Embed Size (px)
Citation preview

Traumatic Brain InjuriesDr. Arif Baradia M. Med (Ortho)Supervisor: Professor Mwangombe
What is Traumatic Brain Injury?
• PROCESS not EVENT
• PRIMARY and SECONDARY BRAIN INJURY
• Penetrating or Non-penetrating
Epidemiology
• 1.5 m per year
MVA 45%Falls 30%Occupational 10%Recreational 10%Assault 5%
Role of Alcohol

Epidemiology
• 40-60% of head injured patients have extremity injury
• 32,000-48,000 head injury survivors with orthopaedic injuries annually

Pathophysiology of Head Injury
• Monroe - Kellie doctrine
CSF 10%
BRAIN 80%
BLOOD 10%
Rigid “Box”Aka The Skull
Cerebral Blood Flow
• 15% C.O
• 750ml/min
• CPP = MAP – ICP maintain above 70 mmHg
Mechanisms of Brain Injury
1.Brain Contusion2.Raised ICP3.Diffuse Axonal Injury4.Stroke
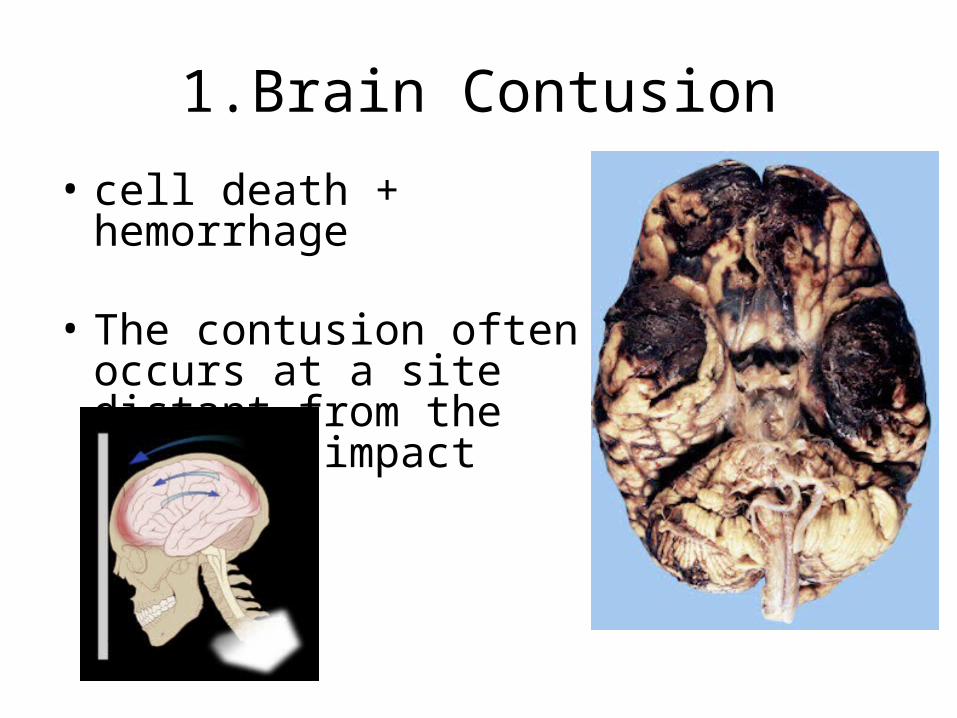
1.Brain Contusion
• cell death + hemorrhage
• The contusion often occurs at a site distant from the point of impact
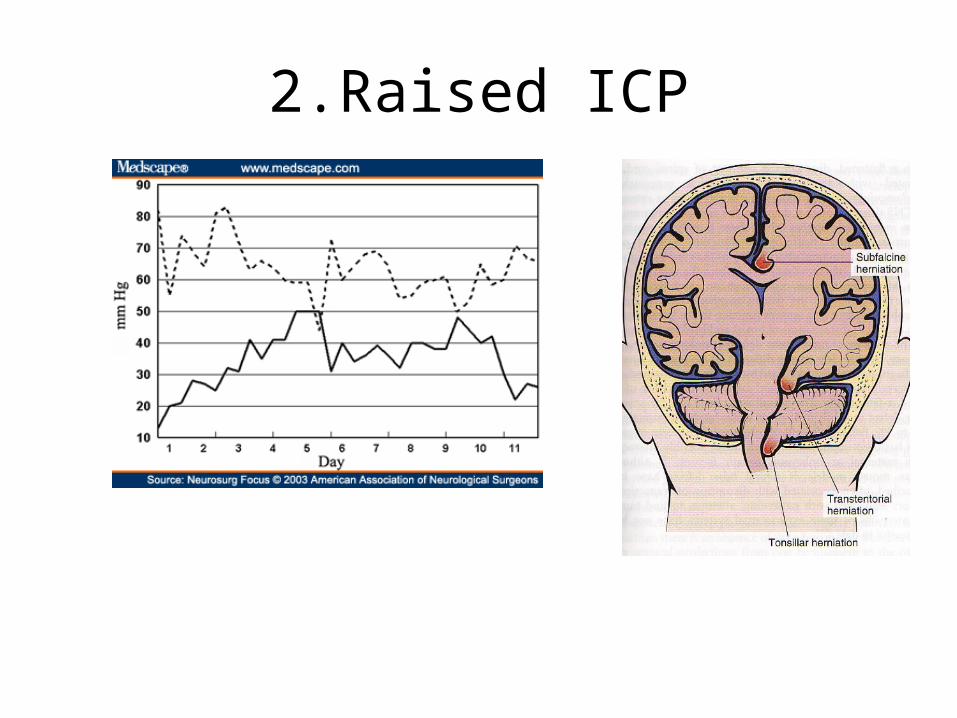
2.Raised ICP

Raised ICP
Brain Oedema/SwellingExtra-dural HematomaSub-Dural Hematoma
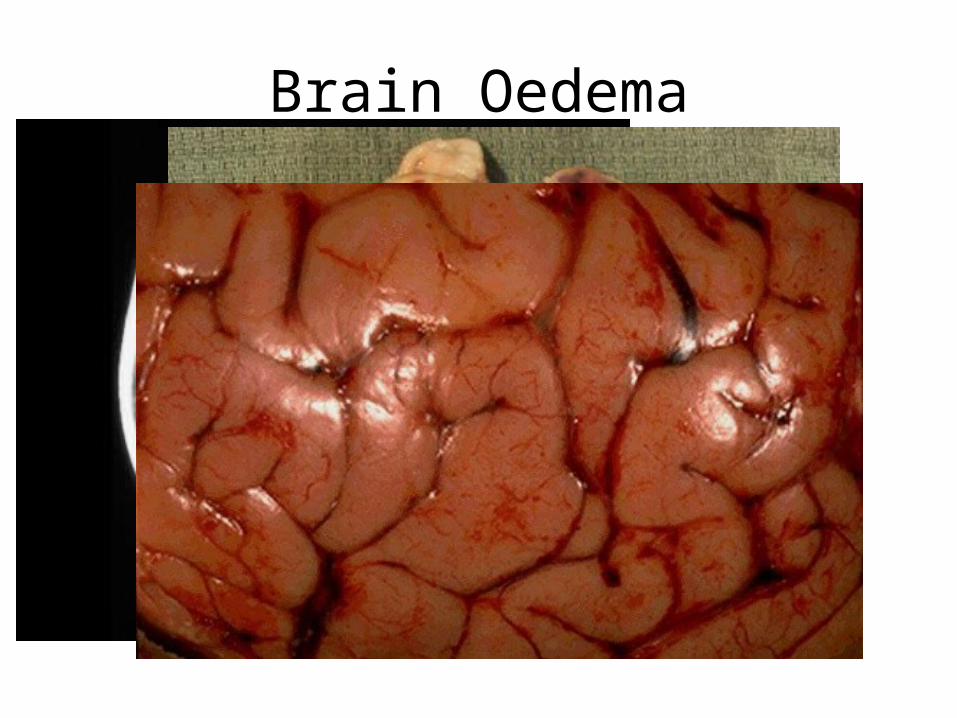
Brain Oedema
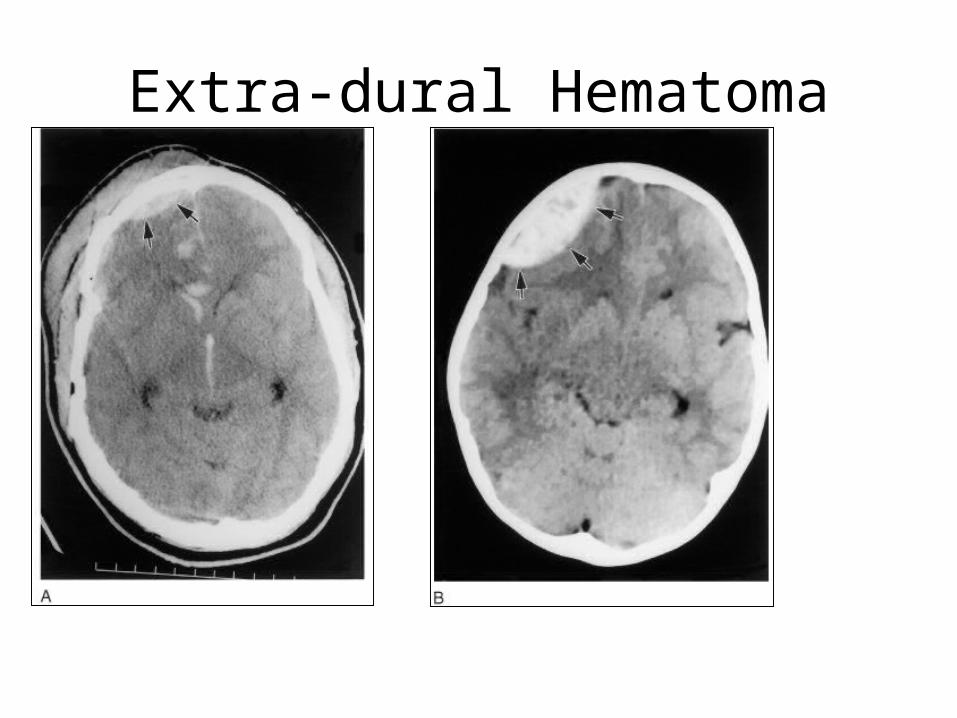
Extra-dural Hematoma
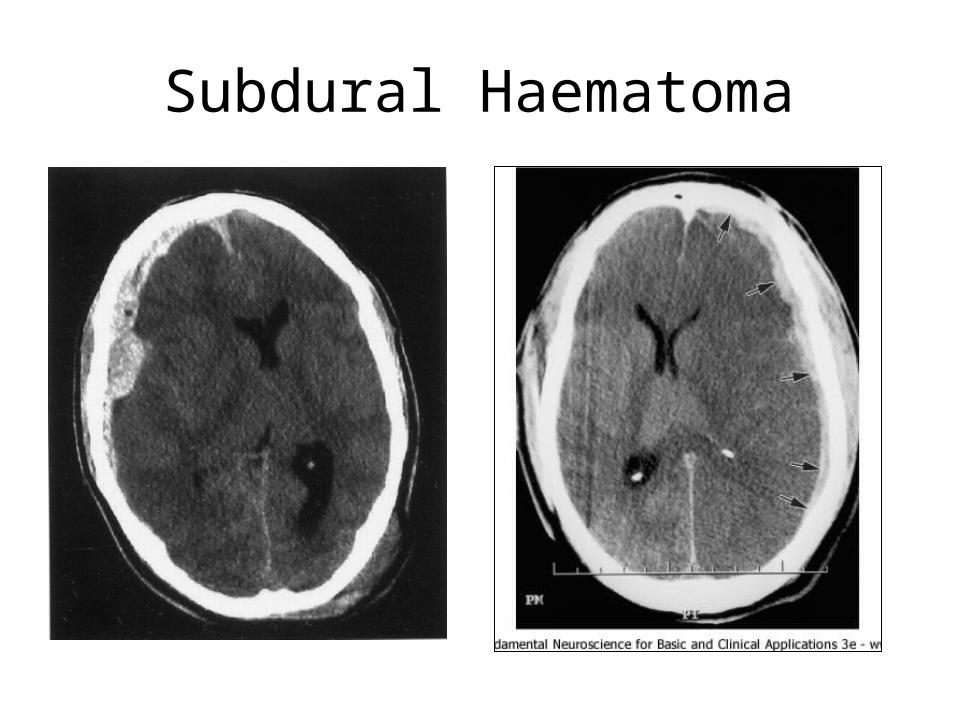
Subdural Haematoma
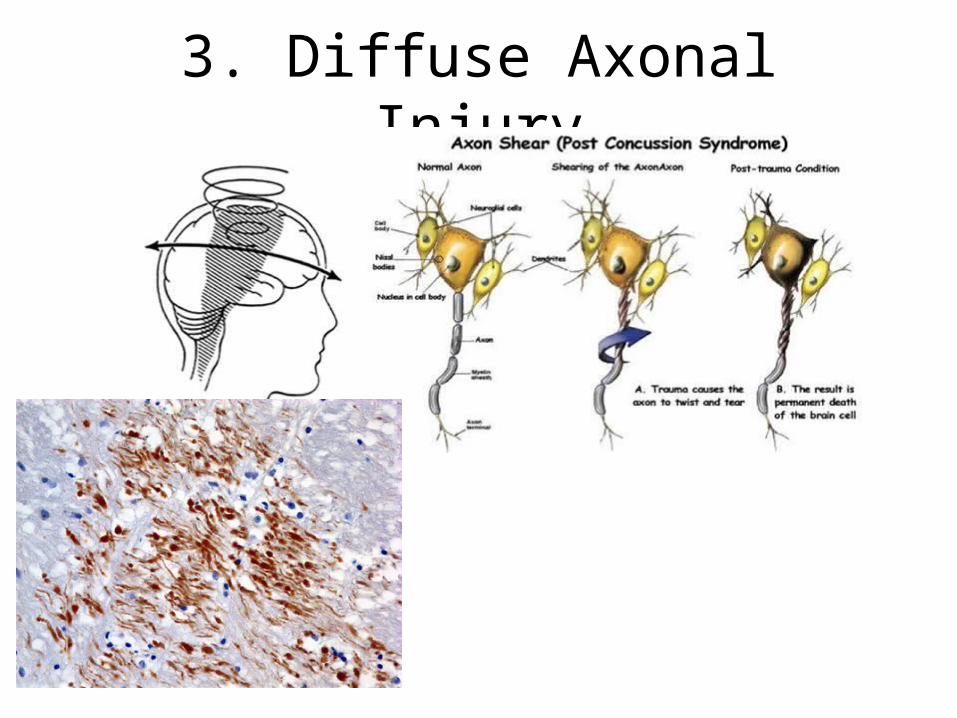
3. Diffuse Axonal Injury
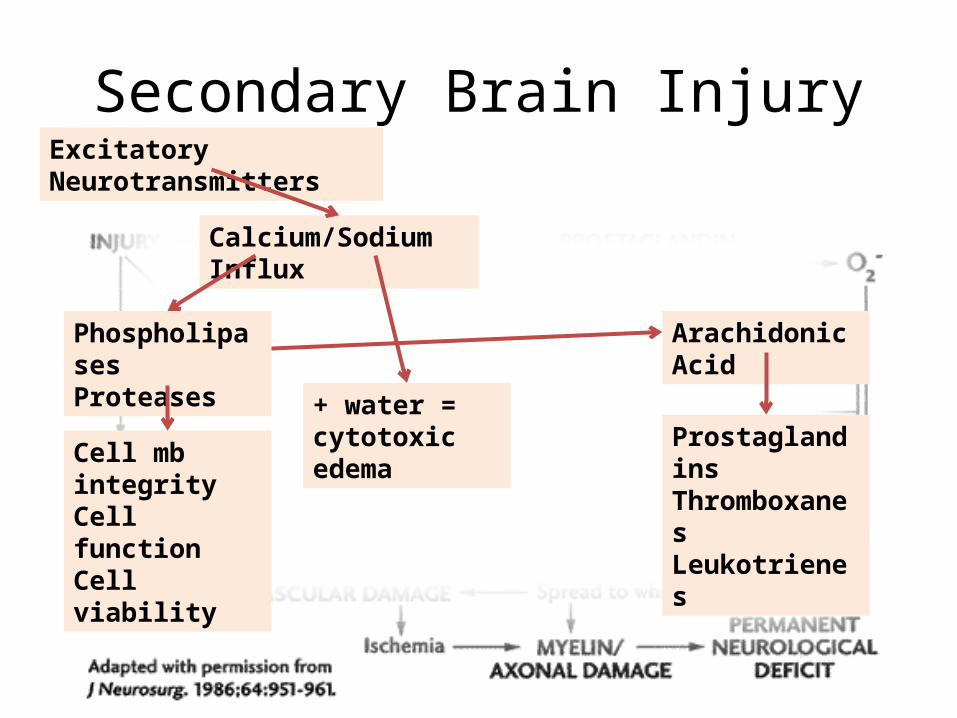
Secondary Brain InjuryExcitatory Neurotransmitters
Calcium/Sodium Influx
PhospholipasesProteases
Cell mb integrityCell functionCell viability
+ water = cytotoxic edema
Arachidonic Acid
ProstaglandinsThromboxanesLeukotrienes

Overview
• Initial evaluation• Prognosis• Management of Head Injury• Orthopaedic Issues– Operative vs. nonoperative treatment
• Timing of surgery• methods
– Fracture healing in head injury– Associated injuries– Complications

Initial Evaluation
Pre-Hospital careEmergency Department
ATLS protocolPrimary SurveySecondary survey
HistoryPhysical Exam – GCS < 9, 9 – 12, > 13, xT, xTPImaging
ABCDE
• GCS < 9 – intubate• Hyperventilation, 100% Oxy sat• BP > 90mmHg• Pupils• GCS• ICP monitoring

Hyperosmolar therapy– Mannitol 0.25 – 1 g/kg infusion– Hypertonic saline– Albumin
HCT 30 – 33%PaCO2 – 35 +/- 2 mmHgCVP 8 – 14 mmHgAvoid dextrose IVMaintain euthermia or hypothermia
Role of Orthopedic Surgeon
• Resuscitation• Treatment Methods/Timing• Associated injuries• Complications
1. Damage Control Surgery
Goal– Limit ongoing hemorrhage, hypotension, and
release of inflammatory factors– Limit stress on injured brain– Initial surgery • <1-2 hrs• limit surgical blood loss
Methods– Initial focus on stabilization• External fixation• Limited debridement• Limited or no internal fixation or definitive care
– Delayed definitive fixation (5-7 days)
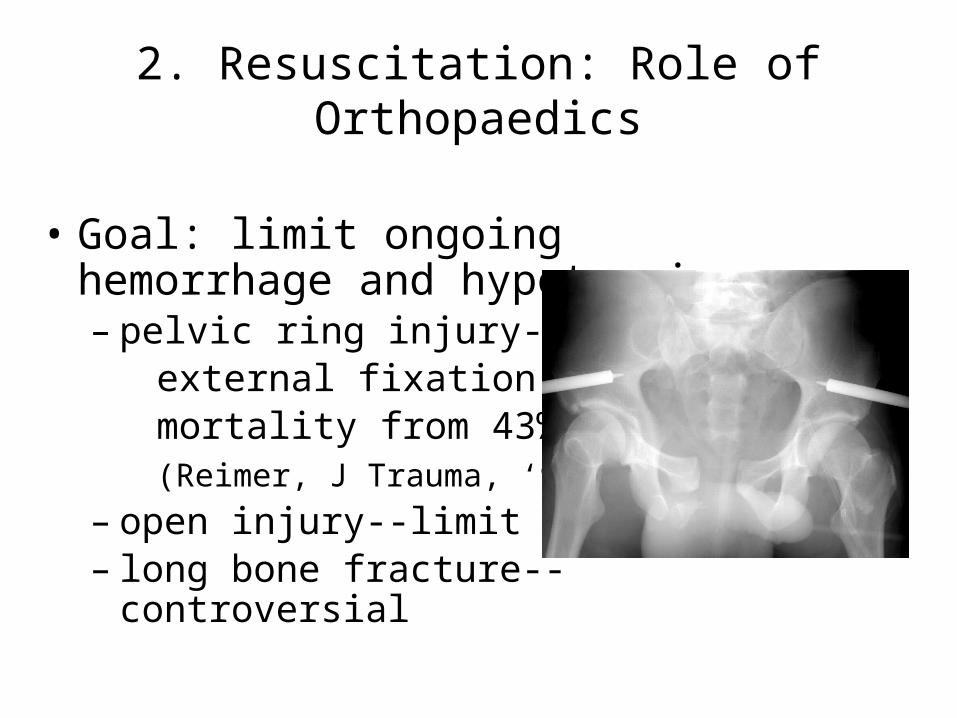
2. Resuscitation: Role of Orthopaedics
• Goal: limit ongoing hemorrhage and hypotension– pelvic ring injury-- external fixation reduced mortality from 43% to 7% (Reimer, J Trauma, ‘93)– open injury--limit bleeding– long bone fracture--controversial
Long Bone Fracture in the Head Injured Patient
• Early fixation (<24 hours) well accepted in the polytrauma patient
• In the head injured patient early fixation may be associated with – hypotension – elevated ICP– blood loss/coagulopathy– Hypoxia– Fat embolism
• Advocates of early and delayed treatment
Early Osteosynthesis
Hofman ‘91, Poole ’92, McKee ’97 – either no difference or lower mortality and GOS
Bone ‘94, Starr ‘98 – delayed fixation worse mortality and 45X pulm complications
Delayed Osteosynthesis
• Reynolds ’95, Jaicks ’97, Townsend ‘98 – more hypotension i.e. more fluid resusc needed, lower discharge GCS

Fracture Care
Decided on a case by case basis but surgery is often optimal–Alignment–Articular congruity–Early rehabilitation–Facilitated nursing care
Non-operative fracture care

BUT
Minimise–Hypotension–Hypoxia–Elevated ICP–Adequate fixation
3. Bone Healing
?enhanced bone healing?– Exuberant callus – Heterotopic ossification
Humoral osteogenic factors released by the injured brain - Klein et al ‘99
?prolactin – Wildburger et al?Growth Factor – Bidner et al
Union rates not significantly affected while malunion rates increased
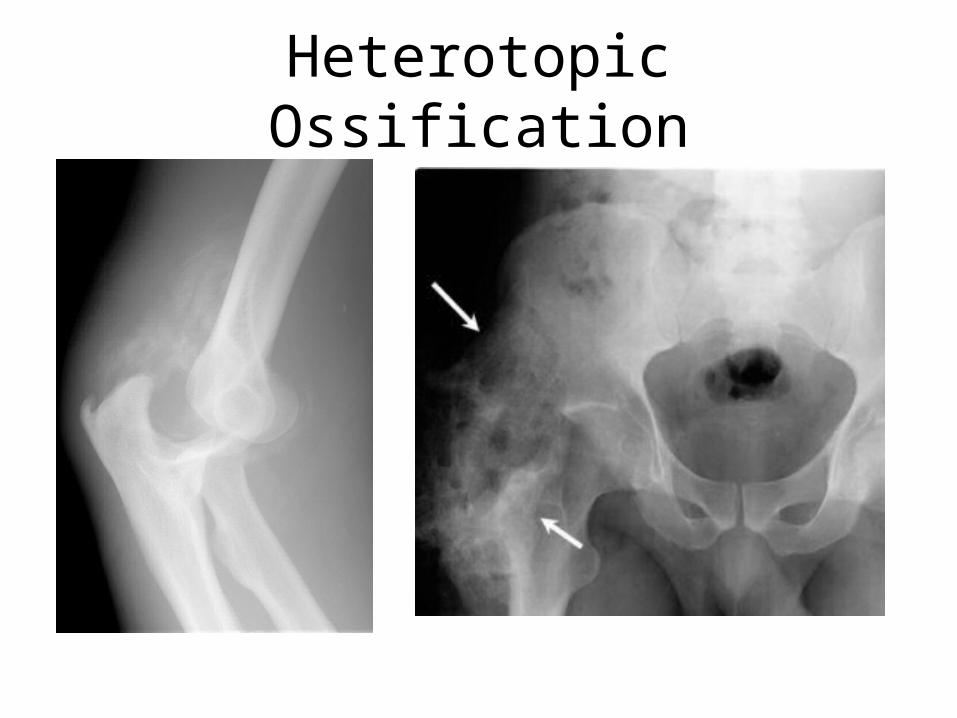
Heterotopic Ossification
Formation of lamellar bone inside soft tissue structures where bone does not normally exist
1) inciting event2) signal from the site of injury 3) supply of mesenchymal cells whose genetic
machinery is not fully committed4) environment which is conducive to the
continued formation of new bone
Associated with ventilator dependencyAvoid periarticular proceduresUse approaches/techniques less associated
with H.O.Prophylaxis
RT – single dose within 48 hours of surgeryIndomethacin – 25 mg tds for 6 weeks
Excision
Occult Injuries
• Fractures, dislocations and peripheral nerve injuries may be “missed”– Up to 11% of orthopaedic injuries may be
“missed”– Peripheral nerve injuries are particularly common
(as high as 34%)– Occult fractures in children with head injury are
also common (37-82%)
Occult Injuries
• Detailed physical exam with radiographs of any suspect area due to bruising, abrasion, deformity, loss of motion
• Consider EMG for unexplained neurologic deficits
• Bone scan advocated in children with severe head injury @ 72 hrs
Thank You