Embed Size (px)
Citation preview
2/25/11
1
Travel Medicine
Infec/ous Diseases in Clinical Prac/ce
February 2011 Brian S. Schwartz, MD
Director, UCSF Travel Medicine and Immuniza/on Clinic
Lecture outline
1. How to prepare your pa/ents for safe travel
2. How to evaluate an ill returning traveler
Travelers crossing interna/onal borders
Keystone. Travel Medicine. 2008

2/25/11
2
What do we know about travelers from the US?
Lesiure 50%
Business 15%
VFR 11%
Research/Educa7on 9%
Service Work 15%
• India • S. Africa/Thailand
• India • Ghana
• India • China
• China • India
• Hai7 • Kenya
Reason for travel and 2 most frequent des/na/ons
N=13,235
Travel related morbidity/mortality
• 20-‐70% report some illness
• 1-‐5% seek medical aVen/on
• 3% report fevers
• 0.1-‐0.01% require medical evacua/on
• 1/100,000 – death Hill DR. CID. 2006

2/25/11
3
PREPARING THE TRAVELER Part 1
Pre-‐travel consulta/on
1. Assessing the health of the traveler
2. Assessing the risk of travel
3. Preventa/ve advice
4. Immuniza/ons/prophylaxis/self treatment
Assessing the health of the traveler

2/25/11
4
Cardiovascular Disease 49%
Injury 22%
Infec7on 1%
Other/Unknown 6%
Cancer 6%
Suicide/Homicide 3%
Medical 14%
Exacerba/on of comorbidi/es is the predominant cause of death in US Travelers:
Hargarten SW. Annals of Emergency Medicine.1991
Asthma in adventure travelers
• 203 w/ asthma assessed pre/post travel
– 88 (43%) had asthma aVacks
– Risk factors for aVacks during travel • Frequent bronchodilator use before travel (RR, 3.35) • Intensive physical exer/on during treks (RR, 2.04)
– Triggers • Trekking (43%), Exercise (41%), Pollu/on (27%), Dust (25%)
Golan Y. Annals Internal Med. 2002
Assessing the risk of travel

2/25/11
5
Infec/ons acquired during stay in developing countries
• 20-‐70 % -‐ Traveler’s diarrhea • 3% -‐ Malaria (no chemoprophylaxis in Africa)
• 1% -‐ Influenza, Dengue • 0.5% -‐ Animal bite, PPD conversion
• 0.05% -‐ Typhoid, Hep A • 0.0001% -‐ Japanese encephali/s • < 0.0001% -‐ Meningococcal disease , polio
Steffen R. J Trav Med. 2008
Assessing the risk of travel
• Vaccine preventable infec/ons • Malaria
• Traveler's diarrhea • Vector borne illness • Other
Vaccine preventable diseases • Rou/ne vaccina/on should be up to date
– Measles and mumps
– Influenza
• “Required” vaccines – Yellow fever: many endemic countries
– Meningococcal vaccine: Haj
• Other vaccines “recommended”
• Live vaccines -‐ avoid in IS/pregnant pa/ents

2/25/11
6
How to determine risk of vaccine preventable diseases?
• CDC Yellow Book – hVp://wwwnc.cdc.gov/travel/default.aspx
• WHO – hVp://www.who.int/ith/en/
• Other – hVp://www.mdtravelhealth.com/
– hVp://www.filortravel.scot.nhs.uk/des/na/ons.aspx
• What do we use in clinic? – Travax™ EnCompass
Malaria • 1997-‐2006: 10,745 malaria cases in US, 54 (0.5%) fatal
• Risk is highly variable by travel region
Freeman DO. NEJM 2008

2/25/11
7
Recommenda/ons for malaria prophylaxis are not always the same for the whole country…
Malaria preven/on • Low risk:
– Insect avoidance: DEET; bednets; long sleeves; avoid being outside at dusk and dawn
– Consider chemoprophylaxis in certain persons: • vulnerable travelers • immigrants visi/ng friends/rela/ves • prolonged travel (> 1 mo) • unreliable access to medical care
• Moderate -‐ High risk: – Chemoprophylaxis
Malaria chemoprophylaxis Drug Direc7ons Side effects
Mefloquine (Lariam™)
Weekly; start 1 week before, during and 4 weeks post
Vivid dreams, avoid if psychiatric or seizure disorder
Doxycycline Daily; start day before, during, 4 weeks post
Photosensi/vity; GI upset
Atovaquone/proguanil (Malarone™)
Daily; start day before, during, 1 week post
Expensive
Chloroquine Weekly; start day before, during, 4 weeks post
GI upset. Only effec)ve in limited areas (West of Panama canal, Hai))
2/25/11
8
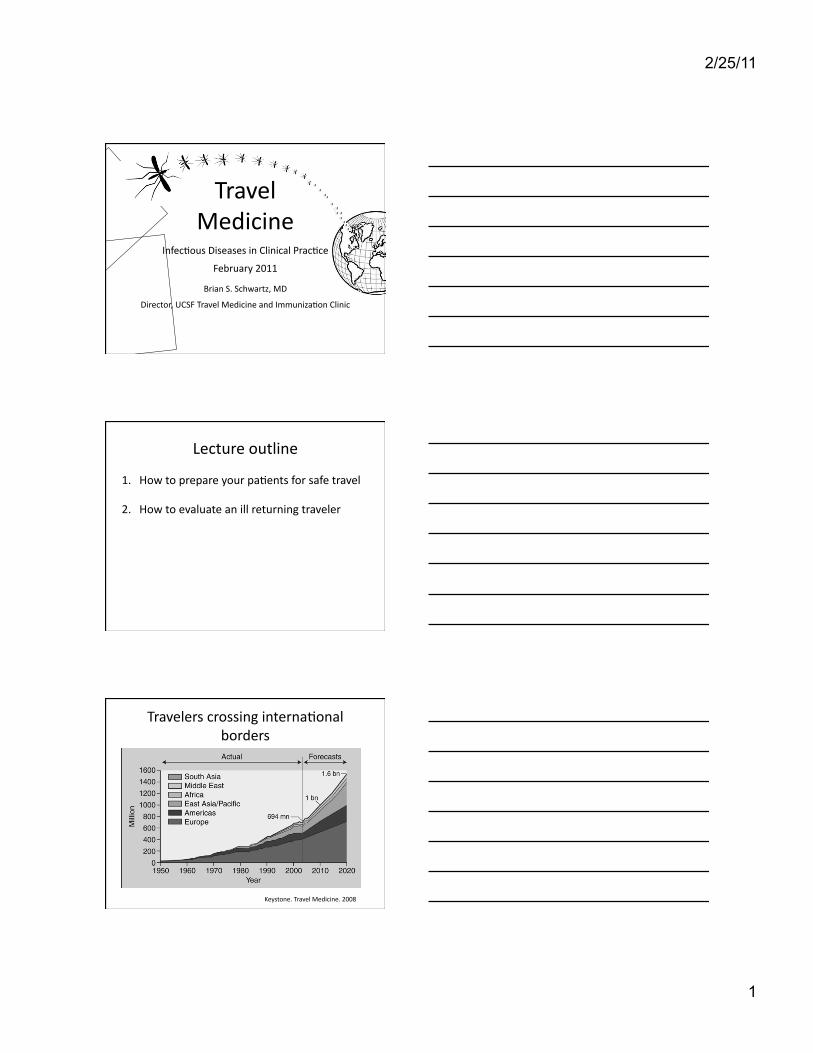
sporozoites
schizont
schizont
trophozoite
merozoites
merozoites
LIVER RBC
Hepatocyte
Lifecycle of P. falciparum
7-14d after infection
Mefloquine Doxycycline Chloroquine
Atovaquone/proguanil
Traveler’s diarrhea (TD)
• #1 travel-‐related illness: 30-‐70% of travelers
• Pathogens: – Bacteria 80-‐90%: ETEC, campy, shigella, salmonella – Viruses 10%: Norovirus, rotavirus
• Course: – Bacterial and viral diarrhea lasts 3-‐5 days – Longer dura/ons suggests other diseases
Preven/on and treatment of TD
• Avoidance: “boil it, peel it, cook or forget it” • Prophylaxis
– Bismuth subsalicylate QID dosing – An/microbials: ciprofloxacin or rifaximin
– Probio/cs?: Studies mixed results
• Self-‐treatment

2/25/11
9
Self-‐treatment of TD
• An/bio/cs – Ciprofloxacin – drug of choice outside SE Asia
• 500 mg PO BID un/l symptoms improve vs. 3 days
– Azithromycin – drug of choice for SE Asia • 500 mg PO QD x 3 days • 1000 mg PO x 1
– Rifaximin – not for invasive infec/ons • 200 mg PO TID x 3 days
• An/-‐mo/lity agents: add in “emergency”
Vector borne illness preven/on
• Dengue fever, chikungunya fever, ricketssial infec/ons…
• Recommenda/ons – Long sleeve clothing, avoid high risk areas – Insect repellents
• DEET ~ 35% for skin, no increased benefit > 50% • Premethrin for clothing
Other infec/ous and non-‐infec/ous risks of travel
• Plan to swim in fresh water? – Leptospirosis – Schistosomiasis
• Travel to High Al/tude: > 8000 x? – Common des/na/ons: Machu Picchu, Tibet, etc… – Some symptoms > 25% – Educate on acclima/za/on
– Acetazolamide prophylaxis

2/25/11
10
Travelers Visi/ng Friends and Rela/ves (VFR)
• Immigrants or 2nd gen persons returning to their homeland to visit friends and rela/ves – Higher degree of exposure – Insufficient protec/on measures
• Immigrant VFR traveler vs. tourist traveler – Malaria risk: 8.7x – Intes/nal parasite: 3.8x – Hospitaliza/on: 8.3x
Leder K. CID. 2006
Other important topics to discuss
• Safe sex
• Avoidance of animals
• Injury preven/on
• Managing symptoms of jet lag
• Sun exposure
Case 1: Bill • 65 year-‐old male planned a 3 week trip to Asia, leaving in 15 days
• I/nerary: – India (1.5 weeks) – Delhi, Jaipur, Mumbai
– Thailand (1.5 weeks) – Bangkok and resort islands
• High end tour, hotels
• “I love Indian and Thai food and I plan to eat where the food is the best, on the street”

2/25/11
11
Assessing the health of the traveler
• Underlying medical condi7ons: – GERD and Hypertension
• Medica7ons – Omeprazole and lisinopril
• Allergies – none
• Immuniza7on history – Polio; Hepa))s B; born before ’57; had varicella
Recommenda/ons based on Bill’s medical issues
• HTN – Keep meds in carry-‐on
– Bring copies of Rx
• PPI use increase risk for traveler’s diarrhea – Avoiding high risk food, consider daily prophylaxis
• Consider obtaining evacua/on insurance – Example: Interna)onal SOS, MEDEX
Which immuniza/ons would you recommend to Bill?
A. Hepa//s A
B. Hepa//s E
C. Japanese encephali/s
D. Typhoid
E. A and D

2/25/11
12
Hepa//s A
• Transmission: – food/water
• Risk: – 1:4,000-‐1:16,000 per/mo abroad
• Vaccine – Intramuscular (inac/vated)
– Life-‐long protec/on axer 2nd dose at 6 mo – Ok to give up un/l departure
Victor JC. NEJM. 2007
Typhoid Fever
• Transmission: – food/water
• > 400 cases annually US – Travel #1 risk factor
• 2 vaccines (50-‐80% protec/ve) – Intramuscular (inac/vated) – booster Q2 years
– Oral (live aVenuated) – booster Q5 years
Hepa//s E
• Transmission: – food/water
• Risk: – Less transmissible than Hepa//s A
• Endemic and epidemics
• High mortality in pregnant women
• No vaccine available Teshale EH. CID 2010

2/25/11
13
Other immuniza/ons to consider in travelers to Asia
• Japanese Encephali/s
• Hepa//s B
• Rabies
• Polio
http://wwwnc.cdc.gov/travel/yellowbook/2010/chapter-2/japanese-encephalitis.aspx
Malaria map of India
http
s://w
ww
.trav
ax.c
om/s
crip
ts/m
ain/
inde
x.as
p
Malaria map of Thailand
http
s://w
ww
.trav
ax.c
om/s
crip
ts/m
ain/
inde
x.as
p

2/25/11
14
Malaria preven/on for Bill?
• Axer weighing risks and benefits..
• Malarone™ for his /me in India
TD preven/on/treatment recommenda/ons for Bill?
• Safe food/water intake
• Prophylaxis – Rifaximin 200 mg PO QD
• Breakthrough treatment – Azithromycin 500 mg PO QD x 3d
• When to seek medical aVen/on – Fever > 2 days, dehydra/on, bloody diarrhea
Dupont HL. Ann Intern Med. 2005
Vector borne illness preven/on
• Travel risk for Bill? – Dengue fever in India and Thailand – Chikungunya fever in S. India
• Recommenda/ons – Long sleeve clothing, avoid high risk areas – Insect repellents
• DEET ~ 35% for skin • Premethrin for clothing

2/25/11
15
Yellow Fever • Transmission: mosquito
• 1970-‐2002: 9 travelers; 8/9 died • Risk:
– W. Africa: 50/100K; S. America: 5/100K
• Only required vaccine • Vaccina/on risk (↑ with age)
– Neurologic Disease (0.8/100K) – Viscerotropic Disease (0.4/100K)
Summary
• Goal is to minimize health risk during travel
– Iden/fy condi/ons that could worsen during travel
– Iden/fy specifics risks of pa/ent’s travel
– Provide advice, PRN treatment, and immunize
– Consider involving a specialist in travel medicine
THE FEBRILE RETURNING TRAVELER Part 2

2/25/11
16
Fever
• 2-‐3% of American/European travelers to developing countries
Hill DR. J Trav Med. 2000
So many diagnoses, how to narrow your DDx?
Geography
Exposures
Incubation Exam findings
Prophylaxis
Diagnosis
Geography
• Where did they go – specifically? – Not just country but ci/es – Time of year
• What is endemic is that region? – Use resources

2/25/11
17
0
100
200
300
400
500
600
700
800
900
1000
Carribean C. America S. America Sub-‐Saharan Africa
South Central Asia
SE Asia
Cases
Freedman DO. NEJM. 2006.
E/ology of fever according to region traveled
Dengue
Unknown
EBV/CMV
Malaria
Rickettsia
Typhoid
Dengue
Incuba/on period?
• Incuba/on period is from /me of exposure
• Marked variability amongst infec/ons
• Very helpful in making diagnosis

2/25/11
18
Clinical Infectious Diseases 2007
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0-‐7 7-‐14 14-‐21 21-‐28 28-‐35 35-‐42 >42
Prop
or7on
of D
iagnoses
Days post-‐travel
7
E/ology of fever according to interval axer travel
Wilson ME. CID. 2007.
Rickettsia
P. falciparum
P. vivax
CMV/EBV
Dengue Typhoid
Other
Malaria Other
7 14 21 28 35 42 49 0
Exposures?
• Insect or animal exposures?
• Fresh water exposure?
• What did they consume?
• Other ill travelers?
• Sexual ac/vity?

2/25/11
19
Specific symptoms or exam findings?
• Symptoms – Diarrhea? – Abdominal pain? – Headache?
• Exam findings – Rash? – Lymphadenopathy? – Arthri/s?
Prophylaxis?
• Vaccina/ons? – Which ones?
– Timing of vaccina/ons?
• Malaria prophylaxis? – Appropriate agents? – Taken appropriately?
What should your ini/al tes/ng include?
• CBC w/ differen/al • LFTs • Blood cultures x 2 • Thick and thin blood smear x 2
• Urinalysis • CXR • Addi/onal tes/ng based on history/exam

2/25/11
20
Case
• 55 year-‐old male returns from a 2 week trip in S. Africa with 4 days of fever.
Case /meline
21 11 13 3 14 19 18
South Africa Return to US
15
Noticed lesion under waist-band, non-tender
Visit to PCP
“Red spots” on chest, arms
20
UCSF ED
February
Fevers, myalgias, fatigue
Physical Exam
• VS. 38.5, 76, 128/70, 16, 99% RA • Gen: rela/vely well appearing • Exam otherwise unremarkable except…
– Lymph – 1 cm R inguinal LAD, minimal tenderness – Skin – papulovesicular rash and 1x 1 cm eschar

2/25/11
21
Labs and Microbiology
3.8>47<214
Chem 7 – wnl
LFTS – wnl
UA -‐ wnl
Bld Cx X 2 – pending
Thick/thin smear – pending
CXR -‐ clear
Assuming that this is an infec/on what is the mode of transmission?
A. Inges/ng contaminated food or water
B. Mosquito
C. Sexual contact
D. Swimming in contaminated water
E. Tick

2/25/11
22
DIFFERENTIAL DIAGNOSIS?
Geography?
Incubation?
Exposures?
Specific features?
Prophylaxis?
Geography
• Geography: Lompopo Valley, South Africa

2/25/11
23
0
100
200
300
400
500
600
700
800
900
1000
Carribean C. America S. America Sub-‐Saharan Africa
South Central Asia
SE Asia
Cases
Freedman DO. NEJM. 2006.
E/ology of fever according to region traveled
Dengue
Unknown
EBV/CMV
Malaria
Rickettsia
Typhoid
Dengue
Incuba/on
• Incuba/on 3-‐11 days
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0-‐7 7-‐14 14-‐21 21-‐28 28-‐35 35-‐42 >42
Prop
or7on
of D
iagnoses
Days post-‐travel
E/ology of fever according to interval axer travel
Wilson ME. CID. 2007.
Rickettsia
P. falciparum
P. vivax
CMV/EBV
Dengue Typhoid
Other
Malaria Other

2/25/11
24
Exposures
• Big game hunt -‐ denied animal or insect bites
• Denies fresh water exposure
• Denies ea/ng uncooked food/ unfiltered water
• Denies exposure to sick contacts
• Denies any sexual ac/vity
Prophylaxis
• Vaccines – Hep A, Typhoid, Yellow Fever, Rabies
• An/-‐malarial prophylaxis – Yes -‐ Atovaquone/proguanil
Diagnos/cs
• Bld cx x 2 – NGTD
• CXR – clear
• Thick/thin smear – nega/ve

2/25/11
25
Specific exam findings
• Eschar – Plague, Tularemia – Cutaneous anthrax – Brown Recluse Spider – Cutaneous leishmaniasis
– RickeVsial infec/ons: • Ricketssialpox • Mediterranean spoVed fever
• African /ck bite fever
• Papulovesicular rash – Varicella (chickenpox) – Variola (smallpox)
– Measles – Enterovirus infec/ons – RickeVsial infec/ons
• RickeVsialpox • African /ck bite fever • Queensland Tick Typhus
Diagnosis: African /ck-‐bite fever
• Travel to Sub-‐Saharan Africa -‐ #2 cause of febrile illness – rickeVsial disease
• Exposure – direct contact with wild animals
• Incuba/on period -‐ ~ 7 days
• Exam -‐ fever, eschar, papulovesicular rash
African Tick Bite Fever (ATBF)
• ATBF due to infec)on with R. africae • TransmiVed in rural sub-‐Saharan Africa by ungulate /cks
• Southern African bont /ck – Aggressive (oxen mul/ple bites)
– Wild ungulates (giraffes, buffalo)
– 70% infected w/ R. africae

2/25/11
26
ATBF in returning travelers from sub-‐equitorial Africa
• Hun/ng as main purpose of travel (OR 10.18)
• Clinical manifesta/ons: – Fever, Headache, Myalgias – Inocula/on eschar, oxen mul/ple – Regional lymphadeni/s – Rash – maculopapular or papulovesicular
• Treatment – Doxycycline x 7 days
Jensenius M. CID 2003; Jensenius M. Lancet Infect Dis 2003; Rauolt D.N Engl J Med 2001, 344 (20)
Case 2
• 32-‐year-‐old woman developed sudden onset of headache, high fever, and extreme fa/gue 2 days axer returning from Central Mexico
• Complained of flushing over face and chest
• Three days later, developed a generalized “splotchy” rash.

2/25/11
27
Physical Exam
• VS: 38.8, 110/65, 87, 18, 98%/RA • GEN: fa/gued, generally uncomfortable
• HEENT: oropharynx clear • NECK: supple, no meningismus
• CV: tachy no murmur
• CHEST: clear • ABD: benign, no HSM
Skin findings
Laboratory findings
• CBC: 1.5 >48.9<37 • Cr -‐ 0.9 • AST/ALT – 124/87 • AP, Bili, PT, PTT -‐ wnl
2/25/11
28
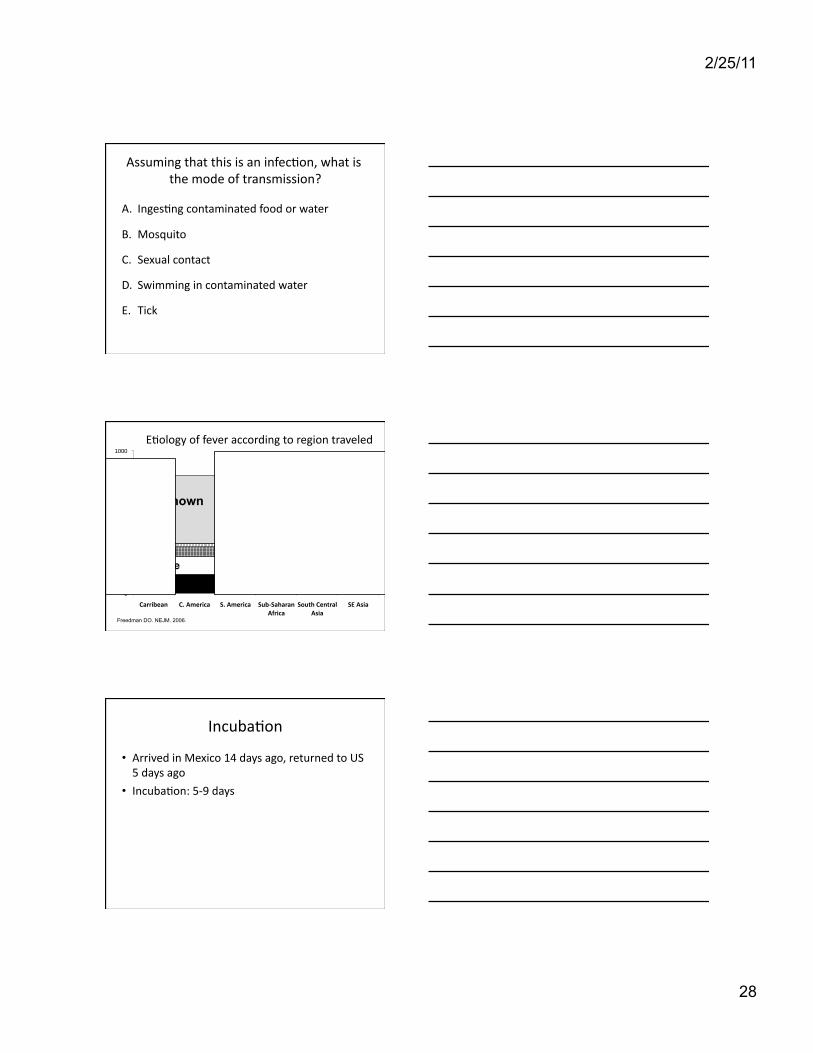
Assuming that this is an infec/on, what is the mode of transmission?
A. Inges/ng contaminated food or water
B. Mosquito
C. Sexual contact
D. Swimming in contaminated water
E. Tick
0
100
200
300
400
500
600
700
800
900
1000
Carribean C. America S. America Sub-‐Saharan Africa
South Central Asia
SE Asia
Cases
Freedman DO. NEJM. 2006.
E/ology of fever according to region traveled
Dengue
Unknown
EBV/CMV
Malaria
Rickettsia
Typhoid
Dengue
Incuba/on
• Arrived in Mexico 14 days ago, returned to US 5 days ago
• Incuba/on: 5-‐9 days

2/25/11
29
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0-‐7 7-‐14 14-‐21 21-‐28 28-‐35 35-‐42 >42
Prop
or7on
of D
iagnoses
Days post-‐travel
E/ology of fever according to interval axer travel
Wilson ME. CID. 2007.
Rickettsia
P. falciparum
P. vivax
CMV/EBV
Dengue Typhoid
Other
Malaria Other
Diagnos/cs
• Blood culture x 2 – No growth
• Thick and thin smear – nega/ve
Diagnosis: Dengue fever
• Travel to C. America -‐ #1 -‐ dengue fever
• Incuba/on period – 7-‐12 days • Unique findings– rash, leukopenia, thrombocytopenia, transamini/s
• Dengue virus /ters -‐ IgM 11.78, IgG< 0.5

2/25/11
30
Dengue fever: Clinical manifesta/ons
• Dengue Fever – Severe headache – Myalgias and arthralgias – Nausea and vomi/ng – Rash: Generalized erythema -‐>maculopapular w/ petechiae
• Dengue Hemorrhagic Fever
• Lab abnormali/es: ↓WBC/PLT, ↑ AST/ALT
Dengue fever: Rx/preven/on
• Treatment is suppor/ve
• No vaccine available
• Preven/on of mosquito exposure – Avoid endemic areas
– DEET – Premetherin treated clothing

2/25/11
31
Summary • Preven/on of infec/on is best
– Educa/on, immuniza/on, prophylaxis
• DDx infec/ons of traveler is finite – Use resources
• Detailed history and exam helps to narrow DDx – Specific des/na/ons – Dura/on of stay (incuba/on period) – Ac/vi/es – Exposures
Ques/ons?