Embed Size (px)
Citation preview

Treatment of Internal Rotation Gait Due to GluteusMedius and Minimus Overactivity in Cerebral Palsy:
Anatomical Rationale of a New Surgical Procedure andPreliminary Results in Twelve Hips
BENJAMIN JOSEPH*
Consultant Orthopaedic Surgeon, Head of Orthopaedic Unit-II, Paediatric Orthopaedic Service, Department of Orthopaedics,Kasturba Medical College, Manipal, Karnataka, India
Spastic overactivity of the anterior fibers of the gluteus medius and minimus can result in aninternal rotation gait associated with excessive hip and pelvic rotation. The currently advocatedoperation for this problem can result in weakness of hip abduction. The anatomical features ofthe gluteal muscles suggest that this gait abnormality can be corrected by selectively reducingthe internal rotator function of the anterior fibers of the glutei without disturbing the abductorfibers. Such an operative procedure was devised and performed on 12 hips. The gait improvedin all hips without any demonstrable weakness of the hip abductor power. Clin. Anat.11:22–28, 1998. r 1998 Wiley-Liss, Inc.
Key words: cerebral palsy; internal rotators; in-toeing gait; hip; glutei; spasticity
INTRODUCTION
Internal rotation gait may not be the most disablinglocomotor aberration in cerebral palsy; nevertheless, itis unsightly and almost always involves excessiveenergy expenditure, a luxury children with cerebralpalsy can ill afford.
Factors contributing to an internal rotation gait incerebral palsy include increased femoral anteversionand spasticity of muscles. The muscles thought tocontribute to this gait abnormality include the medialhamstrings, the iliopsoas, and the gluteus medius andminimus. The surgical procedure currently advocatedfor correcting internal rotation gait due to gluteusmedius and minimus overactivity is the one devisedby Steel (1980). This procedure entails advancinganteriorly the insertion of these muscles, therebyreducing or eliminating their internal rotator function.However, the procedure also markedly reduces theabductor moment arm; and, quite predictably, Steelreported abductor weakness and a Trendelenburg gaitin some of the patients on whom this operation wasperformed.
The present report attempts to 1) analyze thepathomechanics of internal rotation gait in cerebralpalsy due to overactivity of the gluteal musculature,
2) outline the anatomical rationale of a new procedurewhich can achieve correction of the gait abnormalitywithout weakening the power of abduction, and 3)present the preliminary results of this procedure in 12hips.
PATIENTS AND METHODS
Patients with an internal rotation gait were identi-fied from among those attending the cerebral palsyclinic during the last four years. Those who, inaddition, had scissoring, crouch, or an equinus gaitwere excluded. Those who then presented with iso-lated internal rotation gait underwent a detailed evalu-ation to exclude clinical evidence of hamstring andiliopsoas tightness or spasticity. The foot progressionangles (Staheli, 1977) were recorded preoperatively.The Steel’s test was performed to demonstrate spastic-ity of the gluteus medius and minimus (Steel, 1980).The test was performed with the child lying pronewith the hips extended and the knees flexed to 90°.
*Correspondence to: Dr. Benjamin Joseph, Paediatric OrthopaedicService, Department of Orthopaedics, Kasturba Medical College,Manipal-576119, Karnataka, India.
Received 12 March 1996; Revised 5 September 1996
Clinical Anatomy 11:22–28 (1998)
r 1998 Wiley-Liss, Inc.
The flexed leg was briskly pushed into externalrotation; if spasticity of the glutei was present the limbwould rebound into internal rotation, and if spasticityof the glutei was not present the leg would remain inexternal rotation. The prone rectus test was alsoperformed to demonstrate spasticity of the rectusfemoris muscle. The passive ranges of internal andexternal rotation of the hips (with the hip in extension)were recorded with the help of a goniometer.
A careful visual assessment of the gait was madeand surface electromyography of the anterior fibers of
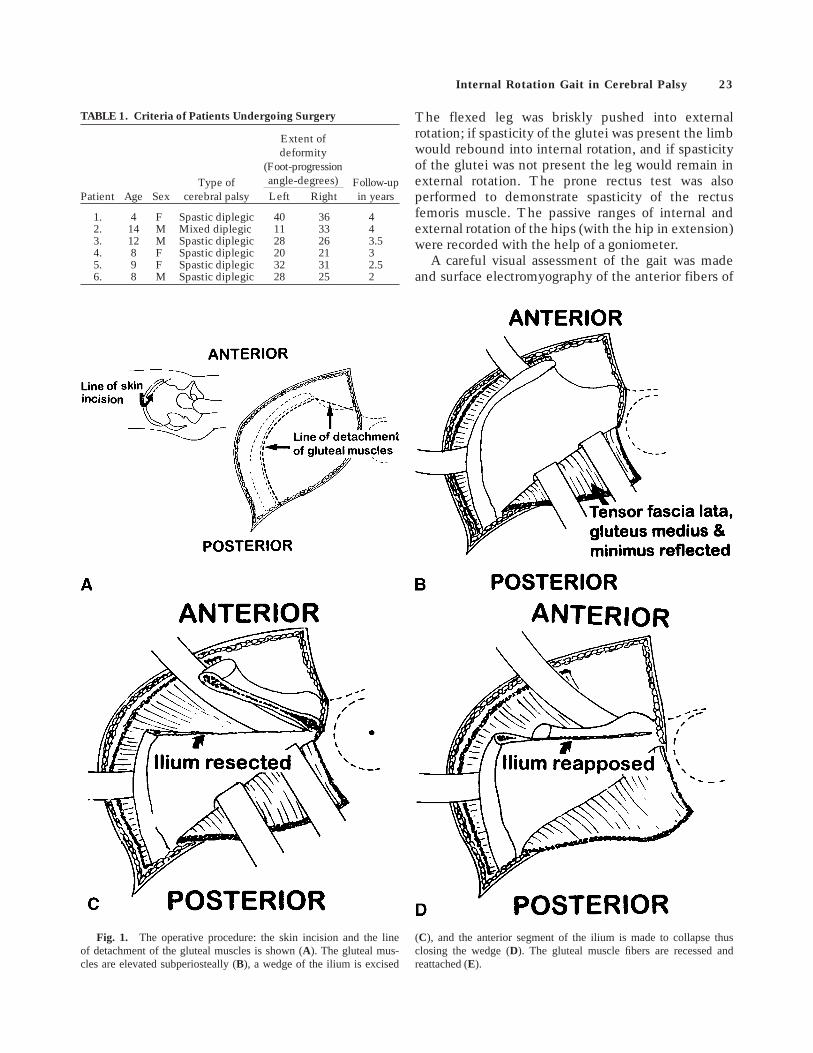
Fig. 1. The operative procedure: the skin incision and the lineof detachment of the gluteal muscles is shown (A). The gluteal mus-cles are elevated subperiosteally (B), a wedge of the ilium is excised
(C), and the anterior segment of the ilium is made to collapse thusclosing the wedge (D). The gluteal muscle fibers are recessed andreattached (E).
TABLE 1. Criteria of Patients Undergoing Surgery
Patient Age SexType of
cerebral palsy
Extent ofdeformity
(Foot-progressionangle-degrees) Follow-up
in yearsLeft Right
1. 4 F Spastic diplegic 40 36 42. 14 M Mixed diplegic 11 33 43. 12 M Spastic diplegic 28 26 3.54. 8 F Spastic diplegic 20 21 35. 9 F Spastic diplegic 32 31 2.56. 8 M Spastic diplegic 28 25 2
Internal Rotation Gait in Cerebral Palsy 23

the gluteus medius was performed as the subjectwalked a few steps. The duration of dynamic EMGrecording was restricted to the length of the electrodeleads available.
The criteria for attributing the excessive internalrotation of the hip during ambulation to overactivity ofthe gluteus medius and minimus were 1) excessiveduration of EMG activity of the glutei during thestance phase, swing phase, or both phases; 2) a positiveSteel’s test (the prone rectus test was invariablypositive also); and 3) no evidence of hamstring oriliopsoas tightness.
Six patients who fulfilled these criteria were identi-fied and underwent the surgical procedure bilaterally(Table 1). The children were followed-up for a mini-mum period of 2 years and reassessed clinically.
Operative Procedure
An incision 1.5 cm distal and parallel to the anteriorhalf of the iliac crest is made (Fig. 1A). The iliac crestis exposed subperiosteally and the gluteal muscula-ture, which takes origin anterior to the coronal plane, iselevated from the ilium (Fig. 1B). The iliacus muscleis also elevated from the anterior third of the iliac wing.
Fig. 2. A,B: Examples of children with cerebral palsy demonstrating the characteristics of the internalrotation gait due to gluteus medius and minimus overactivity. Excessive femoral and pelvic rotation areevident.
A. B.
Fig. 1 (Continued).
24 Joseph
A wedge of the iliac wing is excised, preserving theanterior iliac spines. The posterior margin of thewedge is in line with the axis of rotation of the hip joint(Fig. 1C). The preserved segment of the anterior iliumwith the iliac spines is made to collapse posteriorly,thus closing the wedge (Fig. 1D). The elevated glutealmuscle fibers are recessed and anchored to the iliaccrest as far posteriorly as possible. This realigns theobliquely running fibers to take an almost verticalcourse down from the iliac crest to the trochanter(Fig. 1E). The wound is closed in layers over a suctiondrain and weight-bearing is permitted after 3 weeks.
OBSERVATIONS
The children walked with the hip internally rotatedduring the swing phase of gait and with excessivepelvic rotation in the transverse plane (Fig. 2A,B).
Consequently, the foot placement was such that itcrossed over the line of progression. The foot progres-sion angle pre-operatively ranged from 11° to 40° ofinternal rotation. The postoperative values of the footprogression angles ranged from 5° of internal rotationto 15° of external rotation.
All 12 hips had 15° or less of external rotationpreoperatively, while the internal rotation ranged be-tween 70° to 90°. The postoperative range of externalrotation improved in all hips (range 20° to 30°),whereas the range of internal rotation remained un-changed. The abductor power of all the hips was gradeV (MRC grade) preoperatively, and no reduction ofpower was noted in any of the twelve hips postopera-tively. Following surgery, the gait patterns improved inall the hips. The excessive pelvic rotation decreasedappreciably and in no case did the foot cross over theline of progression.
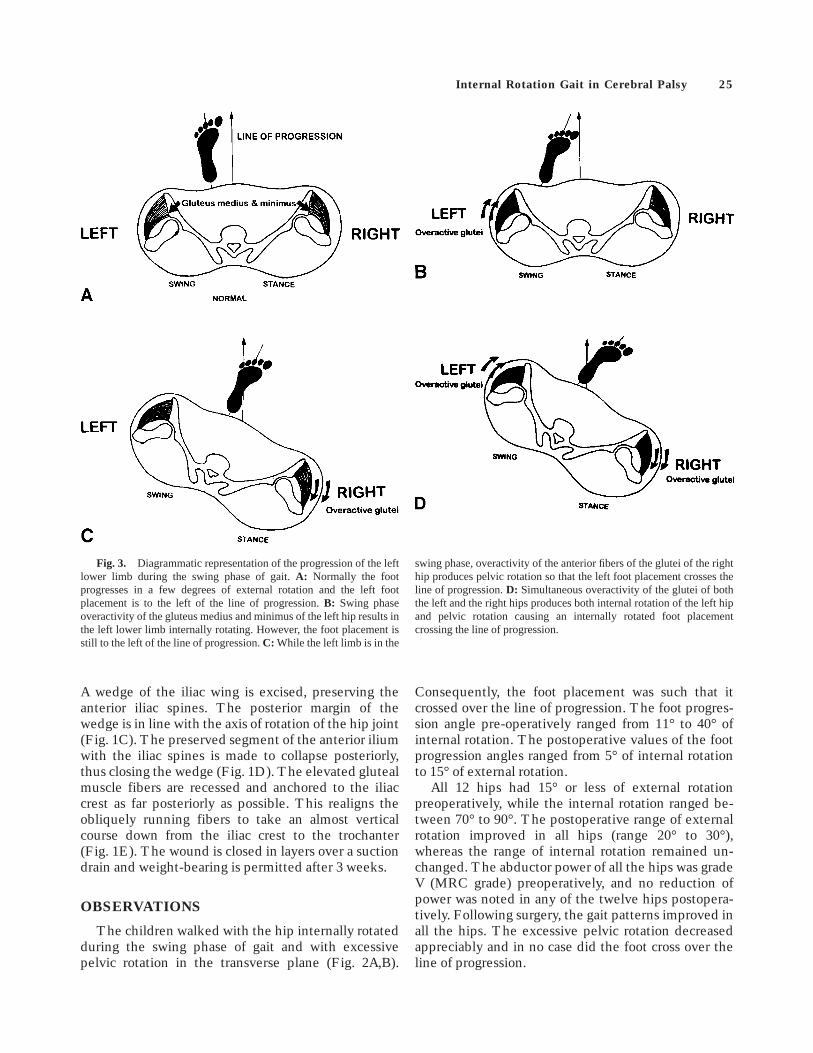
Fig. 3. Diagrammatic representation of the progression of the leftlower limb during the swing phase of gait.A: Normally the footprogresses in a few degrees of external rotation and the left footplacement is to the left of the line of progression.B: Swing phaseoveractivity of the gluteus medius and minimus of the left hip results inthe left lower limb internally rotating. However, the foot placement isstill to the left of the line of progression.C: While the left limb is in the
swing phase, overactivity of the anterior fibers of the glutei of the righthip produces pelvic rotation so that the left foot placement crosses theline of progression.D: Simultaneous overactivity of the glutei of boththe left and the right hips produces both internal rotation of the left hipand pelvic rotation causing an internally rotated foot placementcrossing the line of progression.
Internal Rotation Gait in Cerebral Palsy 25
DISCUSSION
The electromyographic study of Csongradi et al.(1980) demonstrated that abnormal biphasic activity ofthe gluteus medius and minimus can occur in cerebralpalsy. Our clinical observations suggest that overactiv-ity of the anterior fibers of the gluteus medius andminimus would produce distinctly identifiable abnor-malities in the gait pattern. Figure 3A–D diagrammati-cally depicts the progression of the left lower limbduring the swing phase with the right lower limb in thestance phase. In the normal child, the left footprogresses in a few degrees of external rotation and thefoot placement occurs to the left of the line ofprogression (Fig. 3A). If the left gluteus medius isoveractive during the swing phase the left lower limbinternally rotates so that the foot placement is ininternal rotation but is still to the left of the line ofprogression (Fig. 3B). While the left lower limb is inthe swing phase, overactivity of the anterior fibers ofthe glutei of the right hip would produce pelvicrotation such that the left foot placement crosses theline of progression. However, the foot is not internallyrotated in relation to the trunk (Fig. 3C). Simultaneousoveractivity of the anterior fibers of the glutei of bothhips would produce both internal rotation of the lefthip and pelvic rotation resulting in internally rotatedfoot placement well across the line of progression (Fig.3D). This was the pattern of gait noted in the patientsshown in Figure 2A,B.
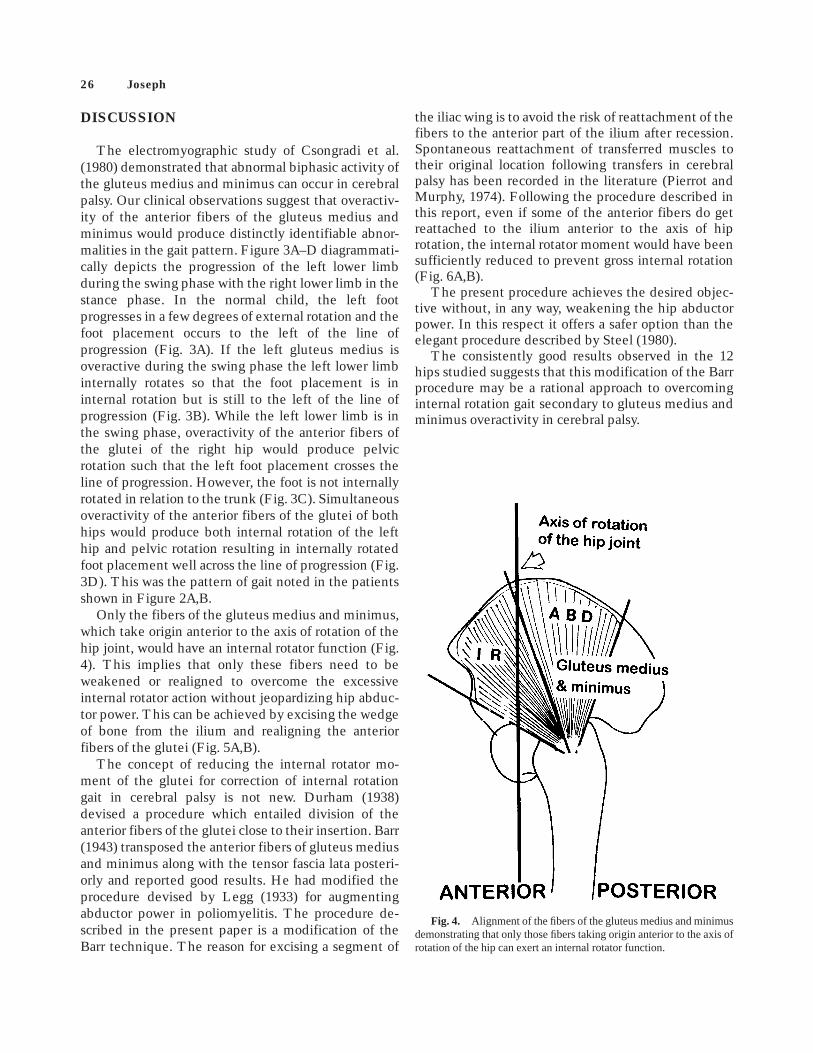
Only the fibers of the gluteus medius and minimus,which take origin anterior to the axis of rotation of thehip joint, would have an internal rotator function (Fig.4). This implies that only these fibers need to beweakened or realigned to overcome the excessiveinternal rotator action without jeopardizing hip abduc-tor power. This can be achieved by excising the wedgeof bone from the ilium and realigning the anteriorfibers of the glutei (Fig. 5A,B).
The concept of reducing the internal rotator mo-ment of the glutei for correction of internal rotationgait in cerebral palsy is not new. Durham (1938)devised a procedure which entailed division of theanterior fibers of the glutei close to their insertion. Barr(1943) transposed the anterior fibers of gluteus mediusand minimus along with the tensor fascia lata posteri-orly and reported good results. He had modified theprocedure devised by Legg (1933) for augmentingabductor power in poliomyelitis. The procedure de-scribed in the present paper is a modification of theBarr technique. The reason for excising a segment of
the iliac wing is to avoid the risk of reattachment of thefibers to the anterior part of the ilium after recession.Spontaneous reattachment of transferred muscles totheir original location following transfers in cerebralpalsy has been recorded in the literature (Pierrot andMurphy, 1974). Following the procedure described inthis report, even if some of the anterior fibers do getreattached to the ilium anterior to the axis of hiprotation, the internal rotator moment would have beensufficiently reduced to prevent gross internal rotation(Fig. 6A,B).
The present procedure achieves the desired objec-tive without, in any way, weakening the hip abductorpower. In this respect it offers a safer option than theelegant procedure described by Steel (1980).
The consistently good results observed in the 12hips studied suggests that this modification of the Barrprocedure may be a rational approach to overcominginternal rotation gait secondary to gluteus medius andminimus overactivity in cerebral palsy.
Fig. 4. Alignment of the fibers of the gluteus medius and minimusdemonstrating that only those fibers taking origin anterior to the axis ofrotation of the hip can exert an internal rotator function.
26 Joseph
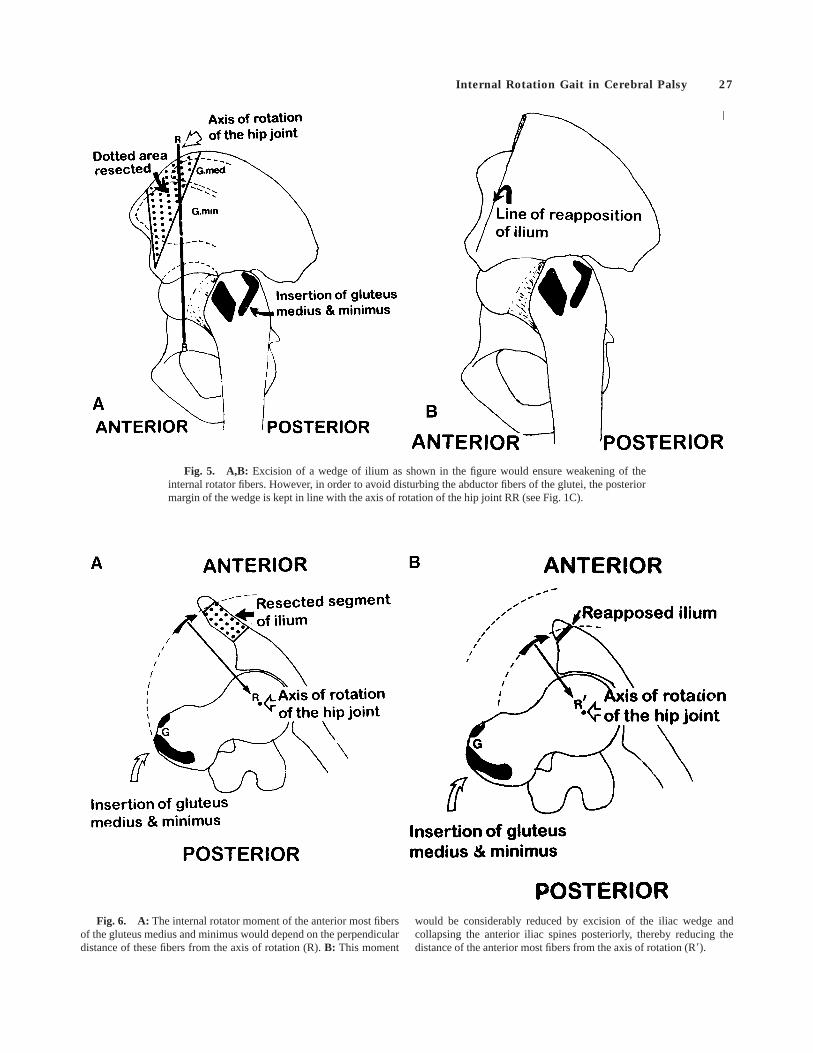
Fig. 5. A,B: Excision of a wedge of ilium as shown in the figure would ensure weakening of theinternal rotator fibers. However, in order to avoid disturbing the abductor fibers of the glutei, the posteriormargin of the wedge is kept in line with the axis of rotation of the hip joint RR (see Fig. 1C).
Fig. 6. A: The internal rotator moment of the anterior most fibersof the gluteus medius and minimus would depend on the perpendiculardistance of these fibers from the axis of rotation (R).B: This moment
would be considerably reduced by excision of the iliac wedge andcollapsing the anterior iliac spines posteriorly, thereby reducing thedistance of the anterior most fibers from the axis of rotation (R8).
Internal Rotation Gait in Cerebral Palsy 27

REFERENCESBarr, J.S. 1943 Muscle transplantation for combined flexion-
internal rotation deformity of the thigh in spastic paralysis.Arch. Surg. 46:605–607.
Csongradi, J., S. Terver, J. Medeiros and E. Bleck 1980Electromyographic study of the gluteus medius during thegait of normal children and cerebral palsy children. Orthopae-dic Transactions 4:72.
Durham, H.A. 1938 A procedure for the correction of internalrotation of the thigh in spastic paralysis. J. Bone Joint Surg.20:339–344.
Legg, A.T. 1933 Tensor fascia femoris transplantation in cases ofweakened gluteus medius. New Eng. J. Med. 209:61–62.
Pierrot, A.H. and O.B. Murphy 1974 Heel cord advancement. Anew approach to the spastic equinus deformity. Orthop.Clin. North Am. 5:117–126.
Staheli, L.T. 1977 Torsional deformity. Ped. Clin. North Am.24:799–811.
Steel, H.H. 1980 Gluteus medius and minimus insertionadvancement for correction of internal rotation gait in spasticcerebral palsy. J. Bone Joint Surg. 62A:919–927.
28 Joseph