Embed Size (px)
Citation preview

e
mpct
www.AJOG.org Reviews
OBSTETRICS
Treatment of abnormal vaginal flora in early pregnancywith clindamycin for the prevention of spontaneouspreterm birth: a systematic review and metaanalysisRonald F. Lamont, BSc, MB, ChB, MD, FRCOG; Chia-Ling Nhan-Chang, MD; Jack D. Sobel, MD;
Kimberly Workowski, MD; Agustin Conde-Agudelo, MD, MPH; Roberto Romero, MDnbo
ptal
rdp
c
Spontaneous preterm labor and deliv-ery is a syndrome caused by multi-
ple pathologic processes that activatethe common pathway of parturition.1,2
Mechanisms of disease involved in the“preterm labor syndrome” include in-fection/inflammation,3-14 vascular dis-ase,15-17 uterine overdistension,18-21
abnormal allograft reaction (eg, rejec-tion),22-24 an allergic-like phenome-non,25-28 a progesterone deficiency,29-32
and cervical disorders.33-36 The firstechanism of disease responsible for
reterm labor and delivery for which aausal link was well-established is infec-ion.3,8,11,13,37-39 Moreover, the mecha-
From the Perinatology Research Branch,NICHD, NIH, DHHS, Bethesda, MD, andDetroit, MI (Drs Lamont, Nhan-Chang,Conde-Agudelo, and Romero); theDepartments of Obstetrics and Gynecology(Drs Lamont and Nhan-Chang) andInfectious Diseases (Dr Sobel), Wayne StateUniversity/Hutzel Hospital, Detroit, MI; theDivision of Infectious Diseases, EmoryUniversity, Atlanta, GA (Dr Workowski);Division of STD Prevention, Centers forDisease Control and Prevention, Atlanta, GA(Dr Workowski).
Received Nov. 16, 2010; revised March 1,2011; accepted March 23, 2011.
Correspondence: Roberto Romero, MD,Perinatology Research Branch, NICHD, NIH,DHHS, Wayne State University/HutzelWomen’s Hospital, 3990 John R, Box 4,Detroit, MI 48201. [email protected].
Supported in part by the PerinatologyResearch Branch, Division of IntramuralResearch, Eunice Kennedy Shriver NationalInstitute of Child Health and HumanDevelopment, National Institutes of Health,Department of Health and Human Services.
0002-9378/$36.00Published by Mosby, Inc.
doi: 10.1016/j.ajog.2011.03.047isms responsible for this process haveeen identified and involve pattern rec-gnition receptors,40-44 chemokines,45-49
or inflammatory cytokines.50-53
A conventional view is that most casesof intrauterine infection responsible forpreterm labor and delivery result fromascending infection;3,8 therefore, multi-
le investigators have attempted to iden-ify the patient at risk for preterm labornd delivery by assessing the microbio-ogic state of the lower genital tract.54-61
Several cohort studies have attempted toestablish a relationship between a changein the lower genital tract flora and therisk of preterm delivery.62-72 Moreover,andomized clinical trials have been un-ertaken to test the effect of antibiotics inatients with bacterial vaginosis (BV),73-87
Trichomonas vaginalis,88 group B strep-tococci (GBS),89,90 Ureaplasma urealyti-um,91,92 and Chlamydia trachomatis.93
The initial expectation that assessing thelower genital tract for the presence of cer-tain microorganisms or changes in the mi-
The purpose of this study was to determinewomen with abnormal vaginal flora at �22birth and late miscarriage. We conducteddomized controlled trials of the early adminmal vaginal flora at �22 weeks of gestationincluded. Clindamycin that was administerewith a significantly reduced risk of pretermmiscarriage. There were no overall differenof gestation, low birthweight, very low birthunit, stillbirth, peripartum infection, and advwomen with abnormal vaginal flora reducesweeks of gestation and late miscarriage. Tcontrolled trials of clindamycin for the preunderstanding of the vaginal microbiome, mvaginosis will be needed to inform the desi
Key words: antibiotic, bacterial vaginosis,
crobial flora (ie, BV) followed by treat-
SEPTEMBER 2011 Am
ment has not met initial hopes. We believethat the disappointing results are not dueto any question about the importance ofinfection in the etiology of preterm laborand delivery (with intact or rupturedmembranes), but rather the limitations ofthe experimental design of the randomizedclinical trials implemented to test the ef-fects of antimicrobial agents.
A fundamental principle of randomizedclinical trials is that all patients included ina particular trial must potentially benefitfrom the intervention under study (in thiscase, antibiotics). Therefore, if the goal ofantibiotic administration is to reduce pre-term labor and delivery, this can only beaccomplished by preventing infection-in-duced preterm labor and delivery.94,95
Consequently, randomized clinical trialsdesigned to test hypotheses must identifypatients at risk for infection, and such risksmust be substantial in order for the trial tohave a reasonable expectation of success.
Intraamniotic infection/inflammationcan be readily identified by analysis of
ether the administration of clindamycin toks of gestation reduces the risk of pretermstematic review and metaanalysis of ran-
ation of clindamycin to women with abnor-ve trials that comprised 2346 women weret �22 weeks of gestation was associatedirth at �37 weeks of gestation and latein the risk of preterm birth at �33 weeksight, admission to neonatal intensive careeffects. Clindamycin in early pregnancy inrisk of spontaneous preterm birth at �37
e is evidence to justify further randomizedtion of preterm birth. However, a deeperosal immunity, and the biology of bacterialof such trials.
damycin, late miscarriage, preterm birth
whweea syistr. Fid a
bceswe
ersethe
hervenuc
gn
clin
amniotic fluid.96 However, it would be
erican Journal of Obstetrics & Gynecology 177

ropctl
t
icagsbbitu
caov
Reviews Obstetrics www.AJOG.org
convenient to identify these patients byexamining changes in the microbial floraof the lower genital tract, because thiswould be relatively easy and non-inva-sive. BV is characterized by a change inthe microbial ecosystem of the va-gina.97,98 Its presence is associated withan increased risk for spontaneous pre-term delivery71,97-108 and intraamnioticinfection.109-112 Therefore, investigatorseason that identification and treatmentf BV would result in a decreased rate ofreterm delivery. Many randomizedlinical trials have been conducted to testhis hypothesis, and the results have beenargely negative;73-81 although, some tri-
als have yielded positive results.82-87
The contradictory results among trialsof BV have been attributed to: (1) thedefinition of BV; (2) the gestational ageat diagnosis and enrollment; (3) thechoice of antimicrobial agent used, aswell as the dose and route of administra-tion; (4) whether antibiotic administra-tion has been followed by a test of cure;(5) the primary outcome of the study(most have used delivery at �37 weeksrather than early preterm delivery, wheremost of the infection-related pretermbirths [PTBs] occur);113 (6) gene-envi-ronment interactions related to the in-flammatory response;114-116 and (7) pa-ient population, etc.
For antibiotics to be effective in reduc-ng the rate of preterm delivery, severalriteria must be met:95 (1) antimicrobi-ls must be effective against the target or-anism or the clinical condition undertudy (eg, BV); (2) antimicrobials shoulde used only in women who can benefitecause they are at substantial risk for
nfection or an infection-related condi-ion; and (3) antimicrobials must besed early enough117 so that eradication
of the microorganisms would be fol-lowed by resolution of any inflammatoryresponse66,118,119 and its unintendedonsequences (eg, damage of the chorio-mniotic membranes, microbial invasionf the amniotic cavity, fetal microbial in-asion, and fetal inflammation).120-122
The importance of the timing of anti-biotic administration has recently be-come more apparent because there is ev-idence that exposure to either bacterial
products (eg, endotoxin or lipopolysac-178 American Journal of Obstetrics & Gynecology
charide) or bacteria itself, which is notenough to signal the onset of preterm la-bor, may predispose to a subsequent vi-ral infection, and this, in turn, leads toboth preterm labor and fetal damage.123
Several systematic reviews and meta-analyses have been conducted to deter-mine the effect of antimicrobial agentsfor the prevention of PTB in women withBV.124-133 Such efforts need to be revis-ited to focus both on clindamycin andearly treatment.86,87,134
The purpose of this study was to con-duct a systematic review and metaanaly-sis to determine whether treatment ofpatients with BV with clindamycin be-fore 22 weeks of gestation can reduce therate of spontaneous PTB. The justifica-tion for the study is that several trialshave suggested a beneficial effect of thisantibiotic in reducing the rate of PTB inpatients at risk when administered earlyduring pregnancy. Most studies aimedat reducing the rate of PTB have usedmetronidazole, and such studies haveyielded negative results.
Materials and methodsThe systematic review was conducted us-ing a prospectively prepared protocoland reported with the use of the Pre-ferred Reporting Items for SystematicReviews and Meta-analyses.135
Literature searchA computerized search was performedwith PubMed, Embase, Cinahl, and Lilacs(all from inception of database to July 31,2011), ISI Web of science (http://www.isiknowledge.com; 1960 to July 31, 2011),the Cochrane Central Register of ControlledTrials (http://www.mrw.interscience.wiley.com/cochrane/cochrane_clcentral_articles_fs.html; 1960 to July 31, 2011), and Re-search Registries of ongoing trials (www.clinicaltrials.gov, www.controlled-trials.com, www.centerwatch.com, www.actr.org.au, www.nrr.nhs.uk, and www.umin.ac.jp/ctr) with a combination of key and textwords that are related to antibiotics, BV,prevention, or PTB. Proceedings of theSociety for Maternal-Fetal Medicine andinternational meetings on PTB, refer-ence lists of identified studies, textbooks,previously published systematic reviews,
and review articles were also explored.SEPTEMBER 2011
No language restrictions were applied.All searches were carried out indepen-dently by 2 authors (R.F.L. and C.N.),and the results were merged. For studiesthat were reported in multiple publica-tions, the data from the publication withthe report of the primary outcomes andthe largest sample size were used.
Study selectionWe included randomized controlled tri-als that compared early treatment ofwomen at �22 completed weeks of ges-tation with abnormal vaginal flora andasymptomatic BV that was diagnosedusing objective criteria, with either oralclindamycin or clindamycin vaginalcream (CVC) vs placebo or no interven-tion. Only studies whose primary aimwas to prevent PTB (delivery at �37weeks of gestation) were included in theanalysis. Quasirandomized studies wereexcluded. Other inclusion criteria con-sisted of pregnant women with a gesta-tional age of �22 weeks of gestation atscreening and commencement of treat-ment who were not in labor, had no vag-inal bleeding, and did not report symp-toms of lower genital tract infection. Thediagnosis of BV was based on first tri-mester or early second trimester screen-ing programs through the identificationof abnormal lower genital tract flora andBV with the use of screening Gram stainsscored by the Spiegel et al,136 Nugent etal,137 Hay et al,71 or Ison and Hay138 cri-teria. Studies with rescreening and re-treatment protocols were included in thefinal analysis. All studies that weredeemed appropriate were retrieved andreviewed independently by the 2 screen-ing authors to determine inclusion. Dis-agreements were resolved through con-sensus discussions.
Outcome measuresThe primary outcomes of interest werespontaneous PTB at �37 completedweeks of gestation and late miscarriage(LM; birth between 16 and 23 completedweeks of gestation). Spontaneous PTB�37 completed weeks of gestation waschosen because this primary outcomewas used in most metaanalyses that
evaluated preventative strategies for
mq2mtsmq(sts
DTtaqtwefegtmt(ad
SDi
cnactawopfpratettesesae
s
oisptsWd�
bti
va
wtcii
zr1
bwn�potpp(ND
www.AJOG.org Obstetrics Reviews
PTB. Secondary outcomes includedbirthweight, low birthweight, very lowbirthweight, gestational age at delivery,early PTB (�30 completed weeks of ges-tation), admission to the neonatal inten-sive care unit (NICU), success of treat-ment according to degree of abnormalflora, persistent or recurrent BV, peri-partum infections, and long-term fol-low-up evaluation.
Study quality assessmentWe developed a quality assessment toolfor studies of clindamycin effectivenessusing the recommendations of HealthTechnology Assessment for the identifi-cation of systematic reviews.139 The for-mat for the quality assessment tool pre-viously has been used in a systematicreview of the efficacy of nifedipine as atocolytic.140,141 The quality of study
ethods was assessed with a tailoreduality checklist that structured items in
broad categories: topic-specific orethod-specific items. Furthermore,
hese items were divided into 3 generalubcategories: selection bias, perfor-
ance bias, and measurement bias. Alluality determinations were scored as1) adequate, (2) inadequate, or (3) nottated in the article. Consensus amonghe authors was reached through discus-ion and reevaluation.
ata abstractionwo reviewers (R.F.L. and C.N.) scanned
he abstracts and titles. Hard copies forll potentially relevant articles were ac-uired and evaluated independently byhe 2 reviewers; authorship of the articlesas not blinded. All outcome data were
xtracted independently, in duplicateorm, by 2 reviewers. Information wasxtracted on study methods, studyroup demographics, intervention de-ails (dose, type, placebo, no treat-
ent), the use of rescreening and re-reatment in the studies, and the outcomesnumber of outcome events). Consensusmong the authors was reached throughiscussion and reevaluation.
tatistical analysisata from each of the studies considered
n this study were organized in 2 � 2 a
ontingency tables that contained theumber of patients who were classifiedccording to pregnancy outcome and thelindamycin treatment (treated, notreated). We calculated the summary rel-tive risk (RR) for dichotomous data andeighted mean difference for continu-us data with associated 95% CIs. Tworespecified subgroup analyses were per-
ormed to compare clindamycin withlacebo/no treatment according to theoute of administration (vaginal vs oral)nd re-treatment (yes vs no). In addi-ion, we conducted sensitivity analyses toxplore the robustness of the findings forhe primary outcome according to a sta-istical model (fixed-effects vs random-ffects), use of placebo (yes vs no), andtudy quality (high vs not high). How-ver, the sensitivity analysis according totudy quality was not performed becausell trials that were included were consid-red as high quality.
Heterogeneity of the results amongtudies was tested with the quantity I2,
which describes the percentage of totalvariation across studies that is due to het-erogeneity rather than chance.142 A value
f 0% indicates no observed heterogene-ty, whereas I2 values of �50% indicate aubstantial level of heterogeneity.142 Welanned to pool data across studies usinghe fixed-effects models if substantialtatistical heterogeneity was not present.
e used random-effects models to poolata across studies if I2 values were50%.We assessed publication and related
iases visually by examining the symme-ry of funnel plots and statistically by us-ng the test of Egger et al.143 The larger
the deviation of the intercept of the re-gression line from zero, the greater theasymmetry and the more likely it wasthat the metaanalysis would yield biasedestimates of effect. As suggested by Eggeret al,143 we considered a probabilityalue of � .1 to indicate significantsymmetry.
We also calculated the number thatas needed to treat (NNT) for an addi-
ional beneficial outcome with its 95%onfidence intervals (CIs) for outcomesn which the treatment effect was signif-cant at the 5% level (the 95% CI for the
bsolute risk difference did not includeSEPTEMBER 2011 Am
ero).144 NNT was computed from theesults of metaanalysis of RRs: NNT �/control group event rate � (1-RR).In this review, NNT for an additional
eneficial outcome is the number ofomen with abnormal vaginal flora whoeed to be treated with clindamycin at22 weeks of gestation rather than with
lacebo or no treatment to prevent 1 casef spontaneous PTB at �37 weeks of ges-ation or 1 LM between 16 and 23 com-leted weeks of gestation. Analyses wereerformed with the Review ManagerRevMan; software version 5.0.23; Theordic Cochrane Centre, Copenhagen,enmark).
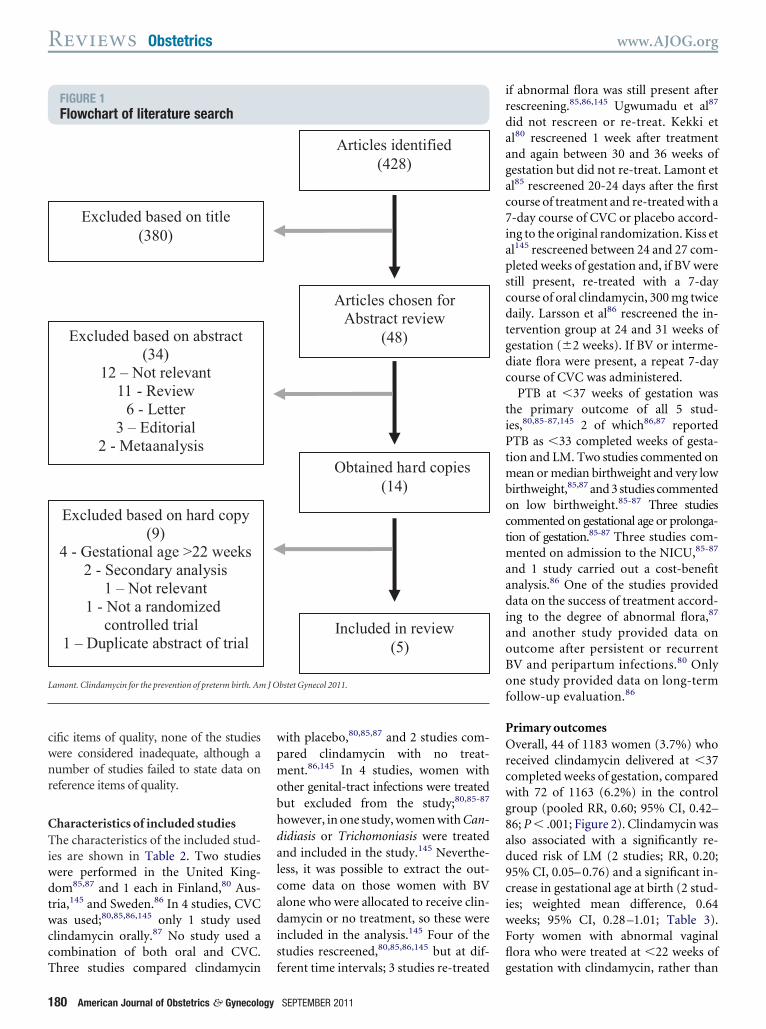
ResultsLiterature identificationThe flow of the electronic literaturesearch is shown in Figure 1. Of the 428potentially relevant citations that wereidentified, 414 were excluded based onthe title or on review of the abstract.Based on abstract review, hard copies of14 articles were obtained. After a detailedreview, 5 studies fulfilled the inclusioncriteria and are included in the analy-sis.80,85-87,145 Of the 9 studies that wereexcluded, 2 were subgroup analyses oflarger studies;75,79 1 article was not a ran-domized controlled trial;84 4 trials in-cluded patients who were screenedand treated at �22 weeks of gesta-tion;74,77,81,105 1 trial was a conferenceabstract146 of 1 of the included studies,85
and 1 article was an observationalstudy.102 We contacted the first authorsof 3 trials74,81,105 to request further infor-mation. None of these authors were ableto provide data for the subgroup ofwomen who were treated at �22 weeksof gestation, so these studies were ex-cluded from the primary analysis. The 5trials comprised a total of 2346 women.
Study quality assessmentThe results of the evaluation of the stud-ies’ adherence to the criteria within the 2domains of quality (method- and topic-specific items) are presented in Table 1.For all the method-specific items ofquality, most of the studies were adequate.For 11 of the 16 topic-specific items ofquality, most of the studies were consid-
ered adequate. In 14 of the 16 topic-spe-erican Journal of Obstetrics & Gynecology 179
t
pmob
lcadis
agac7ia
tgdc
ti
octm
di
Reviews Obstetrics www.AJOG.org
cific items of quality, none of the studieswere considered inadequate, although anumber of studies failed to state data onreference items of quality.
Characteristics of included studiesThe characteristics of the included stud-ies are shown in Table 2. Two studieswere performed in the United King-dom85,87 and 1 each in Finland,80 Aus-ria,145 and Sweden.86 In 4 studies, CVC
was used;80,85,86,145 only 1 study usedclindamycin orally.87 No study used acombination of both oral and CVC.
FIGURE 1Flowchart of literature search
Excluded based on title (380)
Excluded based on abstract (34)
12 – Not relevant 11 - Review
6 - Letter 3 – Editorial
2 - Metaanalysis
Excluded based on hard copy (9)
4 - Gestational age >22 weeks 2 - Secondary analysis
1 – Not relevant 1 - Not a randomized
controlled trial 1 – Duplicate abstract of trial
Lamont. Clindamycin for the prevention of preterm birth. Am
Three studies compared clindamycin
180 American Journal of Obstetrics & Gynecology
with placebo,80,85,87 and 2 studies com-ared clindamycin with no treat-ent.86,145 In 4 studies, women with
ther genital-tract infections were treatedut excluded from the study;80,85-87
however, in one study, women with Can-didiasis or Trichomoniasis were treatedand included in the study.145 Neverthe-ess, it was possible to extract the out-ome data on those women with BVlone who were allocated to receive clin-amycin or no treatment, so these were
ncluded in the analysis.145 Four of thetudies rescreened,80,85,86,145 but at dif-
Articles identified (428)
Obtained hard copies (14)
Included in review (5)
Articles chosen for Abstract review
(48)
bstet Gynecol 2011.
ferent time intervals; 3 studies re-treated
SEPTEMBER 2011
if abnormal flora was still present afterrescreening.85,86,145 Ugwumadu et al87
did not rescreen or re-treat. Kekki etal80 rescreened 1 week after treatmentnd again between 30 and 36 weeks ofestation but did not re-treat. Lamont etl85 rescreened 20-24 days after the firstourse of treatment and re-treated with a-day course of CVC or placebo accord-ng to the original randomization. Kiss etl145 rescreened between 24 and 27 com-
pleted weeks of gestation and, if BV werestill present, re-treated with a 7-daycourse of oral clindamycin, 300 mg twicedaily. Larsson et al86 rescreened the in-ervention group at 24 and 31 weeks ofestation (�2 weeks). If BV or interme-iate flora were present, a repeat 7-dayourse of CVC was administered.
PTB at �37 weeks of gestation washe primary outcome of all 5 stud-es,80,85-87,145 2 of which86,87 reported
PTB as �33 completed weeks of gesta-tion and LM. Two studies commented onmean or median birthweight and very lowbirthweight,85,87 and 3 studies commented
n low birthweight.85-87 Three studiesommented on gestational age or prolonga-ion of gestation.85-87 Three studies com-
ented on admission to the NICU,85-87
and 1 study carried out a cost-benefitanalysis.86 One of the studies provided
ata on the success of treatment accord-ng to the degree of abnormal flora,87
and another study provided data onoutcome after persistent or recurrentBV and peripartum infections.80 Onlyone study provided data on long-termfollow-up evaluation.86
Primary outcomesOverall, 44 of 1183 women (3.7%) whoreceived clindamycin delivered at �37completed weeks of gestation, comparedwith 72 of 1163 (6.2%) in the controlgroup (pooled RR, 0.60; 95% CI, 0.42–86; P � .001; Figure 2). Clindamycin wasalso associated with a significantly re-duced risk of LM (2 studies; RR, 0.20;95% CI, 0.05– 0.76) and a significant in-crease in gestational age at birth (2 stud-ies; weighted mean difference, 0.64weeks; 95% CI, 0.28 –1.01; Table 3).Forty women with abnormal vaginalflora who were treated at �22 weeks of
J O
gestation with clindamycin, rather than

swamt
. Am
www.AJOG.org Obstetrics Reviews
with placebo, were needed to prevent 1case of spontaneous PTB (95% CI, 25–121). The corresponding NNT for LM is66 (95% CI, 47–228).
Sensitivity analysisHaving obtained no additional datafrom the trials that included women whowere screened and treated at �22 weeksof gestation,74,81,105 we performed a sen-itivity analysis by adding data for 100omen from the trial by Guaschino et
l81 (mean gestational age at enroll-ent, 19.2 weeks) and 302 women from
TABLE 1Assessment of quality items
Variable
Stu
Ke20
Method specific items of quality..........................................................................................................
Randomization Un..........................................................................................................
Concealment Ina..........................................................................................................
Blinding Ad..........................................................................................................
Attrition bias Ad..........................................................................................................
A priori sample size calculation Ad...................................................................................................................
TOPIC-SPECIFIC ITEMS OF QUALITY
Selection bias..........................................................................................................
Age Ad..........................................................................................................
Parity Ad..........................................................................................................
Socioeconomic status Un..........................................................................................................
Race Un..........................................................................................................
Smoking Un..........................................................................................................
Substance abuse Un..........................................................................................................
Previous preterm birth Un..........................................................................................................
Previous late miscarriage Un...................................................................................................................
Performance bias..........................................................................................................
Frequency Ad..........................................................................................................
Dose Ad..........................................................................................................
Duration Ad..........................................................................................................
Route of administration Ad..........................................................................................................
Measurement bias Ad..........................................................................................................
Rescreening Ad..........................................................................................................
Re-treating Ina..........................................................................................................
Long-term follow up Un...................................................................................................................
Lamont. Clindamycin for the prevention of preterm birth
he trial by Joesoef et al74 who were en-
rolled at �21 weeks of gestation.Women from the study by McGregor etal105 were not included in this sensitivityanalysis because the mean gestationalage at enrollment was 21.5 weeks. We as-sumed that frequencies of PTB at �37weeks of gestation in clindamycin andplacebo groups were similar to those ofwomen of all gestational ages who wereenrolled in each group. The significantlydecreased risk of PTB at �37 weeks ofgestation was demonstrated even inthis sensitivity analysis (7 studies; 2748women; RR, 0.72; 95% CI, 0.54 – 0.96;
et al,0
Lamont et al,200385
Ugwumadu200387
.........................................................................................................................
ed Adequate Adequate.........................................................................................................................
uate Adequate Adequate.........................................................................................................................
ate Adequate Adequate.........................................................................................................................
ate Adequate Adequate.........................................................................................................................
ate Adequate Adequate.........................................................................................................................
.........................................................................................................................
ate Adequate Adequate.........................................................................................................................
ate Adequate Adequate.........................................................................................................................
ed Unstated Unstated.........................................................................................................................
ed Adequate Adequate.........................................................................................................................
ed Adequate Unstated.........................................................................................................................
ed Adequate Unstated.........................................................................................................................
ed Adequate Adequate.........................................................................................................................
ed Unstated Adequate.........................................................................................................................
.........................................................................................................................
ate Adequate Adequate.........................................................................................................................
ate Adequate Adequate.........................................................................................................................
ate Adequate Adequate.........................................................................................................................
ate Adequate Adequate.........................................................................................................................
ate Adequate Adequate.........................................................................................................................
ate Adequate Inadequate.........................................................................................................................
uate Adequate Inadequate.........................................................................................................................
ed Unstated Unstated.........................................................................................................................
J Obstet Gynecol 2011.
I2, 40%).
SEPTEMBER 2011 Am
The random-effects analysis of the pri-mary outcome of spontaneous PTB at�37 weeks of gestation yielded an effectsize similar in magnitude and directionto that obtained from the fixed-effectsanalysis, although it was not significant(RR, 0.64; 95% CI, 0.39 –1.05; Table 4).The decrease in the risk of PTB at �37weeks of gestation was nominallygreater in trials that used placebo (RR,0.55; 95% CI, 0.27–1.11) than in trialsthat did not use placebo (RR, 0.87; 95%CI, 0.45–1.68).
The significantly decreased risk of PTB
al, Kiss et al,2004145
Larsson et al,200686
..................................................................................................................
Adequate Adequate..................................................................................................................
Adequate Adequate..................................................................................................................
Inadequate Inadequate..................................................................................................................
Adequate Adequate..................................................................................................................
Adequate Adequate..................................................................................................................
..................................................................................................................
Unstated Adequate..................................................................................................................
Adequate Adequate..................................................................................................................
Unstated Unstated..................................................................................................................
Adequate Unstated..................................................................................................................
Unstated Adequate..................................................................................................................
Unstated Unstated..................................................................................................................
Adequate Adequate..................................................................................................................
Unstated Unstated..................................................................................................................
..................................................................................................................
Unstated Unstated..................................................................................................................
Adequate Unstated..................................................................................................................
Adequate Adequate..................................................................................................................
Adequate Adequate..................................................................................................................
Adequate Adequate..................................................................................................................
Adequate Adequate..................................................................................................................
Adequate Adequate..................................................................................................................
Unstated Adequate..................................................................................................................
dy
kki018
et
......... .........
stat......... .........
deq......... .........
equ......... .........
equ......... .........
equ......... .........
......... .........
equ......... .........
equ......... .........
stat......... .........
stat......... .........
stat......... .........
stat......... .........
stat......... .........
stat......... .........
......... .........
equ......... .........
equ......... .........
equ......... .........
equ......... .........
equ......... .........
equ......... .........
deq......... .........
stat......... .........
at �37 weeks of gestation was demon-
erican Journal of Obstetrics & Gynecology 181
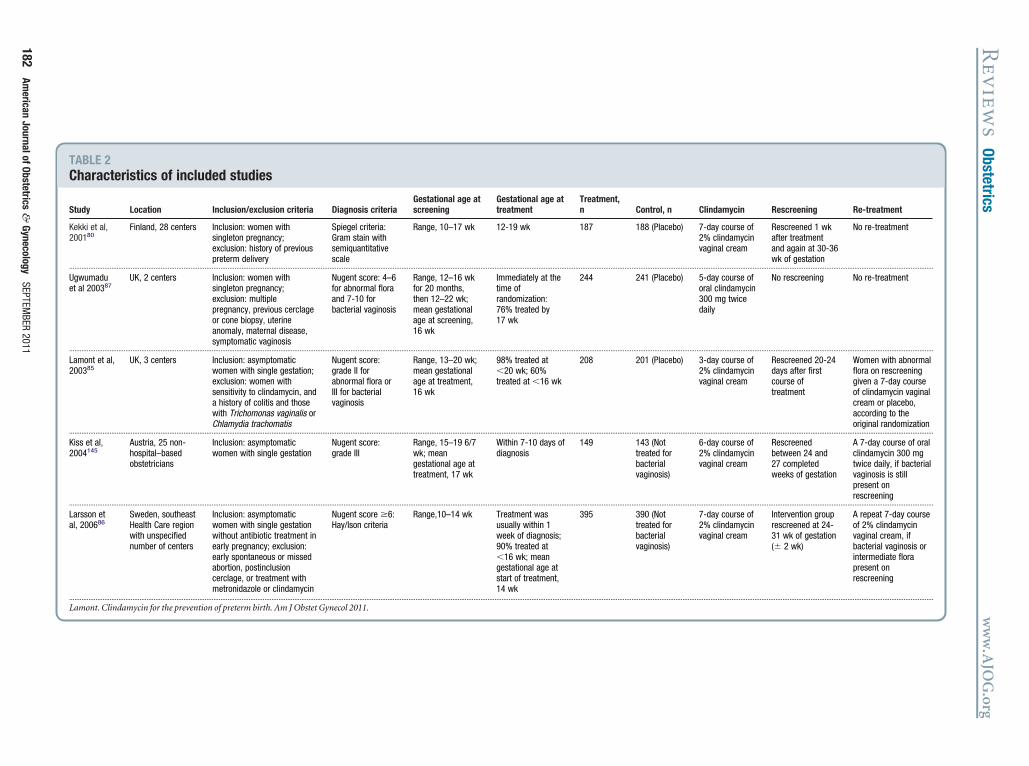
TABLE 2Characteristics of included studies
Study Location Inclusion/exclusion criteria Diagnosis criteriaGestational age atscreening
Gestational age attreatment
Treatment,n Control, n Clindamycin Rescreening Re-treatment
Kekki et al,200180
Finland, 28 centers Inclusion: women withsingleton pregnancy;exclusion: history of previouspreterm delivery
Spiegel criteria:Gram stain withsemiquantitativescale
Range, 10–17 wk 12-19 wk 187 188 (Placebo) 7-day course of2% clindamycinvaginal cream
Rescreened 1 wkafter treatmentand again at 30-36wk of gestation
No re-treatment
............................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
Ugwumaduet al 200387
UK, 2 centers Inclusion: women withsingleton pregnancy;exclusion: multiplepregnancy, previous cerclageor cone biopsy, uterineanomaly, maternal disease,symptomatic vaginosis
Nugent score: 4–6for abnormal floraand 7-10 forbacterial vaginosis
Range, 12–16 wkfor 20 months,then 12–22 wk;mean gestationalage at screening,16 wk
Immediately at thetime ofrandomization:76% treated by17 wk
244 241 (Placebo) 5-day course oforal clindamycin300 mg twicedaily
No rescreening No re-treatment
............................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
Lamont et al,200385
UK, 3 centers Inclusion: asymptomaticwomen with single gestation;exclusion: women withsensitivity to clindamycin, anda history of colitis and thosewith Trichomonas vaginalis orChlamydia trachomatis
Nugent score:grade II forabnormal flora orIII for bacterialvaginosis
Range, 13–20 wk;mean gestationalage at treatment,16 wk
98% treated at�20 wk; 60%treated at �16 wk
208 201 (Placebo) 3-day course of2% clindamycinvaginal cream
Rescreened 20-24days after firstcourse oftreatment
Women with abnormalflora on rescreeninggiven a 7-day courseof clindamycin vaginalcream or placebo,according to theoriginal randomization
............................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
Kiss et al,2004145
Austria, 25 non-hospital–basedobstetricians
Inclusion: asymptomaticwomen with single gestation
Nugent score:grade III
Range, 15–19 6/7wk; meangestational age attreatment, 17 wk
Within 7-10 days ofdiagnosis
149 143 (Nottreated forbacterialvaginosis)
6-day course of2% clindamycinvaginal cream
Rescreenedbetween 24 and27 completedweeks of gestation
A 7-day course of oralclindamycin 300 mgtwice daily, if bacterialvaginosis is stillpresent onrescreening
............................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
Larsson etal, 200686
Sweden, southeastHealth Care regionwith unspecifiednumber of centers
Inclusion: asymptomaticwomen with single gestationwithout antibiotic treatment inearly pregnancy; exclusion:early spontaneous or missedabortion, postinclusioncerclage, or treatment withmetronidazole or clindamycin
Nugent score �6:Hay/Ison criteria
Range,10–14 wk Treatment wasusually within 1week of diagnosis;90% treated at�16 wk; meangestational age atstart of treatment,14 wk
395 390 (Nottreated forbacterialvaginosis)
7-day course of2% clindamycinvaginal cream
Intervention grouprescreened at 24-31 wk of gestation(� 2 wk)
A repeat 7-day courseof 2% clindamycinvaginal cream, ifbacterial vaginosis orintermediate florapresent onrescreening
............................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
Lamont. Clindamycin for the prevention of preterm birth. Am J Obstet Gynecol 2011.
Rev
iews
Obstetricsw
ww
.AJO
G.org
182Am
ericanJournalofObstetrics
&Gynecology
SEPTEMBER
2011

mwp
ddeNg
fmNcLr
www.AJOG.org Obstetrics Reviews
strated in the subgroup of 1 trial (485women) that used oral clindamycin (RR,0.39; 95% CI, 0.20 – 0.76). Nevertheless,no statistically significant differences be-tween groups were seen in the subgroupof trials that used vaginal clindamycin (4trials; RR, 0.73; 95% CI, 0.47–1.14) orthat used (3 trials; RR, 0.63; 95% CI,0.38 –1.04) or did not use (2 trials; RR,0.67; 95% CI, 0.21–2.18) re-treatment,although this may be due to the weight-ing of the trial of Ugwumadu et al.87
FIGURE 2Preterm birth at <37 weeks of ges
df, degrees of freedom; M-H, Mantel-Haenszel test.
Lamont. Clindamycin for the prevention of preterm birth. Am
TABLE 3Effect of clindamycin on spontaneo
Outcome
Spontaneous preterm birth �37 weeks of gesta.............................................................................................................................
Late miscarriage.............................................................................................................................
Spontaneous preterm birth �37 weeks of gestaor late miscarriage.............................................................................................................................
Spontaneous preterm birth �33 weeks of gesta.............................................................................................................................
Gestational age at delivery, wks.............................................................................................................................
Low birthweight.............................................................................................................................
Very low birthweight.............................................................................................................................
Birthweight, g.............................................................................................................................
Admission to neonatal intensive care unit.............................................................................................................................
Stillbirth.............................................................................................................................
Peripartum infection.............................................................................................................................
Adverse effects...................................................................................................................
CI, confidence interval; NA, not applicable.a Fixed effects model.
Lamont. Clindamycin for the prevention of preterm birth. Am
Secondary outcomesThere was no overall difference in therisk of PTB at �33 weeks of gestation,low birthweight, very low birthweight,admission to NICU, stillbirth, peripar-tum infection, and adverse effects, al-though these outcomes were recorded inonly 1 or 2 trials.
Larsson et al86 demonstrated that theean number of days spent in the NICUas 45 for those in the control group com-ared with 18 for those who received clin-
ion (5 studies; fixed effects model)
bstet Gynecol 2011.
preterm birth and perinatal/materna
Number oftrials
Number of events/total numbor total number
Clindamycin, n/N (%) Place
580,85-87,145 44/1183 (3.7) 72/1....................................................................................................................................
286,87 2/639 (0.3) 12/6....................................................................................................................................
286,87 24/639 (3.8) 50/6
....................................................................................................................................
286,87 4/639 (0.6) 9/6....................................................................................................................................
285,87 442 434....................................................................................................................................
285,87 38/444 (8.6) 38/4....................................................................................................................................
285,87 13/444 (2.9) 8/4....................................................................................................................................
180 244 241....................................................................................................................................
180 18/238 (7.6) 23/2....................................................................................................................................
285,87 2/386 (0.5) 4/3....................................................................................................................................
180 21/187 (11.2) 33/1....................................................................................................................................
280,87 23/426 (5.4) 14/4.........................................................................................................................
J Obstet Gynecol 2011.
SEPTEMBER 2011 Am
amycin (P � .14) and the cumulativeays were 223 and 70, respectively. With anstimated cost of $1602 per day in theICU, the additional cost for the control
roup was approximately $245,136.Clindamycin appeared to be most ef-
ective the greater the degree of abnor-al flora. In women with the highestugent score (10), those who received
lindamycin had a 5.4% rate of PTB andM, compared with 35.7% in those whoeceived placebo.87
utcomes
Relative risk or meandifference (95% CI) I2, %n/N (%)
(6.2) 0.60 (0.42–0.86)a 41.............................................................................................................................
(1.9) 0.20 (0.05–0.76) 0.............................................................................................................................
(7.9) 0.53 (0.20–1.40) 73
.............................................................................................................................
(1.4) 0.44 (0.14–1.41) 0.............................................................................................................................
0.64 (0.28–1.01) 0.............................................................................................................................
(9.0) 0.95 (0.62–1.45) 0.............................................................................................................................
(1.9) 1.54 (0.64–3.67) 37.............................................................................................................................
�12.0 (�128.6 to 104.2) NA.............................................................................................................................
(10.1) 0.75 (0.42–1.35) NA.............................................................................................................................
(1.0) 0.49 (0.09–2.67) 0.............................................................................................................................
(17.6) 0.64 (0.38–1.06) NA.............................................................................................................................
(3.3) 1.65 (0.86–3.16) 11..................................................................................................................
tat
J O
us l o
er
bo,
tion 163.......... .........
31.......... .........
tion 31
.......... .........
tion 31.......... .........
.......... .........
20.......... .........
20.......... .........
.......... .........
28.......... .........
81.......... .........
88.......... .........
27......... .........
erican Journal of Obstetrics & Gynecology 183

w3rwddtaaAa
toc
. Am
Reviews Obstetrics www.AJOG.org
In one study, BV persisted in 31% (115of 375) and recurred in 7% (26 of 375) ofthe study population.80 The overall rateof PTB and peripartum infection was al-most 3 times higher in women in whomBV persisted or recurred during preg-nancy (40 of 141; 28%) compared withthose in whom BV was cured (12 of 121;10%; odds ratio, 2.9; 95% CI, 1.3–5.2).Excluding women with intermediateGram stain findings and including onlythose who attended both follow-up vis-its, the rate of PTB was 15% (4 of 26) inthe subgroup in which BV was first curedbut later recurred, compared with only2% (2 of 121) in the subgroup in whichBV did not recur (odds ratio, 9.3; 95%CI, 1.6 –53.5). Kekki et al80 rescreened 1
eek after treatment and again between0 and 36 weeks of gestation but did note-treat. Nevertheless, 21 women (6%)ere given additional CVC for what theyescribed as “suspected symptomatic BVuring the rest of the pregnancy,” al-hough this was not defined. Kiss etl145 found that BV alone persisted inpproximately 10% of women (44/447).fter rescreening at 23 weeks, Larsson etl86 found that BV had resolved in 70%
of women; therefore, 30% of the women
TABLE 4Sensitivity and subgroup analysis oon spontaneous preterm birth at <
Subgroup Trials, n
Statistical analysis..........................................................................................................
Fixed effects 580,85-87,145
..........................................................................................................
Random effects 580,85-87,145
...................................................................................................................
Route of administration..........................................................................................................
Vaginal 480,85,86,145
..........................................................................................................
Oral 187
...................................................................................................................
Use of placebo..........................................................................................................
Yes 380,85,87
..........................................................................................................
No 286,145
...................................................................................................................
Re-treatment..........................................................................................................
Yes 385,86,145
..........................................................................................................
No 280,87
...................................................................................................................
CI, confidence interval; NA, not applicable.
Lamont. Clindamycin for the prevention of preterm birth
were re-treated. At 31 weeks of gestation,
184 American Journal of Obstetrics & Gynecology
10% of the women had experienced re-lapse and were again re-treated.
One study reported on long-term out-comes of preterm (but not term) in-fants.86 Twenty-one preterm infantswere followed up to 4 years. Among chil-dren in the control group, 1 child hadretrolental fibroplasia that requiredstrong eyeglasses, and 1 child was diag-nosed with bronchopulmonary dyspla-sia in the neonatal period, but persistedat 4 years of age. No severe treatment-related adverse events were noted.86 Allfunnel plots showed no asymmetry, ei-ther visually or in terms of statistical sig-nificance (P � .10 for all, by Eggertest143).
CommentPrincipal findings of the studyThis systematic review and metaanalysisof randomized clinical trials shows thatwhen clindamycin is administered topregnant women with evidence of BVbefore 22 weeks of gestation: (1) the rateof PTB before 37 weeks of gestation issignificantly lower than in the controlgroup. The reduction in the risk of PTBbefore 37 weeks of gestation was only sta-tistically significant for oral clindamycin
he effect of clindamycinweeks of gestation
Clindamycin, n/N (%) Placebo, n/N
.........................................................................................................................
44/1183 (3.7) 72/1163 (6.2).........................................................................................................................
44/1183 (3.7) 72/1163 (6.2).........................................................................................................................
.........................................................................................................................
33/939 (3.5) 44/922 (4.8).........................................................................................................................
11/244 (4.5) 28/241 (11.6).........................................................................................................................
.........................................................................................................................
28/639 (4.4) 54/630 (8.6).........................................................................................................................
16/544 (2.9) 18/533 (3.4).........................................................................................................................
.........................................................................................................................
24/752 (3.2) 37/734 (5.0).........................................................................................................................
20/431 (4.6) 35/429 (8.2).........................................................................................................................
J Obstet Gynecol 2011.
but not for vaginal clindamycin; (2) the v
SEPTEMBER 2011
mean gestational age at delivery was sig-nificantly higher in women treated withclindamycin than those allocated to thecontrol group; and (3) the rate of LM waslower (clindamycin vs control group)than in the control group.
Strengths of the studyThis study used rigorous methods forperforming a systematic review of ran-domized controlled trials, used a broadliterature search, assessed the qualityof the studies and is based on studiesthat have low-to-moderate statisticalheterogeneity. Moreover, the robustnessof the results for the primary outcome ofspontaneous PTB before 37 weeks wasexamined after performing a sensitivityanalysis by adding hypothetical datafrom 2 excluded studies.
Metronidazole vs clindamycinfor the treatment of BVAlthough both antibiotics have been rec-ommended for the treatment of symp-tomatic BV,147 their antimicrobial spec-rum is not identical. Clindamycin andther macrolides have a broader antimi-robial activity against organisms in-
Relative risk or meandifference (95% CI) I2, %
..................................................................................................................
0.60 (0.42–0.86) 41..................................................................................................................
0.64 (0.39–1.05) 41..................................................................................................................
..................................................................................................................
0.73 (0.47–1.14) 31..................................................................................................................
0.39 (0.20–0.76) NA..................................................................................................................
..................................................................................................................
0.55 (0.27–1.11) 55..................................................................................................................
0.87 (0.45–1.68) 0..................................................................................................................
..................................................................................................................
0.63 (0.38–1.04) 27..................................................................................................................
0.67 (0.21–2.18) 75..................................................................................................................
f t37
(%)
......... .........
......... .........
......... .........
......... .........
......... .........
......... .........
......... .........
......... .........
......... .........
......... .........
......... .........
......... .........
olved in BV, including Mobiluncus spp.

tpertMatw3
GstI
i
vh4
unht
l
pafce
cznPmywsehdaadwep
DaiTTmrstrdtbmAtnspc
www.AJOG.org Obstetrics Reviews
and mycoplasmas.98,148-151 Importantly,hese antibiotics have antiinflammatoryroperties.152-156 Patients with the high-st Nugent score (who have the most se-ious disruption in the microbial ecosys-em of the vagina, and in which
obiluncus spp. is frequently found) hadsignificantly lower rate of PTB when
reated with clindamycin, in comparisonith those in the placebo group (5.4% vs5.7%).87 Such observation is in keeping
with a subgroup analysis of anotherstudy,85 in which women with a grade III
ram stain (Nugent score, 7-10) re-ponded better to clindamycin thanhose who had intermediate flora (gradeI Gram stain, Nugent score 4-6).157
The cure rate of BV after treatmentwith oral clindamycin has been reportedto be as high as 90%,158 while the cure/mprovement rate for CVC is 70.8%.134
The 70.8-90% appears better than the40-77% cure rate after a 2-day course ofmetronidazole,78,159 or the use of clinda-mycin cream late in pregnancy.74,160
Two factors seem to influence responseto therapy: (1) choice of antibiotic; and(2) gestational age at which it isadministered.
Another issue which has not receivedfull attention is whether there is a need tofollow patients, confirm that treatmenthas been effective and the detection ofrecurrence and appropriate retreatment.Both antimicrobials can cure BV in alarge number of women, but the condi-tion can recur, and a second treatment3-6 weeks after eradication is still able tocure or improve BV in 50% of the pa-tients in whom the condition persistedor recurred (Lamont RF, Taylor-Robin-son D, unpublished personal communi-cation, 2009). However, there is no solidevidence that this can lead to a reductionin the rate of spontaneous PTB.
The route of administration of clinda-mycin appears to be important. Vaginaladministration delivers the highest con-centration of the antibiotic to the sitein which the vaginal ecosystem haschanged. If microorganisms have gainedaccess to the endometrium/decidua,CVC may not be effective at this site, andoral therapy may be beneficial. It is note-worthy that, in this review, CVC admin-
istration was not associated with a statis-tically significant reduction in the rate ofPTB.
A potential drawback of clindamycintreatment is the risk for C. difficile; how-ever, this complication has also been re-ported with other antibiotics.161 Theaginal preparation of clindamycinas limited systemic absorption (only%),162 and therefore, appears to be safer
than oral clindamycin.134
Insofar as metronidazole, in vitrostudies have demonstrated that metroni-dazole and other nitroimidazoles arelargely inactive against Gardnerella vagi-nalis, Mycoplasma hominis, Ureaplasma
realyticum,163,164 and Atopobium vagi-ae.165,166 Similarly, these compoundsave little or no activity against strep-ococci or Staphylococcus aureus.167
Yet, metronidazole administration towomen with symptomatic BV is associ-ated with a treatment success rate similarto clindamycin.168 This has been attrib-uted to the activity of the hydroxy me-tabolite of the drug in vivo, which is ef-fective against the organisms involved inBV. Another potential explanation isthat the administration of metronida-zole changes the microbial flora by erad-icating bacteria susceptible to it (eg, an-aerobes and other organisms), and thisfavors cure of BV.169
The need to examine the potentialvalue of clindamycinThe role of antibiotics in the preventionof PTB was considered to have promisenearly 2 decades ago. However, the re-sults of several studies in which antibiot-ics were administered to patients whosegenital tract was colonized with particu-lar microorganisms (eg, GBS, Urea-plasma urealyticum, Chlamydia tracho-matis, Trichomonas vaginalis) yieldedlargely negative results. We believe thatthe primary reason for this is that colo-nization with GBS,170 Ureaplasma urea-yticum,171,172 or infection of the endo-
cervix with Chlamydia trachomatis173 inthe absence of a systemic adaptive im-mune response is not a risk factor forpreterm delivery. Therefore, treatmentwith antibiotics of patients colonized orinfected with these organisms should notbe expected to reduce the rate of preterm
delivery, and that has been proven to be PSEPTEMBER 2011 Am
correct.90-93 In the case of BV in whichthere is an increased risk for preterm de-livery, such risk is modest and is nowknown to be affected by gene-environ-ment interactions.114-116 For example,
atients with symptomatic BV who carrypolymorphism for the tumor necrosis
actor-� receptor gene have a signifi-antly increased risk of preterm deliv-ry;114-116,174 yet, randomized clinical
trials have not taken into considerationthe maternal genotype that may conferrisk.
Results of clinical trials of antibioticsin patients with BV did not provide clearevidence of benefit,73-81 and in someases, the administration of metronida-ole was associated with adverse preg-ancy outcome (an excess rate ofTB).88 Alternatively, clindamycin ad-inistration early in pregnancy has
ielded more promising results.87 Yet,hen systematic reviews and metaanaly-
es have been conducted, all trials haveither not been included or the studiesave considered metronidazole and clin-amycin as equivalent, and gestationalge at the initiation of therapy has notlways been taken into account. We con-ucted this metaanalysis to explorehether clindamycin treatment of BV in
arly pregnancy could be of value for therevention of PTB.
oes clindamycin prevent PTBnd late spontaneous miscarriagen patients with BV?he findings of this study (Figure 2 andable 3) suggest that clindamycin ad-inistration before 22 weeks reduces the
ate of PTB at �37 weeks. However, sen-itivity analysis performed according tohe statistical model indicated that theeduction in PTB (�37 weeks) was onlyetected using a fixed effect model (rela-ive risk [RR], 0.60; 95% CI, 0.42– 0.86),ut not when using a random effectodel (RR, 0.64; 95% CI, 0.39 –1.05).lthough the point estimates of the rela-
ive risk are quite similar, the results areot significant in both analyses, and thisuggests some instability in the results,robably attributed to heterogeneity oflinical trials (heterogeneity, I2 � 41).
When the outcome was spontaneous
TB �33 weeks of gestation, the reduc-erican Journal of Obstetrics & Gynecology 185

dna[t
Reviews Obstetrics www.AJOG.org
tion in PTB was not statistically signifi-cant (0.6% [4/639] vs 1.4% [9/631]).This may reflect a limitation in samplesize as treatment was associated with a 2fold decrease in the rate of PTB. This par-ticular endpoint is important becauseearly PTB is expected to be associatedwith infection more frequently than latePTB, and most morbidity of preterm ne-onates is found among those born before33 weeks of gestation.
Of major interest, is that treatmentwith clindamycin before 22 weeks wasassociated with a significant reduction inlate spontaneous miscarriage (0.31% [2/639] vs 1.9% [12/631]). Nevertheless,these results are only based on 2 studies(Table 3).
Subgroup analysis indicated that theroute of administration of clindamycinis important. Oral clindamycin was asso-ciated with a significant 61% reductionin the rate of PTB �37 weeks (4.5% [11/244] vs 11.6% [28/241]). However, thisis only based on 1 study.87 Vaginal clin-
amycin was associated with a nonsig-ificant 27% reduction in the rate of PTBt �37 weeks (3.5% [33/939] vs 4.8%44/922]; RR, 0.73; 95% CI, 0.47–1.14; 4rials).80,85,86,145
Finally, retreatment of BV was notfound to have a significant effect on therate of spontaneous PTB (�37 weeks).This was based on the results of 3 stud-ies, which use retreatment and 2 inwhich retreatment was not employed(Table 4).
BV as a syndromeBV has traditionally been considered asingle condition in which the vaginal mi-crobial ecosystem has changed, and itspresence is associated with a greater riskof adverse pregnancy outcome, and spe-cifically, PTB. However, a number ofquestions remain about the etiology,pathophysiology, diagnosis and treat-ment of BV. We have recently proposedthat BV is a syndrome, and not a singlecondition.175 This is based on observa-tions which indicate that the profileof proinflammatory cytokines variesamong women with BV diagnosed with aGram stain. Some women have highconcentrations of proinflammatory cy-
tokines, and others do not.118,119,176 The186 American Journal of Obstetrics & Gynecology
outcome of pregnancy in this subset ofpatients may vary. Such differences mayaccount, in part, for the negative resultsof clinical trials. It is possible that thepredictive value of the Nugent score forspontaneous PTB may be improved bystudying the inflammatory response ofpatients with BV, or the genotype of themother for genes involved in the inflam-matory response or the microbiome ofthe vagina.175
Future studiesThe results of this systematic review andmetaanalysis suggest that some patientswith BV may benefit from early treat-ment with clindamycin. It would seemthat oral treatment is superior to vaginaltreatment. Additional randomized clini-cal trials are required to confirm thefindings of this metaanalysis. However, amuch deeper knowledge of the biology,diagnosis, taxonomy, and response totherapy are required to design such tri-als. An important conclusion of this re-view is that some late spontaneous mis-carriages may be prevented by treatmentwith clindamycin. This endpoint shouldbe included in future studies. f
REFERENCES1. Romero R, Sepulveda W, Baumann P, et al.The preterm labor syndrome: biochemical, cy-tologic, immunologic, pathologic, microbio-logic, and clinical evidence that preterm labor isa heterogeneous disease. Am J Obstet Gynecol1993;168:287.2. Romero R, Mazor M, Munoz H, Gomez R,Galasso M, Sherer DM. The preterm labor syn-drome. Ann N Y Acad Sci 1994;734:414-29.3. Romero R, Mazor M, Wu YK, et al. Infection inthe pathogenesis of preterm labor. Semin Peri-natol 1988;12:262-79.4. Gibbs RS, Romero R, Hillier SL, EschenbachDA, Sweet RL. A review of premature birth andsubclinical infection. Am J Obstet Gynecol1992;166:1515-28.5. Minkoff H. Prematurity: infection as an etio-logic factor. Obstet Gynecol 1983;62:137-44.6. Gomez R, Ghezzi F, Romero R, Munoz H,Tolosa JE, Rojas I. Premature labor and intra-amniotic infection. Clinical aspects and role ofthe cytokines in diagnosis and pathophysiol-ogy. Clin Perinatol 1995;22:281-342.7. Goldenberg RL, Hauth JC, Andrews WW. In-trauterine infection and preterm delivery. N EnglJ Med 2000;342:1500-7.8. Romero R, Espinoza J, Goncalves LF, Ku-
sanovic JP, Friel L, Hassan S. The role of inflam-SEPTEMBER 2011
mation and infection in preterm birth. Semin Re-prod Med 2007;25:21-39.9. DiGiulio DB, Romero R, Amogan HP, et al.Microbial prevalence, diversity and abundancein amniotic fluid during preterm labor: a molec-ular and culture-based investigation. PLoS One2008;3:e3056.10. DiGiulio DB, Romero R, Kusanovic JP, et al.Prevalence and diversity of microbes in the am-niotic fluid, the fetal inflammatory response, andpregnancy outcome in women with pretermpre-labor rupture of membranes. Am J ReprodImmunol 2010;64:38-57.11. Fidel PI Jr, Romero R, Maymon E, Hertel-endy F. Bacteria-induced or bacterial product-induced preterm parturition in mice and rabbitsis preceded by a significant fall in serum proges-terone concentrations. J Matern Fetal Med1998;7:222-6.12. Fidel PL Jr, Romero R, Wolf N, et al. Sys-temic and local cytokine profiles in endotoxin-induced preterm parturition in mice. Am J Ob-stet Gynecol 1994;170:1467-75.13. Hirsch E, Wang H. The molecular patho-physiology of bacterially induced preterm labor:insights from the murine model. J Soc GynecolInvestig 2005;12:145-55.14. Lamont RF. Infection and preterm labour.BJOG 1998;105:1339-40.15. Arias F, Rodriquez L, Rayne SC, Kraus FT.Maternal placental vasculopathy and infection:two distinct subgroups among patients with pre-term labor and preterm ruptured membranes.Am J Obstet Gynecol 1993;168:585-91.16. Kim YM, Bujold E, Chaiworapongsa T, et al.Failure of physiologic transformation of the spi-ral arteries in patients with preterm labor andintact membranes. Am J Obstet Gynecol2003;189:1063-9.17. Kim YM, Chaiworapongsa T, Gomez R, etal. Failure of physiologic transformation of thespiral arteries in the placental bed in pretermpremature rupture of membranes. Am J ObstetGynecol 2002;187:1137-42.18. Manabe Y, Sakaguchi M, Mori T. Distentionof the uterus activates its multiple pacemakersand induces their coordination. Gynecol ObstetInvest 1994;38:163-8.19. Manabe Y, Sakaguchi M, Nakajima A. Initi-ation of uterine contractions by purely mechan-ical stretching of the uterus at midpregnancy. IntJ Biol Res Pregnancy 1981;2:63-9.20. Leguizamon G, Smith J, Younis H, NelsonDM, Sadovsky Y. Enhancement of amniotic cy-clooxygenase type 2 activity in women with pre-term delivery associated with twins or polyhy-dramnios. Am J Obstet Gynecol 2001;184:117-22.21. Many A, Hill LM, Lazebnik N, Martin JG. Theassociation between polyhydramnios and pre-term delivery. Obstet Gynecol 1995;86:389-91.22. Kim CJ, Romero R, Kusanovic JP, et al. Thefrequency, clinical significance, and pathologi-cal features of chronic chorioamnionitis: a lesionassociated with spontaneous preterm birth.
Mod Pathol 2010;23:1000-11.
www.AJOG.org Obstetrics Reviews
23. Kim JS, Romero R, Kim MR, et al. Involve-ment of Hofbauer cells and maternal T cells invillitis of unknown aetiology. Histopathology2008;52:457-64.24. Kim MJ, Romero R, Kim CJ, et al. Villitis ofunknown etiology is associated with a distinctpattern of chemokine up-regulation in the feto-maternal and placental compartments: implica-tions for conjoint maternal allograft rejection andmaternal anti-fetal graft-versus-host disease.J Immunol 2009;182:3919-27.25. Romero R, Kusanovic JP, Munoz H, GomezR, Lamont RF, Yeo L. Allergy-induced pretermlabor after the ingestion of shellfish. J MaternFetal Neonatal Med 2010;23:351-9.26. Bytautiene E, Romero R, Vedernikov YP, ElZeky F, Saade GR, Garfield RE. Induction of pre-mature labor and delivery by allergic reaction andprevention by histamine H1 receptor antagonist.Am J Obstet Gynecol 2004;191:1356-61.27. Bytautiene E, Vedernikov YP, Saade GR,Romero R, Garfield RE. Endogenous mast celldegranulation modulates cervical contractility inthe guinea pig. Am J Obstet Gynecol 2002;186:438-45.28. Romero R, Mazor, M, Avila C, Quintero R,Munoz H. Uterine “allergy”: a novel mechanismfor preterm labor. Am J Obstet Gynecol1991;164:375.29. Hassan SS, Romero R, Vidyadhari D, et al.Vaginal progesterone reduces the rate of pre-term birth in women with a sonographic shortcervix: a multicenter, randomized, double-blind,placebo-controlled trial. Ultrasound Obstet Gy-necol 2011;38:18-31.30. Mesiano S. Roles of estrogen and proges-terone in human parturition. Front Horm Res2001;27:86-104.31. Mesiano S. Myometrial progesterone re-sponsiveness and the control of human partu-rition. J Soc Gynecol Investig 2004;11:193-202.32. Pieber D, Allport VC, Bennett PR. Proges-terone receptor isoform A inhibits isoform B-mediated transactivation in human amnion. EurJ Pharmacol 2001;427:7-11.33. Hassan SS, Romero R, Berry SM, Dang K,Blackwell SC, Treadwell MC et al. Patients withan ultrasonographic cervical length � or �15mm have nearly a 50% risk of early spontane-ous preterm delivery. Am J Obstet Gynecol2000;182:1458-67.34. Iams JD, Johnson FF, Sonek J, Sachs L,Gebauer C, Samuels P. Cervical competenceas a continuum: a study of ultrasonographiccervical length and obstetric performance. Am JObstet Gynecol 1995;172:1097-103.35. Heath VC, Southall TR, Souka AP, ElisseouA, Nicolaides KH. Cervical length at 23 weeks ofgestation: prediction of spontaneous pretermdelivery. Ultrasound Obstet Gynecol 1998;12:312-7.36. Smith CV, Anderson JC, Matamoros A,Rayburn WF. Transvaginal sonography of cer-vical width and length during pregnancy. J Ul-
trasound Med 1992;11:465-7.37. Gravett MG, Witkin SS, Haluska GJ, Ed-wards JL, Cook MJ, Novy MJ. An experimentalmodel for intraamniotic infection and pretermlabor in rhesus monkeys. Am J Obstet Gynecol1994;171:1660-7.38. Hirsch E, Saotome I, Hirsh D. A model ofintrauterine infection and preterm delivery inmice. Am J Obstet Gynecol 1995;172:1598-603.39. Romero R, Mazor M, Wu YK, Avila C, Oyar-zun E, Mitchell MD. Bacterial endotoxin and tu-mor necrosis factor stimulate prostaglandinproduction by human decidua. ProstaglandinsLeukot Essent Fatty Acids 1989;37:183-6.40. Abrahams VM, Bole-Aldo P, Kim YM, et al.Divergent trophoblast responses to bacterialproducts mediated by TLRs. J Immunol 2004;173:4286-96.41. Abrahams VM, Mor G. Toll-like receptorsand their role in the trophoblast. Placenta2005;26:540-7.42. Elovitz MA, Wang Z, Chien EK, Rychlik DF,Phillippe M. A new model for inflammation-in-duced preterm birth: the role of platelet-activat-ing factor and Toll-like receptor-4. Am J Pathol2003;163:2103-11.43. Kim YM, Romero R, Chaiworapongsa T, etal. Toll-like receptor-2 and -4 in the chorioam-niotic membranes in spontaneous labor at termand in preterm parturition that are associatedwith chorioamnionitis. Am J Obstet Gynecol2004;191:1346-55.44. Mor G, Romero R, Aldo PB, Abrahams VM.Is the trophoblast an immune regulator? Therole of Toll-like receptors during pregnancy. CritRev Immunol 2005;25:375-88.45. Kelly RW, Leask R, Calder AA. Choriode-cidual production of interleukin-8 and mecha-nism of parturition. Lancet 1992;339:776-7.46. Romero R, Ceska M, Avila C, Mazor M,Behnke E, Lindley I. Neutrophil attractant/acti-vating peptide-1/interleukin-8 in term and pre-term parturition. Am J Obstet Gynecol 1991;165:813-20.47. Romero R, Gomez R, Galasso M, et al.Macrophage inflammatory protein-1 alpha interm and preterm parturition: effect of microbialinvasion of the amniotic cavity. Am J ReprodImmunol 1994;32:108-13.48. Hamill N, Romero R, Gotsch F, et al. Exo-dus-1 (CCL20): evidence for the participation ofthis chemokine in spontaneous labor at term,preterm labor, and intrauterine infection. J Peri-nat Med 2008;36:217-27.49. Nhan-Chang CL, Romero R, Kusanovic JP,et al. A role for CXCL13 (BCA-1) in pregnancyand intra-amniotic infection/inflammation. JMatern Fetal Neonatal Med 2008;21:763-75.50. Romero R, Mazor M, Sepulveda W, Avila C,Copeland D, Williams J. Tumor necrosis factorin preterm and term labor. Am J Obstet Gynecol1992;166:1576-87.51. Romero R, Manogue KR, Mitchell MD, et al.Infection and labor: IV, cachectin-tumor necro-sis factor in the amniotic fluid of women withintraamniotic infection and preterm labor. Am J
Obstet Gynecol 1989;161:336-41.SEPTEMBER 2011 Am
52. Romero R, Avila C, Santhanam U, SehgalPB. Amniotic fluid interleukin 6 in preterm labor:association with infection. J Clin Invest 1990;85:1392-400.53. Romero R, Brody DT, Oyarzun E, et al. In-fection and labor. III. Interleukin-1: a signal forthe onset of parturition. Am J Obstet Gynecol1989;160:1117-23.54. Meis PJ, Goldenberg RL, Mercer B, et al.The preterm prediction study: significance ofvaginal infections: National Institute of ChildHealth and Human Development Maternal-Fe-tal Medicine Units Network. Am J Obstet Gyne-col 1995;173:1231-5.55. Hay P, Czeizel AE. Asymptomatic trichomo-nas and candida colonization and pregnancy out-come. Best Pract Res Clin Obstet Gynaecol2007;21:403-9.56. Andrews WW, Klebanoff MA, Thom EA, etal. Midpregnancy genitourinary tract infectionwith Chlamydia trachomatis: association withsubsequent preterm delivery in women withbacterial vaginosis and Trichomonas vaginalis.Am J Obstet Gynecol 2006;194:493-500.57. Cotch MF, Pastorek JG, Nugent RP, et al.Trichomonas vaginalis associated with low birthweight and preterm delivery. The Vaginal Infec-tions and Prematurity Study Group. SexTransm Dis 1997;24:353-60.58. Donders GG, Desmyter J, De Wet DH, VanAssche FA. The association of gonorrhoea andsyphilis with premature birth and low birth-weight. Genitourin Med 1993;69:98-101.59. Association of Chlamydia trachomatis andMycoplasma hominis with intrauterine growthretardation and preterm delivery. The JohnHopkins Study of Cervicitis and Adverse Preg-nancy Outcome. Am J Epidemiol 1989;129:1247-57.60. Breugelmans M, Vancutsem E, NaessensA, Laubach M, Foulon W. Association of abnor-mal vaginal flora and Ureaplasma species asrisk factors for preterm birth: a cohort study.Acta Obstet Gynecol Scand 2010;89:256-60.61. Kimberlin DF, Andrews WW. Bacterial vagi-nosis: association with adverse pregnancy out-come. Semin Perinatol 1998;22:242-50.62. Lamont RF, Taylor-Robinson D. The role ofbacterial vaginosis, aerobic vaginitis, abnormalvaginal flora and the risk of preterm birth. BJOG2010;117:119-21.63. Donders GG, Bosmans E, DekeersmaeckerA, Vereecken A, Van BB, Spitz B. Pathogenesisof abnormal vaginal bacterial flora. Am J ObstetGynecol 2000;182:872-8.64. Donati L, Di VA, Nucci M, et al. Vaginal mi-crobial flora and outcome of pregnancy. ArchGynecol Obstet 2010;281:589-600.65. Minkoff H, Grunebaum AN, Schwarz RH, etal. Risk factors for prematurity and prematurerupture of membranes: a prospective study ofthe vaginal flora in pregnancy. Am J Obstet Gy-necol 1984;150:965-72.66. Donders GG, Vereecken A, Bosmans E,Dekeersmaecker A, Salembier G, Spitz B. Def-
inition of a type of abnormal vaginal flora that iserican Journal of Obstetrics & Gynecology 187

17apmO7Rt(c7attrd7rwNvU7ads8Rdp
Reviews Obstetrics www.AJOG.org
distinct from bacterial vaginosis: aerobicvaginitis. BJOG 2002;109:34-43.67. Minkoff H, Grunebaum A, Feldman J, Cum-mings M, McCormack WM. Relationship ofvaginal pH and Papanicolaou smear results tovaginal flora and pregnancy outcome. Int JGynaecol Obstet 1987;25:17-23.68. Carey JC, Klebanoff MA. Is a change in thevaginal flora associated with an increased risk ofpreterm birth? Am J Obstet Gynecol 2005;192:1341-6.69. Mass SB, Brennan JP, Silverman N, vanHoeven KH. Association between a shift in vag-inal flora on Papanicolaou smear and acutechorioamnionitis and preterm delivery. DiagnCytopathol 1999;21:7-9.70. Usui R, Ohkuchi A, Matsubara S, et al. Vag-inal lactobacilli and preterm birth. J Perinat Med2002;30:458-66.71. Hay PE, Lamont RF, Taylor-Robinson D,Morgan DJ, Ison C, Pearson J. Abnormal bac-terial colonisation of the genital tract and sub-sequent preterm delivery and late miscarriage.BMJ 1994;308:295-8.72. McDonald HM, O’Loughlin JA, Jolley PT,Vigneswaran R, McDonald PJ. Changes in vag-inal flora during pregnancy and association withpreterm birth. J Infect Dis 1994;170:724-8.73. Duff P, Lee ML, Hillier SL, Herd LM, KrohnMA, Eschenbach DA. Amoxicillin treatment ofbacterial vaginosis during pregnancy. ObstetGynecol 1991;77:431-5.74. Joesoef MR, Hillier SL, Wiknjosastro G, etal. Intravaginal clindamycin treatment for bacte-rial vaginosis: effects on preterm delivery andlow birth weight. Am J Obstet Gynecol
995;173:1527-31.5. Rosenstein IJ, Morgan DJ, Lamont RF, etl. Effect of intravaginal clindamycin cream onregnancy outcome and on abnormal vaginalicrobial flora of pregnant women. Infect Disbstet Gynecol 2000;8:158-65.6. McDonald HM, O’Loughlin JA, Vigneswaran, et al. Impact of metronidazole therapy on pre-
erm birth in women with bacterial vaginosis floraGardnerella vaginalis): a randomised, placeboontrolled trial. BJOG 1997;104:1391-7.7. Vermeulen GM, Bruinse HW. Prophylacticdministration of clindamycin 2% vaginal creamo reduce the incidence of spontaneous pre-erm birth in women with an increased recur-ence risk: a randomised placebo-controlledouble-blind trial. BJOG 1999;106:652-7.8. Carey JC, Klebanoff MA, Hauth JC, et al. Met-onidazole to prevent preterm delivery in pregnantomen with asymptomatic bacterial vaginosis:ational Institute of Child Health and Human De-elopment Network of Maternal-Fetal Medicinenits. N Engl J Med 2000;342:534-40.9. Kurkinen-Raty M, Vuopala S, Koskela M, etl. A randomised controlled trial of vaginal clin-amycin for early pregnancy bacterial vagino-is. BJOG 2000;107:1427-32.0. Kekki M, Kurki T, Pelkonen J, Kurkinen-aty M, Cacciatore B, Paavonen J. Vaginal clin-amycin in preventing preterm birth and peri-
artal infections in asymptomatic women with188 American Journal of Obstetrics & Gynecology
bacterial vaginosis: a randomized, controlledtrial. Obstet Gynecol 2001;97:643-8.81. Guaschino S, Ricci E, Franchi M, et al.Treatment of asymptomatic bacterial vaginosisto prevent pre-term delivery: a randomised trial.Eur J Obstet Gynecol Reprod Biol 2003;110:149-52.82. Hauth JC, Goldenberg RL, Andrews WW,DuBard MB, Copper RL. Reduced incidence ofpreterm delivery with metronidazole and eryth-romycin in women with bacterial vaginosis.N Engl J Med 1995;333:1732-6.83. Morales WJ, Schorr S, Albritton J. Effect ofmetronidazole in patients with preterm birth inpreceding pregnancy and bacterial vaginosis: aplacebo-controlled, double-blind study. Am JObstet Gynecol 1994;171:345-7.84. McGregor JA, French JI, Parker R, et al.Prevention of premature birth by screening andtreatment for common genital tract infections:results of a prospective controlled evaluation.Am J Obstet Gynecol 1995;173:157-67.85. Lamont RF, Duncan SL, Mandal D, BassettP. Intravaginal clindamycin to reduce pretermbirth in women with abnormal genital tract flora.Obstet Gynecol 2003;101:516-22.86. Larsson PG, Fahraeus L, Carlsson B, Ja-kobsson T, Forsum U. Late miscarriage andpreterm birth after treatment with clindamycin: arandomised consent design study according toZelen. BJOG 2006;113:629-37.87. Ugwumadu A, Manyonda I, Reid F, Hay P.Effect of early oral clindamycin on late miscar-riage and preterm delivery in asymptomaticwomen with abnormal vaginal flora and bacte-rial vaginosis: a randomised controlled trial.Lancet 2003;361:983-8.88. Klebanoff MA, Carey JC, Hauth JC, et al.Failure of metronidazole to prevent preterm de-livery among pregnant women with asymptom-atic Trichomonas vaginalis infection. N EnglJ Med 2001;345:487-93.89. Grable IA, Garcia PM, Perry D, Socol ML.Group B Streptococcus and preterm prema-ture rupture of membranes: a randomized, dou-ble-blind clinical trial of antepartum ampicillin.Am J Obstet Gynecol 1996;175:1036-42.90. Klebanoff MA, Regan JA, Rao AV, et al.Outcome of the Vaginal Infections and Prema-turity Study: results of a clinical trial of erythro-mycin among pregnant women colonized withgroup B streptococci. Am J Obstet Gynecol1995;172:1540-5.91. Ogasawara KK, Goodwin TM. Efficacy ofazithromycin in reducing lower genital Urea-plasma urealyticum colonization in women atrisk for preterm delivery. J Matern Fetal Med1999;8:12-6.92. Eschenbach DA, Nugent RP, Rao AV, et al.A randomized placebo-controlled trial of eryth-romycin for the treatment of Ureaplasma urea-lyticum to prevent premature delivery. The Vag-inal Infections and Prematurity Study Group.Am J Obstet Gynecol 1991;164:734-42.93. Martin DH, Eschenbach DA, Cotch MF, etal. Double-Blind Placebo-Controlled Treatment
Trial of Chlamydia trachomatis Endocervical In-SEPTEMBER 2011
fections in Pregnant Women. Infect Dis ObstetGynecol 1997;5:10-7.94. Romero R, Mazor M, Oyarzun E, Sirtori M,Wu YK, Hobbins JC. Is there an associationbetween colonization with group B Streptococ-cus and prematurity? J Reprod Med 1989;34:797-801.95. Romero R, Sibai B, Caritis S, et al. Antibiotictreatment of preterm labor with intact mem-branes: a multicenter, randomized, double-blinded, placebo-controlled trial. Am J ObstetGynecol 1993;169:764-74.96. Romero R, Sirtori M, Oyarzun E, et al. Infec-tion and labor. V. Prevalence, microbiology, andclinical significance of intraamniotic infection inwomen with preterm labor and intact mem-branes. Am J Obstet Gynecol 1989;161:817-24.97. Lamont RF. Bacterial vaginosis. In: Critch-ley H, Bennett P, Thornton S, eds. Pretermbirth. London: RCOG Press; 2004:163-80.98. Hillier SL, Holmes KK. Bacterial vaginosis.In: Holmes KK, Markowitz LE, Spellacy W, Wig-gins R, eds. Sexually transmitted diseases, 2nded. New York: McGraw-Hill; 1990:547-50.99. Eschenbach DA, Gravett MG, Chen KC,Hoyme UB, Holmes KK. Bacterial vaginosisduring pregnancy: an association with prema-turity and postpartum complications. ScandJ Urol Nephrol Suppl 1984;86:213-22.100. McDonald HM, O’Loughlin JA, Jolley P,Vigneswaran R, McDonald PJ. Prenatal micro-biological risk factors associated with pretermbirth. BJOG 1992;99:190-6.101. Kurki T, Sivonen A, Renkonen OV, Savia E,Ylikorkala O. Bacterial vaginosis in early preg-nancy and pregnancy outcome. Obstet Gyne-col 1992;80:173-7.102. Riduan JM, Hillier SL, Utomo B, Wikn-josastro G, Linnan M, Kandun N. Bacterial vagi-nosis and prematurity in Indonesia: associationin early and late pregnancy. Am J Obstet Gyne-col 1993;169:175-8.103. Hillier SL, Nugent RP, Eschenbach DA, etal. Association between bacterial vaginosis andpreterm delivery of a low-birth-weight infant: theVaginal Infections and Prematurity Study group.N Engl J Med 1995;333:1737-42.104. Holst E, Goffeng AR, Andersch B. Bacte-rial vaginosis and vaginal microorganisms in id-iopathic premature labor and association withpregnancy outcome. J Clin Microbiol 1994;32:176-86.105. McGregor JA, French JI, Jones W, et al.Bacterial vaginosis is associated with prematu-rity and vaginal fluid mucinase and sialidase:results of a controlled trial of topical clindamycincream. Am J Obstet Gynecol 1994;170:1048-59.106. Gratacos E, Figueras F, Barranco M, et al.Spontaneous recovery of bacterial vaginosisduring pregnancy is not associated with an im-proved perinatal outcome. Acta Obstet Gyne-col Scand 1998;77:37-40.107. Jacobsson B, Pernevi P, Chidekel L, Jor-gen Platz-Christensen J. Bacterial vaginosis in
early pregnancy may predispose for preterm
21
www.AJOG.org Obstetrics Reviews
birth and postpartum endometritis. Acta ObstetGynecol Scand 2002;81:1006-10.108. Vogel I, Thorsen P, Hogan VK, Schieve LA,Jacobsson B, Ferre CD. The joint effect of vag-inal Ureaplasma urealyticum and bacterial vagi-nosis on adverse pregnancy outcomes. ActaObstet Gynecol Scand 2006;85:778-85.109. Gravett MG, Nelson HP, DeRouen T,Critchlow C, Eschenbach DA, Holmes KK. In-dependent associations of bacterial vaginosisand Chlamydia trachomatis infection with ad-verse pregnancy outcome. JAMA 1986;256:1899-903.110. Gravett MG, Hummel D, Eschenbach DA,Holmes KK. Preterm labor associated with sub-clinical amniotic fluid infection and with bacterialvaginosis. Obstet Gynecol 1986;67:229-37.111. Newton ER, Piper J, Peairs W. Bacterialvaginosis and intraamniotic infection. Am J Ob-stet Gynecol 1997;176:672-7.112. Martius J, Eschenbach DA. The role ofbacterial vaginosis as a cause of amniotic fluidinfection, chorioamnionitis and prematurity—areview. Arch Gynecol Obstet 1990;247:1-13.113. Goldenberg RL, Culhane JF, Iams JD, Ro-mero R. Epidemiology and causes of pretermbirth. Lancet 2008;371:75-84.114. Macones GA, Parry S, Elkousy M, ClothierB, Ural SH, Strauss JF III. A polymorphism in thepromoter region of TNF and bacterial vaginosis:preliminary evidence of gene-environment inter-action in the etiology of spontaneous pretermbirth. Am J Obstet Gynecol 2004;190:1504-8.115. Gomez LM, Sammel MD, Appleby DH, etal. Evidence of a gene-environment interactionthat predisposes to spontaneous preterm birth:a role for asymptomatic bacterial vaginosis andDNA variants in genes that control the inflam-matory response. Am J Obstet Gynecol 2010;202:386.116. Romero R, Chaiworapongsa T, Kuivani-emi H, Tromp G. Bacterial vaginosis, the inflam-matory response and the risk of preterm birth: arole for genetic epidemiology in the preventionof preterm birth. Am J Obstet Gynecol 2004;190:1509-19.117. Fidel P, Ghezzi F, Romero R, et al. Theeffect of antibiotic therapy on intrauterine infec-tion-induced preterm parturition in rabbits. JMatern Fetal Neonatal Med 2003;14:57-64.118. Cauci S, Guaschino S, De AD, et al. Inter-relationships of interleukin-8 with interleukin-1beta and neutrophils in vaginal fluid of healthyand bacterial vaginosis positive women. MolHum Reprod 2003;9:53-8.119. Donders GG, Vereecken A, Bosmans E,Spitz B. Vaginal cytokines in normal pregnancy.Am J Obstet Gynecol 2003;189:1433-8.120. Gomez R, Romero R, Ghezzi F, Yoon BH,Mazor M, Berry SM. The fetal inflammatory re-sponse syndrome. Am J Obstet Gynecol 1998;179:194-202.121. Gotsch F, Romero R, Kusanovic JP, et al.The fetal inflammatory response syndrome. ClinObstet Gynecol 2007;50:652-83.122. Kim SK, Romero R, Chaiworapongsa T, et
al. Evidence of changes in the immunopheno-type and metabolic characteristics (intracellularreactive oxygen radicals) of fetal, but notmaternal, monocytes and granulocytes in thefetal inflammatory response syndrome. J Peri-nat Med 2009;37:543-52.123. Cardenas I, Means RE, Aldo P, et al. Viralinfection of the placenta leads to fetal inflamma-tion and sensitization to bacterial products pre-disposing to preterm labor. J Immunol 2010;185:1248-57.124. Guise JM, Mahon SM, Aickin M, Helfand M,Peipert JF, Westhoff C. Screening for bacterialvaginosis in pregnancy. Am J Prev Med
001;20:62-72.25. Hutzal CE, Boyle EM, Kenyon SL, et al.
Use of antibiotics for the treatment of pretermparturition and prevention of neonatal morbid-ity: a metaanalysis. Am J Obstet Gynecol 2008;199:620-8.126. Koumans EH, Markowitz LE, Hogan V. In-dications for therapy and treatment recommen-dations for bacterial vaginosis in nonpregnantand pregnant women: a synthesis of data. ClinInfect Dis 2002;35:S152-72.127. Leitich H, Brunbauer M, Bodner-Adler B,Kaider A, Egarter C, Husslein P. Antibiotic treat-ment of bacterial vaginosis in pregnancy: ameta-analysis. Am J Obstet Gynecol 2003;188:752-8.128. McDonald HM, Brocklehurst P, GordonA. Antibiotics for treating bacterial vaginosis inpregnancy. Cochrane Database Syst Rev2007;1:CD000262.129. Okun N, Gronau KA, Hannah ME. Antibi-otics for bacterial vaginosis or Trichomonasvaginalis in pregnancy: a systematic review.Obstet Gynecol 2005;105:857-68.130. Riggs MA, Klebanoff MA. Treatment of vag-inal infections to prevent preterm birth: a meta-analysis. Clin Obstet Gynecol 2004;47:796-807.131. Simcox R, Sin WT, Seed PT, Briley A,Shennan AH. Prophylactic antibiotics for theprevention of preterm birth in women at risk: ameta-analysis. Aust N Z J Obstet Gynaecol2007;47:368-77.132. Swadpanich U, Lumbiganon P, Praser-tcharoensook W, Laopaiboon M. Antenatallower genital tract infection screening andtreatment programs for preventing pretermdelivery. Cochrane Database Syst Rev 2008;2:CD006178.133. Varma R, Gupta JK. Antibiotic treatment ofbacterial vaginosis in pregnancy: multiple meta-analyses and dilemmas in interpretation. Eur JObstet Gynecol Reprod Biol 2006;124:10-4.134. Lamont RF, Jones BM, Mandal D, Hay PE,Sheehan M. The efficacy of vaginal clindamycinfor the treatment of abnormal genital tractflora in pregnancy. Infect Dis Obstet Gynecol2003;11:181-9.135. Liberati A, Altman DG, Tetzlaff J, et al. ThePRISMA statement for reporting systematic re-views and meta-analyses of studies that evalu-ate healthcare interventions: explanation and
elaboration. BMJ 2009;339:b2700.SEPTEMBER 2011 Am
136. Spiegel CA, Amsel R, Holmes KK. Diagno-sis of bacterial vaginosis by direct Gram stain ofvaginal fluid. J Clin Microbiol 1983;18:170-7.137. Nugent RP, Krohn MA, Hillier SL. Reliabilityof diagnosing bacterial vaginosis is improved by astandardized method of gram stain interpretation.J Clin Microbiol 1991;29:297-301.138. Ison CA, Hay PE. Validation of a simplifiedgrading of Gram stained vaginal smears for usein genitourinary medicine clinics. Sex TransmInfect 2002;78:413-5.139. Centre for Reviews and Dissemination.Undertaking systematic reviews of research oneffectiveness. No. 4 (2nd ed). 2001.140. Lamont RF, Khan KS, Beattie B, et al. Thequality of nifedipine studies used to assess to-colytic efficacy: a systematic review. J PerinatMed 2005;33:287-95.141. Lamont RF. A quality assessment tool toevaluate tocolytic studies. BJOG 2006;113(suppl3):96-9.142. Higgins JP, Thompson SG, Deeks JJ, Alt-man DG. Measuring inconsistency in meta-analyses. BMJ 2003;327:557-60.143. Egger M, Davey Smith G, Schneider M,Minder C. Bias in meta-analysis detected by asimple, graphical test. BMJ 1997;315:629-34.144. Altman DG. Confidence intervals for thenumber needed to treat. BMJ 1998;317:1309-12.145. Kiss H, Petricevic L, Husslein P. Prospec-tive randomised controlled trial of an infectionscreening programme to reduce the rate of pre-term delivery. BMJ 2004;329:371.146. Alvi SA, Lamont RF. Pregnancy outcomefollowing the use of clindamycin intravaginalcreams. J Soc Gynecol Invest 1999;6:S94A.147. Workowski KA, Berman S, Centers forDisease Control and Prevention. Sexually trans-mitted diseases treatment guidelines, 2010.MMWR Recomm Rep 2010;59:1-110.148. Barry AL, Thornsberry C, Jones RN. Invitro activity of a new macrolide, A-56268, com-pared with that of roxithromycin, erythromycin,and clindamycin. Antimicrob Agents Che-mother 1987;31:343-5.149. Spiegel CA, Eschenbach DA, Amsel R,Holmes KK. Curved anaerobic bacteria in bac-terial (nonspecific) vaginosis and their responseto antimicrobial therapy. J Infect Dis 1983;148:817-22.150. Young RA, Gonzalez JP, Sorkin EM. Roxi-thromycin: a review of its antibacterial activity,pharmacokinetic properties and clinical effi-cacy. Drugs 1989;37:8-41.151. Spiegel CA. Susceptibility of Mobiluncusspecies to 23 antimicrobial agents and 15 othercompounds. Antimicrob Agents Chemother1987;31:249-52.152. Esterly NB, Furey NL, Flanagan LE. Theeffect of antimicrobial agents on leukocyte che-motaxis. J Invest Dermatol 1978;70:51-5.153. Hand WL, Hand DL, King-Thompson NL.Antibiotic inhibition of the respiratory burst re-sponse in human polymorphonuclear leuko-cytes. Antimicrob Agents Chemother 1990;34:
863-70.erican Journal of Obstetrics & Gynecology 189

t1
Reviews Obstetrics www.AJOG.org
154. Konno S, Asano K, Kurokawa M, Ikeda K,Okamoto K, Adachi M. Antiasthmatic activity ofa macrolide antibiotic, roxithromycin: analysis ofpossible mechanisms in vitro and in vivo. IntArch Allergy Immunol 1994;105:308-16.155. Mikasa K, Kita E, Sawaki M, et al. Theanti-inflammatory effect of erythromycin in zy-mosan-induced peritonitis of mice. J Antimi-crob Chemother 1992;30:339-48.156. Takeshita K, Yamagishi I, Harada M,Otomo S, Nakagawa T, Mizushima Y. Immuno-logical and anti-inflammatory effects of clari-thromycin: inhibition of interleukin 1 productionof murine peritoneal macrophages. Drugs ExpClin Res 1989;15:527-33.157. Rosenstein IJ, Morgan DJ, Sheehan M,Lamont RF, Taylor-Robinson D. Bacterial vagi-nosis in pregnancy: distribution of bacterial spe-cies in different gram-stain categories of thevaginal flora. J Med Microbiol 1996;45:120-6.158. Ugwumadu A, Reid F, Hay P, Manyonda I.Natural history of bacterial vaginosis and inter-mediate flora in pregnancy and effect of oralclindamycin. Obstet Gynecol 2004;104:114-9.159. McDonald HM, O’Loughlin JA, VigneswaranR, Jolley PT, McDonald PJ. Bacterial vaginosis inpregnancy and efficacy of short-course oral met-ronidazole treatment: a randomized controlledtrial. Obstet Gynecol 1994;84:343-8.160. Vermeulen GM, van Zwet AA, Bruinse HW.Changes in the vaginal flora after two percent clin-damycin vaginal cream in women at high risk ofspontaneous preterm birth. BJOG 2001;108:697-700.161. McFarland LV. Antibiotic-associated diar-rhea: epidemiology, trends and treatment. Fu-
ture Microbiol 2008;3:563-78.190 American Journal of Obstetrics & Gynecology
162. Borin MT, Powley GW, Tackwell KR, BattsDH. Absorption of clindamycin after intravaginalapplication of clindamycin phosphate 2% cream.J Antimicrob Chemother 1995;35:833-41.163. Goldstein EJ, Citron DM, Merriam CV,Warren YA, Tyrrell KL, Fernandez HT. In vitroactivities of Garenoxacin (BMS 284756) against108 clinical isolates of Gardnerella vaginalis. An-imicrob Agents Chemother 2002;46:3995-6.64. Xiao JC, Xie LF, Fang SL, et al. Symbiosis
of Mycoplasma hominis in Trichomonas vagina-lis may link metronidazole resistance in vitro.Parasitol Res 2006;100:123-30.165. De Backer E, Dubreuil L, Brauman M, AcarJ, Vaneechoutte M. In vitro activity of secnida-zole against Atopobium vaginae, an anaerobicpathogen involved in bacterial vaginosis. ClinMicrobiol Infect 2010;16:470-2.166. Ferris MJ, Masztal A, Aldridge KE, Forten-berry JD, Fidel PL Jr, Martin DH. Association ofAtopobium vaginae, a recently described met-ronidazole resistant anaerobe, with bacterialvaginosis. BMC Infect Dis 2004;4:5.167. Donders GG, Van Calsteren K, Bellen G, etal. Predictive value for preterm birth of abnormalvaginal flora, bacterial vaginosis and aerobicvaginitis during the first trimester of pregnancy.BJOG 2009;116:1315-24.168. Workowski KA, Berman SM. Centers forDisease Control and Prevention sexually trans-mitted diseases treatment guidelines. Clin InfectDis 2007;44(suppl 3):S73-6.169. Bradshaw CS, Morton AN, Hocking J, etal. High recurrence rates of bacterial vaginosisover the course of 12 months after oral metro-nidazole therapy and factors associated with
recurrence. J Infect Dis 2006;193:1478-86.SEPTEMBER 2011
170. Valkenburg-van den Berg AW, Sprij AJ,Dekker FW, Dorr PJ, Kanhai HH. Associationbetween colonization with Group B Strepto-coccus and preterm delivery: a systematic re-view. Acta Obstet Gynecol Scand 2009;88:958-67.171. Lee SE, Romero R, Kim EC, Yoon BH. Ahigh Nugent score but not a positive culture forgenital mycoplasmas is a risk factor for sponta-neous preterm birth. J Matern Fetal NeonatalMed 2009;22:212-7.172. Romero R, Mazor M, Oyarzun E, Sirtori M,Wu YK, Hobbins JC. Is genital colonization withMycoplasma hominis or Ureaplasma urealyti-cum associated with prematurity/low birthweight? Obstet Gynecol 1989;73:532-6.173. Andrews WW, Klebanoff MA, Thom EA,et al. Midpregnancy genitourinary tract infec-tion with Chlamydia trachomatis: associationwith subsequent preterm delivery in womenwith bacterial vaginosis and Trichomonasvaginalis. Am J Obstet Gynecol 2006;194:493-500.174. Jones NM, Holzman C, Friderici KH, et al.Interplay of cytokine polymorphisms and bacte-rial vaginosis in the etiology of preterm delivery.J Reprod Immunol 2010;87:82-9.175. Lamont RF, Sobel JD, Akins RA, et al. Thevaginal microbiome: new information aboutgenital tract flora using molecular based tech-niques. BJOG 2011;118:533-49.176. Donders G, Bellen G, Rezeberga D. Aero-bic vaginitis in pregnancy. BJOG Jun 14 2011[Epub ahead of print]. doi: 10.1111/j.1471-
0528.2011.03020.x.