Embed Size (px)
Citation preview

See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/20606969
Traumatic sternal segment dislocation
Article in Chest · October 1989
DOI: 10.1378/chest.96.3.684 · Source: PubMed
CITATIONS
19
READS
69
5 authors, including:
Some of the authors of this publication are also working on these related projects:
Bioartificial Liver View project
Yoshito Ikada
Nara Medical University
884 PUBLICATIONS 35,818 CITATIONS
SEE PROFILE
All content following this page was uploaded by Yoshito Ikada on 22 May 2014.
The user has requested enhancement of the downloaded file.
DOI 10.1378/chest.96.3.684 1989;96;684-686Chest
S Watanabe, T Nakamura, Y Shimizu, S Hitomi and Y Ikada Traumatic sternal segment dislocation in a child.
http://chestjournal.chestpubs.org/content/96/3/684
can be found online on the World Wide Web at: The online version of this article, along with updated information and services
) ISSN:0012-3692http://chestjournal.chestpubs.org/site/misc/reprints.xhtml(without the prior written permission of the copyright holder.reserved. No part of this article or PDF may be reproduced or distributedChest Physicians, 3300 Dundee Road, Northbrook, IL 60062. All rights
ofbeen published monthly since 1935. Copyright1989by the American College is the official journal of the American College of Chest Physicians. It hasChest
© 1989 American College of Chest Physicians by guest on July 10, 2011chestjournal.chestpubs.orgDownloaded from

684 fraumatic Sternal Segment Dislocation (I�%btanabe et a!)
and necessitates radiation exposure, the 2D echocardiogram
is the most reliable and simplest test to perform foridentification ofleft ventricular thrombi.
Despite the controversy over the value of anticoagulationin reducing the mortality after an AM!, all trials have shown
a reduction in thromboembolic complications both clinicallyand at autopsy.
Pulmonary emboli in a setting of MI originate primarily
in deep venous thromboses ofthe lower extremities. To date,
the right ventricle has not been studied or reported as asource of embolization in MI, although as previously noted
right ventricular mural thrombi have been described inassociation with blunt chest trauma,#{176}right-sided catheten-zation,3 and in RVMI at necropsy.”#{176}’#{176}Controversy regarding
the prevalence of the RV mural thrombi in autopsy studies
by Wade’#{176}and Isner et al” (80 percent and 9 percent,
respectively), plus rarity of this condition in actual clinicalsetting, could indicate that most ofthrombi in RV, ifany, areoverlooked or not pursued diagnostically. Alternatively, it is
possible that the incidence of RV mural thrombi during
acute RVMI is minimal and the high incidence of thrombus
in autopsy series may represent a select population. Review
ofthe literature failed to reveal any case report of pulmonary
embolic event related to RV infarction. Since a significant
portion of inferior MIs are associated with RVMI, careful
evaluation of the area, especially with a four-chamber apicalview by 2D echocardiographic study, should be considered
in appropriate cases. Even though 2D echo was able to
detect the RV thrombi in blunt chest trauma patients,2 the
peculiar muscular trabeculae, chordal structures and prom-inent papillary muscles might make this test unsuitable tostudy the RV for thrombi compared with the left side.
We believe that events leading to RV mural thrombi may
have the same pathophysiologic and similar natural historyas LV mural thrombi. We suggest that those patients
clinically thought to have RV infarction should undergo
careful evaluation by echocardiography (which has been
shown to be the superior study in evaluating LV thrombi).
This small subgroup of RV infarction with mural thrombishould then be anticoagulated and followed serially.
ACKNOWLEDGMENT: We wish to express grateful appreciationto Archie F Wilson, M.D. , Ph.D. for his expertise in editing thismanuscript.
REFERENCES
1 IsnerJM, Robert WC. Right ventricular infarction complicating
left ventricular infarction secondary to coronary heart disease.Am J Cardiol 1978; 42:885-94
2 Kessler KM, Mallon SM, Bolooki H, Myerburg RJ. Peduncu-
lated right ventricular thrombus due to repeated blunt chesttrauma. Am Heart J 1981; 102:1064-66
3 Phibbs B, Marriott HJ. Complication ofpermanent transvenous
pacing. N Engl J Med 1985; 22:1428-314 Stowers SA, Leiboff RH, Wasserman AG. Right ventricular
thrombus formation in association with acute myocardial infarc-
lion. Am J Cardiol 1983; 52:912-13
5 Reeder CS, Lengyel M, Tajik AJ, Seward JB, Smith HC,Danielson CK. Mural thrombus in left ventricular aneurysm.Mayo Clin Proc 1981; 56:77
6 Stratton JR, Lighty CW, Pearlman AS, Ritchie JL. Detection ofleft ventricular thrombus by two dimensional echocardiography:
sensitivity, specificity and causes of uncertainty. Circulation
1982;66:156
7 Barnett HJM. Heart in ischemic stroke-a changing emphasis.Neruol Clin 1983; 1:291-313
8 Stratton JR. Ritchie JL, Hammermeister KE, Kennedy JW,
Hamilton CW. Detection of left ventricular thrombi by radio-nucide angiography. Am J Cardiol 1981; 48:565
9 Stratton JR, Ritchie JL, Hamilton JW, Hammermeister KE,Harker LA. Left ventricular thrombi: in-vivo detection by
indium-ill platelet imaging and two-dimensional echo cardi-
ography. Am J Cardiol 1981; 47:874
10 Wade WC. The pathogenesis ofinfarction ofthe right ventricle.Br Heart J 1959; 21:545-54
11 IsnerJM, Roberts WC. Right ventricular infarction complicatingleft ventricular infarction secondary to coronary heart disease.
Am J Cardiol. 1978; 42:885-94
Traumatic Sternal SegmentDislocation in a ChildSatoshi Watanabe, M.D.;* Tatsuo Nakamura, M.D.;t
Yasuhiko Shimizu, M.D.;t Shigeki Hitomi, M.D., EC.C.P;* and
Yoshito Ikada, Ph.D.t
We present an extremely rare case of traumatic dislocationofa sternal body segment in a child. We treated this sternalsegment dislocation by means of open reduction using anewly developed pin made from poly-L-lactide containing
10 percent by weight hydroxyapatite. It is not necessary toremove this type of pin later because it is degradable andabsorbed within the body within about one year after
implantation. A two-year follow-up of this case revealed agood clinical result. (Chest 1989; 96:684-86)
eports of fractures of the sternum in children seldom
appear in the literature. Dislocation of a sternalsegment in a child is also extremely rare. Recently wesurgically treated a child with dislocation of a sternal body
segment by reduction using a bioabsorbable pin made frompoly-L-lactide and containing hydroxyapatite.
CASE REPORT
A three-year-old girl bent forward and complained of anteriorchest pain after her body had been caught in a narrow iron fence
at her home at the end of April, 1986. After consultation with a
doctor at a nearby hospital, roentgenograms confirmed a sternalsegment dislocation. After a follow-up ofabout two months, she was
admitted to our department on June 27 for further investigation of
the sternal segment dislocation. Although unevenness in the upper
portion of the sternum was palpable, there was no complaint of
oppressive tenderness at that point. Respiratory and cardiac sounds
were normal. Laboratory results on admission showed no abnormal
findings, for instance, negative C-reactive protein and normal
electrocardiogram. A lateral chest x-ray film revealed an inner
depression of the first segment of the sternal body, although no
abnormality was noted within the bony structure on a posteroante-
rior x-ray film (Fig 1). We decided to perform open reduction of
this sternal segment dislocation because the first segment of the
*Depar�ent of Thoracic Surgery, Chest Disease Research Insti-
bite, Kyoto University, Kyoto, Japan.tResearch Center for Medical Polymers and Biomaterials, Kyoto
University, Kyoto, Japan.Reprint requests: Dt W.ztanabe, Research Center jbr MedicalPolymers and Bicmaterials K�to Universit�,#{231}Shogoin, Sak�p-ku,Kipto 606, Japan
© 1989 American College of Chest Physicians by guest on July 10, 2011chestjournal.chestpubs.orgDownloaded from

FIGURE 1 . Preoperative chest roentgenograms. The lateral film demonstrates inner depression of the first
segment ofthe sternal body (arrow), although no abnormality is apparent within the bony structure on the
posteroanterior film.
�L1
CHEST I 96 I 3 1 SEPTEMBER, 1989 685
sternal body showed severe displacement toward the interior. On
J uly 4, we exposed the upper portion of the sternum by means of
an approximately 4-cm long transverse skin incision of the anterior
chest. The first segment ofthe sternal body was displaced interiorly
at almost a right angle in the second intercostal space, and�r
FIGURE 2. Photographs taken during surgery, showing the reduction
of the dislocated segment of the sternal body. Upper: Isolation of
the dislocated segment (arrow). Lower: Reduction of the dislocated
segment with a bioabsorbable pin made from poly-L-lactide and
containing 10 percent by weight hydroxyapatite.
connective tissue lay between the dislocated segment and the
sternal manubrium. We isolated this dislocated segment (measuring
about 1.5 x 1.0 cm) and reduced it by pinning with a bioabsorbable
poly-L-lactide pin containing 10 percent by weight hydroxyapatite
(Fig 2). We fixed and reinforced this reduction of the segment by
suturing with five pieces of 3-0 Vicryl thread. It was necessary to
restrict the patient’s body movement using a thoracic bandage for
one week after the operation and to sedate her using a sedative
when we removed the drainage tube and skin suture threads. The
patient was discharged from the hospital uneventfully on July 21.
We followed her postoperative course by chest roentgenography for
two years. Lateral chest x-ray films demonstrated good results with
regard to reduction of the dislocated sternal segment, although
atrophic change in the isolated segment and slight inner depression
of the sternum were seen (Fig 3).
DISCUssION
There have been few reports of fractures of the sternum
in children.I2 The sternum is anatomically protected from
fracture by surrounding ligaments and cartilaginous attach-
ments to the ribs. In children, these structures are even
more elastic and the ribs are more flexible than in adults,
making a child’s sternum even less susceptible to fracture.
Dislocation of a sternal segment in children also is a rare
event. The segments start to ossify early in childhood, but
synostosis formation between the segments starts in about
the seventh year. Our present patient sustained a traumatic
dislocation of the first segment ofthe sternal body when her
chest became compressed in an iron fence. We were able to
collect only a few case reports from the literature of sternal
segment dislocation in children. These included an unusual
case involving a five-year-old boy who suffered a truly
spontaneous segment dislocation of the sternal body due to
bone necrosis. The authors reported that surgery was
necessary in order to remove the displaced segment.3
Another case involved a ten-year-old boy, who suffered
traumatic separation ofthe sternal body synchondrosis while
wrestling. He was treated by open reduction and fixation of
the separated segment with Kirschner wires.4
© 1989 American College of Chest Physicians by guest on July 10, 2011chestjournal.chestpubs.orgDownloaded from
686 Pleuroperitoneal Shunt (�pe, Joseph)
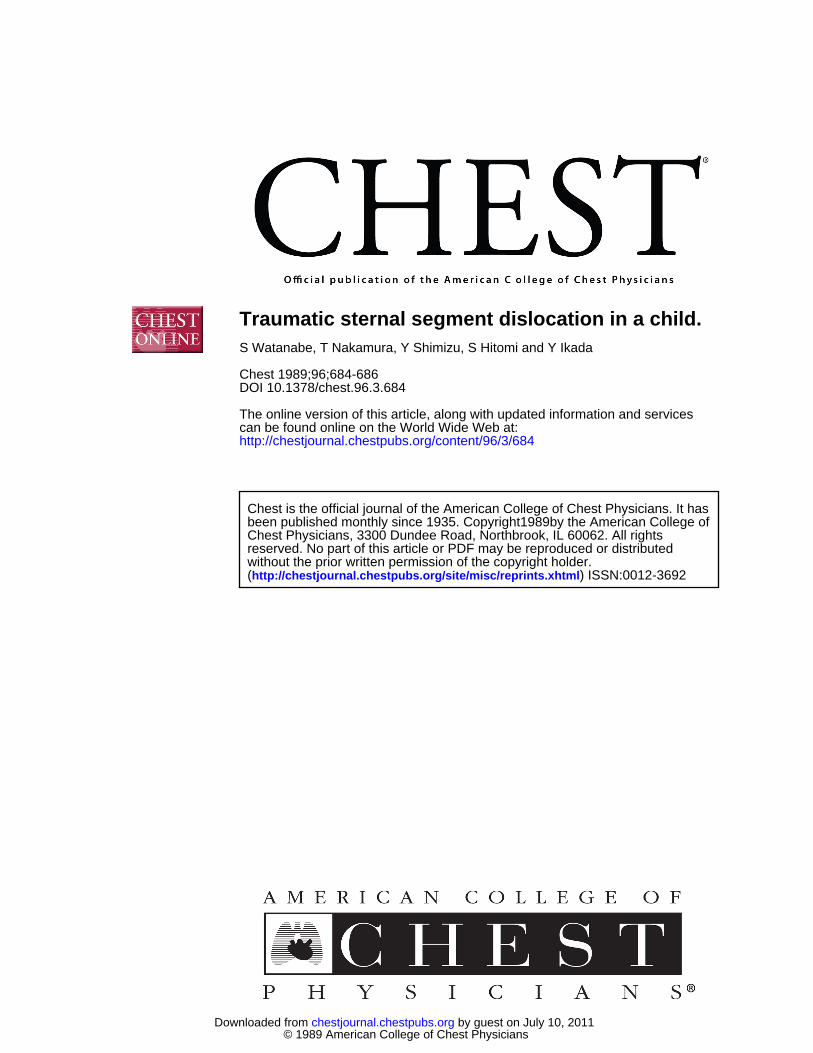
FIGURE 3. Follow-up lateral chest roentgenogram obtained twoyears after the operation showing good results with regard to
reduction of the dislocated sternal segment.
We have developed bioabsorbable rib-connecting pins
made from poly-L-lactide and containing 5 to 10 percent by
weight hydroxyapatite, which have a high modulus of
elasticity and bending strength produced by being drawn in
a uniaxial direction.� These pins have shown excellent
compatibility with bony tissue and no significant inflamma-
tory reactions, and were found to be absorbed about one
year after implantation in animal experiments using mongreldogs.� We applied our biodegradable pin for reduction of
the severe dislocation of the sternal body segment in thepresent patient and obtained good clinical results after a
two-year follow-up.
REFERENCES
1 Perez FL, Coddington RC. Case report: a fracture ofthe sternum
in a child. J Pediatr Orthop 1983; 3:513-15
2 James T Curiosa paediatrica. XI: sternal fracture. S Afr Med J1987; 71:124-25
3 Scudamore CH, Ashmore PG. Spontaneous sternal segment
dislocation: a case report. J Pediatr Surg 1982; 17:61-63
4 Okada M, Tsuchiya M , Ochi K, Suzuki H. Traumatic separation
of the sternal synchondrosis: a case report. J Kanto Orthop
Traumat 1984; 15:116-195 Nakamura T, Isobe J, Ike 0, Watanabe S, Shimizu Y, Shimamoto
T, et al. Experimental study on bioabsorbable rib-connectingpins prepared from poly-L-Iactide containing hydroxyapatite.
Japan J ArtifOrgans 1987; 16:1419-22
6 Nakamura T, Hitomi S, Watanabe S, Shimizu Y, Jamshidi K,Hyon SH, et al. Bioabsorption of polylactides with different
molecular properties. J Biomed Mater Res (in press)
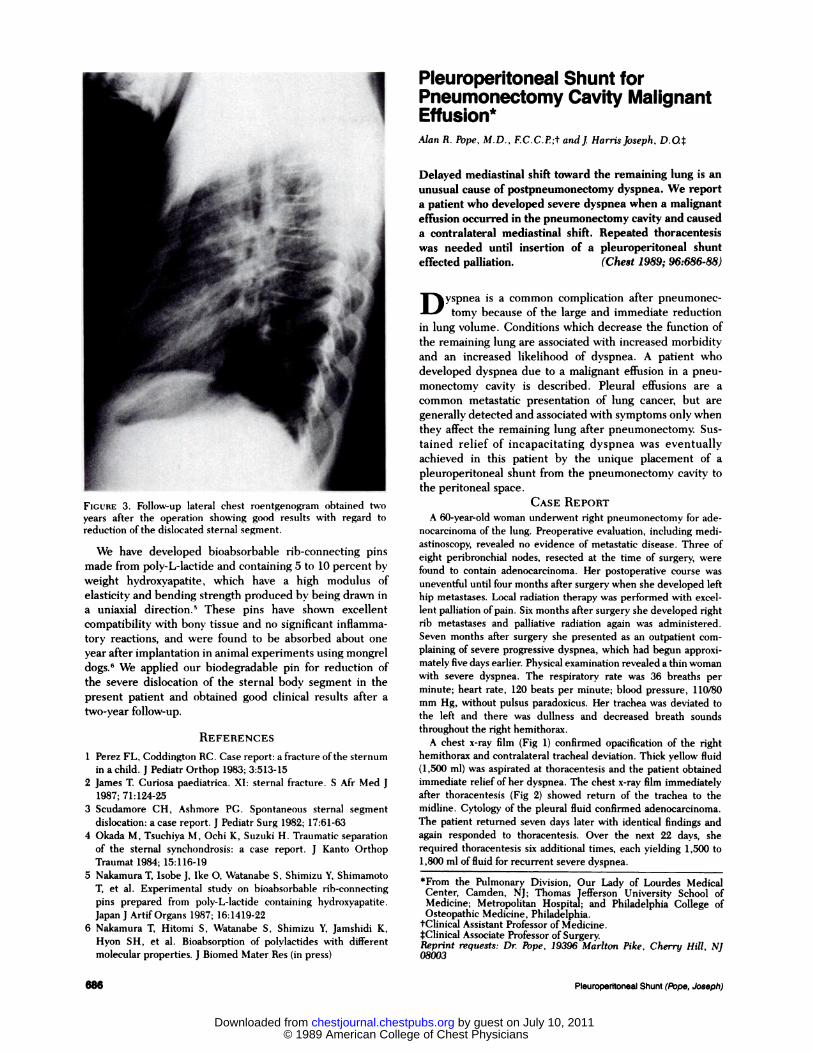
Pleuroperitoneal Shunt forPneumonectomy Cavity MalignantEffusion*Alan R. Pope, M.D., F.C.C.P;t andj HarrisJoseph, D.04
Delayed mediastinal shift toward the remaining lung is an
unusual cause of postpneumonectomy dyspnea. We report
a patient who developed severe dyspnea when a malignant
effusion occurred in the pneumonectomy cavity and causeda contralateral mediastinal shift. Repeated thoracentesiswas needed until insertion of a pleuroperitoneal shunt
effected palliation. (Chest 1989; 96:686-88)
D yspnea is a common complication after pneumonec-
tomy because of the large and immediate reduction
in lung volume. Conditions which decrease the function of
the remaining lung are associated with increased morbidity
and an increased likelihood of dyspnea. A patient who
developed dyspnea due to a malignant effusion in a pneu-
monectomy cavity is described. Pleural effusions are a
common metastatic presentation of lung cancer, but are
generally detected and associated with symptoms only when
they affect the remaining lung after pneumonectomy. Sus-
tamed relief of incapacitating dyspnea was eventually
achieved in this patient by the unique placement of a
pleuroperitoneal shunt from the pneumonectomy cavity to
the peritoneal space.
CASE REPORT
A 60-year-old woman underwent right pneumonectomy for ade-nocarcinoma of the lung. Preoperative evaluation, including medi-
astinoscopy, revealed no evidence of metastatic disease. Three of
eight peribronchial nodes, resected at the time of surgery, were
found to contain adenocarcinoma. Her postoperative course was
uneventful until four months after surgery when she developed left
hip metastases. Local radiation therapy was performed with excel-
lent palliation ofpain. Six months after surgery she developed right
rib metastases and palliative radiation again was administered.
Seven months after surgery she presented as an outpatient com-plaining of severe progressive dyspnea, which had begun approxi-
mately five days earlier. Physical examination revealed a thin womanwith severe dyspnea. The respiratory rate was 36 breaths per
minute; heart rate, 120 beats per minute; blood pressure, 110/80mm Hg, without pulsus paradoxicus. Her trachea was deviated tothe left and there was dullness and decreased breath sounds
throughout the right hemithorax.
A chest x-ray film (Fig 1) confirmed opacification of the right
hemithorax and contralateral tracheal deviation. Thick yellow fluid
(1 ,500 ml) was aspirated at thoracentesis and the patient obtained
immediate relief of her dyspnea. The chest x-ray film immediatelyafter thoracentesis (Fig 2) showed return of the trachea to the
midline. Cytology of the pleural fluid confirmed adenocarcinoma.
The patient returned seven days later with identical findings and
again responded to thoracentesis. Over the next 22 days, she
required thoracentesis six additional times, each yielding 1 ,500 to
1,800 ml of fluid for recurrent severe dyspnea.
*From the Pulmonary Division, Our Lady of Lourdes Medical
Center, Camden, NJ; Thomas Jefferson University School ofMedicine; Metropolitan Hospital; and Philadelphia College ofOsteopathic Medicine, Philadelphia.
tClinical Assistant Professor of Medicine.
tClinical Associate Professor of Surgery.Reprint requests: Dr. Pope, 19396 Marlton Pike, Cherry Hill, NJo8cK�’3
© 1989 American College of Chest Physicians by guest on July 10, 2011chestjournal.chestpubs.orgDownloaded from

DOI 10.1378/chest.96.3.684 1989;96; 684-686Chest
S Watanabe, T Nakamura, Y Shimizu, S Hitomi and Y IkadaTraumatic sternal segment dislocation in a child.
July 10, 2011This information is current as of
http://chestjournal.chestpubs.org/content/96/3/684Updated Information and services can be found at:
Updated Information & Services
http://www.chestpubs.org/site/misc/reprints.xhtmlonline at: Information about reproducing this article in parts (figures, tables) or in its entirety can be foundPermissions & Licensing
http://www.chestpubs.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
Reprints
the right of the online article.Receive free e-mail alerts when new articles cite this article. To sign up, select the "Services" link to
Citation Alerts
slide format. See any online figure for directions. articles can be downloaded for teaching purposes in PowerPointCHESTFigures that appear in Images in PowerPoint format
© 1989 American College of Chest Physicians by guest on July 10, 2011chestjournal.chestpubs.orgDownloaded from
View publication statsView publication stats