Embed Size (px)
Citation preview

Treatment of Conjunctival and CornealEpithelial Neoplasia with Retinoic Acid andTopical Interferon Alfa-2b: Long-termFollow-up
Matthew Krilis, MBBS,1 Hughie Tsang, MBBS,2 Minas Coroneo, MD, FRACS2
Objective: To evaluate the long-term recurrence rate of conjunctival and corneal intraepithelial neoplasia(CIN) treated with retinoic acid and topical interferon alfa-2b.
Design: Retrospective, noncomparative, interventional case series.Participants: A total of 89 eyes of 89 patients from 1 institution who were treated between September 2003
and February 2010 for CIN lesions used topical interferon alfa 1 million IU/ml drops 4 times daily and retinoic acid0.01% once every second day.
Methods: Diagnosis was made by biopsy and impression cytology. Patients’ notes and clinical photographswere reviewed, and data were analyzed. All eyes were monitored for the possibility of recurrence with a minimumof 1 year of follow-up from the time of documented clinical resolution.
Main Outcome Measures: All eyes were monitored for the possibility of recurrence with a minimum of 1year of follow-up from the time of documented clinical resolution.
Results: Complete clinical resolution of the CIN lesions was achieved in 87 of the 89 eyes treated(97.75%). Two of the 89 eyes treated (2.25%) had only a partial response to treatment; of these 2 patients,1 was taking cyclosporine for keratitis sicca. For the 87 eyes with complete response, resolution occurredafter a mean of 1.69 months (range, 19 days to 6.5 months). Mean follow-up after clinical resolution(tumor-free period) was 51.5 months (range, 11– 84 months). Four of the 87 patients with complete responsedeveloped a mild allergic papillary conjunctivitis that settled on halving the interferon dose to 0.5 million IUdrops and reducing the frequency to 3 times daily. Side effects were limited to 1 case of epithelial microcystsand 1 case of marginal keratitis.
Conclusions: In this group of patients observed with CIN lesions, combination treatment of topical retinoicacid and interferon alfa-2b was effective in treating lesions with minimal self-limited side effects with faster andgreater resolution and a longer tumor-free period compared with studies using interferon alfa-2b alone. Wehypothesize that topical all-trans retinoic acid and interferon alfa-2b may act synergistically. We believe thatcombination treatment of interferon alfa-2b and retinoic acid may offer a superior alternative to interferon alfa-2balone in treating CIN.
Financial Disclosure(s): Proprietary or commercial disclosure may be found after the references.
Ophthalmology 2012;119:1969–1973 © 2012 by the American Academy of Ophthalmology.bcclbtntnic
t
Conjunctival and corneal intraepithelial neoplasia (CIN) arecommon, slowly growing lesions that may evolve to squamouscell carcinoma although they carry only a small risk of malig-nancy.1,2 Sight can be affected when corneal extension occurs.
A number of risk factors exist for CIN. Nonmodifiablerisk factors include certain patient characteristics, such aslight hair and ocular pigmentation, and family origin in theBritish Isles, Austria, or Switzerland.3 Men are more com-monly affected than women, and risk increases with age.4
Other risk factors include ultraviolet exposure4 and both thehuman immunodeficiency virus5 and the human papillomavirus.6,7 In addition to this, exposure to petroleum prod-ucts,3 heavy cigarette use,3 and contact lens wear (InvestOphthalmol Vis Sci 1992:33:1292) have been identified as
risk factors for CIN. g© 2012 by the American Academy of OphthalmologyPublished by Elsevier Inc.
Conjunctival and corneal intraepithelial neoplasia andenign limbal lesions can sometimes be differentiated bylinical appearance but require pathologic examination forertitude. Conjunctival and corneal intraepithelial neoplasiaesions typically involve the limbus, are elevated, and maye papilliform, leukoplakic, or gelatinous with characteristicufts of blood vessels. Pterygium, keratinization of the cor-eal epithelium, pannus, anterior basement membrane dys-rophy, and malignant melanoma are all differential diag-oses for CIN.8 Biopsy of the suspicious lesion is necessaryf the diagnosis is in question.9,10 Corneal involvementonsists of a gray, opaque, thickened epithelium.10
Conventional treatment includes wide excision of theumor combined with cryotherapy to the surgical mar-
ins.11,12 External beam radiation, phototherapeutic kera-1969ISSN 0161-6420/12/$–see front matterhttp://dx.doi.org/10.1016/j.ophtha.2012.03.045

srt
D
Cmtasat
opritpjmbeTttac
asCtstm
ewcamep
NMCRM
Ophthalmology Volume 119, Number 10, October 2012
tectomy with the excimer laser, and photodynamic therapyalso have been used to treat CIN.13 Topical therapy withimmune modulators or chemotherapeutic agents, such asinterferon and mitomycin C, and immunotherapy have be-come more prevalent in recent times.14–17
The major issue regarding the management of CIN is thatof recurrence. The issues of late recurrence and malignantpotential have led some to argue that patients with a historyof CIN require follow-up for the remainder of their lives onan annual basis.18
We recently reported a case of a rapid response ofrefractory ocular surface dysplasia to combination treatmentwith topical all-trans retinoic acid and interferon alfa-2b.19
This study reports the success and long-term recurrence rateusing combination topical therapy of retinoic acid and top-ical interferon alfa-2b for CIN.
Subjects and Methods
This study was a retrospective chart review approved by theSoutheastern Sydney Area Health Service Human Research EthicsCommittee (Eastern Section) 03/268.
A total of 89 patients with CIN and 89 eyes treated in a referralpractice (MTC) associated with the Prince of Wales Hospital inSydney, Australia, were included in this study.
A retrospective review of all patients treated with retinoic acidand topical interferon alfa-2b between September 2003 and Feb-ruary 2010 was conducted.
A total of 103 eyes of 103 patients were reviewed. Inclusioncriteria included a diagnosis of CIN based on biopsy or impressioncytology. Exclusion criteria included patients whose biopsy orimpression cytology revealed a diagnosis other than CIN, and 14patients’ eyes were excluded on these grounds. Of the 89 patientsincluded, 42 were diagnosed on biopsy and 47 were diagnosed onimpression cytology.
Patients were prescribed topical interferon alfa-2b drops 1million IU/ml 4 times daily and retinoic acid 0.01% once everysecond day.
Patients were observed clinically, and therapy was continueduntil there was complete clinical resolution of the CIN lesionsbased on slit-lamp biomicroscopy and clinical photographs. Sixty-three of the patients were seen at 1-, 6-, and 12-month intervals.Sixteen of the patients were seen at 1- and 12-month intervals.Eight of the patients were seen after 3 and 12 months. All subjectswere seen 6 months after resolution and were followed up for aminimum of 1 year after resolution. Most patients continued top-ical interferon alfa-2b drops and retinoic acid 0.01% once everysecond day for 12 months after clinical resolution of the tumor.Patients’ charts were reviewed, and data were systematized usingExcel (Microsoft Corp, Redmond, WA).
Results
Complete clinical resolution of the CIN lesions was achieved in 87of the 89 eyes treated (97.75%). Two of the 89 eyes treated(2.25%) had only a partial response to treatment; of these 2patients, 1 was taking cyclosporine for keratitis sicca. For the 87eyes with complete response, resolution occurred after a mean of1.69 months (range, 19 days to 6.5 months). Mean follow-up afterclinical resolution (tumor-free period) was 51.5 months (range,11–84 months) (Table 1). Four of the 87 patients with complete
response developed a mild allergic papillary conjunctivitis that t1970
ettled on halving the interferon dose to 0.5 million IU drops andeducing the frequency to 3 times daily. Side effects were limitedo 1 case of epithelial microcysts and 1 case of marginal keratitis.
iscussion
onjunctival and corneal intraepithelial neoplasia are theost common neoplasms of the ocular surface.1 The tradi-
ional treatment has been wide local surgical excision withdjunctive cryotherapy; however, incompletely excised le-ions are associated with a higher incidence of recurrencefter surgery than complete excision, and excision margin athe time is the greatest risk factor for recurrence.1
A major issue involving the management of CIN is thatf recurrence. The issues of late recurrence and malignantotential have led some to propose annual follow-up for theemainder of the patient’s life.12 Conjunctival and cornealntraepithelial neoplasia can spread along the basal conjunc-ival layers beyond the clinical lesion. In a study of 120atients undergoing excision with or without possible ad-unctive radiation, there was a 53% recurrence rate whenargins were involved. Other recurrence rates have varied
etween 7% and 69%, depending on the involvement ofxcised margins, primary treatment, and follow-up time.hus, surgical excision offers a fast and definitive approach
o patients; however, because of the high recurrence rates,he existence of nonresectable lesions, and the risk of dam-ge to limbal stem cells, it may not be the ideal option, andhemotherapeutic agents may prove to be superior.
A major advantage of topical treatment is that the ther-peutic agent comes into contact with much of the ocularurface. Mitomycin C has been used effectively to treatIN,18,20 however, patients report pain due to surface epi-
heliopathy.20 Furthermore, allergic reaction and punctaltenosis are associated with mitomycin C use.20 In additiono this, a recent study points to an association with mito-ycin C and limbal stem cell deficiency.21
Combination treatment of topical retinoic acid 0.01% oncevery second day and interferon alfa-2b alone avoids surgery,hich can cause limbal stem cell depletion and ocular surface
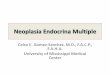
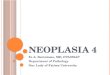
ompromise. Of note in our study (Fig 1A–J), the tissueppearance and in particular the limbal appearance were nor-al after lesion resolution. The use of retinoic acid 0.01% once
very second day and interferon alfa-2b largely prevents theotential surface toxicity and pain of topical mitomycin C and
Table 1. Analysis of Number of Eyes, Time to Resolution,Treatment Time, and Follow-up for the 87 Patients with
Conjunctival and Corneal Intraepithelial Neoplasia TreatedSuccessfully with Combination Therapy of Topical Retinoic
Acid and Topical Interferon Alfa-2b
o. of Eyes 87edian time to resolution 1.69 mosomplete resolution 97.75%ecurrence rate 2.25%edian follow-up 51.5 mos
he possibility of corneoscleral melting, which can be seen

ar
cw
e and
Krilis et al � CIN Retinoic Acid and Interferon Alfa-2b
after mitomycin C, as well as the risk of punctal stenosis andlimbal stem cell deficiency. Therefore, combination treatmentof topical retinoic acid and interferon alfa-2b is a viable andpossibly superior alternative to radiation, topical mitomycin C,or surgical excision with cryotherapy. Our study shows that
Figure 1. Photographs of eyes from representative patients with corneal itopical interferon alfa-2b. Each individual patient was photographed befor
combination treatment of retinoic acid and topical interferon r
lfa-2b is an effective and efficient treatment for primary orecurrent CIN.
The effects of the interferons in inducing apoptosis areomplex. Microarray studies in certain cell lines treatedith interferon reveal �300 induced genes, and both indi-
ithelial neoplasia (CIN) treated with a combination of retinoic acid andafter treatment. 1 and 3 � before treatment; 2 and 4 � after treatment.
ntraep
ect and direct effects are mediated by gene expression. This
1971

hd
oiiac
namsCttoe
R
1
1
1
1
1
Ophthalmology Volume 119, Number 10, October 2012
results in modulation of receptors for other cytokines, reg-ulatory proteins on immune effector cell surfaces, and en-zyme activity involved in cellular growth and function.Retinoids exert their modulatory effects on cell growth bybinding to the retinoid acid receptors and retinoid x recep-tors, each of which has 3 subtypes (�, �, and �) and acts asa transcription factor. A feature of transformation in manymalignant solid tumors and certain premalignant lesions isloss of expression of retinoid acid receptor-�. We previ-ously demonstrated involvement of matrix metalloprotei-nases in the pathogenesis of pterygium22 and showed thatmatrix metalloproteinases play a role in the pathogenesis ofocular surface squamous neoplasia.23 In addition, retinoidsare able to reverse upregulation of matrix metalloprotei-nase;24 thus, retinoids have been shown to have an inhibi-tory effect on ocular surface squamous neoplasia.23,24
Furthermore, the antiproliferative effects of combinedtreatment in cell culture systems have long been recog-nized25 and applied in clinical studies, with antitumor ef-fects being demonstrated in advanced carcinoma of the skinand cervix.26,27 As a basic framework, in a premalignantmodel of cervical carcinoma, retinoic acid is thought toreduce dysplastic differentiation and interferon-alpha in-duces apoptosis. Given the results of our study and theproven efficacy of combined therapy, we believe that topicalall-trans retinoic acid and interferon alfa-2b may actsynergistically.
In our study, the combination treatment of topical reti-noic acid 0.01% once every second day and interferonalfa-2b demonstrated successful clinical regression of 87 of89 lesions. The mean time to resolution was 1.69 months(range, 19 days to 6.5 months). A long-term tumor-freeocular surface was maintained when retinoic acid and in-terferon alfa-2b were used in concentrations of 0.01% onceevery second day and 1 million IU/ml 4 times daily. Nopatient in this study experienced any systemic side effects.The only side effects in our study were epithelial microcystsin 1 patient and marginal keratitis in 1 patient.
Compared with recent studies of the use of interferonalfa-2b alone,28 as illustrated in Table 2, our study of largernumbers and longer follow-up shows that combinationtreatment results in a faster and greater resolution and alonger tumor-free period.
Four of the 87 patients with complete response devel-
Table 2. Comparison of Number of Eyes, Time to Resolution,Resolution, Recurrence Rate, and Follow-up for the Patients
with Conjunctival and Corneal Intraepithelial NeoplasiaTreated with Combination Therapy of Topical Retinoic Acid
and Topical Interferon Alfa-2b versus Topical InterferonAlfa-2b Alone
Current StudyInterferonAlone28
Combination RetinoicAcid and Interferon19
No. of eyes 27 89Median time to resolution 2.0 mos 1.6 mosComplete resolution 96.4% 97.75%Recurrence rate 3.7% 2.25%Median follow-up 42.4 mos 51.5 mos
oped a mild allergic papillary conjunctivitis that settled on
1972
alving the interferon dose to 0.5 million IU drops 3 timesaily.
Furthermore, our recent report of a rapid response ofcular surface dysplasia to combination treatment with top-cal all-trans retinoic acid 0.01% once every second day andnterferon alfa-2b that had been refractory to interferonlfa-2b and retinoic acid alone19 further supports the con-ept of synergism.
In conclusion, we hypothesize that topical all-trans reti-oic acid 0.01% once every second day and interferonlfa-2b may act synergistically and that combination treat-ent of interferon alfa-2b and retinoic acid may offer a
uperior alternative to interferon alfa-2b alone in treatingIN. Further studies into the efficacy of this combination
reatment should be undertaken. Masked, randomized, con-rolled studies will be required to prove synergy; however,n available evidence, combination treatment is safe andfficacious.
eferences
1. Grossniklaus HE, Green WR, Luckenbach M, Chan CC. Con-junctival lesions in adults: a clinical and histopathologicalreview. Cornea 1987;6:78–116.
2. Pizzarello LD, Jakobiec FA. Bowen’s disease of theconjunctiva: a misnomer. In: Jakobiec FA, ed. Ocular andAdnexal Tumors. Birmingham, AL: Aesculapius; 1978:553–71.
3. Napora C, Cohen EJ, Genvert GI, et al. Factors associatedwith conjunctival intraepithelial neoplasia: a case controlstudy. Ophthalmic Surg 1990;21:27–30.
4. Lee GA, Williams G, Hirst LW, Green AC. Risk factors in thedevelopment of ocular surface epithelial dysplasia. Ophthal-mology 1994;101:360–4.
5. Karp CL, Scott IU, Chang TS, Pflugfelder SC. Conjunctivalintraepithelial neoplasia: a possible marker for human immu-nodeficiency virus infection. Arch Ophthalmol 1996;114:257–61.
6. McDonnell JM, Mayr AJ, Martin WJ. DNA of human papil-lomavirus type 16 in dysplastic and malignant lesions of theconjunctiva and cornea. N Engl J Med 1989;320:1442–6.
7. Scott IU, Karp CL, Nuovo GJ. Human papillomavirus 16 and18 expression in conjunctival intraepithelial neoplasia. Oph-thalmology 2002;109:542–7.
8. Carroll J, Kuwabara T. A classification of limbal epitheliomas.Arch Ophthalmol 1965;73:545–51.
9. Erie JC, Campbell RJ, Leisegang TJ. Conjunctival and cornealintraepithelial and invasive neoplasia. Ophthalmology 1986;93:176–83.
0. Waring GO III, Roth AM, Ekins MB. Clinical and patholog-ical description of 17 cases of corneal intraepithelial neopla-sia. Am J Ophthalmol 1984;97:547–59.
1. Zaki AA, Farid SF. Management of intraepithelial and inva-sive neoplasia of the cornea and conjunctiva: a long-termfollow up. Cornea 2009:28:986–8.
2. Peksayar G, Soyturk MK, Demiryont M. Long-term results ofcryotherapy on malignant epithelial tumors of the conjunctiva.Am J Ophthalmol 1989;107:337–40.
3. Cerezo L, Otero J, Aragon G, et al. Conjunctival intraepithe-lial and invasive squamous cell carcinomas treated withstrontium-90. Radiother Oncol 1990;17:191–7.
4. Ferry AP, Meltzer MA, Taub RN. Immunotherapy with dini-
trochlorobenzene (DNCB) for recurrent squamous cell tumor
2
2
2
2
2
2
Krilis et al � CIN Retinoic Acid and Interferon Alfa-2b
of the conjunctiva. Trans Am Ophthalmol Soc 1976;74:154–71.
15. Karp CL, Moore JK, Rosa RH Jr. Treatment of conjunctivaland corneal intraepithelial neoplasia with topical interferonalpha-2b. Ophthalmology 2001;108:1093–8.
16. Frucht-Pery J, Rozenman Y. Mitomycin C therapy for cornealintraepithelial neoplasia. Am J Ophthalmol 1994;117:164–8.
17. Wilson MW, Hungerford JL, George SM, Madreperla SA.Topical mitomycin C for the treatment of conjunctival andcorneal epithelial dysplasia and neoplasia. Am J Ophthalmol1997;124:303–11.
18. Tabin G, Levin S, Snibson G, et al. Late recurrence and thenecessity for long-term follow-up in corneal and conjunctivalintraepithelial neoplasia. Ophthalmology 1997;104:485–92.
19. Skippen B, Tsang HH, Assad NN, Coroneo MT. Rapid re-sponse of refractory ocular surface dysplasia to combinationtreatment with topical all–trans retinoic acid and interferonalfa-2b [letter]. Arch Ophthalmol 2010;128:1368–9.
20. Khong JJ, Muecke J. Complications of mitomycin C therapyin 100 eyes with ocular surface neoplasia. Br J Ophthalmology2006;90:819–22.
21. Lichtinger A, Pe’er J, Frucht-Pery J, Solomon A. Limbal stemcell deficiency after topical mitomycin C therapy for primaryacquired melanosis with atypia. Ophthalmology 2010:117:431–7.
22. Di Girolamo N, Chui J, Coroneo MT, Wakefield D. Patho-
Footnotes and Financial Disclosures
Australia.
FTp
CMWA
genesis of pterygia: role of cytokines, growth factors, andmatrix metalloproteinases. Prog Retin Eye Res2004;23:195–228.
3. Ng J, Coroneo MT, Wakefield D, Di Girolamo N. Ultravioletradiation and the role of matrix metalloproteinases in thepathogenesis of ocular surface squamous neoplasia. InvestOphthalmol Vis Sci 2008;49:5295–306.
4. Uchida G, Yoshimura K, Kitano Y, et al. Tretinoin reversesupregulation of matrix metalloproteinase-13 in human keloid-derived fibroblasts. Exp Dermatol 2003;12(Suppl):35–42.
5. Marth C, Daxenbichler G, Dapunt O. Synergistic antiprolif-erative effect of human recombinant interferons and retinoicacid in cultured breast cancer cells. J Natl Cancer Inst 1986;77:1197–202.
6. Lippman SM, Kavanagh JJ, Paredes-Espinoza M, et al.13-cis-retinoic acid plus interferon alpha-2a: highly activesystemic therapy for squamous cell carcinoma of the cervix.J Natl Cancer Inst 1992;84:241–5.
7. Lippman SM, Shimm DS, Meyskens FL Jr. Nonsurgical treat-ments for skin cancer: retinoids and alpha-interferon. J Der-matol Surg Oncol 1988;14:862–9.
8. Schechter BA, Koreishi AF, Karp CL, Feuer W. Long-termfollow-up of conjunctival and corneal intraepithelial neoplasiatreated with topical interferon alfa-2b. Ophthalmology 2008;
115:1291–6.Originally received: August 14, 2011.Final revision: March 3, 2012.Accepted: March 27, 2012.Available online: June 14, 2012. Manuscript no. 2011-1223.1 Royal Prince Alfred Hospital, University of Sydney, Sydney, Australia.2 Prince of Wales Hospital, University of New South Wales, Sydney,
inancial Disclosure(s):he author(s) have made the following disclosure(s): Dr. Coroneo has aatent related to the treatment described in this study.
orrespondence:inas Coroneo, MD, FRACS, Department of Ophthalmology, Prince ofales Hospital, University of New South Wales, Randwick, Sydney,
ustralia. E-mail: [email protected].1973