Embed Size (px)
Citation preview

Infant Mental Health Journal, Vol. 18(2) 145–157 (1997)© 1997 Michigan Association for Infant Mental Health CCC 0163-9641/97/020145–13
Treating Infants and Mothers in Psychic Distress: A Mental
Health Program for Infancy
MARIA CORDEIRO
Infancy Unit, Department of Child Psychiatry, Hospital D. Estefânia, Lisboa, Portugal
ABSTRACT: Our purpose is to outline a program of mental health for mothers and infants up to the age of 3.The theoretical background of the program refers to the psychoanalytical genetic point of view developed byFrench and American authors. The therapeutic objectives consist of promoting the infant’s self-development andthe mother’s reflective self-capacity to improve the infant’s resiliency. These objectives aim to have preventivepurposes. The program has clinical, research and training activities and a multidisciplinary staff. The clinicalpopulation is referred by medical services, from families with a middle-low socioeconomic status. With the datacollected during the assessment phase, we establish a diagnosis based on a psychodynamic analysis of thepathological process and the evaluation of the risk and protective factors. Our multidisciplinary approach com-bines individual therapeutic modalities focused on mothers, child or mother–child relationship, with family in-terventions in our Unit or in the community. An evaluation of our intervention based on Parent– InfantRelationship-Global Assessment Scale (PIR-GAS) is presented.
RESUMEN: El propósito es describir un programa de salud mental para madres e infantes hasta la edad de 3años. La base teórica del programa nos refiere a los puntos de vista genéticos sicoanalíticos desarrollados porlos autores franceses y norteamericanos. Los objetivos terapéuticos consisten en promover el desarrollo propiodel infante y la propia capacidad reflexiva de la madre con el fin de mejorar la capacidad del niño para reac-cionar. Estos objetivos apuntan hacia propósitos preventivos. El programa tiene actividades clínicas, de investi-gación y de entrenamiento, así como personal multidisciplinario. La población clínica es referida por losservicios médicos, y proviene de familias que tienen medio o bajo S.E.S. Con la información recogida durantela fase de evaluación, se establece un diagnóstico basado en un análisis sicodinámico del proceso patológico y laevaluación de riesgo y factores de protección. Nuestro aceramiento multidisciplinario combina modalidades ter-apéuticas individuales que se enfocan en las madres, en los niños o en la relación entre madres y niños, y en lasintervenciones de familia que llevamos a cabo en nuestra Unidad o en la comunidad. Se presenta una evaluaciónde la intervención basada en la escale PIR-GAS.
RÉSUMÉ: Notre but est de tracer les grandes lignes d’un programme de Santé Mentale pour Mères et Bébésjusqu’à l’âge de 3 ans. L’arrière-plan théorique du programme fait référence au point de vue psychanalytiquegénétique développé par des auteurs français et américains. Les objectifs thérapeutiques consistent à promou-voir le développement personnel du bébé et la capacité de réflexion qu’a la mère de façon à améliorer l’élasticitédu bébé. Les objectifs sont d’avoir des buts de prévention. Le programme a des activités cliniques, de
145
The Author would like to thank all members of the program’s staff for their collaboration. Data were col-lected by Maria João Nascimento (Nurse), Eduarda Rodrigues, Cristina Marques, and Pedro C. Silva (ChildPsychiatrists). Correspondence should be addressed to the author at Av. Estados Unidas da America, 73-7 Esq.,1700 Lisboa, Portugal.
641_96-302 4/24/97 12:32 PM Page 145 (Black plate)
recherches, et de formation, et une équipe multidisciplinaire. La population clinique est envoyée par des ser-vices médicaux, de familles avec un S.E.S. moyen à bas. Avec les données recueillies durant la phase d’évalua-tion, un diagnostique basé sur une analyse psychodynamique du processus pathologique et sur l’évaluation defacteurs de risque et protecteurs est établi. Notre approche multidisciplinaire combine des modalités thérapeu-tiques individuelles concentrées sur les mères, l’enfant ou la relation mère-enfant, et des interventions familialesdans notre Unité ou dans la communauté. Une évaluation de l’intervention basée sur l’échelle PIR-GAS estprésentée.
ZUSAMMENFASSUNG: Der Zweck dieser Arbeit ist es, eine Einrichtung für die seelische Gesundheit vonMüttern und deren Kinder bis zum 3. Lebensjahr zu umreißen. Der theoretische Hintergrund unserer Arbeit istdie psychoanalytische, kausale Sichtweise, wie sie von französischen und amerikanischen Autoren entwickeltwurde. Die therapeutischen Ziele sind die Unterstützung der Selbstentwicklungskräfte des Kleinkindes und dermütterlichen Selbstreflexion, um dadurch eine harmonische Entwicklung des Kleinkindes zu ermöglichen.Unser Ziel ist es dadurch präventiv zu arbeiten. Unsere Einrichtung unfaßt Behandlung, Forschung und Unter-richt und wird von einem multidisziplinärem Team betreut. Die Kranken werden von medizinischen Einrichtun-gen zugewiesen, die Familien kommen aus der Mittel- und Unterschicht. Auf Grund der Informationen, die wirin der Untersuchungsphase sammeln erstellen wir eine Diagnose, die sich auf die psychodynamische Analysedes pathologischen Prozeß und einer Einschätzung der schützenden und der gefährdenden Faktoren stützt.Unser multidispziplinärer Ansatz kombiniert sowohl individualtherapeutische Angebote für Mütter, Kinder, oderdie Mutter-Kind Beziehung, als auch Familientherapie entweder in unserer Einrichtung, oder am Wohnort. EineEvaluation unserer Behandlung, die sich auf die Verwendung der PIR-GAS (PIR-GAS 5 Parent-Infant-Rating:General Adaptation Score 5 Eltern-Kind-Beurteilung: Wertung der Anpassungsleistung) Skala bezieht, wirdpräsentiert.
146 Infant Mental Health Journal
Benefitting from the impact of the 1st World Congress of Infant Mental Health on theMental Health officials in our country,1 in 1983 we founded an out-patient clinic in Lis-bon oriented toward the diagnosis and treatment of infant mental health disorders andguidance for the mother–child relationship. The importance of continuity and quality ofcaregiving relationships for the child’s emotional and cognitive development was high-lighted by Spitz’s (1968) pioneering studies on analytic depression and by Bowlby’s(1982) later conclusions on maternal deprivation.
As Emde puts it “in thinking about early experience, we must think about caregivingrelationship” and the “facilitation of infant development is virtually synonymous with fa-cilitation of the caregiving relationship” (1989, p. 33).
Since then, studies on mother – child early interaction and on the infant’s competen-cies have expanded remarkably. The way in which the mother and infant behave to-gether during interactive sequences, promoting infant’s learning about socialization(Stern, 1991) the role of affective signalling in the orientation of interactive experi-
1The Congress was held in 1980 in Estoril, near Lisbon. The author was one of the members of the LocalCommittee.
641_96-302 4/24/97 12:33 PM Page 146 (Black plate)

ences (Emde, 1983), as well as the infant’s capacities to organize mother’s behaviour(Brazelton, 1982; Stern, 1991) were some of the first and the most important advancesin this field. The separation – individualization process described by Mahler (1979) hasbeen another important contribution. It allowed a better understanding of the mecha-nism of internalization of the sense of the self and perceiving the way the image of theself becomes separated from others and from the external world. In spite of the manyauthors’ criticism (Bowlby, 1982; Stern, 1985) and the fact that some of her conceptsneed to be reviewed, Mahler’s (1979) framework has proved to be helpful for under-standing the development of psychopathology. Also Greenspan’s (Greenspan &Lieberman, 1989) structural theory, describing the different stages of ego develop-ment, according to the specific developmental tasks, organizing properties and mean-ing has been important for clinical practice.
Another theoretical milestone is Bowlby’s (1982) attachment theory. The attach-ment behavior is considered of central importance for the establishment ofmother – child relationship, as well as for infant socio-emotional development. Basedon the subsequent studies of Ainsworth (1971, 1982), the attachment theory has beenclarified and simplified and it is now seen as one of the most important frameworks forunderstanding psychic functioning.
Further theoretical advances came with Lebovici’s (1989) formulations on transgen-erational transmission of conflicts and on the role of the “bébé imaginaire” in mother–child relationships. These ideas support Fraiberg’s conclusions (1980) about the mother’s transference upon the baby of her infantile objectal relationships. The func-tion of transference/countertransference shifts in producing a therapeutic change dur-ing mother–child consultation, as Lebovici (1983) has formulated, have proved to be useful in our clinical practice.
More recently, Cramer (Cramer & Palacio, 1993) has expanded these ideas, by usingbrief mother–child psychotherapy, which confirmed the importance of parental projec-tions on triggering off infant’s symptoms.
In general terms, these were the main ideas that guided our work and provided theframework for the setting up of our Unit.
OBJECTIVES
From a genetic point of view and in general terms, infant mental health programs haveprimary and secondary preventive purposes. Nevertheless, epidemiological studies aboutthe lasting effects of identified risk factors on the individual’s mental health have pro-duced inconclusive results. Furthermore, research based on symptoms and behavioral pat-terns have not revealed consistent continuities in mental health disorders. Therefore,concepts such as individual vulnerability and resiliency (Demos, 1989) seem more ap-propriate to understand the psychopathological process of the risk, rather than the simplepresence of risk factors (Sameroff & Leiffer, 1983).
From our clinical experience, we consider that individual vulnerability and resiliencyare determined by psychic mechanisms linked to the development of the self. As weknow, the early organization of the self depends on the quality and continuity of the expe-rience of the infant with the caregiver. By interpreting the baby’s manifestations and act-ing according to them, by reducing tension, by focusing attention and sharing affective
M. Cordeiro 147
641_96-302 4/24/97 12:33 PM Page 147 (Black plate)
states, the mother transforms the infant’s fragmented perceptions and sensations intoemotional experiences that progressively become self-experiences. Also, the baby, bygenerating strong emotional experiences in the caregiver, is an active partner in the rela-tionship. Not only do his innate capacities influence the maternal interactive behavior, buthis presence reactivates the mother’s unconscious fantasies, which may affect dramati-cally the quality of the interaction.
Therefore, the mother’s past relationships, mainly with her own mother (“the mother-hood constellation,” Stern, 1996) as well as life events, losses, marital relationships, andfamily support influence the quality of mother–child relationships and, consequently, theself-organization of the baby.
Returning to the concepts of resiliency and vulnerability, schematically, we could saythat:
148 Infant Mental Health Journal
Therefore, the continuity of mental pathology cannot be seen in phenomenologicalterms. Rather it is based on the self-incapacity to deal with the anxiety and the conflictslinked either to developmental crisis (oedipal phase, adolescence, etc.) or to the stressprovoked by life events.
With these ideas in mind, our objectives consist of:1. providing the babies with good and continuous emotional experiences, promoting
self-development;2. helping mothers to improve their insight and their capacity to develop the reflec-
tive self-function (Fonagy, Steele, Steele, Moran, & Higgitt, 1991) to understand andadapt to their babies’ needs; and
3. stimulating and reinforcing the protective factors in the family and social environ-ment, when necessary.
We believe that this therapeutic model, promoting the infant’s self-development and in-dividual resiliency can be considered as a preventive intervention in mental health.
641_96-302 4/24/97 12:33 PM Page 148 (Black plate)

THE INFANCY UNIT
Location
Our Unit is located in a small three-floor building with an open space. Although be-longing to the Department of Child Psychiatry of a Paediatric Hospital, the Infancy Unit(“UPI”) is away from the hospital and designed to provide a warm and comfortable re-ception for mothers and infants aged up to 3, who are in distress.
Staff
The staff includes 3 child psychiatrists, one of them a psychoanalyst, 2 clinical psy-chologists, 1 psychiatric nurse and 1 social worker, all of whom have had training and ex-perience in child psychiatry and child psychotherapy. Some members of the team haveworked together in the infant mental health area since the unit was founded and othershave received training in the unit. Education professionals interested in infancy regularlycollaborate with us on a volunteer basis. All staff participate in clinical, research, training,and planning activities.
Clinical Activity
In our clinical activity, we intend to evaluate in each case all of the factors involved inthe infant’s disturbance including parental, child, and environmental issues and their dy-namic relationships. Further, we establish therapeutic modalities adapted the requirementsor risk within each specific situation. Our multidisciplinary approach combines individualtherapeutic modalities focused on mother, child, or mother–child relationships, with fam-ily interventions in our unit or in the community (family home, nursery, etc).
We also provide information and counseling to the institutions’ staff concerned with in-fant health and welfare (courts, social services, nurseries, etc).
Research
Although our activity has developed essentially in a clinical setting, research has beenalways considered as a necessary component to improve our understanding of the psy-chopathological process and therapeutic intervention.
Interactive studies. The aim of our initial studies was to identify the risk and the pro-tective factors in our populations to establish intervention strategies. We defined themother–child interaction as a central issue in our work and training. Systematic videoand direct observations of interaction has been, therefore, the object of methodologicalanalysis in regular staff meetings. Previously, we had established parameters based on lit-erature studies (Greenspan & Lieberman, 1980; Massie & Campbell, 1983; Anders, 1989).
We compared the quality of the interactions with the infant’s mental and developmentalcondition and grouped it in three different types: adapted, insufficiently adapted, and in-adequate. The “adapted” interactions were more often present in situations of better prog-nosis and were considered as a potential protective factor for infant development(Cordeiro & Fornelos, 1990). Specific interactive patterns were described in situationswith language delays (Cordeiro, 1990) and infant’s anorexia (Cordeiro & coll., 1990).They were characterized by striking contradictions between the mother’s interactive be-havior and speech reflected in maternal hostility toward the child. More recently, we have
M. Cordeiro 149
641_96-302 4/24/97 12:33 PM Page 149 (Black plate)
studied maternal representations in infant anorexia, in which the mother’s low self-esteemappears to be an important issue (Cordeiro et al., 1993).
Diagnostic classification studies. As the Infancy Unit’s activity has been developing,we deal progressively with a larger range of syndromes and chronic conditions, with dif-ferent prognoses, such as autism and pervasive developmental disorders (DSM-IV) or parent–child disorders secondary to organic conditions. This situation influenced us tochoose a diagnostic classification for infancy, helping us in our diagnostic and therapeuticevaluations or in our case studies.
We have been coordinating our work on infant diagnoses with the Zero to Three Task-Force for Diagnostic Classification in Infancy in the United States and the newly devel-oped European group. Progressively, we introduced the use of Diagnostic Classification(DC: 0–3) (Zero to Three, 1994) in our work and established contacts in Europe withcolleagues from France, Austria, and Germany. We are now using, systematically, Axis Iand II of DC: 0–3 classification, as well as the Parent– Infant Relationship Global As-sessment Scale (PIR-GAS). The comparative studies of psychological profiles assessedby the Griffith scales provide additional information and are complementary of our diag-nostic studies, namely for relating and communicating disorders.
Training
Our training program oriented to the permanent staff and trainees includes weeklyteam discussions on diagnostic classification and interaction, case presentations, and su-pervision. A journal club session is scheduled monthly.
Moreover, we have developed a 1-year postgraduate training program focused on clinicalpractice for psychologists, medical doctors in child psychiatric training, and professionalsin education. Other professionals receiving short-term training include paediatricians, childneurologists, and nurses in psychiatric training. Students of faculties of psychology have a1-year undergraduate training program included in their curriculum (2 students per year).We organize symposia or workshops and also participate in meetings of other medical spe-cialties to promote wider scientific exchanges. Half-day meetings with outside profession-als working in the field or special speakers are usually organized 2–3 times a year.Furthermore, we have organized a video-library and a library with sponsorship from privategroups to provide more extensive scientific and training support.
POPULATION AND CLINICAL PROCEDURE
Population
The Infancy Unit is a program directed toward children of up to 3 years of age andtheir caregivers (parents or others). The large majority of children are referred to our pro-gram by general practitioners or pediatricians. Over 100 new cases are referred every yearand the reasons for referral are multiple. Simultaneously, we have developed a liaison ac-tivity in three infant wards providing pediatric services. Most families attending the pro-gram are organized, with a middle to low socioeconomic status, and live in Lisbon orsuburban areas of Lisbon.
In contrast, problems such as extreme poverty, isolated or adolescent mother, and drugaddiction are more often addressed by socially oriented programs. These families, lacking
150 Infant Mental Health Journal
641_96-302 4/24/97 12:33 PM Page 150 (Black plate)
the ability to organize the child’s care and to use health services on a regular basis, re-quire very concrete support which is often beyond our capacities.
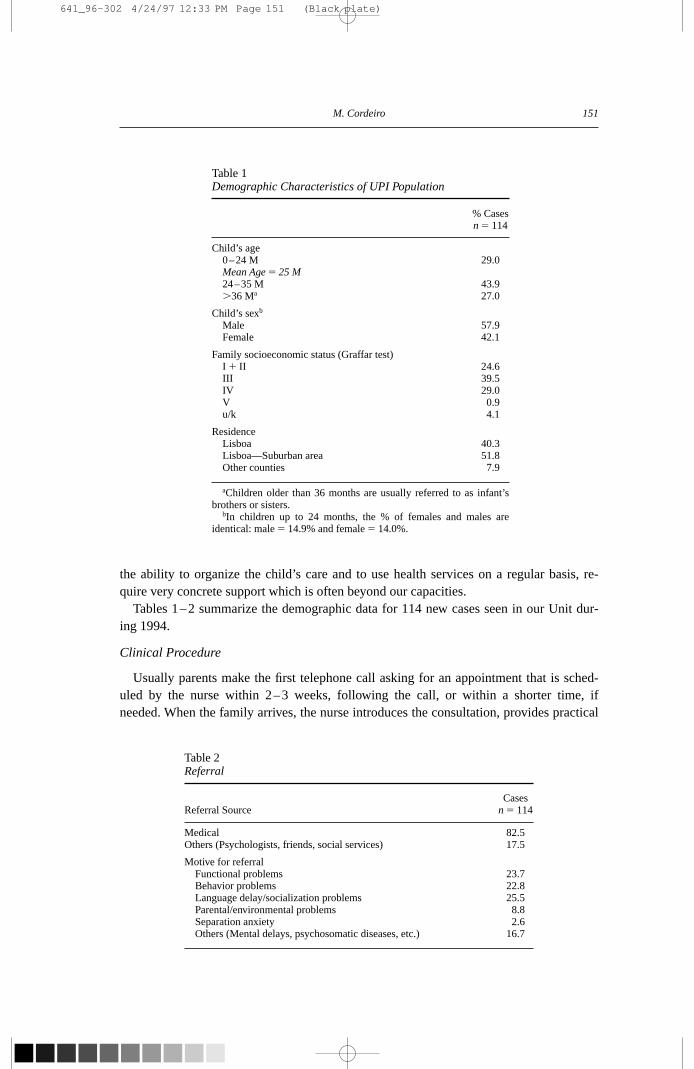
Tables 1–2 summarize the demographic data for 114 new cases seen in our Unit dur-ing 1994.
Clinical Procedure
Usually parents make the first telephone call asking for an appointment that is sched-uled by the nurse within 2–3 weeks, following the call, or within a shorter time, ifneeded. When the family arrives, the nurse introduces the consultation, provides practical
M. Cordeiro 151
Table 1Demographic Characteristics of UPI Population
% Casesn 5 114
Child’s age0–24 M 29.0Mean Age 5 25 M24–35 M 43.9.36 Ma 27.0
Child’s sexb
Male 57.9Female 42.1
Family socioeconomic status (Graffar test)I 1 II 24.6III 39.5IV 29.0V 0.9u/k 4.1
ResidenceLisboa 40.3Lisboa—Suburban area 51.8Other counties 7.9
aChildren older than 36 months are usually referred to as infant’sbrothers or sisters.
bIn children up to 24 months, the % of females and males areidentical: male 5 14.9% and female 5 14.0%.
Table 2Referral
CasesReferral Source n 5 114
Medical 82.5Others (Psychologists, friends, social services) 17.5
Motive for referralFunctional problems 23.7Behavior problems 22.8Language delay/socialization problems 25.5Parental/environmental problems 8.8Separation anxiety 2.6Others (Mental delays, psychosomatic diseases, etc.) 16.7
641_96-302 4/24/97 12:33 PM Page 151 (Black plate)

information to the parents about our procedures, and attempts to evaluate their motiva-tion. Information about the child and the parents, family structure and support, parents’educational background and profession is collected at that time. We consider this initialcontact with our nurse, which leads to the assessment phase, to be an important step in es-tablishing a rather informal climate and leading to positive collaboration between parentsand the team.
The assessment phase includes a semidirected interview with the parents and baby’s di-rect and videotaped observation, which is coordinated by a child psychiatrist. Often a de-velopmental evaluation with tests by a clinical psychologist is necessary. The entireassessment phase can take up to 2–3 sessions of 90 min each. We collect data regardingthe parents, the child and the parent–child communication. During the interview, we areparticularly attentive to the parents’ complaints and their perceptions of the baby’s activ-ity and functioning, the quality and intensity of their involvement with the baby, the in-fant’s role in father’s/mother’s representations and the intrafamilial relationships. We askquestions about the symptoms, the child’s medical and developmental history, the infant’stemperament, the child’s life events, the parents’ life events influencing the parent–childrelationship, the baby’s daily life, and caregiving modalities. The parental behavior to-ward the child during the interview, as well as the child’s behavior are recorded by an ob-server inside the room and a free-play session with a short separation sequence isvideotaped.
The data collected during the assessment phase by the nurse, the child psychiatrist, theinteractional observer (usually a trainee), and possibly the psychologist, as well as theirclinical impressions, are discussed in clinical meetings with all staff. In each case, we es-tablish a diagnosis based on the psychodynamic analysis of the pathological process, theevaluation of the risk and the protective factors involved for either the parents or infants,and the capacity of each element to respond to treatment (parents’ personality vs. infant’scharacteristics).
Our multidisciplinary assessment and discussion are important issues in our work. Asall staff feel involved in the process, it facilitates the communication and strengthens itscohesion. It provokes richer and deeper understandings of the cases and reduces the ef-fects of countertransferential feelings influencing the therapeutic decision-makingprocess. Among the 114 cases assessed during 1994, 17 cases (15%) were referred toother programs. A specific intervention in the program was proposed for 97 cases (85%).
152 Infant Mental Health Journal
Table 3Distribution of Therapeutic Intervention (Duration)
Cases %No. Sessions n 5 97
Short interventions,3 sessions/3 months 5.1
Long-term interventions.10 sessions and/or 6 months 61.9
Periodical evaluation 6.2
Drop-out cases 26.8
641_96-302 4/24/97 12:33 PM Page 152 (Black plate)
These figures show a high specificity from referral sources. Among the latter, 26 cases(26.81%) abandoned the program during or just after the assessment. Of the cases thatdropped out, 7 cases (30.7%) came from organized families, 14 (49.9%) came from disor-ganized families, and 5 (19.3%) children did not live with their biological parents.
Therapeutic intervention lasting more than 6 months and including 10–12 sessions aswell as long-lasting psychotherapeutic interventions were the most frequent (Table 3).
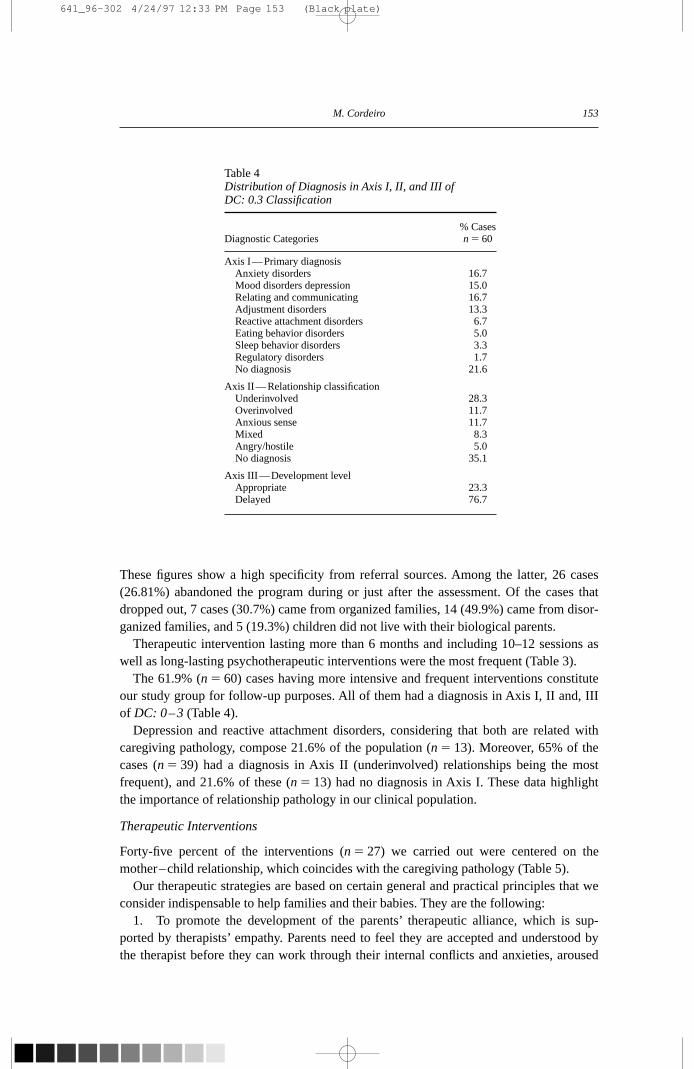
The 61.9% (n 5 60) cases having more intensive and frequent interventions constituteour study group for follow-up purposes. All of them had a diagnosis in Axis I, II and, IIIof DC: 0–3 (Table 4).
Depression and reactive attachment disorders, considering that both are related withcaregiving pathology, compose 21.6% of the population (n 5 13). Moreover, 65% of thecases (n 5 39) had a diagnosis in Axis II (underinvolved) relationships being the mostfrequent), and 21.6% of these (n 5 13) had no diagnosis in Axis I. These data highlightthe importance of relationship pathology in our clinical population.
Therapeutic Interventions
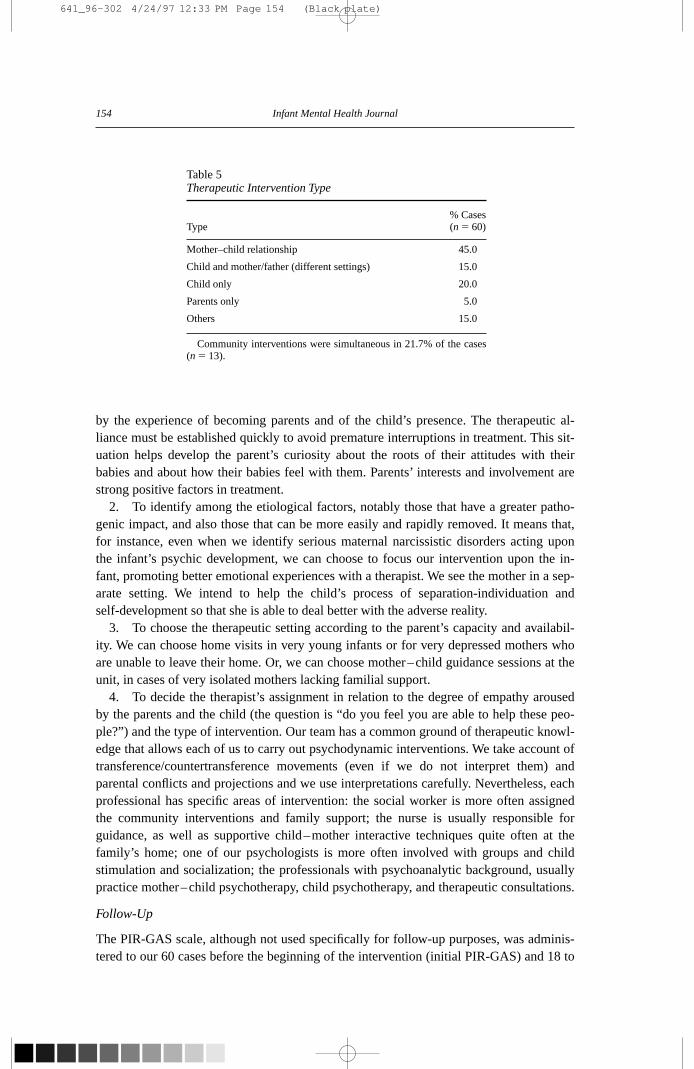
Forty-five percent of the interventions (n 5 27) we carried out were centered on themother–child relationship, which coincides with the caregiving pathology (Table 5).
Our therapeutic strategies are based on certain general and practical principles that weconsider indispensable to help families and their babies. They are the following:
1. To promote the development of the parents’ therapeutic alliance, which is sup-ported by therapists’ empathy. Parents need to feel they are accepted and understood bythe therapist before they can work through their internal conflicts and anxieties, aroused
M. Cordeiro 153
Table 4Distribution of Diagnosis in Axis I, II, and III of DC: 0.3 Classification
% CasesDiagnostic Categories n 5 60
Axis I—Primary diagnosisAnxiety disorders 16.7Mood disorders depression 15.0Relating and communicating 16.7Adjustment disorders 13.3Reactive attachment disorders 6.7Eating behavior disorders 5.0Sleep behavior disorders 3.3Regulatory disorders 1.7No diagnosis 21.6
Axis II—Relationship classificationUnderinvolved 28.3Overinvolved 11.7Anxious sense 11.7Mixed 8.3Angry/hostile 5.0No diagnosis 35.1
Axis III—Development levelAppropriate 23.3Delayed 76.7
641_96-302 4/24/97 12:33 PM Page 153 (Black plate)
by the experience of becoming parents and of the child’s presence. The therapeutic al-liance must be established quickly to avoid premature interruptions in treatment. This sit-uation helps develop the parent’s curiosity about the roots of their attitudes with theirbabies and about how their babies feel with them. Parents’ interests and involvement arestrong positive factors in treatment.
2. To identify among the etiological factors, notably those that have a greater patho-genic impact, and also those that can be more easily and rapidly removed. It means that,for instance, even when we identify serious maternal narcissistic disorders acting uponthe infant’s psychic development, we can choose to focus our intervention upon the in-fant, promoting better emotional experiences with a therapist. We see the mother in a sep-arate setting. We intend to help the child’s process of separation-individuation andself-development so that she is able to deal better with the adverse reality.
3. To choose the therapeutic setting according to the parent’s capacity and availabil-ity. We can choose home visits in very young infants or for very depressed mothers whoare unable to leave their home. Or, we can choose mother–child guidance sessions at theunit, in cases of very isolated mothers lacking familial support.
4. To decide the therapist’s assignment in relation to the degree of empathy arousedby the parents and the child (the question is “do you feel you are able to help these peo-ple?”) and the type of intervention. Our team has a common ground of therapeutic knowl-edge that allows each of us to carry out psychodynamic interventions. We take account oftransference/countertransference movements (even if we do not interpret them) andparental conflicts and projections and we use interpretations carefully. Nevertheless, eachprofessional has specific areas of intervention: the social worker is more often assignedthe community interventions and family support; the nurse is usually responsible forguidance, as well as supportive child–mother interactive techniques quite often at thefamily’s home; one of our psychologists is more often involved with groups and childstimulation and socialization; the professionals with psychoanalytic background, usuallypractice mother–child psychotherapy, child psychotherapy, and therapeutic consultations.
Follow-Up
The PIR-GAS scale, although not used specifically for follow-up purposes, was adminis-tered to our 60 cases before the beginning of the intervention (initial PIR-GAS) and 18 to
154 Infant Mental Health Journal
Table 5Therapeutic Intervention Type
% CasesType (n 5 60)
Mother–child relationship 45.0
Child and mother/father (different settings) 15.0
Child only 20.0
Parents only 5.0
Others 15.0
Community interventions were simultaneous in 21.7% of the cases(n 5 13).
641_96-302 4/24/97 12:33 PM Page 154 (Black plate)
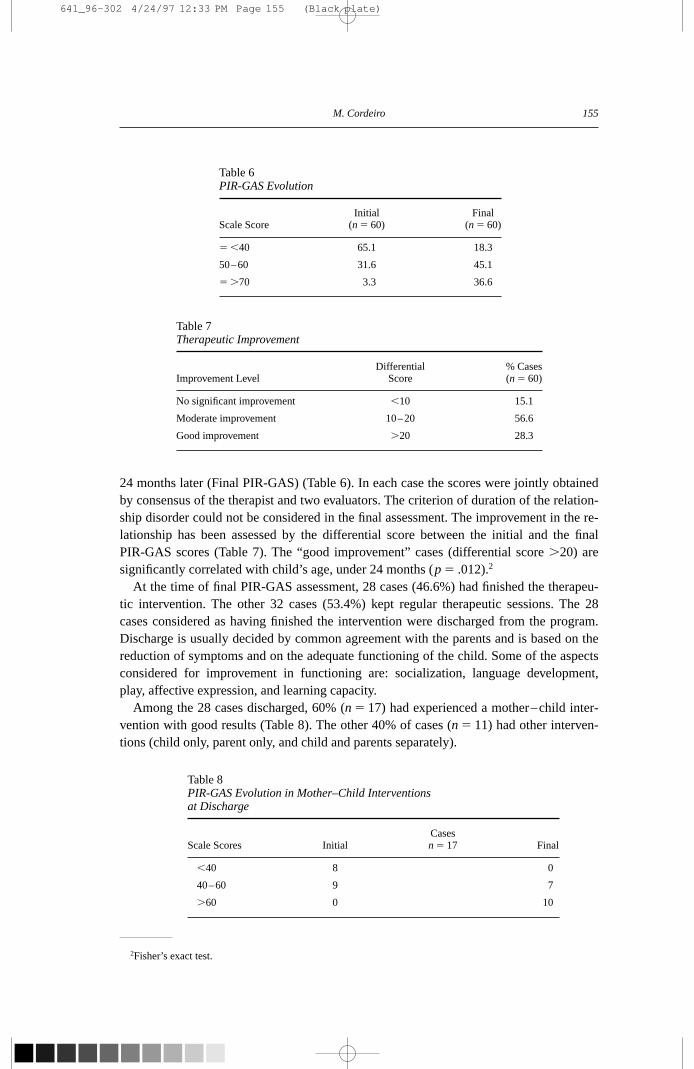
24 months later (Final PIR-GAS) (Table 6). In each case the scores were jointly obtainedby consensus of the therapist and two evaluators. The criterion of duration of the relation-ship disorder could not be considered in the final assessment. The improvement in the re-lationship has been assessed by the differential score between the initial and the finalPIR-GAS scores (Table 7). The “good improvement” cases (differential score .20) aresignificantly correlated with child’s age, under 24 months (p 5 .012).2
At the time of final PIR-GAS assessment, 28 cases (46.6%) had finished the therapeu-tic intervention. The other 32 cases (53.4%) kept regular therapeutic sessions. The 28cases considered as having finished the intervention were discharged from the program.Discharge is usually decided by common agreement with the parents and is based on thereduction of symptoms and on the adequate functioning of the child. Some of the aspectsconsidered for improvement in functioning are: socialization, language development,play, affective expression, and learning capacity.
Among the 28 cases discharged, 60% (n 5 17) had experienced a mother–child inter-vention with good results (Table 8). The other 40% of cases (n 5 11) had other interven-tions (child only, parent only, and child and parents separately).
M. Cordeiro 155
Table 6PIR-GAS Evolution
Initial FinalScale Score (n 5 60) (n 5 60)
5 ,40 65.1 18.3
50–60 31.6 45.1
5 .70 3.3 36.6
Table 7Therapeutic Improvement
Differential % CasesImprovement Level Score (n 5 60)
No significant improvement ,10 15.1
Moderate improvement 10–20 56.6
Good improvement .20 28.3
2Fisher’s exact test.
Table 8PIR-GAS Evolution in Mother–Child Interventions at Discharge
CasesScale Scores Initial n 5 17 Final
,40 8 0
40–60 9 7
.60 0 10
641_96-302 4/24/97 12:33 PM Page 155 (Black plate)

CONCLUSIONS
Our data have demonstrated the importance of the mother–child relationship for thepsychic development of the child and the efficacy of early interventions. Consistent withthese ideas, mother–child interventions were shown to have impressively good results forour discharged cases.
We believe that we fulfilled our initial objectives to help infants and toddlers have moresatisfactory and adequate relationship experiences and to help mothers/fathers to betterunderstand and accept their babies.
Nevertheless, we feel that the moment has come for some of our efforts placed on diag-nostic issues need to be shifted to an evaluation of therapeutic change and longer termoutcome studies. We intend to develop a Global Adaptive Functioning scale (DSM-IV)(American Psychiatric Association, 1995) in the future, adapted to infants and toddlers.
The variety of activities and clinical conditions we deal with provide a stimulating andrewarding experience. Such diversity helps decrease monotony at work, keeps the teaminvolved, widens our scientific knowledge and exchanges, and improves our clinicalskills.
REFERENCES
Ainsworth, M. D. S., Bell, S., & Stayton, D. J. (1971). Individual differences in strange situation behaviour ofone year olds. In H. R. Schaffer (Ed.), The Origins of Human Social Relations (pp. 17–57). London: Acad-emic Press.
Ainsworth, M. (1982). Attachment. Retrospect and prospect. In C. M. Parker & J. Stevenson-Hinde (Eds.), ThePlace of Attachment in Human Behaviour (pp. 30–31). London: Tavistock Publications.
American Psychiatric Association. (1995). Diagnostic and Statistical Manual of Mental Disorders—DSM-IV.International version (4th ed.). Washington, DC: Author.
Anders, T. (1989). Clinical syndromes and their assessment. In A. Sameroff & R. Emde (Eds.), RelationshipDisturbances in Early Childhood (pp. 125–144). New York: Basic Books.
Bowlby, J. (1982). Attachment behaviour. In J. Bowlby (Ed.), Attachment and Loss (Vol. 1, 2nd ed.). (pp.221–230). London: Hogart Press.
Brazelton, B. (1982). Assessment techniques for enhancing infant development. In J. Call, E. Galenson,R. Tyson (Eds.), Frontiers of Infant Psychiatry (pp. 347–362). New York: Basic Books.
Cramer, B., & Palacio, E. F. (1993). La Pratique des Psychotherapies Mères—Bébé. Paris: PUF.
Cordeiro, M. Gonçalves, Rodrigues, E., & Caldeira da Silva, P. (1990). Interaction et psychopathologie précoce.Anoréxie du nourisson. Annales Medico-Psychologiques 148, 824–829.
Cordeiro, M. Gonçalves (1990). Le dévelopement de la communication verbale dans l’interaction mère-infant. Devenir 1, 34–45.
Cordeiro, M. Gonçalves, Rodrigues, E., & Caldeira da Silva, P. (1993). L’anorexie du nourisson. Une étude clin-ique. Devenir 5, 35–50.
Cordeiro, M. Gonçalves, & Fornelos, M. (1990). Modalités d’interaction précoce et developpement infantil. Annales Medico-Psychologiques 148, 818–823.
Demos, E. V. (1989). Resiliency in infancy. In T. F. Dugan & R. Coles (Eds.), The Child in Our Times. Studiesin the Development of Resiliency. (pp. 3–22). New York: Bruner/Mazel, Inc.
Emde, R., & Source, J. F. (1983). The rewards of infancy: Emotional availability and maternal referencing. In J. Call, E. Galenson, & R. Tyson (Eds.), Frontiers of Infant Psychiatry (pp. 17–30). New York: Basic BookPublishers.
Emde, R. (1989). Infant’s relationship experience: developmental and affective aspects. In A. Sameroff & R. Emde (Eds.), Relationship Disturbances in Early Childhood (pp. 33–51). New York: Basic Books.
Fonagy, P., Steele, M., Steele, H., Moran G., & Higgitt, A. (1991). The capacity for understanding mental states:
156 Infant Mental Health Journal
641_96-302 4/24/97 12:33 PM Page 156 (Black plate)
The reflective self/parent in mother and child and its significance for security of attachment. Infant MentalHealth Journal, 12, 201–218.
Fraiberg, S., Shapiro, V., & Cherniss, D. (1980). Treatment modalities. In S. Fraiberg & L. Fraiberg (Es.), Clini-cal Studies in Infant Mental Health: First Year of Life (pp. 49–77). New York: Basic Books.
Fraiberg, S., Adelson, E., & Shapiro, V. (1980). Ghosts in nursery: A psychoanalytic approach to the problemsof impaired infant–mothers. In S. Fraiberg & L. Fraiberg (Eds.), Clinical Studies in Infant Mental Health:First Year of Life (pp. 164–196). New York: Basic Books.
Greenspan, J., & Lieberman, A. (1980). Infants, mothers and their interaction: A quantitative clinical approachto developmental assessment. In S. Greenspan & G. Polock (Eds.), The Course of Life: PsychoanalyticContributions towards Understanding Personality Development Vol. I: Infancy and Early Childhood (pp.503–560). Washington, DC: Government Printing Office.
Lebovici, S. (1983). Le Nourisson, La Mère et e Psychanaliste (pp. 239–362). Paris: Le Centurion.
Lebovici, S. (1989). Les liens intergerationels (transmission, conflits). Les interactions fantasmatiques. In S. Lebovici & F. Weil-Halpern (Eds.), Psychopathologie du Bébé (pp. 141–146). Paris: Le Centurion.
Mahler, M. (1979). The selected papers of Magareth Mahler, Vol. II: Separation-Individuation (pp. 77 –98).New York: Jason Aronson.
Massie, H., & Campbell, K. (1983). The Massie–Campbell Scale of mother– infant attachment indicators dur-ing stress (AIDS scale). In J. Call, E. Gallenson, & E. Tyon (Eds.), Frontiers of Infant Psychiatry(pp. 394–412). New York: Basic Books.
Sameroff, A., & Seiffer, R. (1983). Familial risk and child competence. Child Development 5, 1254–1268.
Spitz, R. (1968). De La Naissance à la Parole. La Première Année de la Vie (pp. 206–225). Paris: PUF.
Stern, D. (1985). The interpersonal world of the infant (pp. 3–344). New York: Basic Books.
Stern, D. (1991). Maternal representations: A clinical and subjective phenomenological view. Infant MentalHealth Journal 12, 171–186.
Stern, D. (1996). Theories of intervention. Plenary Session, WAIMH Sixth World Congress, Tampere.
Zero to Three. (1994). Diagnostic classification of mental health and development disorders of infancy andearly childhood. (DC: 0–3) Arlington, VA: National Center for Clinical Infant Programs. Author.
M. Cordeiro 157
641_96-302 4/24/97 12:33 PM Page 157 (Black plate)