Embed Size (px)
Citation preview

Treatment of Lower Eyelid Malposition withDermis Fat Grafting
Bobby S. Korn, MD, PhD,1 Don O. Kikkawa, MD,1 Steven R. Cohen, MD,2 Morris Hartstein, MD,3
Christine C. Annunziata, MD1
Purpose: To report a new technique in the repair of lower eyelid malposition using dermis fat as a posteriorlamellar spacer graft.
Design: Retrospective, consecutive, nonrandomized interventional case series.Participants: Eleven patients who underwent surgical correction for symptomatic lower eyelid malposition
using dermis fat as a spacer graft.Methods: Patients with symptomatic lower eyelid malposition after blepharoplasty, trauma, craniofacial
syndromes, and human immunodeficiency virus-associated lipodystrophy were treated with midfacial liftingcombined with dermis fat posterior lamellar spacer grafting.
Main Outcome Measures: Preoperative and postoperative measurements of eyelid position, margin-to-reflex distance (defined as the distance from the upper eyelid to the central corneal light reflex and the distancefrom the lower eyelid to the corneal light reflex), lagophthalmos, corneal staining, presence of ocular surfacesymptoms, and patient satisfaction.
Results: All patients who underwent dermis fat spacer grafting during lower eyelid malposition repair notedimprovement in ocular surface symptoms and restoration of normal eyelid position.
Conclusions: Dermis fat is a novel posterior lamellar spacer graft and offers numerous advantages overconventional lower eyelid spacer grafts for repair of lower eyelid malposition. Ophthalmology 2007;xx:xxx © 2007by the American Academy of Ophthalmology.
ARTICLE IN PRESS
Lower eyelid malpositions are vexing conditions facingpatients and are among the most challenging conditionsfacing surgeons. The causes of lower eyelid malposition arevaried and include postblepharoplasty eyelid retraction,posttraumatic eyelid retraction, volume loss, and eyelidretraction seen in human immunodeficiency virus (HIV)-associated lipodystrophy and congenital eyelid colobo-mas.1–3 These malpositions can result in both symptomatickeratopathy and unacceptable cosmetic appearance.
There are multiple mechanisms responsible for eyelidmalpositions. In the case of postblepharoplasty eyelid re-traction, excess removal of skin (anterior lamella), scarringof the orbital septum (middle lamella), and unrecognizedlower eyelid laxity are among the causative factors.4 Thereare numerous methods of lower eyelid malposition repair.Common to many of these methods is the use of poste-rior lamellar spacer grafts such as hard palate mucosa,
Originally received: February 19, 2007.Final revision: June 22, 2007.Accepted: June 26, 2007.Available online: ●●●. Manuscript no. 2007-231.1 Division of Ophthalmic Plastic and Reconstructive Surgery, Departmentof Ophthalmology, Shiley Eye Center University of California, San Diego,La Jolla, California.2 Division of Plastic and Reconstructive Surgery, University of California,
San Diego, La Jolla, California.© 2007 by the American Academy of OphthalmologyPublished by Elsevier Inc.
ear cartilage, and acellular dermis in conjunction with mid-face lifting and lower eyelid tightening.5–7 Each of thesespacer grafts has inherent complications with its use.
The use of dermis fat as a composite graft has been welldescribed in anophthalmic orbits.8,9 However, there havebeen few reports of its use in functional orbits and none asa lower eyelid spacer graft. Several features make autolo-gous dermis fat a suitable spacer graft, including the abilityto supply both posterior lamella on the dermis face, volumeon the fat side, no risk of a transmissible agent, and lowincidence of tissue rejection.
In this study, the efficacy of dermis fat was evaluated asa posterior lamellar spacer graft during the repair of lowereyelid malpositions. Eleven patients with lower eyelid mal-positions from various causes were evaluated, treated withdermis fat grafting to the lower eyelid, and followed upclinically.
3 Division of Ophthalmic Plastic and Reconstructive Surgery, St. LouisUniversity School of Medicine, St. Louis, Missouri.
Supported by grants from the Bell Charitable Foundation, Rancho SantaFe, California; Fenley family, in honor of Joseph B. Fenley; and Howardand Toby Cohen family. These funding organizations had no role in thedesign or conduct of the research.
The authors have no proprietary interests related to the article.
Correspondence to Bobby S. Korn, MD, PhD, Shiley Eye Center, Depart-ment of Ophthalmology, University of California, San Diego, 9415 Cam-
pus Point Drive, La Jolla, CA 92093-0946. E-mail: [email protected].1ISSN 0161-6420/07/$–see front matterdoi:10.1016/j.ophtha.2007.06.039

Ophthalmology Volume xx, Number x, Month 2007ARTICLE IN PRESS
Patients and Methods
Patients
This study was approved by the Institutional Human Re-search Protections Program and conforms to the principlesoutlined in the Declaration of Helsinki. The medical recordsof 11 patients with lower eyelid malposition were reviewedretrospectively over a 1-year period, noting age, gender,past medical and surgical history, details from ophthalmicexamination, follow-up interval, and external photographs.The ophthalmic data included the presence of ocular symp-toms, visual acuity, eyelid position, margin-to-reflex dis-tance (defined as the distance from the upper eyelid to thecentral corneal light reflex and the distance from the lowereyelid to the corneal light reflex), lagophthalmos, and cor-neal staining.
Review of Literature
A search of the PubMed database was performed to deter-mine if there were previously published reports using der-mis fat as a spacer graft for lower eyelid malposition. Thekey words used were dermis fat and eyelid. In this manner,25 publications were identified, most of which detailed itsuse in the anophthalmic orbit and none describing the use ofdermis fat in lower eyelid malposition repair. When thesearch was refined further to include malposition or retrac-tion, no publications were found.
Lower Eyelid Retraction Repair and MidfaceSuspension Technique
To facilitate exposure, a lateral canthotomy and inferiorcantholysis was performed. A transconjunctival incisionthen was made beneath the inferior tarsal border. All scartissue was liberated extensively to the arcus marginalis. Theorbitomalar ligament then was released completely with acombination of blunt dissection and electrocautery along theanterior aspect of the inferior orbital rim. If a midface liftwas performed, a subperiosteal dissection plane then wascreated and extended inferiorly to liberate the entire mid-face. Next, an upper eyelid crease incision was made andblunt dissection was performed inferolaterally along thepreperiosteal plane to communicate with the lower eyelidincision. A 5-0 polygalactin suture (Ethicon, Inc., Piscat-away, NJ) then was anchored to the suborbicularis oculi fatto achieve an optimal superolateral traction vector. A finehemostat then was used to direct the suture under the lateralcanthal tissues through the upper eyelid crease incision.This suborbicularis oculi fat suture then was secured to theperiosteum at the level of the frontozygomatic suture. Aslight overcorrection is desirable, allowing for postoperativedescent.
Harvest of Dermis Fat Graft
The source of dermis fat for lower eyelid reconstruction wasthe hip, inferior and posterior to the superior iliac crest. Thesize of the graft used depended on the degree of lower
eyelid retraction as well as the amount of lower eyelid2
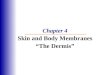
volume loss. In general, an ellipse measuring 25�50 mmwas marked on the skin. After marking the ellipse of skin,a diamond burr rotating at 20 000 rpm was used to denudethe epithelium with the Stryker Total Performance Systemhand piece (Stryker, Inc., Kalamazoo, MI). The drill wasused to burr down to the level of the deep dermis, and theend point of debridement was a fine, uniform hyperemiaof the underlying dermis (Fig 1A). After removal of theepithelium, the graft was removed with sharp dissection andthe underlying defect was closed with absorbable sutures(Fig 1B).
Dermis Fat Graft PlacementThe dermis fat graft was trimmed down to size and volumeafter in situ placement. The nasal and lateral edges of thegraft were tapered and placed with the dermis side facingthe ocular surface and the fat side directed anteriorly. Fig 1Cshows the orientation of the graft with respect to the fornix.The graft was anchored deep in the fornix and secured to thecut edges of the conjunctiva with interrupted 6-0 fast-absorbing gut suture (Ethicon, Inc.). If any lower eyelidlaxity was present, a lateral tarsal strip procedure was per-formed. In cases of severe lower eyelid retraction of�3 mm, the lower eyelid was placed on stretch with a Frostsuture on foam bolsters and the eye was patched for 1 week(Fig 1D). Because of the necessity of prolonged occlusionfrom the Frost suture, eyelid malposition repairs were per-formed one side at a time.
Results
Repair of lower eyelid malpositions using dermis fat as aspacer graft was performed in a total of 11 cases, dividedinto 4 groups: postblepharoplasty, trauma, congenital eyelidmalposition, and HIV-associated lipodystrophy. Each of thegroups was treated according to the degree of eyelid retrac-tion and lagophthalmos present. The following patients arerepresentative cases in each group.
The first group consisted of the post-blepharoplasty eye-lid retraction. Table 1 (available at http://aaojournal.org)summarizes the clinical findings and treatments for eachpatient. All patients had blurred vision and foreign bodysensation in one or both eyes at presentation. On examina-tion, each patient exhibited inferior scleral show with lowereyelid retraction, lagophthalmos, and punctate keratopathyon the affected side despite aggressive ocular lubrication.
Case 1 had symptomatic exposure keratopathy on theright side after transcutaneous lower eyelid blepharoplastyat presentation. She previously underwent failed lower eye-lid retraction repair using mucosal hard palate grafting.Adnexal examination revealed 1 mm of lagophthalmos andinferior scleral show in the right eye. A transconjunctivalrelease of the lower eyelid cicatrix was performed combinedwith dermis fat spacer grafting and midface suspension onthe right eyelid. After surgery, the patient noted completeresolution of her ocular symptoms. Fig 2 shows restorationof the normal lower eyelid position on the right eyelid onfrontal view and elevation of the lateral eyelid on side view.
The patient remained stable at 1-year follow-up.
Korn et al � Treatment of Lower Eyelid Malposition with Dermis Fat GraftingARTICLE IN PRESS
Case 2 is an example of severe bilateral exposure keratopa-thy symptoms after transcutaneous lower eyelid blepharo-plasty. On examination, she had 2 mm of lagophthalmos,lower eyelid retraction, and shortage of lower eyelid anteriorlamella. Slit-lamp examination revealed marked punctatestaining and neovascularization of the inferior cornea. Lowereyelid retraction repair was performed with a large, 12�25-mm dermis fat graft combined with midface lifting. At 9months of follow-up, the patient remained free of exposurekeratopathy symptoms and showed restoration of normaleyelid position and closure (Fig 3).
In the next group of patients, dermis fat grafting wasused for posttraumatic lower eyelid retraction. Case 5 wasreferred for lower eyelid malposition 2 years after a motorvehicle accident. He previously underwent orbital floorfracture repair with a titanium mesh implant. On examina-tion, there was right malar hypoplasia, lower eyelid retrac-
Figure 1. A, Photograph showing debridement of epithelium. After marepithelial surface. Debridement continues until a fine hyperemia of the ungraft. The graft is initially oversized because of shrinkage after harvestinginto inferior fornix. The graft is oriented with dermis side toward the ocucut edges of the conjunctiva with interrupted sutures deep in the fornix.immobilize the eyelid for 1 week after surgery. Two 5-0 polypropylene sutabove the brow on foam bolsters.
tion, hypoglobus, and cicatricial entropion of the lower
eyelid. A lateral canthotomy and inferior cantholysis wasperformed, followed by transconjunctival release. A densecicatrix in the inferior fornix was present and anchored tothe titanium mesh. All scar tissue was liberated from theorbital implant, and a subperiosteal dissection plane wascreated. The midface was fixated to the frontozygomaticperiosteum with 2 separate sutures for added support. Basedon the amount of posterior lamella shortening and volumedeficit, a large graft, measuring 15�30 mm on the dermisface and 20 mm in thickness of the subcutaneous fat, wassecured to the cut edges of the conjunctiva. Overcorrectionof both the lower eyelid retraction and volume loss was thegoal. At 6 months of follow-up, resolution of the cicatricialentropion, lower eyelid retraction, and volume loss werenoted (Fig 4).
The third group of patients consisted of those withlower eyelid malpositions seen in craniofacial syn-
an ellipse of skin, a high-speed diamond tip burr is used to remove theng dermis is noted. B, Photograph showing gross appearance of dermis fats contoured in situ. C, Photograph showing placement of dermis fat graftrface and the fat side directed anteriorly. The graft then is secured to thehotograph showing temporary closure of eyelid. Frost sutures are used tore passed from the lower tarsus and through the upper tarsus and fixated
kingderlyiand ilar suD, Pures a
dromes. Case 10 is a typical example of a patient with
3

) the
Ophthalmology Volume xx, Number x, Month 2007ARTICLE IN PRESS
Treacher-Collins syndrome who exhibited lower eyelidretraction and lagophthalmos. Right lower eyelid short-ening, midfacial lifting, and dermis fat grafting wereperformed (Fig 5). After surgery, the patient had marked
Figure 2. A, Preoperative photograph of case 1 showing right lower eyelposition on the right panel after dermis fat grafting and midface lifting. Clower eyelid retraction on (D) the postoperative view compared with (C
Figure 3. A, Preoperative photograph of case 2 showing marked bilatera
sequential dermis fat grafting and midface elevation showing a return of norm4
improvement in her lower eyelid retraction and midfacialhypoplasia that remained stable at the 1-year follow-up.In Fig 5, the fullness of the left lower eyelid in thepreoperative photograph is the result of prior injection of
raction. B, Postoperative photograph of case 1 showing improved eyelidhotographs of case 1 showing, on the side view, marked improvement inpreoperative view.
r eyelid retraction. B, Postoperative photograph of case 2 obtained after
id ret, D, P
l lowe
al lower eyelid position.
Korn et al � Treatment of Lower Eyelid Malposition with Dermis Fat GraftingARTICLE IN PRESS
hyaluronic acid gel, which dissipated on long-term post-operative photographs.
In the fourth group, dermis fat grafting was applied to thelower eyelid retraction and fat atrophy seen in the setting ofHIV-associated lipodystrophy. Case 11 had bilateral lowereyelid retraction, lagophthalmos, and deep superior sulcusresulting from atrophy of orbital fat (Fig 6A, C, E). Bilaterallower eyelid dermis fat grafting and canthoplasty withoutmidface lifting was performed. After surgery, the patienthad marked improvement in eyelid position. The frontalview in Fig 6 shows improvement in the lower eyelidretraction as well as resolution of lagophthalmos and thesuperior sulcus deficit (Fig 6B, D, F). The side view dem-onstrates how the augmentation of dermis fat graft elevatesthe lower eyelid and restores a more natural appearance. At9 months of follow-up, the patient remained stable with nofurther periocular lipodystrophy despite continued antiret-roviral treatment.
For each group, all patients noted improvement in for-eign body sensation and blurred vision, if present, andreported less use of topical lubricants. Furthermore, all ofthe patients reported marked cosmetic improvement andhigh satisfaction after the reconstructive surgery.
Figure 4. A, Preoperative photograph of case 5 showing that the patieB, Postoperative photograph of case 5 obtained after midface lifting,improvement.
Figure 5. A, Preoperative photograph of case 10 showing right lower eobtained after dermis fat grafting, midface lifting, and lateral canthoplasty
fullness in the right panel.Discussion
To the best of the authors’ knowledge, this is the first reportthat describes the use of dermis fat as a posterior lamellargraft for the repair of lower eyelid malposition. Althoughdermis fat has been used successfully for many years inanophthalmic orbits, its application for lower eyelid malpo-sitions has not been well described.
Mucosal hard palate has been used successfully as alower eyelid spacer since its initial description in 1985.10
However, there are several complications that can arisefrom usage of hard palate, principally at the donor site. Oro-nasal fistula formation and donor site candidiasis were notedin 2 cases, whereas others have reported donor site granu-loma formation, chronic mucoid discharge, prolonged donorsite hemorrhage, and formation of torus palatinus.11–13 Ad-ditionally, leukoplakic changes and prolonged gingivalbleeding were noted in 1 patient who underwent hard palategraft harvesting. Subsequent histopathologic examination ofthe mucosal graft demonstrated invasive stage I, grade 3squamous cell carcinoma that was present in the originalgraft.12 Ocular complications include graft keratinizationcausing ocular surface irritation and potential infection fromoronasal flora.14
s cicatricial right lower eyelid retraction, entropion, and hypoglobus.ized dermis fat grafting, and lower eyelid tightening showing marked
retraction and lagophthalmos. B, Postoperative photograph of case 10e right eyelid showing marked improvement in lower eyelid position and
nt haovers
yelidto th
5

Ophthalmology Volume xx, Number x, Month 2007ARTICLE IN PRESS
Acellular dermis is another widely used spacer graft forlower eyelid retraction repair and is derived from humancadaveric dermis.15 The primary advantage of acellular der-mis is its immediate commercial availability without theneed to harvest from a second surgical site. However, acel-lular dermis has a postoperative contraction rate of 57% andcan demonstrate growth of fine hairs.15,16 Finally, there isthe theoretical risk of transmission of an infectious agentand possible immunogenic rejection despite postharvesttesting and processing.
The principle concerns with use of dermis fat grafting are
Figure 6. A, Preoperative photograph of case 11 showing lower eyelid retrof case 11 obtained after dermis fat grafting and lateral canthoplasty sphotographs of case 11 showing, on the side views, lower eyelid retraction aand elevation of the lower eyelids after dermis fat graft placement.
surface keratinization and growth of hairs leading to ocular
6
surface complications.17 Hair follicles exist primarily in theepithelium and, to a smaller degree, in the early dermis.18 Inthis series, the authors specifically looked for, but did notnote, any ocular surface irritation from dermis fat grafting.This may be technique dependent. The removal of theepidermis traditionally has been performed using mechani-cal debridement with a blade or a carbon dioxide resurfac-ing laser.19,20 The latter approach may be expected to pro-duce a more uniform removal of the epithelium; however,this would require multiple passes to reach the level of thedeep dermis and may be associated with higher risk of
n, superior sulcus deficit, and lagophthalmos. B, Postoperative photographg restoration of lower eyelid volume and position. C, E, Preoperativelume loss. D, F, Postoperative photographs of case 11 showing the fullness
actiohowinnd vo
thermal injury. The authors performed mechanical debride-

Korn et al � Treatment of Lower Eyelid Malposition with Dermis Fat GraftingARTICLE IN PRESS
ment of the epithelium using a high-speed diamond tip toburr down to the level of the deep dermis. They believe thatthis is essential to avoid graft complications. In this manner,they have not observed any postoperative hair growth, sur-face keratinization, or any major complications. Further-more, meticulous end-to-end approximation of the dermisside of the graft with the conjunctival edge allows foruniform migration of the conjunctival epithelial cells overthe dermal graft surface. Finally, the graft is placed deep inthe fornix, where corneal apposition is minimal.
The authors also applied dermis fat grafting to lowereyelid malpositions resulting from rare causes. Long-termtreatment of HIV infection with highly active antiretrovi-ral therapy can be associated with lipodystrophy andmuscle wasting.21 In particular, facial lipodystrophy is awell-recognized stigma of chronic HIV infection, andnumerous treatments have been reported including recom-binant human growth hormone and a variety of filler mate-rials.2 An often unrecognized complication of HIV-associatedlipodystrophy and muscle wasting is orbital fat hollowingand eyelid retraction.22 None of the prior treatments forfacial lipodystrophy has addressed the periocular complica-tions observed with HIV infection. The authors performeddermis fat grafting in a patient (case 11) with severe eyelidretraction and orbital fat atrophy with excellent functionaland cosmetic improvement, and at 9 months of follow-up,the dermis fat graft remained stable. Because follow-up wasnot more than 1 year, the longevity of the dermis fat graft inthe setting of continued antiretroviral therapy remainsunknown.
In addition to HIV-associated lipodystrophy, dermis fatgrafting was applied to the lower eyelid malpositions seenin Treacher-Collins (mandibulofacial dysostosis) syndrome.Lower eyelid colobomas, eyelid retraction, lateral canthaldystopia, and maxillary hypoplasia are some of the perioc-ular malpositions seen in Treacher-Collins syndrome.3 Avariety of treatments have been described, including autol-ogous bone grafting, alloplastic augmentation of the maxillaand zygoma, subcutaneous dermis grafting, and Z-plastyand musculocutaneous eyelid flaps.23 Dermis fat grafting tothe lower eyelid previously was reported, but often requiresrepeat grafting owing to graft resorption.24 The use ofdermis fat in this study differs from that of previouslyreported studies. First, the dermis side was used as a spacergraft in conjunction with lower eyelid retraction repair andmidface suspension. Additionally, a large adipose bed washarvested to supply volume in the lower eyelid. In thismanner, no significant decrease in volume or return of lidretraction was observed at 1 year of follow-up.
Dermis fat has many advantages over other spacer ma-terials in the repair of lower eyelid retraction. First, no otherspacer graft singly can provide both posterior lamellar aug-mentation as well as volume replacement. Compared withthe hard palate, the size of the dermis fat graft is virtuallyunlimited, and healing of the donor site is more comfort-able. Isolated fat pearls or subcutaneous fat injections aresusceptible to numerous complications, including graft re-sorption and an irregular texture. Furthermore, the authorsbelieve that the presence of adipose tissue on the dermis
face may play an important role in long-term surgical suc-cess partly because of an antifibrotic effect on the middlelamella. In postblepharoplasty eyes and traumatic eyelidmalposition, exuberant scarring of the middle lamella of thelower eyelid is a principle driving force for lower eyelidretraction. Complete and meticulous lysis of this middlelamellar cicatrix and prevention of subsequent scarring isessential for a successful outcome. The authors postulatethat the presence of adipose tissue on the dermis face mayplay a role in this long-term success. During the cicatricialphase of wound healing, the fat may serve as an antiinflam-matory buffer to prevent subsequent scarring.
This series is limited by its retrospective nature and thesmall sample size of 11 patients. The follow-up period alsois limited, and despite no evidence of surface keratinizationor new hair growth, these complications may arise at timepoints longer than the follow-up period. Furthermore, ahead-to-head prospective comparison of dermis fat com-pared with other spacer materials in fellow eyes to deter-mine which is the superior graft was not performed.
Future studies are planned to observe patients for periodsof more than 1 year. Long-term surgical correction will beevaluated, and signs of late dermal keratinization, hairgrowth, and evidence of graft fat atrophy will be monitored.Additional studies will address the efficacy of dermis fatgrafting for eyelid retraction secondary to thyroid-relatedorbitopathy, and a prospective, randomized study will bedesigned to evaluate the efficacy of dermis fat comparedwith other grafts. Serial orbital imaging will be performed todetermine the rate of resorption of the dermis and fat com-ponents. Finally, the authors plan to compare the efficacy ofdermis fat harvested from different donor sites.
In summary, dermis fat grafting is an excellent adjunct inlower eyelid malposition repair, restores normal eyelidfunction, and provides a well-received cosmetic outcome.
References
1. Kikkawa DO, Kim JW. Lower-eyelid blepharoplasty. Int Oph-thalmol Clin 1997;37:163–78.
2. Engelhard P. Correction options for lipoatrophy in HIV-infected patients. AIDS Patient Care STDS 2006;20:151– 60.
3. Hertle RW, Ziylan S, Katowitz JA. Ophthalmic features andvisual prognosis in the Treacher-Collins syndrome. Br J Oph-thalmol 1993;77:642–5.
4. Patel BC, Patipa M, Anderson RL, McLeish W. Managementof postblepharoplasty lower eyelid retraction with hard palategrafts and lateral tarsal strip. Plast Reconstr Surg 1997;99:1251–60.
5. Cohen MS, Shorr N. Eyelid reconstruction with hard palatemucosa grafts. Ophthal Plast Reconstr Surg 1992;8:183–95.
6. Aldave AJ, Maus M, Rubin PA. Advances in the managementof lower eyelid retraction. Facial Plast Surg 1999;15:213–24.
7. Glatt HJ. Tarsoconjunctival flap supplementation: an approachto the reconstruction of large lower eyelid defects. OphthalPlast Reconstr Surg 1997;13:90–7.
8. Hawtof D. The dermis fat graft for correction of the eyeliddeformity of enophthalmos. Mich Med 1975;74:331–2.
9. Aguilar GL, Shannon GM, Flanagan JC. Experience with
dermis-fat grafting: an analysis of early postoperative compli-7

Ophthalmology Volume xx, Number x, Month 2007ARTICLE IN PRESS
cations and methods of prevention. Ophthalmic Surg 1982;13:204–9.
10. Siegel RJ. Palatal grafts for eyelid reconstruction. Plast Re-constr Surg 1985;76:411–4.
11. Wearne MJ, Sandy C, Rose GE, et al. Autogenous hard palatemucosa: the ideal lower eyelid spacer? Br J Ophthalmol 2001;85:1183–7.
12. Pang NK, Bartley GB, Bite U, Bradley EA. Hard palatemucosal grafts in oculoplastic surgery: donor site lessons.Am J Ophthalmol 2004;137:1021–5.
13. Kim JW, Kikkawa DO, Lemke BN. Donor site complicationsof hard palate mucosal grafting. Ophthal Plast Reconstr Surg1997;13:36–9.
14. Bartley GB, Kay PP. Posterior lamellar eyelid reconstructionwith a hard palate mucosal graft. Am J Ophthalmol 1989;107:609–12.
15. Sullivan SA, Dailey RA. Graft contraction: a comparison ofacellular dermis versus hard palate mucosa in lower eyelidsurgery. Ophthal Plast Reconstr Surg 2003;19:14–24.
16. Shorr N, Goldberg RA, Hoenig J, et al. More information onAlloderm [letter]. Ophthal Plast Reconstr Surg 2001;17:
153–4.8
17. Bosniak SL. Complications of dermis-fat orbital implantation.Adv Ophthalmic Plast Reconstr Surg 1990;8:170–81.
18. Mou C, Jackson B, Schneider P, et al. Generation of theprimary hair follicle pattern. Proc Natl Acad Sci U S A 2006;103:9075–80.
19. Bonavolontà G, Tranfa F, Salicone A, Strianese D. Orbitaldermis-fat graft using periumbilical tissue. Plast ReconstrSurg 2000;105:23–6.
20. Biesman BS. Carbon dioxide laser skin resurfacing. SeminOphthalmol 1998;13:123–35.
21. Corcoran C, Grinspoon S. Treatments for wasting in patientswith the acquired immunodeficiency syndrome. N Engl J Med1999;340:1740–50.
22. Wang G, McCulley TJ. Eyelid retraction and incompleteeyelid closure secondary to human immunodeficiency virus-associated muscle wasting. Ophthal Plast Reconstr Surg 2006;22:479–80.
23. Kobus K, Wojcicki P. Surgical treatment of Treacher Collinssyndrome. Ann Plast Surg 2006;56:549–54.
24. Leipziger LS, Dufresne CR. Autogeneous and allogenic ma-terials. In: Dufresene CR, Carson BS, Zinreich J, eds. Com-plex Craniofacial Problems: A Guide to Analysis and Treat-
ment. New York: Churchill Livingstone; 1992:489–97.
Ophthalmology Volume xx, Number x, Month 2007ARTICLE IN PRESS
Group Case No.
Preoperative Marto Reflex Distan
Margin to RefleDistance2
Right L
Postblepharoplasty 1 6.0/8.0 6.02 3.5/8.0 3.5
3 1.5/8.5 1.5
4 4.0/7.5 4.0
Posttrauma 5 2.0/7.5 3.0
6 3.5/7.0 3.5
7 2.5/8.0 2.5
Congenital eyelid malposition(Treacher–Collins)
8 4.0/7.0 4.0
9 3.5/8.5 3.0
10 4.0/7.0 4.0
HIV lipodystrophy 11 5.5/7.0 5.5
HIV � human immunodeficiency virus.
Table 1. Clinical Findings and
gince1/x Preoperative
Lagophthalmos
Preoperative Symptomseft Right Left
/6.5 1 0 Foreign body sensation and poor cosmesis/8.0 2 2 Foreign body sensation, poor cosmesis,
and decreased vision/8.0 2 2 Foreign body sensation, poor cosmesis,
and decreased vision
/7.5 1 1 Foreign body sensation and poor cosmesis
/4.5 1 0 Foreign body sensation, poor cosmesis,and decreased vision
/4.0 1 0 Poor cosmesis
/4.5 2 0 Poor cosmesis
/6.0 1 0 Poor cosmesis
/7.0 2 1 Poor cosmesis
/5.5 1 0 Poor cosmesis
/7.0 2 2 Foreign body sensation and poor cosmesis
8.e1

Korn et al � Treatment of Lower Eyelid Malposition with Dermis Fat GraftingARTICLE IN PRESS
Treatments for All Patients
Treatment
Postoto Re
Ma
Right
Right midface lifting and dermis fat grafting 6.0/6.0Bilateral midface lifting and bilateral dermis fat grafting 3.5/5.0
Bilateral midface lifting, bilateral upper lid ptosis repair,and bilateral lower eyelid dermis fat grafting withlateral canthoplasty
5.0/6.0
Bilateral midface lifting, dermis fat grafting,canthoplasty, and cheek implants
4.0/6.0
Right midface lifting, lysis of lower eyelid cicatrix,dermis fat grafting, and lower eyelid shortening
3.5/4.0
Right midface lifting, lysis of lower eyelid cicatrix,dermis fat grafting, and lateral canthoplasty
3.5/6.0
Right midface lifting, lysis of lower eyelid cicatrix,dermis fat grafting, cheek implant and canthoplasty.
2.5/4.5
Right midface lifting, dermis fat grafting, and lowereyelid shortening
4.0/6.5
Bilateral midface lifting, bilateral lower eyelidshortening, bilateral lower eyelid dermis fat grafting,and bilateral lateral rim augmentation
3.5/6.5
Right midface lifting, dermis fat grafting, and lateralcanthoplasty
4.0/5.5
Bilateral dermis fat grafting and bilateral canthoplasty 5.5/5.5
perative Marginflex Distance1/
rgin to ReflexDistance2
PostoperativeLagophthalmos
Length of Follow-upLeft Right Left
6.0/6.5 0 0 1 yr3.5/5.0 0 0 9 mos
5.0/6.0 0 0 1 yr
4.0/5.5 0 0 9 mos
3.0/4.5 0 0 6 mos
3.5/4.0 0 0 8 mos
3.5/4.5 0 0 6 mos
4.0/6.0 0.5 0 1 yr
3.0/5.5 0.5 0 10 mos
4.0/5.5 0 0 1 yr
5.5/5.5 0 0 9 mos
8.e2