Embed Size (px)
Citation preview

Treatment of Chronic Traumatic Bone Wounds
Microvascular Free Tissue Transfer: A 13-Year Experience in 96 Patients
JAMES W. MAY, JR., M.D.,* JESSE B. JUPITER, M.D.,t G. GREGORY GALLICO, III, M.D.,*DOUGLAS M. ROTHKOPF, M.D.,* and PAULA ZINGARELLI*
During a 13-year period at the Massachusetts General Hospital,Boston, Massachusetts, 97 microvascular free tissue transfershave been performed for soft-tissue reconstruction in 96 patientsfollowing bone debridement for chronic traumatic bone wounds.These 96 patients comprise a continuation study of 18 originalpatients reported in 1982. During a 13-year follow-up period(mean, 77.1 months), 95.8% of these 96 patients have enjoyedcomplete wound closure with a lack of drainage after the de-bridement and free tissue transfer. Most of the patients (89.6%)encountered in this study are ambulatory without assist and 5.2%of patients have undergone amputation. Twenty-three per centof patients required subsequent segmental bone defect recon-struction in the lower extremity after infection eradication. Thepathophysiology of chronic traumatic bony wounds is differentfrom that of chronic hematogenous osteomyelitis and thus a highincidence of long-term successful management can be seenthrough complete wound debridement and adequate soft-tissuecoverage.
D ~\ ESPITE ADVANCES MADE in medical and surgicalmanagement, chronic traumatic bony woundscontinue to present a difficult problem in patient
management.' 22 The etiology ofbone wounds has shiftedfrom a primary infectious origin to trauma with the in-creasing mobility of our society. 3,4,23-33
In 1982, as a preliminary report,' we presented 18 pa-tients in whom microvascular free tissue transfers wereused to close chronic traumatic lower extremity woundswith no reported recurrence ofdrainage seen in any patientduring a mean 19.3-month follow-up interval.' Free tissuetransfers" 34"43 were chosen as the soft-tissue treatment forthese patients because the degree of bone debridementwould not be limited by the amount of available localreconstructive tissues. 19,20,44-72 The purpose ofthis report
Presented at the 11 1th Annual Meeting of the American Surgical As-sociation, April 11-13, 1991, Boca Raton, Florida.
Address reprint requests to James W. May, Jr., M.D., MassachusettsGeneral Hospital, ACC-4, Suite 453, Boston, MA 02114.
Accepted for publication April 22, 1991.
From the Division of Plastic and Reconstructive Surgery,Departments of Surgery* and Orthopedic Surgery,t
Massachusetts General Hospital, Harvard Medical School,Boston, Massachusetts
is to present the long-term follow-up data for those initial18 patients and to add 78 additional patients to this initialgroup. Thus the total of 96 patients have been followedafter bone wound debridement and free tissue transferreconstruction for a mean 77.1 months.
Patients and Methods
In our series of 96 patients a mean period of chronicbone exposure and drainage was 39.6 months, with a rangeof 6 weeks to 41 years. The mean age was 32.8 years, witha range from 11 years to 66 years and including 11 femaleand 85 male patients.
Five criteria for the diagnosis of chronic bone woundswere applied for patient selection in this study,' includingchronic open draining bony wounds for more than 6weeks, a positive culture from the wound at the time ofdebridement,73'74 histologic evidence of nonliving bonewith inflammatory changes, with or without bacteria, andx-ray findings consistent with chronic bone infections.With increasing experience scans75'02 have now been de-leted from our preoperative assessmentl'03 because intra-operative bone debridement"'" is now used in determin-ing with accuracy the extent of bone involvement.'05
Regional bone wounds included skull (1), upper ex-tremity (1), femur (7), tibia (66), and ankle-foot (21). Inall patients a microvascular free tissue transfer operationwas carried out, including latissimus dorsi muscle flapwith skin graft or skin island (80 flaps) gracilis muscleflap with skin graft (11 flaps), and groin flap (6 flaps). Ineach case a flap was chosen that adequately provided anabundance of well-perfused wound closing tissues. No
241

Ann. Surg. * September 1991
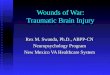
FIGS. IA and IB. (A) X-rayof distal tibial nonunion in a38-year-old woman with a6-year history of chronicdrainage and infected tibialnonunion. (B) Femoral an-giogram showing intact pos-terior tibial artery.
patient was included in whom local healthy flap tissueswere available.
Patient Management
Each patient was assessed clinically and a mutual de-cision was made regarding the possibility of treatmentresulting in a functional extremity."' 05"'06 Once decisionfor debridement and reconstruction was made, anarteriogram 105-108 was performed (Figs. la and b). Aninitial wound debridement was carried out under generalanesthesia where all exposed and contaminated or necroticbone was debrided under loupe magnification with a me-chanical burr. During debridement cultures and biopsyspecimens were taken from bone as well as soft tissue torule out a chronic cutaneous carcinoma.44"09'1'0 Thewound was then treated with moist dressings with repeatclinical examination of the wound to be certain that allnonvitalized and devascularized bone had been removed.If gross tissue necrosis persisted, an additional formal de-bridement was done. At the final procedure, redebride-ment was performed under intravenous antibiotic ad-ministration and a microvascular free tissue transfer (Fig.
2) was performed by two surgical teams working in donorand recipient sites. Free muscle flaps with skin grafts areused almost exclusively, with the procedure lasting be-tween 6 and 8 hours. Immediately before, during, andafter the operation, antibiotics were administered intra-venously for at least 1 week. Antibiotics were selected byour infectious disease consultants based on culture dataachieved at the time of initial bone debridement. In mostof our patients, antibiotics were administered intrave-nously for 6 weeks after operation.2""1'"2 After soft-tissuehealing, bone grafting was done ifindicated, and 6 monthsafter operatively, as in this case, ambulation and rehabil-itation (Figs. 3a to c) were well underway.
Results (Tables 1, 2, and 3)*Fate ofthe Initial 18 Patients*
The original 18 patients have now been followed for amean of 124.3 months (range, 114 to 156 months). A
* Study period ended August 1990.
242 MAY AND OTHERS

CHRONIC TRAUMATIC BONE WOUNDS
FIG. 2. Bony wound at thetime of surgical debridementand free latissimus dorsi flapcoverage.
single patient underwent a secondary tibial realignmentprocedure 1 year after successful wound debridement andclosure. Following this procedure the wound drained for10 days after operation, with antibiotic resolution of cul-ture identified pseudomonas aeruginosa organisms similarto those from his original chronic wound. He has unitedhis tibial osteotomy and has remained drainage free forthe following 7 years. An additional patient underwentfoot amputation for a painful foot and ankle 2 years aftersuccessful free flap chronic ankle wound closure. At thistime his wound was well healed and vessels were patentby direct operative inspection with negative deep culturestaken at the time of amputation.Thus recurrence of drainage occurred in 7.1% of the
original 18 patients followed for more than 10 years.
13- Year Cumulative Study in 96 Patients*
Ofthe patients in our cumulative study, a single patienthad microvascular failure of two sequential gracilis mi-crovascular free tissue transfers. The flaps were debridedin this patient and he ultimately had wound closure bylocal flap expansion techniques. He has remained drainagefree. Thus the ultimate free tissue transfer failure rate inthis study was 2.1%.
During the mean postoperative follow-up period of77.1months (range, 15 months to 156 months), there havebeen three additional patients that have manifested furtherdrainage after their initial operative sequence (Table 3).In one patient chronic drainage since 1942 following an
attempted knee fusion was unsuccessfully treated by de-bridement and free latissimus dorsi flap transfer. In thispatient drainage reoccurred 24 weeks after the initial flaptreatment and has persisted since that time. An additionalpatient developed drainage from the area ofa distal tibialnonunion, which previously had been draining for 6 years.This patient's drainage reoccurred 1.5 years after initialtreatment and responded to re-elevation of the flap andsecondary removal ofthe retained sequestrum. After thisthe patient has remained drainage free for the past 5 years.A third patient underwent a free latissimus dorsi transferto multiple areas oftibial chronic drainage with recurrentdrainage occurring from the distal tibial region within 2weeks of flap transfer. This area responded favorably toredebridement and adjustment of the initial flap. Thispatient ultimately underwent an above-the-knee ampu-tation for instability of the knee and poor lower leg func-tion. At the time of the above-the-knee amputation, no
evidence of chronic bony drainage or chronic bone in-fection could be found (Table 3).
Three patients in this series have died (Table 3). Thecause ofdeath in this group included metastatic sarcoma,intraoperative anesthetic death at the time of bone graftreconstruction, and nonmedicinal drug overdosage. Atthe time ofpatient death, all free flaps were healed withoutevidence of drainage.
Four patients with wounds ofthe femur, 3 with woundsofthe ankle-foot, and 27 of 66 patients with involvementof the tibia required bone grafting as tertiary procedures.All underwent successful bone graft procedures with
243VOl. 214.o NO. 3

MAY AND OTHERS
FIGS. 3A-C. (A) Appearance of muscle flap donor sitethrough short transaxillary incision. (B, C) Lateral viewand front view ofcontoured muscle with healed skin graft,5 months after operation and 3.5 months after a cancellous(tibial three centimeter defect) iliac wing bone graft. Shewas ambulatory 6 months after operation without braceor crutch.
union, with the exception of two tibial patients who cur-rently have established nonunions (Table 2). The patientswith healed bone grafts and all other living patients areambulatory, with the exception of one additional patientwho underwent below-the-knee amputation for a painfulbone graft with tibial nonunion, but without evidence ofinfection (Table 3).
DiscussionThe pathogenesis of chronic traumatic bony wounds
is substantially different from that of hematogenous os-teomyelitis. With hematogenous osteomyelitis,33 bonyinfection usually occurs in the sinusoids of the endostealblood supply33"'3'114 in the metaphyseal region of longbones. Here pathologic bacteria come to rest in a regionof relative blood stagnation with low oxygen tension. The
infection becomes established in this region and beginsto overwhelm the local host response,"5 as pus underpressure begins to spread down the medullary cavity.33"'6When the advancing infection has overcome the perfusioncharacteristics of the endosteal blood supply, frank bonynecrosis may intervene."7 This is even more likely in caseswhen the infection perforates through the bony cortexand begins to elevate the periosteum with additional lossof blood supply. A patient may be treated successfullywith intravenous antibiotics alone, but if progressive bonenecrosis has occurred, it becomes more difficult for thehost defense mechanisms plus antibiotics to counter ef-fectively the persistence of bacteria plus dead bone.' 16,117The ultimate result of this process may be significant bonenecrosis potentially extending throughout the length ofthe involved long bone.32'33'118
244 Ann. Surg. * September 1991

CHRONIC TRAUMATIC BONE WOUNDS
TABLE 1. Complications ofFree Tissue Transfer Wound ClosureSeen in 96 Patients
PercentageComplication Number of total
1. Free flap failure 2 2.12. Re-exploration of flaps 7 7.33. Recurrent drainage 4 4.24. Brachial plexus neuropraxia 7 7.35. Donor/recipient site hematoma 6 6.36. Skin graft loss 4 4.2
This well-established pathophysiologic process shouldbe contrasted with a dissimilar process seen in most cases
of traumatic bone infection. Under traumatic circum-stances a perfectly healthy and viable bone becomes in-vaded by bacteria through traumatic introduction. Duringthis process bony"19-2 and soft-tissue blood supply in theregion oftrauma may be interrupted, creating severe tissuedamage and cellular death'26"127 in varying degrees to thebone and soft tissues.'28 Under these circumstances, ifthewound were sterile and could be closed with well-perfusedsoft tissues, the devascularized bone could be invaded byvascular cutting cones and ultimately would be revascu-
larized and repopulated with osteocytes."7 This is an
identical process to that observed to occur when bonegrafts are accomplished under sterile conditions or whenwounds with minimal contamination are closed with earlywell-vascularized soft-tissue coverage.' However, undertraumatic circumstances with a high concentration of in-oculated bacteria, an ideal milieu exists devoid of bloodsupply'29 for the proliferation and feeding of bacteria inthe accompaniment ofserum-filled dead space. When thebacterial process is active with significant proliferation,the vascular cutting cone mechanism for revascularizationis halted.' 17 Under these circumstances the extent of ne-
crotic bone is usually limited to that amount of bone ini-
TABLE 2. Classification ofChronic Traumatic Tibial Bone Wounds(after surgical debridement)
Time toNo. of Ambulation*
Classificiation Patients (months)
Type I (tibia intact not requiring bonegraft) 39 1.5
Type II (tibia intact with bone graftrequired for functional structuralsupport) 5 5.5
Type IIlt (tibial defect 6 cm or less,with intact fibula) 14 11.4
Type IVt (tibial defect larger than 6 cm,with intact fibula) 5 12.0
Type V (tibial defect larger than 6 cm,without intact ipsilateral fibula) 3 12.7
* Time to ambulation without crutch or upper extremity assist.t A single patient underwent amputation for a painful leg in this group.
245TABLE 3. Ultimate Result ofBone Wound Closure
and Reconstruction in 96 Patients*
PatientResult Number Percentage
Drainage recurrence 4 4.2Amputation for inadequate
leg or foot 5 5.2Died 3 3.1Tibial nonunion 2 2.1Ambulatory without assist 86 89.6
* Percentages total more than 100% because some patients are includedin more than one category.
tially devascularized because the wound is in fact openedby the traumatic process before it becomes contaminatedand infected. Thus pus under pressure cannot extend thebone necrosis process. This is the reverse of what occursin hematogenous osteomyelitis, which may need to beopened (incised and drained) by the surgeon to avoid theextension of bone necrosis. Thus the extent of nonlivingbone seen in traumatic bony wounds is usually dictatedby the initial trauma and is not likely to be as extensiveas that seen in severe and neglected cases of chronic he-matogenous osteomyelitis.49
If the differences in the pathophysiology as describedcan be translated into practice management, then it shouldbe possible in traumatic chronic bony wounds to debridecompletely the localized ischemic"0 130-134 or nonlivingbone and soft tissues and to close the wound with well-perfused tissues.49"35"36We have selected a subset group of our patients who
have required free tissue transfers as our study group totest this hypothesis. In this group the size ofthe flap chosento fill the defect was not limited by the availability oflocaltissues. Thus the bone and soft-tissue debridement couldbe based only on disease removal considerations ratherthan the concern always present when local tissues areused as to whether there will be enough tissue to close thewound. 149
In this 13-year study, 4 of 95 patients (4.2%) with suc-cessful free transfers have manifested recurrent drainageafter initial treatment. After secondary treatment only asingle patient remains with recalcitrant drainage. An ad-ditional subgroup of patients (five) underwent amputa-tion. This group comprises one patient who had persistentdrainage and an unsatisfactory extremity and four patientsin whom, in retrospect, an incorrect judgment was madeas to the salvageability ofthe patients' lower legs and feet.It is our feeling that the initial drainage recurrence ratein four patients represented our inability to recognize anddebride completely the wound and should not suggestthat the thesis of long-term, successful wound treatmentin chronic traumatic bony wounds is not possible. It is ofinterest to note that ofthe three patients with tibial chronic
VOl. 214.-NO. 3

MAY AND OTHERS
bony wounds who failed to maintain wound closure, allthree had type I (intact tibia) tibial status after wounddebridement. In two of these patients it was recognizedthat a borderline debridement was done to avoid makingthe tibia unstable, thus avoiding a more complex defectbone graft reconstruction. Thus ironically it was psycho-logically easier for the surgeon to debride a tibia that al-ready had a defect than it was to debride an intact tibiato the point that a defect was created to solve the boneinfection problem.
Experimentally it has been shown that well-perfusedmuscle flaps'08"'37 with increased oxygen7'130'138-143 dealwith bony wounds in an optimal way and promote woundhealing.'" In the experience of others4` 129,35,42,43 145 andin the discussion of our initial patient presentation,' itwas noted by experienced workers in this field that oneshould not overstate the findings of our preliminary re-port.146"47 We fully agreed with this position and statedit in our initial report: "one cannot say that chronic boneinfection was permanently cured or prevented in any pa-tient in this study." However we went on to state that itwas encouraging that the mean drainage-free period of19.3 months for the patients in our initial report was seen'considering that most patients with failure of treatmentof chronic bony wounds will recur within the first yearafter treatment.4"48 If one looks at the long-term resultsof our original 18 patients presented in 1982,' there hasbeen recurrence of drainage in a single patient with an-tibiotic resolution during a mean follow-up period of 1 16months (10.3 years). This 7.1% drainage recurrence rateis in the same range as our 4.2% drainage recurrence rateseen in our overall cumulative series followed for a mean77 months. It is of interest that in the overall series ourfour recurrent drainage patients drained within a mean 7months ofthe their original treatment, making it unlikelythat the overall group recurrence rate will be significantlygreater than that of our initial 18 patients.The primary cause, in our series, of failure in chronic
bony wound treatment was inadequate bone debride-ment."49 The microsurgical free tissue transfer has donemore in our patient management to allow freedom ofdebridement than any other single development in themanagement of patients with chronic bony wounds. Ifonly a small amount of nonliving bone and significantbacteria are left behind,'50 an established sequestrum andseed for ultimate failure over time may ensue. 142,105,135,150
It is possible that the degree and the extent of boneinfection could require a debridement, which is inconsis-tent with skeletal reconstruction from a practical viewpoint. Under these circumstances draining woundmaintenance or even amputation surgery may be in thepatient's best interest. 151"152 Using our recently developedclassification'05 for chronic bony wounds ofthe tibia (Ta-
ble 2), our ability has been enhanced in advising the pa-tient as to the time and bone reconstructive commitmentthat will be needed to achieve a functional limb.We continue to be enthusiastic over the use of free
muscle transfers "'05 53'154 covered with skin grafts.'05"155"156This method of wound closure provides minimal donorsite deformity, and with denervated muscle'57-'6' used tofill the recipient site, excellent wound contour has beenachieved and maintained'62 during the length ofour study.Of course a free tissue transfer should only be used whenan adequate and well-tolerated local means of soft-tissuewound closure is not available.'33"'05 However the decisionas to how much bone and soft tissue to debride shouldbe based on local tissue viability and not on the volumeoflocal reconstructive tissue available to close the wound.
It would appear that chronic traumatic bony wounds aretheoretically successfully treatable by thorough debridementand soft-tissue reconstruction. One would find little dis-agreement with the concept that extremity amputation cancure chronic bony wounds.'5' Thus the concept of localwound (bone and soft tissue) amputation with extremitysalvage by soft- and hard-tissue reconstruction should notseem illogical. A 4.2% recurrence rate during a mean 77-month follow-up period in these 96 patients compares fa-vorably with other reports5 9s1 29,30,35,43145152,163-165 andmethods.4'5'7'8"l1133, 166-188The treatment of chronic traumatic bony wounds is
difficult and it is not surprising that significant pessimismhas existed concerning the cure of such patients.35"47"89On the other hand, it is possible that this pessimism31 inpart has been based on the lack of total involved boneand soft-tissue wound debridement in the face ofinabilityto completely cover the recipient wound with well-vas-cularized tissues. Perhaps some day "cure rates"4 will bereported in patient series with chronic traumatic bonywounds rather than disease-free interval.4"90 We believethat the freedom ofdebridement provided by the almost-unlimited microsurgical free tissue wound closure tech-nique has provided a very high chance of successful long-term wound management in patients with chronic trau-matic bony wounds. It would appear that the results fromour 13-year study are consistent with this interpretation.Bony reconstruction of the lower extremity after infectioneradication is the major challenge facing reconstructivesurgeons in the future.
Acknowledgments
The authors thank the surgical residents and fellows in the Divisionof Plastic Surgery and Orthopedic Surgery who assisted in the manage-ment of the patients reported. They also thank Drs. Al Shiller, HenryMankin, A. W. Karchmer, and Ronald Malt for their advice, support,and assistance in this study and Marjorie Ciampa for technical assistancein preparing this manuscript.
246 Ann. Surg. * Septembet 1991

Vol. 214 * No.3 CHRONIC TRAUMATIC BONE WOUNDS 247References
1. May JW Jr, Gallico GG III, Lukash FN. Microvascular transfer offree tissue for closure ofbone wounds ofthe distal lower extremity.N Engl J Med 1982; 306:253-257.
2. Waldvogel FA, Medoff G, Swartz MN. Osteomyelitis: a review ofclinical features, therapeutic considerations and unusual aspects.N Engl J Med 1970; 282:198-206, 260-266, 316-322.
3. Waldvogel FA, Vasey H. Osteomyelitis: the past decade. N Engl JMed 1980; 303:360-370.
4. Davis JC, Heckman JD, DeLee JC, Buckwald FJ. Chronic non-hematogenous osteomyelitis treated with adjuvant hyperbaricoxygen. J Bone Joint Surg 1986; 68A(8):1210-1217.
5. Clawson DK, Davis FJ, Hansen ST Jr. Treatment of chronic os-teomyelitis with emphasis on closed suction-irrigation technic.Clin Orthop 1973; 96:88-97.
6. Davis JC. Refractory osteomyelitis of the extremities and axialskeleton. In Davis JC, Hunt TK, eds. Hyperbaric Oxygen Ther-apy. Bethesda, MD: Undersea Medical Society, 1977, pp 217-227.
7. Depenbusch Fl, Thompson RE, Hart GB. Use ofhyperbaric oxygenin the treatment of refractory osteomyelitis. A preliminary report.J Trauma 1972; 12:807-812.
8. Slack WK, Thomas DA, Perrins D. Hyperbaric oxygenation inchronic osteomyelitis. Lancet 1965; i: 1093-1094.
9. Morrey BF, Dunn JM, Heimbach RD, Davis J. Hyperbaric oxygenand chronic osteomyelitis. Clin Orthop 1979; 144:121-127.
10. Strauss MB. Chronic refractory osteomyelitis: review and role ofhyperbaric oxygen. Hyperbaric Oxygen Rev 1980; 1:231-256.
11. Kelly PJ, Martin WJ, Coventry MB. Chronic osteomyelitis. II.Treatment with closed irrigation and suction. JAMA 1970; 213:1843-1848.
12. Klemm K, Contzen H, Lennert KH. Gentamycin-PMMA-Kugelnbei knochen-und weichteilinfektionen-ergebnisse aus der ber-ufsgenossenschaftlichen. Unfalklinik Frankfurt/Main. AktuelProbl Chir Orthop 1979; 12:128-132.
13. Anderson LD, Horn LG. Irrigation-suction technic in the treatmentof acute hematogenous osteomyelitis, chronic osteomyelitis andacute and chronic joint infections. South Med J 1970; 63(7):745-754.
14. Mayers BR, Berson, BL, Gilber M, Hirschman SZ. Clinical patternsof osteomyelitis due to gram-negative bacteria. Arch Intern Med1973; 131:228-233.
15. Taylor AR, Maudsley RH. Instillation-suction technique in chronicosteomyelitis. J Bone Joint Surg 1970; 52B(1):88-92.
16. Webster DA, Spadaro JA, Becker RO, Kramer S. Silver anodetreatment ofchronic osteomyelitis. Clin Orthop and Rel Res 1981;161:105-115.
17. Kelly PJ. Osteomyelitis in the adult. Orthop Clin North Am 1975;6:973-981.
18. Brown RF. The management of traumatic tissue loss in the lowerlimb, especially when complicated by skeletal injury. J PlastSurg(Br), 1965; 18:26-50.
19. Ger R. Muscle transposition for treatment and prevention ofchronicpost-traumatic osteomyelitis of the tibia. J Bone Joint Surg(Am)1977; 59:784-791.
20. West WF, Kelly PJ, Martin WJ. Chronic osteomyelitis. I. Factorsaffecting the results of treatment in 186 patients. JAMA 1970;213: 1837-1842.
21. Burri C. Post-traumatic osteomyelitis. Berne: Hans Huber, 1975,pp 252-288.
22. Arnold PG, Irons GB. Lower extremity muscle flaps. Orthop ClinNorth Am 1984; 15(3):441-449.
23. Rosenthal RE, MacPhail JA, Ortiz JE. Nonunion in open tibialfractures: analysis of reasons for failure of treatment. J Bone JointSurg(Am) 1977; 59:244-248.
24. Carpenter EB, Dobbie JJ, Siewers CF. Fractures of the shaft of thetibia and fibula. Arch Surg 1952; 64:443-456.
25. Gustilo RB, Anderson JT. Prevention ofinfection in the treatmentof one thousand and twenty five open fractures of long bones:
retrospective and prospective analyses. J Bone Joint Surg(Am)1976; 58(4):453-458.
26. Cierny G, Byrd HS, Jones RE. Primary versus delayed soft tissuecoverage for severe open tibial fractures. A comparison ofresults.Clin Orthop 1983; 178:54-63.
27. Edwards P. Fracture of the shaft of the tibia: 493 consecutive casesin adults-importance of soft tissue injury. Acta Orthop Scand1965; 76(Suppl): 1-82.
28. Tonnesen PA, Heerfordt J, Pers M. 150 open fractures ofthe tibialshaft-the relation between necrosis of the skin and delayedunion. Acta Orthop Scand 1975; 46:823-835.
29. West WF, Kelly PJ, Martin WJ. Chronic osteomyelitis. I Factorsaffecting the results of treatment in 186 patients. JAMA 1970;213:1837-1842.
30. Fitzgerald RH, Ruttle PE, Arnold PG, et al. Local muscle flaps inthe treatment of chronic osteomyelitis. J Bone Joint Surg 1985;67A(2): 175-185.
31. Kelly PJ. Osteomyelitis in the adult. Orthop Clin North Am 1975;6(4):983-989.
32. Alho A, Koskinen EVS, Malmberg H. Treatment of chronic he-matogenous osteomyelitis: a clinical study of 65 cases. Int Surg1970; 54:366-374.
33. Starr C. Acute hematogenous osteomyelitis. Arch of Surg 1922; 4:567-587.
34. Daniel RK, Taylor GI. Distant transfer ofan island flap by micro-vascular anastomoses. Plast Reconstr Surg 1973; 52:111-117.
35. Weiland AJ, Moore JR, Daniel RK. The efficacy of free tissuetransfer in the treatment of osteomyelitis. J Bone Joint Surg 1984;66A(2): 181-193.
36. Garrett JC, Buncke HJ. Free groin flap transfer for skin defectsassociated with orthopaedic problems ofthe extremitips. Am Surg1979; 45:597-601.
37. Serafin D, Sabatier RE, Morris RL, Georgiade NG. Reconstructionof the lower extremity with vascularized composite tissue: im-proved tissue survival and specific indications. Plast ReconstrSurg 1980; 66:230-241.
38. Maxwell GP, Hoopes JE. Management of compound injuries ofthe lower extremity. Plast Reconstr Surg 1979; 63:176-185.
39. Mathes SJ, Nahai F, Vasconez L. Myocutaneous free-flap transfer.Plast Reconstr Surg 1978; 62:162-166.
40. Irons GB, Witzke DJ, Arnold PG, et al. Use of the omental freeflap for soft tissue reconstruction. Ann Plast Surg 1983; 11:501-507.
41. Mathes SJ. Letter to the editor. N Eng J Med 1982; 307(2): 121.42. Swartz WM, Mears DC. The role of free tissue transfers in lower
extremity reconstruction. Plast Reconstr Surg 1985; 76(3):364-373.
43. Wood MB, Cooney WP, Irons GB. Lower extremity salvage andreconstruction by free tissue transfer. Clin Orthop and Rel Res1985; 201:151-161.
44. Lord JP. The closure of chronic osteomyelitis cavities by plasticmethods. Surg Gynecol Obstet 1935; 60:853-856.
45. Mercer W. Orthopedic Surgery, 3rd Edition. Baltimore: Williams& Wilkins, 1944.
46. Gutierrez A. El procedimiento de avelino gutierrez en el tratamientode las osteomielitis cronicas. Rev de cir de Buenos Aires. 1941;20:143-162.
47. Marques S. Preenchimento das cavidades osseas osteomieliticascom transplante muscular. Arq Brasil de Cir e Ortop 1936; 4:223-233.
48. Stotz W. Die muskellappenplastik bei der schuss-osteomyelitis.Zentralbl fchir 1942; 69:427-435.
49. Stark WJ. The use of pedicled muscle flaps in the surgical treatmentof chronic osteomyelitis resulting from compound fractures. JBone Joint Surg 1946; 28:343-350.
50. Prigge EK. The treatment of chronic osteomyelitis by the use ofmuscle transplant or iliac graft. J Bone Joint Surg 1946; 28:576-593.
51. Harrison SH. Fractures ofthe tibia complicated by skin loss. J PlastSurg(Br) 1968; 21:262-276.
52. Barfod B, Pers M. Gastrocnemius-plasty for primary closure of

248 MAY AND OTHERS Ann. Surg. - September 1991
compound injuries of the knee. J Bone Joint Surg(Br) 1970; 52:124-127.
53. Cave EF. Filling defect large bone defects with muscle transplants.Bull Hosp Joint Dis 1960; 21:129-135.
54. Ger R. The management of pretibial skin loss. Surg 1968; 63:757-763.
55. Ger R, Efron G. New operative approach in the treatment ofchronicosteomyelitis of the tibial diaphysis: a preliminary report. ClinOrthop 1970; 70:165-169.
56. Ger R. The management of open fracture of the tibia with skinloss. J Trauma 1970; 10: 112-121.
57. Mathes SJ, McCraw JB, Vasconez LO. Muscle transposition flapsfor coverage oflower extremity defects; anatomic considerations.Surg Clin North Am 1974; 54:1337-1354.
58. Pers M, Medgyesi S. Pedicle muscle flaps and their applications inthe surgery of repair. J Plast Surg(Br) 1973; 26:313-321.
59. Prigge EK. The treatment of chronic osteomyelitis by the use ofmuscle transplant or iliac graft. J Bone Joint Surg 1946; 28:576-593.
60. Vasconez LO, Bostwick J III, McCraw J. Coverage of exposed boneby muscle transposition and skin grafting. Plast Reconstr Surg1975; 53:526-530.
61. Jayes PH. Cross-leg flaps: a review of sixty cases. Br Plast Surg1951; 3:1-5.
62. Stark RB. The cross-leg flap procedure. Plast Reconstr Surg 1952;9:173-204.
63. Cannon B, Lischer CE, Davis WB, et al. The use of open jumpflaps in lower extremity repairs. Plast Reconstr Surg 1947; 2:336-341.
64. Feldman JJ, Cohen BE, May JW Jr. The medial gastrocnemiusmyocutaneous flap. Plast Reconstr Surg 1978; 61:531-539.
65. Arnold PG, Prunes-Carrillo F. Vastus medialis muscle flap forfunctional closure of the exposed knee joint. Plast Reconstr Surg1981; 68:69-72.
66. Arnold PG, Mixter RC. Making the most of the gastrocnemiusmuscles. Plast Reconstr Surg 1983; 62:38-48.
67. McCraw J, Fishman JH, Sharzer LA. The versatile gastrocnemiusmyocutaneous flap. Plast Reconstr Surg 1978; 62:15-23.
68. Mathes SJ, Nahai F. Muscle flap transposition with function pres-ervation. Technical and clinical consideration. Plast ReconstrSurg 1980; 66:242-249.
69. Mathes S, Nahai F. Clinical Atlas of Muscle and MusculocutaneousFlaps. St. Louis: CV Mosby, 1979.
70. Dibbell DG, Edstrom LE. The gastrocnemius myocutaneous flap.Clin Plast Surg 1980; 7:45-50.
71. Ger R. The technique of muscle transposition in the operativetreatment oftraumatic and ulcerative lesions of the leg. J Trauma1971; 11:502-510.
72. Jurkiewicz MJ, Bostwick J III, Hester TR, et al. Infected mediansternotomy wound: successful treatment by muscle flaps. AnnSurg 1980; 191:738-744.
73. Mackowsiak PA, Jone SR, Smith JW. Diagnostic value of sinustract cultures in chronic osteomyelitis. JAMA 1978; 239:2772-2775.
74. Kelly PJ. Infected nonunion of the femur and tibia. Orthop ClinNorth Am 1984; 15(3):481-490.
75. Sayle B, Cierny G, Mader J. Indium-Ill chloride imaging in thedetection of osteomyelitis. J Nuc Med 1983; 24(5):72(abstr).
76. Graham GD, Lunday MM, Frederick PJ, et al. Predicting the cureof osteomyelitis under treatment: concise communication. J NuclMed 1983; 24:110-113.
77. Graham GD, Lundy MM, Moreno AJ, et al. The role of Tc-99mMDP and Ga-67 citrate in predicting the cure of osteomyelitis.Clin Nucl Med 1983; 8:344-346.
78. Hartshorne GG, Lancaster J, Berger D. Gallium-67/technitrium99m methylene diphosphorate ratio imaging-Early rabbit os-teomyelitis and fracture. J Nuc Med 1985; 26(3):272-277.
79. Park HM, Wheat U, Siddiqui AR, et al. Scintigraphic evaluationof diabetic osteomyelitis: Concise communication. J Nucl Med1982; 23:569-573.
80. Lisbona R, Rosenthall L. Observations on the sequential use of99mTc-phosphate complex and 6"Ga imaging in osteomyelitis,cellulitis, and septic arthritis. Radiology 1977; 123:123-129.
81. Treves S, Khettry J, Broker FH, et al. Osteomyelitis: early scinti-graphic detection in children. Pediatrics 1976; 57:173-186.
82. Trackler RT, Miller KE, Sutherland DH, et al. Childhood pelvicosteomyelitis presenting as a "cold" lesion on bone scan: casereport. J Nucl Med 1976; 17:620-622.
83. Tilden RL, Jackson J, Enneking WF, et al. 99gm Te-polyphosphate:histological localization in human femurs by autoradiography. JNucl Med 1973; 14(8):576-578.
84. Garnett ES, Cockshott WP, Jacobs J. Classical acute osteomyelitiswith a negative bone scan. Br J Radiol 1977; 50(598):757-760.
85. Kaye M, Silverton S, Rosenthal L. Technetium-99m-pyrophos-phate: studies in vivov and vitro. J Nucl Med 1975; 16(l):40-45.
86. Howie DW, Savage JP, Wilson TG, et al. The technetium phosphatebone scan in the diagnosis of osteomyelitis in childhood. J BoneJoint Surg(Am) 1983; 65:431-437.
87. Erasmie U, Hirsch G. Acute haematogenous osteomyelitis in chil-dren-the reliability of skeletal scintigraphy. Z Kinderchir 1981;32:360-366.
88. Gelfand MJ, Silberstein EB. Radionuclide imaging: use in diagnosisof osteomyelitis in children. JAMA 1977; 237:245-247.
89. Gilday DL, Paul DJ, Paterson J. Diagnosis ofosteomyelitis in chil-dren by combined blood pool and bone imaging. Radiology 1975;117:331-335.
90. O'Mara RE, Wilson GA, Burke AM. Skeletal imaging in osteo-myelitis. J Nucl Med 1983; 24:71-72(abstr).
91. Genant HK, Rautovich GL, Singh M, et al. Bone-seeking radio-nuclides: an in vivo study of factors effecting skeletal uptake.Radiology 1974; 113(2):373-382.
92. Majd M, Frankel RS. Radionuclide imaging in skeletal inflam-matory and ischemic disease in children. AJR 1976; 126:832-841.
93. Lisbona R, Rosenthal L. Radionuclide imaging of septic joints andtheir differentiation from periarticular osteomyelitis and cellulitisin pediatrics. Clin Nucl Med 1977; 10:337-343.
94. Merkel KD, Fitzgerald RH Jr, Brown ML, et al. Comparison ofindium-WBC and sequential Tc-Ga imaging in suspected low-grade osteomyelitis with surgical correlation. (Abstract) OrthopTrans 1983; 7:326.
95. Ganel A, Horozowski H, Zaltman S, et al. Sequential use of90mTc-MDP and Ga imaging in bone infection. Orthop Rev 1981; 7:73-77.
96. Handmaker H, Leonards R. The bone scan in inflammatory osseousdisease. Semin Nucl Med 1976; 6:95-105.
97. Hemborg PF, Kempi AV; van der Linden W. Scintigraphy with99mmTc-tripolyphosphate in the early diagnosis of osteomyelitis.Nuklearmedizin 1976; 15:53-55.
98. Zamoukian MH, Pera A. Diagnosing osteomyelitis. Surgical Roundsfor Orthopedics 1988; 17-26.
99. Sayle BA, Fawcett D, Wilkey DJ, et al. Indium III chloride imagingin chronic osteomyelitis. J Nuc Med 1985; 26:225-229.
100. Silver IA. Cellular microenvironment in healing and non-healingwounds. In Hunt TK, Heppenstall RB, Pines E, Rovee D, eds.Soft and Hard Tissue Repair, Biological and Clinical Aspects.New York: Praeger, 1984, pp 50-66.
101. Staab EV, McCartney WH. Role of gallium 67 in inflammatorydisease. Semin Nucl Med 1978; 8:193-204.
102. Davis MA, Jones AG. Comparison of 99m Tc-labeled phosphateand phosphonate agents skeletal imaging. Semin Nucl Med 1976;6:19-31.
103. Wheat J. Diagnostic stratagies in osteomyelitis. Am J Med 1985;78(6B):218-224.
104. Damhold VV. Treatment of chronic osteomyelitis. Acta OrthopScand 1982; 53:715-720.
105. May JW Jr, Jupiter JB, Weiland AJ, Byrd HS. Current ConceptsReview. Clinical classification of post-traumatic tibial osteomy-elitis. J Bone Joint Surg 1989; 71A(9):1422-1428.

Vol. 214 * No.3 CHRONIC TRAUMATIC BONE WOUNDS 249
106. May JW Jr, Gallico GG III, Jupiter JB, Savage RC. Free latissimusdorsi muscle flap with skin graft for the treatment of chronicbony wounds. Plast Reconstr Surg 1984; 73:641-651.
107. May JW Jr, Athansoulis CA, Donelan MB. Preoperative magni-fication angiography ofdonor and recipient sites for clinical freetransfer of flaps or digits. Plast Reconstr Surg 1979; 64:483-490.
108. Mathes SJ, Alpert BS, Chang N. The use of the muscle flap inchronic osteomyelitis. Experimental and clinical correlation. PlastReconstr Surg 1982; 69:815-828.
109. Fitzgerald RH, Brewer NS, Dahlin DC. Squamous-cell carcinomacomplicating chronic osteomyelitis. J Bone Joint Surg(Am) 1976;58:1146-1148.
110. Look P, Kleinau W, Henze E. Das Fistelkarzinom aufdem Bodender chronischen Osteomyelitis. Zentralbi Chir 1977; 102:998-1005.
111. Heckman RO, Buckner CD, Cleft, RA, et al. A modified rightatrial catheter for access of the venous system in marrow trans-plant recipients. Surg Gynecol Obstet 1979; 148:871-874.
112. Eisenberg JM, Kitz DS. Savings from outpatient antibiotics therapyof osteomyelitis. JAMA 1986; 255(12):1584-1588.
113. Trueta J. Acute haematogenous osteomyelitis: its pathology andtreatment. Bull Hosp Joint Dis 1953; 14:5-23.
114. Trueta J, Morgan JD. The vascular contribution to osteogenesis.J Bone Joint Surg 1960; 42B:97-109.
115. Hohn DC, MacKay RD, Halliday B, Hunt TK. Effect of 02 tensionon microbicidal function of leukocytes in wound and in vitro.Surg Forum 1976; 27(62): 18-20.
116. Brodie Sir BC, Lecture on abscess of the tibia. London MedicalGazette 1845; 36:1399-1403.
117. Cierny G, MaderJT. Adult chronic osteomyelitis. Orthopedics 1984;7(10):1557-1564.
118. Winters JL, Cahen I. Acute hematogenous osteomyelitis: a reviewof sixty-six cases. J Bone Joint Surg 1960; 42(1):691-704.
119. Gross PM, Marcus ML, Heistad DD. Measurement of blood flowto bone and marrow in experimental animals by means of themicrosphere technique. (Current Concepts Review) J Bone JointSurg 1981; 3A(6):1028-1031.
120. Brookes M. The blood supply ofbone. London: Butterworths, 1971.121. Cumming JD. A study of blood flow through bone marrow by a
method of venous effluent collection. J Physiol 1962; 162:13-20.
122. Kane WJ, Grim E. Blood flow to canine hind-limb bone, muscle,and skin. A quantitative method and its validation. J Bone JointSurg 1969; 51A:309-322.
123. Kelly PJ, Yipintosoi T, Bassingthwaighte JB. Blood flow in caninetibial diaphis estimated by iodoantipyrine-'25 I Washout. J ApplPhysiol 1971; 31:38-47.
124. Laumen EL, Kelly PJ. Blood flow, oxygen consumption, carbondioxide production, and blood calcium and pH changes in tibialfractures in dogs. J Bone Joint Surg 1969; 5 1A:298-308.
125. Paradis GR, Kelly PJ. Blood flow and mineral deposition in caninetibial fractures. J Bone Joint Surg 1975; 57A:220-226.
126. Rhinelander FW. Tibial blood supply in relation to fracture healing.Clin Orthop 1974; 105:37-81.
127. Berggren A, Weiland AJ, Dorfman H. The effect ofprolonged isch-emia time on osteocyte and osteoblast survival in composite bonegrafts revascularized by microvascular anastomoses. Plast Re-constr Surg 1982; 69(2):290-293.
128. Holden CA. The role of blood supply to soft tissue in the healingof diaphyseal fractures. J Bone Joint Surg 1972; 54A:993-1000.
129. Niinikoski J, Hunt TK. Oxygen tensions in healing bone. SurgGynecol Obstet 1972; 134(5):746-750.
130. Hamblin DL. Hyperbaric oxygenation. Its effect on experimentalstaphylococcal osteomyelitis in rats. J Bone Joint Surg 1968; 5OA:1129-1141.
131. Hunt TK, Twomey P, Zederfeldt B, Dunphy JE. Respiratory gastensions and pH in healing wounds. Am J Surg 1967; 114:302-307.
132. Mader Jt, Brown GL, Guckian JC, et al. A mechanism for the
amelioration by hyperbaric oxygen ofexperimental staphylococcalosteomyelitis in rabbits. J Infect Dis 1980; 142:915-922.
133. Morrey BF, Dunn JM, Heimbach RD, Davis J. Hyperbaric oxygenand chronic osteomyelitis. Clin Orthop 1979; 144:121-127.
134. Remensnyder JP, Majno G. Oxygen gradients in healing wounds.Am J Pathol 1968; 52:301-323.
135. Key JA. Sulfonamides in the treatment of chronic osteomyelitis.J Bone Joint Surg 1944; 26:63-70.
136. Calderon W, Chang N, Mathes SJ. Comparison of the effect ofbacterial inoculation in musculotaneous and fasciocutaneousflaps. Plast Reconstr Surg 1986; 77(5):785-792.
137. Chang N, Mathes SJ. Comparison of the effect of bacterial inoc-ulation in musculocutaneous and Rondour pattern flaps. PlastReconstr Surg 1982; 70(1):1-9.
138. Hohn DC, MacKay RK, Halliday B, Hunt TK. The effect of 02tension on the microbicidal function of leukocytes in woundsand in vitro. Surg Forum 1976; 27:18-20.
139. Hunt TK, Pai MP. The effect of varying ambient oxygen tensionson wound metabolism and collagen synthesis. Surg Gynec andObstet 1972; 135:561-567.
140. Hunt TK, Linsey M, Grislis G, et al. The effect ofdiffering ambientoxygen tensions on wound infection. Ann Surg 1975; 181:35-39.
141. Hunt TK, Halliday B, Knigton DR, et al. Impairment of micro-bicidal function in wounds: correction with oxygenation. In HuntTK, Heppenstall RB, Pines E, Rovee D, eds. Soft and Hard TissueRepair, Biological and Clinical Aspects. New York: Praeger, 1984,pp 455-468.
142. Knighton DR, Halliday B, Hunt TK. Oxygen as an antibiotic: theeffect of inspired oxygen on infection. Arch Surg 1984; 119:199-204.
143. Mader JT, Guckian JC, Glass DL, Reinarz JA. Therapy with hy-perbaric oxygen for experimental osteomyelitis due to staphy-lococcus aureus in rabbits. J Infect Dis 1978; 138:312-318.
144. Mokhtar A, Murray KA, Russell RC, Zook EG. Experimentalevaluation of free tissue transfer to promote healing of infectedwounds in dogs. Ann of Plast Surg 1986; 17(l):6-12.
145. Wood MB, Cooney WP. Vascularized bone segment transfers formanagement ofchronic osteomyelitis. Orthop Clin ofNorth Am1984; 15(3):461-473.
146. Ger R. The muscle flap for management of osteomyelitis. Letterto the editor. N Eng J Med 1982; 307(2): 121.
147. Moore JR, Weiland AJ. Free vascularized bone and muscle flapsfor osteomyelitis. Orthop 1986; 9(6):819-824.
148. Alho A, Koskinen EVS, Malmberg H. Osteomyelitis in nonoper-ative and operative fracture treatment. A survey of 49 adults.Clin Orthop and Related Res 1972; 82:123-133.
149. Ger R, Efron G. New operative approach in the treatment ofchronicosteomyelitis of the tibial diaphysis. A preliminary report. ClinOrthop and Rel Res 1970; 70:165-169.
150. Masem M, Greenberg BM, Hoffman C, et al. Comparative bacterialclearances of muscle and skin/subcutaneous tissues with andwithout dead bone: a laboratory study. Plast Reconstr Surg 1990;85(5):773.
151. Horwitz T. Surgical treatment of chronic osteomyelitis. Compli-cating fractures. Clin Orthop 1973; 96:118-29.
152. Cierny G III, Mader JT, Penninck JJ. A clinical staging system foradult osteomyelitis. Contemp Orthop 1985; 10(5): 17-37.
153. Bartlett SP, May JW Jr, Yaremchuk MJ. The latissimus dorsi mus-cle: a fresh cadaver study of the primary neurovascular pedicle.Plast Reconstr Surg 1981; 67:631-636.
154. Guignard RM, Krupp S. The role of microvascular free soft tissuetransfer in reconstructive surgery. Ann of Plast Surg 1986; 16(5):399-409.
155. May JW Jr, Lukash FN, GallicoGG III. Latissimus dorsi free muscleflap in lower-extremity reconstruction. Plast Reconstr Surg 1981;68:603-607.
156. Gordon L, Buncke HJ, Alpert BS. Free latissimus dorsi muscleflap with split thickness skin graft cover: a report of 16 cases.Plast Reconstr Surg 1982; 70(2):173-178.

250 MAY AND OTHERS Ann. Surg. September 1991
157. Knowlton GC, Hines HM. Kinetics of muscle atrophy in differentspecies. Proc Soc Exp Biol Med 1936; 35:394-398.
158. Tower SS. Atrophy and degeneration in skeletal muscle. Am JAnat 1935; 56:1-43.
159. Guttman E. Effect of delay of innervation on recovery of muscleafter nerve lesions. J Neurophysiol 1948; 11:279-294.
160. Sunderland S, Ray LJ. Denervation changes in mammalian striatedmuscle. J Neurol Neurosurg Psychiatry 1950; 13:159-177.
161. Gutman E, Zelena J. Morphological changes in the denervatedmuscle. In Guttman E, ed. The Denervated Muscle. Prague:Publishing House ofthe Czechoslovak Academy of Science, 1962,pp 57-102.
162. Daniel RK, May JW Jr. Free flaps: An overview. Clin Orthop 1978;133:122-131.
163. Off HW. The treatment of osteomyelitis and other infected woundsby drainage and rest. Surg Gynec and Obstet 1927; 45:446-464.
164. Irons GB, Fisher J, Schmitt EH. Vascularized muscular and mus-culocutaneous flaps for management of osteomyelitis. Ortho ClinNorth Am 1984; 15(3):473-480.
165. Hall BB, Fitzgerald RH Jr, Rosenblatt JE. Anerobic osteomyelitis.J Bone Joint Surg (Am) 1983; 65:30-35.
166. Mowlem R. Cancellous chip bone-grafts. Lancet 1944; 2:746-768.167. Knight MP, Wood GO. Surgical obliteration of bone cavities fol-
lowing traumatic osteomyelitis. J Bone Joint Surg 1945; 27:547-556.
168. Robertson JM, Barron JN. A method of treatment of chronic in-fective osteitis. J Bone Joint Surg 1946; 28:19-28.
169. Higgs SL. The use of cancellous chips in bone grafting. J BoneJoint Surg 1946; 28:15-18.
170. Hogmman KE. Treatment ofinfected bone defects with cancellousbone-chip grafts. Acta Chir Scand 1949; 98:576-590.
171. Coleman HM, Bateman JE, Dale GM, et al. Cancellous bone graftsfor infected bone defmcts. Surg Gynekol Obstet 1946; 83:392-398.
172. Bickel WH, Bateman JG, Johnson WE. Treatment of chronic he-matogenous osteomyelitis by means of saucerization and bonegrafting. Surg Gynecol Obstet 1953; 96:265-274.
173. Hazlett JW. The use of cancellous bone grafts in the treatment ofsubacute and chronic osteomyelitis. J Bone Joint Surg 1954; 36B:584-590.
174. Winter FE. The surgical treatment of pyogenic osteomyelitis. ClinOrthop 1967; 51:139-149.
175. DeOliveira JC. Bone grafts and chronic osteomyelitis. J Bone JointSurg 1971; 53B:672-683.
176. Sudmann E. Treatment of chronic osteomyelitis by free grafts ofautologous bone tissue. Acta Orthop Scand 1979; 50:145-150.
177. Rhinelander FW. Minimal internal fixation of tibial fractures. ClinOrthop 1975; 107:188-220.
178. Papineau LJ. L'excision-greffe avec fermeture retardee delibereedans l'osteomyelite chronique. Nouv Presse Med 1973; 2:2753-2755.
179. Papineau LJ, Alageme A, Dalcourt JP, et al. Osteomyelite chro-nique: excision et greffe de spongieux a l'air libre apres mises aplat extensives. Int Orthop 1979; 3:165-176.
180. Lerat JL. L'operation de papineau dans le traitement des pertes desubstance ossense infectees du membre inferieur. A propos de40 observations. Lyon Chirurgical 1981; 77:155-158.
181. Lortat-Jacob A, Lelong P, Benoit J, et al. Les gestes complementairesde I operation de Papineau. Rev Chir Orthop 1981; 67:115-120.
182. Piganiol G, Mosser JJ, Hezard P, et al. Chirurgie de 1 infectionosseuse. Lyon Chirurgical 1979; 75:115-117.
183. Roy-Camille R, Reignier B, Saillant G, et al. Technique et histoirenaturelle de d'intervention de Papineau: excasion-greffe de spon-gieux a l'aar libre. Rev Chir Orthop 1976; 62:337-345.
184. Canbanela ME. Open cancellous bone grafting. Orthop Clin NorthAm 1984; 15(3):427-440.
185. Bigham EL, Hart GB. Hyperbaric oxygen treatment of refractoryosteomyelitis. Postgrad Med 1977; 61(6):70-76.
186. Klemm K, Contzen H, Lennert KH. Gentamycin-PMMA-Kugelnbei Knochen-und Weichteilinfektionen-Ergebnisse aus derBerufsgenossenschaftlichen. Unfallklinik Frankfurt/Main AktuelProbl Chir Orthop 1979; 12:128-132.
187. Strauss MB. Chronic refractory osteomyelitis. Review and role ofhyperbaric oxygen. Hyperbaric Oxygen Rev 1980; 1:231-256.
188. Kohnlein HE. Changes in the prognosis of osteomyelitis in childrenas a result of antibiotic therapy. Deutch Med Wschr 1962; 87(49):2524-2527.
189. Ruttle PE, Kelly PJ, Arnold PG, et al. Chronic osteomyelitis treatedwith a muscle flap. Orthop Clin North Am 1984; 15(3):451-459.
190. Bosworth DM, Liebler WA, Nastasi A, Hamadea K. Resection ofthe tibial shaft for osteomyelitis in children. J Bone Joint Surg1966; 48A(7): 1328-1339.
DISCUSSION
DR. M. J. JURKIEWICZ (Atlanta, Georgia): Dr. May had 190 referencesin this article. Clearly he researched the literature. He neglected a sig-nificant paper, however, that was published in 1920 by Alan Kanavel inSurgery, Gynecology, and Obstetrics. It was read before the Chicago Sur-gical Society on the management of wounds with noncollapsing walls.Kanavel observed that dead space management in patients with suchwounds was enhanced by flap transposition, and he usually used muscle.He applied the principle with success in patients with osteomyelitis
of the femur and of the mandible, with chronic empyema, and withchronic draining sinus tracts of the frontal bone, pelvis, and lower ab-domen.
These data by Dr. May and his colleagues confirm the observationsof Kanavel, unaccountably lost and forgotten until the past decade.
So too do our data at Emory, compiled by George Cierny of the Or-thopedic Service and Foad Nahai on the Plastic Surgery service. Therewere 189 patients treated in this 5-year period, 91 by transposition ofmuscle and 98 by free flap transfers, similar to the data from the MGH.There was a 97% long-term relapse-free rate in this 5-year period. Therewere no free flap losses at all in this series.Our patients are evaluated for treatment options by taking into account
not only the extent of trauma, nonviable dead bone, and wound factorsall under the rubric of dead space management, but also by consideringhost factors.May I ask what factors you take into account in an attempt to answer
the often crucial question ofamputation versus attempt at limb salvage?
You rely on 6 weeks of IV systemic antibiotics based on recommen-dations ofyour infection disease consultants. Ifour patients are candidatesfor 6 weeks of antibiotics, Cierny incorporates this into the dead spacemanagement by appropriate antibiotic-impregnated beads. These beadsthen are removed in 6 weeks, preserving the cavity and thus facilitatingthe secondary bone grafting. About half of our patients are so treatedand the other half by primary grafting as part of the initial dead spacemanagement. I wonder if you would comment on this approach.
Finally I think you need to elaborate on the 7.3% rate of neuropraxiain harvesting the donor muscle in your series.
I believe the study has broad implications in chronic wound manage-ment, well beyond osteomyelitis of bone, in treatment of wounds withnoncollapsing walls from whatever cause and in whatever location. Con-sider Kanavel's principle in the use of a well-vascularized flap transferfor wound management.
DR. STEPHEN J. MATHES (San Francisco, California): This paper nicelydemonstrates the versatility of microvascular composite tissue trans-plantation for coverage of complex wounds, whether they be located inthe lower extremity or in other areas.Of interest in 1983 here in Boca Raton, I had the opportunity to
present a paper entitled "Coverage of the Infected Wound," which alsoincluded a review of the use of muscle flaps in a retrospective group ofpatients who presented with complex open infected wounds. My studyincluded 27 patients with chronic osteomyelitis involving the lower ex-tremity. Because all these patients are now well beyond 5 years since


![Drug Delivery Systems and Materials for Wound Healing ... · Wounds can be categorized into acute and chronic types [8]. Acute wounds are the outcome of traumatic or surgical events](https://img.pdfslide.us/doc/110x75/610c28f6b504c101f07ce5f5/drug-delivery-systems-and-materials-for-wound-healing-wounds-can-be-categorized.jpg)