Embed Size (px)
Citation preview

328
HeLa cells. However, the two isolates produced a-haemolysin onoxoid CM-55 agar containing 7% defibrinated sheep blood’ andexpressed Gal-Gal binding adhesin, as assessed by agglutination ofhuman OPl erythrocytes in 4% D-mannose. A gene probe for theGal-Gal binding adhesin’ hybridised with the DNA of the twostrains, confirming the Gal-Gal binding phenotype.
This is the first report of pyelonephritic E coli strains beingpathogenic in the intestine and of a bacterium being responsible forbenign rectal bleeding associated with ecchymotic lesions of
rectosigmoid mucosa in the neonatal period. We hypothesise thatboth x-haemolysin and Gal-Gal binding adhesin are involved in thepathogenesis. ot-Haemolysin damages several cell types in vitro andcauses tissue injury.s Moreover enteritis in swine and otherdomestic animals is associated with an a-haemolysin producing Ecoli in the gut.6 On the other hand E coli strains possessing Gal-Galbinding adhesins have been shown to colonise enterocytic cells.7 Weare studying whether the expression in the distal colon and therectum of cell receptors for Gal-Gal binding adhesin, especially thehuman blood group antigens Pi’ Pz, and Pk, are restricted to theneonatal period, as described for other blood group substances.8
We thank Jean-Luc Beretti for technical assistance, Agnes Labigne-Roussel and Pascale Courcoux for testing for Gal-Gal binding adhesin gene,Marylene Bohnert for testing for Sta-P and Sta-H gene, and Marie-LaurenceFoumeaux for typing.
Microbiology Laboratory,Department of Paediatrics,
and Pathology Laboratory,Hôpital Necker-Enfants Malades,75015 Paris, France
J. L. GAILLARDG. CHERONJ. F. MOUGENOTJ. P. DESLYSC. NEZELOFM. VERONJ. SCHMITZ
1. O’Hanley P, Low D, Romero I, et al. Gal-Gal binding and hemolysin phenotypes andgenotypes associated with uropathogenic E coli. N Engl J Med 1985; 313: 414-20.
2. Dupont C, Badoual J, Le Luyer B, et al. Rectosigmoidoscopic findings during isolatedrectal bleeding in the neonate J Pediatr Gastroenterol Nutr 1987; 6: 257-64.
3. Bohnert M, d’Hauteville H. Sansonetti P. Detection of enteric pathotypes byhybridisation using six DNA probes. Ann Inst Pasteur (Microbiol) 1988; 139:189-202.
4. Archambaud M, Courcoux P, Labigne-Roussel A. Detection by molecular
hybridisation of PAP, AFA and SFA adherence systems in Escherichia coli strainsassociated with urinary and enteral infections Ann Inst Pasteur (Microbiol) 1988;149: 575-88.
5. Cavalieri SJ, Bohach GA, Snyder I S. Eschenchia coli &agr;-hemolysin: characteristics andprobable role in pathogenicity. Microbiol Rev 1984; 48: 326-43.
6. Gregory DW. Role of the &bgr;-hemolytic coliform organisms in edema disease of swine.Vet Med 1955; 50: 609-10.
7. Wold AE, Thorssen M, Hull S, Svanborg Eden C. Attachment of Escherichia coli viamannose- or Gal &agr; 1 → 4 Gal &bgr;-containing receptors to human colonic epithelialcells Infect Immun 1988; 56: 2531-37.
8. Wiley EL, Murphy P, Mendelsohn G, Eggleston JC. Distribution of blood groupsubstances in normal human colons: use of the unlabeled antibody (PAP)immunoperoxidase technic to identify A and B blood group substances. Am J ClinPathol 1981; 76: 806-09.
GENDER AND SURVIVAL IN NEUROBLASTOMA
SIR,-In published series of patients with neuroblastomasurvival tends to be better in females than in mates," and in UK’and Germans studies this superiority was significant. We would liketo suggest an explanation.
Since January, 1982, details of all newly diagnosed cases ofneuroblastoma presenting at the twenty-three hospitals in theEuropean Neuroblastoma Study Group (ENSG) have been
collated in a central registry. Treatment for boys and girls isidentical. By June, 1988, 757 cases had been registered. 5-yearactuarial survival has been 50% for girls and 44% for boys.However, boys were less likely than girls to have good prognosisdisease6 (stages ivs, I, and 11). When stages were ordered as lvs,1,11,III, iv a statistical test for ordered categorical data confirmed atendency for males to be at a more advanced disease stage thanfemales (p < 0-05):
Gender IVs I 11 III IVMale 47 49 49 54 58Female 53 51 51 46 42
The outcome for boys and girls within each individual stage is verysimilar. Analysis by age at diagnosis (less than or greater than oneyear), which is, apart from stage, the only established independent
prognostic criterion in neuroblastoma, also revealed no differencebetween the genders. The median age at diagnosis was similar forboys and girls.
Little is known about what influences the aggressiveness oftumours. In neuroblastoma the association between amplificationof the oncogene N-myc and advanced stage is well known Perhapsthere are gender-associated differences in N-myc amplification (orother natural biological response modifiers) in children withneuroblastoma.
We thank colleagues in the ENSG for supplying data and Dr G. Draper forhelpful advice. The Cancer Research Campaign and Neuroblastoma Society(a parents’ charity) provided financial support.
Department of Haematologyand Oncology,
Hospital for Sick Children,London WC1N 3JH,
and UK Children’s Cancer Study Group,University of Leicester
JON PRITCHARDJ. M. BARNESS. M. GERMONDK. R. WALLENDSZUS,For the EuropeanNeuroblastoma Study Group
1. Thomas PRM, Lee JY, Fineberg BB, et al. An analysis of neuroblastoma at a singleinstitution. Cancer 1984; 53: 2079-82.
2. Carlsen NLT. Epidemiological investigations on neuroblastomas in Denmark1943-80. Br J Cancer 1986; 54: 977-88.
3. Evans AE, S’Angio GJ, Propert K, et al. Prognostic factors in neuroblastoma. Cancer1987; 59: 1853-59.
4. Kinnear Wilson LM, Draper GJ. Neuroblastoma, its natural history and prognosis.Br Med J 1984; 289: 301-07.
5. Berthold F, Brandeis WE, Lampert F. Neuroblastoma: diagnostic advances andtherapeutic results in 370 patients. Monogr Paediatr 1986; 18: 206-23.
6. Pritchard J, Kemshead J. Neuroblastoma: recent developments in assessment andmanagement. Rec Results Cancer Res 1983; 88: 69-78.
7. Schwab M, Ellison J, Busch M et al. Enhanced expression of the human gene N-mycconsequent to amplification of DNA may contribute to malignant progression ofneuroblastoma. Proc Natl Acad Sci (USA) 1984; 81: 4940-44.
TREATMENT OF HYPONATRAEMIA SECONDARYTO WATER OVERLOAD
SiR,—Dr Tanneau and colleagues (Oct 29, p 1031) report a caseof fatal central pontine myelinolysis in a polydipsic, hyponatraemicschizophrenic patient after spontaneous correction of
hyponatraemia. The patient, who also had chronic alcoholism andinadequate nutrition, had water intoxication after further reducingfood intake and ingesting large quantities of beer. 3 days later, afterfluid restriction alone had led to a rise in serum sodium from 110 to135 mmol/l, the patient had spastic quadriparesis and pseudobulbarpalsy. Tanneau et al recommend that vasopressin be administeredduring fluid restriction in such patients to slow the rate of rise inserum sodium.
In agreement with Dr Seckl (Nov 26, p 1254), we caution againstadministering vasopressin in these patients since they may have aprimary disorder in thirst! and are notoriously resourceful in
finding fluids to ingest. Furthermore we" and others3,4 have foundthat water restriction is not only safe in hyponatraemicschizophrenic inpatients (many of whom, as did Tanneau andcolleagues’ patient, have a history of alcohol abuse),5 but also, wheninstituted after precipitous drops in serum sodium, preventsepisodes of water intoxication.We weigh inpatients with a history of water intoxication three
times weekly and when staff observe prodromal signs of severehyponatraemia (ataxia, confusion, tremors, nausea, vomiting).When weight increases above a predetermined level, serum sodiumis measured and if below 125 mmol/1 (or lower, depending on thepatient’s basal sodium level), we eliminate all fluids for 16 hours,except for those on the meal tray. We measured serum sodiumbefore and after 16 hours of fluid restriction in 5 patients during sixof these hyponatraemic episodes. Serum sodium rose from an initialmean level of 119 [SD 3] mmol/1 to a final level of 138 [3] mmol/1 (arise of 14-21 mmot/1), for a mean rate of increase of 1 1 [0-2] mmol/1per hour. Weight fell on average 7-0 kg. We have instituted thisintervention over fifty times in more than 20 patients with episodicwater intoxication who had initial sodium levels between 110 and125 mmol/1. All showed similar degrees of spontaneous diuresis,and none had delayed neurological symptoms.We believe that the concurrent alcohol abuse and associated
malnutrition in the patient reported by Tanneau et al were likely

329
critical elements in the development of that patient’s central pontinemyelinolysis. In otherwise healthy schizophrenic patients(including those with a history of alcohol abuse), targeted fluidrestriction for at least 16 hours is a safe and effective means of
preventing the morbidity and mortality associated with waterintoxication.
University of Chicago Medical Center,Chicago, Ilinois 60637, USA;and Illinois State Psychiatric Institute,
Chicago
MORRIS B. GOLDMANDANIEL J. LUCHINSGARY L. ROBERTSON
1 Goldman MB, Luchins DJ, Robertson GL. Mechanisms of altered water metabolismm psychotic patients with polydipsia and hyponatremia. N Eegl J Med 1988; 318:397-403
2. Goldman MB, Luchins DJ. Prevention of episodic water intoxication with targetweight procedure. Am J Psychiatry 1987; 144: 365-66.
3 Ashby YT Planned change: the development of a program for the management ofself-induced water intoxication. Can J Psychiatr Nurs 1987, 28: 12-14.
4. Delva NJ, Crammer JL Polydipsia in chronic psychiatric patients: body weight andplasma sodium. Br J Psychiatry 1988; 144: 1626.
5 Ripley TL, Millson RC, Kocapski AB. Self-induced water intoxication and alcoholabuse Am J Psychiatry 1989; 146: 101-02.
THE WHITE-COAT EFFECT AND SELF-RECORDINGOF BLOOD PRESSURE
SIR,-Self-recording of blood pressure at home is of increasingimportance in the management of hypertension. With multiplemeasurements knowledge of an individual’s average blood pressureis improved and, more importantly, the physician is no longer at riskof treating a condition evoked by himself-the so-called white-coateffect. We observed in a large group of patients accustomed toself-recording that the physician-induced blood pressure rise
diminished with time. To study this effect in more detail, werandomly assigned 16 hypertensive patients (8 female, 8 male; age58 [SD 3] years) to trained self-recording or "passive" controlgroups. All patients’ blood pressures were first measured by aphysician in the clinic and the patients were maintained on theirusual drugs for two weeks. Then the same physician repeated themeasurement at the same time of day and in the same surroundings;self-recording patients presented their records with blood pressuremeasurements done three times daily.As expected, the average self-recorded blood pressure levels were
significantly lower than the physician’s first result. Interestingly, inthis group the physician’s second blood pressure result was alsosignificantly diminished (161 [SD 5]/96 [4] vs 150 [4]/87 [4] mmHg,p < 0.05) and did not differ from the patients’ averages. In thecontrols there was no such effect (161 [5]/93 [3] vs 162 [6]/94 [3] mmHg).To interpret this result in a small group of patients the possible
effects of actively involving patients in the management of theircondition have to be considered and studied separately. It would beinteresting to see, over one or more years, whether there is a
lessening of the self-recording effect on blood pressure in the clinicand the "white coat" supervenes after all.
Second Department of Internal Medicine,University of Vienna,A-1090 Vienna, Austria
BRIDGITTE STANEKULRIKE BRUCKNER
CD4+ T-CELL DAMAGE TO ISLET BETA CELLS
SIR,-Dr Vento and Dr Garofano (Nov 19, p 1200) discuss ourstudy of CD4 + cytotoxic T cell damage to islet p cells in type Idiabetes (Oct 8, p 823). Our results were unexpected and the reportwas preliminary. We did not rule out other mechanisms of islet celldamage. Because of the shortage of histocompatible humanpancreatic islets, we could do only two experiments (not one, asVento and Garofano state) with three Vp8 positive T cell clonesfrom a newly diagnosed type I diabetic patient. Histocompatibilitywas achieved only with respect to HLA DR3 and possibly otherclass II antigens and not class I antigens, and for this reason, andbecause of the limited number of clones tested, we cannot rule outthe killing of p cells by CD8 cytotoxic T cells.
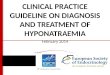
Lysis by CD4 clone of HLA class II induced histocompatible isletcells.
Islet target cells, from two donors (HP72, HP73) were cultured for 2 daysin presence of 50 U/ml each of IFNy and TNFa, to induce HLA class IIantigens. Class II expression was confirmed by immunostaining withmonoclonal antibody L243. HLA phenotype of diabetic patient was A2B8,62 DR1,3. Cytotoxicity assay was done as previously described.
We report here another experiment with class II DR
haploidentical islets which were lysed, and class II incompatibleislets which were not (figure). These data accord with our previousreport. Haskins et all published an account of a CD4 T cell clonefrom the non-obese diabetic mouse which was specific for islet cellpreparations and mediated the destruction of islet P cells in
syngeneic mice. Vento and Garofano point out that our results are atvariance with their stated claim that the "majority of T cellssurrounding affected islets are CD8 + ". This claim is exaggerated;Bottazzo’s report2 was from a single patient coming to necropsy whohad "mainly CD8 cells but CD4 cells were also present". Thereis no mention of CD8 cells in the Foulis and Farquarson3 papercited.Vento et a14 have used the lymphocyte-migration inhibitory
factor assay to study immune regulation in hepatitis B and urges usto do this for type I diabetes. We think that the analysis of T cellclones from patients (raised from single cells) is a better tool todissect the complexity of the immune system. We would like toinvestigate patients in the prediabetic period (ie, before the onset ofthe disease process) but there is no reliable method to detect suchindividuals. Unlike hepatitis B, type I diabetes is a disease ofunknown aetiology, and to suggest a list of probable antigens is tocomplicate an already difficult field.Vento and Garofano suggest that CD8+ suppressor cells may
recognise class II positive cells, and they cite a recent symposiumpresentation. The suppressor cell literature is in considerable
disarray,s and we cannot comment on unpublished presentations.Medical Clinic I,Universitá la Sapienza, Rome, Italy
Charing Cross Sunley Research Centre
Department of Surgery,Leicester Royal Infirmary
Department of Endocrinology,Charing Cross Hospital
Charing Cross Sunley Research Centre,Lurgan Avenue,London W6 8LW
P. DE BERARDINIS
M. LONDEI
R. F. L. JAMESS. P. LAKE
P. H. WISE
M. FELDMANN
1. Haskins K, Portas M, Bradley B, Wegmann D, Lafferty K. T-lymphocyte clonespecific for pancreatic islet antigen Diabetes 1988; 37: 1444-48.
2. Bottazzo GF, Dean BM, McNally JM, Mackay EH, Swift PGF, Gamble DR. In situcharacterisation of autoimmune phenomena and expression of HLA molecules inpancreas in diabetic insulinitis. N Engl J Med 1985; 313: 353-60.
3. Foulis AK, Farquharson MA. Aberrant expression of HLA-DR antigens by insulincontaining beta cells in recent onset type I diabetes mellitus. Diabetes 1986; 35:1215-24.
4. Vento S, Rondanelli EG, Raneiri S, O’Brien CJ, Williams R, Eddleston ALWF.Prospective study of cellular immunity to hepatitis-B-virus antigens from the earlyincubation phase of acute hepatitis B. Lancet 1987; ii: 119-22.
5 Moller G. Do suppressor T cells exist? Scand J Immunol 1988, 27: 247-50.