Embed Size (px)
Citation preview

Treating Diabetes To Lower
Cardiovascular Disease Risk
Anne Peters, MD
Professor, USC Keck School of Medicine
Director, USC Clinical Diabetes Programs

Disclosure of Financial Relationships—2015
Consultantship
Abbott Diabetes Care
Amgen
BD, Biodel
Janssen, Lexicon, Lilly
Medscape, Merck
NovoNordisk
Sanofi, Takeda
FDA
Speakers Bureau
Janssen
Research Funding
Janssen
Medtronic Foundation

Gregg EW et al. N Engl J Med 2014;370:1514-1523
Share:
Preventive care for adults with diabetes has improved substantially in recent decades. We examined trends in the incidence of
diabetes-related complications in the United States from 1990 through 2010.
We used data from the National Health Interview Survey, the National Hospital Discharge Survey, the U.S. Renal Data System,
and the U.S. National Vital Statistics System to compare the incidences of lower-extremity amputation, end-stage renal disease,
acute myocardial infarction, stroke, and death from hyperglycemic crisis between 1990 and 2010, with age standardized to the
U.S. population in the year 2000.
Rates of all five complications declined between 1990 and 2010, with the largest relative declines in acute myocardial infarction
(−67.8%; 95% confidence interval [CI], −76.2 to −59.3) and death from hyperglycemic crisis (−64.4%; 95% CI, −68.0 to −60.9),
followed by stroke and amputations, which each declined by approximately half (−52.7% and −51.4%, respectively); the smallest
decline was in end-stage renal disease (−28.3%; 95% CI, −34.6 to −21.6). The greatest absolute decline was in the number of
cases of acute myocardial infarction (95.6 fewer cases per 10,000 persons; 95% CI, 76.6 to 114.6), and the smallest absolute
decline was in the number of deaths from hyperglycemic crisis (−2.7; 95% CI, −2.4 to −3.0). Rate reductions were larger among
adults with diabetes than among adults without diabetes, leading to a reduction in the relative risk of complications associated
with diabetes. When expressed as rates for the overall population, in which a change in prevalence also affects complication
rates, there was a decline in rates of acute myocardial infarction and death from hyperglycemic crisis (2.7 and 0.1 fewer cases
per 10,000, respectively) but not in rates of amputation, stroke, or end-stage renal disease.
Rates of diabetes-related complications have declined substantially in the past two decades, but a large burden of disease
persists because of the continued increase in the prevalence of diabetes. (Funded by the Centers for Disease Control and
Prevention.)
ORIGINAL ARTICLE
Changes in Diabetes-Related Complications in the United States, 1990–2010Edward W. Gregg, Ph.D., Yanfeng Li, M.D., Jing Wang, M.D., Nilka Rios Burrows, M.P.H., Mohammed K. Ali, M.B., Ch.B., Deborah Rolka, M.S.,
Desmond E. Williams, M.D., Ph.D., and Linda Geiss, M.A.
N Engl J Med 2014; 370:1514-1523 April 17, 2014 DOI: 10.1056/NEJMoa1310799
Twenty-one years ago, the Diabetes Control and Complications Trial (DCCT) showed that intensive glycemic control could
reduce the microvascular complications of type 1 diabetes mellitus. Subsequent studies showed that macrovascular and
microvascular complications could be substantially reduced with tight control of glucose levels, blood pressure, and lipid levels in
adults with type 2 diabetes. Collectively, these studies focused attention on diabetes as a public health problem, with a course
that could be altered by a combination of changes in clinical care (e.g., intensive management of risk factors), the health system
(e.g., organization of care), health promotion (e.g., support for patients in modifying lifestyle), and society (e.g., tobacco-control
policies). These studies were followed by steady improvements in diabetes care, self-management behaviors, and risk-factor
control and by the dissemination of new, effective pharmacologic approaches and medical procedures, such as statin use and
coronary revascularization. Given these important trends, we assembled data on four sentinel indicators of diabetes-related
Abstract
Article
1
2-5
6-8
8-10
NEJM — http://www.nejm.org/doi/full/10.1056/NEJMoa1310799?viewT...
1 of 8 4/25/14, 10:05 PM

LDL Cholesterol Targets in Diabetes
Residual Risk of CVD
? Role of other lipid and non-lipid factors
Risk Attributable
to LDL-C
60 80 100 120 140 160 180 200 220
LDL Cholesterol (mg/dl)
Clin
ical E
ven
t R
ate
4S
CARE
HPS
LIPID
CARDS
Post CABG
ASCOT
PROVE IT

Aggregate Endpoint 1997 2007
Any diabetes related endpoint RRR: 12% 9%
P: 0.029 0.040
Microvascular disease RRR: 25% 24%
P: 0.009 0.001
Myocardial infarction RRR: 16% 15%
P: 0.052 0.014
All-cause mortality RRR: 6% 13%
P: 0.44 0.007
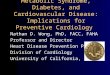
UKPDS: “Legacy Effect” of Insulin/Sulfonylurea
Therapy
RRR = Relative Risk Reduction P = Log Rank
Holman RR, et al. New England Journal of Medicine 2008; 359:1577-1589
After median 8.8 years post-trial followup

UKPDS: “Legacy Effect” of Insulin/Sulfonylurea
vs Metformin Therapy
Holman RR, et al. New England Journal of Medicine 2008; 359:1577-1589

Ray KK, et al. Lancet. 2009;373:1765-1772.
Meta-Analysis of Glycemic Control Trials
and Coronary Heart Disease

Why haven’t trials shown CHD risk reduction?
• Possible reasons that individual trials failed to
show a beneficial effect on CHD
– Event rates were lower than expected
– Differences in glycemic control were not large enough
– The intervention or observation period was too short
– Need to start intervention earlier in natural history of
the disease
Mazzone T. Lancet. 2009. 23;373:1737-1738.

Management of Hyperglycemia in
Type 2 Diabetes, 2015:
A Patient-Centered Approach
Update to a Position Statement of the American Diabetes Association (ADA)
and the European Association for the Study of Diabetes (EASD)
Diabetes Care 2015;38:140–149
Diabetologia 2015;10.1077/s00125-014-3460-0

The ADA/EASD Position Statement on Management of
Hyperglycemia in Type 2 Diabetes
ADA EASD
Richard M. Bergenstal MDInt’l Diabetes Center, Minneapolis, MN
John B. Buse MD, PhDUniversity of North Carolina, Chapel Hill, NC
Anne L. Peters MDUniv. of Southern California, Los Angeles, CA
Richard Wender MDThomas Jefferson University, Philadelphia, PA
Silvio E. Inzucchi MD (co-chair)
Yale University, New Haven, CT
Michaela Diamant MD, PhDVU University, Amsterdam, The Netherlands
Ele Ferrannini MDUniversity of Pisa, Pisa, Italy
Michael Nauck MDDiabeteszentrum, Bad Lauterberg, Germany
Apostolos Tsapas MD, PhDAristotle University, Thessaloniki, Greece
David R. Matthews MD, DphilOxford University, Oxford, UK

1. Patient-Centered Approach“...providing care that is respectful of and responsive to individual patient preferences, needs, and values -
ensuring that patient values guide all clinical decisions.”
• Gauge patient’s preferred level of involvement.
• Explore, where possible, therapeutic choices. Consider using decision aids.
• Shared Decision Making – a collaborative process between patient and clinician, using best available evidence and taking into account the patient’s preferences and values
• Final decisions regarding lifestyle choices ultimately lie with the patient.
Diabetes Care 2012;35:1364–1379; Diabetologia 2012;55:1577–1596
ADA-EASD Position Statement Update: Management of Hyperglycemia in T2DM, 2015

Impact of Intensive Therapy for Diabetes:
Summary of Major Clinical Trials
Study Microvasc CVD Mortality
UKPDS
DCCT /
EDIC*
ACCORD
ADVANCE
VADT
Long Term Follow-up
Initial Trial
* in T1DM
Kendall DM, Bergenstal RM. © International Diabetes Center 2009UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998;352:854. Holman RR et al. N Engl J Med. 2008;359:1577. DCCT Research Group. N Engl J Med 1993;329;977.Nathan DM et al. N Engl J Med. 2005;353:2643. Gerstein HC et al. N Engl J Med. 2008;358:2545.Patel A et al. N Engl J Med 2008;358:2560. Duckworth W et al. N Engl J Med 2009;360:129. (erratum: Moritz T. N Engl J Med 2009;361:1024)

Lessons from Accord
Severe Hypoglycemia and Mortality Risk
ACCORD ADVANCE VADT
Severe Hypo Intensive Standard Intensive Standard Intensive Standard
(%/ year) 3.1% 1.1% 0.7% 0.4% 12.0% 4.0%
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
Intensive
Standard
1.3%
1.0%
2.8%
4.9%
Annual mortality
Bonds et al. BMJ 2010;340:b4909

Severe Hypoglycemia in ACCORD
• “Patients with type 2 diabetes who experience
symptomatic, severe hypoglycaemia are at
increased risk of death, regardless of the intensity of
glucose control.”
• “The increased risk of death seen in the ACCORD
trial among participants in the intensive glycaemia
control arm cannot be attributed to the increased
rate of severe hypoglycaemia in intensive arm
participants.”
Bonds et al. BMJ 2010;340:b4909

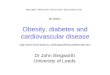
3. ANTI-HYPERGLYCEMIC THERAPY
• Glycemic targets
- HbA1c < 7.0% (mean PG 150-160 mg/dl [8.3-8.9 mmol/l])
- Pre-prandial PG <130 mg/dl (7.2 mmol/l)
- Post-prandial PG <180 mg/dl (10.0 mmol/l)
- Individualization is key:
Tighter targets (6.0 - 6.5%) - younger, healthier
Looser targets (7.5 - 8.0%+) - older, comorbidities, hypoglycemia prone, etc.
- Avoidance of hypoglycemia
PG = plasma glucose
ADA-EASD Position Statement Update: Management of Hyperglycemia in T2DM, 2015
Diabetes Care 2012;35:1364–1379; Diabetologia 2012;55:1577–1596

more
stringent
less
stringent
Patient attitude and
expected treatment efforts highly motivated, adherent,
excellent self-care capacities
less motivated, non-adherent,
poor self-care capacities
Risks potentially associated
with hypoglycemia and
other drug adverse effects
low high
Disease durationnewly diagnosed long-standing
Life expectancylong short
Important comorbiditiesabsent severefew / mild
Established vascular
complications absent severefew / mild
Readily available limited
Usually not
modifiable
Potentially
modifiable
HbA1c7%
PATIENT / DISEASE FEATURES
Approach to the managementof hyperglycemia
Resources and support
system
Figure 1. Modulation of the intensiveness of glucose lowering therapy in T2DM
Diabetes Care 2015;38:140-149; Diabetologia 2015;10.1077/s00125-014-3460-0

peripheralglucose uptake
hepatic glucose production
pancreatic insulinsecretion
pancreatic glucagonsecretion
gutcarbohydratedelivery &absorption
incretineffect
HYPERGLYCEMIA
?
Adapted from: Inzucchi SE, Sherwin RS in: Cecil Medicine 2011
Multiple, Complex Pathophysiological Abnormalities in T2DM
_
_
+renal glucose excretion

peripheralglucose uptake
hepatic glucose production
pancreatic insulinsecretion
pancreatic glucagonsecretion
gutcarbohydratedelivery &absorption
incretineffect
HYPERGLYCEMIA
?
Adapted from: Inzucchi SE, Sherwin RS in: Cecil Medicine 2011
Multiple, Complex Pathophysiological Abnormalities in T2DM
_
_
+renal glucose excretion
DA agonists
T Z D sMetformin
S U sGlinides
DPP-4 inhibitors
GLP-1Ragonists
A G I s
Amylinmimetics
Insulin
Bile acidsequestrants

Healthy eating, weight control, increased physical activity & diabetes education
Metforminhigh
low risk
neutral/loss
GI / lactic acidosis
low
If HbA1c target not achieved after ~3 months of monotherapy, proceed to 2-drug combination (order not meant to denoteany specific preference - choice dependent on a variety of patient- & disease-specific factors):
Metformin+
Metformin+
Metformin+
Metformin+
Metformin+
high
low risk
gain
edema,HF, fxs
low
Thiazolidine-dione
intermediate
low risk
neutral
rare
high
DPP-4 inhibitor
highest
high risk
gain
hypoglycemia
variable
Insulin (basal)
Metformin+
Metformin+
Metformin+
Metformin+
Metformin+
Basal Insulin +
Sulfonylurea
+
TZD
DPP-4-i
GLP-1-RA
Insulin§
or
or
or
or
Thiazolidine-dione
+SU
DPP-4-i
GLP-1-RA
Insulin§
TZD
DPP-4-ior
or
or GLP-1-RA
high
low risk
loss
GI
high
GLP-1 receptoragonist
Sulfonylurea
high
moderate risk
gain
hypoglycemia
low
SGLT2 inhibitor
intermediate
low risk
loss
GU, dehydration
high
SU
TZD
Insulin§
GLP-1 receptoragonist
+
SGLT-2 Inhibitor
+SU
TZD
Insulin§
Metformin+
Metformin+
or
or
or
or
SGLT2-i
or
or
or
SGLT2-i
Mono-therapy
Efficacy*
Hypo risk
Weight
Side effects
Costs
Dualtherapy†
Efficacy*
Hypo risk
Weight
Side effects
Costs
Tripletherapy
or
or
DPP-4 Inhibitor
+SU
TZD
Insulin§
SGLT2-i
or
or
or
SGLT2-i
or
DPP-4-i
If HbA1c target not achieved after ~3 months of dual therapy, proceed to 3-drug combination (order not meant to denoteany specific preference - choice dependent on a variety of patient- & disease-specific factors):
If HbA1c target not achieved after ~3 months of triple therapy and patient (1) on oral combination, move to injectables, (2) on GLP-1 RA, addbasal insulin, or (3) on optimally titrated basal insulin, add GLP-1-RA or mealtime insulin. In refractory patients consider adding TZD or SGLT2-i:
Metformin+
Combinationinjectabletherapy‡
GLP-1-RAMealtime Insulin
Insulin (basal)
+
Figure 2. Anti-hyperglycemic therapy in T2DM: General recommendations Diabetes Care 2015;38:140-149; Diabetologia 2015;10.1077/s00125-014-3460-0

Healthy eating, weight control, increased physical activity & diabetes education
Metforminhigh
low risk
neutral/loss
GI / lactic acidosis
low
If HbA1c target not achieved after ~3 months of monotherapy, proceed to 2-drug combination (order not meant to denoteany specific preference - choice dependent on a variety of patient- & disease-specific factors):
Metformin+
Metformin+
Metformin+
Metformin+
Metformin+
high
low risk
gain
edema,HF, fxs
low
Thiazolidine-dione
intermediate
low risk
neutral
rare
high
DPP-4 inhibitor
highest
high risk
gain
hypoglycemia
variable
Insulin (basal)
Metformin+
Metformin+
Metformin+
Metformin+
Metformin+
Basal Insulin +
Sulfonylurea
+
TZD
DPP-4-i
GLP-1-RA
Insulin§
or
or
or
or
Thiazolidine-dione
+SU
DPP-4-i
GLP-1-RA
Insulin§
TZD
DPP-4-ior
or
or GLP-1-RA
high
low risk
loss
GI
high
GLP-1 receptoragonist
Sulfonylurea
high
moderate risk
gain
hypoglycemia
low
SGLT2 inhibitor
intermediate
low risk
loss
GU, dehydration
high
SU
TZD
Insulin§
GLP-1 receptoragonist
+
SGLT-2 Inhibitor
+SU
TZD
Insulin§
Metformin+
Metformin+
or
or
or
or
SGLT2-i
or
or
or
SGLT2-i
Mono-therapy
Efficacy*
Hypo risk
Weight
Side effects
Costs
Dualtherapy†
Efficacy*
Hypo risk
Weight
Side effects
Costs
Tripletherapy
or
or
DPP-4 Inhibitor
+SU
TZD
Insulin§
SGLT2-i
or
or
or
SGLT2-i
or
DPP-4-i
If HbA1c target not achieved after ~3 months of dual therapy, proceed to 3-drug combination (order not meant to denoteany specific preference - choice dependent on a variety of patient- & disease-specific factors):
If HbA1c target not achieved after ~3 months of triple therapy and patient (1) on oral combination, move to injectables, (2) on GLP-1 RA, addbasal insulin, or (3) on optimally titrated basal insulin, add GLP-1-RA or mealtime insulin. In refractory patients consider adding TZD or SGLT2-i:
Metformin+
Combinationinjectabletherapy‡
GLP-1-RAMealtime Insulin
Insulin (basal)
+
Figure 2. Anti-hyperglycemic therapy in T2DM: General recommendations Diabetes Care 2015;38:140-149; Diabetologia 2015;10.1077/s00125-014-3460-0

Healthy eating, weight control, increased physical activity & diabetes education
Metforminhigh
low risk
neutral/loss
GI / lactic acidosis
low
If HbA1c target not achieved after ~3 months of monotherapy, proceed to 2-drug combination (order not meant to denoteany specific preference - choice dependent on a variety of patient- & disease-specific factors):
Metformin+
Metformin+
Metformin+
Metformin+
Metformin+
high
low risk
gain
edema,HF, fxs
low
Thiazolidine-dione
intermediate
low risk
neutral
rare
high
DPP-4 inhibitor
highest
high risk
gain
hypoglycemia
variable
Insulin (basal)
Metformin+
Metformin+
Metformin+
Metformin+
Metformin+
Basal Insulin +
Sulfonylurea
+
TZD
DPP-4-i
GLP-1-RA
Insulin§
or
or
or
or
Thiazolidine-dione
+SU
DPP-4-i
GLP-1-RA
Insulin§
TZD
DPP-4-ior
or
or GLP-1-RA
high
low risk
loss
GI
high
GLP-1 receptoragonist
Sulfonylurea
high
moderate risk
gain
hypoglycemia
low
SGLT2 inhibitor
intermediate
low risk
loss
GU, dehydration
high
SU
TZD
Insulin§
GLP-1 receptoragonist
+
SGLT-2 Inhibitor
+SU
TZD
Insulin§
Metformin+
Metformin+
or
or
or
or
SGLT2-i
or
or
or
SGLT2-i
Mono-therapy
Efficacy*
Hypo risk
Weight
Side effects
Costs
Dualtherapy†
Efficacy*
Hypo risk
Weight
Side effects
Costs
Tripletherapy
or
or
DPP-4 Inhibitor
+SU
TZD
Insulin§
SGLT2-i
or
or
or
SGLT2-i
or
DPP-4-i
If HbA1c target not achieved after ~3 months of dual therapy, proceed to 3-drug combination (order not meant to denoteany specific preference - choice dependent on a variety of patient- & disease-specific factors):
If HbA1c target not achieved after ~3 months of triple therapy and patient (1) on oral combination, move to injectables, (2) on GLP-1 RA, addbasal insulin, or (3) on optimally titrated basal insulin, add GLP-1-RA or mealtime insulin. In refractory patients consider adding TZD or SGLT2-i:
Metformin+
Combinationinjectabletherapy‡
GLP-1-RAMealtime InsulinFigure 2. Anti-hyperglycemic therapy in T2DM: General recommendations Diabetes Care 2015;38:140-149; Diabetologia 2015;10.1077/s00125-014-3460-0
Insulin (basal)
+

Healthy eating, weight control, increased physical activity & diabetes education
Metforminhigh
low risk
neutral/loss
GI / lactic acidosis
low
If HbA1c target not achieved after ~3 months of monotherapy, proceed to 2-drug combination (order not meant to denoteany specific preference - choice dependent on a variety of patient- & disease-specific factors):
Metformin+
Metformin+
Metformin+
Metformin+
Metformin+
high
low risk
gain
edema,HF, fxs
low
Thiazolidine-dione
intermediate
low risk
neutral
rare
high
DPP-4 inhibitor
highest
high risk
gain
hypoglycemia
variable
Insulin (basal)
Metformin+
Metformin+
Metformin+
Metformin+
Metformin+
Basal Insulin +
Sulfonylurea
+
TZD
DPP-4-i
GLP-1-RA
Insulin§
or
or
or
or
Thiazolidine-dione
+SU
DPP-4-i
GLP-1-RA
Insulin§
TZD
DPP-4-ior
or
or GLP-1-RA
high
low risk
loss
GI
high
GLP-1 receptoragonist
Sulfonylurea
high
moderate risk
gain
hypoglycemia
low
SGLT2 inhibitor
intermediate
low risk
loss
GU, dehydration
high
SU
TZD
Insulin§
GLP-1 receptoragonist
+
SGLT-2 Inhibitor
+SU
TZD
Insulin§
Metformin+
Metformin+
or
or
or
or
SGLT2-i
or
or
or
SGLT2-i
Mono-therapy
Efficacy*
Hypo risk
Weight
Side effects
Costs
Dualtherapy†
Efficacy*
Hypo risk
Weight
Side effects
Costs
Tripletherapy
or
or
DPP-4 Inhibitor
+SU
TZD
Insulin§
SGLT2-i
or
or
or
SGLT2-i
or
DPP-4-i
If HbA1c target not achieved after ~3 months of dual therapy, proceed to 3-drug combination (order not meant to denoteany specific preference - choice dependent on a variety of patient- & disease-specific factors):
If HbA1c target not achieved after ~3 months of triple therapy and patient (1) on oral combination, move to injectables, (2) on GLP-1 RA, addbasal insulin, or (3) on optimally titrated basal insulin, add GLP-1-RA or mealtime insulin. In refractory patients consider adding TZD or SGLT2-i:
Metformin+
Combinationinjectabletherapy‡
GLP-1-RAMealtime Insulin
Insulin (basal)
+
Diabetes Care 2015;38:140-149; Diabetologia 2015;10.1077/s00125-014-3460-0

Healthy eating, weight control, increased physical activity & diabetes education
Metforminhigh
low risk
neutral/loss
GI / lactic acidosis
low
If HbA1c target not achieved after ~3 months of monotherapy, proceed to 2-drug combination (order not meant to denoteany specific preference - choice dependent on a variety of patient- & disease-specific factors):
Metformin+
Metformin+
Metformin+
Metformin+
Metformin+
high
low risk
gain
edema,HF, fxs
low
Thiazolidine-dione
intermediate
low risk
neutral
rare
high
DPP-4 inhibitor
highest
high risk
gain
hypoglycemia
variable
Insulin (basal)
Metformin+
Metformin+
Metformin+
Metformin+
Metformin+
Basal Insulin +
Sulfonylurea
+
TZD
DPP-4-i
GLP-1-RA
Insulin§
or
or
or
or
Thiazolidine-dione
+SU
DPP-4-i
GLP-1-RA
Insulin§
TZD
DPP-4-i
GLP-1-RA
high
low risk
loss
GI
high
GLP-1 receptoragonist
Sulfonylurea
high
moderate risk
gain
hypoglycemia
low
SGLT2 inhibitor
intermediate
low risk
loss
GU, dehydration
high
SU
TZD
Insulin§
GLP-1 receptoragonist
+
SGLT-2 Inhibitor
+SU
TZD
Insulin§
Metformin+
Metformin+
or
or
or
or
SGLT2-i
or
or
or
SGLT2-i
Mono-therapy
Efficacy*
Hypo risk
Weight
Side effects
Costs
Dualtherapy†
Efficacy*
Hypo risk
Weight
Side effects
Costs
Tripletherapy
or
or
DPP-4 Inhibitor
+SU
TZD
Insulin§
SGLT2-i
or
or
or
SGLT2-i
or
DPP-4-i
If HbA1c target not achieved after ~3 months of dual therapy, proceed to 3-drug combination (order not meant to denoteany specific preference - choice dependent on a variety of patient- & disease-specific factors):
If HbA1c target not achieved after ~3 months of triple therapy and patient (1) on oral combination, move to injectables, (2) on GLP-1 RA, addbasal insulin, or (3) on optimally titrated basal insulin, add GLP-1-RA or mealtime insulin. In refractory patients consider adding TZD or SGLT2-i:
Metformin+
Combinationinjectabletherapy‡
GLP-1-RAMealtime Insulin
HbA1c ≥9%
Metformin intolerance or
contraindication
Uncontrolled hyperglycemia
(catabolic features, BG ≥300-350 mg/dl,
HbA1c ≥10-12%)
Insulin (basal)
+
or
or
or
Diabetes Care 2015;38:140-149; Diabetologia 2015;10.1077/s00125-014-3460-0

Healthy eating, weight control, increased physical activity & diabetes education
Metforminhigh
low risk
neutral/loss
GI / lactic acidosis
low
If HbA1c target not achieved after ~3 months of monotherapy, proceed to 2-drug combination (order not meant to denoteany specific preference - choice dependent on a variety of patient- & disease-specific factors):
Metformin+
Metformin+
Metformin+
Metformin+
Metformin+
high
low risk
gain
edema,HF, fxs
low
Thiazolidine-dione
intermediate
low risk
neutral
rare
high
DPP-4 inhibitor
highest
high risk
gain
hypoglycemia
variable
Insulin (basal)
Metformin+
Metformin+
Metformin+
Metformin+
Metformin+
Basal Insulin +
Sulfonylurea
+
TZD
DPP-4-i
GLP-1-RA
Insulin§
or
or
or
or
Thiazolidine-dione
+SU
DPP-4-i
GLP-1-RA
Insulin§
TZD
DPP-4-i
GLP-1-RA
high
low risk
loss
GI
high
GLP-1 receptoragonist
Sulfonylurea
high
moderate risk
gain
hypoglycemia
low
SGLT2 inhibitor
intermediate
low risk
loss
GU, dehydration
high
SU
TZD
Insulin§
GLP-1 receptoragonist
+
SGLT-2 Inhibitor
+SU
TZD
Insulin§
Metformin+
Metformin+
or
or
or
or
SGLT2-i
or
or
or
SGLT2-i
Mono-therapy
Efficacy*
Hypo risk
Weight
Side effects
Costs
Dualtherapy†
Efficacy*
Hypo risk
Weight
Side effects
Costs
Tripletherapy
or
or
DPP-4 Inhibitor
+SU
TZD
Insulin§
SGLT2-i
or
or
or
SGLT2-i
or
DPP-4-i
If HbA1c target not achieved after ~3 months of dual therapy, proceed to 3-drug combination (order not meant to denoteany specific preference - choice dependent on a variety of patient- & disease-specific factors):
If HbA1c target not achieved after ~3 months of triple therapy and patient (1) on oral combination, move to injectables, (2) on GLP-1 RA, addbasal insulin, or (3) on optimally titrated basal insulin, add GLP-1-RA or mealtime insulin. In refractory patients consider adding TZD or SGLT2-i:
Metformin+
Combinationinjectabletherapy‡
GLP-1-RAMealtime Insulin
Figure 2B. Anti-hyperglycemic therapy in T2DM: Avoidance of hypoglycemia
or
or
or
Insulin (basal)
+
Diabetes Care 2015;38:140-149; Diabetologia 2015;10.1077/s00125-014-3460-0

Healthy eating, weight control, increased physical activity & diabetes education
Metforminhigh
low risk
neutral/loss
GI / lactic acidosis
low
If HbA1c target not achieved after ~3 months of monotherapy, proceed to 2-drug combination (order not meant to denoteany specific preference - choice dependent on a variety of patient- & disease-specific factors):
Metformin+
Metformin+
Metformin+
Metformin+
Metformin+
high
low risk
gain
edema,HF, fxs
low
Thiazolidine-dione
intermediate
low risk
neutral
rare
high
DPP-4 inhibitor
highest
high risk
gain
hypoglycemia
variable
Insulin (basal)
Metformin+
Metformin+
Metformin+
Metformin+
Metformin+
Basal Insulin +
Sulfonylurea
+
TZD
DPP-4-i
GLP-1-RA
Insulin§
or
or
or
or
Thiazolidine-dione
+SU
DPP-4-i
GLP-1-RA
Insulin§
TZD
DPP-4-i
GLP-1-RA
high
low risk
loss
GI
high
GLP-1 receptoragonist
Sulfonylurea
high
moderate risk
gain
hypoglycemia
low
SGLT2 inhibitor
intermediate
low risk
loss
GU, dehydration
high
SU
TZD
Insulin§
GLP-1 receptoragonist
+
SGLT-2 Inhibitor
+SU
TZD
Insulin§
Metformin+
Metformin+
or
or
or
or
SGLT2-i
or
or
or
SGLT2-i
Mono-therapy
Efficacy*
Hypo risk
Weight
Side effects
Costs
Dualtherapy†
Efficacy*
Hypo risk
Weight
Side effects
Costs
Tripletherapy
or
or
DPP-4 Inhibitor
+SU
TZD
Insulin§
SGLT2-i
or
or
or
SGLT2-i
or
DPP-4-i
If HbA1c target not achieved after ~3 months of dual therapy, proceed to 3-drug combination (order not meant to denoteany specific preference - choice dependent on a variety of patient- & disease-specific factors):
If HbA1c target not achieved after ~3 months of triple therapy and patient (1) on oral combination, move to injectables, (2) on GLP-1 RA, addbasal insulin, or (3) on optimally titrated basal insulin, add GLP-1-RA or mealtime insulin. In refractory patients consider adding TZD or SGLT2-i:
Metformin+
Combinationinjectabletherapy‡
GLP-1-RAMealtime Insulin
Figure 2B. Anti-hyperglycemic therapy in T2DM: Avoidance of weight gain
Insulin (basal)
+
or
or
or
Diabetes Care 2015;38:140-149; Diabetologia 2015;10.1077/s00125-014-3460-0

Healthy eating, weight control, increased physical activity & diabetes education
Metforminhigh
low risk
neutral/loss
GI / lactic acidosis
low
If HbA1c target not achieved after ~3 months of monotherapy, proceed to 2-drug combination (order not meant to denoteany specific preference - choice dependent on a variety of patient- & disease-specific factors):
Metformin+
Metformin+
Metformin+
Metformin+
Metformin+
high
low risk
gain
edema,HF, fxs
low
Thiazolidine-dione
intermediate
low risk
neutral
rare
high
DPP-4 inhibitor
highest
high risk
gain
hypoglycemia
variable
Insulin (basal)
Metformin+
Metformin+
Metformin+
Metformin+
Metformin+
Basal Insulin +
Sulfonylurea
+
TZD
DPP-4-i
GLP-1-RA
Insulin§
or
or
or
or
Thiazolidine-dione
+SU
DPP-4-i
GLP-1-RA
Insulin§
TZD
DPP-4-ior
or
or GLP-1-RA
high
low risk
loss
GI
high
GLP-1 receptoragonist
Sulfonylurea
high
moderate risk
gain
hypoglycemia
low
SGLT2 inhibitor
intermediate
low risk
loss
GU, dehydration
high
SU
TZD
Insulin§
GLP-1 receptoragonist
+
SGLT-2 Inhibitor
+SU
TZD
Insulin§
Metformin+
Metformin+
or
or
or
or
SGLT2-i
or
or
or
SGLT2-i
Mono-therapy
Efficacy*
Hypo risk
Weight
Side effects
Costs
Dualtherapy†
Efficacy*
Hypo risk
Weight
Side effects
Costs
Tripletherapy
or
or
DPP-4 Inhibitor
+SU
TZD
Insulin§
SGLT2-i
or
or
or
SGLT2-i
or
DPP-4-i
If HbA1c target not achieved after ~3 months of dual therapy, proceed to 3-drug combination (order not meant to denoteany specific preference - choice dependent on a variety of patient- & disease-specific factors):
If HbA1c target not achieved after ~3 months of triple therapy and patient (1) on oral combination, move to injectables, (2) on GLP-1 RA, addbasal insulin, or (3) on optimally titrated basal insulin, add GLP-1-RA or mealtime insulin. In refractory patients consider adding TZD or SGLT2-i:
Metformin+
Combinationinjectabletherapy‡
GLP-1-RAMealtime Insulin
Figure 2C. Anti-hyperglycemic therapy in T2DM: Minimization of costs
Insulin (basal)
+
Diabetes Care 2015;38:140-149; Diabetologia 2015;10.1077/s00125-014-3460-0

LookAHEAD Study Objective
The Look AHEAD Research Group. N Engl J Med 2013;369:145-154
To determine the long-term effects (up to
13.5 years) of an intensive lifestyle
intervention program designed to produce
weight loss and increase physical activity
on cardiovascular morbidity and mortality
in overweight or obese persons with
type 2 diabetes.

Seattle
Los
Angeles
San AntonioHouston
Baton Rouge
Minneapolis
Memphis
Birmingham
Winston-Salem
Baltimore
PhiladelphiaNew York
Providence
Boston
Pittsburgh
Clinical
Site
Coordinating
Center
Denver
16 Clinical Sites
PhoenixShiprock

Results: Weight Loss
The Look AHEAD Research Group. N Engl J Med, June 24, 2013
Mean F/U 9.6 years
1-yr wt loss: 8.6% ILI0.7% control group
Study end:6.0% ILI3.5% control group

Results: Primary Outcome
The Look AHEAD Research Group. N Engl J Med, June 24, 2013
Events/100 person-yrs:
1.83 ILI1.92 Control
Hazard ratio 0.95(95% CI 0.83-1.09, P=0.51)

N=174
(19.6%)
+2
0
2
4
6
8
10
12
14
16
18
1 2 3 4
Pe
rce
nta
ge
We
igh
t L
os
s4-Yr Wt Loss Trajectories of 887 ILI Participants
Who Lost ≥ 10% Initial Weight at Yr 1 (~35%)
Years
0-5%
5-6.9%
7-
10%
≥ 10%
Gained
N=374
(42.2%)
N=152
(17.1%)
N=99
(11.2%)
N=88
(9.9%)
+4

Mean Annual Number of
Meal Replacements Used
in Years 2-4
p < .05
0
20
40
60
80
100
120
140
> 10% 5 - 9.9% 0 - 4.9% Gained
Weight Change- Year 4
Me
al R
ep
lac
em
en
ts
p < .02
125.7 103.2 80.8 84.2
Mean Weekly Kcal
Expenditure at Year 4 (as
Determined by Paffenbarger)
0
500
1000
1500
2000
2500
> 10% 5 - 9.9% 0 - 4.9% Gained
Weight Change- Year 4
Kca
l/w
k o
f A
cti
vit
y
1997.9 1406.2 1127.3 949.3
p < 0.005 for all
comparisons
with > 10%
group

Metformin: The Only Choice in Type 2 DM?
• Most commonly used therapy for T2 DM (2/3rds of
patients)
• Clinical effects
• Lowers A1C 1-2% (especially at high baseline A1C), no weight gain
• Maximal clinical effect at 1500-2000 mg/day
• Possible side effects and precautions
• GI side effects common – less well tolerated by up to 10%
• Not advised if significant renal or liver disease, heart failure (~20%)
• Other features
• Lower CV risk in obese patients (UKPDS)
• Extensive clinical experience and lower cost
• ? Favorable impact on cancer risk and mortality

Sulfonylureas and the SecretagoguesHow Do We Use Them Now?
• Most common (traditional) 2nd agent in T2 DM
• Stimulate insulin release – during hyperglycemia and post-meal
• Clinical Use
• Inexpensive and commonly used, rapid glucose lowering
• Limited dose effect and limited “durability” of effect
• Side effects
• Associated with weight gain and risk of hypoglycemia
• Precautions and contraindications
• Associated with risk of severe hypoglycemia (elderly, renal disease)
• Highest risk of hypoglycemia with GLYBURIDE
• May not be good for those at CVD risk (longstanding discussion)

Thiazolidinediones (TZDs) Do We Target Insulin Resistance?
• Clinical application
• Targeted patients with clinical markers of insulin resistance
• Dyslipidemia, HTN, established CVD, central obesity
• May limit CVD risk and alter progression of diabetes
• Adverse effects and considerations
• Significant weight gain and increase risk of edema and HF
• Increased risk of long-bone fractures
• Macular edema
• Patient selection
• Higher CVD risk – particularly with dyslipidemia, est. CVD
• Those at lower risk for fracture and with central obesity, NASH
Grey A et al. J Clin Endocrinol Metab. 2007;92:1305-1310.

Summary Of Pioglitazone Clinical TrialsCenter for Drug Evaluation & Research, July 30, 2007
Hazard Ratio0.5 0.75
PIO Meta-analysis
- without PROactive
PROactive
PIO Meta-Analysis
plus PROactive
0.83
0.84
0.75
375 450
8554 7836
1.0
PIO COMP
#CV Events
# of Subjects

DPP-4 Inhibitors: Sitagliptin (Januvia), Saxagliptin
(Onglyza), Linagliptin (Tradjenta) and Alopglitin (Nesina)
• Clinical Use
• Moderate effectiveness (A1C reduction ~0.5-0.8%)
• Use in both combo and mono therapy
• Unique Features
• Limited side effect profile, very well tolerated, pancreatitis?
• Weight neutral, no significant weight loss, no hypoglycemia
• Variable clinical response (A1C reduction 0.2-1.1%)
• Reduced dosing in chronic kidney disease (except for linagliptin)
• Saxagliptin increased risk of CHF in high risk population

GLP-1 RA’s: Exenatide (Byetta, Bydureon), liraglutide
(Victoza), albiglutide (Tanzuem), dulaglutide (Trulicity)
• Clinical Use
• Lowers A1C 1 – 1.5%
• Often associated with weight loss
• Side Effects/Features
• Injected once or twice daily or once weekly
• GI side effects common; rare hypoglycemia
• Warnings: pancreatitis; MCT
• Drug-specific features
• Potential CVD benefits

Potential Cardiovascular Effects of GLP-1-Based Therapies
Improved weight, SBP, lipids
Improved endothelial function
Increased vasorelaxation
Increased peripheral and coronary flow
Increased ventricular function
Decreased microvascular permeability
Reduced inflammation
Okerson T, Chilton R. Cardiovasc Ther 30:e146-55, 2012

Incretin Cardiovascular Outcome Trials
EXSCEL - Exenatide LAR n=14,000
LEADER - Liraglutide n=9,340
REWIND - Dulaglutide n=9,622
ELIXA -Lixisenatide n=6,000
TECOS - Sitagliptin n=14,000
SAVOR-TIMI 53 - Saxagliptin n=16,500
EXAMINE -Alogliptin n=5,400
CAROLINA (vs SU) - Linagliptin n=6,000
September 2013
September 2018
December 2014
September 2013
April 2018
April 2019
January 2015
October 2015
SUSTAIN 6 - Semaglutide n=3,297 January 2016
Risk Factors Stable CAD-CVD-PAD ACS patients
CARMELINA (vs pbo) - Linagliptin n=8,300
January 2018

SGLT-2 Inhibitors—Canagliflozin, Dapagliflozin, Empagliflozin
Clinical Effects
• Novel mechanism of action/oral agent
• Most will respond—action independent of beta-cell function
• A1C reduction ~1% with 2-3 kg weight loss
Possible Side Effects and Precautions
• Mycotic genital infections
• Findings due to volume depletion
• Don’t use if eGFR <45%
Other Features
• Lowers BP slightly
• Raises LDL cholesterol
Jacobsen LV, et al. Br J Clin Pharmacol. 2009;68:898-905. Linnebjerg H, et al. Br J Clin Pharmacol. 2007;64:317-327.

Screening
T2DM on metformin alone
HbA1c >6.8% at screening
< 10 years duration at randomization
Randomization
n=5000 eligible subjects
Sulfonylurea
(glimepiride)
n=1250
DPP-IV inhibitor
(sitagliptin)
n=1250
GLP-1 analog
(liraglutide)
n=1250
Insulin
(glargine)
n=1250
HbA1c 6.8-8.5% at final run-in visit
Glycemia Reduction Approaches in Diabetes:
A Comparative Effectiveness Study
Metformin run-inTitrate metformin to 1000 (min) – 2000 (goal) mg/day

Reducing CVD Risk Treating T2DM
o Use statins, control BP, give aspirin
o Use diabetes drugs that don’t cause
hypoglycemia or minimize hypos in drugs that do
o Improve control early and maintain it
o Never forget importance of lifestyle
RxList, 2014.

Thank You
RxList, 2014.