Embed Size (px)
DESCRIPTION
Treatment of Biliary Cancers. Abby B. Siegel, MD, MS Columbia University Co-Chair, SWOG Hepatobiliary Committee NCI Task Force, Hepatobiliary Cancers. Biliary Anatomy. Adapted from De Groen et al, NEJM 1999 Oct 28;341(18):1368-78 . - PowerPoint PPT Presentation
Citation preview

Treatment of Biliary Cancers
Abby B. Siegel, MD, MS Columbia University
Co-Chair, SWOG Hepatobiliary CommitteeNCI Task Force, Hepatobiliary Cancers

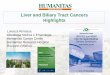
Biliary Anatomy
Adapted from De Groen et al, NEJM 1999 Oct 28;341(18):1368-78

Treatment arm Gem Gem + Cis
Number of patients n=206 n=204
Deaths n(%)141
(68.5) 122 (59.8)
Median survival (mo) 8.3 11.7Log rank p value 0.002Hazard ratio (95% CI) 0.70 (0.54, 0.89)
Gemcitabine With or Without Cisplatin in Advanced or Metastatic Biliary Cancer
(UK ABC-02 trial)

Gemcitabine/Cisplatin in Perspective
• A standard for advanced disease• Study results influenced by:
• GB vs IHCC vs EHCC• Included ampullary cancers• Patient selection:
– AST/ALT/Alk phos<3XULN– T Bili < 1.5 ULN– Accrual in select centers with experience– 27% locally advanced disease
• Caution about using Gem/cis as the only backbone in first line therapy
• What about other effective therapies: Gem/cape?

Single Agent Targeted Therapy
Target Agents in testing Study type # of patients Results
VEGF/Ras-Raf-MAPK
Sorafenib (SWOG 0514)
Phase II single agentNCT01093222
N=31 Median PFS 3 moMedian OS 9 mo
Sorafenib Phase II single agentNCT00238212
N=46 Median PFS 2.3 moMedian OS 4.4 mo
EGFR/Her-2 neu Trastuzumab Phase II single agent Closed d/t slow accrual1CR
Erlotinib Phase II single agentNCT00033462
N=42 Median TTP 2.6 moMedian OS 7.5 mo
Lapatinib Phase II single agent N=17 Median PFS 1.8 moMedian OS 5.2 mo
mTOR Sirolimus Phase II single arms for HCC and ICC
N=9 3/9 SDMedian survival 7 mo
MEK MEK-162 Phase I N=26 1CR
AZD6244 Phase II single agent N=28 1 CRMedian TTP 5.4 mo
AKT MK-2206 Phase II single agent(Second line)
On-going
Bengala C et al, British Journal of Cancer 2010,102: 68 – 72; Rizell et al, Int J Clin Oncol 2007 13:66-70 Philip, P. A. et al. J Clin Oncol 2006, 24:3069-3074, Ramantaan et al, Cancer Chemother Pharmacol 2009 64:777–783

Combination Targeted Agents
Targets Agents Study type Number of patients
Results
VEGF/EGFR Bevacizumaband Erlotinib
Phase II(Ph II consortium)
34 pts (interim report)
RR 17%Median TTP 8 months
Bevacizumab and Erlotinib
Phase II (Wisconsin)NCT00356889
53 RR 12%Median TTP 4.4OS 9.9 months
Bevacizumab and Erlotinib
Phase II (Denmark)NCT00350753
On-going
VEGF/EGFRRas/Raf
Sorafenib and Erlotinib
Phase II(SWOG0941)NCT01093222
32 RR 6% (unconf)PFS 2 monthsOS 6 months

Cytotoxic Chemotherapy with Targeted AgentsCombination Targeted
agent(s)Study type Number Results
Gemcitabine, oxaliplatin
Cetuximab Rand Phase II 150 RR 29%Median PFS 6 moMedian OS 12.4 mo
Gemcitabine, oxaliplatin
Erlotinib Phase III 268 RR 30%Median PFS 5.8 moMedian OS 9.5 mo
Gemcitabine, oxaliplatin
Bevacizumab Phase II 35 RR 40%PFS 8.8 moOS 11.6 mo
Gemcitabine, oxaliplatin, capecitabine
Panitumumab Phase IINCT00779454
On-going
Gemcitabine, oxaliplatin
Sorafenib Phase IINCT00955721
On-going
Gemcitabine, cisplatin
Sorafenib Phase II (MSK)NCT00919061
On-going
Gemcitabine, capecitabine
Bevacizumab Phase IINCT01007552
On-going
Gemcitabine Vandetanib (VEGFR/EGFR)
Randomized Phase IINCT00753675
On-going

Adjuvant Therapy for Biliary Cancers
• No clear prospective randomized data
• Best evidence so far is a meta-analysis
• 6712 patients, non significant improvement in OS for any adjuvant therapy (HR 0.74, p=0.06)

Adjuvant Therapy for Biliary Cancer:
Horgan A M et al. JCO 2012;30:1934-1940

Adjuvant Therapy for Biliary Cancers
• No large randomized trials yet, and no clear guidelines
• Metaanalysis suggests possible benefit of chemotherapy for all, particularly for node (+) and margin positive disease
• Radiation is often added in margin (+) disease
I usually give 6 months gem or gem/cis for margin (-), consider XRT + chemo for margin (+) disease; consider re-resection also
Horgan et al. JCO 2012;30:1934-1940

Adjuvant Therapy: SWOG 0809• Eligibility
– Gallbladder cancer or EHCC– At least one of the following:
• T2-T4• N1• Positive margins
Gemcitabine 1000 mg/m2 IV over 30 min D1 and D8
+ Capecitabine 750 mg/m2 PO BID x 14 days
X
4 cycles
Concurrent EBRT withCapecitabine 665 mg/m2 BID
x 7 days
For 6 weeks
4500 cGy (5 days a week, 180 cGy daily) with 900 cGy boost

Adjuvant Therapy in Biliary Cancers: Current Landscape
• BILCAP (UK): Phase 3: capecitabine versus observation in GB, IHCC, EHCC (n=360)
• French phase 3 study: gemcitabine and oxaliplatin versus observation in GB, IHCC, EHCC (n=190)
• ACTICCA-01: Phase 3: adjuvant gemcitabine and cisplatin versus BSC or capecitabine (depends on BILCAP)

Potential New Targets in Cholangiocarcinoma
• MEK
• IDH1/2
• FGFR

MEK Inhibition in Cancer TherapyRAS-RAF-MEK pathway
implicated in many tumors
• B-Raf mutations:
0-22% Bile duct tumors
• K-Ras mutations 3-54% Bile duct tumors
H-Ras K-Ras N-Ras
A-Raf B-Raf C-Raf
MEK1&2
ERK1&2
Receptor Tyrosine Kinase
Mutated and activatedin multiple cancers
Activation of Transcription/Proliferation

MEK Inhibitors in Biliary CancerTreatment Target No. of
Patients RR (%) PFS
(months)OS (months)
Toxicity Profile ( grade 3 and 4)
AZD6244 (first and second line)
MEK1/2
28 12 1 CR
5.4 9.8 Fatigue (8%), diarrhea ( 16%), rash, cellulitis
No ocular toxicities reported
MEK162 (ARRY-438162)
(first and second line)
MEK 1/2
26 eval 8
1 CR
2.6 N/A Anasarca, hypokalemia, hyponatremia, upper/lower gastrointestinal hemorrhage and mucositis (1 pt each)
Retinopathy was the most frequently reported event (6 pts)
Bekaii-Saab et al. JCO 2011 29:2357-63, Finn et al, GI ASCO 2012

Mek Inhibition Second Line: Trametinib(SWOG 1310)
Patients with refractory advanced biliary cancer
who have failed one prior line of treatment
Randomize
5-FU or capecitabinea
(N = 40)
Single Agent Trametinib
(2mg QD) (N=40)

IDH PathwayYen et al, Oncologist 2012 17:5-8
Yen et al, Oncologist 2012 17:5-8

IDH Mutations Seen in CholangiocarcinomasBorger et al, Oncologist, 2010 17:72-79
Borger et al, Oncologist, 2010 17:72-79

IDH Inhibitors• Isocitrate dehydrogenase mutations lead to
production of 2-hydroxyglutamate
• 2HG as potential non-invasive biomarker of response– Plasma– MRS
• Inhibitors being actively developed

FGFR2 Fusions Define a Unique Molecular Subtype of Cholangiocarcinoma
Wu Y et al. Cancer Discovery 2013;3:636-647, Arai et al, Hepatology 2013, EPUB ahead of print

Optimizing the Evaluation of Targeted Agents in Cholangiocarcinoma
• Choosing the “relevant” target(s) or combination of targets
• Having appropriate preclinical models• Stratifying by site if target differs based on
location• Enriching clinical trial population for target