Embed Size (px)
Citation preview

Surgical Neurolog
Aneurysm
Traumatic middle meningeal artery aneurysm causing intracerebral
hematoma: a case report and review of literature
Manmohan Singh, Mch4, Faiz Uddin Ahmad, MBBS, Ashok K. Mahapatra, MchDepartment of Neurosurgery, All India Institute of Medical Sciences, Ansari Nagar, New Delhi-110029, India
Received 7 October 2005; accepted 10 November 2005
Abstract Background: Traumatic aneurysms of middle meningeal artery (MMA) are rare. Traumatic MMA
www.surgicalneurology-online.com
0090-3019/$ – see fro
doi:10.1016/j.surneu.2
Abbreviations: C
hematoma; MMA, m
STA, superficial temp
4 Corresponding
11 26588207.
E-mail address: m
aneurysms usually present with extradural hematomas, whereas intradural intraparenchymal
hematomas are exceedingly rare.
Case Discussion: We report a 30-year-old man who presented 1 year after head injury with
spontaneous right frontal intraparenchymal hematoma. Investigations revealed a MMA pseudoa-
neurysm, which was successfully treated surgically.
Conclusion: Traumatic MMA pseudoaneurysm producing intracerebral hematoma (ICH) is rare and
can be listed as a cause of spontaneous acute ICH.
D 2006 Elsevier Inc. All rights reserved.
Keywords: Head injury; Intracerebral hematoma; Middle meningeal artery; Posttraumatic; Pseudoaneurysm
1. Introduction
Traumatic aneurysms of MMA are rare, and they usually
present with extradural hemorrhage [2,3]. Such lesions
presenting with ICH are extremely rare. It is important to
diagnose and treat these aneurysms at the earliest to prevent
catastrophic events. Association of MMA traumatic aneur-
ysms with skull fractures has been well documented [5,7].
In patients in whom fracture line crosses the MMA,
possibility of false aneurysm should be kept in mind.
Patients with traumatic pseudoaneurysms are more likely to
have delayed bleeds, which accounts for typical prolonged
lucid interval. This may explain the delayed appearance of
intracranial hemorrhages on CT scans. To the best of the
authors’ knowledge, only 2 such cases, who presented with
ICH, have been described in English literature [1,7]. We
report a patient with traumatic pseudoaneurysm of MMA,
who presented with spontaneous frontal intraparenchymal
hematoma, 1 year after trauma.
nt matter D 2006 Elsevier Inc. All rights reserved.
005.11.029
T, computerized tomography; ICH, intracerebral
iddle meningeal artery; MR, magnetic resonance;
oral artery.
author. Tel.: +91 11 26588700x4914; fax: +91
[email protected] (M. Singh).
2. Case report
A 30-year-old man was admitted in February 2004, after
a road traffic accident, with history of unconsciousness for
20 minutes. On admission, patient was conscious but
irritable. Plain CT scan of head showed bifrontal contusions
without significant mass effect (Fig. 1). He was managed
conservatively and discharged 1 week later. In January
2005, he was admitted with complaints of sudden onset of
severe headache and one episode of generalized seizure.
Computed tomography scan of the head revealed a
hematoma in the right frontal lobe (Fig. 2). Because there
was no history of trauma immediately preceding his
symptoms, an angiogram was done to ascertain the cause
of bleed. Angiogram revealed a pseudoaneurysm, arising
from MMA (Fig. 3). He was taken up for surgery, and right
frontal craniotomy was performed. There was no extradural
hematoma, and surface of the dura was apparently normal.
On dural opening, the brain cortex was stuck to the dura.
The dura was gently separated of the cortex. On the inner
surface of dura, there was an irregular-shaped aneurysm
arising from the MMA, penetrating the cortex of the frontal
lobe. The parent vessel along with the aneurysm was
coagulated. Frontal hematoma was evacuated. Patient made
a good postoperative recovery and was well after 8 months
of follow-up.
y 66 (2006) 321–323

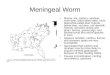
Fig. 2. Noncontrast CT scan of head showing right frontal lobe hematoma
with mass effect.
M. Singh et al. / Surgical Neurology 66 (2006) 321–323322
3. Discussion
Traumatic aneurysms of the MMA, although rare in
occurrence, have been known as an etiology of acute
epidural hematoma of delayed onset [2,3]. Schulze [10]
reported the first case of traumatic MMA aneurysm in 1957.
Until 2002, Bruneau et al [1] had reviewed 40 cases of
traumatic MMA aneurysms reported in the world literature.
However, such aneurysms causing ICH are distinctly rare.
There are only 2 cases of ICHs caused by rupture of
traumatic MMA pseudoaneurysms reported in English
literature until now [1,7]. Bruneau et al [1] reported a
64-year-old woman who suffered a massive spontaneous
intracerebral frontotemporal hemorrhage with ventricular
spread, caused by a traumatic pseudoaneurysm of the
MMA. Despite surgical evacuation, the patient died after
24 hours. Rambaugh et al [7] reported a 63-year-old woman
who presented with right temporal hematoma, and angiog-
raphy revealed an MMA false aneurysm at the level of
sphenoid ridge. The patient made a good recovery after
surgical evacuation of the hematoma. Two cases of non-
traumatic MMA aneurysms causing ICH have also been
described in literature [9,11]. Ushikoshi et al [11] reported
a patient with ICH caused by a nontraumatic aneurysm
arising from MMA that provided collateral flow to poste-
rior cerebral artery territory, after the parent artery was
blocked by atherosclerotic disease. Sandin et al [9] reported
a 46-year-old man who developed a spontaneous tempor-
oparietal hematoma after rupture of such an aneurysm. In
the reported cases, the usual delay between trauma and
abrupt neurologic deterioration varies from 3 to 30 days [8].
However, present case is unique in this respect, presenting
1 year after trauma. This, we believe, is the longest reported
delay in presentation until now.
The natural history of these aneurysms is not completely
known, but they have been demonstrated to grow on repeat
angiograms [6]. It is thought that they develop after a small
Fig. 1. Noncontrast CT scan of head showing bifrontal contusions.
tear in the meningeal artery, which is sealed off by a clot,
recanalizing later and forms a false lumen. These pseudoa-
neurysms gradually enlarge and rupture anytime [1]. Hence,
this aneurysm must always be treated expeditely, especially
because the surgical management is technically easy.
Kinoshita et al [4] recommended that the cases of
epidural hematoma treated conservatively should be fol-
lowed up by MR imaging and MR angiography using the fat
suppression technique to rule out formation of pseudoa-
neurysms. The presence of traumatic pseudoaneurysm
should be considered in those patients who show delayed
and abrupt neurologic deterioration because of the ICH after
head injury. In these patients, angiography should also
include external carotid artery injections, including manual
compression and occlusion of STA to remove confusion
from overlapping of STA branches [8].
Fig. 3. Right external carotid artery injection shows MMA aneurysm
(black arrow).

M. Singh et al. / Surgical Neurology 66 (2006) 321–323 323
4. Conclusion
Rupture of MMA pseudoaneurysm should be kept in
mind in the differential diagnosis of patients presenting with
delayed onset of intracranial hematoma after trauma.
Carotid artery angiography with external carotid artery
injection should be performed to rule out pseudoaneurysm
of MMA. Such patients should be managed surgically at the
earliest to prevent rebleed.
References
[1] Bruneau M, Gustin T, Zekhnini K, Gilliard C. Traumatic false
aneurysm of the middle meningeal artery causing an intracerebral
hemorrhage: case report and literature review. Surg Neurol 2002;57:
174 -8.
[2] Garza-Mercado R, Rangel RA. Extradural hematoma associated with
traumatic middle meningeal artery pseudo aneurysm. Report of two
cases. Neurosurgery 1979;5:200 -3.
[3] Kimora T, Sako K, Satoh M, Nakai H, Yonemasu Y, Takeuchi E,
Ishikura H. Post-traumatic pseudoaneurysm of the middle meningeal
artery. A case report. No Shinkei Geka 1995;23:1021-5.
[4] Kinoshita Y, Yasukouchi H, Tsuru E, Okudera T, Yokota A. Delayed
epidural bleeding caused by traumatic pseudo-aneurysm of the middle
meningeal artery: case report. No Shinkei Geka 2004;32:1139-43.
[5] Kuhn RA, Kugler H. False aneurysms of middle meningeal artery.
J Neurosurg 1950;7:106-14.
[6] Meder JF, Gaston A, Merienne L, Godon-Hardy S, Fredy D.
Traumatic aneurysms of the internal and external carotid arteries.
One case and review of literature. J Neuroradiol 1992;19:248-55.
[7] Rambaugh CL, Bergeron T, Kurze T. Intracranial vascular damage
associated with skull fracture: radiological aspects. Radiology 1972;
104:81-7.
[8] Roski RA, Owen M, White RJ, Takaoka Y, Bellon EM. Middle
meningeal artery trauma. Surg Neurol 1982;17:200 -3.
[9] Sandin JA, Salamat SA, Baskaya M, Dempsey RJ. Intracerebral
hemorrhage caused by the rupture of a non-traumatic middle
meningeal artery aneurysm. J Neurosurg 1999;90:951 -4.
[10] Schulze A. Seltene verlaufsformen epiduraler hamatome. Zentralbl
Neurochir 1957;17:40 -7.
[11] Ushikoshi S, Houkin K, Itoh F, et al. Ruptured aneurysm of the middle
meningeal artery associated with occlusion of the posterior cerebral
artery. J Neurosurg 1996;84:269-71.
Commentary
It is nice to learn from this case that a traumatic aneurysm
of the middle meningeal artery can cause an intracerebral
hematoma 1 year later, without an extradural hematoma.
Gerard Debrun, MD
29360 Paris, France

















![Prognostic models for intracerebral hemorrhage: systematic ......related ICH Equation Discharge Hematoma diameter and CT signs of ischemia. – Bhatia [65] 2013 Primary ICH Equation](https://img.pdfslide.us/doc/110x75/60f59ef972fda8313e2cbea5/prognostic-models-for-intracerebral-hemorrhage-systematic-related-ich-equation.jpg)