Embed Size (px)
Citation preview

18.08.2012 Chemist+Druggist 15
CPD Zone update
chemistanddruggist.co.uk/update
this module covers:
● The incidence, prevalence and symptoms of endometriosis
● How endometriosis is diagnosed and pain is managed
● The hormonal and surgical options available for treatment
● The answers to common questions on fertility
Dr Sharmila Chauhan PhD MRPharmS
Endometriosis affects 10 to 15 per cent of all menstruating women aged 25 to 44 years. The condition can range from mild to severe and can be both physically and emotionally debilitating. Currently around 1.5 million women in the UK suffer from endometriosis and a significant number remain undiagnosed.1
Endometriosis is characterised by the presence of endometrial-like cells outside the uterus. These are most commonly found inside the pelvis, around the ovaries and fallopian tubes, on the ligaments, intestines, bladder, vagina and the rectum. In rarer cases, these ‘misplaced’ cells also grown into the muscle layer of the uterus (adenomyosis), the skin, eyes, spine, lungs and the brain.
The precise cause is unclear. Research has suggested a number of contributing factors, including endometrial cells travelling back up the fallopian tubes and onto the ovaries during menstruation, endometrial cells replacing other cells in tissues outside the uterus, transportation of endometrial cells to other parts of the body via the blood or lymphatic system, and immune dysfunction.
Endometriosis is an inherited condition and common in first-degree relatives of women with the condition. It is most common in menstruating women and generally becomes remissive after the menopause. It is more common in women who have: ● their first baby after age 30 years● never had a baby● short menstrual cycles (less than 27 days)● certain structural abnormalities of the uterus.
The condition is less common in women who have had several pregnancies, use low-dose oral contraceptives, or who exercise.
symptomsLike their uterine counterparts, endometrial cells outside the uterus are also under
Treating endometriosis
UPDATEmodule 1623
August» Women's health month
● Menstrual problems August 4
● Endometriosis August 18
● Lupus August 25
the influence of sex hormones during menstruation, and will undergo proliferation and swelling under the influence of oestrogen before a period. However, since there is nowhere for them to be shed, they accumulate and cause inflammation, pain and, eventually, the formation of scar tissue.
Bands of fibrous tissue (adhesions) may form between the structures in the abdominal cavity, causing neighbouring organs to stick together, leading to further complications.2,3
Typical symptoms include:2,3 ● severe dysmenorrhoea ● pain in lower abdomen between menstrual
cycles (this may not be as painful as period pain but may be more constant)● painful sexual intercourse● menstrual irregularities● bowel or bladder symptoms (eg need to urinate frequently, pain during urination, constipation, rectal bleeding during menstruation).
Adhesions on the ovaries can form a cyst that bleeds into itself each month, often called a ‘chocolate cyst’. In severe cases of endometriosis, the adhesions may block the fallopian tubes, impairing fertility. Infertility has also been reported in women with mild ▶
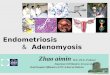
SPL
the organs inside a woman's abdomen. Possible sites where endometriosis can develop are indicated in blue
Abdominal wall
Intestines
Peritoneum
Appendix
Fallopian tubes and ovaries
Uterus
Cervix
Bladder
Rectum
Vulva

16 Chemist+Druggist 18.08.2012
CPD Zone update CPD Zone update
if inserted during laparoscopic surgery, can reduce the recurrence of dysmenorrhea.
Androgens (eg danazol) act through an inhibition of the midcycle follicle-stimulating hormone (FSH) and luteinising hormone (LH) surges as well as prevention of steroidogenesis in the corpus luteum.
Although studies show danazol is as eff ective as the newer agents, its adverse eff ects reduce its acceptability. These include acne, oily skin, weight gain, deepening of the voice, and facial hirsutism. It also has a number of side eff ects related to low oestrogen levels: hot fl ushes, emotional lability, vaginal dryness, and reversible breast atrophy. The usual dose is 200 to 800mg daily in up to four divided doses, adjusted to achieve amenorrhoea, usually for three to six months. These can bring on an ‘artifi cial menopause’ as they reduce oestrogen and progesterone production.
GnRH analogues (eg buserelin, goserelin,
4
cases of the disease but the mechanism by which this occurs is not understood. Between 25 and 50 per cent of women who are infertile have endometriosis.2,3
Endometriosis has a number of psychological eff ects and women with the condition may report depression, isolation and anxiety.
DiagnosisDiagnosis of endometriosis cannot be made on symptoms alone, and in many women can be delayed by up to 12 years. This is because of a lack of awareness among women, lack of specialists, the asymptomatic nature of the condition and reluctance of women to ask for help until the condition is severe.
The diagnosis of endometriosis is all too often a consequence of a diff erent medical investigation, for example, during investigation of fertility issues.1 Improved awareness of the condition together with provision of resources to enable diagnosis may help to improve prognosis of women with the condition.
Tips for your CPD entry on treating endometriosis
Reflect What are the main symptoms of endometriosis? What are the adverse eff ects associated with GnRH analogues? How does endometriosis aff ect fertility?
Plan This article discusses endometriosis and includes information about causes, symptoms and diagnosis. It also describes the hormonal and surgical treatments available and answers common questions that patients with endometriosis might have about fertility.
Act Read the article and the suggested reading below then take the 5 Minute Test. Update subscribers can then access their answers and a pre-fi lled CPD logsheet.read more about endometriosis on the Patient uK website http://tinyurl.com/endometriosis11 Find out about the advice you could give to patients who are suff ering from long term pain on the Nhs Choices websitehttp://tinyurl.com/endometriosis12 research self-help organisations and websites for women who suff er from endometriosis. Find out about local groups and print out any useful information leafl ets.Consider carrying out training with your pharmacy staff so that women who prefer to talk to a female or older or younger person can be made to feel more at ease.
Evaluate Are you now confi dent in your knowledge of the symptoms and treatment of endometriosis? Could you and your staff confi dently give advice to patients?
Diagnosis requires specialist investigation. Currently the gold standard is laparoscopy, which allows the pelvis to be visually inspected and the size and location of adhesions in the abdominal cavity to be assessed.
treatmentManagement of endometriosis currently includes symptomatic treatment, hormonal intervention, and surgery.
First-line treatment usually includes non-steroidal anti-infl ammatory drugs (NSAID), such as ibuprofen, naproxen, mefenamic acid, or diclofenac. These are usually prescribed to women who are experiencing a lot of pain, those who do not wish to use hormonal treatments, and those who are awaiting referral from their GP to a specialist. However, the Royal College of Obstetricians and Gynaecologists (RCOG) states “that although NSAIDs may be eff ective in endometriosis-associated pain, there are too few randomised controlled trials to assess their eff ectiveness”.3
Patients who cannot take NSAIDs (eg those with stomach ulcers or asthma) can be prescribed paracetamol, and studies suggest regular use of the drug may be more eff ective than as-required use. In patients in whom adequate pain relief is not achieved, codeine may be added to paracetamol and/or an NSAID.
Hormone therapyHormonal treatments are used to interfere with oestrogen production and/or activity at its receptors, thereby shrinking the adhesion size. These treatments can also be used to treat the pain and bleeding disorders associated with endometriosis.
Combined oral contraceptives (COCs) are considered the fi rst-line hormonal treatment, and may be taken continuously without a break, or in a tricycling (taking three packs without a break) regimen to control endometriosis. Women taking a COC may report benefi cial eff ects such as lighter and less painful periods. Other symptoms such as painful sex and pain in the pelvic area may also improve.
Progesterone agents act by decidualisation and atrophy of the endometrium. In studies, medroxyprogesterone has been shown to be eff ective in pain suppression. Adverse eff ects of this type of drug include weight gain, fl uid retention, depression, and breakthrough bleeding.
Long-acting progesterones can be used in patients with compliance issues and also in women who are uncomfortable with a daily tablet intake. They may be more acceptable in patients who are familiar with depot or intrauterine devices for contraceptive use.
Women should be reassured that long-acting devices are eff ective and studies show that the levonorgestrel intrauterine system (LNG-IUS) can reduce endometriosis-associated pain and,
Patient questions on endometriosis
1. Will i be able to have a baby? The majority (60 to 70 per cent) of women with endometriosis have no problems getting pregnant. If a woman wants conceive in the future, she should discuss this with her doctor, since this will play a role in the management of the condition. Pharmacological treatment for endometriosis should be avoided for women who are trying to conceive.3
2. What are the options if i want to have a baby and have diffi culty conceiving?Data on the benefi ts of intrauterine insemination (IUI) in women with endometriosis are unclear, although IVF can be considered. Pregnancy rates, however, are lower in women with endometriosis than those with tubal infertility.3
3. Will having a baby ‘cure’ my endometriosis? Pregnancy is not a ‘cure’ for endometriosis, although some women may experience temporary benefi t while pregnant. In most cases, symptoms return after giving birth and the menstrual cycle resumes.1
4. Can i use any alternative medicines? Systemic reviews indicate that a variety of alternative medications have been shown to relieve dysmenorrhoea, including: high frequency TENS, acupuncture, vitamin B1 and magnesium. One randomised controlled trial provided evidence that vitamin E may relieve primary dysmenorrhoea and reduce blood loss. The effi cacy of these treatments in endometriosis-associated dysmenorrhoea is unclear.

CPD Zone update
18.08.2012 Chemist+Druggist 17
CPD Zone update
1. Endometriosis is characterised by the presence of endometrial-like cells outside the uterus. True or false?2. Adenomyosis is where endometrial cells appear in the skin, eyes, lungs, spine or brain. True or false?3. Between 25 and 50 per cent of infertile women have endometriosis. True or false?4. Evidence suggests that endometriosis is not an inherited condition. True or false?5. Endometriosis generally worsens after the menopause. True or false?6. Women who have long menstrual cycles have an increased risk of endometriosis. True or false?7. Endometriosis is less common in women
who have had several pregnancies. True or false?8. The first-line treatment of endometriosis usually includes NSAIDs. True or false?9. Side effects of danzol include acne, weight gain, voice deepening and facial hirsutism. True or false?10. Endometriosis is less likely to reoccur after a pregnancy. True or false?
Get a CPD log sheet for this moduleGet a CPD log sheet for your portfolio when you successfully complete the 5 Minute Test online.
Enrol for Update 2012 for only £32+VAT. Sign up at http://www.chemistanddruggist.co.uk/update or by calling 0207 921 8425.
Take the 5 Minute Test
5 minute test
■ Sign up to take the 5 Minute Test and get your answers marked online: chemistanddruggist.co.uk/update
nafarelin, leuprorelin, and triptorelin) inhibit pituitary gonadotrophin release. Preparations are taken as a nasal spray or injection. Goserelin and leuprorelin are the most commonly used agonists and have been shown in studies to reduce pain associated with endometriosis.
Reports suggest that as many as 85 to 100 per cent of women experience pain suppression following GnRH therapy and that these benefits may persist for between six to 12 months after treatment cessation. Research also shows GnRH treatment can also relieve the pain and bleeding associated with extrapelvic distant endometriosis.
Adverse effects of GnRH agonists include hot flushes, vaginal dryness, reduced sex drive, headaches, reduced bone density, insomnia and amenorrhoea, some of which disappear on cessation. Pharmacists should remind patients that they may experience flare up in symptoms during the first few days of treatment.
Manufacturers recommend a single course of six months duration, although some specialists may prescribe a repeated or extended course. There is limited data regarding the safety and efficacy of this approach. Alternatives include using a three-month course or repeated shorter courses. The latter may offer sustained beneficial effect combined with lower impact on bone mineral density and fewer hypo-oestrogenic adverse effects.
There is debate as to whether oestrogen/progesterone "add-back" therapy should be used to prevent osteoporosis and hypo-oestrogenic symptoms experienced by women receiving GnRH therapy for endometriosis. Low-dose hormone replacement therapy (HRT) has been shown to prevent loss in bone density and to relieve vasomotor symptoms without compromising the efficacy of GnRH regimens; these data suggest that inclusion may be beneficial for many women.
Surgical treatmentThe RCOG guidelines3 outline the ideal treatment of endometriosis as diagnosis
followed by surgical removal of adhesions. There are three types of surgery:
● Conservative – reproductive potential is maintained● Semiconservative – reproductive ability is diminished but ovarian function is retained● Radical – when the uterus and ovaries are completely removed.
Surgery usually includes removal of adhesions and correction of related anatomical distortions. The former are ablated using either laser energy or electrosurgical techniques.
Laparoscopic uterine nerve ablation (LUNA) involves the destruction of a small segment of
For training and CPD for pharmacists and pharmacy staff
»chemistanddruggist.co.uk/cpd
ligament that carries nerve fibres within the pelvis. However, it has not been shown to be efficacious and therefore is not advised for this patient group.
When deciding on the type of surgery, the patient’s age, desire for children and their current quality of life should all be considered.Dr Sharmila Chauhan is a pharmacist and medical writer with a PhD in clinical pharmacology
Further information and references are available online at http://www.chemistanddruggist.co.uk/update