Embed Size (px)
Citation preview

REVIEW
Treatment of Atopic Dermatitis with Biologic Drugs
Gabriella Fabbrocini . Maddalena Napolitano . Matteo Megna .
Nicola Balato . Cataldo Patruno
Received: July 19, 2018 / Published online: September 4, 2018� The Author(s) 2018
ABSTRACT
Atopic dermatitis (AD) is a chronic, pruritic,inflammatory skin disease which predominatelyaffects children and usually clears up duringinfancy or childhood. However, AD may persistwith a chronic relapsing course until adulthoodor develop at a later age. AD treatment can oftenbe complicated. Treating moderate-to-severeAD can be challenging: only a few therapeuticoptions are available, with cyclosporine beingthe only approved and labeled systemic drug. Inthe last few years, advances in the knowledge ofAD pathogenesis have been made that canprovide the basis for developing new topicaland systemic drugs. Among them, biologicdrugs targeting specific cytokines involved inthe development of the disease will probablyrevolutionize AD therapy. Currently, dupilu-mab, a monoclonal antibody that binds to the
shared alpha chain subunit of the receptors forIL-4 and IL-13, is the only biologic drug licensedfor the treatment of AD in adults. However,other biologic drugs that selectively target somekey cytokines in AD pathogenesis (IL-13, IL-31,and IL-22) are also being studied. In this review,we discuss all of the biologic drugs that havebeen studied for AD treatment.
Keywords: Atopic dermatitis; Biologic drug;Biologics; Therapy; Treatment
INTRODUCTION
Atopic dermatitis (AD) is the most commoninflammatory skin disease of childhood, affect-ing about 20% of children [1]. AD usuallyresolves before adolescence. However, it some-times persists in adulthood (persistent AD), andin some cases the disease starts in adulthood(adult-onset AD) [2]. It is reported that theprevalence of childhood AD is steadily increas-ing, especially in industrialized countries [3]. Inthe same way, it is likely that the frequency ofthe adult form has also been increasing inrecent years, as even reported for elderlypatients [4]. Current prevalence data regardingadult AD are very variable, with values rangingfrom 0.3 to 14.3%, even though most authorsagree that AD affects 1–3% of adults [5]. AD hasa chronic relapsing course and significantly
Enhanced Digital Features To view enhanced digitalfeatures for this article go to https://doi.org/10.6084/m9.figshare.6990209.
G. Fabbrocini � M. Megna � N. Balato �C. Patruno (&)Department of Dermatology, University of NaplesFederico II, Naples, Italye-mail: [email protected]
M. NapolitanoDepartment of Medicine and Health Science‘‘Vincenzo Tiberio’’, University of Molise,Campobasso, Italy
Dermatol Ther (Heidelb) (2018) 8:527–538
https://doi.org/10.1007/s13555-018-0258-x

affects the quality of life of patients, especiallyadults with severe and long-lasting AD [6]. Thediagnosis of adult AD is usually clinical, sincetraditional diagnostic criteria used for childrenare not always applicable to adults [5]. Studiesare now underway that aim to better define theclinical characteristics of the disease [7, 8]. Inmild cases, topical treatment includes corticos-teroids and calcineurin inhibitors in addition toemollient agents, which are the cornerstone oftreatment in all cases of AD [1]. Adjunctivesystemic treatment is needed in moderate-to-severe cases [9]. Phototherapy, cyclosporine A(CsA), methotrexate, and azathioprine are themain immunosuppressors used in AD treat-ment, while corticosteroids are used only foracute exacerbations [1]. Currently, cyclosporineis the only labeled medicament available for thetreatment of AD. Due to the chronicity of thecondition, long-term immunosuppressivetreatment is often required. Subsequently, con-tinuous follow-up is needed, as all of theabovementioned drugs may have importantside effects [9]. Moreover, these therapies showdifferent efficacies [9]. In recent years, severalstudies have elucidated the pathogenesis of thedisease, especially as regards the roles of somecytokines [10]. This has led to the introductionof new drugs targeting individual cells or amediator of the inflammatory response [1, 9].Among these new drugs, biologic agents areplaying a leading role. Currently, the mono-clonal antibody dupilumab is the only biologicdrug licensed for the treatment of AD in adults[1, 7]. Dupilumab blocks interleukin (IL)-4 andIL-13, two cytokines that play a key role in thedevelopment of type 2 helper (Th2) lympho-cyte-mediated skin inflammation in AD [11].Other biologic medicaments—drugs that selec-tively inhibit some cytokines (namely IL-13, IL-31, and IL-22) that play prominent roles in thepathogenesis of DA—are also under investiga-tion [1].
This review summarizes currently availablebiologic therapies for adult AD based on ananalysis of the literature in this field, andhighlights possible future scenarios for this kindof treatment.
METHODS
For the current review, relevant literature pub-lished in English was searched for. The studieswe selected concerned systemic biologic ther-apy of adult atopic dermatitis. We selectedcontrolled phase II and III trials as well asreviews, guidelines, and consensus. Researchwas carried out by searching the followingdatabases through to June 30, 2018: PubMed,Embase, The Cochrane Library, Google Scholar,EBSCO, and clinicaltrials.gov. The followingkeywords were used: ‘‘atopic dermatitis,’’ ‘‘atopiceczema,’’ ‘‘adult atopic dermatitis,’’ ‘‘adult atopiceczema,’’ ‘‘systemic treatment,’’ ‘‘systemic ther-apy,’’ ‘‘biologics,’’ ‘‘monoclonal antibody,’’ ‘‘IL-4monoclonal antibody,’’ ‘‘IL-13 monoclonalantibody,’’ ‘‘IL-31 monoclonal antibody,’’ and‘‘IL-22 monoclonal antibody.’’ This article isbased on previously conducted studies and doesnot involve any new study of human or animalsubjects performed by any of the authors.
BIOLOGIC DRUGS
The development of biological therapies hasprogressed rapidly in the last few years. Biologicdrugs are a class of pharmacological agents thatare engineered to target specific mediators ofinflammation. Recently, multiple clinical trialshave demonstrated the efficacy of targetedtherapy involving the blocking of cytokines ormediators that play a pivotal role in thepathogenesis of AD. Dupilumab is currently theonly biologic drug that has been approved byboth the US Food and Drug Administration(FDA) and the European Medicines Agency(EMA) for the treatment of adult patients withinadequately controlled moderate-to-severe AD[12]. Biological drugs appear to be promisingtreatments for adult AD patients because theyoffer more convenient dose regimens and allowless frequent laboratory monitoring than othersystemic therapies, as well as having fewer sideeffects [1]. Future studies are needed to fulfillunmet needs and achieve better standards ofcare for AD patients, to clarify the roles of otherbiologic drugs under investigation for AD
528 Dermatol Ther (Heidelb) (2018) 8:527–538

therapy, and to completely revolutionize adultAD treatment.
IL-4 and/or IL-13 Inhibitors
Dupilumab is a fully human monoclonal anti-body that binds to the shared alpha chain sub-unit of the receptors for IL-4 and IL-13 [13]. Thisresults in downregulation of receptor signalingdownstream of the JAK/STAT pathway, whichregulates the expression of many genesinvolved in the pathogenesis of AD [14]. InMarch 2017, dupilumab received its firstnational approval, from the USA, for its use inthe treatment of adult patients with moderate-to-severe AD whose disease is not adequatelycontrolled with topical therapies, or when thosetherapies are not advisable. In September 2017,it was also approved in Europe by EMA as asystemic first-line treatment for adults sufferingfrom AD [9]. Dupilumab is supplied in a single-dose pre-filled syringe and is administered bysubcutaneous injection into the thigh, abdo-men, or upper arm. The recommended dosage isa loading dose of 600 mg (two 300-mg injec-tions at different sites) followed by 300 mgevery other week, with rotation of the injectionsite. Dupilumab can be used with or withoutconcomitant topical corticosteroids (TCS) [15].It has also showed efficacy in patients withpersistent asthma and elevated eosinophils,where it improved lung function, reducedexacerbations, and decreased Th2 biomarkers[16]. Randomized, double-blind, placebo-con-trolled trials involving adults who had moder-ate-to-severe AD were performed to check theapplicability of dupilumab in the treatment ofadults with moderate-to-severe AD. The firsttwo clinical trials, SOLO 1 (NCT02277743) andSOLO 2 (NCT02277769), investigated the safetyand efficacy of the dupilumab dosage regimencompared with placebo [17]. Patients were ran-domly assigned in a 1:1:1 ratio to receive weekly(qw) subcutaneous injections of dupilumab(300 mg) or placebo or the same dose of dupi-lumab every other week (q2w) alternating withplacebo for 16 weeks. Significantly, more of thepatients receiving dupilumab showed animprovement of at least 75% in the Eczema Area
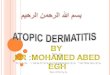
and Severity Index (EASI) score compared to theplacebo group. The percentages of the patientswho reached EASI-50 and EASI-90 as well as theimprovement in the Scoring Atopic Dermatitis(SCORAD) and the decrease in the affected bodysurface area were all significantly higher in thedupilumab groups than in the placebo group(Table 1). A further phase III trial, LIBERTY ADCHRONOS, aimed to analyze the long-termmanagement of moderate-to-severe AD withdupilumab and concomitant topical corticos-teroids [18] (Table 1). At week 52, more of thepatients who received dupilumab plus topicalcorticosteroids achieved the co-primary end-points of IGA 0/1 and EASI-75 compared to theother two groups (Table 1). The efficacy ofdupilumab has been demonstrated in adultpatients with a history of inadequate responseto/intolerance of CsA [19]. In the LIBERTY ADCAFE trial, 390 patients with an inadequateresponse to/intolerance of CsA or for whom CsAtreatment was medically inadvisable werescreened [19]. The proportion of the patientsachieving EASI-75 at week 16 was significantlyhigher in the dupilumab qw ? TCS and q2w ?
TCS groups compared to placebo ? TCS. In allof the clinical studies performed in this field todate, dupilumab has shown a favorable safetyprofile with no dose-limiting toxicity and fewadverse effects. The most common adverseevents (AEs) associated with dupilumab areinjection-site reactions, which mainly consist oftransient erythema or edema. Conjunctivitisseems the only specific side effect, and this canbe treated successfully with fluorometholone0.1% eye drops or tacrolimus 0.03% eye oint-ment [20]. The reason why dupilumab causesconjunctivitis is not fully understood, and iscurrently being evaluated in ophthalmologicalsubtrials. It was hypothesized that blockage ofIL-4 and IL-13 would increase the activities ofspecific ligands involved in atopic keratocon-junctivitis, such as the OX40 ligand [21]. Gen-erally, the severity of dupilumab-inducedconjunctivitis in the majority ([ 90%) ofpatients is only mild or moderate, and itresolves easily. Actually, there is only one caseof bilateral conjunctivitis with consequentcicatricial ectropion associated with dupilumabtherapy for AD in the literature [22].
Dermatol Ther (Heidelb) (2018) 8:527–538 529

Table1
The
mainfeatures
ofclinicaltrialsregardingbiologicdrugsformoderate-to-severeatopicderm
atitis
Drug[ref.]
Trial
phaseand
no.of
patients
enrolled
Dosageanddu
ration
Results
Dupilumab
[17]
III
N=671
(1)Aninitialdose
of600mgdupilumab
(two300mg
injections)on
day1,
followed
by300mgonce
every
2weeks
(q2w
);(2)an
initialdose
of600mg
dupilumab
onday1followed
by300mgonce
weekly
(qw);or
(3)matchingplacebo
Duration:
16weeks
The
percentage
ofpatientswho
hadascoreof
0or
1(clear
or
almostclear)
intheInvestigator
GlobalAssessm
ent(IGA)at
16weeks
was
38%
inthegroupthat
received
dupilumab
every
otherweek,37%in
thedupilumab
weeklygroup,and10%in
the
placebogroup(P
\0.0001)
Areductionof
75%or
morein
EASI
scorewasmorecommon
for
the300-mgdupilumab
group(q2w
andqw
)withrespectto
placebo(51.3%
and52.5%
vs14.7,P
\0.0001)
MeanSC
ORAD
percentageswere57.7
±2.7in
thedupilumab
w2q
arm
and29.0
±3.21
forplacebo(P
\0.001)
Changefrom
baselin
epruritus
NRSscoreat
week16:-
51.0,
-48.9,and
-26.1
intheq2w,q
w,and
placebogroups,
respectively
Dupilumab
[17]
III
N=701
(1)Aninitialdose
of600mgdupilumab
(two300mg
injections)on
day1,
followed
by300mgonce
every
2weeks
(q2w
);(2)an
initialdose
of600mg
dupilumab
onday1,followed
by300mgonce
weekly
(qw);or
(3)matchingplacebo
Duration:
16weeks
The
percentage
ofpatientsthat
hadascoreof
0or
1(clear
or
almostclear)
intheInvestigator
GlobalAssessm
ent(IGA)at
16weeks
was
36.1%
inthegroupthat
received
dupilumab
every
otherweek,36.4%
inthedupilumab
weeklygroup,and8.5%
in
theplacebogroup(P
\0.0001)
Areductionof
75%or
morein
EASI
scorewasmorecommon
for
the300-mgdupilumab
group(q2w
andqw
)withrespectto
placebo(44.2%
and48.1%
vs11.9,P
\0.0001)
MeanSC
ORAD
percentageswere51.1
±2.02
inthedupilumab
w2q
arm
and19.7
±2.52
forplacebo(p\
0.001)
Changefrom
baselin
epruritus
NRSscoreat
week16:-
44.3,
-48.3,and
-15.4
intheq2w,q
w,and
placebogroups,
respectively
530 Dermatol Ther (Heidelb) (2018) 8:527–538
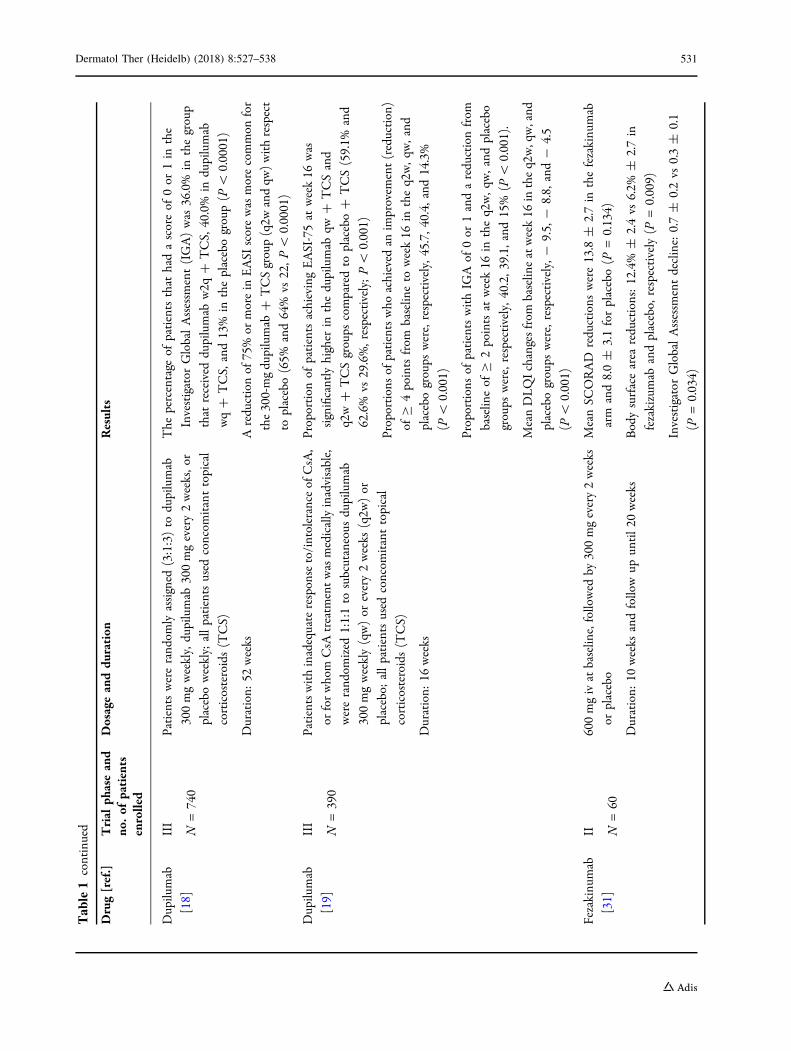
Table1
continued
Drug[ref.]
Trial
phaseand
no.of
patients
enrolled
Dosageanddu
ration
Results
Dupilumab
[18]
III
N=740
Patientswererand
omlyassigned
(3:1:3)to
dupilumab
300mgweekly,dupilumab
300mgevery2weeks,o
r
placeboweekly;allpatientsused
concom
itanttopical
corticosteroids(TCS)
Duration:
52weeks
The
percentage
ofpatientsthat
hadascoreof
0or
1in
the
Investigator
GlobalAssessm
ent(IGA)was
36.0%
inthegroup
that
received
dupilumab
w2q
?TCS,
40.0%
indupilumab
wq?
TCS,
and13%
intheplacebogroup(P
\0.0001)
Areductionof
75%or
morein
EASI
scorewasmorecommon
for
the300-mgdupilumab
?TCSgroup(q2w
andqw
)withrespect
toplacebo(65%
and64%
vs22,P
\0.0001)
Dupilumab
[19]
III
N=390
Patientswithinadequateresponseto/intolerance
ofCsA,
orforwhom
CsA
treatm
entwasmedicallyinadvisable,
wererand
omized
1:1:1to
subcutaneous
dupilumab
300mgweekly(qw)or
every2weeks
(q2w
)or
placebo;
allpatientsused
concom
itanttopical
corticosteroids(TCS)
Duration:
16weeks
Proportion
ofpatientsachievingEASI-75at
week16
was
significantlyhigher
inthedupilumab
qw?
TCSand
q2w?
TCSgroups
comparedto
placebo?
TCS(59.1%
and
62.6%
vs29.6%,respectively;P\
0.001)
Proportionsof
patientswho
achieved
anim
provem
ent(reduction)
ofC
4pointsfrom
baselin
eto
week16
intheq2w,q
w,and
placebogroups
were,respectively,4
5.7,
40.4,and
14.3%
(P\
0.001)
Proportionsof
patientswithIG
Aof
0or
1andareductionfrom
baselin
eof
C2pointsat
week16
intheq2w,q
w,and
placebo
groups
were,respectively,4
0.2,
39.1,and
15%
(P\
0.001).
MeanDLQIchangesfrom
baselin
eatweek16
intheq2w,qw,and
placebogroups
were,respectively,-
9.5,
-8.8,
and-
4.5
(P\
0.001)
Fezakinu
mab
[31]
II N=60
600mgivat
baselin
e,followed
by300mgevery2weeks
orplacebo
Duration:
10weeks
andfollowup
until20
weeks
MeanSC
ORAD
reductions
were13.8
±2.7in
thefezakinu
mab
arm
and8.0±
3.1forplacebo(P
=0.134)
Bodysurfacearea
reductions:12.4%
±2.4vs
6.2%
±2.7in
fezakizumab
andplacebo,
respectively(P
=0.009)
Investigator
GlobalAssessm
entdecline:0.7±
0.2vs
0.3±
0.1
(P=0.034)
Dermatol Ther (Heidelb) (2018) 8:527–538 531

Table1
continued
Drug[ref.]
Trial
phaseand
no.of
patients
enrolled
Dosageanddu
ration
Results
Lebrikizumab
[29]
II N=209
125mgsingledose,2
50mgsingledose,1
25mgevery
4weeks
orplacebo
Duration:
12weeks
EASI-50was
reachedin
82.4%
ofpatientswithlebrikizum
ab
125mgevery4weeks
and62.3%
intheplacebogroup
(P=0.026)
Patientsreceivingasingledose
oflebrikizum
abshow
edno
statistically
significant
improvem
entin
EASI-50comparedwith
placebo
Nem
olizum
ab
[35]
II N=264
0.1,
0.5,
or2.0mg/kg
(subcutaneous)or
placeboevery
4weeks
oran
exploratorydose
of2.0mg/kg
every
8weeks
Duration:
12weeks
Changesin
thepruritus
visual-analoguescalewere-
43.7%in
the
0.1mggroup,
-59.8%
inthe0.5mggroup,
and-
63.1%
in
the2.0mggroupversus
-20.9%
intheplacebogroup
(P\
0.01)
EASI
reductions:-
23.0,-
42.3,and
-40.9%,respectively,in
thenemolizum
abgroups
versus
-26.6%
intheplacebogroup
Changes
inbody-surface
area
affected
byatopicderm
atitiswere
-7.5,-
20.0,and
-19.4%withnemolizum
abversus
-15.7%
withplacebo
Nem
olizum
ab
[36]
II N=191
0.1,
0.5,
or2.0mg/kg
scevery4or
8weeks
Duration:
52weeks
Changefrom
baselin
ein
pruritus
visualanalog
scalescoreat
week
64:-
73.0,-
89.6,-
74.7,and
-79.1in
the0.1,0.5,and2.0-
mg/kg
q4wand2.0-mg/kg
q8wgroups,respectively
EASI
reductions:-
68.5,-
75.8,-
78.9,and
-69.3in
the0.1-,
0.5-,and
2.0-mg/kg
q4wand2.0-mg/kg
q8wgroups,respectively
532 Dermatol Ther (Heidelb) (2018) 8:527–538
Table1
continued
Drug[ref.]
Trial
phaseand
no.of
patients
enrolled
Dosageanddu
ration
Results
Tralokinu
mab
[25]
II N=204
45,1
50,o
r300mgof
subcutaneous
tralokinum
abor
placeboevery2weeks
Duration:
12weeks
300mgof
tralokinum
absignificantlyim
proved
thechange
from
baselin
eEASI
scoreversus
placebo(adjustedmeandifference,
-4.94;95%
CI-
8.76
to-
1.13;P=0.01)
Agreaterpercentage
ofthesubjectstreatedwith300mgachieved
anInvestigator
GlobalAssessm
entresponse
withrespectto
placebo(26.7%
vs11.8%,P
=0.06)
Areductionof
50%or
morein
EASI
scorewasmorecommon
for
the300-mgtralokinum
abgroupwithrespectto
placebo(73.4%
vs51.9%,P
=0.03)
The
percentage
ofparticipantswithareductionof
75%or
morein
EASI
scorewas
higher
inthe300mgtralokinum
abgroup
(42.5%
)than
intheplacebogroup(15.5%
,P=0.003)
Dermatol Ther (Heidelb) (2018) 8:527–538 533

As with all therapeutic proteins, dupilumabhas the potential for immunogenicity. Anti-drug antibodies were developed by approxi-mately 7% of patients with AD who receiveddupilumab 300 mg every 2 weeks for 16 weeksin SOLO 1 and 2 [23]. Approximately 30% ofpatients with anti-drug antibodies (2% overall)had neutralizing antibodies. Similarly, approxi-mately 7% of the patients who received dupi-lumab 300 mg once every 2 weeks (plus TCS) for52 weeks in CHRONOS developed antibodies todupilumab, with approximately 14% of thosepatients (1% overall) having neutralizingantibodies.
Several ongoing studies involving both chil-dren and adolescents will show if these sub-groups of the AD population experience equallypositive effects, expanding the treatment indi-cation for dupilumab even further [24].
Tralokinumab is a human monoclonal anti-body (mAb) that specifically neutralizes IL-13[25]. IL-13 is a pleiotropic Th2 cytokine that hasbeen implicated in the pathogenesis of AD, as itimpairs skin barrier function by downregulatingfilaggrin [26, 27]. IL-13 is increased in bothlesional and nonlesional skin of AD subjects,and correlates with disease severity [28]. A ran-domized, placebo-controlled, double-blind,clinical phase II study involving 204 adultpatients with moderate-to-severe AD was per-formed [25]. At week 12, a dose of 300 mg oftralokinumab every 2 weeks resulted in a sig-nificant improvement in AD compared withplacebo (Table 1). Indeed, the drug significantlyimproved the EASI change from baseline versusplacebo (P = 0.01; Table 1). In particular, agreater percentage of the 300 mg tralokinumab-treated participants achieved EASI-50 versusplacebo at week 12 (73.4% vs 51.9%, P = 0.03)as well as EASI-75 (42.5% vs 15.5%, P = 0.003),although concomitant TCS use may constitute aconfounding factor that could explain the highplacebo efficacy. Interestingly, patients withhigher concentrations of biomarkers ofincreased IL-13 levels showed a better responseto tralokinumab. The most frequent AEs in allgroups were upper respiratory tract infections,nasopharyngitis, and headache [25]. All of thesedata indicated that tralokinumab treatment wasassociated with early improvements in AD
symptoms and an acceptable safety and tolera-bility profile.
Lebrikizumab is a humanized monoclonalantibody that specifically targets IL-13 [29]. Aphase II randomized, double-blind, prospective,placebo-controlled, multicenter study has beenperformed in adult subjects with moderate-to-severe AD [30]. In total, 209 patients were ran-domized (1:1:1:1) to lebrikizumab 125 mg sin-gle dose, lebrikizumab 250 mg single dose,lebrikizumab 125 mg every 4 weeks for12 weeks, or placebo every 4 weeks for 12 weeks.At week 12, EASI-50 was more commonlyachieved in patients receiving lebrikizumab125 mg every 4 weeks than in placebo patientsevery 4 weeks (82.4% vs 62.3%, P = 0.026). Thehigh placebo performance may due to thebackground of daily TCS application (Table 1).Lebrikizumab was well tolerated; adverse eventswere similar between groups (66.7% all lebrik-izumab vs 66.0% placebo) and were mostly mildor moderate; no AE dose–response relationshipswere found for the drug. In that study, theefficacy of lebrikizumab 125 mg every 4 weeksled to a significant improvement in patientswith moderate-to-severe AD.
IL-22 Inhibitor
IL-22 was found to be increased in both acuteand chronic AD lesions, correlating with ADseverity [28]. It is produced primarily by Th22cells and is able to impair epithelial barrierfunction through its effect on keratinocytes[31].
Fezakinumab is a fully human monoclonalantibody directed against IL-22. A recent ran-domized, double-blind, placebo-controlled trialwith intravenous fezakinumab monotherapyevery 2 weeks for 10 weeks and follow-upassessments until 20 weeks has been completed[32]. Sixty-seven adult AD patients were asses-sed for eligibility, and 60 patients were ran-domized 2:1 to fezakinumab (n = 40) or placebo(n = 20). Results showed that the SCORADimprovement was significantly greater withfezakinumab versus placebo in patients withsevere AD at 12 weeks (36.4% vs 22.3%,P\ 0.05) and 20 weeks (46.2% vs 22.6%,
534 Dermatol Ther (Heidelb) (2018) 8:527–538

P\ 0.01), while patients with moderate ADseemed to be less responsive to treatment(Table 1) [31]. AEs occurred with similar fre-quencies in the fezakinumab and placebogroups [32]. Taken together, these data showedthat fezakinumab was well tolerated, with sus-tained clinical improvements after the last drugdosing.
IL-31 Receptor Inhibitor
It is already known that the skin expression ofIL-31 and IL-31R is increased in patients withAD [33]. Moreover, AD subjects also showhigher serum levels of IL-31 as well as IL-31-producing lymphocytes [34]. In addition, bothserum and skin IL-31 levels have been shown tocorrelate with AD severity [33, 34], indicatingan important role for IL-31 in AD pathogenesisapart from itch pathophysiology [35].
Nemolizumab is a monoclonal antibodydirected against IL-31 receptor A [33]. A phaseII, randomized, double-blind, placebo-con-trolled, 12-week trial involving 264 adultpatients with moderate-to-severe AD has beenrecently completed [36]. Patients received sub-cutaneous nemolizumab (at doses of 0.1, 0.5, or2.0 mg/kg of body weight) or placebo every4 weeks. Significant reductions in pruritus wereseen from baseline to week 12 in all armsreceiving nemolizumab every 4 weeks; theresult was statistically significant with respect toplacebo in all drug groups (Table 1). EASI scorechanges were significantly higher for 0.5 and2 mg nemolizumab with respect to placebo(Table 1). AD exacerbation, nasopharyngitis,upper respiratory tract infection, peripheraledema, and increased creatine kinase levelswere the most common AEs registered. In par-ticular, exacerbation of AD and peripheraledema were more common in the nemolizumabgroups than in the placebo group.
More recently, the long-term efficacy andsafety of nemolizumab injected subcutaneouslyevery 4 weeks (q4w) or 8 weeks (q8w) wereevaluated in a phase II, 52-week, double-blindextension trial [37]. Patients (n = 191) contin-ued the previous nemolizumab dose (0.1, 0.5, or2.0 mg/kg q4w or 2.0 mg/kg q8w) [36]. An
improvement from baseline in the pruritusvisual analog scale score was maintained/in-creased from weeks 12 to 64, with the greatestimprovement seen for the 0.5-mg/kg q4w group(Table 1). The EASI improvement was alsomaintained/increased to week 64, with thehighest results observed with a dosage of2.0 mg/kg q4w (Table 1), showing that nemoli-zumab for up to 64 weeks was efficacious andwell tolerated overall in patients with moderate-to-severe AD inadequately controlled by topicaltherapy. The most common AEs in patientstreated over the long term with nemolizumab(C 5% of patients were randomized to nemoli-zumab throughout the study period) werenasopharyngitis (27%), exacerbation of AD(25%), increased blood creatine phosphokinase(11%), upper respiratory tract infection (9%),headache (8%), peripheral edema (6%), andimpetigo (6%).
CONCLUSION
The frequency of AD is increasing all over theworld, especially in industrialized countries andurbanized areas. The frequency of this disease inadults also seems to be increasing, although it isprobably underdiagnosed. Due to its chronicityand subjective symptoms, the disease greatlyimpacts on the quality of life of the patients.Currently, only few systemic immunosuppres-sive drugs are available for moderate-to-severeforms, and CsA is the only licensed drug for thetreatment. Moreover, the important side effectsof immune suppressors limit their use. There-fore, having more secure and effective medici-nes would be desirable. Over the last few years,increased knowledge about AD pathogenesishas made it possible to develop new therapeuticagents capable of blocking individual mediatorsof inflammation. Some monoclonal antibodiesagainst specific cytokines (IL-4, IL-13, IL-22, IL-31) have been developed. Data obtained fromthe trials regarding efficacy and safety areencouraging for most of the agents. Dupilumab(anti-IL-4/IL-13) is the only biologic agentapproved for AD in some countries. In conclu-sion, biologic therapies will probably markedlychange the natural history of AD. Indeed, they
Dermatol Ther (Heidelb) (2018) 8:527–538 535
will hopefully be able to increase the disease-free periods and decrease the number of exac-erbations, thus improving the quality of life ofAD patients.
ACKNOWLEDGEMENTS
Funding. No funding or sponsorship wasreceived for this study or the publication of thisarticle.
Authorship. All named authors meet theInternational Committee of Medical JournalEditors (ICMJE) criteria for authorship for thismanuscript, take responsibility for the integrityof the work as a whole, and have given finalapproval for the version to be published.
Disclosures. Cataldo Patruno is an investi-gator for AbbVie and Almirall, an advisoryboard member and speaker for Sanofi Genzyme,and a speaker for Novartis. Gabriella Fabbrocini,Maddalena Napolitano, Matteo Megna, andNicola Balato have nothing to disclose.
Compliance with Ethics Guidelines. Thisarticle is based on previously conducted studiesand does not involve any new study of humanor animal subjects performed by any of theauthors.
Open Access. This article is distributedunder the terms of the Creative CommonsAttribution-NonCommercial 4.0 InternationalLicense (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommer-cial use, distribution, and reproduction in anymedium, provided you give appropriate creditto the original author(s) and the source, providea link to the Creative Commons license, andindicate if changes were made.
REFERENCES
1. Megna M, Napolitano M, Patruno C, Villani A,Balato A, Monfrecola G, Ayala F, Balato N. Systemic
treatment of adult atopic dermatitis: a review.Dermatol Ther (Heidelb). 2017;7:1–23.
2. Napolitano M, Megna M, Patruno C, Gisondi P,Ayala F, Balato N. Adult atopic dermatitis: a review.G Ital Dermatol Venereol. 2016;151:403–11.
3. Dinulos JG, Trickett A, Crudele C. New science andtreatment paradigms for atopic dermatitis. CurrOpin Pediatr. 2018;30:161–8.
4. Katsarou A, Armenaka MC. Atopic dermatitis inolder patients: particular points. J Eur Acad Der-matol Venereol. 2011;25:12–8.
5. Silvestre Salvador JF, Romero-Perez D, Encabo-Duran B. Atopic dermatitis in adults: a diagnosticchallenge. J Investig Allergol Clin Immunol.2017;27:78–88.
6. Kim DH, Li K, Seo SJ, et al. Quality of life and dis-ease severity are correlated in patients with atopicdermatitis. J Korean Med Sci. 2012;27:1327–32.
7. Megna M, Patruno C, Balato A, Rongioletti F, Stin-geni L, Balato N. An Italian multicentre study onadult atopic dermatitis: persistent versus adult-on-set disease. Arch Dermatol Res. 2017;309:443–52.
8. Calzavara Pinton P, Cristaudo A, Foti C, et al.Diagnosis and management of moderate to severeadult atopic dermatitis: a consensus by the ItalianSociety of Dermatology and Venereology (SIDe-MaST), the Italian Association of Hospital Derma-tologists (ADOI), the Italian Society of Allergy,Asthma and Clinical Immunology (SIAAIC), andthe Italian Society of Allergological, Environmentaland Occupational Dermatology (SIDAPA). G ItalDermatol Venereol. 2018;153:133–45.
9. Wollenberg A, Barbarot S, Bieber T, et al. Consen-sus-based European guidelines for treatment ofatopic eczema (atopic dermatitis) in adults andchildren: part II. J Eur Acad Dermatol Venereol.2018;32:850–78.
10. Rerknimitr P, Otsuka A, Nakashima C, KabashimaK. The etiopathogenesis of atopic dermatitis: barrierdisruption, immunological deragement, and pruri-tus. Inflamm Regen. 2017;37:14.
11. Eshtiaghi P, Gooderham MJ. Dupilumab: an evi-dence-based review of its potential in the treatmentof atopic dermatitis. Core Evid. 2018;13:13–20.
12. Schmitt J. After the approval of dupilumab formoderate-to-severe atopic dermatitis: what is nexton the research agenda? Br J Dermatol.2018;178:992–3.
536 Dermatol Ther (Heidelb) (2018) 8:527–538

13. Seegraber M, Srour J, Walter A, Knop M,WollenbergA. Dupilumab for treatment of atopic dermatitis.Expert Rev Clin Pharmacol. 2018;11:467–74.
14. Bao L, Zhang H, Chan LS. The involvement of theJAK-STAT signaling pathway in chronic inflamma-tory skin disease atopic dermatitis. Jakstat.2013;2:e24137.
15. US FDA. Dupixent (dupilumab) injection, for sub-cutaneous use: US prescribing information. 2017.https://www.fda.gov. Accessed 2 May 2018.
16. Wenzel S, Ford L, Pearlman D, et al. Dupilumab inpersistent asthma with elevated eosinophil levels.N Engl J Med. 2013;368:2455–66.
17. Simpson EL, Bieber T, Guttman-Yassky E, et al. Twophase 3 trials of dupilumab versus placebo in atopicdermatitis. N Engl J Med. 2016;375:2335–48.
18. Blauvelt A, de Bruin-Weller M, Gooderham M, et al.Long-term management of moderate-to-severeatopic dermatitis with dupilumab and concomitanttopical corticosteroids (LIBERTY AD CHRONOS): a1-year, randomised, double-blinded, placebo-con-trolled, phase 3 trial. Lancet. 2017;389:2287–303.
19. de Bruin-Weller M, Thaci D, Smith CH, et al.Dupilumab with concomitant topical corticosteroidtreatment in adults with atopic dermatitis with aninadequate response or intolerance to ciclosporin Aor when this treatment is medically inadvisable: aplacebo-controlled, randomized phase III clinicaltrial (LIBERTY AD CAFE). Br J Dermatol.2018;178:1083–101.
20. Wollenberg A, Ariens L, Thurau S, van Luijk C,Seegraber M, de Bruin-Weller M. Conjunctivitisoccurring in atopic dermatitis patients treated withdupilumab—clinical characteristics and treatment.J Allergy Clin Immunol Pract. 2018;18:30089-8 (pii:S2213-2198).
21. Mennini M, Dahdah L, Fiocchi A. Two phase 3 trialsof dupilumab versus placebo in atopic dermatitis.N Engl J Med. 2017;376:1090.
22. Barnes AC, Blandford AD, Perry JD. Cicatricialectropion in a patient treated with dupilumab. Am JOphthalmol Case Rep. 2017;7:120–2.
23. Shirley M. Dupilumab: first global approval. Drugs.2017;77:1115–21.
24. Blakely K, Gooderham M, Papp K, Dupilumab A.Monoclonal antibody for atopic dermatitis: areview of current literature. Skin Therapy Lett.2016;21:1–5.
25. Wollenberg A, Howell MD, Guttman-Yassky E, Sil-verberg JI, Kell C, Ranade K, Moate R, van der
Merwe R. Treatment of atopic dermatitis withtralokinumab, an anti-IL-13 monoclonal antibody.J Allergy Clin Immunol. 2018;18:30850–9. https://doi.org/10.1016/j.jaci.2018.05.029 (pii: S0091-6749).
26. Hamann CR, Thyssen JP. Monoclonal antibodiesagainst interleukin 13 and interleukin 31RA indevelopment for atopic dermatitis. J Am Acad Der-matol. 2018;78:S37–42.
27. Kim BE, Leung DY, Boguniewicz M, et al. Loricrinand involucrin expression is down-regulated byTh2 cytokines through STAT-6. Clin Immunol.2008;126:332–7.
28. Ungar B, Garcet S, Gonzalez J, Dhingra N, da RosaJC, Shemer A, et al. An integrated model of atopicdermatitis biomarkers highlights the systemic nat-ure of the disease. J Invest Dermatol.2017;137:603–13.
29. Tazawa T, Sugiura H, Sugiura Y, Uehara M. Relativeimportance of IL-4 and IL-13 in lesional skin ofatopic dermatitis. Arch Dermatol Res.2004;295:459–64.
30. Simpson EL, Flohr C, Eichenfield LF, et al. Efficacyand safety of lebrikizumab (an anti-IL-13 mono-clonal antibody) in adults with moderate-to-severeatopic dermatitis inadequately controlled by topicalcorticosteroids: a randomized, placebo-controlledphase II trial (TREBLE). J Am Acad Dermatol.2018;78(863–871):e11.
31. Gittler JK, Shemer A, Suarez-Farinas M, et al. Pro-gressive activation of T(H)2/T(H)22 cytokines andselective epidermal proteins characterizes acute andchronic atopic dermatitis. J Allergy Clin Immunol.2012;130:1344–54.
32. Guttman-Yassky E, Brunner PM, Neumann AU,et al. Efficacy and safety of fezakinumab (an IL-22 monoclonal antibody) in adults with moderate-to-severe atopic dermatitis inadequately controlledby conventional treatments: a randomized, double-blind, phase 2a trial. J Am Acad Dermatol.2018;78:872–81.
33. Hamann CR, Thyssen JP. Monoclonal antibodiesagainst interleukin 13 and interleukin 31RA indevelopment for atopic dermatitis. J Am Acad Der-matol. 2018;78:S37–42.
34. Szegedi K, Kremer AE, Kezic S, et al. Increased fre-quencies of IL-31-producing T cells are found inchronic atopic dermatitis skin. Exp Dermatol.2012;21:431–6.
35. Sonkoly E, Muller A, Lauerma AI, et al. IL-31: a newlink between T cells and pruritus in atopic skin
Dermatol Ther (Heidelb) (2018) 8:527–538 537

inflammation. J Allergy Clin Immunol.2006;117:411–7.
36. Ruzicka T, Hanifin JM, Furue M, et al. Anti-Inter-leukin-31 receptor A antibody for atopic dermatitis.N Engl J Med. 2017;376:826–35.
37. Kabashima K, Furue M, Hanifin JM, Pulka G, Wol-lenberg A, Galus R, Etoh T, Mihara R, Nakano M,Ruzicka T. Nemolizumab in patients with moder-ate-to-severe atopic dermatitis: randomized, phaseII, long-term extension study. J Allergy ClinImmunol. 2018;10(18):30698-5 pii: S0091-6749.
538 Dermatol Ther (Heidelb) (2018) 8:527–538