-
8/10/2019 trating food refusal in adolescent with asperger's
disorder
1/14
http://ccs.sagepub.com/Clinical Case Studies
http://ccs.sagepub.com/content/9/4/260The online version of this
article can be found at:
DOI: 10.1177/15346501103735002010 9: 260 originally published
online 18 June 2010Clinical Case Studies
Michael P. Roth, Keith E. Williams and Candace M. PaulTreating
Food and Liquid Refusal in an Adolescent With Asperger's
Disorder
Published by:
http://www.sagepublications.com
can be found at:Clinical Case StudiesAdditional services and
information for
http://ccs.sagepub.com/cgi/alertsEmail Alerts:
http://ccs.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://ccs.sagepub.com/content/9/4/260.refs.htmlCitations:
What is This?
-Jun 18, 2010Proof
- Jul 12, 2010Version of Record>>
by Andreea Nicoleta Nicolae on October 12,
2011ccs.sagepub.comDownloaded from
http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/content/9/4/260http://ccs.sagepub.com/content/9/4/260http://www.sagepublications.com/http://www.sagepublications.com/http://ccs.sagepub.com/cgi/alertshttp://ccs.sagepub.com/cgi/alertshttp://ccs.sagepub.com/subscriptionshttp://www.sagepub.com/journalsReprints.navhttp://www.sagepub.com/journalsReprints.navhttp://www.sagepub.com/journalsPermissions.navhttp://www.sagepub.com/journalsPermissions.navhttp://ccs.sagepub.com/content/9/4/260.refs.htmlhttp://ccs.sagepub.com/content/9/4/260.refs.htmlhttp://online.sagepub.com/site/sphelp/vorhelp.xhtmlhttp://online.sagepub.com/site/sphelp/vorhelp.xhtmlhttp://ccs.sagepub.com/content/early/2010/06/16/1534650110373500.full.pdfhttp://ccs.sagepub.com/content/early/2010/06/16/1534650110373500.full.pdfhttp://ccs.sagepub.com/content/9/4/260.full.pdfhttp://ccs.sagepub.com/content/9/4/260.full.pdfhttp://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/http://online.sagepub.com/site/sphelp/vorhelp.xhtmlhttp://ccs.sagepub.com/content/early/2010/06/16/1534650110373500.full.pdfhttp://ccs.sagepub.com/content/9/4/260.full.pdfhttp://ccs.sagepub.com/content/9/4/260.refs.htmlhttp://www.sagepub.com/journalsPermissions.navhttp://www.sagepub.com/journalsReprints.navhttp://ccs.sagepub.com/subscriptionshttp://ccs.sagepub.com/cgi/alertshttp://www.sagepublications.com/http://ccs.sagepub.com/content/9/4/260http://ccs.sagepub.com/
-
8/10/2019 trating food refusal in adolescent with asperger's
disorder
2/14
Clinical Case Studies9(4) 260272
The Author(s) 2010
Reprints and permission:
http://www.sagepub.com/journalsPermissions.nav
DOI: 10.1177/1534650110373500http://ccs.sagepub.com
Treating Food and LiquidRefusal in an Adolescent
With Aspergers Disorder
Michael P. Roth1, Keith E. Williams2,
and Candace M. Paul2
Abstract
Food refusal is a complicated condition that has both medical
and social implications. In this study,
a 16-year-old boy with Aspergers disorder, dependent on
gastrostromy tube feedings for9 years, is treated with a behavioral
intervention. The intervention consists of several
components,including stimulus fading for both solids and liquids, a
token economy for solids, and an escapeprevention component for
liquids. Before treatment, the participant consumes three
different
foods and water. After treatment, the participant is consuming
78 foods and 13 beverages. Atthe end of 14 days of treatment, all
of the participants intakes are received orally, tube feedingsare
eliminated, and the patient has gained more than 1 pound on oral
feedings. The intervention
is generalized to both home and school settings, and maintenance
of treatment gains is reportedby parents 3 months after the end of
treatment.
Keywords
food refusal, autism spectrum disorder, token economy, stimulus
fading
1 Theoretical and Research Basis
Food refusal has been described as a child failing to consume
enough by mouth to maintain nutri-
tional needs and having a height-to-weight ratio below the 5th
percentile (Williams, Hendy, &
Knecht, 2008). It has been linked to medical conditions, for
example, gastroesophogeal reflux
disease; cystic fibrosis (Field, Garland, & Williams, 2003;
Linscheid, 2006; Piazza, Patel, Gulotta,
Sevin, & Layer, 2003); genetic disorders, for example,
TreacherCollin syndrome, RusselSilversyndrome (Ahearn, Castine,
Nault, & Green, 2001; Coe et al., 1997); and psychological
issues, for
example, choking phobia (Burklow & Linscheid, 2004).
Till date, only one study has examined the use of a token
economy in the treatment of food
refusal. Kahng, Boscoe, and Byrne (2003) found that a token
economy in conjunction with dif-
ferential negative reinforcement of alternative behavior was
more effective in increasing food
acceptance and reducing refusal behaviors than would a token
economy with differential posi-
tive reinforcement of alternative behavior with or without
physical guidance. Though this study
1Pennsylvania State University, Harrisburg
2Penn State Milton S. Hershey Medical Center
Corresponding Author:
Keith E. Williams, Feeding Program, 905 W. Governor Road,
Hershey, PA 17033
E-mail: [email protected]
by Andreea Nicoleta Nicolae on October 12,
2011ccs.sagepub.comDownloaded from
http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/
-
8/10/2019 trating food refusal in adolescent with asperger's
disorder
3/14
Roth et al. 261
demonstrated utility of a token economy as a component of
treatment, the study had some
limitations. The study involved only pureed fruits and
vegetables and included no foods of
higher texture or other additional food groups such as dairy,
fats, grains, and meats. The food
was presented on a Nuk brush, and it was unclear whether there
was a transition to other feeding
utensils. Furthermore, it was not reported whether the
participant had advanced his feeding skillsat the time of
follow-up. This study was, however, unique in that it did not
involve the use of
escape prevention.
Although a range of interventions has been used to treat food
refusal in children and adoles-
cents, most interventions consist of several components,
including some form of escape preven-
tion in which the child is required to consume the food offered
(Kerwin, 1999). One escape
prevention procedure, often termed exit criterion, involves
having the child to eat a specified
amount of food, often initially a single bite, before being
allowed to exit the session (Farrel,
Hagopian, & Kurtz, 2001; Paul, Williams, Riegel, &
Gibbons, 2007). Another component that
has been included in interventions for food refusal is some form
of stimulus fading, which has
typically involved the gradual increase in bite size or texture
(Freeman & Piazza, 1998; Luiselli,
2000; Luiselli, & Gleason, 1987; Paul et al., 2007). Fading
has also been used to increase vol-ume of previously avoided drinks
without eliciting negative behaviors (Babbitt, Shore, Smith,
Williams & Coe, 2001; Luiselli, Ricciardi, & Gilligan,
2005; Patel, Piazza, Kelley, Ochsner, &
Santana, 2001). This study examined use of a multicomponent
intervention that included a
token economy and fading procedure for solid food and a fading
procedure plus escape preven-
tion for liquids.
Objectives
The goal of treatment was to eliminate need for gastrostomy tube
feeds by increasing the volume
and variety of foods eaten to meet all of the participants
nutritional needs. Liquid consumptionwould also be increased both
to increase caloric intake and to ensure adequate hydration.
2 Case Presentation
Tyler (pseudonym) was a 16-year-old White boy diagnosed with
Aspergers disorder. Tyler was
enrolled in a public school and participated in general
education classes with his peers. He
attended a learning-support classroom to receive additional
instruction for math, but otherwise
received no additional educational services. Tyler resided at
home with his biological parents
and younger brother.
3 Presenting Complaints
Tyler was referred to the feeding program, due to lack of weight
gain, poor growth, and food
refusal. Before treatment Tylers weight was 29.94 kilograms, and
his height was 141centime-
ters, which was below the 3rd percentile in height and weight
compared to boys of his age.
Furthermore, it was calculated that Tyler had the height of an
average 10-year-old and the weight
of an average 9.5-year-old.
According to Tylers parents, Tylers began to refuse most foods
at 5 years of age but was a
very selective eater at 4 years of age. They also reported that
his diet became progressively more
selective until his intake was so limited that he became
nutritionally compromised and required
tube feedings. His parents did not report medical conditions
that could serve as a possible etiol-
ogy to his initial food refusal, and a review of his medical
records did not reveal possible biologi-
cal factors. His parents did report that by the age of 16, Tyler
had been dependent on gastrostomy
by Andreea Nicoleta Nicolae on October 12,
2011ccs.sagepub.comDownloaded from
http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/
-
8/10/2019 trating food refusal in adolescent with asperger's
disorder
4/14
262 Clinical Case Studies 9(4)
tube feeds for 9 years. Before treatment, his daily nutritional
needs were met predominantly by
32 ounces of Nutren 2.0 formula delivered through gastrostomy
tube. Tyler drank only water and
ate small amounts of a specific brand of three different foods.
Though these three foodsbowtie
pasta, ham steak, and cerealwere of different textures, Tyler
mentioned not liking how some
foods felt in his mouth. In addition to being selective by type
and texture, he only used specificutensils and dishes and only ate
dinner. Tyler was given the diagnosis of food refusal as he did
not eat enough to sustain growth; however, he did not fit the
more typical pattern of children with
food refusal. A recent review of food refusal examined 38
interventions studies and found that
212 of 218 participants described in these food refusal
intervention studies had some form of
medical issue that could have served as an etiology to the food
refusal (Williams, Field, &
Seiveling, 2010). In a sample of children referred to feeding
programs, the most common feed-
ing problem found among the children with autism spectrum
disorders was food selectivity
(Field et al., 2003), but the severity of the feeding problems
in these children was not as extreme
as exhibited by Tyler.
4 History
Tyler had a gastrostomy tube placed at 7 years of age, secondary
to poor growth and malnutrition.
Other than his chronic refusal to eat, Tyler presented with no
medical conditions (e.g., gastro-
esophageal reflux disease, oral-motor deficits, delayed gastric
emptying, vomiting, etc.) that
would have interfered with his ability to eat or drink. Tyler
had been diagnosed with Aspergers
disorder as a preschooler. Previous attempts to address his food
refusal by community providers
and by two outpatient visits to a feeding program were not
successful in improving his food and
beverage intake.
5 Assessment
Before treatment, Tylers parents completed a developmental,
medical, and feeding history. The
parents also provided a list of all food and liquids eaten
before treatment. In reviewing the history
with Tylers parents, they described behaviors such as refusal to
speak on a telephone or demon-
strating distress at the sound of a vacuum that rose to the
level of specific phobias.
Baseline meals were conducted and data collected on the
dependent measures are described
in Section 7.1. In these baseline meals, Tyler was presented
with six foods and told he could eat
any of the foods presented but was not required to eat anything.
During baseline meals, Tyler
was presented with both the three foods he ate before treatment
as well as novel foods from all
food groups. During baseline, Tyler ate only foods he had
previously eaten and avoided all novelfoods. After three baseline
meals, during which Tyler ate only small amounts of previously
eaten
foods, it was decided to implement treatment. As Tyler had only
eaten the same foods for several
years, and the baseline meals confirmed this pattern of
consumption, it was determined that
additional baseline meals were not necessary.
Potential reinforcers were determined by interviewing both Tyler
and his parents. These rein-
forcers included access to his laptop, preferred videos, and
computer games.
5.1 Interobserver Agreement
Interobserver agreement data were recorded to account for
experimenter bias while providing
treatment to Tyler. Data were collected by having either an
independent observer collecting data
through a one-way observation mirror or by observing
videorecordings of meals. These data were
compared to the data collected by the therapist who conducted
the meal session. Interobserver
by Andreea Nicoleta Nicolae on October 12,
2011ccs.sagepub.comDownloaded from
http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/
-
8/10/2019 trating food refusal in adolescent with asperger's
disorder
5/14
Roth et al. 263
agreement for bites consumed, negative
vocalization,andgaggingwas calculated for 28% of the
meals conducted and was calculated to be 93.38%, 100%, and 100%,
respectively. For the depen-
dent variable liquid consumed,no agreement data were collected.
Each beverage consumed was
weighed before and after treatment (using the same kitchen
scale).
5.2 Treatment Integrity
Meals were videorecorded across the course of treatment. These
videorecordings were rated
using a 14-item treatment integrity checklist developed by the
experimenters to ensure consistent
implementation of treatment procedures. Each video was rated by
an experimenter who was not
involved in implementation of the meal being rated. Overall
treatment integrity was calculated
to be 99.6% of the 17 sessions recorded.
6 Case Conceptualization
The participants age and high level of functioning makes him
dissimilar to not only to previouspatients treated for food refusal
in this feeding program (who tend to be younger and have more
significant delays in development) but also to participants in
other published food refusal inter-
vention studies (Williams, Field, & Seiveling, 2010). A
significant consideration in the develop-
ment of this intervention were the characteristics of the
participant. His parents described him as
being anxious, which led us to focus more on the use of
establishing operations and antecedent
manipulations rather than the escape extinction procedures used
in past research (Williams &
Seiverling, 2010). Although escape extinction has been shown to
be a highly effective compo-
nent in the treatment of food refusal, like all extinction
procedures, it can be accompanied with
negative side-effects such as crying or tantrums. One of the
unique aspects to this intervention
was the way in which the daily schedule of meals was presented.
Though the daily schedule ofmeals is often not mentioned in
articles describing the treatment of food refusal, some
descrip-
tions of interventions describe participants receiving between
three (Linscheid, 2006) and five
(Patel, Piazza, Layer, Coleman, & Swartzwelder, 2005) meals
or sessions per day. In this treat-
ment, a meal was presented, the participant completed the meal,
exchanged his tokens for time
in his arcade, and then when the time earned in the arcade had
elapsed, another meal was
presented. Thus, the participant controlled the number of meals
that occurred per day through his
response effort in meals. The greater number of bites and drinks
consumed at a meal would not
only result in more minutes spent in his arcade but would also
limit the number of meals pre-
sented per day. The participant learned this relationship
quickly and would verbalize during
meals that he would eat more to get a long break.Even though
this intervention consisted of several components including
appetite manipula-
tion, stimulus fading for both solids and liquids, token economy
for solids, and escape prevention
for liquids, it was not clear which of the components were
necessary in producing the positive
outcome. Appetite manipulation, in this case the elimination of
tube feeds, has been suggested as
being the most important component in the treatment of food
refusal (Linscheid, 2006) and
was probably important in this intervention. Before elimination
of the tube feeds, the participant
was not able to consume enough calories to meet caloric goals,
but after elimination of the tube
feeds his intake increased rapidly and dramatically. Before
treatment, the participant refused to
taste novel foods to the point of crying and gagging for his
parents. The stimulus fading for both
the solids and liquids possibly reduced the response effort to
the point that the participant was
able to successfully consume bites and drinks without collateral
behaviors. Numerous times
across the course of treatment, the participant verbalized that
he liked a particular food or that the
food tasted good to foods that his parents reported he had
previously refused without tasting. The
by Andreea Nicoleta Nicolae on October 12,
2011ccs.sagepub.comDownloaded from
http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/
-
8/10/2019 trating food refusal in adolescent with asperger's
disorder
6/14
264 Clinical Case Studies 9(4)
stimulus fading may have made it possible for the participant to
taste novel foods and thus
develop preferences for them. It has been suggested that
positive reinforcement alone cannot
increase acceptance of food in children with food refusal but
may decrease negative vocaliza-
tions and inappropriate behavior in some children (Piazza,
2008).
Although our participant verbalized his liking for the preferred
activities in his arcade, itwas not clear whether access to these
items was responsible for his eating behavior. Though his
solid and liquid consumption dramatically increased during
treatment when compared to base-
line, functional control was not demonstrated. We did
demonstrate that the treatment package
increased intake when compared to baseline. Though we had
planned a usewithdraw design,
removing the token economy, to examine the effectiveness of the
treatment, this plan was not
successful. On the fifth day of treatment, meal without the
token economy was conducted. At this
meal, the participants intake was equivalent to previous
treatment meals. When the participant
was informed that he would not be earning tokens, he stated he
liked his arcade, but just really
needed a break, perhaps indicating that the tokens were not as
important in increasing feeding
behavior as was the backup reinforcer of earning time for a
break. Although the participants
performance in this probe meal was equivalent with meals
conducted with the token economy, itwas decided to continue the
token economy until his intake goals were met and then
eliminate
the token economy for generalization training. For the last 3
days of treatment, the participant
was offered meals without the token economy in a variety of
settings in preparation for dis-
charge. This intervention could also be conceptualized as being
based on negative reinforcement,
with the participant being able to avoid frequent meals by
expending a greater response effort
during meals and taking a greater number of bites and
drinks.
Although the solid food portion of this intervention could be
conceptualized as being based
on positive reinforcement as tokens were earned for consumption,
it is likely that negative rein-
forcement, in terms of avoiding more frequent meals by expending
a greater response effort and
eating more, is a significant factor in the success of the
intervention. There was no escape pre-vention component for solid
foods; however, it was included for liquids to ensure a minimal
level
of liquid consumption because the participant had been dependent
on tube feeds for 9 years and
it was unclear whether he would drink enough to maintain
hydration. There were only 11 meals
during the entire course of treatment when the participant had
to sit in the therapy room beyond
the 15-minute meal duration to complete his liquids. The escape
prevention contingency never
came into effect after the eighth day of treatment. Given the
participants success with the food,
it is possible that the escape prevention component was not
necessary.
7 Course of Treatment and Assessment of Progress
Treatment sessions were conducted in a therapy room equipped
with two tables, three chairs, an
observation window, and a camcorder. Tokens consisted of three
stacks of laminated cards in the
shape of a lions paw, each of a different color. Also, an
electronic kitchen scale was used to
measure liquid consumption before and after every meal.
7.1 Dependent Measures
Data were collected on four variables. The participants solid
intake was measured by bites
consumed, operationally defined as the number of bites the
participant placed in his mouth and
swallowed. Liquid consumedwas measured in ounces by subtracting
the postweights of the
beverages offered from their preweights. Water and other
beverages (e.g., milk, juice) were
measured separately.Number of solid foods was used as a measure
of diet variety and determined
by counting each food eaten by the participant, but only if two
tablespoons of that food was
by Andreea Nicoleta Nicolae on October 12,
2011ccs.sagepub.comDownloaded from
http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/
-
8/10/2019 trating food refusal in adolescent with asperger's
disorder
7/14
-
8/10/2019 trating food refusal in adolescent with asperger's
disorder
8/14
266 Clinical Case Studies 9(4)
In meals where the participant did not consume the beverages
within the 15-minute period, a
timer was set to record the time that had elapsed between the
end of the session and the con-
sumption of the drinks. The participant was required to finish
the three rated beverages before
leaving the room and exchanging his tokens. This was the only
escape prevention contingency
used in the intervention.There was also a stimulus-fading
criterion for the liquids. If the participant completed any
rated beverage within the 15-minute time limit, the quantity of
this particular beverage was
increased by 0.25 ounce. If the participant did not finish a
particular drink before the timer rang,
it remained at the same quantity for the next session. Once the
drinks were consumed (either
before or after the timer rang), the participant was permitted
to exchange the tokens for access to
the arcade. Once the participant was in the arcade, the timer
was set to the number of tokens
exchanged (1 bite/1 drink =1, 2, or 3 minutes of arcade time
depending on the rating of food and
drink consumed). On each treatment day, the participant picked
three beverages from his rated
liquid list that were not used during the previous treatment
day. As it was expected that there
would not be an even distribution of beverages among the three
categories, multiple drinks were
sometimes used from the same category. For example, two drinks
from Category 2, one drinkfrom Category 3, and no drink from
Category 1. Again, having the child choose different bever-
ages on subsequent days was done to increase exposure to a wider
range of drinks.
7.2.3 Liquid Procedure Modified. As gastrostomy tube feeds were
eliminated on the firstday of treatment and the participant was not
receiving the nutritional supplement administered
through a gastrostomy tube, it was decided to increase milk
consumption as a means of increas-
ing the participants daily caloric intake. This was accomplished
by modifying the liquid proce-
dure on the third day of treatment. Milk was also systematically
increased using the same
criterion as the other beverages. Milk was included for all
meals and as milk was increased the
amount of water was decreased by the same amount. Consistent
with the other beverages,
changes in volume of milk were not made, unless the milk was
completely consumed before thetimer sounded. By the eighth day of
treatment, Tyler was drinking a range of beverages in addi-
tion to milk and water. It was decided at this point to reduce
the number of beverages offered to 3,
one drink from his rated liquid list, milk and water.
7.3 Generalization Training
During the last 3 treatment days, meals were conducted as they
would be in the participants
home and school settings. For each meal, the participant was
given one main dish or entre
(e.g., Salisbury steak, turkey sandwich, cheeseburger, peanut
butter and jelly sandwich, French
toast sticks), and three or four side dishes (e.g., cooked
vegetables, salad, fresh fruit, cookies,chips). During each session
for each of these 3 days, no food items were presented consecu-
tively. Data were collected on each bite consumed during each
generalization meal. Throughout
the generalization training, no tokens were distributed and no
foods were ranked. However, the
participant did receive breaks contingent on the number of bites
consumed. It was determined
that if the participant consumed less than 25 bites he would
receive a 20-minute break, but if he
consumed 25 bites or more then he received at least a 45-minute
break. During these breaks, he
was not permitted to watch preferred videos, play electronic
games, or use his laptop. He was
allowed to take walks, look at books, or magazines and converse
with parents or staff.
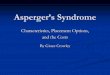
7.4 OutcomesThere was a substantial increase in bites
consumedacross the course of treatment as shown in
Figure 1. As demonstrated in Figure 1, the participant consumed
10 bites in the first treatment
by Andreea Nicoleta Nicolae on October 12,
2011ccs.sagepub.comDownloaded from
http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/
-
8/10/2019 trating food refusal in adolescent with asperger's
disorder
9/14
Roth et al. 267
0
10
20
30
40
50
60
1 4 7 10 1 3 1 6 19 2 2 2 5 28 3 1 3 4 37 4 0 4 3 46 4 9 5 2 55
5 8 6 1 64 6 7 7 0 73 7 6 7 9 82 8 5 8 8 91
Numberofbitesconsumed
Meal
Baseline
Treatment
Generalization
Figure 1.Number of bites consumed per mealNote: The data depict
three baseline meals (solid diamond) followed by the treatment
package (solid square). A singleprobe meal without token economy
(open triangle) was conducted with a return to the treatment
package. The finalphase depicts generalization without the token
economy (open triangle). The graph only shows number of bites
anddoes not display the increase in bite size that occurred across
treatment.
meal and 45 bites on the last treatment meal. As described in
the solid food procedure, bite size
for each food was increased as Tyler met criterion for that
food; thus, the bite size of each food
started at the size of a grain of rice, then progressed to pea
size, half teaspoon, and finally fullteaspoon size. Although not
depicted in the graphs, the bite size of foods was increased as
each
particular food met criterion. Thus, not only did the number of
bites increase across the course of
treatment but the size of the individual bites also increased.
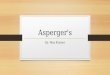
Across treatment, the number of
meals per day decreased as the number of bites increased. These
changes are shown in Figure 2.
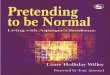
Liquid consumedwas measured in terms of ounces consumed, with
water and milk displayed
as separate data paths in Figure 3. On the third day of
treatment, milk was introduced, and
3.25 ounces were consumed for the day. On the last treatment
day, a total of 31 ounces of milk
were consumed. In only 11 of the 93 meals did the participant
take longer than the allotted
15 minutes to consume the liquids for a particular meal. All of
these 11 meals were in the initial
8 days of treatment.Again, before treatment, the participant
consumed only three foods; at the end of treatment,
the number of solid foodsthat the participant consumed totaled
78 foods. At the 1-month follow-
up, the participants parents reported he had added an additional
27 new foods to his diet. Before
treatment, the participant drank only water. At the end of
treatment, the number of liquidscon-
sumed was a total of 13 different drinks and at the 1-month
follow-up visit the participant had
added 2 more drinks to his diet. Tyler drank only water before
treatment; he drank milk and a
variety of other beverages, mostly juices, by the end of
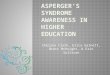
treatment. When analyzing data from the
two aberrant behaviors recorded, negative vocalization and
gagging, it was found that on the first
treatment day the participant had engaged in a total eight
occurrences of these two behaviors,
and, after the first day of treatment, the participant never
exceeded two instances of negative
vocalizing or gagging when combined per day as shown in Figure
4.
Before treatment, the participant was largely dependent on tube
feeds, receiving 2000 calories
per day through tube feeds. All tube feeds were eliminated, and
the participant remained off all
by Andreea Nicoleta Nicolae on October 12,
2011ccs.sagepub.comDownloaded from
http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/
-
8/10/2019 trating food refusal in adolescent with asperger's
disorder
10/14
268 Clinical Case Studies 9(4)
0
1
2
3
4
5
6
7
8
9
0
5
10
15
20
25
30
35
40
45
50
1 1 2 3 4 5 6 7 8 9 10 11 12 13 14
Mealsconducted
Averagenumberofbitescons
umed
Treatment Day
Average number of bitesconsumedMeals
BL Treatment Generalization
Figure 2.Average number of bites consumed per treatment dayNote:
This graph depicts the increase in bites per meal across both the
treatment and generalization (solidsquares) phases. Stimulus fading
was used across the course of the treatment phase, where the size
of the biteswas systematically increased. The number of bites
increased further across the generalization phase. The graphonly
shows average number of bites consumed per day and does not display
the average increase in bite size thatoccurred across each day.
0
1
2
3
4
5
6
7
8
9
0
1
2
3
4
5
6
7
8
1 1 2 3 4 5 6 7 8 9 10 11 12 13 14
Mealsconducted
Average
volumeconsumed(ounces)
Treatment day
Water
Milk
Meals
TreatmentBL Generalization
Figure 3.Average volume of liquids consumed per treatment
dayNote: On each day of treatment, the researchers added the total
number of ounces consumed for both milk andwater and divided it by
the number of sessions conducted each day. The z-axis measures the
number of mealsconducted, the abscissa measures what treatment day
the data were recorded, and the ordinate measures the
average volume of liquid consumed. The solid black squares
represent average water consumption per meal pertreatment day,
whereas the solid black circle markers represent average milk
consumption per meal per treatmentday. The figure demonstrates that
as milk was increased water was decreased, through the specified
fading protocol.Before treatment, the participant only drank
water.
by Andreea Nicoleta Nicolae on October 12,
2011ccs.sagepub.comDownloaded from
http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/
-
8/10/2019 trating food refusal in adolescent with asperger's
disorder
11/14
Roth et al. 269
tube feeds at the 1-month follow-up. Across the 3-week course of
treatment, the participant
gained 1 pound and 4 ounces.
7.5 Social Validation of Treatment Protocol
A total of 5 weeks after the conclusion of the study, the
participants parents were sent a satisfac-
tion questionnaire. They were asked 13 questions pertaining to
their satisfaction of the program
and using a 5-point Likert-type scale, they reported the highest
level of satisfaction for every
question. The parents also reported that family meals were more
enjoyable and that family stress
was reduced. The parents also provided additional comments
describing their childs success
stating that now their child never hesitates to taste a novel
food, began bringing a lunch to school,
and even eats leftover food from other family members
plates.
8 Complicating Factors
There were no complicating factors in the clients history of
significant importance that was not
already discussed in the client history section. Tyler was
compliant for a majority of treatment
and displayed low rates of inappropriate behavior as
demonstrated in Figure 4.
9 Managed Care Considerations
Tylers treatment was rapid and produced long-term success. In a
previous study, the cost of tube
feeding was reported for several patients. The lowest of the
costs reported was US$16, 320 per
year for the cost of the tube feeding supplies and formula
(Williams, Riegel, Gibbons, & Field,
2007). Tylers treatment was paid by state medical assistance who
was charged less than US$500/
day as a result of a contractual arrangement between the medical
facility and the medical
0
1
2
3
4
5
6
7
8
9
1 2 3 4 5 6 7 8 9 10 11 12 13 14
NumberofOccurrence
s
Treatment day
Negative vocalizations
Gagging
Total of abherrant behaviors
Figure 4.Aberrant behaviorsNote: The table depicts the data
collected for both negative vocalization (open square) and gagging
(open diamond)during each treatment day. As demonstrated, when
combining the occurrences of each behavior (open circle),
thebehaviors never appeared more than twice after the initial day
of treatment.
by Andreea Nicoleta Nicolae on October 12,
2011ccs.sagepub.comDownloaded from
http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/
-
8/10/2019 trating food refusal in adolescent with asperger's
disorder
12/14
270 Clinical Case Studies 9(4)
assistance program and the state. We estimate the cost of
treatment to the state medical assistance
program was lower than the cost of tube feeding for a period of
1 year. Tyler had received tube
feedings for 9 years; if intensive treatment had been provided
earlier with this same level of suc-
cess, the cost savings would have been substantial.
10 Follow-Up
Follow-up visits were scheduled 2 and 4 weeks after treatment in
the clinic. During these visits,
Tyler and his parents met with the licensed psychologist and
graduate intern feeding therapist to
discuss ongoing progress, to record stature to weight
proportions and answer any questions that
Tyler and his parents may have had, and to construct a timeline
for the complete removal of
Tylers gastrostomy tube. It was decided at these follow-up
meetings that the gastrostomy tube
would be removed in the spring due to the predicted active flu
season. In addition, follow-up was
also conducted over the phone once a week for 2 months. During
the placed phone calls, Tylers
variety of foods and liquids consumed as well as any weight or
height gains that were made since
the previous visit or phone call were discussed.As discussed
earlier, Tyler continued to add new foods and beverages to his diet
after dis-
charge. He eats meals without the token economy and is gaining
weight at faster rate than when
he was dependent on tube feedings.
11 Treatment Implications of the Case
It is with little argument that gastrostomy tubes and other tube
feeding methods (e.g., nasogastric
intubation) can be considered life saving. However, the effect
of gastrostomy tube placement on
an individuals quality of life has been reported as being both
physically and socially intrusive
and producing adverse psychological consequences (Jordan,
Philpin, Warring, Cheung, &Williams, 2006). The current study
demonstrated a successful intervention for the treatment of
food refusal that was brief in duration (14 days), easy to
implement, and generalized to both the
home and school settings. This type of intervention, in which
the number of meals and the dura-
tion of reinforcement is dependent on the participants amount of
response effort, may be well
suited for older children or adolescents who could understand
the contingencies and for whom
more intrusive escape prevention techniques are less socially
acceptable.
12 Recommendations to Clinicians and Students
To further develop the literature in this area, it is
recommended that future clinicians and studentsattempt a scientific
design that underlines the effectiveness of each component of this
treatment
package. Though it is believed that the combination of appetite
manipulation, stimulus fading,
and reinforcement made the treatment successful, the
contribution of each component was not
assessed.
This study also had the participant evaluate the difficulty of
each novel food and rate each
food on the basis of the perceived difficulty in eating that
food. Although this was not difficult
for staff, it was not clear whether this was necessary. It is
also recommended that future studies
examine other possible alternatives to having a participant earn
break time without having to
rank foods according to a level of perceived difficulty.
Declaration of Conflicting Interests
The authors declared that they had no conflicts of interests
with respect to their authorship or the publica-
tion of this article.
by Andreea Nicoleta Nicolae on October 12,
2011ccs.sagepub.comDownloaded from
http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/
-
8/10/2019 trating food refusal in adolescent with asperger's
disorder
13/14
Roth et al. 271
Funding
The authors received no financial support for the research
and/or authorship of this article.
References
Ahearn, W. H., Castine, T., Nault, K., & Green, G. (2001).
An assessment of food acceptance in children
with autism or pervasive developmental disorder-not otherwise
specified.Journal of Autism and Devel-
opmental Disorders, 31, 505-511.
Babbitt, R. L., Shore, B. A., Smith, M., Williams, K. E., &
Coe, D. A. (2001). Stimulus fading in the treat-
ment of adipsia.Behavioral Interventions, 16, 1-11.
Burklow, K. A., & Linscheid, T. (2004). Rapid inpatient
behavioral treatment for choking phobia in
children. Childrens Health Care, 33, 93-107.
Coe, D. A., Babbitt. R. L., Williams, K. E., Hajimihalis, C.,
Snyder, A. M., Ballard, C., . . . Efron, L. A.
(1997). Use of extinction and reinforcement to increase food
consumption and reduce expulsion.Jour-
nal of Applied Behavior Analysis, 30, 581-583.
Farrel, D. A., Hagopian, L. P., & Kurtz, P. F. (2001). A
hospital- and home-based behavior intervention
for a child with chronic food refusal and gastrostomy tube
dependence. Journal of developmental and
Physical Disabilities, 13, 407-418.
Field, D., Garland, M., & Williams, K. (2003). Correlates of
specific childhood feeding problems.Journal
of Paediatric and Child Health, 39, 299 -304.
Freeman, K. A., & Piazza, C. C. (1998). Combining stimulus
fading, reinforcement, and extinction to treat
food refusal.Journal of Applied Behavior Analysis, 31,
691-694.
Jordan, S., Philpin, S., Warring, J., Cheung, W. Y., &
Williams, J. (2006). Percutaneous endoscopic gastros-
tomies: The burden of treatment from a patient
perspective.Journal of Advanced Nursing, 56, 270-281.
Kahng, S., Boscoe, J. H., & Byrne, S. (2003). The use of
escape contingency and a token economy to
increase food acceptance.Journal of Applied Behavior Analysis,
36, 349-353.Kerwin, M. E. (1999). Empirically supported treatments
in pediatric psychology: Severe feeding problems.
Journal of Pediatric Psychology, 24, 193-214.
Linscheid, T. R. (2006). Behavioral treatments for pediatric
feeding disorders.Behavior Modification, 30,
6-23.
Luiselli, J. K. (2000). Cueing, demand fading, and positive
reinforcement to establish self-feeding and oral
consumption in a child with chronic food refusal.Behavior
Modification, 24, 348-358.
Luiselli, J. K., & Gleason, D. J. (1987). Combining sensory
reinforcement and texture fading procedures
to overcome chronic food refusal.Journal of Behavioral Therapy
and Experimental Psychiatry, 18,
149-155.
Luiselli, J. K., Ricciardi, J. N., & Gilligan, K. (2005).
Liquid fading to establish milk consumption by achild with
autism.Behavioral Interventions, 20, 155-163.
Patel, M.R., Piazza, C.C., Kelly, M.L., Ochsner, C.A., &
Santana,C.M. (2001) Using a fading procedure
to increase fluid consumption in a child with feeding problems.
Journal of Applied Behavior Analysis,
34, 357 -360.
Patel, M. R., Piazza, C. C., Layer, S. A., Coleman, R., &
Swartzwelder, D. M. (2005). A systematic evalua-
tion of food texture to decrease packing and increase oral
intake in children with pediatric feed disorder.
Journal of Applied Behavior Analysis, 38, 89-100.
Paul, C., Williams, K. E., Riegel, K., & Gibbons, B. (2007).
Combining repeated taste exposure and escape
prevention: An intervention for the treatment of extreme food
selectivity.Appetite, 49, 708-711.
Piazza, C. C. (2008). Feeding disorders and behavior: What have
we learned?Developmental Disabilities
Research Reviews, 14, 174-181.
Piazza C. C., Patel M. R., Gulotta, C. S., Sevin, B. M., &
Layer, S. A. (2003). On the relative contributions
of positive reinforcement and escape extinction in treatment of
food refusal. Journal of Applied Behavior
Analysis, 36, 309-324.
by Andreea Nicoleta Nicolae on October 12,
2011ccs.sagepub.comDownloaded from
http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/http://ccs.sagepub.com/
-
8/10/2019 trating food refusal in adolescent with asperger's
disorder
14/14
272 Clinical Case Studies 9(4)
Williams, K. E., Hendy, H., & Knecht, S. (2008). Parent
feeding practices and child variables associated
with childhood feeding problems.Journal of Developmental and
Physical Disabilities, 20, 231-242.
Williams, K.E., Seiverling, L., & Field, D.G. (2010). Food
refusal: A review of the literature.Research in
Developmental Disabilities, 31, 625-633.
Williams, K. E., Riegel, K., Gibbons, B., & Field, D. G.
(2007) Intensive behavioral treatment for severefeeding problems: A
cost-effective alternative to tube feeding. Journal of Physical and
Developmental
Disabilities, 19, 227-235.
Bios
Michael Roth, M.A., recently graduated with his Masters in
Applied Behavior Analysis from the Penn
State University, Harrisburg Campus. His clinical interests
include working with children with autism spec-
trum disorders.
Keith Williams, Ph.D., is the Director of the Feeding Program at
the Penn State Hershey Medical Center.
His research interests include the study of ingestive behaviors
in children with chronic health problems.
Candace Paul, M.A., is a Feeding Therapist II in the Feeding
Program at the Penn State Hershey Medical
Center. Her research interests include working with children
with food selectivity and choking phobias.




















![Asperger's syndrome final[1]](https://img.pdfslide.us/doc/110x75/5463f4edaf795969338b46dc/aspergers-syndrome-final1.jpg)