Embed Size (px)
Citation preview

Management of Diabetes andHyperglycemia in HospitalsSTEPHEN CLEMENT MD, CDE
1
SUSAN S. BRAITHWAITE, MD2
MICHELLE F. MAGEE, MD, CDE3
ANDREW AHMANN, MD4
ELIZABETH P. SMITH, RN, MS, CANP, CDE1
REBECCA G. SCHAFER, MS, RD, CDE5
IRL B. HIRSCH, MD6
ON BEHALF OF THE DIABETES IN HOSPITALS
WRITING COMMITTEE
D iabetes increases the risk for disor-ders that predispose individuals tohospitalization, including coronary
artery, cerebrovascular and peripheralvascular disease, nephropathy, infection,and lower-extremity amputations. Themanagement of diabetes in the hospital isgenerally considered secondary in impor-tance compared with the condition thatprompted admission. Recent studies (1,2)have focused attention to the possibilitythat hyperglycemia in the hospital is notnecessarily a benign condition and thataggressive treatment of diabetes and hy-perglycemia results in reduced mortalityand morbidity. The purpose of this tech-nical review is to evaluate the evidencerelating to the management of hypergly-
cemia in hospitals, with particular focuson the issue of glycemic control and itspossible impact on hospital outcomes.The scope of this review encompassesadult nonpregnant patients who do nothave diabetic ketoacidosis or hyperglyce-mic crises.
For the purposes of this review, thefollowing terms are defined (adaptedfrom the American Diabetes Association[ADA] Expert Committee on the Diagno-sis and Classification of Diabetes Mellitus)(3):
● Medical history of diabetes: diabeteshas been previously diagnosed and ac-knowledged by the patient’s treatingphysician.
● Unrecognized diabetes: hyperglycemia(fasting blood glucose �126 mg/dl orrandom blood glucose �200 mg/dl)occurring during hospitalization andconfirmed as diabetes after hospitaliza-tion by standard diagnostic criteria, butunrecognized as diabetes by the treat-ing physician during hospitalization.
● Hospital-related hyperglycemia: hyper-glycemia (fasting blood glucose �126mg/dl or random blood glucose �200mg/dl) occurring during the hospital-ization that reverts to normal after hos-pital discharge.
What is the prevalence of diabetes inhospitals?The prevalence of diabetes in hospitalizedadult patients is not known. In the year2000, 12.4% of hospital discharges in theU.S. listed diabetes as a diagnosis. Theaverage length of stay was 5.4 days (4).Diabetes was the principal diagnosis inonly 8% of these hospitalizations. The ac-curacy of using hospital discharge diag-nosis codes for identifying patients withpreviously diagnosed diabetes has beenquestioned. Discharge diagnosis codesmay underestimate the true prevalence ofdiabetes in hospitalized patients by asmuch as 40% (5,6). In addition to havinga medical history of diabetes, patients pre-senting to hospitals may have unrecog-nized diabetes or hospital-relatedhyperglycemia. Umpierrez et al. (1) re-ported a 26% prevalence of known diabe-tes in hospita l ized pat ients in acommunity teaching hospital. An addi-tional 12% of patients had unrecognizeddiabetes or hospital-related hyperglyce-mia as defined above. Levetan et al. (6)reported a 13% prevalence of laboratory-documented hyperglycemia (blood glu-cose �200 mg/dl (11.1 mmol) in 1,034consecutively hospitalized adult patients.Based on hospital chart review, 64% ofpatients with hyperglycemia had preex-isting diabetes or were recognized as hav-ing new-onse t d i abe t e s dur inghospitalization. Thirty-six percent of thehyperglycemic patients remained unrec-ognized as having diabetes in the dis-charge summary, although diabetes or“hyperglycemia” was documented in
● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
From the 1Georgetown University Hospital, Washington, DC; the 2University of North Carolina, Chapel Hill,North Carolina; 3Medstar Research Institute at Washington Hospital Center, Washington, DC; the 4OregonHealth and Science University, Portland, Oregon; the 5VA Medical Center, Bay Pines, Florida; and the6University of Washington, Seattle, Washington.
Address correspondence and reprint requests to Dr. Stephen Clement, MD, Georgetown UniversityHospital, Department of Endocrinology, Bldg. D, Rm. 232, 4000 Reservoir Rd., NW, Washington, DC20007. E-mail: [email protected]..
Received and accepted for publication 1 August 2003.S.C. has received honoraria from Aventis and Pfizer. S.S.B. has received honoraria from Aventis and
research support from BMS. M.F.M. has been on advisory panels for Aventis; has received honoraria fromAventis, Pfizer, Bristol Myers Squibb, Takeda, and Lilly; and has received grant support from Aventis, Pfizer,Lilly, Takeda, Novo Nordisk, Bayer, GlaxoSmithKline, and Hewlett Packard. A.A. has received honorariafrom Aventis, Bayer, BMS, GlaxoSmithKline, Johnson & Johnson, Lilly, Novo Nordisk, Pfizer, and Takedaand research support from Aventis, BMS, GlaxoSmithKline, Johnson & Johnson, Lilly, Novo Nordisk, Pfizer,Roche, and Takeda. E.P.S. holds stock in Aventis. I.B.H. has received consulting fees from Eli Lilly, Aventis,Novo Nordisk, and Becton Dickinson and grant support from Novo Nordisk.
Additional information for this article can be found in two online appendixes at http://care.diabetesjournals.org.
Abbreviations: ADA, American Diabetes Association; AMI, acute myocardial infarction; CDE, certifieddiabetes educator; CHF, congestive heart failure; CK, creatinine kinase; CQI, continuous quality improve-ment; CRP, C-reactive protein; CSII, continuous subcutaneous insulin infusion; CVD, cardiovascular dis-ease; DIGAMI, Diabetes and Insulin-Glucose Infusion in Acute Myocardial Infarction; DSME, diabetesself-management education; DSWI, deep sternal wound infection; FFA, free fatty acid; GIK, glucose-insulin-potassium; ICAM, intercellular adhesion molecule; ICU, intensive care unit; IL, interleukin; IIT, intensiveinsulin therapy; JCAHO, Joint Commission of Accredited Hospital Organization; LIMP, lysosomal integralmembrane protein; MCP, monocyte chemoattractant protein; MI, myocardial infarction; MRI, magneticresonance imaging; MRS, magnetic resonance spectroscopy; NF, nuclear factor; NPO, nothing by mouth;PAI, plasminogen activator inhibitor; PCU, patient care unit; PKC, protein kinase C; PBMC, peripheral bloodmononuclear cell; PMN, polymorphonuclear leukocyte; ROS, reactive oxygen species; TNF, tumor necrosisfactor; TPN, total parenteral nutrition; UKPDS, U.K. Prospective Diabetes Study.
A table elsewhere in this issue shows conventional and Systeme International (SI) units and conversionfactors for many substances.
© 2004 by the American Diabetes Association.
R e v i e w s / C o m m e n t a r i e s / P o s i t i o n S t a t e m e n t sT E C H N I C A L R E V I E W
DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004 553

the progress notes for one-third of thesepatients.
Norhammar et al. (7) studied 181consecutive patients admitted to the cor-onary care units of two hospitals in Swe-den with acute myocardial infarction(AMI), no diagnosis of diabetes, and ablood glucose �200 mg/dl (�11.1mmol/l) on admission. A standard 75-gglucose tolerance test was done at dis-charge and again 3 months later. The au-thors found a 31% prevalence of diabetesat the time of hospital discharge and a25% prevalence of diabetes 3 months af-ter discharge in this group with no previ-ous diagnosis of diabetes.
Using the A1C test may be a valuablecase-finding tool for identifying diabetesin hospitalized patients. Greci et al. (8)reported that an A1C �6% was 100%specific and 57% sensitive for identifyingpersons with diabetes in a small cohort ofpatients admitted through the emergencydepartment of one hospital with a randomblood glucose �126 mg/dl (7 mmol/l)and no prior history of diabetes.
From the patient’s perspective, 24%of adult patients with known diabetes sur-veyed in 1989 reported being hospital-ized at least once in the previous year (9).The risk for hospitalization increasedwith age, duration of diabetes, and num-ber of diabetes complications. Personswith diabetes reported being hospitalizedin the previous year three times more fre-quently compared with persons withoutdiabetes. In summary, the prevalence ofdiabetes in hospitalized adults is conser-vatively estimated at 12.4–25%, depend-ing on the thoroughness used inidentifying patients.
WHAT IS THE LINKBETWEEN HIGH BLOODGLUCOSE AND POOROUTCOMES? POSSIBLEMECHANISMS — The mechanismof harm from hyperglycemia on variouscells and organ systems has been studiedin in vitro systems and animal models.This research has centered on the im-mune system, mediators of inflammation,vascular responses, and brain cell re-sponses.
Hyperglycemia and immune functionThe association of hyperglycemia and in-fection has long been recognized, al-though the overall magnitude of theproblem is still somewhat unclear
(10,11). From a mechanistic point ofview, the primary problem has been iden-tified as phagocyte dysfunction. Studieshave reported diverse defects in neutro-phil and monocyte function, includingadherence, chemotaxis, phagocytosis,bacterial killing, and respiratory burst(10–20). Bagdade et al. (14) were amongthe first to attach a glucose value to im-provement in granulocyte function whenthey demonstrated significant improve-ment in granulocyte adherence as themean fasting blood glucose was reducedfrom 293 � 20 to 198 � 29 mg/dl(16.3–11 mmol/l) in 10 poorly controlledpatients with diabetes. Other investiga-tors have demonstrated similar improve-ments in leukocyte function withtreatment of hyperglycemia (17,21–23).In vitro trials attempting to define hyper-glycemic thresholds found only rough es-timates that a mean glucose �200 mg/dl(11.1 mmol/l) causes leukocyte dysfunc-tion (13,14,16,24–26).
Alexiewicz et al. (17) demonstratedelevated basal levels of cytosolic calciumin the polymorphonuclear leukocytes(PMNs) of patients with type 2 diabetesrelative to control subjects. Elevated cyto-solic calcium was associated with reducedATP content and impaired phagocytosis.There was a direct correlation betweenPMN cytosolic calcium and fasting serumglucose. These were both inversely pro-portional to phagocytic activity. Glucosereduction with glyburide resulted in re-duced cytosolic calcium, increased ATPcontent, and improved phagocytosis.
Classic microvascular complicationsof diabetes are caused by alterations in thealdose reductase pathway, AGE pathway,reactive oxygen species pathway, and theprotein kinase C (PKC) pathway (rev. in27). Several of these pathways may con-tribute to immune dysfunction. PKC maymediate the effect of hyperglycemia onneutrophil dysfunction (28). Liu et al.(29) found that decreased phagocytic ac-tivity in diabetic mice correlated inverselywith the formation of AGEs, although adirect cause-and-effect relationship wasnot proven. Ortmeyer and Mohsenin (30)found that hyperglycemia caused im-paired superoxide formation along withsuppressed activation of phospholipaseD. Reduced superoxide formation hasbeen linked to leukocyte dysfunction. An-other recent study found a link amonghyperglycemia, inhibition of glucose-6-phosphate dehydrogenase, and reduced
superoxide production in isolated humanneutrophils (31). Sato and colleagues(32–34) used chemiluminescence to eval-uate neutrophil bactericidal function. Theauthors confirmed a relationship betweenhyperglycemia and reduced superoxideformation in neutrophils. This defect wasimproved after treatment with an aldosereductase inhibitor. This finding suggeststhat increased activity of the aldose reduc-tase pathway makes a significant contri-bution to the incidence of diabetes-related bacterial infections.
Laboratory evidence of the effect ofhyperglycemia on the immune systemgoes beyond the granulocyte. Nonenzy-matic glycation of immunoglobulins hasbeen reported (35). Normal individualsexposed to transient glucose elevationshow rapid reduction in lymphocytes, in-cluding all lymphocyte subsets (36). Inpatients with diabetes, hyperglycemia issimilarly associated with reduced T-cellpopulations for both CD-4 and CD-8 sub-sets. These abnormalities are reversedwhen glucose is lowered (37).
In summary, studies evaluating theeffect of hyperglycemia on the immunesystem comprise small groups of normalindividuals, patients with diabetes of var-ious duration and types, and animal stud-ies. These studies consistently show thathyperglycemia causes immunosuppres-sion. Reduction of glucose by a variety ofmeans reverses the immune functiondefects.
Hyperglycemia and thecardiovascular systemAcute hyperglycemia has numerouseffects on the cardiovascular system. Hy-perglycemia impairs ischemic precondi-tioning, a protective mechanism forischemic insult (38). Concomitantly, in-farct size increases in the setting of hyper-glycemia. The same investigatorsdemonstrated reduced coronary collat-eral blood flow in the setting of moder-ately severe hyperglycemia (39). Acutehyperglycemia may induce cardiac myo-cyte death through apoptosis (40) or byexaggerating ischemia-reperfusion cellu-lar injury (41).
Other vascular consequences of acutehyperglycemia relevant to inpatient out-comes include blood pressure changes,catecholamine elevations, platelet abnor-malities, and electrophysiologic changes.Streptozotocin-induced diabetes in ratsresults in significant hemodynamic
Management of diabetes and hyperglycemia in hospitals
554 DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004

changes as well as QT prolongation (42).These changes were reversed with correc-tion of hyperglycemia. In humans,Marfella et al. (43) reported increased sys-tolic and diastolic blood pressure and in-creased endothelin levels with acutehyperglycemia in patients with type 2 di-abetes. The same researchers also inducedacute hyperglycemia (270 mg/dl or 15mmol/l) over 2 h in healthy men. Thisproduced elevated systolic and diastolicblood pressure, increased pulse, elevationof catecholamine levels, and QTc prolon-gation (44). Other investigators havedemonstrated an association betweenacute hyperglycemia and increased vis-cosity, blood pressure (45), and natiureticpeptide levels (46).
Hyperglycemia and thrombosisMultiple studies have identified a varietyof hyperglycemia-related abnormalities inhemostasis, favoring thrombosis (47–51).For example, hyperglycemic changes inrats rapidly reduce plasma fibrinolytic ac-tivity and tissue plasminogen activator ac-tivity while increasing plasminogenactivator inhibitor (PAI)-1 activity (52).Human studies in patients with type 2 di-abetes have shown platelet hyperactivityindicated by increased thromboxane bio-synthesis (47). Thromboxane biosynthe-sis decreases with reduction in bloodglucose. Hyperglycemia-induced eleva-tions of interleukin (IL)-6 levels havebeen linked to elevated plasma fibrinogenconcentrations and fibrinogen mRNA(53,54).
Increased platelet activation as shownby shear-induced platelet adhesion andaggregation on extracellular matrix hasbeen demonstrated in patients with dia-betes (48). As little as 4 h of acute hyper-glycemia enhances platelet activation inpatients with type 2 diabetes (51). In thiscrossover, double-blind study, 12 pa-tients were subjected to hyperglycemic(250 mg/dl, 13.9 mmol/l) and euglycemic(100 mg/dl, 5.55 mmol/l) clamps. Hyper-glycemia precipitated stress-inducedplatelet activation as well as platelet P-selectin and lysosomal integral membraneprotein (LIMP) expression. Hyperglyce-mia also caused increased plasma vonWillebrand factor antigen, von Wille-brand factor activity, and urinary 11-dehydro-thromboxane B2 (a measure ofthromboxane A2 production). Thesechanges were not seen in the euglycemicstate.
If hyperglycemia-induced platelet hy-perreactivity is particularly evident withhigh–shear stress conditions, as sug-gested in the above studies, this findingmay explain the increased thromboticevents commonly seen in hospitalized pa-tients with diabetes.
Hyperglycemia and inflammationThe connection between acute hypergly-cemia and vascular changes likely in-volves inflammatory changes. Culturedhuman peripheral blood mononuclearcells (PBMCs), when incubated in highglucose medium (594 mg/dl, 33 mmol/l)for 6 h produce increased levels of IL-6and tumor necrosis factor (TNF)-� (53).TNF-� is apparently involved in IL-6 pro-duction. Blocking TNF-� activity withanti-TNF monoclonal antibody blocksthe stimulatory effect of glucose on IL-6production by these cells. Other in vitrostudies suggest that glucose-induced ele-vations in IL-6, TNF-�, and other factorsmay cause acute inflammation. This in-flammatory response to glucose has beenseen in adipose tissue, 3T3-L1 adipocytecell lines, vascular smooth muscle cells,PBMCs, and other tissues or cell types(55–61).
In humans, moderate elevation ofglucose to 270 mg/dl (15 mmol/l) for 5 hhas been associated with increased IL-6,IL-18, and TNF-� (62). Elevations ofthese various inflammatory factors havebeen linked to detrimental vascular ef-fects. For example, TNF-� extends thearea of necrosis following left anterior de-scending coronary artery ligation in rab-bits (63). In humans, TNF-� levels areelevated in the setting of AMI and corre-late with severity of cardiac dysfunction(63,64). TNF-� may also play a role insome cases of ischemic renal injury and incongestive heart failure (CHF) (57,65).Ischemic preconditioning is associatedwith decreased postischemic myocardialTNF-� production (66). IL-18 has beenproposed to destabilize atheroscleroticplaques, leading to acute ischemic syn-dromes (67).
One of the most commonly demon-strated relationships between hyperglyce-mia and inflammatory markers is the invitro induction of the proinflammatorytranscriptional factor, nuclear factor(NF)-�B by exposure of various cell typesto 1–8 days of hyperglycemia (58,59,68–71). In patients with type 1 diabetes, ac-t ivation of NF-�B in PBMCs was
positively correlated to HbA1c level (r �0.67, P � 0.005) (72). A recent study bySchiefkofer et al. (73) demonstrated invivo exposure to hyperglycemia (180 mg/dl, 10 mmol/l) for 2 h caused NF-�B ac-tivation.
Hyperglycemia and endothelial celldysfunctionOne proposed link between hyperglyce-mia and poor cardiovascular outcomes isthe effect of acute hyperglycemia on thevascular endothelium. In addition to serv-ing as a barrier between blood and tissues,vascular endothelial cells play a criticalrole in overall homeostasis. In the healthystate, the vascular endothelium maintainsthe vasculature in a quiescent, relaxant,antithrombotic, antioxidant, and antiad-hesive state (rev. in 74,75). During illnessthe vascular endothelium is subject todysregulation, dysfunction, insufficiency,and failure (76). Endothelial cell dysfunc-tion is linked to increased cellular adhe-sion, perturbed angiogenesis, increasedcell permeability, inflammation, andthrombosis. Commonly, endothelialfunction is evaluated by measuring endo-thelial-dependent vasodilatation, lookingmost often at the brachial artery. Humanin vivo studies utilizing this parameterconfirm that acute hyperglycemia to thelevels commonly seen in the hospital set-ting (142–300 mg/dl or 7.9 –16.7mmol/l) causes endothelial dysfunction(77–82). Only one study failed to showevidence of endothelial cell dysfunctioninduced by short-term hyperglycemia(83). The degree of endothelial cell dys-function after an oral glucose challengewas positively associated with the peakglucose level, ranging from 100 to 300mg/dl (5.5–16.7 mmol/l) (78,79). Hyper-glycemia may directly alter endothelialcell function by promoting chemical inac-tivation of nitric oxide (84). Other mech-anisms include triggering production ofreactive oxygen species (ROS) or activat-ing other pathways (rev. in 27). Despitecompelling experimental data, studies ex-amining a possible association among hy-perglycemia, endothelial function, andoutcomes have not to date been done inhospitalized patients.
Hyperglycemia and the brainAcute hyperglycemia is associated withenhanced neuronal damage following in-duced brain ischemia (85–98). Explora-t ion o f genera l mechan i sms o f
Clement and Associates
DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004 555

hyperglycemic damage has used variousmodels of ischemia and various measuresof outcomes. Models differ according totransient versus permanent ischemia aswell as global versus localized ischemia.There is some indication from animalstudies that irreversible ischemia or endarterial ischemia is not affected by hyper-glycemia (87,99,100). The major portionof the brain that is sensitive to injury fromhyperglycemia is the ischemic penumbra.This area surrounds the ischemic core.During evolution of the stroke, the isch-emic penumbra may evolve into infarctedtissue or may recover as viable tissue(87,99,101,102). One of the primarymechanistic links between hyperglycemiaand enhanced cerebral ischemic damageappears to be increased tissue acidosisand lactate levels associated with elevatedglucose concentrations. This has beenshown in various animal models with rareexception (94,102–108). Lactate hasbeen associated with damage to neurons,astrocytes, and endothelial cells (104). Inhumans, Parsons et al. (109) demon-strated that the lactate-to-choline ratiodetermined by proton magnetic reso-nance spectroscopy (MRS) had value inpredicting clinical outcomes and final in-farct size in acute stroke. More recently,the same investigators used this methodto demonstrate a positive correlation be-tween glucose elevations and lactate pro-duction (110). Through this mechanism,hyperglycemia appears to cause hypoper-fused at-risk tissue to progress to infarction.
Animal studies have shown addi-tional association of hyperglycemia withvarious acute consequences that likelyserve as intermediaries of adverse out-comes. For example, hyperglycemiacauses accumulation of extracellular glu-tamate in the neocortex. Increased gluta-mate levels predict ensuing neuronaldamage (95). A unique hippocampal cellculture model of “in vitro ischemia” dem-onstrated a similar relationship betweenhyperglycemia, glutamate activity, andincreased intracellular calcium with en-hanced cell death (98). Hyperglycemiahas also been associated with DNA frag-mentation, disruption of the blood-brainbarrier, more rapid repolarization in se-verely hypoperfused penumbral tissue,�-amyloid precursor protein elevation, aswell as elevated superoxide levels in neu-ronal tissue (111–115).
Many of the same factors noted ear-lier, linking hyperglycemia to cardiovas-
cular event outcomes, likely contribute toacute cerebrovascular outcomes. Specifi-cally, in brain ischemia models exposedto hyperglycemia, hydroxyl free radicalsare elevated and positively correlate withtissue damage (116). Likewise, antioxi-dants have a neuroprotective effect (117).Elevated glucose levels have also beenlinked to inhibition of nitric oxide gener-ation, increased IL-6 mRNA, decreasedcerebral blood flow, and evidence of vas-cular endothelial injury (90,92,118,119).Again, the composite of evidence sup-ports scientifically viable mechanisms ofcentral nervous system injury from hy-perglycemia in the acute setting.
Hyperglycemia and oxidative stressOxidative stress occurs when the forma-tion of ROS exceeds the body’s ability tometabolize them. Attempts to identify aunifying basic mechanism for many of thediverse effects of acute hyperglycemiapoint to the ability of hyperglycemia toproduce oxidative stress (58,69,120).Acute experimental hyperglycemia tolevels commonly seen in hospitalized pa-tients induces ROS generation. Endothe-lial cells exposed to hyperglycemia invitro switch from producing nitric oxideto superoxide anion (84). Increased ROSgeneration causes activation of transcrip-tional factors, growth factors, and second-ary mediators. Through direct tissueinjury or via activation of these secondarymediators, hyperglycemia-induced oxi-dative stress causes cell and tissue injury(58,59,62,70,72,74,80,121–127). In allcases studied, abnormalities were re-versed by antioxidants or by restoring eu-glycemia (58,59,70,72,80,122,127).
Is insulin per se therapeutic?Two large, well-done prospective studiessupport the relationship between insulintherapy and improved inpatient out-comes (2,128). The prevalent assumptionhas been that insulin attained this benefitindirectly by controlling blood glucose.However, a growing body of literatureraises the question of whether insulin mayhave direct beneficial effects independentof its effect on blood glucose (121,129–132).
Multiple studies suggest cardiac andneurological benefits of glucose-insulin-potassium (GIK) infusions (133–154).One may propose that such therapy sup-ports a direct effect of the insulin sinceblood glucose control is not the goal of
these infusions and the benefits have beendisplayed in normal humans and animals.Although the direct effect of insulin mayplay a significant role in benefits of GIKtherapy, other metabolic factors are likelyto be major contributors to the mecha-nism of this therapy. The theory promot-ing this form of therapy centers on theimbalance between low glycolytic sub-strate in the hypoperfused tissue and ele-vated free fatty acids (FFAs) mobilizedthrough catecholamine-induced lipolysis(41,155–159). In ischemic cardiac tissue,there is decreased ATP and increased in-o rgan i c phospha t e p roduc t i on(148,156,159). Adequate glycolytic ATPis important for maintaining cellularmembranes, myocardial contractility, andavoidance of the negative effect of fattyacids as substrate for ischemic myocar-dium (155,158–161). FFAs are associ-ated with cardiac sympathetic overactivity,worsened ischemic damage, and possiblyarrhythmias. Accordingly, using a modelof 60-min low-flow ischemia followed by30 min of reperfusion in rat hearts, inves-tigators have demonstrated the ability ofGIK infusion to increase glycolysis, de-crease ATP depletion, and maintain lowerinorganic phosphate levels in the affectedtissue (148). These effects extrapolated toimproved systolic and diastolic functionin this model. In other animal models,GIK infusion in improved left ventricularcontractility, decreased tissue acidosis,and decreased infarct size (144,152,162).
In small studies of individuals with orwithout diabetes undergoing coronary ar-tery bypass surgery, GIK therapy is asso-ciated with shorter length of intubationand shorter length of stay (142,143,163).As therapy for patients with an AMI, GIKtherapy is associated with the expecteddecrease in FFAs, decreased heart failure,and a suggestion of improved short-termsurvival (133–135,139,164). In fol-low-up of a first myocardial infarction(MI), individuals who received GIK ther-apy reported better stress tolerance, an el-evated ischemic threshold, and improvedmyocardial perfusion by 99 m-Tc-tetrofosmin–gated single photon emis-sion computed tomography (SPECT)compared with those receiving saline in-fusion (149). These studies of classic GIKtherapy with emphasis on glucose deliv-ery have been small and more suggestivethan conclusive. No large, randomized,placebo-controlled studies have been re-ported. Even less information is available
Management of diabetes and hyperglycemia in hospitals
556 DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004

regarding the use of GIK therapy instrokes or cerebral ischemia. Limitedstudies have demonstrated safety of GIKtherapy in the acute stroke patient, with atrend to reduced mortality, and a decreasein blood pressure (147,150). However,the data are clearly inadequate to makeany conclusions of benefit.
Beyond GIK therapy, one finds in-creasing support for a direct effect of in-sulin on many of the abnormalities thatunderlie inpatient complications. Insulintreatment, ranging in duration from briefeuglycemic-hyperinsulinemic clamps to2 months of ongoing therapy, improvesendothelial cell function (165–171).There are rare exceptions to this finding(172). Insulin also has vasodilatory prop-erties in the internal carotid and femoralarteries (165,167). The vasodilatoryproperties of insulin appear to be medi-ated at least in part by stimulating nitricoxide release (165,166). Aortic endothe-lial cell cultures have also demonstratedinsulin-induced nitric oxide synthase ac-tivity and increased nitric oxide levels(172,173). In a rat model, insulin inhibits
the upregulation of the endothelial adhe-sion molecule P-selectin expression seenas a consequence of elevated glucose lev-els (121).
Insulin infusion has anti-inflamma-tory effects (129,174,175). In a largestudy of intensive insulin infusion ther-apy in the intensive care unit, investiga-tors found decreased C-reactive protein(CRP) levels in insulin-treated patients(176). Cell culture studies have shownthe ability of insulin incubation to reduceoxidative stress and its associated apopto-sis in cardiomyocytes (177). In additionto the induction of endothelial-derivednitric oxide, human aorta cell and humanmononuclear cell culture studies haveshown dose-dependent reductions inROS, the proinflammatory transcriptionfactor NF-�B, intercellular adhesion mol-ecule (ICAM)-1, and the chemokinemonocyte chemoattractant protein(MCP)-1 (173,178–180). Insulin also in-hibits the production TNF-� and theproinflammatory transcription factorearly growth response gene (Egr)-1 (181).
These effects suggest a general anti-inflammatory action of insulin.
In an animal model of myocardialischemia, insulin given early in the acuteinsult reduced infarct size by �45%(182). This effect was mediated throughthe Akt and p70s6 kinase–dependent sig-naling pathway and was independent ofglucose. There is preliminary evidence ofinsulin’s ability to improve pulmonarydiffusion and CHF in humans (183).Studies have also suggested that insulinprotects from ischemic damage in thebrain, kidney, and lung (184–186). Incatabolic states such as severe burns, hy-perglycemia promotes muscle catabo-lism, while exogenous insulin producesan anabolic effect (187). Insulin therapyhas also been associated with an im-proved fibrinolytic profile in patients atthe time of acute coronary events, reduc-ing fibrinogen and PAI-1 levels (132). Fi-nally, insulin infusion reduces collagen-induced platelet aggregation and severalother parameters of platelet activity in hu-mans. This effect was attenuated in obeseindividuals (188).
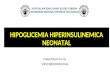
Figure 1—Link between hyperglyce-mia and poor hospital outcomes. Hy-perglycemia and relative insulindeficiency caused by metabolic stresstriggers immune dysfunction, releaseof fuel substrates, and other mediatorssuch as ROS. Tissue and organ injuryoccur via the combined insults of in-fection, direct fuel-mediated injury,and oxidative stress and other down-stream mediators. See text for details.
Clement and Associates
DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004 557

In summary, the overwhelming bal-ance of evidence supports a beneficial ef-fect of insulin in the acute setting.Whether these benefits are the result of adirect pharmacologic effect of insulin orrepresent an indirect effect by improvedglucose control, enhanced glycolysis, orsuppressed lipolysis is more difficult todetermine. Studies in cell cultures controlfor glucose but have other physiologiclimitations. Nevertheless, the data areprovocative and certainly leave the im-pression that insulin therapy in the hos-pital has significant potential for benefit.Considering the numerous contraindica-tions to the use of oral agents in the hos-pital, insulin is the clear choice for glucosemanipulation in the hospitalized patient.
Potential relationships betweenmetabolic stress, hyperglycemia,hypoinsulinemia, and poor hospitaloutcomesTo explain the dual role of glucose andinsulin on hospital outcomes, Levetanand Magee (189) proposed the followingrelationships. Elevations in counterregu-larory hormones accelerate catabolism,hepatic gluconeogenesis, and lipolysis.These events elevate blood glucose, FFAs,ketones, and lactate. The rise in glucoseblunts insulin secretion via the mecha-nism of glucose toxicity (190), resultingin further hyperglycemia. The vicious cy-cle of stress-induced hyperglycemia andhypoinsulinemia subsequently causesmaladaptive responses in immune func-tion, fuel production, and synthesis ofmediators that cause further tissue and or-gan dysfunction (Fig. 1). Thus, the com-bination of hyperglycemia and relativehypoinsulinemia is mechanistically posi-tioned to provide a plausible explanationfor the poor hospital outcomes seen inobservational studies.
WHAT ARE THE TARGETBLOOD GLUCOSE LEVELSFOR THE HOSPITALIZEDPATIENT?A rapidly growing body of literature sup-ports targeted glucose control in the hos-pital setting with potential for improvedmortality, morbidity, and health care eco-nomic outcomes. The relationship of hos-pital outcomes to hyperglycemia has beenextensively examined. Hyperglycemia inthe hospital may result from stress, de-compensation of type 1 diabetes, type 2diabetes, or other forms of diabetes
and/or may be iatrogenic due to adminis-tration of pharmacologic agents, includ-ing glucocorticoids, vasopressors, etc.Distinction between decompensated dia-betes and stress hyperglycemia is oftennot made or alternatively is not clear at thetime of presentation with an acute illness.When hyperglycemia is treated alongwith other acute problems, outcomes aregenerally improved. This section will re-view the evidence for outcomes from ob-servational and interventional studies inhospitalized patients with hyperglycemia.While observational reports abound, in-terventional studies that report improvedoutcomes with targeted glucose control—though few in number—are now begin-ning to provide a source of evidence in theliterature.
To make the case for defining targetsfor glucose control in hospital settings, itis necessary to examine the literature onboth short- and long-term mortality. Dataregarding diabetes and hyperglycemia-associated morbidity have emerged fromspecific clinical settings. These data in-clude infection rates, need for intensivecare unit admission, functional recovery,and health economic outcomes such aslength of stay and hospital charges. Fortheir practical implications and for thepurpose of this review, literature on theassociation of blood glucose level withoutcomes will be grouped into the medi-cal and surgical areas in which studieshave been reported as follows: generalmedicine and surgery, cardiovascular dis-ease (CVD) and critical care, and neuro-logic disorders (Table 1).
General medicine and surgeryObservational studies suggest an associa-tion between hyperglycemia and in-creased mortality. Recently, investigatorshave reported on outcomes correlatedwith blood glucose levels in the generalmedicine and surgery setting. Pomposelliet al. (191) studied 97 patients with dia-betes undergoing general surgery proce-dures. Blood glucose testing occurredevery 6 h. The authors found that a singleblood glucose level �220 mg/dl (12.2mmol/l) on the first postoperative day wasa sensitive (85%), but relatively nonspe-cific (35%), predictor of nosocomial in-fections. Patients with a blood glucosevalue(s) �220 mg/dl (12.2 mmol/l) hadinfection rates that were 2.7 times higherthan the rate for patients with blood glu-cose values �220 mg/dl (12.2 mmol/l).
When minor infections of the urinarytract were excluded, the relative risk (RR)for serious postoperative infection, in-cluding sepsis, pneumonia, and woundinfections, was 5.7.
Umpierrez et al. (1) reviewed 1,886admissions for the presence of hypergly-cemia (fasting blood glucose �126 mg/dlor random blood glucose �200 mg/dl ontwo or more occasions). Care was pro-vided on general medicine and surgeryunits. Among these subjects, there were223 patients (12%) with new hyperglyce-mia and 495 (26%) with known diabetes.Admission blood glucose for the normo-glycemic group was 108 � 10.8 mg/dl(6 � 0.6 mmol/l); for the new hypergly-cemia group, it was 189 � 18 mg/dl(10.5 � 1 mmol/l); and for known diabe-tes, it was 230.4 � 18 mg/dl (12.8 � 1mmol/l). After adjusting for confoundingfactors, patients with new hyperglycemiahad an 18-fold increased inhospital mor-tality and patients with known diabeteshad a 2.7-fold increased inhospital mor-tality compared with normoglycemic pa-tients. Length of stay was higher for thenew hyperglycemia group compared withnormoglycemic and known diabetic pa-tients (9 � 0.7, 4.5 � 0.1, and 5.5 � 0.2days, respectively, P � 0.001). Both thenew hyperglycemia and known diabeticpatients were more likely to require inten-sive care unit (ICU) care when comparedwith normoglycemic subjects (29 vs. 14vs. 9%, respectively, P � 0.01) and weremore likely to require transitional or nurs-ing home care. There was a trend towarda higher rate of infections and neurologicevents in the two groups with hypergly-cemia (1). It is likely that the “new” hy-perglycemic patients in this report were aheterogeneous population made up of pa-tients with unrecognized diabetes, predi-abetes, and/or stress hyperglycemiasecondary to severe illness.
The observational data from these twostudies suggest that hyperglycemia fromany etiology in the hospital on general med-icine and surgery services is a significantpredictor of poor outcomes, relative to out-comes for normoglycemic subjects. Patientswith hyperglycemia, with or without diabe-tes, had increased risk of inhospital mortal-ity, postoperative infections, neurologicevents, intensive care unit admission andincreased length of stay. The Pomposelli ar-ticle (191) found that a blood glucose levelof 220 mg/dl (12.2mmol/l) separated pa-tients for risk of infection. Data from the
Management of diabetes and hyperglycemia in hospitals
558 DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004

Tab
le1—
Evi
denc
efo
ras
soci
atio
nof
bloo
dgl
ucos
ele
velw
ith
clin
ical
outc
omes
Clin
ical
sett
ing
Thr
esho
ldBG
leve
ls[m
g/dl
,(m
mol
/l)]
Out
com
esan
dco
mm
ents
Gen
eral
med
icin
ean
dsu
rger
yM
orta
lity,
ICU
adm
its,
leng
thof
stay
,and
nurs
ing
hom
eor
tran
siti
onal
care
adm
its
corr
elat
edw
ith
BGan
dgl
ucos
eto
lera
nce
stat
us:
Nor
mog
lyce
mia
�10
8�
10.8
(6�
0.6)
;N
ewhy
perg
lyce
mia
�18
9�
18(1
0.5
�1)
;K
now
ndi
abet
es�
230.
4�
18(1
2.8
�1)
.
Rev
iew
ofBG
leve
lsof
pati
ents
onge
nera
lmed
icin
ean
dsu
rger
yw
ards
.Hyp
ergl
ycem
iade
fined
astw
oor
mor
em
easu
rem
ents
wit
hfa
stin
gBG
�12
6(7
)an
d/or
rand
om�
200
(11.
1).H
ospi
talm
orta
lity
for
norm
ogly
cem
icpa
tien
tsw
as1.
7%.W
ith
know
ndi
abet
esm
orta
lity
was
3%an
dw
ith
“new
”hy
perg
lyce
mia
itw
as16
%.A
fter
adju
stm
ent
for
vari
able
s,th
e“n
ew”
hype
rgly
cem
iagr
oup
had
an18
.3-f
old
incr
ease
dm
orta
lity
rate
com
pare
dw
ith
a2.
7-fo
ldin
crea
sew
ith
know
ndi
abet
es.P
atie
nts
wit
hne
why
perg
lyce
mia
also
had
anin
crea
sed
leng
thof
stay
,wer
em
ore
likel
yto
requ
ire
ICU
care
,and
wer
em
ore
likel
yto
requ
ire
tran
siti
onal
ornu
rsin
gho
me
care
(Obs
,n�
1,88
6)(1
).In
fect
ion
rate
sco
rrel
ated
wit
hBG
abov
e22
0.5.
9-fo
ldin
crea
sein
seri
ous
infe
ctio
ns,i
nclu
ding
seps
is,p
neum
onia
,and
wou
ndin
fect
ions
for
BGov
er22
0(1
2.2)
,w
hich
was
ase
nsit
ive
(85%
)pr
edic
tor
ofno
soco
mia
linf
ecti
on(O
bs,n
�97
)(1
91).
CV
Dan
dcr
itic
alca
reA
cute
MI
Mor
talit
y,C
HF,
and
card
ioge
nic
shoc
kri
skco
rrel
ated
wit
hBG
Abo
ve10
9.8
(6),
inpa
tien
tsw
itho
utkn
own
diab
etes
;A
tor
abov
e12
4(6
.9),
wit
hdi
abet
esdi
agno
sis.
Lite
ratu
rere
view
.Rel
ativ
eri
sk(R
R)
for
inho
spit
alm
orta
lity
incr
ease
d3.
9-fo
ldin
subj
ects
wit
hout
diab
etes
wit
hBG
ator
abov
era
nge
of10
9.8–
144
(6.1
–8),
95%
CI
2.9–
5.4;
risk
ofC
HF
and
card
ioge
nic
shoc
kw
asal
soin
crea
sed.
RR
for
mod
erat
ein
crea
sein
mor
talit
yw
ith
know
ndi
abet
esw
ith
was
1.7
(14
arti
cle
revi
eww
ith
met
a-an
alys
is)
(192
).
Adm
itBG
,str
atifi
edac
cord
ing
toW
HO
crit
eria
and
corr
elat
edw
ith
mor
talit
y:I.
BGle
ssth
an10
0.8
(5.6
)to
IV.B
Ggr
eate
rth
anor
equa
lto
199.
8(1
1)
One
-yea
rm
orta
lity
was
19.3
%fo
rBG
�10
0.8
(5.6
)at
tim
eof
adm
issi
on,c
ompa
red
wit
h44
%w
hen
BG�
199.
8(1
1).
Mor
talit
yw
ashi
gher
inpa
tien
tsw
ith
diab
etes
than
inth
ose
wit
hout
(40
vs.1
6%,P
�0.
05)
(Obs
,n�
336)
(193
).M
orta
lity
corr
elat
edw
ith
BGin
inte
nsiv
ein
sulin
ther
apy
grou
pw
here
mea
nBG
�17
2.8
�59
.4(9
.6�
3.3)
com
pare
dw
ith
conv
enti
onal
ther
apy
grou
pw
here
mea
nBG
�21
0.6
�73
.8(1
1.7
�4.
1).
Inte
nsiv
ein
sulin
ther
apy
inpa
tien
tsw
ith
acut
eM
I,fo
llow
edby
mul
tish
otre
gim
enfo
r3
orm
ore
mon
ths,
wit
h29
%re
duct
ion
inm
orta
lity
at1
year
.Ben
efit
exte
nds
toat
leas
t3.
4ye
ars.
One
life
save
dfo
rni
nepa
tien
tstr
eate
d(I
nt,
n�
620)
(128
).C
ardi
acsu
rger
yM
orta
lity
posi
tive
lyco
rrel
ated
wit
hBG
ina
dose
-dep
ende
ntm
anne
r,w
ith
the
low
est
mor
talit
yin
the
grou
pw
here
mea
npo
stop
erat
ive
BG�
150
(8.3
).O
bser
vati
onal
stud
ies
usin
ghi
stor
ical
cont
rols
.Bot
hm
orta
lity
and
inci
denc
eof
DSW
Isw
ere
redu
ced
toth
eno
ndia
beti
cra
nge
afte
rim
plem
enti
ngin
sulin
infu
sion
prot
ocol
sw
ith
prog
ress
ivel
ylo
wer
BGta
rget
sov
erti
me
(196
,197
).C
riti
calc
are
Mor
talit
yan
dse
psis
risk
corr
elat
edw
ith
BG.I
nten
sive
insu
linth
erap
yar
mw
ith
mea
nBG
103
�19
(5.7
�1.
06);
conv
enti
onal
trea
tmen
tar
mw
ith
mea
nBG
153
�33
(8.5
�1.
8).
Pros
pect
ive
rand
omiz
edco
ntro
lled
stud
yof
adul
tsad
mit
ted
tosu
rgic
alIC
Uan
don
mec
hani
calv
enti
lati
on.S
ixty
perc
ent
had
had
card
iac
surg
ery,
maj
orit
yof
othe
rsal
sosu
rgic
alpa
tien
ts.I
ITto
mai
ntai
nBG
in80
–110
(4.4
–6.1
)ra
nge
com
pare
dw
ith
conv
enti
onal
ther
apy
(CT
)to
targ
etBG
to18
0–20
0(1
0–11
.1).
IIT
redu
ced
ICU
mor
talit
yby
40%
from
8.0
to4.
6%,P
�0.
04.F
orea
ch20
mg/
dlin
crea
sein
BG,r
isk
ofde
ath
was
incr
ease
dby
30%
.IIT
also
redu
ced
inci
denc
eof
seps
isby
46%
and
over
allh
ospi
talm
orta
lity
by34
%.A
grad
uald
eclin
ein
risk
for
ICU
and
hosp
ital
deat
hw
ith
decl
ine
inBG
leve
lwas
obse
rved
,wit
hno
iden
tifia
ble
thre
shol
dbe
low
whi
chth
ere
was
nofu
rthe
rri
skre
duct
ion.
Prol
onge
din
flam
mat
ion,
defin
edas
elev
atio
nin
CR
Pab
ove
150
mg/
dlfo
rov
er3
days
,w
asas
soci
ated
wit
hm
ean
BGle
vel(
per
20m
g/dl
adde
d)w
ith
orof
1.16
(95%
CI
1.06
–1.2
4),P
�0.
0006
.Th
resh
old
may
behi
gher
than
110
(6.1
)(In
t,n
�1,
548)
(2,2
00).
Neu
rolo
gic
diso
rder
sA
cute
stro
keM
orta
lity
and
func
tion
alre
cove
ryaf
ter
acut
eis
chem
icst
roke
corr
elat
edw
ith
BG.
Adm
issi
onBG
over
110
(6.1
)fo
rm
orta
lity;
over
121
for
func
tion
alre
cove
ry.
Lite
ratu
rere
view
(196
6–20
00).
Aft
eris
chem
icst
roke
,adm
issi
ongl
ucos
ele
vel�
110–
126
(�6.
1–7)
asso
ciat
edw
ith
incr
ease
dri
skof
inho
spit
alor
30-d
aym
orta
lity
inpa
tien
tsw
itho
utdi
abet
eson
ly(R
R3.
8;95
%C
I2.
32–4
.64)
.St
roke
surv
ivor
sw
itho
utdi
abet
esan
dBG
over
121–
144
(6.7
–8)
had
RR
of1.
41(1
.16–
1.73
)fo
rpo
orfu
ncti
onal
reco
very
(met
aana
lysi
s,26
stud
ies)
(96)
.N
euro
logi
cfu
ncti
onaf
ter
acut
est
roke
corr
elat
edw
ith
adm
issi
onBG
.O
dds
for
neur
olog
icim
prov
emen
tde
crea
sed
wit
hO
Rof
0.76
for
each
100
mg/
dlBG
incr
ease
.
Con
trol
led,
rand
omiz
edtr
ialo
fmol
ecul
arhe
pari
nin
acut
est
roke
.Mea
nad
mis
sion
BG14
4�
68(8
�3.
8)as
soci
ated
wit
hne
urol
ogic
impr
ovem
ent
at3
mon
ths.
Inth
ose
wit
hout
impr
ovem
ent,
BGw
as16
0�
84(8
.9�
4.7)
.As
BGin
crea
sed,
odds
for
neur
olog
icim
prov
emen
tde
crea
sed,
wit
hO
R�
0.76
per
100-
mg/
dlin
crea
sein
adm
issi
onBG
(95%
CI
0.61
–0.9
5,P
�0.
01)
(Obs
,n�
1,25
9)(2
01).
Func
tion
alou
tcom
esan
dre
turn
tow
ork
afte
rst
roke
corr
elat
edw
ith
adm
issi
onBG
.A
dmis
sion
BGun
der
120
(6.7
)w
ith
posi
tive
rela
tion
ship
.
Pros
pect
ive
data
.Str
oke-
rela
ted
defic
its
wer
em
ore
seve
rew
hen
adm
issi
ongl
ucos
eva
lues
wer
e�
120
(6.7
).O
nly
43%
ofpa
tien
tsw
ith
anad
mis
sion
gluc
ose
valu
eof
�12
0m
g/dl
able
tore
turn
tow
ork,
whe
reas
76%
ofpa
tien
tsw
ith
low
ergl
ucos
eva
lues
rega
ined
empl
oym
ent
(202
).
RtP
A-i
nduc
edhe
mor
rhag
ein
toan
infa
rct
corr
elat
edw
ith
BGov
er30
0(1
6.7)
.C
entr
alco
llect
ion
ofre
tros
pect
ive
and
pros
pect
ive
data
onac
ute
isch
emic
stro
ketr
eate
din
clin
ical
prac
tice
sw
ith
alte
plas
e.BG
�30
0m
g/dl
anin
depe
nden
tri
skfa
ctor
for
hem
orrh
age
into
anin
farc
tw
hen
trea
tmen
tw
ith
reco
mbi
nant
RtP
Ais
give
n(O
bs,n
�1,
205)
(203
).M
orta
lity,
leng
thof
stay
,and
char
ges
incr
ease
dw
ith
adm
issi
onBG
�13
0(7
.2).
Hos
pita
lizat
ion
for
acut
eis
chem
icst
roke
.Hyp
ergl
ycem
ia(r
ando
mBG
ator
abov
e13
0)pr
esen
tin
40%
atad
mis
sion
.M
ost
rem
aine
dhy
perg
lyce
mic
wit
hm
ean
BGva
lues
of20
6(1
1.4)
.Ran
dom
adm
issi
onse
rum
gluc
ose
�13
0(7
.2)
inde
pend
entl
yas
soci
ated
wit
hin
crea
sed
risk
ofde
ath
at30
days
(HR
1.87
)an
d1
year
(HR
1.75
),bo
thP
�0.
01.
Oth
ersi
gnifi
cant
corr
elat
esw
ith
hype
rgly
cem
ia,w
hen
com
pare
dw
ith
norm
alBG
,wer
ele
ngth
ofst
ay(7
vs.6
days
,P�
0.01
5)an
dch
arge
s($
5,26
2vs
.$6,
611,
P�
0.00
1)(O
bs,n
�65
6)(2
05).
Hyp
ogly
cem
iari
skan
d4
wee
km
orta
lity
wit
hBG
targ
eted
to72
–126
(4–7
).G
luco
se-i
nsul
inin
fusi
onin
acut
est
roke
wit
hm
ild-t
o-m
oder
ate
hype
rgly
cem
ia.E
xam
ined
the
safe
tyof
trea
ting
toa
targ
etgl
ucos
eof
72–1
26(4
–7).
Low
erin
gBG
was
foun
dto
bew
itho
utsi
gnifi
cant
risk
ofhy
pogl
ycem
iaor
4-w
eek
exce
ssm
orta
lity
inpa
tien
tsw
ith
acut
est
roke
and
mild
-to-
mod
erat
ehy
perg
lyce
mia
(147
).Pe
num
bral
salv
age,
final
infa
rct
size
,and
func
tion
alou
tcom
ein
pati
ents
wit
hm
edia
nac
ute
BGra
ngin
gfr
om10
4.4
to17
2.8
(5.8
–9.6
).St
udy
ofM
RI
and
MR
Sin
acut
est
roke
.Pro
spec
tive
eval
uati
onw
ith
seri
aldi
ffus
ion-
wei
ghte
dan
dpe
rfus
ion-
wei
ghte
dM
RI
and
acut
eBG
mea
sure
men
ts.M
edia
nac
ute
BGw
as13
3.2
mg/
dl(7
.4m
mol
/l),r
ange
104.
4–17
2.8
mg/
dl(5
.8–9
.6m
mol
/l).A
doub
ling
ofBG
from
5to
10m
mol
/lle
dto
a60
%re
duct
ion
inpe
num
bral
salv
age
and
a56
-cm
3in
crea
sein
final
infa
rct
size
.In
pati
ents
wit
hac
ute
perf
usio
n-di
ffus
ion
mis
mat
ch,a
cute
hype
rgly
cem
iaw
asal
soco
rrel
ated
wit
hre
duce
dsa
lvag
eof
mis
mat
chti
ssue
from
infa
rcti
on,g
reat
erfin
alin
farc
tsi
ze,a
ndw
orse
func
tion
alou
tcom
e,in
depe
nden
tof
base
line
stro
kese
veri
ty,l
esio
nsi
ze,a
nddi
abet
icst
atus
(Obs
,n�
63)
(110
).
BG,b
lood
gluc
ose;
CT
,con
vent
iona
lthe
rapy
;DM
,dia
bete
sm
ellit
us;H
R,h
azar
dra
tio;
Int,
inte
rven
tion
alst
udy;
Obs
,obs
erva
tion
alst
udy;
RtP
A,r
ecom
bina
ntti
ssue
plas
min
ogen
acti
vato
r;R
x,th
erap
y.
Clement and Associates
DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004 559

Umpierrez study (1) and most of the litera-ture from other disciplines, as outlined else-where in this review, would suggest a lowerthreshold for optimal hospital outcomes.Evidence for a blood glucose threshold.The Umpierrez study demonstrated bet-ter outcomes for patients with fasting andadmission blood glucose �126 mg/dl (7mmol/l) and all random blood glucoselevels �200 mg/dl (11.1 mmol/l). Be-cause the Pomposelli and Umpierrezstudies are observational, a causal link be-tween hyperglycemia and poor outcomescannot be established.
CVD and critical careNumerous articles contain data linkingblood glucose level to outcomes in AMIand cardiac surgery, for which patientsreceive care predominantly in the ICUsetting. The majority of these trials are ob-servational, but the literature also in-c ludes seve ra l l a rge , l andmarkinterventional studies that have markedlyincreased awareness of the need for tar-geted glycemic control in these settings.AMI. In 2000, Capes et al. (192) re-viewed blood glucose levels and mortalityin the setting of AMI from 15 previouslypublished studies and performed a meta-analysis of the results to compare the RRof in-hospital mortality and CHF in bothhyper- and normoglycemic patients withand without diabetes. In subjects withoutknown diabetes whose admission bloodglucose was �109.8 mg/dl (6.1 mmol/l),the RR for in-hospital mortality was in-creased significantly (RR 3.9, 95% CI2.9–5.4). When diabetes was present andadmission glucose was �180 mg/dl (10mmol/l), risk of death was moderately in-creased (1.7, 1.2–2.4) compared with pa-t i ents who had diabetes but nohyperglycemia on admission.
Bolk et al. (193) analyzed admissionblood glucose values in 336 prospective,consecutive patients with AMI with aver-age follow-up to 14.2 months. Twelvepercent of this cohort had previously di-agnosed diabetes. Multivariate analysisrevealed an independent association ofadmission blood glucose and mortality.The 1-year mortality rate was 19.3% insubjects with admission plasma glucose�100.8 mg/dl (5.6 mmol/l) and rose to44% with plasma glucose �199.8 mg/dl(11 mmol/l). Mortality was higher in pa-tients with known diabetes than in thosewithout diabetes (40 vs. 16%, P � 0.05.).
From the frequently cited Diabetes
and Insulin-Glucose Infusion in AcuteMyocardial Infarction (DIGAMI) study,Malmberg and colleagues (128,194) havepublished the results of a prospective in-terventional trial of insulin-glucose infu-sion followed by subcutaneous insulintreatment in diabetic patients with AMI,reporting mortality at 1 year. Of 620 per-sons with diabetes and AMI, 306 wererandomized to intensive treatment withinsulin infusion therapy, followed by amultishot insulin regimen for 3 or moremonths. Patients randomized to conven-tional therapy received standard diabetestherapy and did not receive insulin unlessclinically indicated. Baseline blood glu-cose values were similar in the intensivetreatment group, 277.2 � 73.8 mg/dl(15.4 � 4.1 mmol/l), and the conven-tional treatment group, 282.6 � 75.6mg/dl (15.7 � 4.2 mmol/l). Blood glucoselevels decreased in the first 24 h in theintervention group to 172.8 � 59.4 mg/dl(9.6 � 3.3 mmol/l; P � 0.001 vs. conven-tional treatment), whereas blood glucosedeclined to 210.6 � 73.8 mg/dl (11.7 �4.1mmol/l). The blood glucose range foreach group was wide: 116.4–232.2 mg/dl(6.5–12.9 mmol/l) in the intensive treat-ment group and 136.8 –284.4 mg/dl(7.6–15.8 mmol/l) in the conventionaltreatment group. Mortality at 1 year in theintensive treatment group was 18.6%,and for the conventional treatment groupit was 26.1%, a 29% reduction in mortal-ity for the intervention arm (P � 0.027).At 3.4 (1.6–5.6) years follow-up, mortal-ity was 33% in the intensive treatmentgroup and 44% in the conventional treat-ment group (RR 0.72, 95% CI 0.55–0.92;P � 0.011), consistent with persistent re-duction in mortality. The benefit of inten-sive control was most pronounced in 272patients who had not had prior insulintherapy and had a less risk for CVD (0.49,0.30–0.80; P � 0.004).
In the DIGAMI study, insulin infu-sion in AMI followed by intensive subcu-taneous insulin therapy for 3 or moremonths improved long-term survival,with a benefit that extends to at least 3.4years (128). An absolute reduction inmortality of 11% was observed, meaningthat one life was saved for every ninetreated patients. The observation thathigher mean glucose levels were associ-ated with increased mortality betweengroups of patients with diabetes wouldsuggest that stress hyperglycemia plays anindependent role in the determination of
outcomes. In addition, it is of interest thatin spite of the observation that blood glu-cose levels between the intensive and con-ventional treatment groups were similar,a significant difference in mortality be-tween these groups was found. A rela-tively modest reduction in blood glucosein the intensive treatment group com-pared with the conventional treatmentgroup produced a statistically significantimprovement in mortality. This suggeststhe possibility that the beneficial effect ofimproved control may be mediatedthrough mechanisms other than a directeffect of hyperglycemia, such as a directeffect of insulin.Evidence for a blood glucose thresholdfor increased mortality in AMI.● The metaanalysis of Capes et al. (192)
reported a blood glucose threshold of�109.8 mg/dl (6.1 mmol/l) for patientswithout diabetes and �180 mg/dl (10mmol/l) for known diabetes.
● The observational study of Bolk et al.(193) identified threshold blood glu-coses, divided by World Health Orga-nization (WHO) classification criteria,with mortality risk of 19.3% for normo-glycemia (blood glucose �100.8 mg/dl[5.6 mmol/l]), which rose progressivelyto 44% for blood glucose �199.8mg/dl (11 mmol/l).
● In the DIGAMI study, mean blood glu-cose in the intensive insulin interven-tion arm was 172.8 mg/dl (9.6 mmol/l),where lower mortality risk was ob-served. In the conventional treatmentarm, mean blood glucose was 210.6mg/dl (11.7 mmol/l). The broad rangeof blood glucose levels within each armlimits the ability to define specific bloodglucose target thresholds.
Cardiac surgery. Attainment of targetedglucose control in the setting of cardiacsurgery is associated with reduced mor-tality and risk of deep sternal wound in-fect ions. Furnary and col leagues(196,197) treated cardiac surgery pa-tients with diabetes with either subcuta-neous insulin (years 1987–1991) or withintravenous insulin (years 1992–2003) inthe perioperative period. From 1991–1998, the target glucose range was 150�200 mg/dl (8.3–11.1 mmol/l); in 1999it was dropped to 125–175 mg/dl (6.9–9.7 mmol/l), and in 2001 it was againlowered to 100 –150 mg/dl (5.5– 8.3mmol/l). Following implementation ofthe protocol in 1991, the authors re-
Management of diabetes and hyperglycemia in hospitals
560 DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004

ported a decrease in blood glucose levelfor the first 2 days after surgery and a con-comitant decrease in the proportion of pa-tients with deep wound infections, from2.4% (24 of 990) to 1.5% (5 of 595) (P �0.02) (198). A recent analysis or the co-hort found a positive correlation betweenthe average postoperative glucose leveland mortality, with the lowest mortalityin patients with average postoperativeblood glucose �150 mg/dl (8.3 mmol/l)(197).
Golden et al. (199) performed a non-concurrent prospective cohort chart re-view study in cardiac surgery patientswith diabetes (n � 411). Perioperativeglucose control was assessed by the meanof six capillary blood glucose measuresperformed during the first 36 h followingsurgery. The overall infectious complica-tion rate was 24.3%. After adjustment forvariables, patients with higher mean cap-illary glucose readings were at increasedrisk of developing infections. Comparedwith subjects in the lowest quartile forblood glucose, those in quartiles 2– 4were at progressively increased risk forinfection (RR 1.17, 1.86, and 1.78 forquartiles 2, 3, and 4, respectively, P �0.05 for trend). These data support theconcept that perioperative hyperglycemiais an independent predictor of infection inpatients with diabetes.Critical care. Van den Berghe et al. (200)performed a prospective, randomizedcontrolled study of 1,548 adults whowere admitted to a surgical intensive careunit and were receiving mechanical ven-tilation. Reasons for ICU admission werecardiac surgery (60%) and noncardiacindications, including neurologic disease(cerebral trauma or brain surgery), otherthoracic surgery, abdominal surgery orperitonitis, vascular surgery, multipletrauma, or burns and transplant (4–9%each group). Patients were randomized toreceive intensive insulin therapy (IIT) tomaintain target blood glucose in the 80–110 mg/dl (4.4–6.1) range or conven-tional therapy to maintain target bloodglucose between 180 and 200 mg/dl (10–11.1 mmol/l). Insulin infusion was initi-ated in the conventional treatment grouponly if blood glucose exceeded 215 mg/dl(11.9 mmol/l), and the infusion was ad-justed to maintain the blood glucose levelbetween 180 and 200 mg/dl (10.0 and11.1 mmol/l). After the patients left theICU they received standard care in thehospital with a target blood glucose of
180 and 200 mg/dl (10.0 and 11.1 mmol/l).
Ninety-nine percent of patients in theIIT group received insulin infusion, ascompared with 39% of the patients in theconventional treatment group. In the IITarm, blood glucose levels were 103 � 19mg/dl (5.7 � 1.1 mmol/l) and in conven-tional treatment 153 � 33 mg/dl (8.5 �1.8 mmol/l). IIT reduced mortality duringICU care from 8.0% with conventionaltreatment to 4.6% (P � 0.04). The benefitof IIT was attributable to its effect on mor-tality among patients who remained in theunit for more than 5 days (20.2% withconventional treatment vs. 10.6% withIIT, P � 0.005). IIT also reduced overallinhospital mortality by 34% (2). In a sub-sequent analysis, Van den Berghe (200)demonstrated that for each 20 mg/dl (1.1mmol/l), glucose was elevated �100mg/dl (5.5 mmol/l) and the risk of ICUdeath increased by 30% (P � 0.0001).Daily insulin dose (per 10 units added)was found as a positive rather than nega-tive risk factor, suggesting that it was notthe amount of insulin that produced theobserved reduction in mortality. Hospitaland ICU survival were linearly associatedwith ICU glucose levels, with the highestsurvival rates occurring in patientsachieving an average blood glucose �110mg/dl (6.1 mmol). An improvement inoutcomes was found in patients who hadprior diabetes as well as in those who hadno history of diabetes.Evidence for a blood glucose thresholdin cardiac surgery and critical care.● Furnary et al. (196) and Zerr et al. (198)
identified a reduction in mortalitythroughout the blood glucose spectrumwith the lowest mortality in patientswith blood glucose �150 mg/dl (8.3mmol/l).
● Van den Berghe et al. (2), using inten-sive intravenous insulin therapy, re-ported a 45% reduction in ICUmortality with a mean blood glucose of103 mg/dl (5.7 mmol/l), as comparedwith the conventional treatment arm,where mean blood glucose was 153mg/dl (8.5 mmol/l) in a mixed group ofpatients with and without diabetes.
Acute neurologic illness and stroke. Inthe setting of acute neurologic illness,stroke, and head injury, data support aweak association between hyperglycemiaand increased mortality and are scanty forpatients with known diabetes. In these
clinical settings, available data, with oneexception, are observational. Capes et al.(96) reported on mortality after stroke inrelation to admission glucose level from26 studies, published between 1996 and2000, where RRs for prespecified out-comes were reported or could be calcu-lated. After ischemic stroke, admissionglucose level �110–126 mg/dl (�6.1–7mmol/l) was associated with increasedrisk of inhospital or 30-day mortality inpatients without diabetes only (RR 3.8,95% CI 2.32– 4.64). Stroke survivorswithout diabetes and blood glucose�121–144 mg/dl (6.7–8 mmol/l) had anRR of 1.41 (1.16–1.73) for poor func-tional recovery. After hemorrhagic stroke,admission hyperglycemia was not associ-ated with higher mortality in either thediabetes or nondiabetes groups.
Several of the studies that were in-cluded in the analysis of Capes et al. (96)contain additional data that support anassociation between blood glucose andoutcomes in stroke. In the Acute StrokeTreatment Trial (TOAST), a controlled,randomized study of the efficacy of a low–molecular weight heparinoid in acuteischemic stroke (n � 1,259), neurologicimprovement at 3 months (a decrease byfour or more points on the National Insti-tutes of Health [NIH] Stroke Scale or afinal score of 0) was seen in 63% of sub-jects. Those with improvement had amean admission glucose of 144 � 68 mg/dl, and those without improvement hadblood glucose of 160 � 84 mg/dl. In mul-tivariate analysis, as admission blood glu-cose increased, the odds for neurologicimprovement decreased with an OR of0.76 per 100 mg/dl increase in admissionglucose (95% CI 0.61–0.95, P � 0.01)(201). Subgroup analysis for patientswith or without a history of diabetes wasnot done. Pulsinelli et al. (202) reportedworse outcomes for both patients with di-abetes and hyperglycemic patients with-out an established diagnosis of diabetescompared with those who were normo-glycemic. Stroke-related deficits weremore severe when admission glucose val-ues were �120 mg/dl (6.7 mmol/l). Only43% of the patients with an admissionglucose value of �120 mg/dl were able toreturn to work, whereas 76% of patientswith lower glucose values regainedemployment.
Demchuk et al. (203) studied the ef-fect of admission glucose level and risk forintracerebral hemorrhage into an infarct
Clement and Associates
DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004 561

when treatment with recombinant tissueplasminogen activator was given to 138patients presenting with stroke. Twenty-three percent of the cohort had knowndiabetes. The authors reported admissionblood glucose and/or history of diabetesas the only independent predictors ofhemorrhage. Kiers et al. (204) prospec-tively studied 176 sequential acute strokepatients and grouped them by admissionblood glucose level, HbA1c level, and his-tory of diabetes. Threshold blood glucosefor euglycemia was defined as fastingblood glucose �140 mg/dl (7.8 mmol/l).The authors divided patients into one offour groups: euglycemia with no historyof diabetes, patients with “stress hyper-glycemia” (blood glucose �140 mg/dl,7.8 mmol/l, and HbA1c �8%), newly di-agnosed diabetes (blood glucose �140mg/dl, 7.8 mmol/l, and HbA1c �8%), andknown diabetes. No difference was foundin the type or site of stroke among the fourgroups. Compared with the euglycemic,nondiabetic patients, mortality was in-creased in all three groups of hyperglyce-mic patients.
Williams et al. (205) reported on theassociation of hyperglycemia and out-comes in a group of 656 acute stroke pa-tients. Fifty-two percent of the cohort hada known history of diabetes. Hyperglyce-mia, defined as a random blood glucose�130 mg/dl (7.22 mmol/l), was presentin 40% of patients at the time of admis-sion. Hyperglycemia was an independentpredictor of death at 30 days (RR 1.87)and at 1 year (RR 1.75) (both P � 0.01).Other outcomes that were significantlycorrelated with hyperglycemia, whencompared with normal blood glucose,were length of stay (7 vs. 6 days, P �0.015) and charges ($6,611 vs. $5,262,P � 0.001).
Recently, Parsons et al. (110) re-ported a study of magnetic resonance im-aging (MRI) and MRS in acute stroke.Sixty-three acute stroke patients wereprospectively evaluated with serial diffu-sion-weighted and perfusion-weightedMRI and acute blood glucose measure-ments. Median acute blood glucose was133.2 mg/dl (7.4 mmol/l), range 104.4–172.8 mg/dl (5.8–9.6 mmol/l). A dou-bling of blood glucose from 90 to 180mg/dl (5�10 mmol/l) led to a 60% reduc-tion in penumbral salvage and a 56 cm3
increase in final infarct size. For patientswith acute perfusion-diffusion mismatch,acute hyperglycemia was correlated with
reduced salvage of mismatch tissue frominfarction, greater final infarct size, andworse functional outcome, independentof baseline stroke severity, lesion size, anddiabetes status. Furthermore, higheracute blood glucose in patients with per-fusion-diffusion mismatch was associatedwith greater acute-subacute lactate pro-duction, which, in turn, was indepen-dently associated with reduced salvage ofmismatch tissue. Acute hyperglycemia in-creases brain lactate production and facil-itates conversion of hypoperfused at-risktissue into infarction, which may ad-versely affect stroke outcome.
These numerous observational stud-ies further support the need for random-ized controlled trials that aggressivelytarget glucose control in acute stroke. Todate, there is just one report of a treat-to-target intervention in stroke patients. TheGlucose Insulin in Stroke Trial (GIST) ex-amined the safety of GIK infusion in treat-ing to a target glucose of 72–126 mg/dl(4–7 mmol/l). Lowering plasma glucoselevels was found to be without significantrisk of hypoglycemia or excess mortalityin patients with acute stroke and mild-to-moderate hyperglycemia (206). No dataon functional recovery were reported.While it is promising that these investiga-tors were able to lower plasma glucosewithout increasing risk of hypoglycemiaor mortality for stroke patients, until fur-ther studies test the effectiveness of thisapproach and possible impact on out-comes, it cannot be considered standardpractice.
Hyperglycemia is associated withworsened outcomes in patients with acutestroke and head injury, as evidenced bythe large number of observational studiesin the literature. It seems likely that thehyperglycemia associated with theseacute neurologic conditions results fromthe effects of stress and release of insulincounterregulatory hormones. The ele-vated blood glucose may well be a markerof the level of stress the patient is experi-encing. The hyperglycemia can bemarked in these patients. Studies areneeded to assess the role of antihypergly-cemic pharmacotherapy in these settingsfor possible impact on outcomes. Clinicaltrials to investigate the impact of targetedglycemic control on outcomes in patientswith stress hyperglycemia and/or knowndiabetes and acute neurologic illness areneeded.
Evidence for a blood glucose thresholdin acute neurologic disorders. Obser-vational studies suggest a correlation be-tween blood glucose level, mortality,morbidity, and health outcomes in pa-tients with stroke.
● Capes et al.’s (96) metaanalysis identi-fied an admission blood glucose �110mg/dl (6.1 mmol/l) for increased mor-tality for acute stroke.
● Studies by Pulsinelli, Jorgenson, andWeir et al. (202) identified an admis-sion blood glucose �120 mg/dl (6.67mmol/l), 108 mg/dl (6 mmol/l), and144 mg/dl (8 mmol/l), respectively, forincreased severity ad mortality for acutestroke.
● Williams et al. (205) reported a thresh-old admission blood glucose �130mg/dl (7.2 mmol/l) for increased mor-tality, length of stay, and charges inacute stroke.
● Scott et al. (206) demonstrated accept-able hypoglycemia risk and no excess4-week mortality with glucose-insulininfusion treatment targeted to bloodglucose range of 72–126 mg/dl (4–7mmol/l) in acute stroke.
● Parsons et al. (110) reported that a dou-bling of blood glucose from 90 to 180mg/dl (5–10 mmol/l) was associatedwith 60% worsening of penumbral sal-vage and a 56-cm3 increase in infarctsize.
HOW ARE TARGET BLOODGLUCOSE LEVELS BESTACHIEVED IN THEHOSPITAL?
Role of oral diabetes agentsNo large studies have investigated the po-tential roles of various oral agents on out-comes in hospitalized patients withdiabetes. A number of observational stud-ies have commented on the outcomes ofpatients treated as outpatients with dietalone, oral agents, or insulin. However,the results are variable and the methodscannot account for patient characteristicsthat would influence clinician selection ofthe various therapies in the hospital set-ting. Of the three primary categories oforal agents, secretagogues (sulfonylureasand meglitinides), biguanides, and thia-zolidinediones, none have been systemat-ically studied for inpatient use. However,all three groups have characteristics thatcould impact acute care.
Management of diabetes and hyperglycemia in hospitals
562 DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004

SulfonylureasConcern about inpatient use of sulfonyl-ureas centers on vascular effects(207,208). Over 30 years ago the report ofthe University Group Diabetes Programproposed increased cardiovascular eventsin patients treated with sulfonylureas(209). This report resulted in an ongoinglabeling caution for sulfonylureas andheart disease, although the findings havebeen questioned and have had very lim-ited influence on prescribing habits. Re-sidual fears seemingly were allayed withthe findings of the U.K. Prospective Dia-betes Study (UKPDS) (210). This largeprospective trial did not find any evidenceof increased frequency of MI among indi-viduals treated with sulfonylureas.Rather, the trend was in the direction ofreduced events. However, questions re-main. For instance, it is possible that con-trol of hyperglycemia by any meansreduces the frequency of vascular eventsto a greater extent than any effect sulfo-nylureas may have to increase vascularevents. A variety of studies have served tofuel continued controversy.
Ischemic preconditioning appears tobe an adaptive, protective mechanismserving to reduce ischemic injury in hu-mans (211,212). Sulfonylureas inhibitATP-sensitive potassium channels, result-ing in cell membrane depolarization, ele-vation of intracellular calcium, andcellular response (213,214). This mecha-nism may inhibit ischemic precondition-ing (215–217). Various methodsevaluating cardiac ischemic precondi-tioning have been used to compare cer-tain of the available sulfonylureas. Forexample, using isolated rabbit hearts, re-searchers found that glyburide but notglimepiride reversed the beneficial effectsof ischemic preconditioning and diazox-ide in reducing infarct size (218). Otherstudies using similar animal heart modelsor cell cultures have found differencesamong the sulfonylureas, usually show-ing glyburide to be potentially moreharmful than other agents studied (219–222). A unique, double-blind, placebo-controlled study using acute balloonocclusion of high-grade coronary steno-ses in humans looked at the relative ef-fects of intravenously administeredplacebo, glimepiride, or glyburide (223).The researchers measured mean ST seg-ment shifts and time to angina. The re-sults again demonstrated suppression ofthe myocardial preconditioning by gly-
buride but not by glimepiride. In per-fused animal heart models, bothglimepiride and glyburide also appear toreduce baseline coronary blood flow athigh doses (220,224).
Cardiac effects of sulfonylureas havealso been compared with other classes oforal diabetes medications. In individualswith type 2 diabetes, investigators foundthat glyburide increased QT dispersion(225). This effect, proposed to reflect riskfor arrhythmias, was measured after 2months of therapy with glyburide or met-formin. Glyburide also increased QTc,while metformin produced no negativeeffects. This study is in contradiction tothe conclusions of a study using isolatedrabbit hearts, where glyburide exerted anantiarrhythmic effect despite repeat evi-dence that it interfered with postischemichyperemia (226). There have been fewother comparisons of sulfonylureas andmetformin with regard to direct cardiaceffects. In a study of rat ventricular myo-cytes, hyperglycemia induced abnormali-ties of myocyte relaxation. Theseabnormalities were improved when myo-cytes were incubated with metformin, butglyburide had no beneficial effect (227).Finally, one experiment recently evalu-ated the relative functional cardiac effectsof glyburide versus insulin (228). In thisstudy of patients with type 2 diabetes, leftventricular function was measured byechocardiography after 12-week treat-ment periods with each agent, attainingsimilar metabolic control. Neither treat-ment influenced resting cardiac function.However, after receiving dipyridamole,glyburide-treated patients experienceddecreased left ventricular ejection fractionand increased wall motion score index.Insulin treatment did not produce thesedeleterious effects on contractility.
Although these various findings usingdifferent research models raise questionsabout potential adverse cardiovascular ef-fects of sulfonylureas in general and gly-buride in particular, they do notnecessarily extrapolate to clinical rele-vancy. A series of observational studieshave attempted to add to our knowledgeabout whether any of the negative effectsof sulfonylureas impact on vascularevents, but they have yielded mixed re-sults. For example, outcomes of directballoon angioplasty after AMI were eval-uated comparing 67 patients taking sulfo-nylureas with 118 patients on otherdiabetes therapies (229). Logistic regres-
sion found sulfonylurea use to be inde-pendently associated with increasedhospital mortality. Others have reportedsimilar trends in patients receiving angio-plasty (230). A third observational studyinvestigated 636 elderly patients with di-abetes (mean age 80 years) and previousMI. The researchers looked for subse-quent coronary events, including fataland nonfatal MI or sudden coronarydeath (231). They found sulfonylureatherapy to be a predictor of new coronaryevents compared with insulin or to diettherapy (82 vs. 69 and 70%, respectively).Not enough metformin-treated patientswere included to comment statistically ona comparison with sulfonylureas.
Conversely, other observational stud-ies have failed to support a relationshipbetween sulfonylurea use and vascularevents. Klaman et al. (232) found no dif-ferences in mortality or creatinine kinase(CK) elevations after acute MI in 245 pa-tients with type 2 diabetes when compar-ing those treated with insulin, thosetreated with oral agents, or those newlydiagnosed. Others have reported a similarlack of association with MI outcomes andsulfonylureas (233–236). In one study,ventricular fibrillation was found to beless associated with sulfonylurea therapythan with gliclazide or insulin (234). Fi-nally, in a related vascular consideration,there was no evidence of increased strokemortality or severity in patients with type2 diabetes treated with sulfonylureas ver-sus other therapies (237).
None of the studies looking at sulfo-nylurea effects on vascular inpatient mor-tality have been prospective. Investigatorshave not made attempts to separate outduration of therapy or whether sulfonyl-ureas were continued after presentationto the hospital. The one prospective studylooking at treatment after admission forAMI indicated a benefit for insulin ther-apy over conventional therapy with sulfo-nylureas, but the improved outcomeswere proposed to occur as a benefit ofimproved glucose control (238). No sug-gestion was made that sulfonylurea ther-apy had specific negative effects.
Despite a spectrum of data raisingconcern about potential adverse effects ofsulfonylureas in the inpatient setting,where cardiac or cerebral ischemia is afrequent problem in an at-risk popula-tion, there are insufficient data to specifi-cally recommend against the use ofsulfonylureas in this setting. However,
Clement and Associates
DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004 563

sulfonylureas have other limitations in theinpatient setting. Their long action andpredisposition to hypoglycemia in pa-tients not consuming their normal nutri-tion serve as relative contraindications toroutine use in the hospital for many pa-tients (239). Sulfonylureas do not gener-ally allow rapid dose adjustment to meetthe changing inpatient needs. Sulfonyl-ureas also vary in duration of action be-tween individuals and likely vary in thefrequency with which they induce hypo-glycemia (240).
MetforminMetformin represents a second agent thatindividuals are likely to be using as anoutpatient, with potential for continua-tion as an inpatient. There is a suggestionfrom the UKPDS that metformin mayhave cardioprotective effects, althoughthe study was not powered to allow for acomparison with sulfonylureas (241).
The major limitation to metforminuse in the hospital is a number of specificcontraindications to its use, many ofwhich occur in the hospital. All of thesecontraindications relate to a potentiallyfatal complication of metformin therapy,lactic acidosis. The most common riskfactors for lactic acidosis in metformin-treated patients are cardiac disease, in-cluding CHF, hypoperfusion, renalinsufficiency, old age, and chronic pul-monary disease (242). In an outpatientsetting, using slightly variable criteria,22–54% of patients treated with met-formin have absolute or relative contrain-dications to its use (242–245). One recentreport noted that 27% of patients on met-formin in the hospital had at least onecontraindication to its use (246). In 41%of these cases, metformin was continueddespite the contraindication. This studyseemingly underestimates the usual fre-quency of contraindications since it iden-tified no individuals with CHF, a riskfactor that has been frequently noted inmany of the outpatient studies. Not sur-prisingly, a recent review of hospitalMedicare data found that 11.2% of pa-tients with concomitant diagnoses of dia-betes and CHF were discharged with aprescription of metformin (247).
Recent evidence continues to indicatelactic acidosis is a rare complication, de-spite the relative frequency of risk factors(248). However, in the hospital,where therisk for hypoxia, hypoperfusion, and re-nal insufficiency is much higher, it still
seems prudent to avoid the use of met-formin in most patients. In addition to therisk of lactic acidosis, metformin hasadded side effects of nausea, diarrhea, anddecreased appetite, all of which may beproblematic during acute illness in thehospital.
ThiazolidinedionesAlthough thiazolidinediones have veryfew acute adverse effects (249,250), theydo increase intravascular volume, a par-ticular problem in those predisposed toCHF and potentially a problem for pa-tients with hemodynamic changes relatedto admission diagnoses (e.g., acute coro-nary ischemia) or interventions commonin hospitalized patients. The same studyof Medicare patient hospital data citedabove (247) found that 16.1% of patientswith diabetes and CHF received a pre-scription for a thiazolidinedione at thetime of discharge. Twenty-four percent ofpatients with these combined diagnosesreceived either metformin or a thiazo-lidinedione, both drugs carrying contra-indications in this setting.
Most recently it has been demon-strated that when exposed to high con-centrations of rosiglitazone, a monolayerof pulmonary artery endothelial cells willexhibit significantly increased permeabil-ity to albumin (251). Although this is apreliminary in vitro study, it raises thepossibility of thiazolidinediones causing adirect effect on capillary permeability.This process may be of greater signifi-cance in the inpatient setting. On the pos-itive side, thiazoladinediones may havebenefits in preventing restenosis of coro-nary arteries after placement of coronarystents in patients with type 2 diabetes(252). For inpatient glucose control,however, thiazolidinediones are not suit-able for initiation in the hospital becausethe onset of effect, which is mediatedthrough nuclear transcription, is quiteslow.
In summary, each of the major classesof oral agents has significant limitationsfor inpatient use. Additionally, they pro-vide little flexibility or opportunity for ti-tration in a setting where acute changesdemand these characteristics. Therefore,insulin, when used properly, may havemany advantages in the hospital setting.
Use of insulinAs in the outpatient setting, in the hospi-tal a thorough understanding of normal
insulin physiology and the pharmacoki-netics of exogenous insulin is essential forproviding effective insulin therapy. Theinpatient insulin regimen must bematched or tailored to the specific clinicalcircumstance of the individual patient.Components of the insulin dose re-quirement defined physiologically. Inthe outpatient setting, it is convenient tothink of the insulin dose requirement inphysiologic terms as consisting of “basal”and “prandial” needs. In the hospital, nu-tritional intake is not necessarily providedas discrete meals. The insulin dose re-quirement may be thought of as consist-ing of “basal” and “nutritional” needs. Theterm “nutritional insulin requirement” re-fers to the amount of insulin necessary tocover intravenous dextrose, TPN, enteralfeedings, nutritional supplements admin-istered, or discrete meals. When patientseat discrete meals without receiving othernutritional supplementation, the nutri-tional insulin requirement is the same asthe “prandial” requirement. The term“basal insulin requirement” is used to re-fer to the amount of exogenous insulinper unit of time necessary to prevent un-checked gluconeogenesis and ketogenesis.
An additional variable that deter-mines total insulin needs in the hospital isan increase in insulin requirement thatgenerally accompanies acute illness. Insu-lin resistance occurs due to counterregu-latory hormone responses to stress (e.g.,surgery) and/or illness and the use of cor-ticosteroids, pressors, or other diabeto-genic drugs. The net effect of these factorsis an increase in insulin requirement,compared with a nonsick population.This proportion of insulin requirementspecific to illness is referred to as “illness”or “stress-related” insulin and varies be-tween individuals (Fig. 2).Is the patient insulin deficient or non–insulin deficient? As in the outpatientsetting, a key component to providing ef-fective insulin therapy in the hospital set-ting is determining whether a patient hasthe ability to produce endogenous insu-lin. Patients who have a known history oftype 1 diabetes are by definition insulindeficient (3). In addition, other clinicalfeatures may be helpful in determiningthe level of insulin deficiency (Table 2).Patients determined to be insulin defi-cient require basal insulin replacement toprevent iatrogenic diabetic ketoacidosis,i.e., they must be treated with insulin atall times.
Management of diabetes and hyperglycemia in hospitals
564 DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004

Subcutaneous insulin therapy. Subcu-taneous insulin therapy may be used toattain glucose control in most hospital-ized patients with diabetes. The compo-nents o f the da i ly insu l in doserequirement can be met by a variety ofinsulins, depending on the particular hos-pital situation. Subcutaneous insulintherapy is subdivided into programmedor scheduled insulin and supplemental orcorrection insulin (Table 3).Scheduled insulin therapy. This reviewwill use the term “programmed” or“scheduled insulin requirement” to referto the dose requirement in the hospitalnecessary to cover the both basal and nu-tritional needs. For patients who are eat-ing discrete meals, it is appropriate toconsider the basal and prandial compo-nents of the insulin requirement separately.Basal insulin therapy for patients whoare eating. Subcutaneous basal insulincan be provided by any one of severalstrategies. These include continuous sub-cutaneous insulin infusion (CSII) or sub-cutaneous injection of intermediate-acting insulin (including premixed insu-
lin) or of long-acting insulin analogs.Some of these methods result in peaks ofinsulin action that may exceed the basalneeds of the patient, causing hypoglyce-mia. This is most likely to occur as theacute illness begins to resolve and basalinsulin requirements that were elevateddue to stress and/or illness begin to returnto normal levels. Although selected inpart for basal coverage, NPH, lente, and tosome extent ultralente insulin also deliverpeaks of insulin that potentially can coverprandial needs, albeit with variable capa-bility for matching the timing of nutri-tional intake. When NPH insulin is usedin very low doses, it can also be adminis-tered four times daily as an alternate wayto provide basal insulin action (253).Prandial insulin therapy for patientswho are eating. Prandial insulin re-placement has its main effect on periph-eral glucose disposal into muscle. Alsoreferred to as “bolus” or “mealtime” insu-lin, prandial insulin is usually adminis-tered before eating. There are occasionalsituations when this insulin may be in-jected immediately after eating, such aswhen it is unclear how much food will beeaten. In such situations, the quantity ofcarbohydrates taken can be counted andan appropriate amount of rapid-actinganalog can be injected. The technique of“carbohydrate counting” may be usefulfor patients practicing insulin self-management. The rapid-acting insulinanalogs, insulin lispro and aspart, are ex-cellent prandial insulins. Regular insulinis more accurately considered to haveboth basal and prandial components dueto its longer duration of action. Similarly,NPH and lente insulins, with their dis-
tinct peaks and prolonged action, can beused for both their basal and prandial in-sulin effects. For hospitalized patientswith severe insulin deficiency, this canbe a disadvantage since the timing ofmeals and the quantity of food is ofteninconsistent.Basal insulin therapy for patients whoare not eating. While not eating, pa-tients who are not insulin deficient maynot require basal insulin. Since reductionof caloric intake may alter insulin resis-tance substantially in type 2 diabetes,sometimes allowing previously insulin-requiring patients to be controlled withendogenous insulin production alone, thebasal requirement is not easily deter-mined. However, withholding basal insu-lin in insulin-deficient patients results in arapid rise in blood glucose by 45 mg/dl(2.5 mmol/l) per hour until ketoacidosisoccurs (rev. in 254). This situation canoccur when “sliding scale” insulin therapyis the sole method of insulin coverage(255). Scheduled basal insulin therapy forpatients who are not eating can be pro-vided by a number of insulin types andmethods.Insulin for patients with intermittentnutritional intake. Hospitalized pa-tients may receive nutrition intermit-tently, as with patients who are beingtransitioned between NPO status and reg-ular diet, patients with anorexia or nau-sea, or patients receiving overnightcycling of enteral feedings. Appropriateinsulins used in combination therapymight include regular, intermediate, andlong-acting insulins or analogs, adminis-tered to cover basal needs and also timedto match the intermittent nutritional intake.Illness-related or stress dose insulintherapy. The illness-related insulin canbe apportioned between the basal insulin,the nutritional or prandial insulin, andthe correction doses. It is important topoint out that illness-related insulin re-quirements decrease as the patient’s con-dition improves and, thus, in manysituations may be difficult to precisely re-place (Fig. 2). In attempting to meet theillness-related insulin requirement, andto later return to lower doses, it is impor-tant to recall that intravenous insulin in-fusion gives the greatest flexibility andthat long-acting analog gives the least,with other preparations or routes beingintermediate. Rapid changes in illness-related insulin requirements necessitateclose blood glucose monitoring and daily
Figure 2—Insulin requirementsin health and illness. Componentsof insulin requirement are dividedinto basal, prandial or nutritional,and correction insulin. When writ-ing insulin orders, the basal andprandial/nutritional insulin dosesare written as programmed(scheduled) insulin, and correc-tion-dose insulin is written as analgorithm to supplement thescheduled insulin (see online ap-pendix 2). Programmed and cor-rection insulin are increased tomeet the higher daily basal andprandial or nutritional require-ments. Total insulin requirementsmay vary widely.
Table 2—Clinical characteristics of the pa-tient with insulin deficiency
● Known type 1 diabetes● History of pancreatectomy or pancreatic
dysfunction● History of wide fluctuations in blood
glucose levels● History diabetic ketoacidosis● History of insulin use for �5 years and/or
a history of diabetes for �10 years
Adapted from the Expert Committee on the Diagno-sis and Classification of Diabetes Mellitus (3) andconsensus from the authors.
Clement and Associates
DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004 565

Tab
le3—
Prac
tica
lgui
deli
nes
for
hosp
ital
use
ofin
suli
n
Clin
ical
sett
ing
Prog
ram
med
/sch
edul
edin
sulin
opti
on(s
)Su
pple
men
tal/c
orre
ctio
n-in
sulin
opti
on(s
)C
omm
ents
Basa
lPr
andi
alan
d/or
nutr
itio
nal
●T
otal
daily
insu
linre
quir
emen
tm
aybe
calc
ulat
edba
sed
onpr
ior
insu
lindo
ses
oras
0.6
unit
s�
kg�
1�
day�
1
●Ba
sali
nsul
inge
nera
llyac
coun
tsfo
r40
–50%
ofda
ilyin
sulin
requ
irem
ent
●Pr
andi
alan
d/or
nutr
itio
nalo
rsu
pple
men
tal/c
orre
ctio
ndo
ses
may
beca
lcul
ated
as10
–20
%of
tota
ldai
lyin
sulin
requ
irem
ent
for
each
dose
●Pa
tien
tsw
ith
type
1di
abet
esal
way
sre
quir
eco
ntin
uous
insu
linco
vera
geto
avoi
dke
tosi
sE
atin
gm
eals
●In
t-I
bid
orhs
●R
eg-I
orra
pid-
Iac
�B&
Dor
B,L,
and
D●
Reg
-Ior
rapi
d-I
ac
/�hs
●G
ive
Reg
-I,3
0–45
min
ac;r
apid
-I,0
–15
min
ac●
LA-I
hsor
am●
Gla
rgin
egi
ven
ason
ce-d
aily
dose
,usu
ally
aths
●In
sulin
drip
●A
void
/min
imiz
eR
eg-I
and
rapi
d-I
dose
sat
hsto
decr
ease
risk
ofno
ctur
nal
hypo
glyc
emia
●70
/30
or75
/25
insu
linm
aybe
used
acbr
eakf
ast
and
dinn
erto
mee
tbo
thba
sala
ndpr
andi
alne
eds
●In
sulin
drip
isR
xof
choi
cein
seve
rely
deco
mpe
nsat
edty
pe1,
wit
hor
wit
hout
DK
A,
and
inty
pe2
wit
hH
HS
Not
eati
ng●
Insu
lindr
ipN
/A●
Reg
-Iq
4–6
hour
s●
Int-
Ibi
dor
hs●
Rap
id-I
q4
hour
s●
LA-I
hsor
amPe
riop
erat
ive
orpe
ripr
oced
ural
Will
eat
post
-op
orpo
stpr
oced
ure
(e.g
.,ca
tara
ctex
trac
tion
,car
diac
cath
eter
izat
ion,
endo
scop
y)
Base
onpr
ior
insu
linR
x:●
Int-
Igi
ve1/
2-2/
3us
uala
mdo
se●
LA-I
glar
gine
,con
tinu
eus
ual
dose
pmpr
ior
Whe
nre
sum
esea
ting
●R
esta
rtpr
ior
dose
sof
Reg
-Ior
rapi
d-I
ac
Unt
ilre
sum
esea
ting
:●
Reg
-Iq
4–6
h●
Rap
id-I
q4
h
●U
sual
insu
linan
d/or
oral
agen
tdo
ses
give
nth
eni
ght
prio
rto
surg
ery
toas
sure
adeq
uate
glyc
emic
cont
rolo
nth
em
orni
ngof
the
proc
edur
e●
Pati
ents
wit
hdi
abet
essh
ould
beon
the
OR
list
for
the
earl
ym
orni
ngto
min
imiz
eam
ount
ofti
me
that
they
will
beke
ptN
PO.T
his
decr
ease
sri
skof
hypo
glyc
emia
and
allo
ws
mai
nten
ance
ofop
tim
umm
etab
olic
hom
eost
asis
Will
not
eat
(e.g
.,m
ajor
surg
ery)
●In
sulin
drip
●R
eg-I
q4–
6ho
urs
●ra
pid-
Iq
4ho
urs
●In
t-I,
give
1⁄2
usua
lam
dose
●LA
-Igl
argi
ne,g
ive
usua
ldai
lydo
se
N/A
Unt
ilre
sum
esea
ting
:●
Reg
-Iq
4–6
h●
Rap
id-I
q4
h
●W
here
apr
olon
ged
post
oper
ativ
enp
ope
riod
isan
tici
pate
d,e.
g.,c
ardi
otho
raci
c,m
ajor
abdo
min
al,C
NS
case
s,in
sulin
drip
Rx
isre
com
men
ded
●St
arti
ngdo
sefo
rpe
riop
erat
ive
mai
nten
ance
insu
lindr
ipis
0.2
unit
s�
kg�
1�
h�1
ICU
Ifnp
oan
d/or
clin
ical
lyun
stab
le:
●In
sulin
drip
●R
eg-I
q4–
6h
●R
apid
-Iq
4h
Ifea
ting
:●
Con
tinu
epr
ior
Int-
Ior
LA-I
Ifnp
o:●
N/A
Ifea
ting
:●
Reg
-Ior
RA
-Iac
and
hs
●R
eg-I
q4–
6h
●R
apid
-Iq
4h
●E
vide
nce-
base
dou
tcom
esst
udie
ssu
ppor
tus
eof
insu
lindr
ipas
Rx
ofch
oice
for
deco
mpe
nsat
eddi
abet
esin
the
ICU
sett
ing
incl
udin
gco
rona
ryca
re(a
cute
myo
card
iali
nfar
ctio
n)an
dsu
rgic
alin
tens
ive
care
unit
s(M
alm
berg
,Van
den
Berg
he,
Furn
ary)
Ent
eral
tube
feed
ing
Con
tinu
ous
24h:
●R
eg-I
q4–
6h
●R
eg-I
q4–
6ho
urs
●Ba
sali
nsul
indo
sege
nera
llyno
mor
eth
an40
%of
tota
ldai
lyin
sulin
requ
irem
ent
toav
oid
hypo
glyc
emia
ifen
tera
lfee
ding
inte
rrup
ted
●In
t-I
bid;
●R
apid
-Iq
4h
●R
apid
-Iq
4ho
urs
●N
utri
tion
alin
sulin
requ
irem
ents
met
wit
hpr
ogra
mm
eddo
ses
ofre
g-I
orra
pid-
I●
LA-I
hsor
am●
May
use
low
-dos
ein
t-I
aths
toco
ntro
lfas
ting
hype
rgly
cem
iaD
ayti
me
only
:●
Int-
Iam
Dur
ing
tube
feed
ing
deliv
ery
peri
odon
ly:
●If
tube
feed
ing
inte
rrup
ted,
e.g.
,for
proc
edur
eor
into
lera
nce,
incr
ease
freq
uenc
yof
finge
rsti
ckBG
chec
ks●
Reg
-Iq
4–6
h●
Rap
id-I
q4
hBo
lus
24h:
●In
t-I
bid;
●LA
-Ihs
oram
●R
eg-I
q4–
6h
●R
apid
-Iq
4h
●R
eg-I
q4–
6h
●R
apid
-Iq
4h
●G
ive
reg-
I,30
–45
min
s,or
rapi
d-I,
0–15
min
spr
ior
tobo
lus
toco
ntro
lpos
t-bo
lus
BGex
curs
ions
●C
heck
finge
rst
ick
BG2
haf
ter
reg-
Ior
1h
afte
rra
pid-
Ito
dete
rmin
edo
sead
just
men
tsfo
rpo
st-b
olus
targ
etBG
�18
0m
g/dl
●M
ayus
elo
w-d
ose
int-
Iat
hsto
cont
rolf
asti
nghy
perg
lyce
mia
Management of diabetes and hyperglycemia in hospitals
566 DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004

changes in the scheduled insulin doses, asthe blood glucose levels dictate.Correction-dose insulin therapy. Alsocalled “supplemental” insulin, this usu-ally refers to the insulin used to treat hy-perglycemia that occurs before meals orbetween meals. At bedtime, correction-dose insulin is often administered in a re-duced dose compared with other times ofthe day in order to avoid nocturnal hypo-glycemia. Correction-dose insulin mayalso refer to insulin used to correct hyper-glycemia in the NPO patient or in the pa-t ient who is receiving schedulednutritional and basal insulin but not eat-ing discrete meals. Correction-dose insu-lin should not be confused with “slidingscale insulin,” which usually refers to a setamount of insulin administered for hy-perglycemia without regard to the timingof the food, the presence or absence ofpreexisting insulin administration, oreven individualization of the patient’ssensitivity to insulin.
The traditional sliding scale insulinregimens, usually consisting of regular in-sulin without any intermediate or long-acting insulins, have been shown to beineffective at best and dangerous at worst(255–257). Problems cited with slidingscale insulin regimens are that the slidingscale regimen prescribed on admission islikely to be used throughout the hospitalstay without modification (255). Second,sliding scale insulin therapy treats hyper-glycemia after it has already occurred, in-stead of preventing the occurrence ofhyperglycemia. This “reactive” approachcan lead to rapid changes in blood glucoselevels, exacerbating both hyperglycemiaand hypoglycemia.
Correction-dose insulin therapy is animportant adjunct to scheduled insulin,both as a dose-finding strategy and as asupplement when rapid changes in insu-lin requirements lead to hyperglycemia. Ifcorrection doses are frequently required,it is recommended that the scheduled in-sulin doses be increased the following dayto accommodate the increased insulinneeds.Writing insulin orders. An example ofan insulin order form that prompts thephysician to address all three componentsof insulin therapy (i.e., basal, prandial,and correction dose) is provided (see on-line appendix 1 [available at http://care.diabetesjournals.org]). The formscan be incorporated into computerizedorder sets and other prompting methodsBo
lus
(con
t.)
Day
tim
eon
ly:
●In
t-I
amD
urin
gbo
lus
deliv
ery
peri
odon
ly:
●R
eg-I
q4–
6h
●R
apid
-Iq
4h
TPN
●R
eg-I
adde
dto
TPN
bags
●R
eg-I
q4–
6h
●Ba
sala
ndnu
trit
iona
lins
ulin
need
sm
etw
ith
reg-
Iad
ded
toT
PNba
gdi
rect
ly●
To
dete
rmin
eda
ilydo
seof
insu
linto
add
toT
PNba
g,co
nsid
erus
eof
sepa
rate
IVin
sulin
infu
sion
for
24h
tode
term
ine
daily
insu
linre
quir
emen
t,th
enad
d2/
3of
this
amou
ntto
subs
eque
ntT
PNba
gs;o
rad
d2/
3of
tota
luni
tsof
insu
linad
min
iste
red
SQth
epr
evio
usda
yto
the
next
day’
sT
PNba
gas
reg-
I,un
tild
aily
dose
dete
rmin
ed●
Use
SQin
sulin
wit
hca
utio
nw
ith
TPN
.Lac
kof
corr
elat
ion
ofin
sulin
peak
san
dtr
ough
sw
ith
nutr
ient
deliv
ery
may
lead
toer
rati
cBG
cont
rol
Tra
nsit
ion
toor
alin
take
●In
t-I
bid
●LA
-Ihs
oram
●R
eg-I
orra
pid-
Iac
●R
eg-I
orra
pid-
Iac
ac
/�hs
●G
ive
reg-
I,30
–45
min
orra
pid-
I0–
15m
inpr
ior
tom
ealt
oco
ntro
lpos
tpra
ndia
lBG
excu
rsio
ns●
Post
pran
dial
targ
etBG
�18
0m
g/dl
●C
heck
finge
rsti
ckBG
2h
afte
rre
g-I
or1
haf
ter
rapi
d-I
tode
term
ine
pran
dial
insu
lindo
sead
just
men
tsH
igh-
dose
gluc
ocor
tico
idR
x●
Insu
lindr
ip;I
nt-I
bid;
LA-I
hsor
amR
eg-I
orR
A-I
:R
eg-I
orra
pid-
I:●
Hig
h-do
segl
ucoc
orti
coid
sra
ise
insu
linre
quir
emen
ts●
ac(B
and
D)
orac
(B,L
,and
D)
ifea
ting
;or
q4–
6h
ifN
PO
●ac
and
hsif
eati
ng;o
rq
4–6
hour
sif
NPO
●A
djus
t/in
crea
sein
sulin
dose
sto
coun
ter
post
pran
dial
hype
rgly
cem
iaan
dBG
peak
that
may
occu
r8–
12h
follo
win
gon
ce-d
aily
GC
dose
●A
lter
nate
-day
ster
oid
dose
sre
quir
eal
tern
ate-
day
insu
lindo
ses
ac,b
efor
em
eals
;am
,mor
ning
;B,b
reak
fast
;BG
,blo
odgl
ucos
e;D
,din
ner;
DK
A,d
iabe
tic
keto
acid
osis
;GC
,glu
coco
rtic
oid;
HH
S,hy
perg
lyce
mic
hype
rosm
olar
stat
e;hs
,bed
tim
e;I,
insu
lin;I
nt-I
,int
erm
edia
teac
ting
insu
lin(N
PHor
Lent
e);I
V,i
ntra
veno
us;L
,lun
ch;L
A-I
,lon
g-ac
ting
insu
lin(g
larg
ine
orul
tral
ente
);O
R,o
pera
ting
room
;q,e
very
;qd,
ever
yda
y;ra
pid-
I,ra
pid
acti
ngin
sulin
(lis
pro
oras
part
);R
eg-I
,reg
ular
insu
lin;S
Q,s
ubcu
tane
ous.
Clement and Associates
DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004 567

to reduce errors. Practice guidelines forusing insulin under various clinical cir-cumstances are summarized in Table 3.Intravenous insulin infusion. The onlymethod of insulin delivery specifically de-veloped for use in the hospital is contin-uous intravenous infusion, using regularcrystalline insulin. There is no advantageto using insulin lispro or aspart in an in-travenous insulin infusion. The medicalliterature supports the use of intravenousinsulin infusion in preference to the sub-cutaneous route of insulin administrationfor several clinical indications amongnonpregnant adults, including diabeticketoacidosis and nonketotic hyperosmo-lar state (258–275); general preoperative,intraoperative, and postoperative care(257,276–290); the postoperative periodfollowing heart surgery (142,196,198,290,291); organ transplantation (297); orcardiogenic shock (128,194,292–296)and possibly stroke (147); exacerbatedhyperglycemia during high-dose glu-cocorticoid therapy (297); NPO status(298); critical care illness (2,299–301);and as a dose-finding strategy, anticipa-tory to initiation or reinitiation of subcu-taneous insulin therapy in type 1 or type 2diabetes (Table 4) (302–304). Some ofthese settings may be characterized by, orassociated with, severe or rapidly chang-ing insulin requirements, generalized pa-tient edema, impaired perfusion ofsubcutaneous sites, requirement for pres-sor support, and/or use of total parenteralnutrition. In these settings the intrave-nous route for insulin administration sur-passes the subcutaneous route withrespect to rapidity of onset of effect incontrolling hyperglycemia, overall ability
to achieve glycemic control, and most im-portantly, nonglycemic patient outcomes.During intravenous insulin infusion usedto control hyperglycemic crises, hypogly-cemia (if it occurs) is short-lived, whereasin the same clinical settings repeated ad-ministration of subcutaneous insulin mayresult in “stacking” of the insulin’s effect,causing protracted hypoglycemia. As analternative to continuous intravenous in-fusion, repeated intravenous bolus ther-apy also has been advocated for patientswith type 2 diabetes during anesthesia(305).
Depending on the indication for in-travenous insulin infusion, caregiversmay establish different glycemic thresh-olds for initiation of intravenous insulintherapy. For patients not hyperglycemicinitially, it is best to assign a blood glucosethreshold for initiation of the insulin in-fusion that is below the upper limit of thetarget range glucose at which the infusionprotocol aims. For patients with type 1diabetes, uninterrupted intravenous insu-lin infusion perioperatively is an accept-able and often the preferred method ofdelivering basal insulin. For these pa-tients, intravenous insulin infusion ther-apy should be started before the end ofthe anticipated timeframe of action of pre-viously administered subcutaneous insu-lin, i.e., before hyperglycemia or ketosiscan develop. For patients having electivesurgery, hourly measurements of capil-lary blood glucose may be ordered, andthe intravenous infusion of insulin may beinitiated at a low hourly rate when risingblood glucose levels (�120 mg/dl, or 6.7mmol/l) indicate waning of the effects ofpreviously administered intermediate or
long-acting insulin. The desirability of in-fusing dextrose simultaneously dependson the blood glucose concentration andthe condition for which the insulin infu-sion is being used (275,288).Mixing the insulin infusion. Depend-ing on availability of infusion pumps thataccurately deliver very low hourly vol-umes, intravenous insulin therapy is con-ducted with regular crystalline insulin in asolution of 1 unit per 1 ml normal saline.The concentrated infusion is piggy-backed into a dedicated running intrave-nous line. Highly concentrated solutionsmay be reserved for patients requiringvolume restriction; otherwise, solutionsas dilute as 1 unit insulin per 10 ml nor-mal saline may be used (306,307). Whenthe more dilute solutions are used, at least50 ml of the insulin-containing solutionshould be allowed to run through the tub-ing before use (308). It is prudent to pre-pare and label the solutions in a centralinstitutional pharmacy, if possible usingthe same concentration for all adultpatients.
The use of a “priming bolus” to initi-ate intravenous insulin infusion is contro-versial (265). The half-l i fe of anintravenous insulin bolus is about 4–5min (309), and, although tissue effects aresomewhat delayed, by 45 min insulinblood levels return virtually to baseline.Because repeated intravenous bolus insu-lin therapy does not maintain adequateblood insulin levels or target tissue actionof insulin, the initial priming bolus of in-travenous insulin, if used, must be fol-lowed by maintenance insulin infusiontherapy (310,311).Insulin infusion initiation. Com-monly, for unstressed normoglycemicadults of average BMI, insulin infusion isinitiated at 1 unit/h but adjusted asneeded to maintain normoglycemia (i.e.,the perioperative setting). The assump-tion that 50% of the ambulatory dailyinsulin dose is the basal requirement canalso be used to estimate initial hourly re-quirements for a normoglycemic, un-stressed patient previously treated withinsulin (312). Alternatively, a weight-based insulin dose may be calculated us-ing 0.02 units � kg�1 � h�1 as a startingrate. A lower initial insulin infusion ratemay be used for patients with low bodyweight or renal or hepatic failure or if theinfusion is started within the timeframe ofaction of previously administered subcu-taneous insulin. A higher initiation rate
Table 4—Indication for intravenous insulin infusion among nonpregnant adults with estab-lished diabetes or hyperglycemia
IndicationStrength ofEvidence
Diabetic ketoacidosis and nonketotic hyperosmolar state AGeneral preoperative, intraoperative, and postoperative care CPostoperative period following heart surgery BOrgan transplantation EMI or cardiogenic shock AStroke EExacerbated hyperglycemia during high-dose glucocorticoid therapy ENPO status in type 1 diabetes ECritically ill surgical patient requiring mechanical ventilation ADose-finding strategy, anticipatory to initiation or reinitiating of
subcutaneous insulin therapy in type 1 or type 2 diabetesC
Management of diabetes and hyperglycemia in hospitals
568 DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004

such as �2 units/h may be used whenhyperglycemia is present, when pread-mission insulin requirements are high, orif the patient has conditions predictingthe presence of insulin resistance. Amonghyperglycemic type 1 and type 2 diabeticpatients who were otherwise well and re-ceiving no concomitant intravenous dex-trose, the prime determinants of the initialhourly intravenous insulin requirementare the initial plasma glucose and BMI.After attainment of normoglycemia, onlythe BMI correlates with the hourly insulininfusion requirement (313). It has beenargued that the maximum biologic effectof insulin might be expected at infusionrates of 10 units/h or less. However, somepatients benefit from higher infusion ratesaccording to setting, and use of hourlyinsulin infusion rates as high as 50 units/hhas been reported, particularly in the in-tensive care setting (2).
Assignment and adjustment of the in-travenous insulin infusion rate is deter-mined by the caregiver, based onknowledge of the condition of the patient,the blood glucose level, and the responseto previous therapy. Blood glucose deter-minations should be performed hourlyuntil stability of blood glucose level hasbeen demonstrated for 6–8 h; then, thefrequency of blood glucose testing can bereduced to every 2–3 h. To avoid un-wanted excursions of blood glucose, es-pecially when making corrective changesin the insulin infusion rate, the pharmaco-dynamics of intravenous insulin adminis-tration and delay of tissue responsivenessfollowing attainment of a given bloodlevel of insulin must be considered. Ifconcomitant infusion of dextrose is used,caregivers must be alert to the effects ofabrupt changes of dextrose infusion rate.Well-conducted insulin infusion therapyshould demonstrate progressively smalleroscillations of the hourly insulin infusionrate and narrower excursions of bloodglucose, as the caregiver discovers thehourly rate that will maintain normogly-cemia for a given patient.
Many institutions use insulin infusionalgorithms that can be implemented bynursing staff (2,189,194,197,200,280,298,301,304,307,314). Algorithmsshould incorporate the concept thatmaintenance requirements differ betweenpatients and change over the course oftreatment. The algorithm should facilitatecommunication between physicians andnurses, achieve correction of hyperglyce-
mia in a timely manner, provide a methodto determine the insulin infusion rate re-quired to maintain blood sugars within adefined the target range, include a rule formaking temporary corrective incrementsor decrements of insulin infusion ratewithout under- or overcompensation,and allow for adjustment of the mainte-nance rate as patient insulin sensitivity orcarbohydrate intake changes. The algo-rithm should also contain directions as tohow to proceed if hypoglycemia or a rapidfall in blood glucose occurs, as well asinstructions as to how to transition thepatient to scheduled subcutaneous insulin.
Physician orders to “titrate drip” to agiven target blood glucose range, or pro-tocols requiring application of mathemat-ical rules by nursing staff, may be difficultto implement. A mathematical algorithmcan be reduced to tabular form, in whicheach column indicates different insulininfusion rates necessary to maintain targetrange control and shows appropriate in-fusions rates necessary for correction atgiven blood glucose levels, accompaniedby a rule for shifting between columns(see online appendix 2 [available at http://care.diabetesjournals.org]) (314). It isprudent to provide inservice teaching ofpharmacy, nursing, and physician staff onthe use of insulin drip protocols (307).Transition from intravenous to subcu-taneous insulin therapy. To maintaineffective blood levels of insulin, it is nec-essary to administer short- or rapid-actinginsulin subcutaneously 1–2 h before dis-continuation of the intravenous insulininfusion (191,199,315–319). An inter-mediate or long-acting insulin must be in-jected 2–3 h before discontinuing theinsulin infusion. In transitioning from in-travenous insulin infusion to subcutane-ous therapy, the caregiver may ordersubcutaneous insulin with appropriateduration of action to be administered as asingle dose or repeatedly to maintainbasal effect until the time of day when thechoice of insulin or analog preferred forbasal effect normally would be provided.For example, a patient who normally usesglargine at bedtime and lispro beforemeals, and whose insulin infusion will bestopped at lunchtime, could receive adose of lispro and a one-time injection ofNPH before interruption of the insulininfusion.Initial scheduled insulin, dose deci-sions, and correction-dose calcula-
tions. The initial doses of scheduledsubcutaneous insulin are based on previ-ously established dose requirements, pre-vious experience for the same patientduring similar circumstances of nutri-tional change or drug administration, re-quirements during continuous insulininfusion (if stable), knowledge of stabilityor instability of medical condition andnutritional intake, assessment of medicalstress, and/or body weight. Correctiondoses for various ranges of total daily in-sulin requirement or body weight can beexpressed in tabular form, as a compo-nent of standardized inpatient orders (seeonline appendix 1). For most insulin-sensitive patients, 1 unit of rapid-actinginsulin will lower blood glucose by 50–100 mg/dl (2.8–5.6 mmol) (320). A re-duction of the correction dose at bedtimeis appropriate to reduce the risk of noc-turnal hypoglycemia. For patients whoseinsulin requirements are unknown andwhose nutritional intake will be adequate,an assumption concerning requirementfor scheduled insulin based on bodyweight would be about 0.5–0.7 units/kginsulin per 24-h period for patients hav-ing type 1 diabetes and 0.4–1.0 units/kgor more for patients having type 2 diabe-tes, starting low and working up to thedose to meet demonstrated needs, withassignment of a corresponding scale forcorrection doses. If nutritional intake isseverely curtailed, for type 1 diabetes theamount of scheduled insulin calculatedby body weight should be reduced by50%. For type 2 diabetes, a safe initialassumption in the absence of nutritionalintake would be that endogenous insulinmight meet needs, requiring supplemen-tation only with correction doses, untilresults of monitoring indicate the furtherneed for scheduled insulin.Perioperative insulin requirements. Inthe perioperative period for all type 1 di-abetic patients and for those type 2 dia-betic patients with demonstrated insulindeficiency, scheduled insulin intended toprovide basal coverage should be admin-istered on the night before surgery to as-sure optimum fasting blood glucose forthe operative room. If insulin intended tomeet basal needs is normally adminis-tered in the morning, in the case of type 1diabetes the morning basal insulin isgiven without dose adjustment, and in thecase of type 2 diabetes 50–100% of thebasal insulin is administered on the morn-ing of surgery. Correction doses may be
Clement and Associates
DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004 569

applied on the morning of surgery if themorning glucose concentration exceeds180 mg/dl.Appropriate use of insulin self-management. Recognition of the patientrights, patient responsibilities, and theimportance of patient-oriented care arecritical to the care of diabetes (321–323).In the ambulatory setting, patient self-management has a favorable impact onglycemic control and quality of life(324,325). Using the tools of multipledaily injections of insulin or CSII, patientself-management has been shown to becapable of improving glycemic controland microvascular outcomes (326–328).In multiple-dose insulin therapy, meal-time treatment with rapid-acting insulinanalog improves hypoglycemia and post-prandial hyperglycemia in comparisonwith conventional therapy in both type 2(329) and type 1 diabetes (253,330 –332). In comparison with conventionalmanagement using intermediate-actinginsulin for basal effect, patients usinglong-acting insulin analog for basal insu-lin effect experience less overall or noctur-nal hypoglycemia (333–336), bettercontrol of fasting plasma glucose levels(333,337), and lower HbA1c levels (333).In CSII therapy, rapid-acting analogs im-prove control for most patients (338 –340). Use of advanced carbohydratecounting and an insulin-to-carbohydrateratio have markedly enhanced the successof patients to implement intensive self-management (341). Patients familiar withtheir own needs sometimes have experi-enced adverse events or, perceiving threatof adverse events, express frustration withrigidity of hospital routine and delegationof decision making to providers who areless likely to understand their immediateneeds.
Self-management in the hospital maybe appropriate for competent adult pa-tients who have stable level of conscious-ness and reasonably stable known dailyinsulin requirements and successfullyconduct self-management of diabetes athome, have physical skills appropriate tosuccessfully self-administer insulin, per-form self-monitoring of blood glucose,and have adequate oral intake. Appropri-ate patients are those already proficient incarbohydrate counting, use of multipledaily injections of insulin or insulin pumptherapy, and sick-day management. Thepatient and physician in consultationwith nursing staff must agree that patient
self-management is appropriate under theconditions of hospitalization. Compo-nents of the program can include a phy-sician order for self-management withrespect to selection of food from a generaldiet, self-monitoring of blood glucose,self-determination and administration ofinsulin dose, and ranges of insulin to betaken. Patient record-keeping, sharing ofresults with nursing staff, and charting bynursing staff of self-determined glucoseresults and insulin administration shouldoccur. If a subcutaneous insulin pump isused, provisions for assistance in trouble-shooting pump problems need to be inplace. Assistance might be required ifequipment familiar to the patient is un-available, if refrigeration is required, or ifphysical autonomy is imperfect. For ex-ample, decision making about dosagemay be intact, but manual dexterity oravailability of easily reached injectionsites may be altered by the conditions ofhospitalization. Additionally, help may berequired in a situation of increasing insu-lin resistance or period of NPO where thepatient may not know how to adjust his orher insulin doses appropriately.
Although the program should be de-veloped in compliance with institutionaland external regulatory requirements,consideration should be given to permit-ting self-use of equipment and drugs al-ready in the possession of the patient butnot normally on formulary. The programshould not create additional burdens fordietary or nursing staff. As one of thelikely barriers to implementation, institu-tions should recognize that fear of notonly causing patient harm, but also of ex-posure of deficiencies of knowledge andskill, may underlie staff resistance to pa-tient self-management programs. Staffmay be trained in advance to understandthat proficiency in making intensive man-agement decisions or using specializedequipment is not expected of them by ei-ther their employer or the patient. Ordersto replace self-management with provid-er-directed care should be written whenchanging the condition of the patientmakes self-management inappropriate(342). Table 5 summarizes the compo-nents necessary for diabetes self-management.
Preventing hypoglycemiaHypoglycemia, especially in insulin-treated patients, is the leading limitingfactor in the glycemic management of
type 1 and type 2 diabetes (343–347). Inthe hospital, multiple additional risk fac-tors for hypoglycemia are present, evenamong patients who are neither “brittle”nor tightly controlled. Patients who donot have diabetes may experience hypo-glycemia in the hospital, in associationwith factors such as altered nutritionalstate, heart failure, renal or liver disease,malignancy, infection, or sepsis (348). Pa-tients having diabetes may develop hypo-glycemia in association with the sameconditions (349). Additional triggeringevents leading to iatrogenic hypoglycemiainclude sudden reduction of corticoste-roid dose; altered ability of the patient toself-report symptoms; reduction of oralintake; emesis; new NPO status; reduc-tion of rate of administration of intra-venous dextrose; and unexpected inter-ruption of enteral feedings or parenteralnutrition. Under-prescribing neededmaintenance antihyperglycemic therapyis not always fully protective against suchcauses of hypoglycemia. Nevertheless,fear of hypoglycemia may contribute toinadequate prescribing of scheduled dia-betes therapy or inappropriate relianceupon “sliding scale” monotherapy(255,256,350).
Despite the preventable nature ofmany inpatient episodes of hypoglyce-mia, institutions are more likely to havenursing protocols for treatment of hypo-glycemia than for its prevention (351–359). Nursing and pharmacy staff mustremain alert to the effects of antihypergly-cemic therapy that may have been admin-istered on a previous shift. Variousconditions creating a high risk for hypo-glycemia are listed in Table 6. If identified,
Table 5—Components for safe diabetes self-management in the hospital
● Perform simultaneous laboratory-measured capillary or venous blood testand patient-performed capillary bloodglucose test. The capillary blood glucosetest should be �15% of the laboratorytest.
● Demonstration that the patient can self-administer insulin accurately.
● Patient is alert and is able to makeappropriate decisions on insulin dose.
● All insulin administered by the patientand nurse is recorded in the medicationrecord.
● Physician writes order that the patientmay perform insulin self-management.
Management of diabetes and hyperglycemia in hospitals
570 DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004

preventive strategies could potentiallyinclude a provision, under protocol or byphysician order, to perform blood glucosetesting more frequently and, for fallinglevels, to take preventive action.
Special situations: TPNHyperglycemia in patients without diabe-tes from TPN is based on a variety of fac-tors—age (360), severity of illness (361),and the rate of dextrose infusion (362)—all of which affect the degree of hypergly-cemia. In individuals with preexistingtype 2 diabetes not previously receivinginsulin therapy, 77% of patients requiredinsulin to control glycemia during TPN(363). Insulin doses in this group aver-aged 100 � 8 units/day.
There are no controlled trials examin-ing which strategies are best for this situ-ation. Adding incremental doses ofinsulin to the TPN is one option, but thismay require days to determine the correctinsulin dose (306). The use of a separateintravenous insulin infusion brings mostpatients within target within 24 h (364).Two-thirds to 100% of the total numberof units of insulin used in the variable rateinfusion over the previous 24-h periodcan subsequently be added to the subse-quent TPN bag(s) (306,365).
Special situations: glucocorticoidtherapyGlucocorticoids are well known to affectcarbohydrate metabolism. They increasehepatic glucose production, inhibit glu-cose uptake into muscle, and have a com-plex effect on �-cell function (366–368).The decrease in glucose uptake with glu-cocorticoids seems to be the major earlydefect (369,370), and thus it is not sur-prising that for hospitalized patients withwell-controlled type 2 diabetes, postpran-dial hyperglycemia is the most significant
problem. Although in some patients thehyperglycemia, if present, may be mild, inothers the glucocorticoids may be respon-sible for hyperosmolar hyperglycemicsyndrome (371). The best predictors ofglucocorticoid-induced diabetes are fam-ily history of diabetes, increasing age, andglucocorticoid dose.
There are few studies examining howto best treat glucocorticoid-induced hy-perglycemia. Thiazolidinediones may beeffective for long-term treatment withglucocorticoids (372), but no insulin sen-sitizer would be appropriate for the initialmanagement of acute hyperglycemia inthe hospital due to the fact their antihy-perglycemic effects will take weeks to oc-cur. There is also an uncontrolled reportsuggesting that chromium may be benefi-cial for this population (373). Insulin isrecommended as the drug of choice forthe treatment of glucocorticoid-inducedhyperglycemia. Although data are notavailable, due to the effect of glucocorti-coids on postprandial glucose, an empha-sis on the use of prandial insulin would beexpected to have the best results. For pa-tients receiving high-dose intravenousglucocorticoids, an intravenous insulininfusion may be appropriate (306). Theinsulin dose requirements are extremelydifficult to predict, but with the insulininfusion it is possible to quickly reach therequired insulin dosing. Furthermore, forshort glucocorticoid boluses of no morethan 2 or 3 days, the insulin infusion al-lows appropriate tapering of insulin infu-sion rates so that glycemic control is notcompromised and hypoglycemic riskscan be minimized as steroid doses are re-duced. It should be emphasized that ifintravenous insulin is not used, there willbe a greater increase in prandial com-pared with basal insulin doses. There areno trials comparing the use of insulin lis-pro or insulin aspart to regular insulin forthis situation.
Special situations: enteral feedingCurrent enteral nutrition formulas aregenerally high in carbohydrate (with anemphasis on low–molecular weight car-bohydrates) and low in fat and dietary fi-ber. Carbohydrates contribute 45–92% ofcalories (374). There are a variety of dif-ferent protein sources in these enteralfeedings, and there are no contraindica-tions for use of any of these in people withdiabetes. Generally, enteral formulas con-tain 7–16% of total calories from protein.
For most institutionalized patients, it isrecommended that protein intake shouldbe 1.2–1.5 g � kg�1 � day�1 (375). Mostcurrently available standard formulascontain 25–40% of total calories from fat.There is current controversy as to howmuch of this fat source should be fromn-3 compared with n-6 fatty acids. Notsurprisingly, products that are lower incarbohydrate and higher in dietary fiberand fat have less of an impact on diabetescontrol (376,377).
There is only one study reporting gly-cemic outcomes for people with type 2diabetes receiving different enteral for-mulas (378). Thirty-four patients wererandomized to a reduced-carbohydrate,modified fat enteral formula or a standardhigh-carbohydrate feeding. After 3months, HbA1c levels were lower for thegroup receiving the reduced-carbohy-drate formula, but this did not reachstatistical significance. For those random-ized to the high-carbohydrate formula,HDL cholesterol levels were lower and tri-glyceride concentrations were higher. In-terestingly, in this small study, the groupreceiving the reduced-carbohydrate for-mula had 10% fewer infections.
There are no clinical trial data exam-ining different strategies of insulin re-placement for this population. Forintermittent enteral feedings such as noc-turnal tube feeding, NPH insulin, usuallywith a small dose of regular insulin, workswell. The NPH insulin provides basal in-sulin coverage, while the regular insulin isadministered before each tube feeding tocontrol postprandial glucose levels. Dosesshould be calculated based on capillaryglucose testing before and 2 h after eachenteral feeding period. Continuous feed-ing may be managed by several differentstrategies; again, however, there are nodata that have examined these manage-ment strategies. One could use once- ortwice-daily insulin glargine. Ideally, onewould start with a small basal dose anduse correction-dose insulin as neededwhile the glargine dose is being increased.Alternatively, the initial dose could be es-timated by the amount of insulin requiredfrom a 24-h intravenous insulin infusion.This, however, may not be an accurateassessment of actual subcutaneous insu-lin needs. The major concern about usinginsulin glargine or ultralente insulin forthis population is that when the enteralfeeding is discontinued, whether plannedor not, the subcutaneous insulin depot
Table 6—Conditions creating high risk forhypoglycemia in patients receiving scheduled(programmed) insulin
● Sudden NPO status or reduction in oralintake
● Enteral feeding discontinued● TPN or intravenous dextrose
discontinued● Premeal insulin given and meal not
ingested● Unexpected transport from nursing unit
after rapid-action insulin given● Reduction in corticosteroid dose
Clement and Associates
DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004 571

will result in a high risk of hypoglycemia,particularly if large doses of insulin arerequired. The use of NPH or regular insu-lin for this situation is also problematicsince the peaks and troughs of insulin donot match the insulin requirements ne-cessitated by the carbohydrate infusion.Although there is no ideal way to managethis problem, the safest appears to main-tain target blood glucose at the high endof the target range using basal insulins.When the tube feeding is discontinued,either enteral or parenteral glucose mustbe infused until the subcutaneous insulinhas dissipated.
HOW CAN SYSTEM DESIGNAND IMPLEMENTATIONIMPROVE DIABETES CAREIN THE HOSPITAL? — The designand implementation of protocols formaintaining glucose control in the hospi-tal may provide useful guidance to thetreating physician. Diabetes managementmay be offered effectively by primary carephysicians or hospitalists, but involve-ment of appropriately trained specialistsor specialty teams may reduce length ofstay, improve glycemic control, and im-prove outcomes (314,379–381). For avariety of conditions, outcomes understandardized pathways or dose titrationprotocols are superior to those achievedby individualization of care (382). In eval-uation of institutional performance, vari-ability of treatment strategies amongproviders may itself be interpreted as arisk factor for unsafe practices, and “stan-dardization to excellence” may be inter-preted as a surrogate for patient safety(322,383). In the care of diabetes, imple-mentation of standardized order sets forscheduled and correction-dose insulinmay reduce reliance on sliding scale man-agement (307). A team approach isneeded to establish hospital pathways. Toimplement intravenous infusion of insu-lin for the majority of patients having pro-longed NPO status, hospitals will needmultidisciplinary support for using insu-lin infusion therapy outside of critical careunits.
Patient safety, quality of care, vari-ability of practice, and medical error havebeen the subjects of increasing nationalconcern (384–390). Quality assessmentprograms that strive to promote a “cultureof safety” commonly focus on diabetes. Ithas been reported that 11% of medicationerrors result from insulin misadministra-
tion (391), and insulin has been identifiedas one of several medications that deservehigh alert status (392,393). Hypoglyce-mia may result from drug-dispensing er-rors, including mistaken administrationof hypoglycemic agents to nondiabeticpatients. For diabetic patients, frank pre-scribing errors, the use of trailing zerosafter decimal points, or misinterpretedabbreviations for insulin may compro-mise patient safety (394–397). Becausecapital “U” can be mistaken for a numeralwhen handwritten, the word “units”s-hould be spelled out in physician orders(391,398). The erroneous administrationof a large dose of rapid-acting insulin inplace of insulin glargine can easily occur,since insulin glargine and rapid-acting in-sulins look the same in the vial (both areclear). Barcoding of drugs and pharmacistparticipation in rounds and in surveil-lance of prescribing patterns may help re-duce errors (399–404). Although someemphasis has been placed on institutionals tandardizat ion of s l iding scales(382,405), sliding scale monotherapy it-self has been considered to be both inef-fective compared with anticipatorymanagement and frequently dangerous. Acomputerized order entry system can re-duce utilization of sliding scale manage-ment (406) . Wi th pre sen t -daymonitoring techniques, the inhouse de-velopment of ketoacidosis or hyperglyce-mic hyperosmolar state is generallypreventable, and any occurrence shouldsuggest the need for a root cause analysis(407–415). By tracking transfers or read-missions to the intensive care unit, it issometimes possible to detect an opportu-nity for improvement, such as a recurrentpattern of failure to administer scheduledsubcutaneous insulin at the terminationof insulin infusion leading to develop-ment of metabolic emergency.
Both hypoglycemia and hyperglyce-mia are patient safety issues appropriatefor continuous quality improvement(CQI) analysis. Nevertheless, as a focusfor institutional CQI activities, hypogly-cemia receives more attention, and hypo-glycemic events are more readily definedand ascertained. Pharmacies can readilytrack for example the dispensing of D50as an “antidote,” administered by nursingstaff without physician orders, or detecthypoglycemia through analysis of reportsof adverse drug reactions (416). In con-trast, although computer searches of thelaboratory databank may be used to help
identify instances of hyperglycemia, atmany institutions point-of-care measure-ments will escape detection unless valuesare scanned into an electronic databank(417). Severe hyperglycemia (at least oneglucose level �400 – 450 mg/dl), pro-longed hyperglycemia (at least three con-secutive glucose levels �250 mg/dl), andketosis all can be used as quality-controlindicators. The time from presentation tothe emergency room with hyperglycemicemergency to the initiation of an insulininfusion may be viewed as a quality issue(268). The use of a balanced emphasis onboth hypoglycemia and hyperglycemia byhospital quality-improvement programshas been linked to changes in practicepatterns that result in improved control(418–420).
WHAT IS THE ROLE OFDIABETES SELF-MANAGEMENT EDUCATIONFOR THE HOSPITALIZEDPATIENT? — Teaching diabetes self-management to patients in hospitals is adifficult and challenging task. Patients arehospitalized because they are ill, are un-der increased stress related to their hospi-talization and diagnosis, and are in anenvironment that is not conducive tolearning. In addition, patients are oftenunable to get the optimal amount of restbecause of various distractions, such asthe telephone, TV, personnel, meal times,testing, and procedures. The shock of di-agnosis, denial, anger, grief, and manyemotions frequently prevent or impair theperson’s ability to meaningfully partici-pate in the educational process. Ideally,people with diabetes should be taught at atime and place conducive to learning: asan outpatient in a nationally recognizedprogram of diabetes education classes.
For the hospitalized patient, diabetes“survival skills” education is generallyconsidered a feasible approach. Patientsare taught sufficient information to enablethem to go home safely. Those newly di-agnosed with diabetes or who are new toinsulin and or blood glucose monitoringneed to be instructed before discharge tohelp ensure safe care upon returninghome. Those patients hospitalized be-cause of a crisis related to diabetes man-agement or poor care at home neededucation to hopefully prevent subse-quent episodes of hospitalization. Goalsof inpatient diabetes self-management ed-ucation (DSME) are listed in Table 7.
Management of diabetes and hyperglycemia in hospitals
572 DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004

The efficacy of hospital-based DSMEon outcomes has not been tested in ran-domized prospective studies. Performingsuch a study that denies the basics ofDSME to a control group is consideredunethical (421). Given the limitations andethics of study design, several studies sug-gest hospital-based DSME has substantialbenefits in outcomes. Using historicalcontrols, Muhlhauser et al. (422) re-ported a 66% reduction in hospitalizationdays and an 86% reduction in episodes ofdiabetic ketoacidosis after implementingan intensive inpatient-based educationprogram for patients with type 1 diabetes.Four deaths occurred in the controlgroup, compared with no deaths in thetreatment group. All deaths were fromacute diabetes-related complications.
Fedderson and Lockwood (423) con-ducted a prospective nonrandomizedstudy at a single 713-bed teaching hospi-tal. Within the hospital, four similar pa-tient care units (PCUs) were identified forthe study intervention. Two units weredesignated as the treatment units and twoas the control units. For the control units,DSME was provided by the regular nurs-ing staff. For the experimental units, a cer-tified diabetes educator (CDE) wasemployed to provide education to boththe staff nurses and directly to diabeticpatients. The nurse CDE conducted threeseparate teaching sessions for the staffnurses in the experimental PCUs on infor-mation that an insulin-requiring patientwith diabetes needs before discharge. Thenurse CDE also provided direct patienteducation. The authors reported a meanreduction in hospital length of stay of 1.3days in the experimental group versus thecontrol group (P � 0.005).
Wood (424) compared the efficacy ofindividualized DSME (control group) toindividualized DSME supplemented by2-h group classes held weekly (experi-mental group). Patients medically unsta-ble were excluded from the study. Based
on a follow-up questionnaire, the experi-mental group reported better adherencefor all self-care behaviors than the controlgroup. Four months postdischarge, theexperimental group had significantlyfewer emergency room visits comparedwith the control group (2 vs. 20 visits,respectively, P � 0.005).
Writing DSME consult requestsWhen writing a request for consultationfor diabetes education, the referral shouldstate the specific reason for the referral(not just state “Diabetes Education”), anypertinent details regarding the patient sta-tus, the discharge plan and person refer-ring for consult, and how to contact them(Table 8). Early referral is encouraged, es-pecially for those patients newly diag-nosed with diabetes. Patients should bemedically stable and able to participate inthe educational process. Patients who arein pain or sedated should not be referredfor DSME until their medical conditionimproves. Including various disciplinesin the plan of care is equally important. Ifcaregivers are involved, it is importantthat they be identified and included in theteaching process. Patients who are cogni-tively impaired are not good candidatesfor teaching and should have alternativeoptions of care considered. Topics to becovered should be relevant to the plan ofcare and ready to implement at the time ofdischarge.
It is best to maximize the time spent
on topics immediately relevant to the pa-tient’s diabetes management. Registereddietitians should be consulted for medicalnutritional therapy and patient teaching.Social workers and case managers shouldbe involved with discharge planning andorders for home-health-nurse follow upupon discharge. Those likely in need ofhome health nursing referrals includenewly diagnosed diabetic patients, pa-tients new to insulin, the aged or infirm,and those for whom there are complianceconcerns.
Patient assessmentPatient assessment assists with definingthe patient’s problems and acknowledg-ing his or her concerns. When seeing aninpatient for an initial consultation, it isimperative to be able to focus on thegreatest needs of the patient at that time.Knowing the reason for the consultationallows the educator to direct precioustime and energy to those specific educa-tional needs and to bring any necessaryteaching materials/supplies to the bed-side. Before actually seeing the patient,the diabetes educator should review thechart and, if necessary, speak with the re-ferring physician or registered nurse whois caring for the patient in order to obtainadditional information. Assessment criti-cal to patient teaching includes:
● Knowledge, psychomotor skills, and af-fective domains
● Current level of self care● Preferred learning styles● Psychological status● Stress factors that impair learning● Social/cultural/religious beliefs● Literacy skills● Readiness to learn● Assessment of abilities—age, mobility,
visual acuity, hearing loss, and dexter-ity
Table 7—Goals of inpatient DSME
● Assess current knowledge and practices of diabetes self-management and how they impactpatient’s health status and reason for hospitalization
● Initiate diabetes education for patients newly diagnosed with diabetes● Provide information on basic self-management skills to help ensure safe care postdischarge● Team approach with other health professionals (e.g., physicians, nurses, dietitians, case
managers, and social workers) coordinating care in the hospital and post discharge● Provide information on community resources and diabetes education programs for
continuing education● The diabetes educator serves as a resource for nursing staff and other health care providers
Table 8—Writing the DSME consult request
Component of request Example
Specific reason for consult anddiagnosis
Diabetes education for insulin administration teachingfor patient with new-onset type 2 diabetes
Discharge medication plan Lantus 30 units hs, Novolog 6 units acSpecific comments/instructions Spanish-speaking patient; lives with daughterContact information John Smith, MD, pager #
ac, before meals; hs, bedtime.
Clement and Associates
DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004 573

Characteristics of adult learnersIn preparing to teach, it is good to keep inmind some of the characteristics of adultlearners:
● Usually self-directed● Must be receptive to learning● Tend to be problem-focused rather
than subject-oriented● Inclusive of past experiences with dia-
betes● Active participation
Deciding what to teach patientsDeciding what to teach patients in a lim-ited timespan is determined mostly bymedical necessity but also by the patient’sprevious experiences and desires. The pa-tient must be psychologically and emo-tionally ready for teaching. Listening toconcerns and acknowledging the patient’sfeelings without being judgmental is animportant aspect of changing behavior.When patients are newly diagnosed withdiabetes, teaching “survival skills” is thefirst step to outlining the principles of di-abetes management. These may include:
● What is diabetes? Principles of treat-ment and prevention of complications
● Norms for blood glucose and target glu-cose levels for the individual
● Recognition, treatment, and preventionof hyperglycemia and hypoglycemia
● Medical nutrition therapy (instructedby a registered dietitian who, prefera-bly, is a CDE)
● Medication● Self-monitoring of blood glucose● Insulin administration (if going home
on insulin)● Sick-day management● Community resources● Universal precautions for caregivers
Patients previously diagnosed withdiabetes need to have specific needs iden-tified, and their instruction must be tar-geted to those needs. Diabetes educationin a hospital setting is not meant to pro-vide comprehensive in-depth knowledgeof diabetes management, but is intendedto provide basic information for people tostart a life-long process of continuing di-abetes education.
Communication and dischargeplanningDocumentation, reviewing chart notes/suggestions, and oral communication are
vital to coordinating care with successfuloutcomes for hospitalized patients withdiabetes. Staff nurses need to work withpatients on developing their skills and re-inforcing knowledge of diabetes manage-ment. Medical orders and the dischargeplan of care need to be appropriate,achievable, and agreeable to the patientand family. For effective discharge plan-ning, collaboration among the treatingphysician, nurses, and the diabetes nurseeducator is essential for providing conti-nuity of care back to the outpatient set-ting. During discharge planning, thefollowing questions should be addressed:
● Does the patient require outpatientDSME?
● Can the patient prepare his or her ownmeals?
● Can the pat ient per form se l f -monitoring of blood glucose at the pre-scribed frequency?
● Can the patient take his or her diabetesmedications or insulin accurately?
● Is there a family member who can assistwith tasks that the patient cannot per-form?
● Is a visiting nurse needed to facilitatetransition to the home?
Discharge diabetes medicationsWhen arranging for hospital discharge,caution should be taken in prescribingantihyperglycemic therapy, especially forthe elderly. A recent hospital discharge isa strong predictor of subsequent seriousoutpatient hypoglycemia (425). This ob-servation should lead to caution in theplanning of antihyperglycemic therapy atdischarge and careful planning for follow-up. Prescribing patterns should take intoconsideration the evidence that amongthe sulfonylureas, glipizide is associatedwith less hypoglycemia than glyburide inthe elderly (426).
WHAT IS THE ROLE OFMEDICAL NUTRITIONTHERAPY IN THEHOSPITALIZED PATIENTWITH DIABETES? — Determiningthe nutritional needs of hospitalized pa-tients with diabetes, writing a diet orderto provide for those needs, and incorpo-rating the current nutrition principles andrecommendations for persons with diabe-tes can be a daunting task. Even thoughhospital diets are commonly ordered bycalorie levels based on the “ADA diet,” it
has been recommended that the term“ADA diet” no longer be used (427). Since1994, the ADA has not endorsed any sin-gle meal plan or specified percentages ofmacronutrients. Current nutrition rec-ommendations advise individualizationbased on treatment goals, physiologic pa-rameters, and medication usage; theserecommendations apply primarily to per-sons living in a home setting who, in con-junct ion wi th a team of hea l thprofessionals, self-manage their diabetes.
The question is, then, how do you usemedical nutrition therapy appropriatelyin the hospital? Nutrient needs often dif-fer in the home versus the hospital setting.The diabetes treatment plan used in thehospital may differ from home, e.g., insu-lin may be used instead of oral medica-tions. The types of food a person can eatmay change, or the route of administra-tion may differ, e.g., enteral or parenteralfeedings may be used instead of solidfoods. And lastly, the ability of institu-tions to individualize meal plans is greatlydecreased. Because of the complexity ofnutrition issues, it is recommended that aregistered dietitian, knowledgeable andskilled in medical nutrition therapy, serveas the team member who provides medi-cal nutrition therapy. The dietitian is re-sponsible for integrating informationabout the patient’s clinical condition, eat-ing, and lifestyle habits and for establish-ing treatment goals in order to determinea realistic plan for nutrition therapy(428). Registered dietitians who special-ize in nutrition support can play an in-valuable role in the management ofcritically ill patients. However, it is essen-tial that all members of the interdiscipli-nary team are knowledgeable of nutritiontherapy.
Goals of medical nutrition therapyFor the hospitalized patient, the goals ofnutrition therapy are multiple:
● Attain and maintain optimal metaboliccontrol of blood glucose levels, lipidlevels, and blood pressure to enhancerecovery from illness and disease
● Incorporate nutrition therapies to treatthe complications of diabetes, includ-ing hypertension, CVD, dyslipidemia,and nephropathy
● Provide adequate calories, as needs areoften increased in illness and during re-covery from surgery
Management of diabetes and hyperglycemia in hospitals
574 DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004

● Improve health through use of nutri-tious foods
● Address individual needs based on per-sonal, cultural, religious, and ethnicfood preferences
● Provide a plan for continuing self-management education and follow-upcare
Nutritional needs of hospitalizedpatientsThe caloric needs of most hospitalized pa-tients can be met through provision of25–35 kcal/kg body wt (429,430). Pro-tein needs vary on the basis of physiologicstress. Mildly stressed patients require 1.0g/kg body wt; moderately to severelystressed patients may need 1.5 g/kg bodywt. These levels are for patients with nor-mal hepatic and renal function. The pre-ferred route of feeding is the oral route. Ifintake is inadequate or if medical condi-tions prohibit oral feeding, then enteral ofparenteral feedings will be needed.
Consistent carbohydrate diabetesmeal-planning systemThe consistent carbohydrate diabetesmeal-planning system was developed toprovide institutions with an up-to-dateway of providing food service to patientsin those settings. The system is not basedon specific calorie levels, but rather on theamount of carbohydrate offered at eachmeal. This amount is consistent frommeal to meal and day to day. Meals arebased on heart-healthy diet principles—saturated fats and cholesterol are limited,and protein content falls within a usualdiet’s content of 15–20% of calories. In-stead of focusing on the type of carbohy-drate foods served, the emphasis is on thetotal amount of carbohydrate containedin the meal. The majority of carbohydratefoods should be whole grains, fruits, veg-etables, and low-fat milk, but some su-crose-containing foods can be included aspart of the total carbohydrate allowance(430). A typical day’s menu provides1,500–2,000 calories, with a range of12–15 carbohydrate servings (187–259g) divided among meals and snacks.
Central to the rationale for this systemis that the glycemic effect of carbohydraterelates more to the total amount of carbo-hydrate rather than the source. While anumber of factors influence glycemic re-sponse to individual foods, ingestion of avariety of foods does not acutely alter gly-cemic response if the amount of carbohy-
drate is similar (430). Sucrose does notincrease glycemia to a greater extent thanisocaloric amounts of starch. The prandial(mealtime) insulin dose is based on themeal’s carbohydrate content. Current rec-ommendations for fat modification (430)are incorporated by basing the meals on acardiac, heart-healthy menu when devis-ing the consistent carbohydrate mealplan.
An advantage to the use of this systemis that prandial insulin dosages can be or-dered on the basis of the known carbohy-drate content of the meal. For patientswith a poor appetite and poor intake, theprandial insulin can be given after themeal based on the amount eaten. Using aconsistent carbohydrate menu makes thiseasy to determine. Providing meals withthis system eases the burden on the healthcare team of trying to individualize diets,especially when it is not practical, such asduring a short hospital stay. Meals for pa-tients with type 1 diabetes can easily beadjusted by altering the number of carbo-hydrate servings and snacks (428). Effi-ciencies in food service are realized andpatient satisfaction is enhanced with thissystem (428,431). Another advantage isthat the system reinforces carbohydratecounting meal planning taught to manypersons with diabetes, particularly type 1diabetic individuals using advanced car-bohydrate counting. It serves as a basis forteaching newly diagnosed patients withdiabetes about meal planning and canserve as a reference for home meals.
The meals served to patients with di-abetes certainly affect glucose control, butit should be remembered it is not the onlyfactor influencing glycemia. Hospitalizedpatients often have poor appetites and in-take is suboptimal. Meals can be delayedor missed entirely due to tests and proce-dures. Other causes of poor glucose con-trol include erratic absorption of insulin,counterregulatory hormone stress re-sponses, increased insulin requirements,the length of time between premeal insu-lin and food consumption, and impairedgut motility caused by diabetic gastropa-resis and medications, particularly nar-cotics (300).
How to order consistentcarbohydrate dietsThere is no single meal-planning systemthat meets the needs of all institutions.Budgetary issues, food-service employeetime, local factors, and administration un-
derstanding and support affect the choiceof a meal planning system (432). Manyinstitutions are familiar with exchange di-ets and, therefore, some facilities still usethem as a system for planning meals. In-troduction of the consistent carbohydratesystem requires a multidisciplinary effort,staff education, and patient education forthe program to succeed, but it can offerclear benefits when implemented. Institu-tions can adapt the consistent carbohy-drate system to meet their needs. A reviewof the implementation of the consistentcarbohydrate system in institutions re-vealed some variations developed by var-ious facilities (431), as described below.
One hospital terms the diet the “con-sistent carbohydrate diabetes diet.” Calo-rie levels are not specified. Menus withfood selections instruct patients to choosethree to five carbohydrate foods at eachmeal, identifying the carbohydrate foods.Each contains 15 g carbohydrate. Dessertitems with 30 g carbohydrate (two carbo-hydrate choices) or 15 g are included atlunch and dinner. Another facility usesthe consistent carbohydrate menu withcalorie ranges from low to very high. Allcarbohydrate-containing foods aregrouped in one list on the menu. Othermodifications of nutrients or textures canbe added. Since no universal guideline ex-ists for consistent carbohydrate diabetesdiet ordering, it is encouraged that hospi-tal nutrition committees specify their ownordering guidelines that meet the uniqueneeds of their patients and capabilities oftheir nutrition staff.
Regardless of the type of meal plan-ning system selected, the use of mealplans such as no concentrated sweets, nosugar added, low sugar, and liberal dia-betic diets are no longer appropriate.These diets unnecessarily restrict sucroseand do not reflect the current evidence-based nutrition recommendations (433).
Special nutrition issuesLiquid diets. Sugar-free liquid diets arenot appropriate for patients with diabetes.Calories and carbohydrates are needed toprovide for normal physiologic processes.Patients given clear or full liquid dietsshould receive 200 g carbohydrate,spread equally throughout the day inmeals and snacks (428).Surgery and progression diets. Aftersurgery it is desirable to initiate feeding assoon as possible in order to protect intes-tinal integrity (428). Advancement from
Clement and Associates
DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004 575

clear liquid to full liquid to solid foodsshould be done as quickly as tolerated.Approximately 200 g carbohydrateshould be provided daily in evenly di-vided doses at meals and snacks. Duringillness and surgery, glucose requirementsincrease. Hypoglycemia can occur with-out sufficient glucose (428).
Catabolic illness and nutritionsupportDuring catabolic illness, nutritional needsare altered. Careful continuous monitor-ing of various nutrition parameters andglycemic status is essential so that nutri-tional needs are met and glycemic controlis maintained. Catabolic illness can alterfluid balance and can lead to shrinkage ofbody fat and body cell mass, making nu-trition assessment difficult. A recentweight loss of 10% indicates a need forthorough nutrition assessment. Moderateprotein-calorie malnutrition can occurwith an unintentional weight loss of 10–20%; if the loss is �20%, severe malnu-trition is likely present (430). The timeperiod over which the weight loss has oc-curred bears investigation, since a morerapid weight loss is more hazardous. Themagnitude of recent weight loss with con-sideration of the presence of excess fluidoften present in critically ill patients, thepresence or absence of clinical markers ofstress, and the amount of time the patientwill be unable to eat should determine theneed for nutrition intervention (429). Aconsultation to the registered dietitian iswarranted in these cases.
Enteral feedings have several advan-tages over parenteral feedings, includinglower costs, avoidance of catheter-relatedcomplications, the trophic effect on gas-trointestinal cells, and the more physio-logic route (429). While parenteralnutrition is necessary in certain situa-tions, it is beneficial to progress to enteraltube feedings or oral intake as soon aspossible. As with solid-food diets, theamount of carbohydrate present will havethe greatest impact on blood glucose re-sponse (428). Medications, particularlyinsulin, can be adjusted to maintain gly-cemic control based on frequent bloodglucose monitoring. The dietitian, in con-sultation with other members of the inter-disciplinary team, determines the bestmethod of feeding, the appropriate en-teral formula, and the amounts of protein,lipid, and carbohydrate in parenteral for-mulations. It is important to not overfeed
patients receiving nutrition support, asoverfeeding can exacerbate hyperglyce-mia, cause abnormal liver function tests,and increase oxygen consumption andcarbon dioxide production (429).
Nutrition guidelines for health careinstitutionsIn 1997 the “Translation of the DiabetesNutrition Recommendations for HealthCare Institutions” technical review (428)and position statement (427) were pub-lished. The position statement has beenrepublished without any substantivemodifications (433). The original paperwas based on the nutrition recommenda-tions current at that time, but both theoriginal and updated position statementsconform to the current evidence-basednutrition recommendations (430).
Discharge planningPatients with newly recognized diabetesrequire DSME during hospitalization andneed detailed discharge planning for dia-betes care. Discharge planning includesassessment of the patient’s ability to payfor diabetes supplies and medications. Ofpatients with no prior history of diabeteswho are found to have hyperglycemia(random blood glucose �125 mg/dl or6.9 mmol/l) during hospitalization, 60%are likely to have diabetes at follow-uptesting (8). For this reason, follow-uptesting for diabetes based on ADA criteria(3) is recommended within 1 month ofhospital discharge.
WHAT IS THE ROLE OFBEDSIDE GLUCOSEMONITORING IN THEHOSPITALIZED PATIENT? —Implementing intensive diabetes therapyin the hospital setting requires frequentand accurate blood glucose data. Thismeasure is analogous to an additional “vi-tal sign” for hospitalized patients with di-abetes. Bedside glucose monitoring usingcapillary blood has advantages over labo-ratory venous glucose testing because theresults can be obtained rapidly at the“point of care,” where therapeutic deci-sions are made. For this reason, the termsbedside and point-of-care glucose moni-toring are used interchangeably.
To date, no study has been conductedtesting the effect of frequency of bedsideglucose testing on the incidence of hyper-glycemia or hypoglycemia in the hospital.Without such data, recommendations are
based only on expert and consensus opin-ion. For patients who are eating, com-monly recommended testing frequenciesare premeal and at bedtime. For patientsnot eating, testing every 4–6 h is usuallysufficient for determining correction in-sulin doses. Patients controlled with con-tinuous intravenous insulin typicallyrequire hourly blood glucose testing untilthe blood glucose levels are stable, thenevery 2 h.
Bedside blood glucose testing is usu-ally performed with portable glucose de-vices that are identical or similar todevices for home self-monitoring of bloodglucose. Characteristics unique to thehospitalized patient and common to thenonhospitalized patient can lead to erro-neous bedside blood glucose testing re-sults (Table 9). Most of these errors can beprevented by implementing and main-taining a strong hospital quality-controlprogram (434,435). The impact of spe-cific interfering substances or hematocritare device-specific (436–440). Elevatedlevels of multiple interfering substancesmay alter bedside glucose results, al-though each substance, by itself, may bebelow the interference threshold specifiedby the manufacturer (441).
New bedside glucose devices allowfor identification of both patient and pro-vider by reading a unique barcode. Theglucose results can also be automaticallydownloaded into the hospital’s central labdatabase, allowing for easier access andmonitoring for quality-control purposes.Most currently used bedside glucosemeters, though designed for capillarywhole-blood testing, are calibrated to re-port results compatible to plasma, whichallows for reliable comparison to the lab-oratory glucose test. For critically ill pa-tients, hypotension, dehydration,anemia, and interfering substances in theblood may render capillary blood glucosetesting inaccurate (437). Using arterial orvenous blood with bedside glucosemeters in these situations is likely morereliable, but frequent comparison withthe laboratory glucose test is recom-mended to avoid errors in insulin ther-apy. Arterial concentrations are 5 mg/dl(0.3 mmol) higher than capillary concen-trations and 10 mg/dl (0.5 mmol)higher than venous concentrations. In thestudy by Van den Berghe et al. (2), inwhich very strict glucose targets weremaintained in critically ill patients, allglucose samples were performed with a
Management of diabetes and hyperglycemia in hospitals
576 DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004

glucose analyzer at 1- to 4-h intervals. Theuse of alternate-site glucose testing (i.e.,arm, leg, or palm) in the hospital has notbeen studied. The use of alternate-siteglucose testing may cause erroneous re-sults when the blood glucose level is rap-id ly r i s ing or fa l l ing and whenhypoglycemia occurs (442).
As with any procedure handlingblood, protective glove use is essential forhealth care personnel performing bedsideglucose monitoring. The use of self-retracting lancet devices has the potentialto eliminate the chance of needlestick in-jury and risk for infection. Table 10 out-lines specific elements of a quality-controlprogram deemed to be necessary for ap-propriate use of bedside blood glucosetesting in the hospital (443). Key partici-pants in the program are clinical labora-tory representatives, nurses, physicians,and hospital administrators. Additionalguidelines are published by the NationalCommittee for Clinical Laboratory Stan-dards (444). For patients practicing dia-betes self-management in the hospital, aquality-control program to test the pa-tient’s blood glucose device and the pa-tient’s testing technique is necessary toensure accurate results.
IS IMPROVED DIABETESCARE IN HOSPITALS COSTEFFECTIVE? — Of the $91.8 billionspent annually in the U.S. for direct med-ical expenditures for diabetes, hospitalcare accounts for the single largest com-ponent of expenditures, comprising $40billion, or 43.9%, of the total cost (445).After adjustment for age, sex, and race/ethnicity, annual per capita costs for hos-pital care is $6,309 for persons withdiabetes versus $2,971 for persons with-
out diabetes—a cost ratio of 2.1. Similarincreased hospital-related cost for dia-betic patients is reported in Europe (446).This increased cost for hospital care is dueto increased frequency of hospital admis-sions (447), increased length of stay, andincreased cost per hospital day due tohigher utilization of intensive care andprocedures (448).
Furnary and colleagues (196,290)performed a cost-effectiveness analysisfollowing implementation of a continu-ous intravenous insulin infusion programfor the first 3 days after cardiac surgicalprocedures in diabetic patients. Com-pared with historical control subjects, theincidence of deep sternal wound infec-tions (DSWIs) was reduced from 1.9 to0.8%, and mortality from DSWIs reduceddecreased from 19 to 3.8% after imple-mentation of the protocol. The averageexcess length of stay from DSWI was 16days, generating an average $26,400 inadditional hospital charges. Furnary et al.(449) estimated the additional expense ofinsulin infusion at $125–150 per patient.Of 1,499 patients in the interventiongroup, the number of DWSIs preventedwas 10, resulting in an average cost toprevent one DSWI at approximately$21,000. This estimate does not incorpo-rate the potential effects of the interven-tion on other outcomes, such as areduction in mortality, cost for chroniccare, and lost income from work.
Van den Berghe et al. (2) reported a34% reduction in hospital mortality incritically ill patients treated with intensiveinsulin therapy. Intensive insulin therapyreduced the duration of intensive care butnot the overall length of stay in the hospi-tal. Subsequent comparison of costs be-tween the groups for rehabilitation,
chronic care, home care, or loss of wagesdue to illness or mortality has not as yetbeen reported.
Levetan et al. (379) reported the im-pact of obtaining an endocrinology con-sultation, either alone or as part ofmultidisciplinary diabetes team (endocri-nologist, diabetes nurse educator, and aregistered dietitian), on hospital length ofstay in patients admitted with the princi-pal diagnosis of diabetes, including hy-perosmolar state, diabetic ketoacidosis,and uncontrolled diabetes. In this non-randomized observational study, the av-erage length of stay of the diabetes teampatients was 3.6 � 1.7 days as comparedwith 8.2 � 6.2 days for patients in theno-consultation group and 5.5 � 3.4 daysfor the patients who received a traditionalindividual endocrine consultation. Possi-ble reasons for shortened length of staywere more rapid normalization of glucoselevels, more efficient transition from in-travenous to subcutaneous insulin, fastertransition to a definitive insulin or oralmedication regimen, and more effectiveteaching of diabetes survival skills. Esti-mated cost savings from reduction inlength of stay for the 34 patients seen bythe diabetes team was $120,000 com-pared with the cost in salaries of $40,000.
In summary, the potential opportu-nity for cost savings from improved hos-pital outcomes, reduced mortality, andshortened length of stay for patients withdiabetes and hospital-related hyperglyce-mia is substantial. Future studies usingrandomized prospective design areneeded to verify these results.
SUGGESTIONS FOR FUTURERESEARCH — While outcomes stud-ies that provide evidence for a clear role
Table 9—Conditions causing erroneous bedside blood glucose results
Sources of analytical error Sources of user error
Low hematocrit* Inadequate meter calibrationHigh hematocrit† Using a test strip that does not match the meter code or that has
passed the expiration dateShock and dehydration‡ Inadequate quality-control testingHypoxia‡ Poor meter maintenanceHyperbilirubinemia, severe lipemia* Poor technique in performing fingerprickSpecimen additives: sodium flouride† Poor technique of applying drop of blood to the test stripDrugs—acetaminophen overdose, ascorbic acid,
dopamine, fluorescein, mannitol, salicylate‡Failure to record results in patient’s chart or to take action if
blood glucose is out of target range
*Falsely elevates result; †falsely lowers result; ‡can either falsely lower or elevate result, depending on the device used.
Clement and Associates
DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004 577

for targeted glucose control in the hospi-tal management of diabetes are beginningto accumulate in the scientific literature,numerous questions related to how tobest manage diabetes in this hospital set-ting remain to be addressed. These ques-tions may be grouped into three mainareas: health care outcomes attributableto glycemic control, specific strategies forinsulin delivery, and processes for opti-mizing diabetes care and education in thehospital setting.
Health care outcomes related toglycemic controlFew studies in the literature contain ran-domized, controlled evidence to supportspecific interventions that target glucosecontrol in various clinical settings. Workis clearly needed to provide rigorous evi-dence in the hospital management of dia-betes in order to:
● Further define the role of targeted glu-cose control and the threshold for im-pact of blood glucose level on healthcare outcomes in diverse clinical set-tings, such as general medicine and sur-gery pa t i en t s , and in spec ificcircumstances, such as stroke, neuro-surgery, and CVDs
● Examine clinical outcomes● Examine health care economic out-
comes such as length of stay and costeffectiveness
● Further examine the impact of special-ist care and diabetes team management
● Define the impact of diabetes educa-tion.
Specific strategies for insulindeliveryDevelopment and implementation of spe-cific strategies for insulin delivery, basedon knowledge of the pharmacokinetics ofthe currently available insulins, will allowphysicians and nurses to overcome barri-ers to its effective use in managing bloodglucose. Such strategies will need to dem-onstrate safety and efficacy of specific ap-plications of insulin therapies thataddress known areas of need, including:
● Optimum methods for delivering basalinsulin under various clinical condi-tions
● Feasibility of using subcutaneousglargine or detemir insulin to meetbasal insulin requirements (e.g., formedicine services) in the operating
Table 10—Characteristics of an effectivebedside glucose monitoring (BGM) quality-control program
Characteristic
● A specifically designated responsibleindividual, preferably a laboratoryprofessional, is involved in theadministration and quality assurance ofthe BGM program.
● A written procedure for the BGMprogram.
● An organized training program thatinvolves laboratory personnel andnursing staff.
● Defined frequencies and requirements formaintenance and cleaning of BGMinstruments.
● Regular performance of quality controltesting on each instrument (daily or byshift), depending on the frequency ofpatient testing.
● A policy to regularly compare the BGMresults from each operator andinstrument with results from acorresponding sample tested in theclinical laboratory. Suggest that all BGMresults are, at least, within �15%variation from the clinical laboratoryresults.
● Participation in an external proficiencytesting program.
● Acknowledgment of the limitations ofBGM and requirement of a clinicallaboratory glucose determination when aBGM result is outside a defined range.
● Acknowledgment of the effect ofhematocrit value variation on BGMresults and establishment of hematocritvalue limitations for the instrument inuse.
● Determination of the bias of theinstrument in use and communication ofthis information to the physicians and theinstitutional quality assurance program.
Adapted from Jones et al. (443).
Table 11—Summary of major recommendations for hospital management of hyperglycemia
RecommendationLevel of
evidence
● Good metabolic control is associated with improved hospital outcomes. Targetplasma glucose levels are:
B
•�110 mg/dl preprandial and �180 mg/dl peak postprandial.● Intensive insulin therapy with intravenous insulin, with the goal of
maintaining blood glucose 80–110 mg/dl, reduces morbidity and mortalityamong critically ill patients in the surgical ICU.
A
● Intravenous insulin infusion is safe and effective for achieving metaboliccontrol during major surgery, hemodynamic instability, and NPO status.
B
● Intravenous insulin infusion is safe and effective for patients who have poorlycontrolled diabetes and widely fluctuating blood glucose levels or who areinsulin deficient or severely insulin resistant.
B
● Intravenous insulin infusion, followed by multidose subcutaneous insulintherapy, improves survival in diabetic patients after myocardial infarction.
A
● For insulin-deficient patients, despite reductions or the absence of caloricintake, basal insulin must be provided to prevent diabetic ketoacidosis.
B
● Use of scheduled insulin improves blood glucose control compared withorders based on sliding scale insulin coverage alone.
B
● For patients who are alert and demonstrate accurate insulin self-administrationand glucose monitoring, insulin self-management should be allowed as anadjunct to standard nurse-delivered diabetes management.
E
● Patients with no prior history of diabetes who are found to have hyperglycemia(random blood glucose �125 mg/dl or 6.9 mmol/l) during hospitalizationshould have follow-up testing for diabetes within 1 month of hospitaldischarge.
E
● Establishing a multidisciplinary team that sets and implements institutionalguidelines, protocols, and standardized order sets for the hospital results inreduced hypoglycemic and hyperglycemic events.
B
● Diabetes education, medical nutrition therapy, and timely diabetes-specificdischarge planning are essential components of hospital-based diabetes care.
C
Management of diabetes and hyperglycemia in hospitals
578 DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004

room and for periprocedural manage-ment
● The role of standardization of diabetesmanagement and algorithmic care andvalidation of such pathways and tools
● Safety and practicality of delivering in-sulin infusion therapy outside the in-tensive care unit
● Simple algorithms for subcutaneousdelivery of programmed basal, prandi-al/nutritional, and correction doses ofinsulin and insulin infusion algorithms.
Improved methods for glucosemonitoringCurrent methods for blood glucose mon-itoring are painful and time consuming.Improved methods for frequent and accu-rate blood glucose monitoring would en-hance the ability to reach target bloodglucose levels safely. Development of con-tinuous glucose monitoring systems thatare safe and accurate is encouraged.
Processes for optimizing diabetescare and education in the hospitalsettingBecause diabetes is seen in a broad spec-trum of inpatients, processes need to bedefined and tested to enable safe and ef-fective patient management and optimi-zation of outcomes. Areas of interestinclude:
● Strategies adopted by institutions to re-duce errors, enhance safety, and im-prove quality of care
● Development and implementation ofnursing policies effective for hypogly-cemia prevention
● Impact of institutional hypoglycemiaprograms on willingness of physiciansto prescribe insulin to adequately con-trol hyperglycemia
● Whether correlation exists between in-stitutional adherence to clinical path-ways and algorithms and outcomes
● Most appropriate CQI measures forevaluation of performance in achievingglycemic control
● Most appropriate focus for regulatoryorganizations such as JCAHO.
CONCLUSIONS — Hyperglycemiais associated with poor hospital out-comes. The key question for guiding ther-apy is whether hyperglycemia observed inthe hospital is a simple marker for theunderlying disease state (i.e., diabetes) or
the severity of illness or if hyperglycemiaitself, in conjunction with relative hypo-insulinemia, is pathogenic for tissue in-jury and poor hospital outcomes. Basedon limited interventional studies in se-lected settings, aggressive control ofblood glucose in the hospital may providean opportunity to improve patient out-comes. Clinical trials are needed to an-swer these questions. The target bloodglucose threshold to optimize outcomesin the hospital is not clearly defined butmay be lower than previously thought.From a cost perspective, research andstrategies targeting glucose control anddiabetes care in the hospital have thepotential to translate to substantial costsavings.
Acknowledgments— Support for this Tech-nical Review was provided by an unrestrictededucational grant from Novo Nordisk.
The authors thank the members of the ADAProfessional Practice Committee for theirthoughtful review of the manuscript. The au-thors also thank Drs. James Lenhard and Ste-phen Hodak for their helpful comments.
References1. Umpierrez GE, Isaacs SD, Bazargan N,
You X, Thaler LM, Kitabchi AE: Hyper-glycemia: an independent marker of in-hospital mortality in patients withundiagnosed diabetes. J Clin EndocrinolMetab 87:978–982, 2002
2. Van den Berghe G, Wouters P, WeekersF, VerWaest C, Bruyninckx F, Schetz M,Vlasselaers D, Ferdinande P, Lauwers P,Bouillon R: Intensive insulin therapy incritically ill patients. N Engl J Med 345:1359–1367, 2001
3. The Expert Committee on the Diagnosisand Classification of Diabetes Mellitus:Report of the Expert Committee on theDiagnosis and Classification of DiabetesMellitus. Diabetes Care 26 (Suppl. 1):S5–S20, 2003
4. Tierney E: Data from the National Hos-pital Discharge Survey Database 2000,Center of Disease Control and Preven-tion, Division of Diabetes Translation,Atlanta, GA, 2003. Personal communi-cation
5. Jencks SF: Accuracy in recorded diag-noses. JAMA 267:2238–2239, 1992
6. Levetan CS, Passaro M, Jablonski K, KassM, Ratner RE: Unrecognized diabetesamong hospitalized patients. DiabetesCare 21:246–249, 1998
7. Norhammar A, Tenerz A, Nilsson G,Hamsten A, Efendic S, Ryden L, Malm-berg K: Glucose metabolism in patients
with acute myocardial infarction and noprevious diagnosis of diabetes mellitus: aprospective study. Lancet 359:2140–2144, 2002
8. Greci LS, Kailasam M, Malkani S, KatzDL, Hulinsky I, Ahmadi R, Nawaz H:Utility of HbA1c levels for diabetes casefinding in hospitalized patients with hy-perglycemia. Diabetes Care 26:1064–1068, 2003
9. Aubert R, Geiss L, Ballard D, Coca-nougher B, Herman W: Diabetes-RelatedHospitalization and Hospital Utilization.2nd ed. Bethesda, MD, National Insti-tutes of Health, 1995, p. 555–556
10. Joshi N, Caputo G, Weitekamp M,Karchmer A: Infections in patients withdiabetes mellitus. N Engl J Med 341:1906–1912, 1999
11. Wheat L: Infection and diabetes melli-tus. Diabetes Care 3:187–197, 1980
12. Mowat A, Baum J: Chemotaxis of poly-morphonuclear leukocytes from pa-tients with diabetes mellitus. N EnglJ Med 284:621–627, 1971
13. Bagdade J, Root R, Bulger R: Impairedleukocyte function in patients withpoorly controlled diabetes. Diabetes 23:9–15, 1974
14. Bagdade JD, Stewart M, Walters E: Im-paired granulocyte adherence. A revers-ible defect in host defense in patientswith poorly controlled diabetes. Diabetes27:677–681, 1978
15. van Oss CJ, Border JR: Influence of in-termittent hyperglycemic glucose levelson the phagocytosis of microorganismsby human granulocytes in vitro. Immu-nol Commun 7:669–676, 1978
16. Davidson N, Sowden J, Fletcher J: Defec-tive phagocytosis in insulin-controlleddiabetics: evidence for a reaction be-tween glucose and opsonizing proteins.J Clin Pathol 37:783–786, 1984
17. Alexiewicz J, Kumar D, SmogorzewskiM, Klin M, Massry S: Polymorphonu-clear leukocytes in non-insulin-depen-dent diabetes mellitus: abnormalities inmetabolism and function. Ann InternMed 123:919–924, 1995
18. Leibovici L, Yehezkelli Y, Porter A, RegevA, Krauze I, Harrell D: Influence of dia-betes mellitus and glycemic control onthe characteristics and outcome of com-mon infections. Diabet Med 13:457–463, 1996
19. Kwoun M, Ling P, Lydon E, Imrich A,Qu Z, Palombo J, Bistrian. B: Immuno-logic effects of acute hyperglycemia innondiabetic rats. J Parenter Enteral Nutr21:91–95, 1997
20. McManus L, Bloodworth R, Prihoda T,Blodgett J, Pinckard R: Agonist-depen-dent failure of neutrophil function indiabetes correlates with extent of hyper-glycemia. J Leukocyte Biol 70:395–404,
Clement and Associates
DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004 579

200121. MacRury S, Gemmell C, Paterson K,
MacCush A: Changes in phagocyticfunction with glycaemic control in dia-betic patients. J Clin Pathol 42:1143–1147, 1989
22. Rassias A, Marrin C, Arruda J, Whalen P,Beach M, Yeager M: Insulin infusion im-proved neutrophil function in diabeticcardiac surgery patients. Anesth Analg88:1011–1016, 1999
23. Rassias A, Givan A, Marrin C, Whalen K,Pahl J, Yeager M: Insulin increases neu-trophil count and phagocytic capacityafter cardiac surgery. Anesth Analg 94:1113–1119, 2002
24. Repine J, Clawson C, Goetz F: Bacteri-cidal function of neutrophils from pa-tients with acute bacterial infections andfrom diabetes. J Infect Dis 142:869–875,1980
25. Nielson C, Hindson D: Inhibition ofpolymorphonuclear leukocyte respira-tory burst by elevated glucose concentra-tions in vitro. Diabetes 38:1031–1035,1989
26. Wilson RM, Reeves WG: Neutrophilphagocytosis and killing in insulin-de-pendent diabetes. Clin Exp Immunol 63:478–484, 1986
27. Sheetz M, King G: Molecular under-standing of hyperglycemia’s adverse ef-fects for diabetic complications. JAMA288:2579–2588, 2002
28. Oldenborg P, Sehlin J: Hyperglycemia invitro attenuates insulin-stimulated che-mokinesis in normal human neutro-phils: role of protein kinase C activation.J Leukocyte Biol 65:635–640, 1999
29. Liu BF, Miyata S, Kojima H, Uriuhara A,Kusunoki H, Suzuki K, Kasuga M: Lowphagocytic activity of resident peritonealmacrophages in diabetic mice: relevanceto the formation of advanced glycationend products. Diabetes 48:2074–2082,1999
30. Ortmeyer J, Mohsenin V: Inhibition ofphospholipase D and superoxide gener-ation by glucose in diabetic neutrophils.Life Sciences 59:255–262, 1996
31. Perner A, Nielsen S, Rask-Madsen J:High glucose impairs superoxide pro-duction from isolated blood neutrophils.Intensive Care Med 29:642–645, 2003
32. Sato N, Kashima K, Ohtani K, ShimizuH, Mori M: Epalrestat, an aldose reduc-tase inhibitor, improves an impairedgeneration of oxygen-derived free radi-cals by neutrophils from poorly con-trolled NIDDM patients. Diabetes Care20:995–998, 1997
33. Boland O, Blackwell C, Clarke B, EwingD: Effects of ponalrestat, an aldose re-ductase inhibitor, on neutrophil killingof Escherichia coli and autonomic func-tion in patients with diabetes mellitus.
Diabetes 42:336–340, 199334. Mazade MA, Edwards MS: Impairment
of type III group B Streptococcus-stimu-lated superoxide production and op-sonophagocytosis by neutrophils indiabetes. Mol Genet Metab 73:259–267,2001
35. Black CT, Hennessey PJ, Andrassy RJ:Short-term hyperglycemia depresses im-munity through nonenzymatic glycosyl-ation of circulating immunoglobulin.J Trauma 30:830–832; discussion 832–833, 1990
36. von Kanel R, Mills P, Dimsdale J: Short-term hyperglycemia induces lympho-penia and lymphocyte subset redistri-bution. Life Sciences 69:255–262, 2001
37. Bouter KP, Meyling FH, Hoekstra JB,Masurel N, Erkelens DW, DieperslootRJ: Influence of blood glucose levels onperipheral lymphocytes in patients withdiabetes mellitus. Diabetes Res 19:77–80, 1992
38. Kersten J, Schmeling T, Orth K, Pagel P,Warltier D: Acute hyperglycemia abol-ishes ischemic preconditioning in vivo.Am J Physiol 275:H721–H725, 1998
39. Kersten J, Toller W, Tessmer J, Pagel P,Warltier D: Hyperglycemia reduces cor-onary collarteral blood flow through anitric oxide-mediated mechanism. Am JPhysiol 281:H2097–H2104, 2001
40. Ceriello A, Quagliaro L, D’Amico M, DiFilippo C, Marfella R, Nappo F, BerrinoL, Rossi F, Giugliano D: Acute hypergly-cemia induces nitrotyrosine formationand apoptosis in perfused heart from rat.Diabetes 51:1076–1082, 2002
41. Verma S, Maitland A, Weisel R, Li S,Fedak P, Pomroy N, Mickle D, Li R, KoL, Rao V: Hyperglycemia exaggeratesischemia-reperfusion-induced cardio-myocyte injury: reversal with endothelinantagonism. J Thorac Cardiovasc Surg123:1120–1124, 2002
42. D’Amico M, Marfella R, Nappo F, Di Fil-ippo C, De Angelis L, Berrino L, Rossi F,Giugliano D: High glucose induces ven-tricular instability and increases vaso-motor tone in rats. Diabetologia 44:464–470, 2001
43. Marfella R, Nappo F, Angelis LD, Pa-olisso G, Tagliamonte M, Giugliano D:Hemodynamic effects of acute hypergly-cemia in type 2 diabetic patients. Diabe-tes Care 23:658–663, 2000
44. Marfella R, Nappo F, Angelis LD, Sinis-calshi M, Rossi F, Giugliano D: The effectof acute hyperglycaemia on QTc dura-tion in healthy man. Diabetologia43:571–575, 2000
45. Cinar Y, Senyol A, Duman K: Blood vis-cosity and blood pressure: role of tem-perature and hyperglycemia. AmericanJ Hypertens 14:433–438, 2001
46. McKenna K, Smith D, Tormey W,
Thompson C: Acute hyperglycaemiacauses elevation in plasma atrial natri-uretic peptide concentrations in type 1diabetes mellitus. Diabet Med 17:512–517, 2000
47. Davi G, Catalano I, Averna M, Notarbar-tolo A, Strano A, Ciabattoni G, PatronoC: Thromboxane biosynthesis and plate-let function in type II diabetes mellitus.N Engl J Med 322:1769–1774, 1990
48. Knobler H, Savion N, Shenkman B,Kotev-Emeth S, Varon D: Shear-inducedplatelet adhesion and aggregation onsubendothelium are increased in dia-betic patients. Thromb Res 90:181–190,1998
49. Davi G, Ciabattoni G, Consoli A, Mez-zetti A, Falco A, Santarone S, Pennese E,Vitacolonna E, Bucciarelli T, CostantiniF, Capani F, Patrono C: In vivo forma-tion of 8-iso-prostaglandin f2alpha andplatelet activation in diabetes mellitus:effects of improved metabolic controland vitamin E supplementation. Circula-tion 99:224–229, 1999
50. Sakamoto T, Ogawa H, Kawano H, HiraiN, Miyamoto S, Takazoe K, Soejima J,Kugiyama K: Rapid change of plateletaggregability in acute hyperglycemia.Detection by a novel laser-light scatter-ing method. Thrombosis & Hemostasis83:475–479, 2000
51. Gresele P, Guglielmini G, DeAngelis M,Ciferri S, Ciofetta M, Falcinelli E, Lalli C,Ciabattoni G, Davi G, Bolli G: Acute,short-term hyperglycemia enhancesshear stress-induced platelet activationin patients with type II diabetes mellitus.J Am Coll Cardiol 41:1013–1020, 2003
52. Pandolfi A, Giaccari A, Cilli C, alberta M,Morviducci L, Filippis ED, BuongiornoA, Pellegrini G, Capani F, Consoli A:Acute hyperglycemia and acute hyperin-sulinemia decrease plasma fibrinolyticactivity and increase plaminogen activa-tor inhibitor type 1 in the rat. Acta Dia-betologica 38:71–77, 2001
53. Morohoshi M, Fujisawa K, Uchimura I,Numano F: Glucose-dependent inter-leukin 6 and tumor necrosis factor pro-duction by human peripheral bloodmonocytes in vitro. Diabetes 45:954–959, 1996
54. Kado S, Nagase T, Nagata N: Circulatinglevels of interleukin-6, its soluble recep-tor and interleukin-6/interleukin-6 re-ceptor complexes in patients with type 2diabetes mellitus. Acta Diabetol 36:67–72, 1999
55. Mohamed-Ali V, Goodrick S, Rawesh A,Katz DR, Miles JM, Yudkin JS, Klein S,Coppack SW: Subcutaneous adipose tis-sue releases interleukin-6, but not tumornecrosis factor-alpha, in vivo. J Clin En-docrinol Metab 82:4196–4200, 1997
56. Pampfer S, Vanderheyden I, De Hertogh
Management of diabetes and hyperglycemia in hospitals
580 DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004

R: Increased synthesis of tumor necrosisfactor-� in uterine explants from preg-nant diabetic rats and in primary cul-tures of uterine cells in high glucose.Diabetes 46:1214–1224, 1997
57. Meldrum DR, Donnahoo KK: Role ofTNF in mediating renal insufficiency fol-lowing cardiac surgery: evidence of apostbypass cardiorenal syndrome. J SurgRes 85:185–199, 1999
58. Guha M, Bai W, Nadler JL, Natarajan R:Molecular mechanisms of tumor necro-sis factor alpha gene expression inmonocytic cells via hyperglycemia-in-duced oxidant stress-dependent and -in-dependent pathways. J Biol Chem 275:17728–17739, 2000
59. Hattori Y, Hattori S, Sato N, Kasai K:High-glucose-induced nuclear factorkappaB activation in vascular smoothmuscle cells. Cardiovasc Res 46:188–197, 2000
60. Coughlan MT, Oliva K, Georgiou HM,Permezel JM, Rice GE: Glucose-inducedrelease of tumour necrosis factor-alphafrom human placental and adipose tis-sues in gestational diabetes mellitus.Diabet Med 18:921–927, 2001
61. Lin Y, Rajala MW, Berger JP, Moller DE,Barzilai N, Scherer PE: Hyperglycemia-induced production of acute phase reac-tants in adipose tissue. J Biol Chem 276:42077–42083, 2001
62. Esposito K, Nappo F, Marfella R, Giugli-ano G, Giugliano F, Ciotola M, Quagli-aro L, Ceriello A, Giugliano D: Inflam-matory cytokine concentrations areacutely increased by hyperglycemia inhumans: role of oxidative stress. Circu-lation 106:2067–2072, 2002
63. Li D, Zhao L, Liu M, Du X, Ding W,Zhang J, Mehta JL: Kinetics of tumor ne-crosis factor alpha in plasma and the car-dioprotective effect of a monoclonalantibody to tumor necrosis factor alphain acute myocardial infarction. AmHeart J 137:1145–1152, 1999
64. Das UN: Free radicals, cytokines and ni-tric oxide in cardiac failure and myocar-dial infarction. Mol Cell Biochem 215:145–152, 2000
65. Ferrari R: Tumor necrosis factor in CHF:a double facet cytokine. Cardiovasc Res37:554–559, 1998
66. Meldrum DR, Dinarello CA, Shames BD,Cleveland JC, Jr., Cain BS, Banerjee A,Meng X, Harken AH: Ischemic precon-ditioning decreases postischemic myo-cardial tumor necrosis factor-alphaproduction: potential ultimate effectormechanism of preconditioning. Circula-tion 98:II214–II218; discussion II218–II219, 1998
67. Mallat Z, Corbaz A, Scoazec A, BesnardS, Leseche G, Chvatchko Y, Tedgui A:Expression of interleukin-18 in human
atherosclerotic plaques and relation toplaque instability. Circulation 104:1598–1603, 2001
68. Romeo G, Liu W, Asnaghi V, Kern T,Lorenzi M: Activation of nuclear fac-tor-�B induced by diabetes and highglucose regulates a proapoptotic pro-gram in retinal pericytes. Diabetes 51:2241–2248, 2002
69. Nishikawa T, Edelstein D, Brownlee M:The missing link: a single unifyingmechanism for diabetic complications.Kidney Int Suppl 77:S26–S30, 2000
70. Yerneni KK, Bai W, Khan BV, MedfordRM, Natarajan R: Hyperglycemia-in-duced activation of nuclear transcriptionfactor �B in vascular smooth musclecells. Diabetes 48:855–864, 1999
71. Morigi M, Angioletti S, Imberti B, Don-adelli R, Micheletti G, Figliuzzi M, Re-muzzi A, Zoja C, Remuzzi G: Leukocyte-endothelial interaction is augmented byhigh glucose concentrations and hyper-glycemia in a NF-kB-dependent fashion.J Clin Invest 101:1905–1915, 1998
72. Hofmann MA, Schiekofer S, Kanitz M,Klevesath MS, Joswig M, Lee V, MorcosM, Tritschler H, Ziegler R, Wahl P, Bier-haus A, Nawroth PP: Insufficient glyce-mic control increases nuclear factor-�Bbinding activity in peripheral bloodmononuclear cells isolated from patientswith type 1 diabetes. Diabetes Care 21:1310–1316, 1998
73. Schiekofer NM, Andrassy M, Chen J, Ru-dofsky G, Schneider J, Wendt T, StefanN, Humpert P, Fritsche A, Stumvoll M,Schleicher E, Haring H, Nawroth P, Bier-haus A: Acute hyperglycemia causes in-tracellular formation of CML andactivation of ras, p42/44 MAPK, and nu-clear factor-�B in PBMCs. Diabetes 52:621–633, 2003
74. Marfella R, Quagliaro L, Nappo F, Ceri-ello A, Giugliano D: Acute hypergly-cemia induces an oxidative stress inhealthy subjects. J Clin Invest 108:635–636, 2001
75. Calles-Escandon J, Cipolla M: Diabetesand endothelial dysfunction: a clinicalperspective. Endocr Rev 22:36–52, 2001
76. Goligorsky MS, Chen J, Brodsky S:Workshop: endothelial cell dysfunctionleading to diabetic nephropathy: focuson nitric oxide. Hypertension 37:744–748, 2001
77. Williams S, Goldfine A, Timimi F, TingH, Roddy M, Simonson D, Roddy M,Simonson D, Creager M: Acute hyper-glycemia attenuates endothelium-depen-dent vasodilation in humans in vivo.Circulation 97:1695–1701, 1998
78. Kawano H, Motoyama T, Hirashima O,Hirai N, Miyao Y, Sakamoto T, Kugiy-ama K, Ogawa H, Yasue H: Hyperglyce-mia rapidly suppresses flow-mediated
endothelium-dependent vasodilation ofbrachial artery. J Am Coll Cardiol34:146–154, 1999
79. Shige H, Ishikawa T, Suzukawa M, Ito T,Nakajima K, Higashi K, Ayaori M, Ta-bata S, Ohsuzu F, Nakamura H: Endo-thelium-dependent flow-mediated vaso-dilation in the postprandial state in type2 diabetes mellitus. Am J Cardiol 84:1272–1274, A1279, 1999
80. Title LM, Cummings PM, Giddens K,Nassar BA: Oral glucose loading acutelyattenuates endothelium-dependent va-sodilation in healthy adults without dia-betes: an effect prevented by vitamins Cand E. J Am Coll Cardiol 36:2185–2191,2000
81. Beckman J, Goldfine A, Gordon M,Creager M: Ascorbate restores endothe-lium-dependent vasodilation impairedby acute hyperglycemia in humans. Cir-culation 103:1618–1623, 2001
82. Giugliano D, Marfella R, Coppola L, Ver-razzo G, Acampora R, Giunta R, NappoF, Lucarelli C, D’Onofrio F: Vascular ef-fects of acute hyperglycemia in humansare reversed by L-arginine: evidence forreduced availability of nitric oxide dur-ing hyperglycemia. Circulation 95:1783–1790, 1997
83. Bagg W, Whalley G, Sathu A, Gamble G,Sharpe N, Braatvedt G: The effect ofacute hyperglycaemia on brachial arteryflow mediated dilatation in normal vol-unteers. Austral NZ J Med 30:344–350,2000
84. Brodsky SV, Morrishow AM, Dharia N,Gross SS, Goligorsky MS: Glucose scav-enging of nitric oxide. Am J Physiol RenalPhysiol 280:F480–F486, 2001
85. Myers RE, Yamaguchi S: Nervous systemeffects of cardiac arrest in monkeys:preservation of vision. Arch Neurol 34:65–74, 1977
86. Pulsinelli WA, Waldman S, RawlinsonD, Plum F: Moderate hyperglycemiaaugments ischemic brain damage: a neu-ropathologic study in the rat. Neurology32:1239–1246, 1982
87. Prado R, Ginsberg MD, Dietrich WD,Watson BD, Busto R: Hyperglycemiaincreases infarct size in collaterally per-fused but not end-arterial vascular terri-tories. J Cereb Blood Flow Metab 8:186–192, 1988
88. Huang N, Wei J, Quast M: A comparisonof the early development of ischemicbrain dmage in normoglycemic and hy-perglycemic rats using magnetic reso-nance imaging. Experimental BrainResearch 109:33–42, 1996
89. Li PA, Kristian T, Shamloo M, Siesjo K:Effects of preischemic hyperglycemia onbrain damage incurred by rats subjectedto 2.5 or 5 minutes of forebrain isch-emia. Stroke 27:1592–1601; discussion
Clement and Associates
DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004 581

1601–1592, 199690. Kawai N, Keep RF, Betz AL, Nagao S:
Hyperglycemia induces progressivechanges in the cerebral microvasculatureand blood-brain barrier transport dur-ing focal cerebral ischemia. Acta Neuro-chir Suppl. (Wien) 71:219–221, 1998
91. Kawai N, Keep R, Betz A: Hyperglycemiaand the vascular effects of cerebral isch-emia. Acta Neurochirugica - Supplemen-tum 70:27–29, 1997
92. Lin B, Ginsberg M, Busto R: Hyperglyce-mic exacerbation of neuronal damagefollowing forebrain ischemia: microglial,astrocytic and endothelial alterations.Acta Neuropathologica 96:610–620, 1998
93. Gisselsson L, Smith M, Siesjo B: Hyper-glycemia and focal brain ischemia.J Cereb Blood Flow Metab 19:288–297,1999
94. Hoxworth JM, Xu K, Zhou Y, Lust WD,LaManna JC: Cerebral metabolic profile,selective neuron loss, and survival ofacute and chronic hyperglycemic ratsfollowing cardiac arrest and resuscita-tion. Brain Res 821:467–479, 1999
95. Li P, Shuaib A, Miyashita H, He Q, SiesjoB, Warner D: Hyperglycemia enhancesextracellular glutamate accumulation inrats subjected to forebrain ischemia.Stroke 31:183–192, 2000
96. Capes S, Hunt D, Malmberg K, Pathak P,Gerstein H: Stress hyperglycemia andprognosis of stroke in nodiabetic and di-abetic patients: a systematic overview.Stroke 32:2426–2432, 2001
97. Park WS, Chang YS, Lee M: Effects ofhyperglycemia or hypoglycemia onbrain cell membrane function and en-ergy metabolism during the immediatereoxygenation-reperfusion period afteracute transient global hypoxia-ischemiain the newborn piglet. Brain Res 901:102–108, 2001
98. Rytter A, Cronberg T, Asztely F, NemaliS, Wieloch T: Mouse hippocampal orga-notypic tissue cultures exposed to invitro “ischemia” show selective and de-layed CA 1 damage that is aggravated byglucose. J Cereb Blood Flow Metab 23:23–33, 2003
99. Ginsberg MD, Prado R, Dietrich WD,Busto R, Watson BD: Hyperglycemia re-duces the extent of cerebral infarction inrats. Stroke 18:570–574, 1987
100. Sieber FE: The neurologic implicationsof diabetic hyperglycemia during surgi-cal procedures at increased risk for brainischemia. J Clin Anesth 9:334–340, 1997
101. Venables GS, Miller SA, Gibson G,Hardy JA, Strong AJ: The effects of hy-perglycaemia on changes during reper-fusion following focal cerebral ischaemiain the cat. J Neurol Neurosurg Psychiatry48:663–669, 1985
102. Anderson RE, Tan WK, Martin HS,
Meyer FB: Effects of glucose and PaO2modulation on cortical intracellular aci-dosis, NADH redox state, and infarctionin the ischemic penumbra. Stroke 30:160–170, 1999
103. Kraig RP, Petito CK, Plum F, PulsinelliWA: Hydrogen ions kill brain at concen-trations reached in ischemia. J CerebBlood Flow Metab 7:379–386, 1987
104. Petito CK, Kraig RP, Pulsinelli WA: Lightand electron microscopic evaluation ofhydrogen ion-induced brain necrosis.J Cereb Blood Flow Metab 7:625–632,1987
105. Guyot LL, Diaz FG, O’Regan MH, SongD, Phillis JW: The effect of streptozoto-cin-induced diabetes on the release ofexcitotoxic and other amino acids fromthe ischemic rat cerebral cortex. Neuro-surgery 48:385–390; discussion 390–381, 2001
106. Schurr A, Payne RS, Miller JJ, Tseng MT:Preischemic hyperglycemia-aggravateddamage: evidence that lactate utilizationis beneficial and glucose-induced corti-costerone release is detrimental. J Neuro-sci Res 66:782–789, 2001
107. Christensen H, Boysen G: Blood glucoseincreases early after stroke onset: a studyon serial measurements of blood glucosein acute stroke. Eur J Neurol 9:297–301,2002
108. Ishii H, Arai T, Segawa H, Morikawa S,Inubushi T, Fukuda K: Effects of propo-fol on lactate accumulation and oedemaformation in focal cerebral ischaemia inhyperglycaemic rats. Br J Anaesth 88:412–417, 2002
109. Parsons MW, Li T, Barber PA, Yang Q,Darby DG, Desmond PM, Gerraty RP,Tress BM, Davis SM: Combined (1)H MRspectroscopy and diffusion-weightedMRI improves the prediction of strokeoutcome. Neurology 55:498–505, 2000
110. Parsons M, Barber P, Desmond P, BairdT, Darby D, Byrnes G, Tress B, Davis S:Acute hyperglycemia adversely affectsstroke outcome: a magnetic resonanceimaging and spectroscopy study. AnnNeurol 52:20–28, 2002
111. Dietrich WD, Alonso O, Busto R: Mod-erate hyperglycemia worsens acuteblood-brain barrier injury after fore-brain ischemia in rats. Stroke 24:111–116, 1993
112. Els T, Rother J, Beaulieu C, de CrespignyA, Moseley M: Hyperglycemia delaysterminal depolarization and enhancesrepolarization after peri-infarct spread-ing depression as measured by serial dif-fusion MR mapping. J Cereb Blood FlowMetab 17:591–595, 1997
113. Li P, Rasquinha I, He Q, Siesjo B, CsiszarK, Boyd C, MacManus J: Hyperglycemiaenhances DNA fragmentation after tran-sient cerebral ischemia. J Cereb Blood
Flow Metab 21:568–576, 2001114. Lin B, Ginsberg MD, Busto R: Hypergly-
cemic but not normoglycemic globalischemia induces marked early intran-euronal expression of beta-amyloid pre-cursor protein. Brain Res 888:107–116,2001
115. Ste-Marie L, Hazell AS, Bemeur C, But-terworth R, Montgomery J: Immunohis-tochemical detection of inducible nitricoxide synthase, nitrotyrosine and man-ganese superoxide dismutase followinghyperglycemic focal cerebral ischemia.Brain Res 918:10–19, 2001
116. Li P, Liu G, He Q, Floyd R, Siesjo B:Production of hydroxyl free radical bybrain tissues in hyperglycemic rats sub-jected to transient forebrain ischemia.Free Rad Biol Med 27:1033–1040, 1999
117. Lockhart B, Bonhomme N, Roger A, Do-rey G, Casara P, Lestage P: Protective ef-fect of the antioxidant 6-ethoxy-2,2-pentamethylen-1,2-dihydroquinoline(S 33113) in models of cerebral neuro-degeneration. Eur J Pharmacol 416:59–68, 2001
118. Prado R, Watson BD, Wester P: Effects ofnitric oxide synthase inhibition on cere-bral blood flow following bilateral ca-rotid artery occlusion and recirculationin the rat. J Cereb Blood Flow Metab 13:720–723, 1993
119. Wang MJ, Huang HM, Hsieh SJ, JengKC, Kuo JS: Resveratrol inhibits inter-leukin-6 production in cortical mixedglial cells under hypoxia/hypoglycemiafollowed by reoxygenation. J Neuroim-munol 112:28–34, 2001
120. Nishikawa T, Edelstein D, Du XL, Yam-agishi S, Matsumura T, Kaneda Y, YorekMA, Beebe D, Oates PJ, Hammes HP,Giardino I, Brownlee M: Normalizingmitochondrial superoxide productionblocks three pathways of hyperglycae-mic damage. Nature 404:787–790, 2000
121. Booth G, Stalker TJ, Lefer AM, Scalia R:Elevated ambient glucose induces acuteinflammatory events in the microvascu-lature: effects of insulin. Am J Physiol En-docrinol Metab 280:E848–E856, 2001
122. Giardino I, Edelstein D, Brownlee M:BCL-2 expression or antioxidants pre-vent hyperglycemia-induced formationof intracellular advanced glycation end-products in bovine endothelial cells.J Clin Invest 97:1422–1428, 1996
123. Graier WF, Posch K, Fleischhacker E,Wascher TC, Kostner GM: Increased su-peroxide anion formation in endothelialcells during hyperglycemia: an adaptiveresponse or initial step of vascular dys-function? Diabetes Res Clin Pract 45:153–160, 1999
124. Mohanty P, Hamouda W, Garg R, AljadaA, Ghanim H, Dandona P: Glucose chal-lenge stimulates reactive oxygen species
Management of diabetes and hyperglycemia in hospitals
582 DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004

(ROS) generation by leucocytes. J ClinEndocrinol Metab 85:2970–2973, 2000
125. Du X, Edelstein D, Dimmeler S, Ju Q, SuiC, Brownlee M: Hyperglycemia inhibitsendothelial nitric oxide synthase activityby posttranslational modification at theAkt site. J Clin Invest 108:1341–1348,2001
126. Guzik TJ, Mussa S, Gastaldi D, SadowskiJ, Ratnatunga C, Pillai R, Channon KM:Mechanisms of increased vascular su-peroxide production in human diabetesmellitus: role of NAD(P)H oxidase andendothelial nitric oxide synthase. Circu-lation 105:1656–1662, 2002
127. Sampson M, Davies I, Brown J, Ivory K,Hughes D: Monocyte and neutrophil ad-hesion molecule expression during ac-tue hyperglycemia and after antioxidanttreatment in type 2 diabetes and controlpatients. Arterio Thromb Vasc Biol 22:1187–1193, 2002
128. Malmberg K, for the DIGAMI studygroup: Prospective randomised study ofintensive insulin treatment on long termsurvival after acute myocardial infarc-tion in patients with diabetes mellitus.BMJ 314:1512–1515, 1997
129. Dandona P, Aljada A, Mohanty P: Theanti-inflammatory and potential anti-atherogenic effect of insulin: a new par-adigm. Diabetologia 45:924–930, 2002
130. Dandona P, Aljada A, Bandyopadhyay A:The potential therapeutic role of insulinin acute myocardial infarction in pa-tients admitted to intensive care and inthose with unspecified hyperglycemia.Diabetes Care 26:516–519, 2003
131. Das UN: Is insulin an endogenous car-dioprotector? Crit Care 6:389–393, 2002
132. Melidonis A, Stefanidis A, Tournis S,Manoussakis S, Handanis S, Zairis M,Dadiotis L, Foussas S: The role of strictmetabolic control by insulin infusion onfibrinolytic profile during an acute cor-onary event in diabetic patients. ClinCardiol 23:160–164, 2000
133. Machtey I, Syrkis I, Nissimov MR, LobelH: Potassium, glucose and insulin ad-ministration in acute myocardial infarc-tion: a five-year study. J Am Geriatr Soc24:534–537, 1976
134. Rogers WJ, Stanley AW, Jr., Breinig JB,Prather JW, McDaniel HG, Moraski RE,Mantle JA, Russell RO, Jr., Rackley CE:Reduction of hospital mortality rate ofacute myocardial infarction with glu-cose-insulin-potassium infusion. AmHeart J 92:441–454, 1976
135. Russell RO, Jr., Rogers WJ, Mantle JA,McDaniel HG, Rackley CE: Glucose-in-sulin-potassium, free fatty acids andacute myocardial infarction in man. Cir-culation 53:I207–209, 1976
136. Rogers WJ, Russell RO, Jr., McDanielHG, Rackley CE: Acute effects of glu-
cose-insulin-potassium infusion onmyocardial substrates, coronary bloodflow and oxygen consumption in man.Am J Cardiol 40:421–428, 1977
137. Rackley CE, Russell RO, Jr., Rogers WJ,Mantle JA, McDaniel HG: Glucose-insu-lin-potassium infusion in acute myo-cardial infarction: review of clinicalexperience. Postgrad Med 65:93–99,1979
138. Mantle JA, Rogers WJ, Smith LR, Mc-Daniel HG, Papapietro SE, Russell RO,Jr., Rackley CE: Clinical effects of glu-cose-insulin-potassium on left ven-tricular function in acute myocardialinfarction: results from a randomizedclinical trial. Am Heart J 102:313–324,1981
139. McDaniel HG, Papapietro SE, RogersWJ, Mantle JA, Smith LR, Russell RO, Jr.,Rackley CE: Glucose-insulin-potassiuminduced alterations in individual plasmafree fatty acids in patients with acutemyocardial infarction. Am Heart J 102:10–15, 1981
140. McDaniel HG, Rogers WJ, Russell RO,Jr., Rackley CE: Improved myocardialcontractility with glucose-insulin-potas-sium infusion during pacing in coronaryartery disease. Am J Cardiol 55:932–936,1985
141. Lazar HL: Enhanced preservation ofacutely ischemic myocardium and im-proved clinical outcomes using glucose-insulin-potassium (GIK) solutions. Am JCardiol 80:90A–93A, 1997
142. Lazar HL, Chipkin S, Philippides G, BaoY, Apstein C: Glucose-insulin-potassiumsolutions improve outcomes in diabeticswho have coronary artery operations.Ann Thorac Surg 70:145–150, 2000
143. Lazar HL, Philippides G, Fitzgerald C,Lancaster D, Shemin RJ, Apstein C: Glu-cose-insulin-potassium solutions en-hance recovery after urgent coronaryartery bypass grafting. J Thorac Cardio-vasc Surg 113:354–360; discussion360–352, 1997
144. Lazar HL, Zhang X, Rivers S, Bernard S,Shemin RJ: Limiting ischemic myocar-dial damage using glucose-insulin-po-tassium solutions. Ann Thorac Surg 60:411–416, 1995
145. Lazar HL, Fitzgerald C, Gross S, HeerenT, Aldea GS, Shemin RJ: Determinants oflength of stay after coronary artery by-pass graft surgery. Circulation 92:II20–II24, 1995
146. Apstein CS: Glucose-insulin-potassiumfor acute myocardial infarction: remark-able results from a new prospective,randomized trial. Circulation 98:2223–2226, 1998
147. Scott JF, Robinson GM, French JM,O’Connell JE, Alberti KG, Gray CS: Glu-cose potassium insulin infusions in the
treatment of acute stroke patients withmild to moderate hyperglycemia: theGlucose Insulin in Stroke Trial (GIST).Stroke 30:793–799, 1999
148. Cave AC, Ingwall JS, Friedrich J, Liao R,Saupe KW, Apstein CS, Eberli FR: ATPsynthesis during low-flow ischemia: in-fluence of increased glycolytic substrate.Circulation 101:2090–2096, 2000
149. Marano L, Bestetti A, Lomuscio A, Ta-gliabue L, Castini D, Tarricone D, DarioP, Tarolo GL, Fiorentini C: Effects of in-fusion of glucose-insulin-potassium onmyocardial function after a recent myo-cardial infarction. Acta Cardiol 55:9–15,2000
150. Scott J, Robinson G, French J, O’ConnellJ, Alberti K, Gray C: Blood pressure re-sponse to glucose potassium insulintherapy in patiens with acute stroke withmild to moderate hyperglycaemia.J Neurol Neurosurg Psych 70:401–404,2001
151. Szabo Z, Arnqvist H, Hakanson E,Jorfeldt L, Svedjeholm R: Effects ofhigh-dose glucose-insulin-potassium onmyocardial metabolism after coronarysurgery in patients with type II diabetes.Clin Sci (Lond) 101:37–43, 2001
152. Ramanathan T, Shirota K, Morita S,Nishimura T, Huang Y, Hunyor S: Glu-cose-insulin-potassium solution im-proved left ventricular mechanics indiabetes. Ann Thorac Surg 73:582–587,2002
153. Svedjeholm R, Huljebrant I, HakansonE, Vanhanen I: Glutamate and high-doseglucose-insulin-potassium (GIK) in thetreatment of severe cardiac failure aftercardiac operations. Ann Thorac Surg 59:S23–S30, 1995
154. Apstein CS, Taegtmeyer H: Glucose-in-sulin-potassium in acute myocardial in-farction: the time has come for a large,prospective trial. Circulation 96:1074–1077, 1997
155. Weiss JN, Lamp ST: Glycolysis preferen-tially inhibits ATP-sensitive K chan-nels in isolated guinea pig cardiacmyocytes. Science 238:67–69, 1987
156. Mallet RT, Hartman DA, Bunger R: Glu-cose requirement for postischemic re-covery of perfused working heart. EurJ Biochem 188:481–493, 1990
157. Eberli FR, Weinberg EO, Grice WN,Horowitz GL, Apstein CS: Protective ef-fect of increased glycolytic substrateagainst systolic and diastolic dysfunc-tion and increased coronary resistancefrom prolonged global underperfusionand reperfusion in isolated rabbit heartsperfused with erythrocyte suspensions.Circ Res 68:466–481, 1991
158. Oliver MF, Opie LH: Effects of glucoseand fatty acids on myocardial ischaemiaand arrhythmias. Lancet 343:155–158,
Clement and Associates
DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004 583

1994159. Xu KY, Zweier JL, Becker LC: Functional
coupling between glycolysis and sarco-plasmic reticulum Ca2 transport. CircRes 77:88–97, 1995
160. Manzella D, Grella R, Marfella R, Giugli-ano D, Paolisso G: Elevated post-pran-dial free fatty acids are associated withcardiac sympathetic overactivity in typeII diabetic patients. Diabetologia 45:1737–1738, 2002
161. Oliver MF: Metabolic causes and pre-vention of ventricular fibrillation duringacute coronary syndromes. Am J Med112:305–311, 2002
162. Zhu P, Lu L, Xu Y, Greyson C, SchwartzGG: Glucose-insulin-potassium pre-serves systolic and diastolic function inischemia and reperfusion in pigs. Am JPhysiol Heart Circ Physiol 278:H595–H603, 2000
163. Szabo Z, Hakanson E, Jorfeldt L, Sved-jeholm R: Myocardial uptake and releaseof substrates in type II diabetics under-going coronary surgery. Scand Cardio-vasc J 35:207–211, 2001
164. Stanley AW, Jr., Moraski RE, Russell RO,Rogers WJ, Mantle JA, Kreisberg RA,McDaniel HG, Rackley CE: Effects ofglucose-insulin-potassium on myocar-dial substrate availability and utilizationin stable coronary artery disease: studieson myocardial carbohydrate, lipid andoxygen arterial-coronary sinus differ-ences in patients with coronary arterydisease. Am J Cardiol 36:929–937, 1975
165. Steinberg HO, Brechtel G, Johnson A,Fineberg N, Baron AD: Insulin-mediatedskeletal muscle vasodilation is nitric ox-ide dependent: a novel action of insulinto increase nitric oxide release. J Clin In-vest 94:1172–1179, 1994
166. Cardillo C, Nambi S, Kilcoyne C,Choucair W, Katz A, Quon M, Panza J:Insulin stimulates both endothelin andnitric oxide activity in the human fore-arm. Circulation 100:820–825, 1999
167. Chaudhuri A, Kanjwal Y, Mohanty P,Rao S, Sung BH, Wilson MF, Dandona P:Insulin-induced vasodilatation of inter-nal carotid artery. Metabolism 48:1470–1473, 1999
168. Vehkavaara S, Makimattila S, SchlenzkaA, Vakkilainen J, Westerbacka J, Yki-Jarvinen H: Insulin therapy improvesendothelial function in type 2 diabetes.Arterioscler Thromb Vasc Biol 20:545–550, 2000
169. Rask-Madsen C, Ihlemann N, Krarup T,Christiansen E, Kober L, Nervil KistorpC, Torp-Pedersen C: Insulin therapy im-proves insulin-stimulated endothelialfunction in patients with type 2 diabetesand ischemic heart disease. Diabetes 50:2611–2618, 2001
170. Gaenzer H, Neumayr G, Marschang p,
Sturm W, Lechleitner M, Foger B, Kirch-mair R, Patsch J: Effect of insulin therapyon endothelium-dependent dilation intype 2 diabetes mellitus. Am J Cardiol 89:431–434, 2002
171. Evans M, Anderson R, Smith J, Khan N,Graham J, Thomas A, Morris K, Deely D,Frenneaux M, Davies J, Rees A: Effects ofinsulin lispro and chronic vitamin Ctherapy on postprandial lipaemia, oxi-dative stress and endothelial function inpatients with type 2 diabetes mellitus.Eur J Clin Invest 33:231–238, 2003
172. Arcaro G, Cretti A, Balzano S, Lechi A,Muggeo M, Bonora E, Bonadonna R: In-sulin causes endothelial dysfunction inhumans: sites and mechanisms. Circula-tion 105:576–582, 2002
173. Aljada A, Dandona P: Effect of insulin onhuman aortic endothelial nitric oxidesynthase. Metabolism 49:147–150, 2000
174. Das UN: Is insulin an antiinflammatorymolecule? Nutrition 17:409–413, 2001
175. Das UN: Insulin and inflammation: fur-ther evidence and discussion. Nutrition18:526–527, 2002
176. Hansen T, Thiel S, Wouters P, Chris-tiansen J, VandenBerghe B: Intensive in-sulin therapy exerts antiinflammatoryeffects in critically ill patients and coun-teracts the adverse effect of low man-nose-gind lectin levels. J Clin EndocrinolMetab 88:1082–1088, 2003
177. Aikawa R, Nawano M, Gu Y, Katagiri H,Asano T, Zhu W, Nagai R, Komuro I:Insulin prevents cardiomyocytes fromoxidative stress-induced apoptosisthrough activationof PI3 kinase/Akt.Circulation 102:2873–2879, 2000
178. Aljada A, Saadeh R, Assian E, Ghanim H,Dandona P: Insulin inhibits the expres-sion of intercellular adhesion mole-cule-1 by human aortic endothelial cellsthrough stimulation of nitric oxide.J Clin Endocrinol Metab 85:2572–2575,2000
179. Aljada A, Ghanim H, Saadeh R, DandonaP: Insulin inhibits NFkappaB andMCP-1 expression in human aortic en-dothelial cells. Journal of Clinical Endocri-nol Metab 86:450–453, 2001
180. Dandona P, Aljada A, Mohanty P, Gha-nim H, Hamouda W, Assian E, Ahmed S:Insulin inhibits intranuclear nuclear fac-tor kappaB and stimulates IkappaB inmononuclear cells in obese subjects: ev-idence for an anti-inflammatory effect?J Clin Endocr Metab 86:3257–3265,2001
181. Aljada A, Ghanim H, Mohanty P, KapurN, Dandona P: Insulin inhibits the pro-inflammatory transcription factor earlygrowth response gene-1 (Egr)-1 expres-sion in mononuclear cells (MNC) andreduces plasma tissue factor (TF) andplasminogen activator inhibitor-1 (PAI-1)
concentrations. J Clin Endocr Metab 87:1419–1422, 2002
182. Jonassen A, Sack M, Mjos O, Yellon D:Myocardial protection by insulin atreperfusion requires early administra-tion and is mediated via Akt and p70s6kinase cell-survival signaling. Circ Res89:1191–1198, 2001
183. Guazzi M, Brambilla R, Vita SD, GuazziM: Diabetes worsens pulmonary diffu-sion in heart failure, and insulin coun-teracts this effect. Am J Respir Crit CareMed 166:978–982, 2002
184. Wiener C, Sylvester J: Effects of insulin,glucose analogues, and pyruvate on vas-cular responses to anoxia in isolated fer-ret lungs. J Appl Physiol 74:2426–2431,1993
185. Hamilton MG, Tranmer BI, Auer RN: In-sulin reduction of cerebral infarctiondue to transient focal ischemia. J Neuro-surg 82:262–268, 1995
186. Melin J, Hellberg L, Larsson E, Zezina L,Fellstrom B: Protective effect of insulinon ischemic renal injury in diabetes mel-litus. Kidney Int 61:1383–1392, 2002
187. Gore D, Wolf S, Herndon D, Wolfe R:Relative influence of glucose and insulinon peripheral amino acid metabolism inseverely burned patients. J Parenter EnterNutr 26:271–277, 2002
188. Westerbacka J, Yki-Jarvinen H, Tur-peinen A, Rissanen A, Vehkavaara S,Syrjala M, Lassila R: Inhibition of plate-let-collagen interaction: an in vivo actionof insulin abolished by insulin resistancein obesity. Arterioscler Thromb Vasc Biol22:167–172, 2002
189. Levetan CS, Magee MF: Hospital man-agement of diabetes. Endocrinol MetabClin North Am 29:745–770, 2000
190. Leahy JL, Bonner-Weir S, Weir GC:�-cell dysfunction induced by chronichyperglycemia: current ideas on mecha-nism of impaired glucose-induced insu-lin secretion. Diabetes Care 15:442–455,1992
191. Pomposelli J, Baxter J, Babineau T, Pom-fret E, Driscoll D, Forse R, Bistrian B:Early postopertive glucose control pre-dicts nosocomial infection rate in dia-betic patients. J Parenter Enter Nutr 22:77–81, 1998
192. Capes S, Hunt D, Malmberg K, GersteinH: Stress hyperglycaemia and increasedrisk of death after myocardial infarctionin patients with and without diabetes: asystematic overview. Lancet 355:773–778, 2000
193. Bolk J, van der Ploeg T, Cornel JH, Ar-nold AE, Sepers J, Umans VA: Impairedglucose metabolism predicts mortalityafter a myocardial infarction. Int J Cardiol79:207–214, 2001
194. Malmberg K, Ryden L, Efendic S, HerlitzJ, Nicol P, Waldenstrom A, Wedel H,
Management of diabetes and hyperglycemia in hospitals
584 DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004

Welin L: Randomized trial of insulin-glucose infusion followed by subcutane-ous insulin treatment in diabeticpatients with acute myocardial infarc-tion (DIGAMI study): effects on mortal-ity at 1 year. J Am Coll Cardiol 26:57–65,1995
195. Malmberg K, Yusuf S, Gerstein HC,Brown J, Zhao F, Hunt D, Piegas L, Cal-vin J, Keltai M, Budaj A: Impact of dia-betes on long-term prognosis in patientswith unstable angina and non-Q-wavemyocardial infarction: results of the OA-SIS (Organization to Assess Strategies forIschemic Syndromes) Registry. Circula-tion 102:1014–1019, 2000
196. Furnary A, Zerr K, Grunkemeier G, StarrA: Continuous intravenous insulin infu-sion reduces the incidence of deep ster-nal wound infection in diabetic patientsafter cardiac surgical procedures. AnnThorac Surg 67:352–362, 1999
197. Furnary AP, Gao G, Grunkemeier GL,Wu Y, Zerr KJ, Bookin SO, Floten HS,Starr A: Continuous insulin infusion re-duces mortality in patients wth diabetesundergoing coronary artery bypassgrafting. J Thorac Cardiovasc Surg 125:1007–1021, 2003
198. Zerr KJ, Furnary AP, Grunkemeier GL,Bookin S, Kanhere V, Starr A: Glucosecontrol lowers the risk of wound infec-tion in diabetics after open heart opera-tions. Ann Thorac Surg 63:356–361,1997
199. Golden S, Peart-Vigilance C, Kao W,Brancati F: Perioperative glycemic con-trol and the risk of infectious complica-tions in a cohort of adults with diabetes.Diabetes Care 22:1408–1414, 1999
200. Van den Berghe G, Wouters PJ, BouillonR, Weekers F, Verwaest C, Schetz M,Vlasselaers D, Ferdinande P, Lauwers P:Outcome benefit of intensive insulintherapy in the critically ill: insulin doseversus glycemic control. Crit Care Med31:359–366, 2003
201. Bruno A, Biller J, Adams HP, Jr., ClarkeWR, Woolson RF, Williams LS, HansenMD: Acute blood glucose level and out-come from ischemic stroke: Trial of ORG10172 in Acute Stroke Treatment(TOAST) Investigators. Neurology 52:280–284, 1999
202. Pulsinelli WA, Levy DE, Sigsbee B,Scherer P, Plum F: Increased damage af-ter ischemic stroke in patients with hy-perglycemia with or without establisheddiabetes mellitus. Am J Med 74:540–544, 1983
203. Demchuk AM, Morgenstern LB, KriegerDW, Linda Chi T, Hu W, Wein TH,Hardy RJ, Grotta JC, Buchan AM: Serumglucose level and diabetes predict tissueplasminogen activator-related intracere-bral hemorrhage in acute ischemic
stroke. Stroke 30:34–39, 1999204. Kiers L, Davis SM, Larkins R, Hopper J,
Tress B, Rossiter SC, Carlin J, Ratnaike S:Stroke topography and outcome in rela-tion to hyperglycaemia and diabetes.J Neurol Neurosurg Psychiatry 55:263–270, 1992
205. Williams LS, Rotich J, Qi R, Fineberg N,Espay A, Bruno A, Fineberg SE, TierneyWR: Effects of admission hyperglycemiaon mortality and costs in acute ischemicstroke. Neurology 59:67–71, 2002
206. Scott JF, Robinson GM, French JM,O’Connell JE, Alberti KG, Gray CS: Prev-alence of admission hyperglycaemiaacross clinical subtypes of acute stroke.Lancet 353:376–377, 1999
207. Brady P, Terzic A: The sulfonylurea con-troversy: more questions from the heart.J Am Coll Cardiol 31:950–956, 1998
208. Howes L, Sundaresan P, Lykos D: Car-diovascular effects of oral hypoglycemicdrugs. Clin Exp Pharmacol Physiol 23:201–206, 1996
209. Meinert C, Knatterud G, Prout T, KlimtC, University Group Diabetes Program:A study of the effects of hypoglycemicagents on vascular complications in pa-tients with adult-onset diabetes II: mor-tality results. Diabetes 19:789–830, 1970
210. UKPDS Study Group: Intensive blood-glucose control with sulphonylureas orinsulin compared with conventionaltreatment and risk of complications inpatients with type 2 diabetes (UKPDS33). Lancet 352:837–853, 1998
211. Murry C, Jennings R, Reimer K: Precon-ditioning with ischemia: a delay of lethalcell injury in ischemic myocardium. Cir-culation 74:1124–1136, 1986
212. Deutsch E, Berger M, Kussmaul W, Hir-shfeld J, Herrmann H, Laskey W: Adap-tation to ischemia during percutaneoustransluminal coronary angioplasty: clinic,hemodynamic, and metabolic features.Circulation 82:2044–2051, 1990
213. Terzic A, Jahangir A, Kurachi Y: CardiacATP-sensitive K channels: regulationby intracellular nucleotides and Kchannel-opening durgs. Am J Physiol269:C525–C545, 1995
214. Ashcroft S, Ashcroft F: The sulfonylureareceptor. Biochim Biophys Acta 1175:45–59, 1992
215. Engler R, Yellon D: Sulfonylurea K-ATPblockade in type II diabets and precon-ditioning in cardiovascular disease: timefor reconsideration. Circulation 94:2297–2301, 1996
216. Cleveland J, Meldrum D, Cain B, Baner-jee A, Harken A: Oral sulfonylurea hy-poglycemic agents prevent ischemicpreconditioning in human myocardium:two paradoxes revisited. Circulation 96:29–32, 1997
217. Tomai F, Crea F, Gaspardone A, Versaci
F, Paulis RD: Ishemic preconditioningduring coronary angioplasty is pre-vented by glibenclamide, a selectiveATP-sensitive K channel blocker. Cir-culation 90:700–705, 1994
218. Horimoto H, Nakai Y, Mieno S, NomuraY, Nakahara K, Sasaki S: Oral hypogly-cemic sulfonylurea glimepiride pre-serves the myoprotective effects ofischemic preconditioning. J Surg Res105:181–188, 2002
219. Gribble F, Tucker S, Seino S, Ashcroft F:Tissue specificity of sulfonylureas: stud-ies on cloned cardiac and beta-cellK(ATP) channels. Diabetes 47:1412–1418, 1998
220. Legtenberg R, Houston R, Oeseburg B,Smits P: Effects of sulfonylurea deriva-tives on ischemia-induced loss of func-tion in the isolated rat heart. EurJ Pharmacol 419:85–92, 2001
221. Mocanu M, Maddock H, Baxter G, Law-rence C, Standen N, Yellon D: Glime-piride, a novel sulfonylurea, does notabolish myocardial protection affordedby either ischemic preconditioning ordiazoxide. Circulation 103:3111–3116,2001
222. Nieszner E, Posa I, Kocsis E, Pogatsa G,Preda I, Koltai M: Influence of diabeticstate and that of different sulfonylureason the size of myocardial infarction withand without ischemic preconditioningin rabbits. Exper Clin Endocr Diab 110:212–218, 2002
223. Klepzig H, Kober G, Matter C, Luus H,Schneider H, Boedeker K, Kiowski W,Amann F, Gruber D, Harris S, Burger W:Sulfonylureas and ischaemic precondi-tioning; a double-blind, placebo-con-trolled evaluation of glimepiride andglibenclamide. Eur Heart J 20:439–446,1999
224. Legtenberg R, Houston R, Smits P, Oese-burg B: Hemodynamic changes causedby glibenclamide in isolated, working,erythrocyte perfused rat heart. Advancesin Exper Med Biol 471:257–263, 1999
225. Najeed S, Khan I, Molnar J, Somberg J:Differential effect of glyburide (gliben-clamide) and metformin on QT disper-sion: a potential adenosine triphosphatesensitive K channel effect. Am J Cardiol90:1103–1106, 2002
226. Dhein S, Pejman P, Krusemann K: Ef-fects of the I(K.ATP) blockers gliben-clamide and HMR 1883 on cardiacelectrophysiology during ischemia andreperfusion. Eur J Pharmacology 398:273–284, 2000
227. Ren J, Dominguez L, Sowers J, DavidoffA: Metformin but not glyburide preventshigh glucose-induced abnormalities inrelaxation and intracellular Ca tran-sients in adult rat ventricular myocytes.Diabetes 48:2059–2065, 1999
Clement and Associates
DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004 585

228. Scognamiglio R, Avogaro A, Kreutzen-berg Sd, Negut C, Palisi M, Bagolin E,Tiengo A: Effects of treatment with sul-fonylurea drugs or insulin on ischemia-induced myocardial dysfunction in type2 diabetes. Diabetes 51:808–812, 2002
229. Garratt KN, Brady PA, Hassinger NL, etal.: Sulfonylurea drugs increase earlymortality in patients with diabetes mel-litus after direct angioplasty for acutemyocardial infarction. J Am Coll Cardiol33:119–124, 1999
230. O’Keefe J, Blackstone E, Sergeant P, Mc-Callister B: The optimal mode of coro-nary revascularization for diabetics. EurHeart J 19:1696–1703, 1998
231. Aronow W, Ahn C: Incidence of newcoronary events in older persons withdiabetes mellitus and prior myocardialinfarction treated with sulfonylureas, in-sulin metformin and diet alone. Am JCardiol 88:556–557, 2001
232. Klamann A, Sarfert P, Launhardt V,Schulte G, Schmiegel W, Nauck M:Myocardial infarction in diabetic vs non-diabetic subjects: sruvival and infarctsize following therapy with sulfonyl-ureas (glibenclamide). Eur Heart J21:220–229, 2000
233. Brady P, Al-Suwaidi J, Kopecky S, TerzicA: Sulfonylureas and mortality in dia-betic patients after myocardial infarc-tion. Circulation 97:709–710, 1998
234. Davis T, Parsons R, Broadhurst R, HobbsM, Jamrozik K: Arrhythmias and mortal-ity after myocardial infarction in diabeticpatients: relationship to diabetes treat-ment. Diabetes Care 21:637–640, 1998
235. Halkin A, Roth A, Jonas M, Behar S: Sul-fonylureas are not associated with in-creased mortality in diabetics treatedwith thrombolysis for acute myocardialinfarction. J Thromb Thrombolysis 12:177–184, 2001
236. Jollis J, Simpson R, Cascio W,Chowdhury M, Crouse J, Smith S: Rela-tion between sulfonylurea therapy, com-plicaions, and outcome for elderlypatients with acute myocardial infarc-tion. Am Heart J 128:S376–S380, 1999
237. Weih M, Amberger N, Wegener S,Dirnagl U, Reuter T, Einhaupl K: Sulfo-nylurea drugs do not influenced initialstroke severity and in-hospital outcomein stroke patients with diabetes. Stroke32:2029–2032, 2001
238. Malmberg K, Norhammar A, Wedel H,Ryden L: Glycometabolic state at admis-sion: important risk marker of mortalityin conventionally treated patients withdiabetes mellitus and acute myocardialinfarction: long-term results from theDiabetes and Insulin-Glucose infusion inAcute Myocardial Infarction (DIGAMI)Study. Circulation 99:2626–2632, 1999
239. Miller C, Phillips L, Ziemer D, Gallina D,
Cook C, El-Kebbi I: Hypoglycemia inpatients with type 2 diabetes mellitus.Arch Intern Med 161:1653–1659, 2001
240. Harrower A: Comparative tolerability ofsulphonylureas in diabetes mellitus.Drug Safety 22:313–320, 2000
241. UKPDS Study Group: Effect of intensiveblood-glucose control with metforminon complications in overweight patientswith type 2 diabetes (UKPDS 34). Lancet352:854–865, 1998
242. Misbin R, Green L, Stadel B, GueriguianJ, Gubbi A, Alexander G: Lactic acidosisin patients with diabetes treated withmetformin. N Engl J Med 338:265–266,1998
243. Emslie-Smith A, Boyle D, Evans J, Sulli-van F, Morris A: Contraindications tometformin therapy in patients with type2 diabetes: a population-based study ofadherence to prescribing guidelines.Diabet Med 18:483–488, 2001
244. Horlen C, Malone R, Bryant B, Dennis B,Carey T, Pignone M, Rothman R: Fre-quency of inappropriate metformin pre-scriptions. JAMA 287:2504–2505, 2002
245. Sulkin T, Bosman D, Krentz A: Contra-indications to metformin therapy in pa-tients with NIDDM. Diabetes Care 20:925–928, 1997
246. Calabrese A, Coley K, DaPos S, SwansonD, Rao R: Evaluation of prescribing prac-tices: risk of lactic acidosis with met-formin therapy. Arch Intern Med 162:434–437, 2002
247. Masoudi FA, Wang Y, Inzucchi SE,Setaro JF, Havranek EP, Foody JM,Krumholz HM: Metformin and thiazo-lidinedione use in Medicare patientswith heart failure. JAMA 290:81–85,2003
248. Salpeter S, Greyber E, Pasternak G, Sal-peter E: Metformin does not increase fa-tal or nonfatal lactic acidosis or bloodlactate levels in type 2 diabetes mellitus(Review Article). Cochrane Database SystRev 2:CD002967, 2002
249. Gillies P, Dunn C: Pioglitazone. Drugs60:333–343, 2000
250. Malinowski J, Bolesta S: Rosiglitazone inthe treatment of type 2 diabetes mellitus:a critical review. Clin Ther 22:1151–1168, 2000
251. Idris I, Gray S, Donnelly R: Rosiglitazoneand pulmonary oedema: an acute dose-dependent effect on human endothelialcell permeability. Diabetologia 46:488–490, 2003
252. Choi S, Choi D, Ko Y, Chang YS, Cho Y,Lim S, Nam M, Lee H, Cha B: Preventiveeffects of rosiglitazone on restenoss aftercoronary stenting in patients with type 2diabetes (Abstract). Diabetes 52 (Suppl.1):A19, 2003
253. Lalli C, Ciofetta M, Del Sindaco P, Tor-lone E, Pampanelli S, Compagnucci P,
Cartechini MG, Bartocci L, Brunetti P,Bolli GB: Long-term intensive treatmentof type 1 diabetes with the short-actinginsulin analog lispro in variable combi-nation with NPH insulin at mealtime.Diabetes Care 22:468–477, 1999
254. Clement S, Still JG, Kosutic G, McAllis-ter RG: Oral insulin product hexyl-insu-lin monoconjugate 2 (HIM2) in type 1diabetes mellitus: the glucose stabiliza-tion effects of HIM2. Diabetes TechnolTher 4:459–466, 2002
255. Queale WS, Seidler AJ, Brancati FL: Gly-cemic control and sliding scale insulinuse in medical inpatients with diabetesmellitus. Arch Intern Med 157:545–552,1997
256. Gearhart J, Duncan JL, Replogle WH,Forbes RC, Walley EJ: Efficacy of slid-ing-scale insulin therapy: a comparisonwith prospective regimens. Fam PractRes J 14:313–322, 1994
257. Walts LF, Miller J, Davidson MB, BrownJ: Perioperative management of diabetesmellitus. Anesthesiology 55:104 –109,1981
258. Genuth SM: Constant intravenous insu-lin infusion in diabetic ketoacidosis.JAMA 223:1348–1351, 1973
259. Kidson W, Casey J, Kraegen E: Treat-ment of severe diabetes mellitus by insu-lin infusion. Br Med J 2:691–694, 1974
260. Page MM, Alberti KG, Greenwood R,Gumaa KAA, Hockaday TD, Lowy C,Nabarro JD, Pyke DA, Sonksen PH,Watkins PJ, West TE: Treatment of dia-betic coma with continuous low dose in-fusion of insulin. Br Med J 2:687–690,1974
261. Semple PF, White C, Manderson WG:Continuous intravenous infusion ofsmall doses of insulin in treatment of di-abetic ketoacidosis. Br Med J 2:694–698, 1974
262. Soler NG, FitzGerald MG, Wright AD,Malins JM: Comparative study of differ-ent insulin regimens in management ofdiabetic ketoacidosis. Lancet2:1221–1224, 1975
263. Kitabchi AE, Ayyagari V, Guerra SMO:The efficacy of low-dose versus conven-tional therapy of insulin for treatment ofdiabetic ketoacidosis. Ann Intern Med 84:633–638, 1976
264. Alberti KGMM: Comparison of differentinsulin regimens in diabetic ketoacido-sis. Lancet 1:83–84, 1976
265. Alberti KGMM: Low-dose insulin in thetreatment of diabetic detoacidosis. ArchIntern Med 137:1367–1376, 1977
266. Fisher JN, Shahshahani MN, KitabchiAE: Diabetic ketoacidosis: low-dose in-sulin therapy by various routes. N EnglJ Med 297:238–241, 1977
267. Bienia R, Ripoll I: Diabetic ketoacidosis.JAMA 241:510–511, 1979
Management of diabetes and hyperglycemia in hospitals
586 DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004

268. Sacks HS, Shahshahani M, Kitabchi AE,Fisher JN, Young RT: Similar respon-siveness of diabetic ketoacidosis to low-dose insulin by intramuscular injectionand albumin-free infusion. Ann InternMed 90:36–42, 1979
269. Levine SN, Loewenstein JE: Treatmentof diabetic ketoacidosis. Arch Intern Med141:713–715, 1981
270. Berger W, Keller U: Treatment of dia-betic ketoacidosis and nonketotic hyper-osmolar diabetic coma. Baillieres ClinEndocrinol Metab 6:1–22, 1992
271. Siperstein MD: Diabetic ketoacidosisand hyperosmolar coma. EndocrinolMetab Clin North Am 21:415–432, 1992
272. Fleckman AM: Diabetic Ketoacidosis.Endocrinol Metab Clin North Am 22:181–207, 1993
273. Umpierrez GE, Kelly JP, Navarrete JE:Hyperglycemic crises in urban blacks.Arch Intern Med 157:669–675, 1997
274. Wagner A, Risse A, Brill HL, Wien-hausen-Wilke V, Rottman M, SondernK, Angelkort B: Therapy of severe dia-betic ketoacidosis: zero-mortality undervery-low-dose insulin application. Dia-betes Care 22:674–677, 1999
275. Kitabchi AE, Umpierrez GE, MurphyMB, Barrett EJ, Kreisberg RA, Malone JI,Wall BM: Management of hyperglycemiccrises in patients with diabetes. DiabetesCare 24:131–153, 2001
276. Gill GV, Sherif IH, Alberti KG: Manage-ment of diabetes during open heart sur-gery. Br J Surg 68:171–172, 1981
277. Alberti KG, Gill GV, Elliot MJ: Insulindelivery during surgery in the diabeticpatient. Diabetes Care 5 (Suppl. 1):65–67, 1982
278. Thomas DJ, Platt HS, Alberti KG: Insu-lin-dependent diabetes during the peri-operative period: an assessment ofcontinuous glucose-insulin-potassiuminfusion, and traditional treatment. An-aesthesia 39:629–637, 1984
279. Husband DJ, Thai AC, Alberti KG: Man-agement of diabetes during surgery withglucose-insulin-potassium infusion.Diabet Med 3:69–74, 1986
280. Watts NB, Gebhart SSP, Clark RV, Phil-lips LS: Postoperative mangement of di-abetes mellitus: steady-state glucosecontrol with bedside algorithm for insu-lin adjustment. Diabetes Care 10:722–728, 1987
281. Pezzarossa A, Taddei F, Cimicchi MC,Rossini E, Contini S, Bonora E, Gnudi A,Uggeri E: Perioperative management ofdiabetic subjects: subcutaneous versusintravenous insulin administration dur-ing glucose-potassium infusion. DiabetesCare 11:52–58, 1988
282. Hirsch IB, McGill JB: Role of insulin inmanagement of surgical patients with di-abetes mellitus. Diabetes Care 13:980–
991, 1990283. Alberti KG: Diabetes and surgery. Anes-
thesiology 74:209–211, 1991284. Mantha S, Rao SM: Peri-operative man-
agement of diabetes mellitus. Anaesthe-sia 46:900, 1991
285. Gavin LA: Perioperative management ofthe diabetic patient. Endocrin Metab ClinNorth Am 21:457–475, 1992
286. Schiff RL, Emanuele MA: The surgicalpatient with diabetes mellitus: guide-lines for management. J Gen Intern Med10:154–161, 1995
287. Gill GV, Alberti KGMM: The care of thediabetic patient during surgery. In Inter-national Textbook of Diabetes Mellitus. Al-berti KGMM, Zimmet P, Keen H,DeFronzo RA, Eds. Chichester, Wiley,1992, p. 1173–1183
288. Aviles-Santa L, Raskin P: Surgery andanesthesia. In Therapy for Diabetes Melli-tus and Related Disorders. 3rd ed. Lebo-vitz HE, Ed. Alexandria, VA, ADA, 1998,p. 224–233
289. Surgery. In Medical Management of Type1 Diabetes. Kelley DB, Ed. Alexandria,VA, ADA, 1998, p. 159–163
290. Ahmann A: Comprehensive manage-ment of the hospitalized patient with di-abetes. Endocrinologist 8:250–259, 1998
291. Hill A: Continuous intravenous insulininfusion in patients with diabetes aftercardiac surgery. Clin Nurse Spec 16:93–95, 2002
292. Mittra B: Potassium, glucose, and insulinin treatment of myocardial infarction.Lancet 2:607–609, 1965
293. Hendra TJ, Yudkin JS: An algorithm fortight glycaemic control in diabetic in-farct survivors. Diabetes Res Clin Pract16:213–220, 1992
294. Malmberg KA, Efendic S, Ryden LE: Fea-sibility of insulin-glucose infusion in di-abetic patients with acute myocardialinfarction. Diabetes Care 17:1007–1014,1994
295. Fath-Ordoubadi F, Beatt KJ: Glucose-in-sulin-potassium therapy for treatment ofacute myocardial infarction: an overviewof randomzied placebo-controlled trials.Circulation 96:1152–1156, 1997
296. Kjellman UW, Bjork K, Dahlin A, EkrothR, Kirno K, Svensson G, Wernerman J:Insulin (GIK) improves myocardial me-tabolism in patients during blod cardio-plegia. Scand Cardiovasc J 34:321–330,2000
297. Braithwaite S: Detection and manage-ment of diabetes mellitus during glu-cocorticoid therapy of nonendocrinedisease. In Endocrine Replacement Ther-apy in Clinical Practice. Meikle AW, Ed.Totowa, NJ, Humana Press, 2003, p.251–282
298. Hirsch IB, Paauw DS, Brunzell J: Inpa-tient management of adults with diabe-
tes. Diabetes Care 18:870–878, 1995299. McWilliam DB: The practical manage-
ment of glucose-insulin infusions in theintensive care patient. Intensive Care Med6:133–135, 1980
300. Woolfson AM: Control of blood glucoseduring nutritional support in ill patients.Intensive Care Med 7:11–14, 1980
301. Brown G, Dodek P: Intravenous insulinnomogram improves blood glucose con-trol in the critically ill. Crit Care Med 29:1714–1719, 2001
302. White NH, Skor D, Santiago JV: Practicalclose-loop insulin delivery: a system forthe maintenance of overnight euglyce-mia and the calculation of basal insulinrequirements in insulin-dependent dia-betics. Ann Intern Med 97:210–213,1982
303. Mao CS, Riegelhuth ME, Van Gundy D,Cortez C, Melendez S, Ipp E: An over-night insulin infusion algorithm pro-vides morning normoglycemia and canbe used to predict insulin requirementsin noninsulin-dependent diabetes melli-tus. J Clin Endocrinol Metab 82:2466–2470, 1997
304. Hawkins JB, Jr., Morales CM, Shipp JC:Insulin requirement in 242 patients withtype II diabetes mellitus. Endocr Pract1:385–389, 1995
305. Hemmerling TM, Schmid MC, SchmidtJ, Kern S, Jacobi KE: Comparison of acontinuous glucose-insulin-potassiuminfusion versus intermittent bolus appli-cation of insulin on perioperative glu-cose control and hormone status ininsulin-treated type 2 diabetics. J ClinAnesth 13:293–300, 2001
306. Hirsch IB, Paauw DS: Diabetes manage-ment in special situations. Endocr MetabClin North Am 26:631–645, 1997
307. Quevedo SF, Sullivan E, Kington R, Rog-ers W: Improving diabetes care in thehospital using guideline-directed or-ders. Diabetes Spectrum 14:226 –233,2001
308. Peterson L, Caldwell J, Hoffman J: Insu-lin adsorbance to polyvinylchloride sur-faces with implications for constant-infusion therapy. Diabetes 25:72–74,1976
309. Turner RC, Grayburn JA, Newman GB:Measurement of the insulin delivery ratein man. J Clin Endocrinol Metab 33:279–286, 1971
310. Clumeck N, Detroyer A, Naeije R: Smallintravenous insulin boluses in the treat-ment of diabetic coma. Lancet 2:416,1975
311. Dunnett M, Steemson J, Sear JW, TurnerRC, Holman RR: Rapid restoration ofnormoglycaemia using intravenous in-sulin boluses. Diabetes Res 15:151–155,1990
312. Beyer J, Krause U, Dobronz A, Fuchs B.
Clement and Associates
DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004 587

Delver JR, Wagner R: Assessment of in-sulin needs in insulin-dependent diabet-ics and healthy volunteers under fastingconditions. Horm Metab Res 24 (Suppl.):71–77, 1990
313. Mokan M, Gerich JE: A simple insulininfusion algorithm for establishing andmaintaining overnight near-normogly-cemia in type I and type II diabetes. J ClinEndocrinol Metab 74:943–945, 1992
314. Markovitz L, Wiechmann R, Harris N,Hayden V, Cooper J, Johnson G, Harel-stad R, Calkins L, Braithwaite SS: De-scription and evaluation of a glycemicmanagement protocol for diabetic pa-tients undergoing heart surgery. EndocrPract 8:10–18, 2002
315. Latham R, Lancaster AD, Covington JF,Pirolo JS, Thomas CS: The association ofdiabetes and glucose control with surgi-cal-site infections among cardiothoracicsurgery patients. Infect Control Hosp Epi-demiol 22:607–612, 2001
316. Carson JL, Scholz PM, Chen AY, Peter-son ED, Gold J, Schneider SH: Diabetesmellitus increases short-term mortalityand morbidity in patients undergoingcoronary artery bypass graft surgery.J Am Coll Cardiol 40:418–423, 2002
317. Metchick LN, Petit WA, Jr., Inzucchi SE:Inpatient management of diabetes mel-litus. Am J Med 113:317–323, 2002
318. Mitka M: Rethinking treatment for pa-tients with diabetes and cardiovasculardisease. JAMA 287:2488–2491, 2002
319. Szabo Z, Hakanson E, Svedjeholm R:Early postoperative outcome and medi-um-term survival in 540 diabetic and2239 nondiabetic patients undergoingcoronary artery bypass grafting. AnnThorac Surg 74:712–719, 2002
320. Intensive Diabetes Management. 2nd ed.Alexandria, VA, ADA, 1998
321. Etzwiler DD: Diabetes transition: a blue-print for the future. Diabetes Care 17:1–4, 1994
322. Institute of Medicine: Crossing the Qual-ity Chasm: A New Health System for the21st Century. Washington, D.C., Aca-demia Press, 2001
323. Etzwiler DD: Don’t ignore the patients.Diabetes Care 24:1840–1841, 2001
324. Peterson CM, Forhan SE, Jones RL: Self-management: an approach to patientswith insulin dependent diabetes melli-tus. Diabetes Care 3:82–87, 1980
325. Greenfield S, Kaplan SH, Ware JE Jr,Yano EM, Frank HJ: Patients’ participa-tion in medical care: effects on bloodsugar control and quality of life in dia-betes. J Gen Intern Med 3:448–457,1988
326. The Diabetes Control and Complica-tions Trial Research Group (DCCT): Theeffect of intensive treatment of diabeteson the development and progression of
long-term complications in insulin-de-pendent diabetes mellitus. N Engl J Med329:977–986, 1993
327. Bode BW, Steed RD, Davidson PC: Re-duction in severe hypoglycemia withlong-term continuous subcutaneous in-sulin infusion in type 1 diabetes. Diabe-tes Care 19:324–327, 1996
328. Rudolph JW, Hirsch IB: Assessment oftherapy with continuous subcutaneousinsulin infusion in an academic diabetesclinic. Endocrine Practice 8:401–405,2002
329. Anderson JH, Brunelle RL, Keohane P,Koivisto VA, Trautmann ME, Vignati L,DiMarchi R: Mealtime treatment with in-sulin analog improves postprandial hy-perglycemia and hypoglycemia inpatients with non-insulin-dependent di-abetes mellitus. Arch Intern Med157:1249–1255, 1997
330. Anderson JH, Brunelle RL, Koivisto VA,Pfutzner A, Trautmann ME, Vignati L,DiMarchi R: Reduction of postprandialhyperglycemia and frequency of hypo-glycemia in IDDM patients on insulin-analog treatment. Diabetes 46:265–270,1997
331. Lindholm A, McEwen J, Riis AP: Im-proved postprandial glycemic controlwith insulin aspart. Diabetes Care 22:801–805, 1999
332. Raskin P, Guthrie RA, Leiter L, Riis A,Jovanovic L: Use of insulin aspart, a fast-acting insulin analog, as the mealtimeinsulin in the management of patientswith type 1 diabetes. Diabetes Care 23:583–588, 2000
333. Pieber TR, Eugene-Jolchine IE, DerobertE: Efficacy and safety of HOE 901 versusNPH insulin in patients with type 1 dia-betes. Diabetes Care 23:157–162, 2000
334. Ratner RE, Hirsch IB, Neifing JL, GargSK, Mecca TE, Wilson CA: Less hypogly-cemia with insulin glargine in intensiveinsulin therapy for type 1 diabetes. Dia-betes Care 23:639–643, 2000
335. Hermansen K, Madsbad S, Perrild H,Kristensen A, Azelsen M: Comparison ofthe soluble basal insulin analog insulindetemir with NPH insulin: a randomizedopen crossover trial in type 1 diabeticsubjects on basal-bolus therapy. Diabe-tes Care 24:296–301, 2001
336. Rosenstock J, Schwartz S, Clark C, ParkG, Donley D, Edwards M: Basal insulintherapy in type 2 diabetes: 28-weekcomparison of insulin glargine (HOE901) and NPH insulin. Diabetes Care 24:631–636, 2001
337. Rosenstock J, Park G, Zimmerman J:Basal insulin glargine (HOE 901) versusNPH insulin in patients with type 1 dia-betes on multiple daily insulin regimens.Diabetes Care 23:1137–1142, 2000
338. Pfutzner A, Kustner E, Forst T, Schultze-
Schleppinghoff B, Trautmann ME, Hasl-beck M, Schatz H, Beyer J: Intensiveinsulin therapy with insulin lispro in pa-tients with type 1 diabetes reduces thefrequency of hypoglycemia episodes.Exp Clin Endocrinol Diabetes 104:25–30,1996
339. Zinman B, Tildesley H, Chiasson J-L,Tsui E, Strack T: Insulin lispro in CSII:results of a double-blind crossoverstudy. Diabetes 46:440–443, 1997
340. Renner R, Pfutzner A, Trautmann M,Harzer O, Sauter K, Landgraf R: Use ofinsulin lispro in continuous subcutane-ous insulin infusion treatment: results ofa multicenter trial. Diabetes Care 784–788, 1999
341. Warshaw HS, Bolderman KM: Advancedcarbohydrate counting. In Practical Car-bohydrate Counting: A How-to-TeachGuide for Health Professionals. Alexan-dria, VA, ADA, 2001, p. 26–28
342. DAFNE Study Group: Training in flexi-ble, intensive insulin management to en-able dietary freedom in people with type1 diabetes: dose adjustment for normaleating (DAFNE) randomised controlledtrial. BMJ 325:746, 2002
343. Malouf R, Brust JC: Hypoglycemia:causes, neurological manifestations, andoutcome. Ann Neurol 17:421–430, 1985
344. Unger RH: Nocturnal hypoglycemia inaggressively controlled diabetes. N EnglJ Med 306:1294, 1982
345. Ben-Ami H, Nagachandran P, Mendel-son A, Edoute Y: Drug-induced hypo-glycemic coma in 102 diabetic patients.Archives of Internal Medicine 159:281–284, 1999
346. Weston PJ, Gill GV: Is undetected auto-nomic dysfunction responsible for sud-den death in Type 1 diabetes mellitus?The “dead in bed” syndrome revisited.Diabet Med 16:626–631, 1999
347. Cryer PE: Hypoglycaemia: the limitingfactor in the glycaemic management oftype I and type II diabetes. Diabetologia45:937–948, 2002
348. Shilo S, Berezovsky S, Friedlander Y,Sonnenblick M: Hypoglycemia in hospi-talized nondiabetic older patients. J AmGeriat Socy 46:978–982, 1998
349. Fischer KF, Lees JA, Newman JH: Hypo-glycemia in hospitalized patients. N EnglJ Med 315:1245–1250, 1986
350. Gaster B, Hirsch IB: Sliding scale insulinuse and rates of hyperglycemia. Arch In-tern Med 158:95, 1998
351. Young M: Hypoglycaemia; a nursingcare study. Nurs Times 66:915–916,1970
352. Stock PL: Action stat! Insulin shock.Nursing 15:53, 1985
353. Macheca MK: Diabetic hypglycemia:how to keep the threat at bay. Am J Nurs93:26–30, 1993
Management of diabetes and hyperglycemia in hospitals
588 DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004

354. Arbour R: Acute hypoglycemia. Nursing24:33, 1994
355. Swithers C: Avoiding hypoglycemia(comment). Nursing 24:4,6, 1994
356. Parker C: Responding quickly to hypo-glycemia. Am J Nurs 94:46, 1994
357. Schaller J, Welsh JR: Myths & factsabout diabetic hypoglycemia. Nursing24:67, 1994
358. Peragallo-Dittko V: Diabetes 2000: acutecomplications. RN 58:36–41, 1995
359. Reising DL: Acute hypoglycemia: keep-ing the bottom from falling out. Nursing25:41–48, 1995
360. Watters JM, Kirkpatrick SM, HopbachD, Norris SB: Aging exaggerates theblood glucose response to total paren-teral nutrition. Can J Surg 39:481–485,1996
361. Bjerke HS, Shabot MM: Glucose intoler-ance in critically ill surgical patients: re-lationship to total parenteral nutritionand severity of illness. Am Surg 58:728–731, 1992
362. Rosmarin DK, Wardlaw GM, Mirtallo J:Hyperglycemia associated with high,continuous infusion rates of total paren-teral nutrition dextrose. Nutr Clin Pract11:151–156, 1996
363. Park RH, Hansell DT, Davidson LE,Henderson G, Legge V, Gray GR: Man-agement of diabetic patients requiringnutritional support. Nutrition 8:316–320, 1992
364. Woolfson AM: An improved method forblood glucose control during nutritionalsupport. J Parenter Enteral Nutr 5:436–440, 1981
365. Sajbel TA, Dutro MP, Radway PR: Use ofseparate insulin infusions with total par-enteral nutrition.J Parenter Enteral Nutr11:97–99, 1987
366. Hollingdal M, Juhl CB, Dall R, Sturis J,Veldhuis JD, Schmitz O, Porksen N:Glucocorticoid induced insulin resis-tance impairs basal but not glucoseentrained high-frequency insulin pulsa-tility in humans. Diabetologia 45:49–55,2002
367. Boyle PJ: Cushings disease, glucocorti-coid excess, glucocorticoid deficiency,and diabetes. Diabetes Reviews 1:301,1993
368. Lambillotte C, Gilon P, Henquin JC: Di-rect glucocorticoid inhibition of insulinsecretion: an in vitro study of dexameth-asone effects in mouse islets. J Clin Invest99:414–423, 1997
369. Dimitriadis G, Leighton B, Parry-BillingsM, Sasson S, Young M, Krause U, BevanS, Piva T, Wegener G, Newsholme EA:Effects of glucocorticoid excess on thesensitivity of glucose transport and me-tabolism to insulin in rat skeletal muscle.Biochem J 321:707–712, 1997
370. Shamoon H, Soman V, Sherwin RS: The
influence of acute physiological incre-ments of cortisol on fuel metabolism andinsulin binding to monocytes in normalhumans. J Clin Endocrinol Metab 50:495–501, 1980
371. Wachtel TJ, Tetu-Mouradjian LM, Gold-man DL, Ellis SE, O’Sullivan PS: Hyper-osmolarity and acidosis in diabetesmellitus: a three-year experience inRhode Island. J Gen Intern Med 6:495–502, 1991
372. Willi SM, Kennedy A, Brant BP, WallaceP, Rogers NL, Garvey WT: Effective useof thiazolidinediones for the treatmentof glucocorticoid-induced diabetes. Dia-betes Res Clin Pract 58:87–96, 2002
373. Ravina A, Slezak L, Mirsky N, BrydenNA, Anderson RA: Reversal of cortico-steroid-induced diabetes mellitus withsupplemental chromium. Diabet Med16:164–167, 1999
374. Coulston AM: Enteral nutrition in thepatient with diabetes mellitus. Curr OpinClin Nutr Metab Care 3:11–15, 2000
375. Haddad RY, Thomas DR: Enteral nutri-tion and enteral tube feeding: review ofthe evidence. Clin Geriatr Med 18:867–881, 2002
376. Sanz-Paris A, Calvo L, Guallard A,Salazar I, Albero R: High-fat versus high-carbohydrate enteral formulae: effect onblood glucose, C-peptide, and ketonesin patients with type 2 diabetes treatedwith insulin or sulfonylurea. Nutrition14:840–845, 1998
377. Peters AL, Davidson MB, Isaac RM: Lackof glucose elevation after simulated tubefeeding with a low-carbohydrate, high-fat enteral formula in patients with type Idiabetes. Am J Med 87:178–182, 1989
378. Craig LD, Nicholson S, SilVerstone FA,Kennedy RD: Use of a reduced-carbohy-drate, modified-fat enteral formula forimproving metabolic control and clini-cal outcomes in long-term care residentswith type 2 diabetes: results of a pilottrial. Nutrition 14:529–534, 1998
379. Levetan CS, Salas JR, Wilets IF, ZumoffB: Impact of endocrine and diabetesteam consultation on hospital length ofstay for patients with diabetes. Am J Med99:22–28, 1995
380. Koproski J, Pretto Z, Poretsky L: Effectsof an intervention by a diabetes team inhospitalized patients with diabetes. Dia-betes Care 290:1553–1555, 1997
381. Levetan CS, Passaro MD, Jablonski KA,Ratner RE: Effect of physician specialtyon outcomes in diabetic ketoacidosis.Diabetes Care 22:1790–1795, 1999
382. Rafoth RJ: Standardizing sliding scale in-sulin orders. Am J Med Qual 17:175–178, 2002
383. Grol R, Dalhuijsen J, Thomas S, Veld C,Rutten G, Mokkink H: Attributes of clin-ical guidelines that influence use of
guidelines in general practice: observa-tional study. Brit Med J 317:858–861,1998
384. Leape LL, Brennan TA, Laird N, Law-thers AG, Localio AR, Barnes BA, HebertL, Newhouse JP, Weiler PC, Hiatt H: Thenature of adverse events in hospitalizedpatients: results of the Harvard MedicalPractice Study II. N Engl J Med 324:377–384, 1991
385. Leape LL: Error in medicine. JAMA 272:1851–1857, 1994
386. Lesar TS, Lomaestro BM, Pohl H: Medi-cation-prescribing errors in a teachinghospital: a 9 -year experience. Arch In-tern Med 157:1569–1576, 1997
387. Chassin MR: Is health care ready for SixSigma quality? Milbank Quarterly76:565–591, 1998
388. Berwick DM, Leape LL: Reducing errorsin medicine. Brit Med J 318:136–137,1999
389. Richardson WC, Berwick DM, BisgardJC: The institute of medicine report onmedical errors. N Engl J Med 343:663–664, 2000
390. Alberti KGMM: Medical errors: a com-mon problem—it is time to get seriousabout them. Brit Med J 322:501–502,2001
391. Cohen MR, Proulx SM, Crawford SY:Survey of hospital systems and commonserious medication errors. J Health RiskManag 18:16–27, 1998
392. Institute of Medicine, Committee onQuality of Health Care in America: ToErr Is Human: Building a Safer Health Sys-tem. Kohn LT, Corrigan JM, DonaldsonMS, Eds. Washington, D.C., NationalAcademy Press, 1999
393. Cohen MR: Medication Errors. Washing-ton, D.C., Institute for Safe MedicationPractices, American Pharmaceutical As-sociation, 1999
394. Bates DW: Unexpected hypoglycemia ina critically ill patient. Ann Intern Med137:110–116, 2002
395. Piotrowski MM, Hinshaw DB: The safetychecklist program: creating a culture ofsafety in intensive care units. Jt Comm JQual Improv 28:306–315, 2002
396. Adlersberg MA, Fernando S, SpollettGR, Inzucchi SE: Glargine and lispro:two cases of mistake identity. DiabetesCare 25:404–405, 2002
397. Ragone M, Lando H: Errors of insulincommission? Clin Diabetes 20:221–222,2002
398. Crowe DJ: The American Diabetes Asso-ciation should be a leader in reducingmedication errors (Letter). Diabetes Care24:1841, 2001
399. Phelps MR, White SJ: The pharmacist’srole in a team approach for diabetic pa-tient education. Hospital Pharmacy 12:78–80, 1977
Clement and Associates
DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004 589

400. Hawkins DW, Fiedler FP, Douglas HL,Eschbach RC: Evaluation of a clinicalpharmacist in caring for hypertensiveand diabetic patients. Am J Hosp Pharm36:1321–1325, 1979
401. Huff PS, Ives TJ, Almond SN, GriffinNW: Pharmacist-managed diabetes edu-cation service. Am J Hosp Pharm 40:991–994, 1983
402. Ponte CD: Monitoring the patient withdiabetes mellitus: how to avoid medica-tion errors. Hospital Pharm 24:280–283,289, 1989
403. Brient K: Barcoding facilitates patient-focused care. Healthc Inform 12:38,40,42, 1995
404. Leape LL, Cullen DJ, Clapp MD, BurdickE, Demonaco HJ, Erickson JI, Bates DW:Pharmacist participation on physicianrounds and adverse drug events in theintensive care unit. JAMA 282:267–270,1999
405. Hanish LR: Standardizing regimens forsliding-scale insulin. Am J Health SystemPharm 54:1046–1047, 1997
406. Achtmeyer CE, Payne TH, Anawalt BD:Computer order entry system decreaseduse of sliding scale insulin regimens.Meth Inform Med 41:277–281, 2002
407. Spenney JG, Eure CA, Kreisberg RA:Hyperglycemic, hyperosmolar, nonke-toacidotic diabetes: a complication ofsteroid and immunosuppressive ther-apy. Diabetes 18:107–110, 1969
408. Ivanova II, Vasiutkova LA, Ivanov VA:Hyperglycemic coma after corticoste-roid therapy. Sovetskaia Meditsina 10:112–113, 1984
409. Bouhanick B, Biquard F, Hadjadj S,Roques MA: Does treatment with an-tenatal glucocorticoids for the risk ofpremature delivery contribute to keto-acidosis in pregnant women with diabe-tes who receive continuous subcutane-ous insulin infusion (CSII)? Arch InternMed 160:242–243, 2000
410. Brocard H, Akoun G, Grand A: Diabetesteroıde complique d’un coma de typehyperosmolaire. Bulletins et Memoires dela Societe Medicale des Hopitaux de Paris116:353–363, 1965
411. Kumar RS: Hyperosmolar non-ketoticcoma. Lancet 1:48–49, 1968
412. Pyorala K, Suhonen O, Pentikainen P:Steroid therapy and hyperosmolar non-ketotic coma. Lancet 1:596–597, 1968
413. Szewczyk Z, Ratajczyk T, Rabczynski J:Hyperosmotic coma in steroid-induceddiabetes complicating subacute glomer-ulonephritis in a 16-year-old boy. PolskiTygodnik Lekarski 26:1988–1990, 1971
414. Woods JE, Zincke H, Palumbo PJ, John-son WJ, Anderson CF, Frohnert PP,Service FJ: Hyperosmolar nonketoticsyndrome and steroid diabetes. JAMA231:1261–1263, 1975
415. Fujikawa LS, Meisler DM, Nozik RA:Hyperosmolar hyperglycemic nonke-totic coma. Ophthalmology 90:1239–1242, 1983
416. Winterstein AG, Hatton RC, Gonzalez-Rothi R, Johns TE, Segal R: Identifyingclinically significant preventable adversedrug events through a hospital’s data-base of adverse drug reaction reports.Am J Health System Pharm 59:1742–1749, 2002
417. Stagnaro-Green A, Barton M, Linekin P,Corkery E, deBeer K, Roman S: Mor-talilty in hospitalized patients with hy-poglycemia and severe hyperglycemia.Mount Sinai J Med 62:422–426, 1995
418. Roman SH, Linekin PL, Stagnaro-GreenA: An inpatient diabetes QI program. JtComm J Qual Improv 21:693–699, 1995
419. Roman SH, Chassin MR: Windows ofopportunity to improve diabetes carewhen patients with diabetes are hospi-talized for other conditions. DiabetesCare 24:1371–1376, 2001
420. Gilman JA: A quality improvementproject for better glycemic control inhospitalized patients with diabetes. Dia-betes Educ 27:541–546, 2001
421. National health promotion and diseaseprevention objectives, full report withcommentary. In Healthy People 2000.Boston, MA, Jones and Bartlet, 1992, p.462
422. Muhlhauser I, Bruckner I, Berger M,Cheta D, Jorgens V, Ionescu-TirgovisteC, Scholz V, Mincu I: Evaluation of anintensified insulin treatment and teach-ing programme as routine managementof type 1 (insulin-dependent) diabetes:the Bucharest-Dusseldorf Study. Diabe-tologia 30:681–690, 1987
423. Feddersen E, Lockwood DH: An inpa-tient diabetes educator’s impact onlength of hospital stay. Diabetes Educ 20:125–128, 1994
424. Wood ER: Evaluation of a hospital-based education program for patientswith diabetes. J Am Diet Assoc 89:354–358, 1989
425. Shorr RI, Ray WA, Daugherty JR, GriffinMR: Incidence and risk factors for seri-ous hypoglycemia in older persons usinginsulin or sulfonylureas. Arch Intern Med157:1681–1686, 1997
426. Shorr RI, Ray WA, Daugherty JR, GriffinMR: Individual sulfonylureas and seri-ous hypoglycemia in older people. J AmGeriat Soc 44:751–755, 1996
427. American Diabetes Association: Transla-tion of the diabetes nutrition recommen-dations for health care institutions.Diabetes Care 20:106–108, 1997
428. Schafer RG, Bohannon B, Franz M, Free-man J, Holmes A, McLaughlin S, HaasLB, Kruger DF, Lorenz RA, McMahonMM: Translation of the diabetes nutri-
tion recommendations for health careinstitutions. Diabetes Care 20:96–105,1997
429. McMahon MM, Rizza RA: Nutrition sup-port in hospitalized patients with diabe-tes mellitus. Mayo Clin Proc 71:587–594,1996
430. American Diabetes Association: Evi-dence-based nutrition principles andrecommendations for the treatment andprevention of diabetes and related com-plications (Position Statement). DiabetesCare 26 (Suppl. 1):S51–S61, 2003
431. Paddock BW: Carbohydrate counting ininstitutions. Diabetes Spectrum 13:149–152, 2000
432. Wheeler ML: A brave new world for nu-trition and diabetes. Diabetes Care 20:109–110, 1997
433. American Diabetes Association: Transla-tion of the diabetes nutrition recommen-dations for health care institutions(Position Statement). Diabetes Care 26(Suppl. 1):S70–S72, 2003
434. Lewandrowski K, Cheek R, Nathan DM,Godine JE, Hurxthal K, Eschenbach K,Laposata M: Implementation of capillaryblood glucose monitoring in a teachinghospital and determination of programrequirements to maintain quality test-ing. Am J Med 93:419–426, 1992
435. Rumley AG: Improving the quality ofnear-patient blood glucose measure-ment. Ann Clin Biochem 34 (Pt. 3):281–286, 1997
436. Tang Z, Lee JH, Louie RF, Kost GJ: Ef-fects of different hematocrit levels onglucose measurements with handheldmeters for point-of-care testing. ArchPathol Lab Med 124:1135–1140, 2000
437. Atkin SH, Dasmahapatra A, Jaker MA,Chorost MI, Reddy S: Fingerstick glu-cose determination in shock. Ann InternMed 114:1020–1024, 1991
438. Tang Z, Du X, Louie RF, Kost GJ: Effectsof drugs on glucose measurements withhandheld glucose meters and a portableglucose analyzer. Am J Clin Pathol 113:75–86, 2000
439. Nichols JH: A critical review of bloodglucose testing. Point of Care 2:49–61,2003
440. Blake D, Nathan DM: Point-of-care test-ing for diabetes. Point of Care 1:155–164, 2002
441. Jain R, Myers TF, Kahn SE, Zeller WP:How accurate is glucose analysis in thepresence of multiple interfering sub-stances in the neonate? (Glucose analysisand interfering substances). J Clin LabAnal 10:13–16, 1996
442. Bina DM, Anderson RL, Johnson ML,Bergenstal RM, Kendall DM: Clinical im-pact of prandial state, exercise, and sitepreparation on the equivalence of alter-native-site blood glucose testing. Diabe-
Management of diabetes and hyperglycemia in hospitals
590 DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004

tes Care 26:981–985, 2003443. Jones BA, Bachner P, Howanitz PJ: Bed-
side glucose monitoring: a College ofAmerican Pathologists Q-Probes studyof the program characteristics and per-formance in 605 institutions. Arch PatholLab Med 117:1080–1087, 1993
444. Point of Care Blood Glucose Testing n Acuteand Chronic Care Facilities; Approved Guide-line. 2nd ed. Wayne, PA, NCCLS, 2002
445. American Diabetes Association: Eco-nomic costs of diabetes in the U.S. in2002. Diabetes Care 26:917–932, 2003
446. Jonsson B: Revealing the cost of type IIdiabetes in Europe. Diabetologia 45:S5–S12, 2002
447. Jiang HJ, Stryer D, Friedman B, AndrewsR: Multiple hospitalizations for patientswith diabetes. Diabetes Care 26:1421–1426, 2003
448. Selby JV, Ray GT, Zhang D, Colby CJ:Excess costs of medical care for patientswith diabetes in a managed care popula-tion. Diabetes Care 20:1396–1402, 1997
449. Shojana K, Duncan B, Mcdonald K:Making Health Care Safer: A Critical Anal-ysis of Patient Safety Practices. EvidenceReport/Technology Assessment No. 43.Rockville, MD, AHRQ publication no.01-E058, 2001
Clement and Associates
DIABETES CARE, VOLUME 27, NUMBER 2, FEBRUARY 2004 591