Embed Size (px)
DESCRIPTION
Trauma
Citation preview

ttotpRp
2
0d
The American Journal of Surgery (2011) 201, 587–591
North Pacific Surgical Association: First Place Residents’ Competition
Trauma induces a hypercoagulable state that is resistantto hypothermia as measured by thrombelastogram
Jerome A. Differding, M.P.H., Samantha J. Underwood, M.S., Philbert Y. Van, M.D.,Rakan A. Khaki, Nicholas J. Spoerke, M.D., Martin A. Schreiber, M.D., F.A.C.S.*
Division of Trauma, Critical Care and Acute Care Surgery, Oregon Health & Science University, 3181 Southwest Sam
Jackson Park Road, Portland, OR 97239, USAAbstractBACKGROUND: The aim of this study was to test the hypothesis that severely injured trauma
patients would be hypercoagulable compared with controls measured by thromboelastography and thatthis hypercoagulability would persist over a broad range of temperatures.
METHODS: A prospective study evaluating the effects of temperature on coagulation in traumapatients with Injury Severity Scores � 15 and controls was completed. Thromboelastography wasperformed 24 hours after admission at 4 temperatures ranging from 32°C to 38°C.
RESULTS: Ninety-two subjects (46 patients) were analyzed. Patients had a median Injury SeverityScore of 20 (interquartile range, 16–26). Time to clot formation increased (P � .001) and fibrincross-linking decreased (P � .01) in both groups as temperature decreased. Between groups, time toclot formation, fibrin cross-linking, and clot strength were significantly different at each temperature(P � .01), with patients being more hypercoagulable. Time to clot formation and fibrin cross-linkingwere more affected by temperature in controls compared with patients (P � .02).
CONCLUSIONS: Severely injured patients are more hypercoagulable than controls throughout abroad range of temperature. Decreasing temperature has a greater effect on coagulation in controlscompared with patients.© 2011 Elsevier Inc. All rights reserved.
KEYWORDS:Trauma;Hypercoagulable;Thromboelastography;Hypothermia
upettacs(asag
Hemorrhage continues to be the leading cause of pre-ventable death in trauma patients.1 Studies have shown thathe triad of hypothermia, acidosis, and coagulopathy con-ribute significantly to the severity of hemorrhage and ratef mortality.2–6 Current methods of estimating coagulopa-hy include the prothrombin time (PT) and partial thrombo-lastin time (PTT). Human studies by Gubler et al7 andeed et al8 showed prolonged PT and PTT at lower tem-eratures. PT and PTT are poor indicators of in vivo coag-
* Corresponding author. Tel.: 503-494-3500; fax: 503-494-6519.E-mail address: [email protected] received November 9, 2010; revised manuscript January
a1, 2011
002-9610/$ - see front matter © 2011 Elsevier Inc. All rights reserved.oi:10.1016/j.amjsurg.2011.01.012
lation for several reasons. First, these assays are routinelyerformed at 37°C in the laboratory, underestimating theffects of hypothermia on coagulation. Second, to performhese assays, blood is centrifuged, excluding the contribu-ion of cellular elements to in vivo coagulation. Finally, PTnd PTT are designed to analyze specific portions of thelotting cascade, not overall clot performance.9 Previouswine studies evaluating the use of thromboelastographyTEG; Haemoscope Corporation, Niles, IL) to estimate co-gulation at various temperatures have shown statisticallyignificant coagulopathy at lower temperatures. Addition-lly, a limited human study of hypothermic patients under-oing neurosurgical procedures demonstrated coagulopathy
t lower temperatures when measured by TEG.6 In a 1987
dt
weutpcC
pab
mtt�tp
pbiwutaoal
mpari
588 The American Journal of Surgery, Vol 201, No 5, May 2011
study of TEG in hypothermic trauma patients, body tem-perature � 34°C correlated with abnormal values on TEG.10
Confounding these findings is the fact that the more hypo-thermic patients had significantly greater Injury SeverityScores (ISS) and received more fluid resuscitation than theless hypothermic patients.11 No study has evaluated theirect effects of temperature on coagulation in trauma pa-ients as measured by TEG.
Methods
This was a prospective, noninterventional, single-centerstudy evaluating the effects of temperature on coagulationmeasured by TEG in normal control subjects and in severelyinjured trauma patients. All trauma patients with ISS � 15
ere eligible to be enrolled in the study. Patients werexcluded from eligibility for the following reasons: currentse of therapeutic anticoagulation, preexisting coagulopa-hy, pregnancy, or inability to obtain consent from either theatient or a legal authorized representative. Patients andontrols were consented before enrollment in the study.ontrols were age and gender matched to patients.
TEG assay
Citrated samples were collected and analyzed usingTEG, a point-of-care coagulation test that uses time-depen-dent viscoelastic properties of whole blood. One milliliter ofblood was placed in a vial containing kaolin, which accel-erates clotting. A fixed quantity of the kaolin-activatedblood (340 �L) and 20 �L of calcium chloride were pi-etted into a cup housed in a carriage assembly. A pinffixed to a torsion wire was lowered into the cup, which
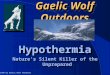
Figure 1 Thromboelastographic tracing co
egins to oscillate at a fixed rate and amplitude. As the cup
oves and clotting is initiated, the blood begins to adhere tohe pin, which in turn deflects the torsion wire. The deflec-ion of the torsion wire increases as the clot strengthens. In
1 hour, the thromboelastographic tracing and its respec-ive values give an interpretation of the entire coagulationanel (Fig. 1).
Analysis of kaolin-activated thromboelastograms wereerformed �24 hours after admission using venous wholelood at 38°C, 36°C, 34°C, and 32°C. For subjects receiv-ng heparin, thromboelastographic assays were run with andithout heparinase. This was done to negate the effects ofnfractionated heparin or low–molecular weight heparin onhe assay. The primary end point was the effect of temper-ture on coagulation status. The institutional review boardf Oregon Health & Science University approved the study,nd written consent was obtained from subjects or theiregal representatives.
Statistical analysis
Statistical analyses were performed using SPSS version18.0 (SPSS, Inc, Chicago, IL). For normally distributeddata, an analysis of variance and Student’s t test were used
Table 1 Demographics
Variable Patients Controls
Age (y) 48 (31–64) 38 (33–50)Men 23 23Women 23 23ISS 20 (16–26) No data
Data are expressed as median (interquartile range) or as numbers.There were no statistical differences between any of the groups (P �.05).
ng 32°C with 38°C in a control participant.

tgfi
bstcpf
titid(
�.
589J.A. Differding et al. Hypercoagulability is resistant to hypothermia
to determine differences between groups. Mann-Whitney Uests were used for nonparametric comparisons betweenroups. Paired t tests and Wilcoxon’s tests were conductedor normally distributed and nonparametric paired compar-sons, respectively. P values � .05 were considered statis-
tically significant.
Results
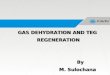
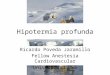
Ninety-two subjects (46 patients) were included in theanalysis. Participant demographics are highlighted in Table1. Both groups were similar with respect to age and gender,and the trauma group was severely injured, as indicated bya median ISS of 20. Time to clot formation increased (P �.001) in both groups as temperature decreased (Fig. 2).Fibrin cross-linking significantly decreased (P � .001) inoth groups with decreasing temperatures (Table 2). Clottrength was unaffected by temperature in both groups, withhe exception that it was greater in the control group at 32°Compared with other temperatures. Patients were more hy-ercoagulable than controls as measured by time to clotormation, clot strength, and fibrin cross-linking at each
Figure 2 Mean differences in time to clot formation (R-time). Ctcontrols; Pt � patients. *P � .001 between 32°C and other
temperatures; #P � .01 between groups.
Table 2 Thromboelastographic data
Variable 32°C 34°C
Fibrin cross-linkingPatients 62.7 (57.4–66.4)* 63.4 (5Controls 54.1 (48.4–57.5)*† 57.0 (5
LysisPatients .05 (.00–.50) .30 (.0Controls .15 (.00–1.50) .20 (.0
Data are expressed as median (interquartile range).*There was significantly less fibrin cross-linking as temperature dec†There was significantly less fibrin cross-linking in controls versus p
emperature (Figs. 2 and 3, Table 2). No difference was seenn the percentage lysis between the groups at any tempera-ure (Table 2). Decreases in temperature produced greaterncreases in time to clot formation (Fig. 4) and greaterecreases in clot strength in controls compared with patientsFig. 5).
Comments
Hemorrhage and coagulopathy continue to complicatethe care of critically injured patients. A number of factorscontribute to coagulopathy after trauma, including hemor-rhage, shock, acidosis, fluid resuscitation, and hypothermia.Hypothermia is common after trauma, with up to 66% oftrauma patients having temperatures �36°C on arrival tothe emergency department. In a group of patients with ISS� 25, the mortality rate increases from 10% to as high as100% when body temperatures fall from 35°C to �32°C.The exact contribution of hypothermia to coagulopathy hasnot been elucidated.
The current standard for measuring coagulation status isPT and activated PTT. These tests do not provide informa-
36°C 38°C
.3)* 67.1 (63.4–70.6)* 67.8 (62.5–69.9)*
.9)*† 57.7 (53.2–61.7)*† 61.6 (55.9–65.3)*†
) .95 (.20–1.60) 1.20 (.50–2.65).50 (.10–1.30) 1.75 (.70–3.30)
ithin group (P � .001).at all temperatures (P � .001).
Figure 3 Mean differences in clot strength. Ct � controls; Pt �patients. *P � .001 between 32°C and other temperatures; #P �01 between groups.
9.2–672.3–60
0–1.030–.75)
reased watients

(
590 The American Journal of Surgery, Vol 201, No 5, May 2011
tion about the entire coagulation and fibrinolytic cascade,are poor indicators of in vivo coagulation, and are notadequately sensitive to detect clinically significant coagu-lopathy. These measurements are performed by drawingand centrifuging the patient’s blood, collecting the plasma,and then adding activating factors to the plasma at 37°C.They represent a poor estimation of in vivo clotting abilitybecause they neglect the cellular contributions to coagula-tion. In addition, running the samples at 37°C ignores thetemperature-dependent depression of enzymatic function.Additionally, PT and activated PTT have been shown to beunable to detect derangements in coagulation in hypother-mic injured swine compared with TEG.
TEG is an excellent test for assessing overall coagulation.TEG rapidly assesses the interaction of platelets with the pro-tein coagulation cascade from the initial platelet-fibrin interac-tion, through platelet aggregation, clot strengthening, and fibrincross-linking, to eventual clot lysis. In �30 minutes, a throm-boelastogram can provide information on clotting factor activ-ity, platelet function, and any clinically significant fibrinolyticprocess.
Figure 4 Median changes in time to clot formation (R). CT �controls; PT � patients. *Significantly lower time between groupsP � .001). **Significantly lower time between groups (P � .02).
Figure 5 Median changes in clot strength (maximum amplitude[MA]). CT � controls; PT � patients. *Significantly less clot
strength (P � .05).TEG has been shown to be effective in the evaluation ofoverall coagulation in trauma patients. Coagulopathies havebeen associated with the severity of injury and temperature.Minimally injured patients have normal results on TEG,whereas moderately injured patients are hypercoagulable byTEG on admission. Severely injured patients are frequentlyhypocoagulable initially, placing them at greatest risk forbleeding. The effect of temperature on TEG in this patientgroup has not been evaluated.
This study allowed us to make several important obser-vations. A reduction in temperature resulted in increasedtime to clot formation and decreased fibrin cross-linking inboth groups. Clot strength was relatively unaffected byreductions in temperature. These findings suggest that clot-ting factor function and fibrin cross-linking are more af-fected by the temperature ranges studied than platelet func-tion. We also found that severely injured trauma patients aremore hypercoagulable than a comparable healthy popula-tion throughout the range of temperatures studied. Interest-ingly, reductions in temperatures had a greater effect oncoagulation in control patients compared with trauma pa-tients, suggesting that hypercoagulability observed after se-vere trauma is resistant to hypothermia.
There were several limitations associated with this study.The effect of temperature on coagulation was measured invitro using TEG, and these measurements may not accu-rately reflect temperature effects in vivo. We chose to per-form coagulation assessments �24 hours after patients wereadmitted to the hospital to obtain a more uniform populationof patients. Whereas hypocoagulability has been shown toincrease with severity of injury at the time admission,12 theincidence of hypercoagulability after resuscitation and sta-bilization of trauma patients is very high.13
Conclusions
Hypothermia is associated with increased time to clottingand decreased fibrin cross-linking in both severely injuredtrauma patients and controls. Stabilized trauma patients aremore hypercoagulable than controls with respect to all as-pects of clotting as measured by TEG regardless of temper-ature. Hypercoagulability in severely injured trauma pa-tients is relatively resistant to hypothermia compared withcontrols.
References
1. Hess J, Brohi K, Dutton R, et al. The coagulopathy of trauma: a reviewof mechanisms. J Trauma 2008;65:748–54.
2. Watts DD, Trask A, Soeken K, et al. Hypothermic coagulopathy intrauma. J Trauma 1998;44:846–54.
3. Douning LK, Ramsay MA, Swygert TH, et al. Temperature correctedthrombelastography in hypothermic patients. Anesth Analg 1995;81:
608–11.
591J.A. Differding et al. Hypercoagulability is resistant to hypothermia
4. Martini WZ, Pusateri AE, Uscilowicz JM, et al. Independent contri-butions of hypothermia and acidosis to coagulopathy in swine.J Trauma 2005;58:1002–10.
5. Kettner SC, Kozek SA, Groetzner JP, et al. Effects of hypothermia onthrombelastography in patients undergoing cardiopulmonary bypass.Br J Anaesth 1998;80:313–7.
6. Kettner SC, Sitzwohl C, Zimpfer M, et al. The effect of gradedhypothermia on hemostasis in anesthetized patients without surgicaltrauma. Anesth Analg. 2003;96:1772–6.
7. Gubler KD, Gentilello LM, Hassantash A, et al. The impact of hypo-thermia on dilutional coagulopathy. J Trauma 1994;36:847–51.
8. Reed RL, Johnston TD, Hudson, JD, et al. The disparity between hypo-thermic coagulopathy and clotting studies. J Trauma 1992;33:465–70.
9. Felfernig M, Blaicher A, Kettner SC, et al. Effects of temperature onpartial thromboplastin time in heparinized plasma in vitro. Eur JAnaesth 2001;18:467–70.
10. Luna GK, Maier RV, Pavlin EG, et al. Incidence and effect of hypo-thermia in seriously injured patients. J Trauma 1987;27:1014–8.
11. Jurkovich GJ, Grieser WB, Luterman A, et al. Hypothermia intrauma victims; an ominous predictor of survival. J Trauma 1987;27:1019 –24.
12. Kaufman CR, Dwyer KM, Crews JD, et al. Usefulness of thrombelasto-gram with common coagulation tests. Thromb Haemast 1981;46:752–6.
13. Schreiber MA, Differding J, Thorborg P, et al. Hypercoagulability ismost prevalent early after injury and in female patients. J Trauma2005;58:475–80.
Discussion
Robert M. Rush, M.D. (Tacoma, WA): When a bleed-ing and sick trauma patient enters the resuscitation bay, thelast thing one thinks of is hypercoagulation. Usually it is the
opposite: “Let’s get this bleeding stopped!” The authorsdescribe a hypercoagulable state associated with severetrauma that is temperature independent and can only bemeasured by thromboelastogram, specifically the Haemo-scope Corp TEG machine in their study. Thromboelastog-raphy (TEG) was first developed in the late 1940s but is stillnot guiding our clinical decision making for trauma pa-tients. Studies by Kaufman and colleagues (Kaufmann CF,et al. J Trauma 1997;42:716–722), as well as other studiesby this group, have shown that many trauma patients areinitially hypercoagulable or become hypercoagulableshortly after initial stabilization in the first 24 to 48 hours.This study adds a very important basic science piece to thecharacterization of TEG with respect to other coagulationparameters.
So when is the crossover? When do we start stopping the“stop the bleeding mentality” and start thinking about thehypercoagulable state that the authors have elucidated, notonly in this paper, but in their prior endeavors? I believe thatwe always have to think about it and thus the currentrecommendation according to the Joint Theater TraumaSystem Clinical Practice Guideline is to “begin DVT pro-phylaxis therapy as soon as coagulopathy is corrected inpatients not otherwise at increased risk of bleeding.” It isquite possible that the thromboelastogram could be thestudy to help determine this crossover point, but certainlynot in a vacuum. The patient’s clinical picture, other coag-ulation studies, and potentially their fibrinogen levels arealso important in determining the safety of initiating higherdoses for chemoprophylaxis of thromboembolic events in
the severely injured.