Embed Size (px)
Citation preview

Treatment and Prophylaxis Guidelines – Where are we up
to?
Dr Jonathan Sandoe, Consultant Microbiologist, Leeds
Management of infections in the vascular patient

Competing interests
• Paid by Pfizer to deliver a lecture on infections in vascular surgical patients in 2011
• Research funding, sponsorship to attend conferences or deliver lectures from Novartis, Pfizer and Merck Sharp and Dohme, Biomet.

Infections in vascular patients
Aim
To persuade you that guidelines have a role in the management of infections in vascular surgical patients…BUTOnly if used in the correct context and as part of a comprehensive infection service.

Infections in vascular patients
Plan
Part 1 – Treatment guideline updatePart 2 – What do we want from guidelines?Part 3 – Prophylaxis guideline update

Part 1
Treatment guideline update

Guidelines for diagnosis and management of infected vascular grafts…


Guidelines for radiological diagnosis and management of infected (mycotic) aneurysms….



Infections in vascular patients
Where are all the guidelines?

Part 2
What do we want from guidelines?

Infections in vascular patients
The aim of treatment
To cure patients of infection with minimal risk of harm in the most efficient way possible.
Secondary aim…to suppress infection…

Infections in vascular patients
The aim of guidelines
To standardise and optimise the care of vascular patients with infection?

Infections in vascular surgery
The aim of guidelines
• Is standardisation possible in complex infection?
Infections in vascular patients
The aim of guidelines
Can anything be standardised?•Diagnostic criteria•Initial investigations•Microbiological processing•Empirical antimicrobial therapy•Directed antimicrobials•Surgery?

Infections in vascular patients
Guideline criticisms
Too manyConflictingUnhelpfulDifficult to followIgnoredHard to findOut of date…….

IDSA: Antibiotic choice for DFI
Adapted from Lipsky (2004) IDSA guidelines: diabetic foot infection.Clin Infect Dis 39: 885–910
Infections in vascular patients
Guideline criticisms
NICE: AB - Diabetic foot infection (DFI)•NICE are unable to make any recommendations on individual agents•Each hospital should have DFI guidelines.

Infections in vascular patients
Making the task manageable
• Infections can be viewed as “specialty-specific” and “general”
• In the assessment of a vascular surgery inpatient with infection, the differential diagnosis may be broad...

Infections in vascular patients
“Specialty specific” infections
1. Surgical site infection (wound, stump, early graft infection)
2. Vascular graft infection (early/late)3. AV fistula infection4. Mycotic aneurysms5. Diabetic foot infection6. Cellulitis/ulcer infection



8179 Jan 2011692 July 2008
“Hits” on antimicrobial guidelines per month

Infections in vascular patients
Contrasting - situations
Mycotic aneurysm Vascular graft infection
Microbiology monomicrobial polymicrobial
Microbiological diagnosis (Blood culture)
reliable unreliable
Comorbidity IE, IVDU, none DM, PVD, CKD
Prosthetic material absent present
Infections in vascular patients
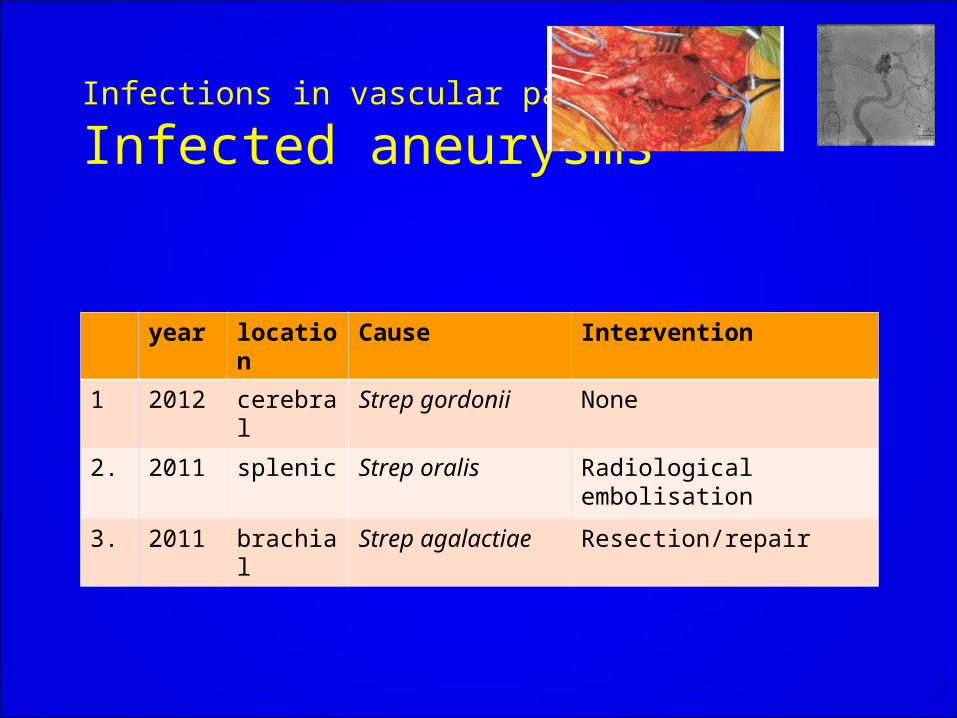
Infected aneurysms
year location Cause Intervention
1 2012 cerebral Strep gordonii None
2. 2011 splenic Strep oralis Radiological embolisation
3. 2011 brachial Strep agalactiae Resection/repair

Vascular graft infection Guideline – “top level recommendations”
• Antimicrobial strategy determined by surgical strategy• Surgical strategy determined by location of graft, patient
choice/suitability for surgery….
• Removal of infected graft and debridement of infected tissue appears to be necessary for cure?

Vascular graft infection
Success of surgical strategy for infection
1. Removal and extra-anatomical bypass2. Removal with replacement with autologous vessel3. Partial removal and replacement4. Endovascular arterial reconstruction5. No surgery

Vascular graft infection
Duration of therapy vs surgical strategy
1. Removal/extra anatomical 6/52 IV2. Removal/ in situ autologous 6/52 IV/po3. Partial removal 6/52 IV + suppression?4. EVAR 6/52 IV + suppression5. No surgery IV + suppression
Vascular graft infection Guideline – Antimicrobial treatment
• Is it appropriate to draw parallels between prosthetic valve endocarditis and vascular graft infection?
• Prolonged (6/52) IV antimicrobials can cure PVE
• Trial data needed

Vascular graft infection
Empirical therapy
1. Vancomycin + piperacillin/tazobactam (appropriate spectrum, low CDI risk, low MRSA colonisation risk)*
2. Vancomycin + ciprofloxacin +metronidazole (penicillin allergic patient)*
(antifungals?)
*Empirical regimen should consider previous microbiology

Part 3
Guidelines for antimicrobial prophylaxis in vascular
(surgery) patients


Infections in vascular patients
Prophylaxis
Peripheral arterial reconstruction (EL 1+)

•Do not use antibiotic prophylaxis routinely for clean non-prosthetic uncomplicated surgery (!)
•DO for all implant surgery
Infections in vascular patients
Prophylaxis

• single dose prophylaxis IV on starting anaesthesia (earlier for operations in which a tourniquet is used).
Infections in vascular patients
Prophylaxis

• No recommendations on choice of agent
• “see local formulary”
Infections in vascular patients
Prophylaxis

Infections in vascular patients
Summary
Guidelines do have a role in the management of infections in vascular surgical patients…BUTOnly if used in the correct context and as part of a comprehensive infection service.
More data are needed – high quality observational studies if trials impractical.