska K.
Soluble interleu-
kin-2 receptors in patients with systemic sclerosis: clinical
and laboratory cor-
relation.Arthritis Rheum. 1990;33:375-380.
24. NeedelmanBW, Wigley FM, StairRW. Interleukin-1,
interleukin-2, interleukin-4,
interleukin-6, tumor necrosis factorand interferon-levels in
sera from pa-
tients with scleroderma.Arthritis Rheum. 1992;35:67-72.
25. Clements PJ, Lachenbruch PA, Sterz M, et al. Cyclosporine in
systemic sclero-
sis.Arthritis Rheum. 1993;36:75-83.
26. RockAH, Freundlich B, JegasothyBV, et al.Treatmentof
systemic sclerosiswith
extracorporeal photochemotherapy: results of a multicenter
trial. Arch Derma-
tol. 1992;128:337-346.
27. Enomoto DN, Mekkes JR, Bossyt PM, et al. Treatment of
patients with systemic
sclerosis with extracorporeal photochemotherapy (photopheresis).
J Am Acad
Dermatol. 1999;41:915-922.
28. Sinclair HD, Williams JD, Rahman MA. Clinical efficacy of
antithymocyte globu-
lin in systemic sclerosis:results of a placebo-controlled
trial[abstract]. Arthritis
Rheum. 1994;36(suppl):s217.
29. Steen VD, Medsger TA Jr, Rodnan GP. D-penicillamine therapy
in progressive
systemicsclerosis (scleroderma): a retrospective analysis.
AnnInternMed. 1982;
97:652-659.
30. Clements PJ,Furst DE,Wong WK,et
al.High-doseversuslow-doseD-penicillamine
in early diffuse systemic sclerosis.Arthritis Rheum.
1999;42:1194-1203.
31. Chetrit-Ben E, Levy M. Colchicine: 1998 update.Semin
Arthritis Rheum. 1998;
28:48-59.
32. Alarcon-Segovia D, Ramos-Niembro F, Ibanez de Kasep G,
Alocer J, Perez-
Tamayo R. Long-term evaluation of colchicine in the treatment of
scleroderma.
J Rheumatol. 1979;6:705-712.
33. Hunzelmann N, Anders S, Fierlberg G, et al. Systemic
scleroderma: multicenter
trial of 1 year of treatment with recombinant interferon
gamma.Arch Dermatol.
1997;133:609-613.
34. Polisson RP, Gilkeson GS, Pyun EH, Pisetsky DS, Smith EA,
Simon LS. A mul-
ticenter trial of recombinant human interferon gamma in patients
with systemic
sclerosis: effects on cutaneousfibrosisand interleukin 2
receptor levels. J Rheu-
matol. 1996;23:654-658.
35. Grassegger A, Schuler G, Hessenberger G, et al.
Interferon-gamma in the treat-
ment of systemic sclerosis: a randomized controlled multicentre
trial.B r
J Dermatol. 1998;139:639-648.
36. Black CM, Silman AJ, Herrick AI, et al. Interferon-alpha
does not improve out-
come at one year in patients with diffuse cutaneous scleroderma:
results from a
randomized, double-blind, placebo-controlled trial. Arthritis
Rheum. 1999;42:
299-305.
37. Unemori EN,PickfordLB, Salles AL,et al.Relaxininduces an
extracellularmatrix-
degrading phenotype in human lung fibroblasts in vitro and
inhibits lung fibro-
sis in a murine model in vivo. J Clin Invest.
1996;98:2739-2745.
38. Seibold JR,KornJH,ClementsPJ, etal.
Recombinanthumanrelaxinin thetreat-
ment of scleroderma: a randomized, double-blind,
placebo-controlled trial.Ann
Intern Med. 2000;132:871-879.
39. Whitman HH III, CaseDB, Laragh JH,et al.Variableresponse to
oralangiotensin-
convertingenzymeblockadein hypertensive sclerodermapatients.
ArthritisRheum.
1982;25:241-248.
40. Alpert MA, Pressly TA, Mukerji V, Lambert CR, Mukerji B.
Short- and long-term
hemodynamic effects of captopril in patients with pulmonary
hypertension and
selected connective tissue disease.Chest.
1992;102:1407-1412.
41. Chang YJ, Spiera H. Renal transplantation in
scleroderma.Medicine. 1999;78:
382-385.
42. Badesch DB, Tapson VF, McGoon MD, et al. Continuous
intravenous epopros-
tenol for pulmonary hypertension due to the scleroderma spectrum
of disease:
a randomized, controlled trial.Ann Intern Med.
2000;132:425-434.
43. dela MataJ, Gomez-Sanchez MA,AranzanaM, Gomez-ReinoJJ.
Long-termilo-
prost infusion therapy for severe pulmonary hypertension in
patients with con-
nective tissue diseases.Arthritis Rheum. 1994;37:1528-1533.
44. Silver EM, Warrick JH, Kinsella MB, Staudt LS, Baumann HM,
Strange C. Cyclo-
phosphamideand low-dose prednisonetherapy in patients
withsystemic sclerosis
(scleroderma) with interstitial lung disease. J Rheumatol.
1993;20:838-844.
45. Akesson A, Scheja A, Lundin A, Wollheim FA. Improved
pulmonary function in
systemicsclerosisafter treatmentwith cyclophosphamide. Arthritis
Rheum. 1994;
37:729-735.
46. White B, Moore WC, Wigley FM, Xiai HQ, Wise RA.
Cyclophosphamide is
associated with pulmonary function and survival benefit in
patients with sclero-
derma and alveolitis.Ann Intern Med. 2000;132:947-954.
47. Le CH, Morales A, Trentham DE. Minocycline in early diffuse
scleroderma.Lan-
cet. 1998;352:1755-1756.
48. Kanekurat T, Fukumaru S, Matsushita S, Terask K, Mizoguchis
S, Kanzaki T.
Successful treatment of scleroderma with PUVA therapy.J
Dermatol. 1996;23:
455-459.
49. SchachnaL, WigleyFM, White B, GelberAC, Rosas I, OrensJB.
Lung transplan-
tation in scleroderma:the Johns Hopkinsexperience [abstract].
Arthritis Rheum.
2000;43(suppl):s392.
50. Marcellus DC, Altomonte VL, Farmer ER, et al. Etretinate
therapy for refractory
sclerodermatous chronic graft-versus-host disease.Blood.
1999;93:66-70.
51. Martini A, Maccario R, Ravelli A, et al. Marked and
sustained improvement two
years after autologous stem cell transplantation in a girl with
systemic sclero-
sis.Arthritis Rheum. 1999;42:807-811.
52. Furst DE, McSweeney P, Nash R, et al. High-dose
immunosuppressive therapy(HDIT)withautologousstem
celltransplantation (SCT)for systemic sclerosis(SSc):
results in the first 8 patients [abstract].Arthritis Rheum.
2000;43(suppl):s392.
53. Elliott MJ, Maini RN, Feldmann M, et al. Randomised
double-blind comparison
of chimeric monoclonal antibody to tumour necrosis factor (cA2)
versus pla-
cebo in rheumatoid arthritis.Lancet. 1994;344:1105-1110.
54. Spencer-Green G. Etanercept (Enbrel): update on therapeutic
use. Ann Rheum
Dis. 2000;59(suppl 1):i46-i49.
55. EllmanMH, McDonaldPA, Hayes FA.Etanercept as treatment
fordiffuse sclero-
derma: a pilot study [abstract].Arthritis Rheum.
2000;43(suppl):s392.
56. Oliver SJ,Moreira A, Kaplan G. Reducedfibrosisand
normalizationof skinstruc-
turein scleroderma patientstreatedwith thalidomide[abstract].
Arthritis Rheum.
1999;42(suppl):s187.
57. Fleischmajer R, Nedwich A. Generalized morphea: histology of
the dermis and
subcutaneous tissue.Arch Dermatol. 1972;106:509-514.
58. Arnett FC, Tan FK, Yosef U, et al. Autoantibodies to the
extracellular matrix mi-
crofibrillar protein fibrillin-1 in patients with localized
scleroderma. Arthritis
Rheum. 1999;42:2656-2659.59. ElstEF, VanSuijlekom-Smit
LW,OranjeAP. Treatmentof linear scleroderma with
oral 1,25-dihydroxyvitamin D3 (calcitriol) in seven
children.Pediatr Dermatol.
1999;16:53-58.
60. Hulshof MM, Pavel S, Breedveld FC, Dijkmans AC, Vermeer BJ.
Oral calcitriol as
a new therapeutic modality for generalized morphea.Arch
Dermatol. 1994;130:
1290-1293.
61. Cunningham BB, Landells IDR, Langman C, Sailer DE, Paller
AS. Topical calci-
potriene for morphea/linear scleroderma.J Am Acad Dermatol.
1998;39(pt 2):
211-215.
62. Kerscher M, Meurer M, Sander C, et al. PUVA-bath
photochemotherapy for lo-
calized scleroderma.Arch Dermatol. 1996;132:1280-1282.
63. Kerscher M, Volkenandt M, Gruss C,et al.Low-dose
phototherapyfor treatment
of localized scleroderma.J Am Acad Dermatol. 1998;38:21-26.
64. Wlaschek M, Briviba K, StricklinP, SiesH,
Scharffetter-KochanekK. Singlet oxy-
gen may mediate the ultraviolet-Ainduced synthesis of
interstitial collagenase.
J Invest Dermatol. 1995;104:194-198.
65. Wallace CA. The use of methotrexate in childhood rheumatic
diseases. ArthritisRheum. 1998;41:381-391.
66. SeygerMMB, vanden HoogenFHJ,de BooT, Elke MGJ, de Jong
MD.Low-dose
methotrexate in the treatmentof widespread morphea.J Am Acad
Dermatol. 1998;
39:220-225.
67. Uziel Y, Feldman BM, Krafchik BR, Yeung RS, Laxer RM.
Methotrexate and cor-
ticosteroid therapy for pediatric localized scleroderma. J
Pediatr. 2000;136:91-
95.
(REPRINTED) ARCH DERMATOL/ VOL 138, JAN 2002
WWW.ARCHDERMATOL.COM105
2002 American Medical Association. All rights reserved.