Embed Size (px)
Citation preview
1
Trauma Clinical Indicators
Most of the Trauma Clinical Quality Indicators (QIs) below have been adopted from Stellfox et al and
were modified and discussed at the NSW ITIM Data Management Committee on 24th March 2015.
“The seven clinical QIs with the addition of 1 (time to Embolisation
and the adjustment of re-intubation within 48hrs to unplanned ICU
admission) with supporting evidence for more than one
measurement domain (but not both validity and reliability) could be
appropriate targets for focused research efforts because they have
promising but incomplete evidence.” (1)
Proposed Trauma Clinical Quality Indicators
1. Scene Time (Pre-Hospital measure)
2. Time to Emergency Laparotomy
3. Time to Emergency Embolisation
4. Unplanned return to operating room within 48 hours of initial procedure
5. Complications (Development of decubitus ulcers, PE or DVT and Iatrogenic complications
during admission)
6. Unplanned admission to ICU
7. Missed Injuries
8. Peer review for preventable mortality
9. Retrieval team turnaround > 60 minutes
10. Referring hospital transfer > 6 hours
DISCLAIMER:
The definitions have been copied from the Queensland Trauma Registry. All definitions and if
agreed, will need to have formal recognition and permission sought for use prior to publication in
any formal document
2
1. Scene Time (Pre-Hospital measure)
Background and Rationale
The length of time a patient spends at the ‘scene of the accident can have significant bearing on the
eventual outcome of the patient. It is important that patients are transported to hospital for
definitive management as soon as possible.
Comments should reflect any event affecting this indicator that is not explained by the extrication
time of the patient on the ambulance report (ARF). If there has been a delay and extraction time has
not been completed, look for an explanation in the notes. Pre hospital scene time is calculated from
Time of Arrival to patient to Scene Departure time.
Categories
1. Pre hospital scene > 20 minutes
2. Pre hospital scene < 20 minutes
8. Not applicable
9. Time unknown
Option 8 Not applicable would include cases where there was no recorded pre-hospital phase.
3
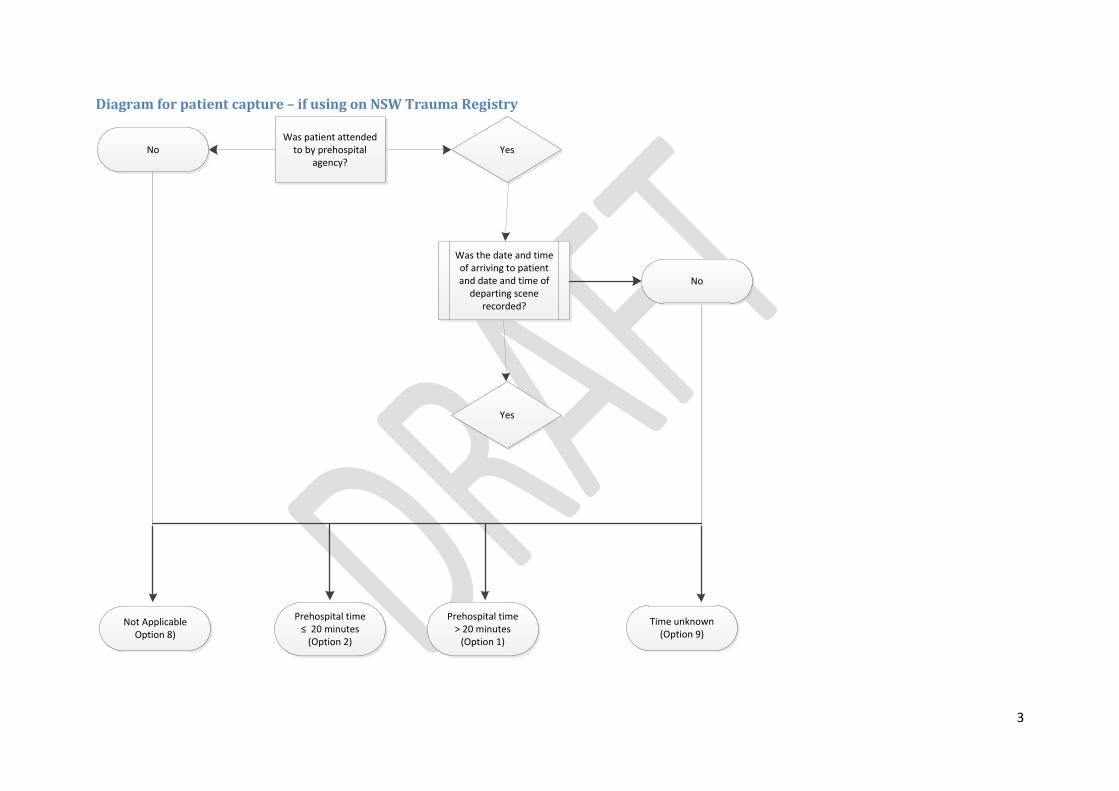
Diagram for patient capture – if using on NSW Trauma Registry
Prehospital time > 20 minutes
(Option 1)
Prehospital time ≤ 20 minutes
(Option 2)
Not ApplicableOption 8)
Was patient attended to by prehospital
agency?No Yes
Was the date and time of arriving to patient and date and time of
departing scene recorded?
No
Yes
Time unknown(Option 9)
4
Calculating proportions
1. Extract all MDS data
2. If patient Pre-hospital scene transport provider agency equals ‘Other’, then this
automatically goes to Option 8
3. If patient Pre-hospital scene transport provider agency equals either:
a. AMRS
b. ASNSW
c. CareFlight
d. Local Retrieval Service
e. NETS
Then check if the either the date or time is missing from Arrived at Patient or Left Location. If
either date/time is missing, then this automatically is assigned to Option 9.
If date/time available for both Arrived at Patient and Left Location, calculate the difference
between date/time of Arrived at Patient from Left Location. If the difference is > 20 minutes,
then assign to Option 1. If the difference is ≤ 20 minutes, then assign to option 2.
4. Proportion of Pre-Hospital Scene Time less than or equal to twenty minutes:
Total number of patients with Scene Time (less than or equal to twenty minutes
Total patient count that were transported by pre-hospital agency (with a valid date and time)
5. Proportion of Pre-Hospital Scene Time greater than twenty minutes:
Total number of patients with Scene Time (greater than twenty minutes
Total patient count that were transported by pre-hospital agency (with a valid date and time)
5
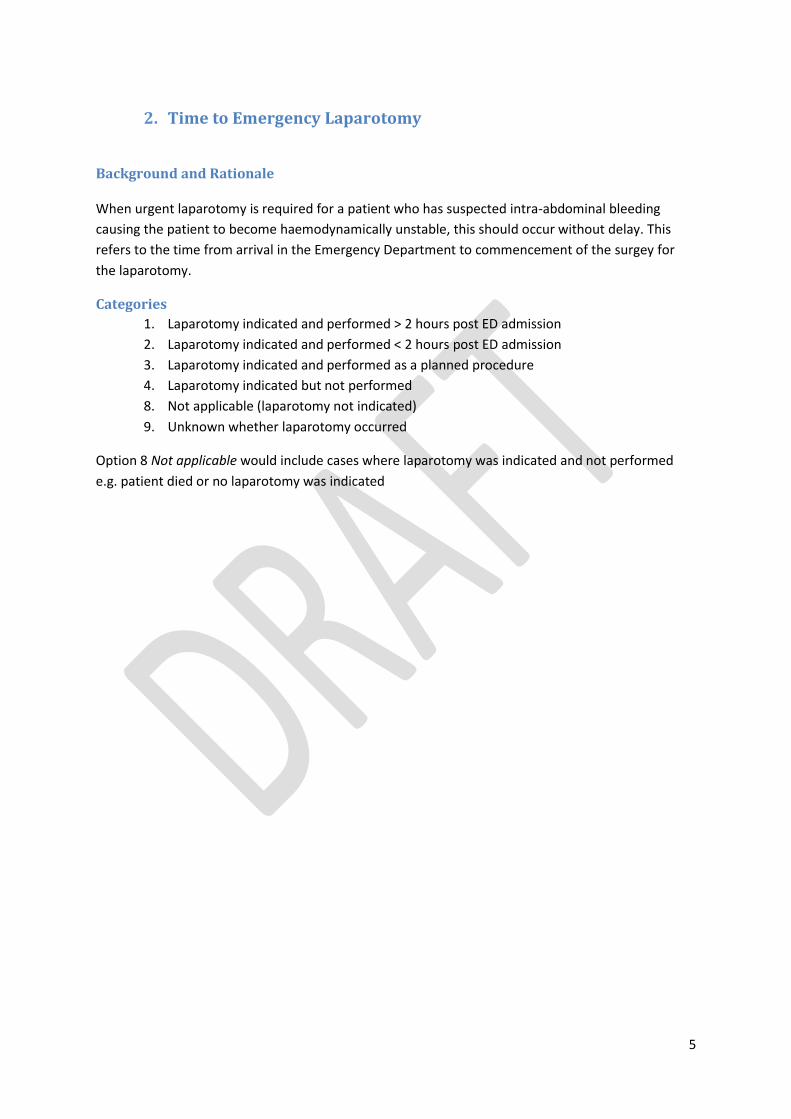
2. Time to Emergency Laparotomy
Background and Rationale When urgent laparotomy is required for a patient who has suspected intra-abdominal bleeding
causing the patient to become haemodynamically unstable, this should occur without delay. This
refers to the time from arrival in the Emergency Department to commencement of the surgey for
the laparotomy.
Categories
1. Laparotomy indicated and performed > 2 hours post ED admission
2. Laparotomy indicated and performed < 2 hours post ED admission
3. Laparotomy indicated and performed as a planned procedure
4. Laparotomy indicated but not performed
8. Not applicable (laparotomy not indicated)
9. Unknown whether laparotomy occurred
Option 8 Not applicable would include cases where laparotomy was indicated and not performed
e.g. patient died or no laparotomy was indicated
6
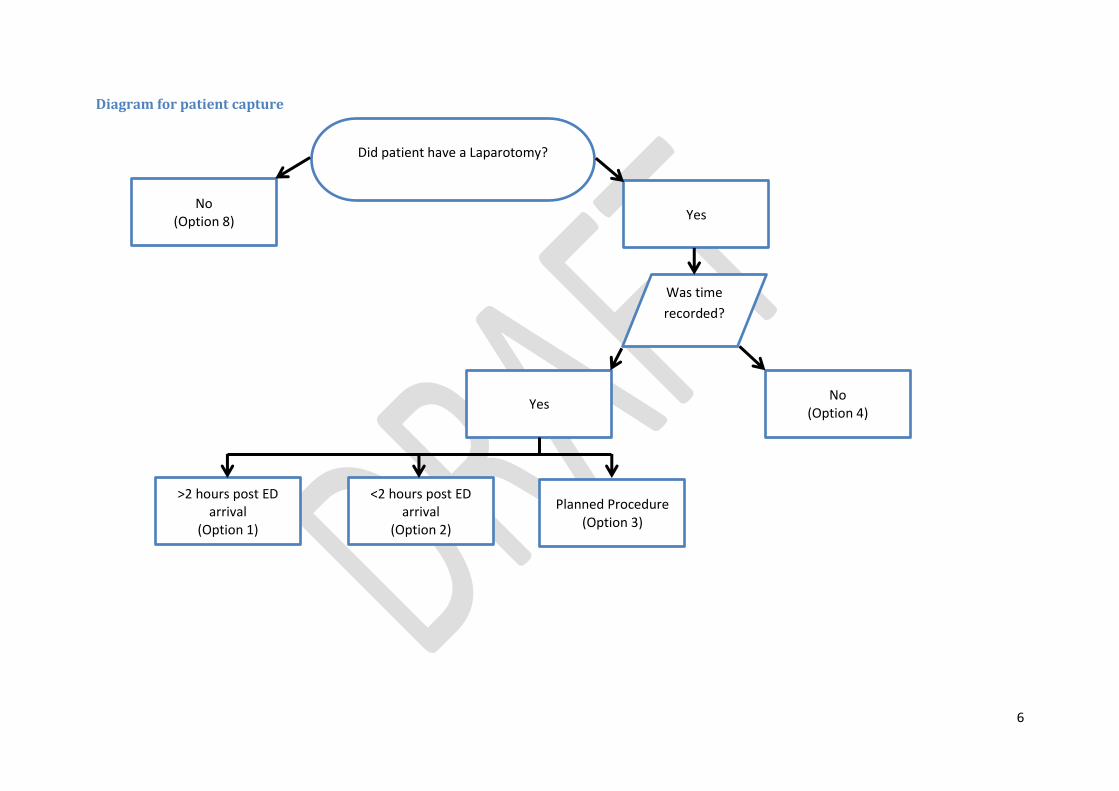
Diagram for patient capture
Did patient have a Laparotomy?
No (Option 8) Yes
Yes
Was time
recorded?
No (Option 4)
Planned Procedure (Option 3)
>2 hours post ED arrival
(Option 1)
<2 hours post ED arrival
(Option 2)
7
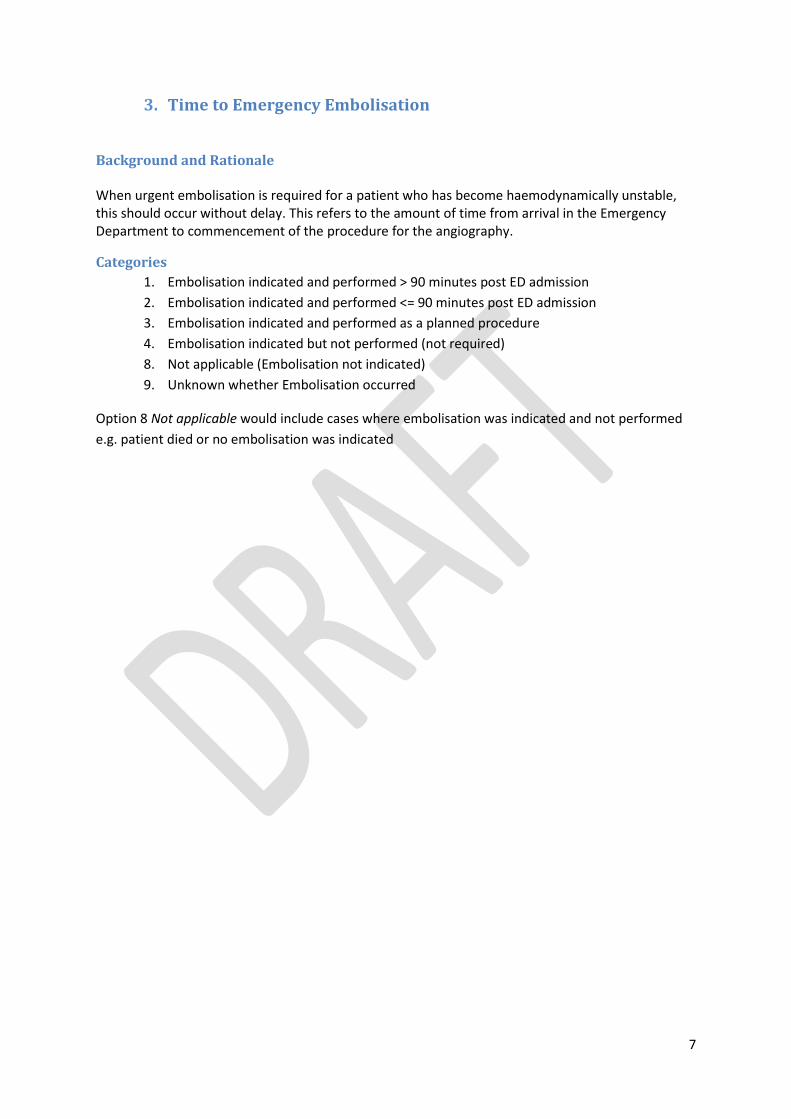
3. Time to Emergency Embolisation
Background and Rationale When urgent embolisation is required for a patient who has become haemodynamically unstable, this should occur without delay. This refers to the amount of time from arrival in the Emergency Department to commencement of the procedure for the angiography.
Categories
1. Embolisation indicated and performed > 90 minutes post ED admission
2. Embolisation indicated and performed <= 90 minutes post ED admission
3. Embolisation indicated and performed as a planned procedure
4. Embolisation indicated but not performed (not required)
8. Not applicable (Embolisation not indicated)
9. Unknown whether Embolisation occurred
Option 8 Not applicable would include cases where embolisation was indicated and not performed
e.g. patient died or no embolisation was indicated
8
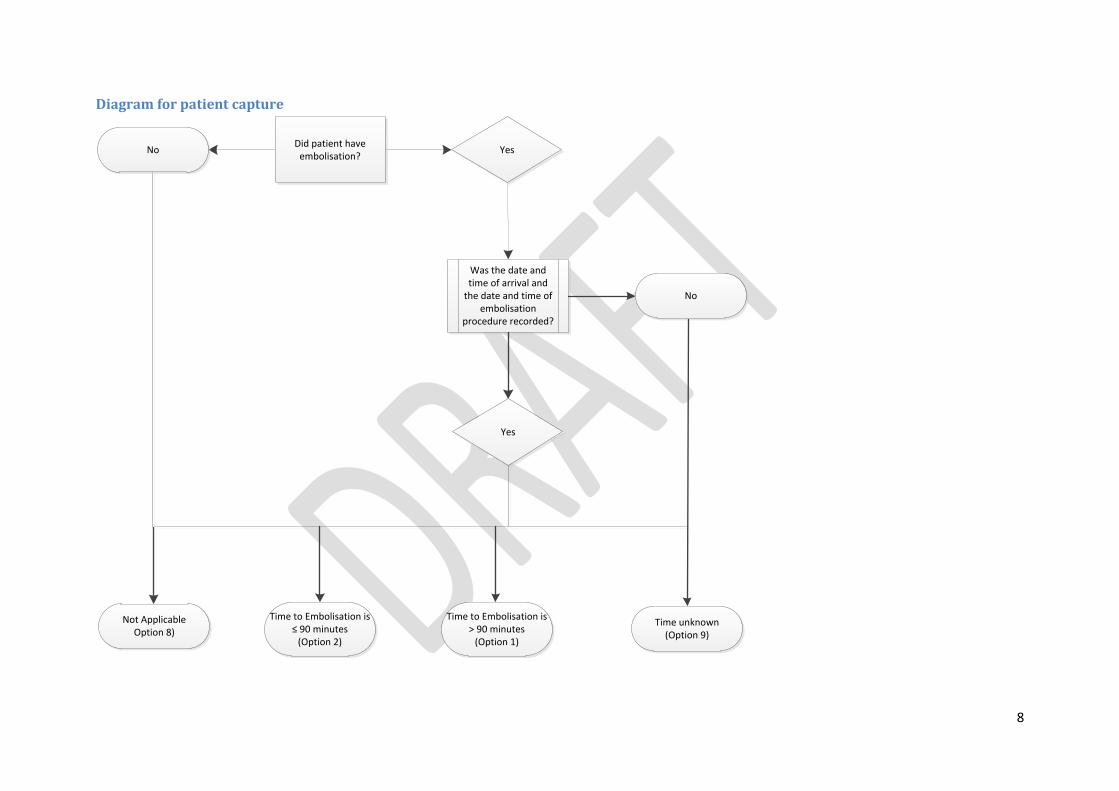
Diagram for patient capture
Was the date and time of arrival and
the date and time of embolisation
procedure recorded?
No
Yes
Not ApplicableOption 8)
Time to Embolisation is ≤ 90 minutes
(Option 2)
Time to Embolisation is > 90 minutes
(Option 1)
Did patient have embolisation?
No Yes
Time unknown(Option 9)
9
4. Unplanned return to the operating room within 48 hours of initial
procedure
Background and Rationale Ideally all operations will be anticipated and planned following Emergency Department assessment. Unplanned operations include return to operating theatre for post-operative haemorrhage, unexpected surgery for missed injuries, or unexpected deterioration of patient's condition.
Categories
1. Unplanned return to OT within 48 hours of initial procedure
2. No unplanned return to OT within 48 hours of initial procedure
8. Not applicable
9. Unknown if patient returned to OT or unknown time of return to OT
Option 8 Not applicable would include no initial visit to OT. Selection of Option 2 indicates that all
operations were planned.
10
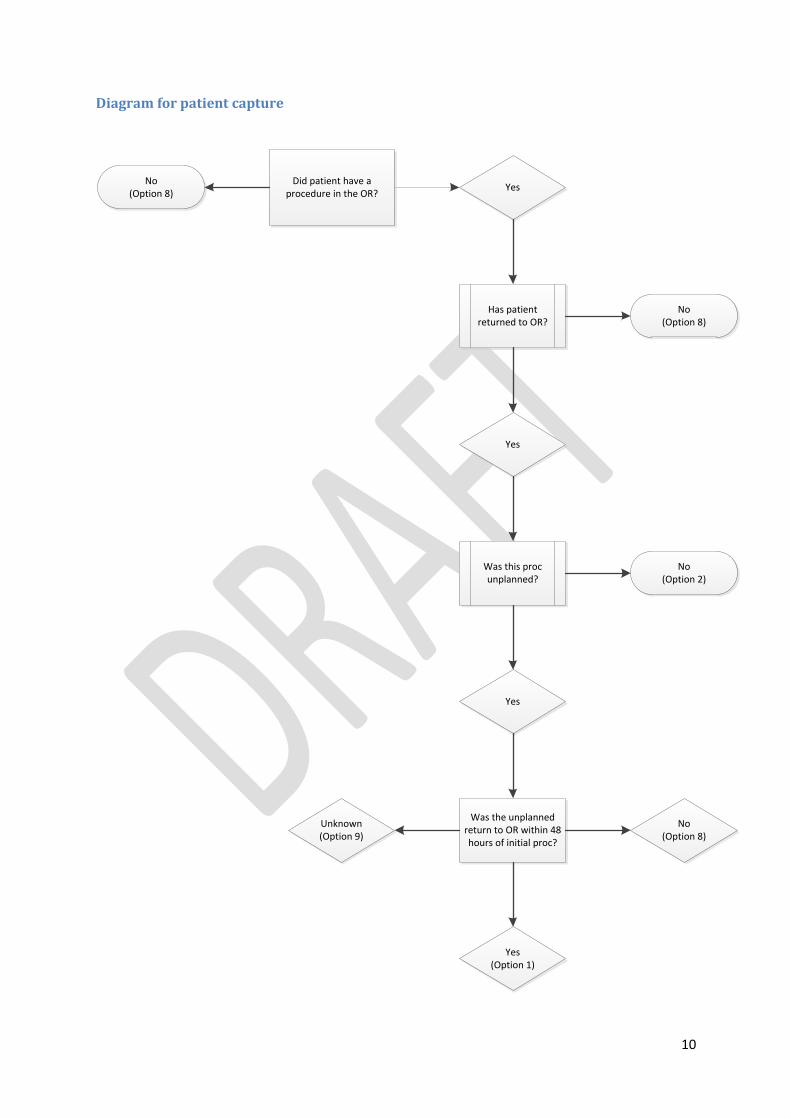
Diagram for patient capture
Did patient have a procedure in the OR?
No(Option 8)
Yes
Has patient returned to OR?
No(Option 8)
Yes
Was this proc unplanned?
No(Option 2)
Yes
Was the unplanned return to OR within 48 hours of initial proc?
Unknown(Option 9)
No(Option 8)
Yes(Option 1)
11
5. Complications
Background and Rationale Development of:
Decubitus ulcers
Pressure ulcers
PE
DVT Iatrogenic complications during admission
Infection
Thromboembolic disease
Anaemia (Hb < 12 if female)
The development of complications during an admission may result in longer hospital inpatient days
and result in differing mortality rates. Iatrogenic complications include adverse events that result
from the delivery of an episode of care, (i.e. liver laceration as a result of ICC insertion). Where a
complication is present during admission, then the type should be supplied in the comment field.
Categories
1. Yes
2. No
8. Not applicable
9. Unknown
Selection of Option 2 indicates no PE, DVT's or decubitus ulcers or iatrogenic complications were
present during that admission.
12
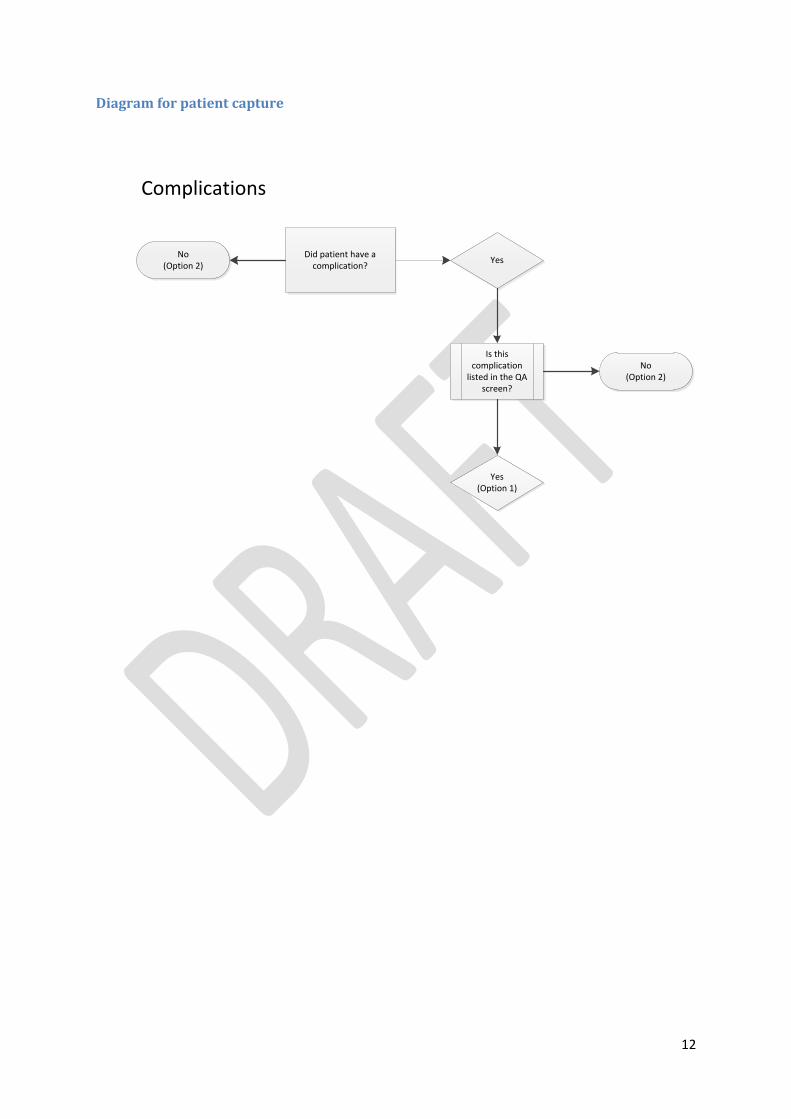
Diagram for patient capture
Complications
Did patient have a complication?
No(Option 2)
Yes
Is this complication
listed in the QA screen?
No(Option 2)
Yes(Option 1)
13
6. Unplanned Admission to ICU
Background and Rationale
This refers to those patients that were transferred to the ward and whose condition deteriorated
requiring prompt admission/re-admission to the Intensive Care Unit (ICU).
It includes patients who were:
• transferred from ICU to the ward and back to ICU, • transferred from Emergency Department to a ward then ICU, • transferred from the ED to theatre and were intended to go to the ward from Recovery but were admitted to ICU.
Categories
1. Admitted to ICU – unplanned
2. Admitted to ICU – planned
3. Admitted to ICU – not known whether planned or unplanned
8. Not applicable (no ICU admission)
9. Unknown ICU admission
Selection of option 2 indicates that all ICU episodes were anticipated and planned.
Option 8 - Not applicable would include no admissions to ICU.
14
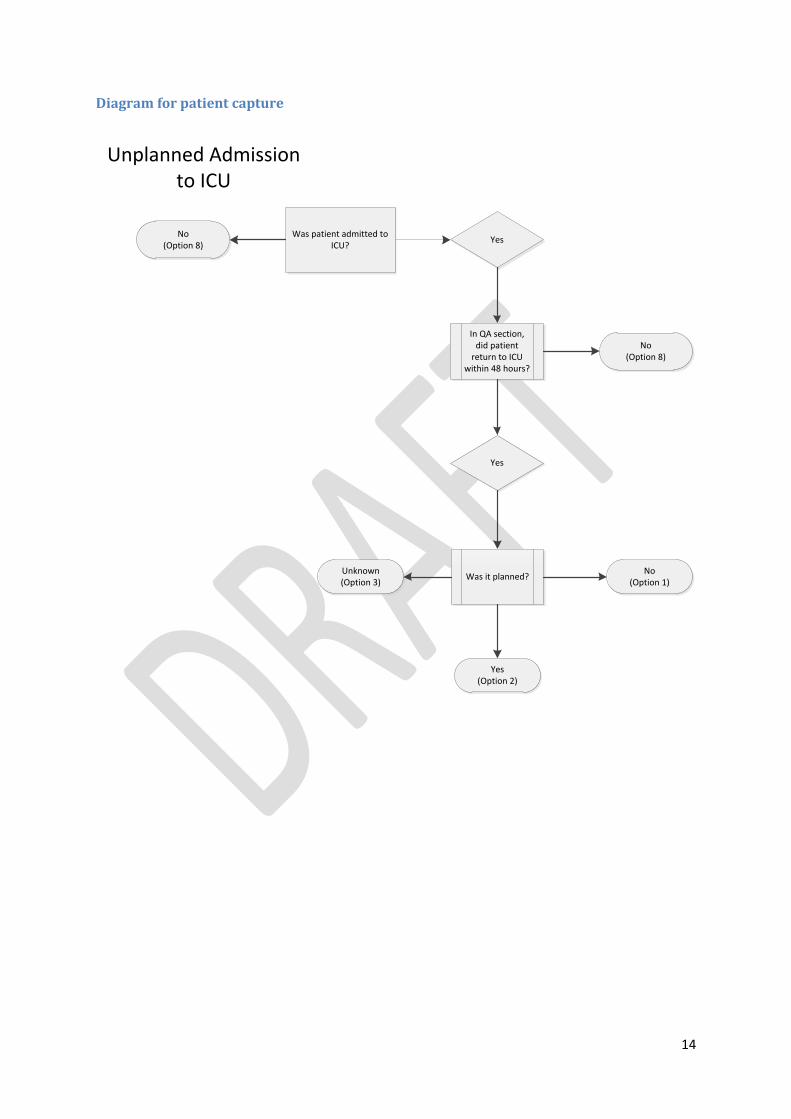
Diagram for patient capture
Unplanned Admission to ICU
Was patient admitted to ICU?
No(Option 8)
Yes
In QA section, did patient
return to ICU within 48 hours?
No(Option 8)
Yes
Was it planned?No
(Option 1)Unknown(Option 3)
Yes(Option 2)
15
7. Missed Injuries (Delay in diagnosis of injuries AIS > 1 post Tertiary
Survey)
Background and Rationale
Ideally all injuries will be diagnosed during the first 24 hours of care. Any injury that is not diagnosed
during the first 24 hours constitutes a missed injury.
Categories
1. Not all injuries of AIS > 1 diagnosed within 24 hours
2. All injuries of AIS > 1 diagnosed within 24 hours
3. No injuries of AIS > 1
8. Not applicable (investigations incomplete – died or transfer within 24 hours)
9. Unknown if all injuries of AIS > 1 diagnosed within 24 hours
Selection of Option 2 indicates that of any missed injuries, none were of an AIS score of greater than
one.
Option 8 - Not Applicable would include patients with no injuries of AIS > 1 or whose investigations
were incomplete e.g. Death or transfer within 24 hours.
16
8. Peer review for preventable mortality (need to identify a suitable
definition/name for the process of peer review i.e. Facility Trauma
M&M)
Background and Rationale
Should this include all cases where if 2 or 3 are selected, it will be automatically referred to be
reviewed by ITIM Clinical Review Officer.
Categories
1. Non preventable
2. Potentially preventable
3. Preventable
8. Case not reviewed, not applicable/did not meet criteria
9. Unknown
17
9. Retrieval team turnaround
Background and Rationale
When the Medical Retrieval Team is used to transfer a patient from the referring hospital, we want
to measure how long the retrieval team spends at the referring hospital (turnaround time, referring
hospital bedside to receiving hospital bedside).
Categories
1. Turnaround> 60 mins
2. Turnaround< 60 mins
8. Not applicable
9. Unknown
18
10. Referral hospital transfer > 6 hours
Background and Rationale
A patient who requires secondary or tertiary referral should reach definitive care as soon as possible.
This indicator measures the length of time from arrival at the referring facility to arrival at the
receiving facility.
Categories
1. Transfer> 6 hours
2. Transfer< 6 hours
8. Not applicable
9. Unknown
References:
(1) Stelfox, H., Straus S., Nathens A., Bobranska-Artiuch B. (2011). Evidence for quality
indicators to evaluate adult trauma care: A systematic review. Critical Care Medicine, 39(4),
846-859





























