Embed Size (px)
Citation preview
Treating Cancer with T Cell-Engaging Antibodies
Flavius Martin M.D.
Vice President Research, Amgen Inc.
For Internal Use Only. Amgen Confidential. 2
Tumor Cell Antigens:- Surface/Presented- Cell autonomous functions
T cells:- Response tuning- Effector function
T cell Tumor Immunotherapy Players
BiTE®
BiTE®
3
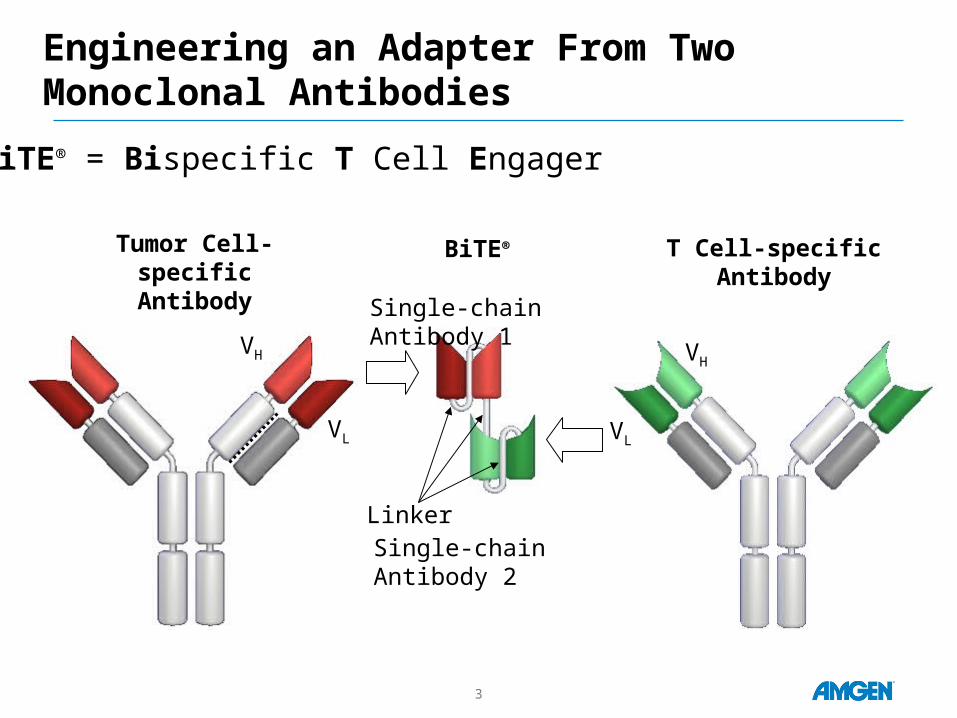
Engineering an Adapter From Two Monoclonal Antibodies
Tumor Cell-specificAntibody
T Cell-specific Antibody
VH
VL
VH
VL
Linker
BiTE®
Single-chain Antibody 1
BiTE® = Bispecific T Cell Engager
Single-chain Antibody 2
4
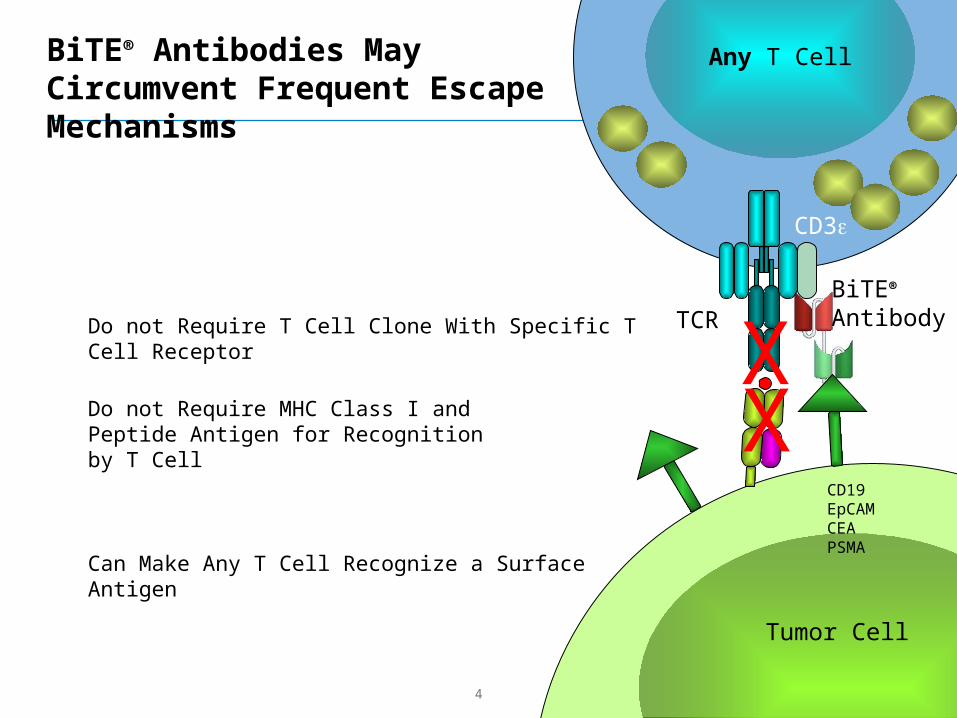
Any T Cell
Tumor Cell
CD3e
Do not Require MHC Class I andPeptide Antigen for Recognition by T Cell
Do not Require T Cell Clone With Specific T Cell Receptor
Can Make Any T Cell Recognize a Surface Antigen
TCRBiTE®
Antibody
BiTE® Antibodies May Circumvent Frequent Escape Mechanisms
XX
CD19EpCAMCEAPSMA
5
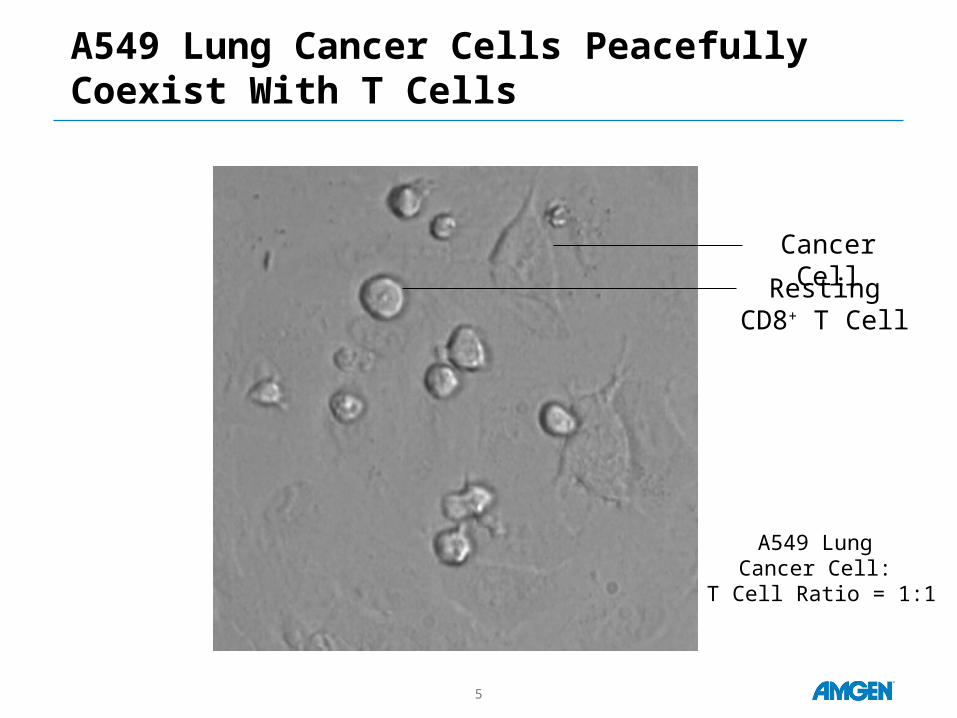
A549 Lung Cancer Cells Peacefully Coexist With T Cells
A549 Lung Cancer Cell:
T Cell Ratio = 1:1
Cancer Cell
RestingCD8+ T Cell
6
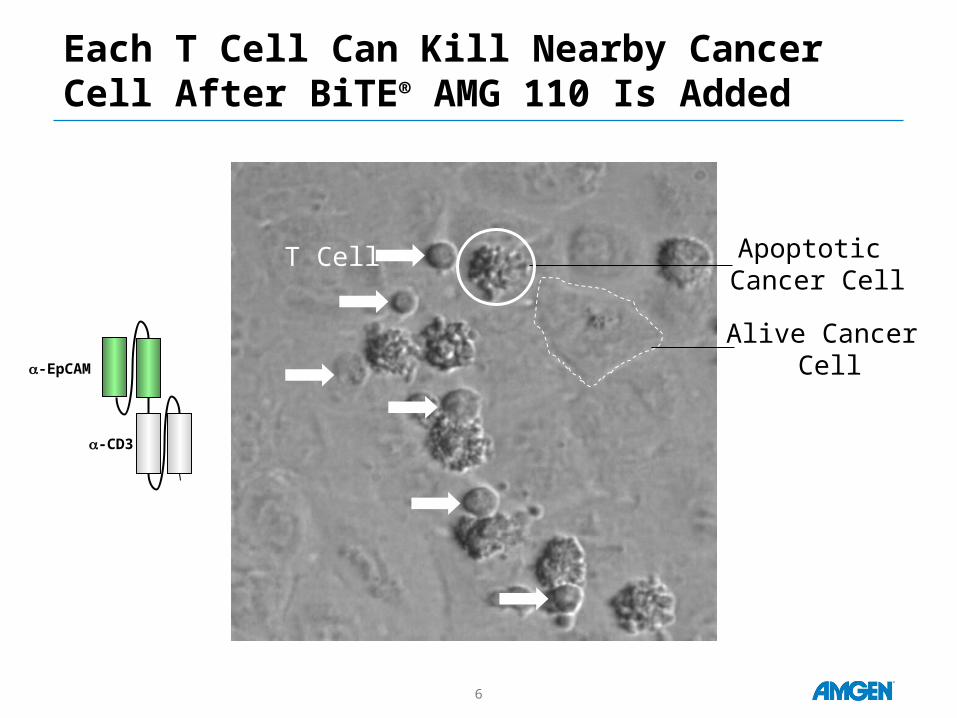
Each T Cell Can Kill Nearby Cancer Cell After BiTE® AMG 110 Is Added
Alive Cancer Cell
T Cell Apoptotic Cancer Cell
-EpCAM
-CD3
7
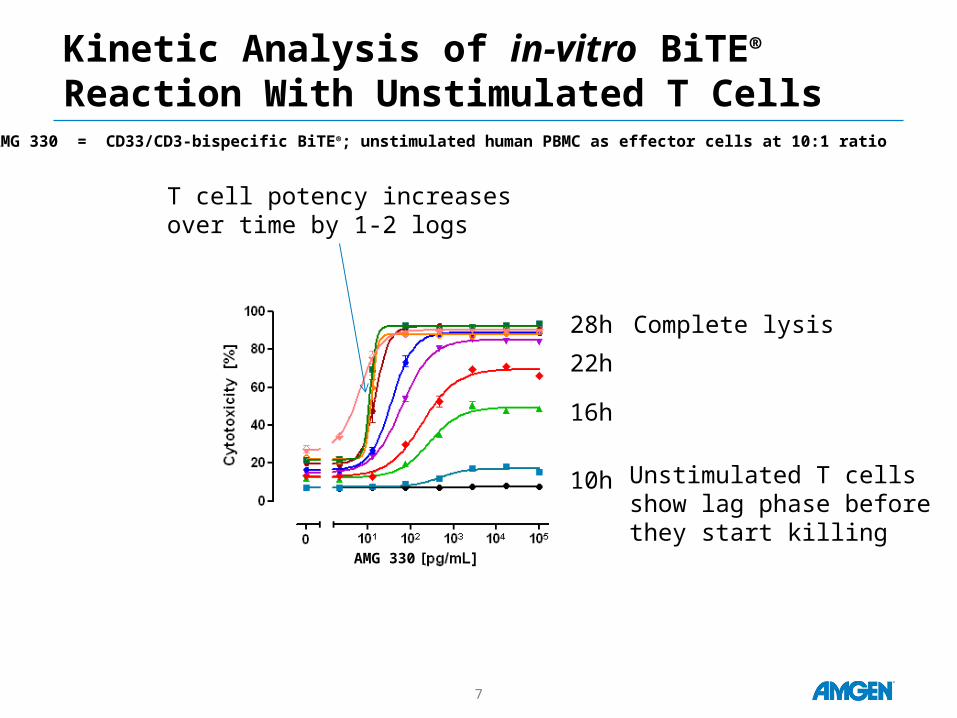
Kinetic Analysis of in-vitro BiTE® Reaction With Unstimulated T Cells
T cell potency increasesover time by 1-2 logs
AMG 330 = CD33/CD3-bispecific BiTE®; unstimulated human PBMC as effector cells at 10:1 ratio
AMG 330 [
10h
16h
22h
28h Complete lysis
Unstimulated T cells show lag phase beforethey start killing
8
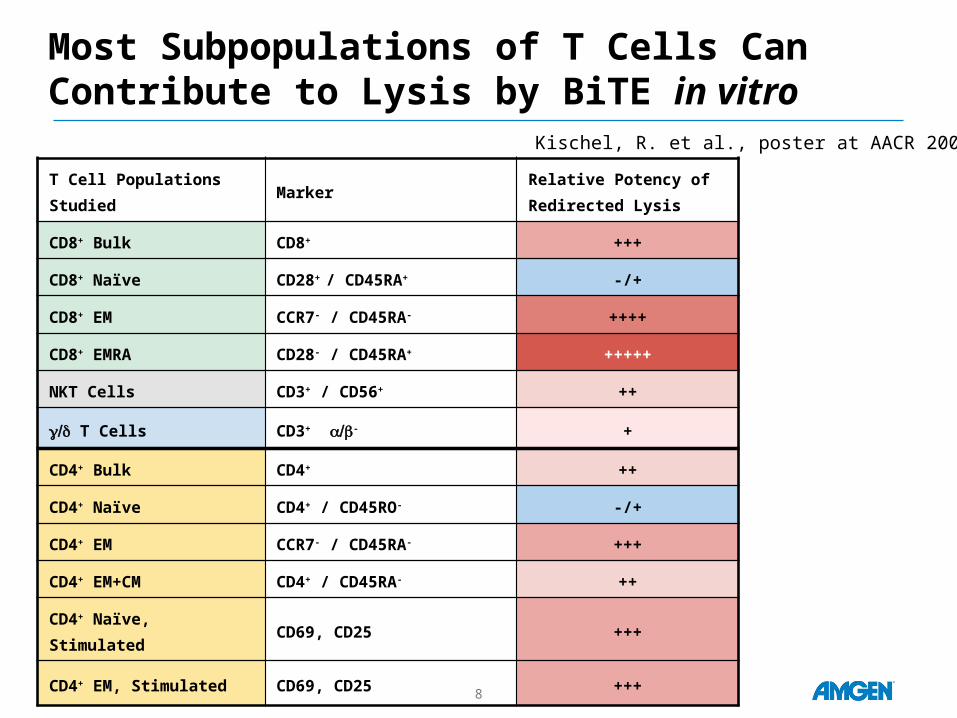
Most Subpopulations of T Cells Can Contribute to Lysis by BiTE in vitro
T Cell Populations Studied MarkerRelative Potency of Redirected Lysis
CD8+ Bulk CD8+ +++
CD8+ Naïve CD28+ / CD45RA+ -/+
CD8+ EM CCR7- / CD45RA- ++++
CD8+ EMRA CD28- / CD45RA+ +++++
NKT Cells CD3+ / CD56+ ++
/g d T Cells CD3+ /a b- +
CD4+ Bulk CD4+ ++
CD4+ Naïve CD4+ / CD45RO- -/+
CD4+ EM CCR7- / CD45RA- +++
CD4+ EM+CM CD4+ / CD45RA- ++
CD4+ Naïve, Stimulated CD69, CD25 +++
CD4+ EM, Stimulated CD69, CD25 +++
Kischel, R. et al., poster at AACR 2009
9
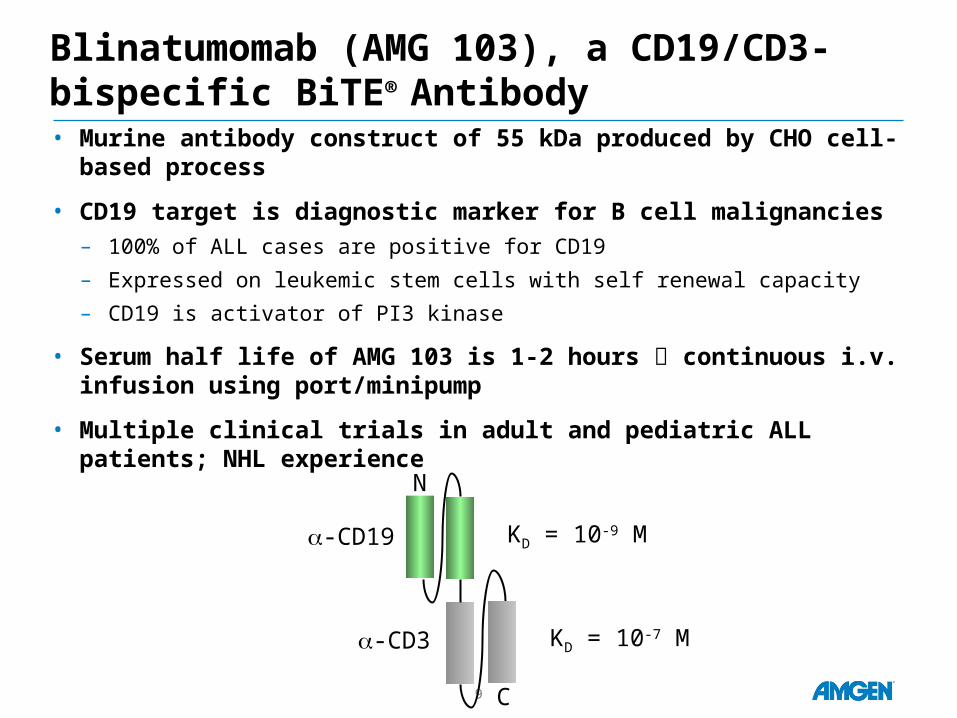
Blinatumomab (AMG 103), a CD19/CD3-bispecific BiTE® Antibody• Murine antibody construct of 55 kDa produced by CHO cell-based
process
• CD19 target is diagnostic marker for B cell malignancies– 100% of ALL cases are positive for CD19
– Expressed on leukemic stem cells with self renewal capacity
– CD19 is activator of PI3 kinase
• Serum half life of AMG 103 is 1-2 hours continuous i.v. infusion using port/minipump
• Multiple clinical trials in adult and pediatric ALL patients; NHL experience
-CD19
-CD3
KD = 10-9 M
KD = 10-7 M
N
C
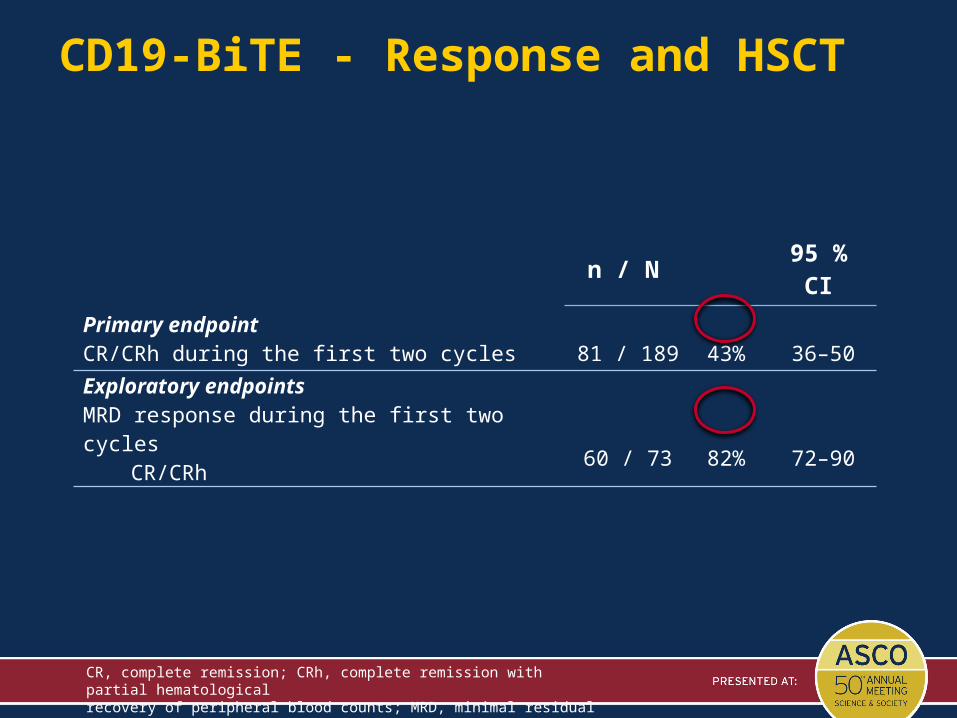
CD19-BiTE - Response and HSCT
n / N 95 % CI
Primary endpointCR/CRh during the first two cycles 81 / 189 43% 36–50
Exploratory endpointsMRD response during the first two cycles
CR/CRh 60 / 73 82% 72–90
CR, complete remission; CRh, complete remission with partial hematologicalrecovery of peripheral blood counts; MRD, minimal residual disease (< 10-4)
11
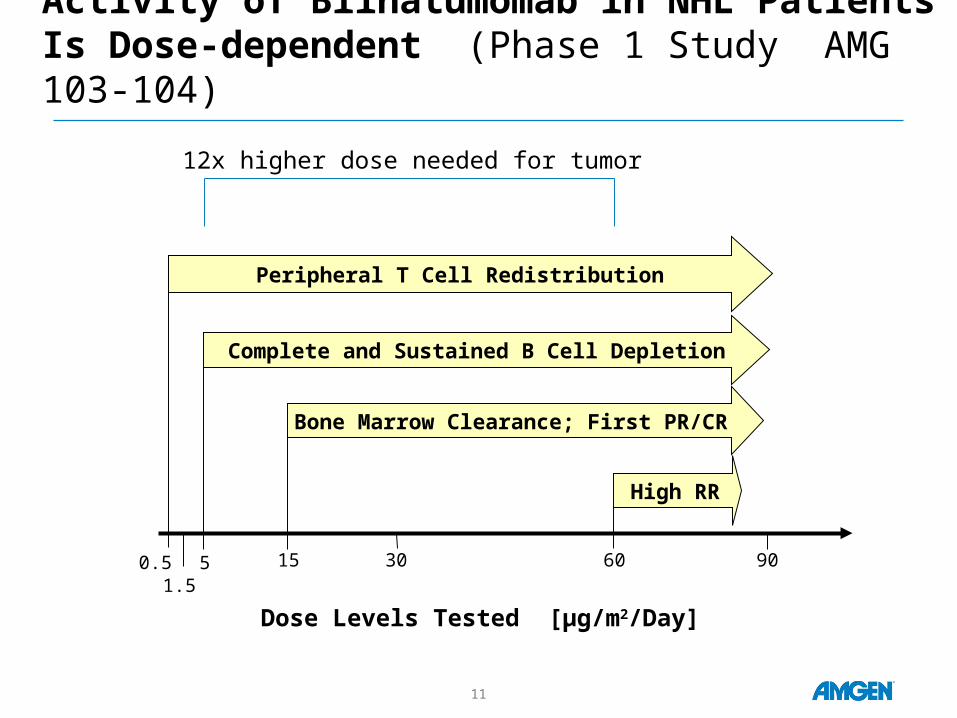
Activity of Blinatumomab in NHL Patients Is Dose-dependent (Phase 1 Study AMG 103-104)
0.51.5
5 15 30 60 90
Dose Levels Tested [µg/m2/Day]
Complete and Sustained B Cell Depletion
Peripheral T Cell Redistribution
Bone Marrow Clearance; First PR/CR
High RR
12x higher dose needed for tumor
12
Preliminary Learnings From Blinatumomab Monotherapy about BiTE® Modality
• Need only very low doses– High response rates in ALL patients at steady state serum levels of
0.5 to 1 ng/ml (<18 pM); cumulative doses of low milligrams per cycle
• Eliminates proliferating and nonproliferating target cells– Potential to eliminate dormant cancer stem cells
• Activity in many locations of body– Antitumor activity seen in blood, bone marrow, lymph nodes, spleen,
lymphoma tissue, liver tissue
• Activity in patients who have exhausted all established therapies, including rituximab regimen and SCT
• Activity in elderly and pediatric patients
• Activity in severly immunocompromised patients– Observed complete response in patients with low to undetectable
peripheral T cell counts
13
Other BiTE® Antibodies in Development
Clinical Phase 1:
• Solitomab (AMG 110: EpCAM) – Advanced solid tumors
• AMG 212 (BAY2010112: PSMA) – Prostate cancer
• AMG 211 (MEDI-565: CEA) – Advanced GI cancers
Pre-clinical:
• AMG 330 (CD33) – Acute myeloid leukemia (AML)
• Multiple myeloma BiTE --
• Solid tumor BiTE® –
14
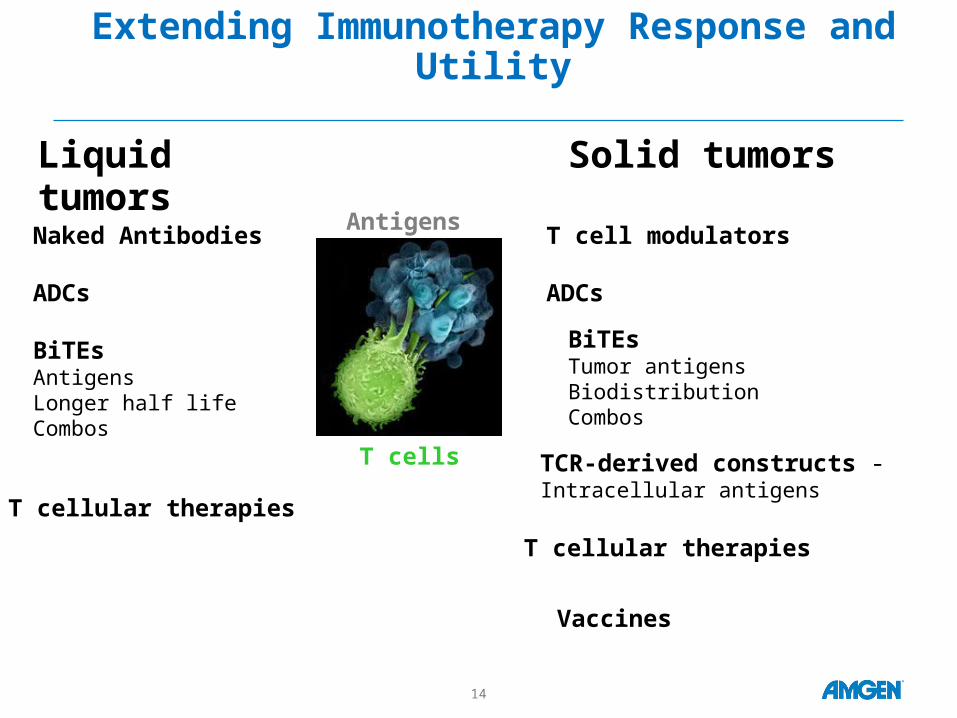
Extending Immunotherapy Response and Utility
Liquid tumors
Antigens
T cells
Solid tumors
Naked Antibodies
ADCs
BiTEsAntigensLonger half lifeCombos
Vaccines
BiTEsTumor antigens Biodistribution Combos
T cell modulators
ADCs
T cellular therapies
TCR-derived constructs -Intracellular antigens
T cellular therapies

Appendix
15
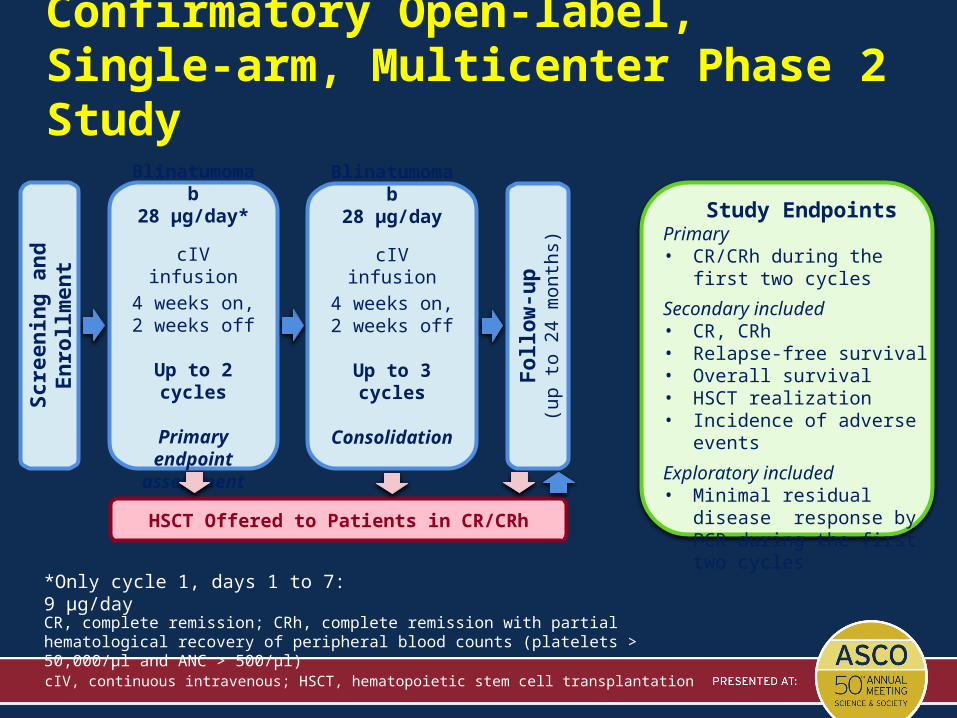
Confirmatory Open-label, Single-arm, Multicenter Phase 2 Study
*Only cycle 1, days 1 to 7: 9 μg/day
cIV, continuous intravenous; HSCT, hematopoietic stem cell transplantation
Scr
een
ing
an
d E
nro
llmen
t
Fo
llow
-up
(up
to 2
4 m
ont
hs)
HSCT Offered to Patients in CR/CRh
Blinatumomab28 μg/day*
cIV infusion
4 weeks on,2 weeks off
Up to 2 cycles
Primary endpoint
assessment
Blinatumomab28 μg/day
cIV infusion
4 weeks on,2 weeks off
Up to 3 cycles
Consolidation
Study EndpointsPrimary• CR/CRh during the first two
cycles
Secondary included• CR, CRh• Relapse-free survival• Overall survival• HSCT realization• Incidence of adverse events
Exploratory included• Minimal residual disease
response by PCR during the first two cycles
CR, complete remission; CRh, complete remission with partial hematological recovery of peripheral blood counts (platelets > 50,000/μl and ANC > 500/μl)
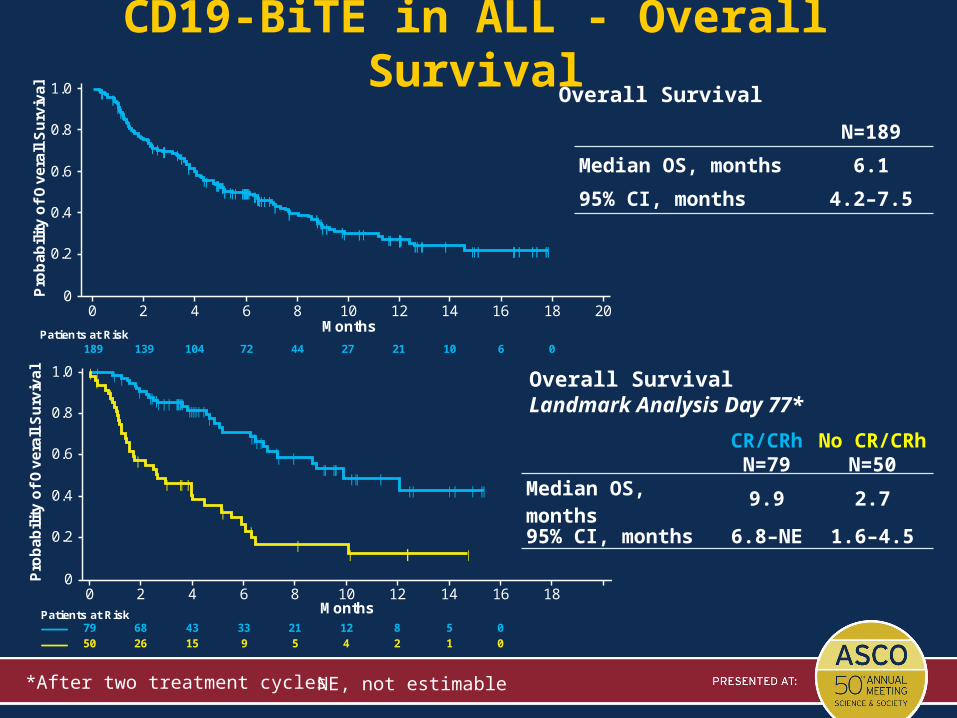
CD19-BiTE in ALL - Overall Survival
Overall SurvivalLandmark Analysis Day 77*
*After two treatment cycles
CR/CRh No CR/CRhN=79 N=50
Median OS, months 9.9 2.795% CI, months 6.8–NE 1.6–4.5
Overall Survival
0
0.2
0.4
0.6
0.8
1.0
Patients at Risk189 139 104 72 44 27 21 10 6 0
Pro
bab
ility
of O
vera
ll Surv
ival
Months0 2 4 6 8 10 12 14 16 18 20
0
0.2
0.4
0.6
0.8
1.0
Patients at Risk Months79 68 43 33 21 12 8 5 050 26 15 9 5 4 2 1 0
Pro
bab
ility
of O
vera
ll Surv
ival
0 2 4 6 8 10 12 14 16 18
N=189
Median OS, months 6.1
95% CI, months 4.2–7.5
NE, not estimable





























