Embed Size (px)
Citation preview

Traumatic Brain Injury&
Brain TumorsFall 2009
John Nation, RN, MSNAdapted from the notes of Marnie
Quick, RN, MSN and Charlene Morris, RN, MSN

The Brain!

Have you read Lewis pages 1481 -1493?
1. Of Course.2. Not yet, but I will
within the next 48 hours.
3. Could you repeat the question?

The Brain

Brain A & PThree major components-Cerebrum
• Right and left hemispheres• Four lobes- frontal, temporal, parietal, and occipital
Frontal Lobe-• Cognitive function• Memory retention• Voluntary eye and motor movements• Expressive speech via Broca’s area
Temporal Lobe-• Speech reception via Wernicke’s area• Visual and auditory integration
Parietal Lobe-• Spatial information and control
Occipital Lobe-• processing of sight

Brain A & P (Cont’d)
Brainstem-– Includes midbrain, pons, and medulla– Respiratory function– Vasomotor function– Cardiac function– Centers for sneezing, coughing, vomiting, sucking,
swallowing, and hicupping

Brain A & P (Cont’d)
Cerebellum-– Located under the occipital lobe of the cerebrum– Coordinates voluntary movement– Trunk stability– Equilibrium

Incidence of Traumatic Brain Injury
• 1.1 million people treated and released annually in the US
• 50,000 people die and 235,000 are hospitalized
• 22% of hospitalized clients die• Men twice as likely to have TBI as
women

Incidence (Cont’d)
• Mortality rate after severe head injury around 35%
• More than half of people who survive severe head injury have serious disability

Risks
• Motor Vehicle Accidents (MVA) - 42,642 deaths due to MVA in 2006 - 3,475 deaths in Texas alone• Elevated Blood Alcohol Levels• Sports-related Trauma• Recreational Activities- Cliff jumping, rock
climbing, mountain biking, etc.• Assault- Firearms, blunt trauma

Brack ED Research

Mechanisms of Injury
• Acceleration Injury- struck in head by a moving object
• Deceleration Injury- head hit non-moving object
• Blunt or penetrating injury to the brain• Closed head injury

Mechanisms of Injury (Cont’d)
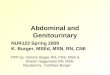
• Coup-countercoup injury- brain rebounds within skull, causing injuries at site of impact (coup) and directly opposite (countercoup)
• Countercoup injury often more severe
Source: Patrick J. Lynch, Creative Commons License 2006

Types of Head Injury
Scalp Lacerations- - external - extensive bleeding secondary to lots of
blood vessels with poor constrictive abilities - care focused on preventing blood loss and
infection

Skull Fractures
Linear Skull Fracture- • Break in continuity of bone• No alteration of relationships of parts• Frequently associated with low- speed injuries• Dura is intact• Accounts for around 80% of all skull fractures

Skull Fractures (Cont’d)
Depressed Skull Fracture-• Inward indentation of skull• Frequently associated with powerful blow/ mechanism
of injury

Skull Fractures (Cont’d)
Simple Skull Fractures-• No fragmentation or communicating lacerations• Associated with low to moderate impact
Comminuted Skull Fractures-• Multiple fractures with bone fragmentation• Associated with direct, high-momentum impact
Compound Skull Fractures-• Scalp laceration and depressed fracture with
communicating pathway to intracranial cavity

Skull Fracture Locations

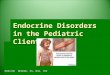
Basilar Skull Fractures
• Fractures along the base of the skull• Can include cranial nerve deficits *Battle’s sign* *Raccoon Eyes*

Battle’s Sign (Postauricular ecchymosis)
Raccoon Eyes(Periorbital ecchymosis)

Basilar Skull Fracture (Cont’d)
Cerebrospinal Fluid (CSF)-• Rhinorrhea- leaking of CSF from the nose• Otorrhea- leaking of CSF from the ear• Client is at high risk for meningitis

Assessment for CSF
• Test fluid for positive glucose reading- CSF gives positive glucose reading
• If blood is also in CSF, testing for glucose is not reliable since blood has glucose as well
• Allow fluid to leak onto 4x4, observe drainage over a few minutes, a yellowish ring around the blood indicates presence of CSF.

Complications of Skull Fracture
• Intracranial infections• Hematoma• Meningeal and brain tissue damage

A client is admitted to the ER with altered level of consciousness and bilateral periobital ecchymosis. Both rhinorrhea and otorrhea are present. The priority nursing diagnosis would be:
Urin
ary
Reten
tion
Ris
k fo
r Infe
ctio
n
Power
less
ness
Dis
turb
ed B
ody Im
age
25% 25%25%25%1. Urinary Retention2. Risk for Infection3. Powerlessness4. Disturbed Body
Image

Types of Skull Fractures (Cont’d)
• Open Skull Fracture- extension of the fracture into the dura or air sinuses
• Closed Skull Fracture- can lead to increased risk for elevated ICP

Minor Brain Injury
• Concussion- – Brief disruption in level of consciousness (LOC)– Retrograde amnesia (difficulty remembering event)– Headache– Usually of short duration– Usually not admitted to hospital if loss of consciousness <
5 minutes

Minor Brain Injury (Cont’d)
• Concussion Precautions: Monitor for:
– worsening headache– Vomiting– Confusion/ change in level of consciousness– Weakness on one side of body– Inability to wake up

Minor Brain Injury (Cont’d)
Post Concussion Syndrome:• Generally 2 weeks to 2 months post injury• Headache, decreased attention span,
personality/ behavioral changes, decreased short term memory, lethargy
• Can significantly impact daily life

Major Head Trauma
Contusion-– Bruising of the brain within an area of the brain– Usually connected with a closed head injury– May involve bleeding, necrosis, and infarction at
the site of a fracture– Clients on anticoagulation therapy with contusion
are at higher risk for severe injury and death– Seizure is a common complication

Major Brain Injury (Cont’d)
Laceration-– Tearing of the brain tissue – Commonly seen with penetrating injuries (ie
gunshot, knife wounds), open fractures, and depressed fractures
– Surgical repair not possible– The larger the area of injury, the worse the
outcome

Major Brain Injury (Cont’d)
Diffuse Axonal Injury (DAI)-– Widespread axonal damage– Can be present with mild to severe TBI– Results in axon swelling and disconnection– Results in decreased LOC, increased ICP, and
global cerebral edema– 90% of clients remain in persistent vegetative
state

Major Brain Injury (Cont’d)
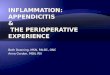
Epidural Hematoma-• Bleeding between the dura and the skull• Is a true emergency• Usually seen with laceration to an artery,
frequently the middle meningeal artery • Frequently initial loss of consciousness
followed by a temporary improvement in condition (called a lucid interval)

Epidural Hematoma (Cont’d)
Signs and Symptoms-– Lucid interval following initial loss of consciousness– Decreased level of consciousness– Headache– Nausea and vomiting– Progresses rapidly
Rapid surgical intervention needed!

Subdural Hematoma
Subdural Hematoma-– Bleed between the outer arachnoid membrane
and the dura mater – Tends to be caused by a venous bleed, though can
be arterial in nature– More common than epidural hematoma– Usually slower to develop than epidural
hematoma

Subdural Hematoma
Signs and Symptoms-– Similar to signs/symptoms of increased ICP– Decreasing LOC– Headache

Types of Subdural HematomasAcute Subacute Chronic
onset 24 to 48hrs p trauma
onset 48 hrs to 2 weeks p
trauma
onset > 20 days p trauma
Immediate decline
Altered mental status
Progressive change in LOC
Tx with craniotomy, evacuation,
decompression
Evacuation and decompression
Evacuation and decompression

Intracerebral Hematoma
Intracerebral hematoma-– Caused by bleeding within the parenchyma (aka
the nervous tissue)– Occurs with around 16% of head injuries

Review
• Scalp lacerations• Skull fractures• Concussions• Contusions• Diffuse Axonal Injury• Epidural Hematoma• Subdural Hematoma• Intracerebral Hematoma

A victim of an automobile accident was found unconscious at the scene of the accident but regained consciousness during transport to the hospital. Shortly after admission, her Glasglow Coma Scale is 8, and an epidural hematoma is suspected. The nurse plans care anticipating the following treatment:
1. IV furosemide2. Immediate
craniotomy3. IV corticosteriods4. Immediate
admission to ICU

Your client with an injury to the brain stem is at risk for which of the following complications?
1. Impaired Balance2. Abnormal hormone
production3. Respiratory
dysfunction4. Impaired temperature
regulation

In planning long-term care for the client following brain trauma, the nurse includes teaching and support for the family primarily because:
1. Clients will always have some residual deficits from the brain trauma
2. Most clients experience seizure disorders in the years following brain trauma
3. Families become dysfunctional and unable to cope during convalesence
4. Clients with head injuries with unconsciousness often have changes in personality with loss of concentration and memory processing

Collaborative Care for TBI
Diagnostic Studies-• CT scan - best diagnostic study to evaluate
head trauma related to rapid diagnosis and treatment
• Spinal x-ray, skull x-ray• MRI• PET (Positron Emission Tomography)• Transcranial Doppler (to measure CSF velocity)

Collaborative Care for TBI (Cont’d)
Diagnostic Tests (Cont’d)-• ABG’s• CBC• Glucose• Electrolytes

Assessment Findings(Pg 1484 in Lewis)
– Fractures/depressions– Battle’s Sign, Raccoon eyes– Cheyne-strokes respirations– Decreased O2 saturation– Pulmonary edema

Assessment Findings (Cont’d)
– Unequal/ dilated pupils– Confusion– Abusive/ slurred speech– Altered LOC– Seizures– Incontinence– Posturing– Glasgow coma scale <12– CSF leaking form ears or nose

Initial Interventions
• Ensure patent airway• Stabilize cervical spine• O2 via non-rebreather• Large bore IV access (2)• Control external bleeding• Ongoing assessment

Ongoing Monitoring (Lewis Pg. 1484)
• Maintain client warmth• Frequent vital signs, level of consiousnes,
SpO2, heart rhythm, Glasgow Coma Scale, pupil size/reactivity
• Assess need for intubation if unable to protect own airway (absent gag reflex)
• Use caution with IV fluids to avoid overload/ increasing ICP

Treatment of TBI
• Prevent secondary injury by managing increased ICP
• Primary treatment is quick diagnosis and surgery if necessary
• In concussion and contusion, usually treated only with observation and management of increased ICP

Managing Increased ICP (At a glance from Module 10)
• Airway management• Elevating head of bed 30 degrees• Temperature regulation• Osmotic diuretics (Mannitol)• Lasix • Invasive monitoring • Surgery

Prevention of Complications
• Medications to prevent increased ICP• Prevent/ treat seizures• Stool softeners to prevent straining• Antipyretics, cooling• TPN, tube feedings, supplements• If CSF leak, do not pack nose/ears, no
suctioning of nose, no blowing/ sniffing of nose. Lightly cover, change PRN,

Surgery for TBI
In depressed and comminuted fractures, frequently a craniotomy to remove fragments– Crainiotomy- opening into the cranium with removal of a
bone flap and opening the dura
If large amount of bone is destroyed, may need:– craniectomy- removal of bone to allow brain to expand– Cranioplasty- repair of a cranial defect using articifial
material

Surgery for TBI (Cont’d)
Acute Subdural and Epidural Hematomas-– Burr-hole openings for rapid decompression– Craniotomy– Drain generally left in place post surgery to
prevent reaccumulation of blood– Evacuation of Subdural Hematoma Video

Nursing Assessment- Review
• Frequent Nuero assessments• Frequent vital signs• Glasgow Coma Scale• Brainstem reflexes (pupils, cough, gag, Doll’s
eyes)• Watch for increased BP, decreased HR, and
altered respirations - Cushing’s Triad- late sign with increased ICP- very bad!
• Watch for CSF leak

Nursing Diagnosis
• Ineffective airway clearance• Ineffective breathing pattern• Ineffective tissue perfusion• Acute pain• Anxiety• Hyperthermia• Decreased cerebral perfusion

Home Care
• Homecare evaluation• Rehabilitation• Nursing home placement• Teaching concerning post-concussion syndrome,
bowel/bladder management, spasticity, dysphagia, nutrition, seizure disorder, personality changs
• Family teaching• Support groups• TBI and Veterans

Ethical Dilemmas
Brain Death-• Coma• Absence of doll’s eyes ocular movements• Absence of pupillary response to light• Gag reflex absent• Complete unresponsiveness• Positive apnea test

Break!
• song• Song
• Tumor Resection

Brain Tumors
• Benign – A growth of cells that is generally slow
growing and non-invasive• Malignant
– A growth of undifferentiated cells that forms an abnormal mass which performs no function and grows at the expense of healthy tissue

• Primary Brain Tumors- a group/mass of cells that starts in the brain
• Secondary (Metastatic) Tumors- a group/ mass of cells that originates outside
the brain

Incidence
• 18,500 new diagnosis in US each year• 12,760 deaths each year related to brain
tumors• 5 year survival rate around 33%• Slightly more prevalent in males than females

Primary Brain Tumors
Primary Brain Tumors-– Rarily metastasize outside the central nervous system– Unknown cause– Most primary brain tumors (around 66%) start in
astrocytes (these tumors are called gliomas)– Greater than 50% of primary brain tumors are malignant– Can occur at any age, but more common in middle age– Must be treated or will lead to death secondary to
increased ICP

A & P Review
• Neurons– Used to communicate motor and sensory information
• Supporting cells (Glial cells):– Surround neurons, and keep them in place– Supply nutrients and oxygen to neurons– Insulate one neuron from another– Remove dead neurons
• Types:– Astrocytes– Oligodendrocytes– Microglia

Types of Primary Brain Tumors(Lewis, pg. 1488)
Gliomas- – Astrocytoma- from supportive, glial cells, and astrocytes.
Low grade to moderate grade malignancy.– Glioblastoma- from primitive stem cell. Highly malignant.– Oligodendroglioma- from oligodendrocytes. Benign– Medulloblastoma- from primitive neuroectodermal cell.
Highly malignant and metastasizes to spinal cord and other parts of the brain.

Type of Brain Tumors (Cont’d)Meningioma- from meninges. Mostly benign but can be
malignantAcoustic Neuroma- from cells that for myelin sheath
around nerves. Usually benign or low-grade malignancy
Pituitary adenonma- originates in pituitary gland. Usually benign.
Hemangioblastoma- from blood vessels of brain. Rare and benign.
Primary CNS lymphoma- forms in lyphocytes. Seen in transplant recipients and AIDS patients

Secondary Brain Tumors
Secondary Brain Tumors-• More common than primary brain tumors• Originate outside the brain, frequently from
lung and breast• Single or multiple brain tumors• Increasing frequency as individuals with
cancer live longer

Clinical Manifestations of Brain Tumors
Clinical Manifestations-– Depend on the location and size of tumor– General symptoms of increased intracranial
pressure- headache, nausea, vomiting, papilledema- increased optic disc swelling
– Seizures

Local Symptoms of Brain Tumors
Frontal Lobe- personality changes, visual disturbances, memory problems, hemiplegia
Parietal Lobe- speech problems, unilateral neglect, spatial disorders, inability to write
Occipital Lobe- visual disturbances and seizuresTemporal Lobe- fewer specific symptoms. When
present, seizures, dysphagia.

Local Symptoms of Brain Tumors (Cont’d)
Cerebellum- gait disturbance, cooridination problems
Brainstem- headache on awakening, visual changes, drowsiness, hearing loss, hemiparesis, dysphagia, dysarthria

Complications
Ventricular enlargement (hydrocephalus)– surgical treatment can be needed to relieve
pressure. – Ventriculoatrial shunt- placement of a shunt with
one way valve from from right lateral ventricle to the right atrium
– Ventriculoperitoneal- placement of a shunt with one way valve from from right lateral ventricle to the peritoneum

Complications (Cont’d)
• Infection- S&S include fever, headache, stiff neck, weakness, seizures
• Death- usually caused by increased intracranial pressure or herniation

Collaborative Care
Diagnostic Tests-– CT Head– MRI– EEG- diagnostic test that measures the electrical
activity of the brain– PET– Angiogram of the head– Tissue Biopsy (usually done in surgery)

Surgery• Used both to remove tumor or for symptom
relief• Complete surgical removal not always an
option secondary to tumor location or involvement of vital parts of the brain– Deep central areas of dominant hemisphere,
posterior corpus callosum, or the upper brainstem are typically considered inoperable

Surgery (Cont’d)
• Supratentorial- cranial surgery above the tenoritum (double fold of dura between the cerebrum and the cerebellum). Post-op HOB up 30-45 degrees
• Infratentorial- surgery below the tentortium- cerebellum and brainstem– HOB angle per MD order

Surgery (Cont’d)
Stereotaxic surgery-– Presision localization of area of brain using 3-
dimensional coordinates– Used for biopsy and dissection– Resection of Brain Tumor Video

Radiation Therapy
• Used alone or with other therapies• Stereotactic radiosurgery
– Closed skull destruction of tumor using intracranial guiding device
– Gamma knife- high dose radiation precisely on tumor
– Surgical lasers also used- create thermal energy to destroy tumor
– Major advantage is decreases damage to surronding tissue

Gamma Knife vs CyberknifeGamma Knife• Fixed head frame
used• Used only on the
head• Uses multiple beams• Isocenter(s) chosen
based on CT findings• Usually 1 doses only• Hospitalized during
treatment
Cyber Knife
• Used on brain and body lesions
• Uses only one beam
• No head frame
• Hospitalization not needed
•X-Rays during treatment used to guide beam

Medications
Chemotherapy- – Limited effectiveness due to blood-brain barrier, tumor-
cell drug resistance, and large variances between types of tumor cells
– Nitrosoureas (CNU, CCNU)– Temozolomide (Temodar)- first agent found to cross
blood-brain barrier– Intrathecal administration delivers to the CNS via Ommaya
Reservoir– Wafer implantion- chemotherapy-laden biodegradeable
wafer placed at tumor site during surgery– Ommaya reservoir

Medications (Cont’d)
• Corticosteroids used to treat edema– Prednisone, Solu-medrol, Decadron
• Anticonvulsants used to prevent seizures– Tegretol, Depakote, Keppra, Neurontin, Lamictal,
Dilantin

Rehabilition
• Coping • Adapting• Assistance as needed• Resources in community

Nursing Assessment
Health History-– Course of symptoms, other cancers
Physical Exam-– Neuro vital signs– Assess for signs of tumor in specific part of brain
(as discussed previously)– Watch for aphasia, visual field loss, motor and
sensory loss– Observe for signs of increased ICP

Nursing Diagnosis
• Impaired tissue perfusion, cerebral• Self-care deficits• Anxiety• Risk for infection• Risk for injury• Acute pain• Disturbed self-esteem• Nutrition• Home care

The End!