Embed Size (px)
Citation preview

Tras los inhibidores de ciclinas.¿Qué quimioterapia y cuándo?
Maria Vidal, MD, PhDMedical Oncology DepartmentTranslational Genomics and Targeted Therapeutics in Solid [email protected]
Viernes , 21 de junio de 2019

Consultancy/speakerPfizer, Lilly, Novartis, Roche, Daiichi
Disclosures

¿Qué quimioterapia y cuándo?




Enfermedad avanzada RE+ Her2 neg
No crisis visceralNo resistencia hormonal
Crisis visceralResistencia hormonal
Quimioterapia (mono/biterapia)Quimioterapia + bevacizumab?
1º línea: HT + Inhibidor Ciclina
Escasa/ No respuestaProgresión visceral
Respuesta mantenidaProgresión no visceral
Valorar ensayo clínicoHT + PI3K/ mTOR...HT...
Algoritmo actual de tratamiento

Datos biológicos de la progresión a inhibidores de ciclinas

50%30%
19%
<1%1%
PrimaryTumor
Tumor Evolution
Treatment
Cejalvo et al. Cancer Treatment Rev. 2018.
MetastasesBrain
Lung
Liver
Bone
Cejalvo et al. Cancer Res.2017
Finn R et al. SABCS 2017
Subtype in HR+/HER2-negative metastatic breast cancer

1. Prat et al. JAMA Oncology 2016
EGF3008 clinical trial (N=644)1 BOLERO-2 clinical trial (N=261)2
HER2-E
Non-HER2-E
0.8
0.6
Surv
ival
Pro
bab
ility
0.4
0.2
0.0
0 10 20 30Months
+ CensoredLogrank P=0.0015
40 50
1.0
Months
0.8
0.6
Ove
rall-
fre
e S
urv
ival
Pro
pro
tio
n
0.4
0.2
0.0
0 10 20 30
P-value <0.0001
40 50
1.0Luminal ALuminal BBasal-likeHER2-enriched
2. Prat et al. The Oncologist 2019
80% of the samples were from the primary tumor
HER2-enriched Subtype and Overall Survival inHR+/HER2-neg Metastatic Breast Cancer (N=905)

mPFS (months)
Palbociclib–letrozole: 24.8
Placebo–letrozole: 14.5
Finn R et al. NEJM 2016
N=455 (68.3%)
Finn R et al. SABCS 2017
50%
30%
19%
N=666
Intrinsic subtype in HR+/HER2-negative metastatic breast cancer (PALOMA-2 retrospective data)

Adapted from Ma et al. Nature Reviews 2015
Figure adapted from Asghar, et al. Nat Rev Drug Dis.
2015;14:130-146
Aleem & Arceci et al.
Front. Cell Dev. Biol 2015
The estrogen receptor (ER) signaling
pathway

The estrogen receptor (ER) signaling pathway
Adapted from Ma et al. Nature Reviews 2015
Estradiol
ERE
AP1 orSP1
CoA C
oA
CoRERE
Transcription
TranscriptionTranscription
Proliferation
PI3K
AKT
mTOR
RAS
RAF
MEK
MAPK
GRFs
GRB2
NOTCH
IGF1R; EGFR; HER2; MET;
FGFR
p38
JNK
CoA
Cytokines; hypoxia; stress
Cytosol
Nucleus

Nicholas C. Turner1, Ben O'Leary1, Ros Cutts2, Yuan Liu3, Sarah Hrebien2, Xin Huang3, Matthew Beaney2, Kerry Fenwick4, Fabrice Andre5, Sibylle Loibl6, Sherene Loi7, Isaac Garcia-
Murillas8, Cynthia Huang Bartlett9, Massimo Cristofanilli10
Cancer Discovery 2018
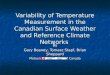
PIK3CA mutations
* both treatment groups combinedp values from McNemar’s test
Day
1
End
of
trea
tmen
t
Genetic landscape of resistance to CDK4/6 inhibition in ctDNA (ctDNA) analysis of the
PALOMA-3 trial
Few mutations acquired:
• RB1 mutations in palbo-arm (4.7%)
• PIK3CA mutations in both arms (8.3%)
• ESR1 mutations in both arms

¿Qué tratamientos reciben las pacientes tras progresión a inh cdk 4/6?

Characteristic
Palbociclib + Fulvestrant
(n=347)
Placebo + Fulvestrant
(n=174)Age, y
Median (min, max) 57 (30, 88) 56 (29, 80)<65, n (%) 261 (75.2) 131 (75.3)65, n (%) 86 (24.8) 43 (24.7)
Race, n (%)White 252 (72.6) 133 (76.4)Asian 74 (21.3) 31 (17.8)Black and other 20 (5.8) 9 (5.2)
Menopausal status at the study entry, n (%) Pre/perimenopausal 72 (20.7) 36 (20.7)Postmenopausal 275 (79.3) 138 (79.3)
Documented sensitivity to prior hormonal therapy, n (%)
Yes 274 (79.0) 136 (78.2)No 73 (21.0) 38 (21.8)
Visceral metastases, n (%) 206 (59.4) 105 (60.3)Prior lines of therapy in the metastatic setting, n (%)
0 74 (21.3) 40 (23.0)1 141 (40.6) 84 (48.3)2 94 (27.1) 37 (21.3)≥3 38 (11.0) 13 (7.5)
Cristofanilli, ESMO 2018
esmo.org
OVERALL SURVIVAL WITH PALBOCICLIB + FULVESTRANT IN WOMEN WITH HORMONE RECEPTOR–POSITIVE, HUMAN EPIDERMAL GROWTH FACTOR RECEPTOR 2–NEGATIVE ADVANCED BREAST CANCER: ANALYSES FROM PALOMA-3
Massimo Cristofanilli,1 Dennis J. Slamon,2 Jungsil Ro,3 Igor Bondarenko,4 Seock-Ah Im,5 Norikazu Masuda,6 Marco
Colleoni,7 Angela DeMichele,8 Sherene Loi,9 Sunil Verma,10 Hiroji Iwata,11 Nadia Harbeck,12 Sibylle Loibl,13 Fabrice
André,14 Kathy Puyana Theall,15 Xin Huang,16 Carla Giorgetti,17 Cynthia Huang Bartlett,18 Nicholas C. Turner19
1Robert H. Lurie Comprehensive Cancer Center of Northwestern University, Feinberg School of Medicine, Chicago, IL, USA; 2David Geffen School of
Medicine at University of California Los Angeles, Santa Monica, CA, USA; 3National Cancer Center, Goyang-si, South Korea; 4Dnipropetrovsk Medical
Academy, City Multiple-Discipline Clinical Hospital #4, Dnipropetrovsk, Ukraine; 5Seoul National University Hospital, Cancer Research Institute, Seoul
National University College of Medicine, Seoul, South Korea; 6NHO Osaka National Hospital, Osaka, Japan; 7Istituto Europeo di Oncologia, Milan, Italy; 8Abramson Cancer Center, University of Pennsylvania, Philadelphia, PA, USA; 9Peter MacCallum Cancer Centre, University of Melbourne, Melbourne,
VIC, Australia; 10Tom Baker Cancer Centre, University of Calgary, Calgary, AB, Canada; 11Aichi Cancer Center Hospital, Nagoya, Japan; 12Brustzentrum
der Universität Muenchen (LMU), Munich, Germany; 13German Breast Group, Neu-Isenburg, Germany; 14Institut Gustave Roussy, Villejuif, France; 15Pfizer Oncology, Cambridge, MA, USA; 16Pfizer Oncology, San Diego, CA, USA; 17Pfizer Oncology, Milan, Italy; 18Pfizer Oncology, Collegeville, PA,
USA; 19Royal Marsden Hospital and Institute of Cancer Research, London, UK
◆ HR+, HER2– ABC◆ Pre/peri- or
postmenopausal ◆ Progressed on prior
endocrine therapy
– On or within 12 months adjuvant
– On therapy for ABC
◆ ≤1 prior chemotherapy regimen for advanced cancer

Palbociclib + Fulvestrant (n=347)
Placebo + Fulvestrant (n=174)
Line of Subsequent Therapy
Treatment, n (%)* First Second Third or Greater First Second
Third or Greater
Any treatment received†
248 182 131 140 113 85
Chemotherapy 138 (56)
133 (73)
121 (92)
87 (62) 76 (67) 76 (89)
Antihormonal 100 (40)
40 (22) 38 (29) 52 (37) 29 (26) 31 (36)
mTOR kinase inhibitor
40 (16) 17 (9) 20 (15) 21 (15) 12 (11) 13 (15)
CDK4/6 inhibitors‡
6 (2) 2 (1) 6 (5) 9 (6) 6 (5) 15 (18)
SYSTEMIC SUBSEQUENT ANTICANCER THERAPIES BY CATEGORY (>10% IN ANY THERAPY LINE)
Cristofanilli, ESMO 2018

Palbociclib–Fulvestrant Group (N = 347) Placebo–Fulvestrant Group (N = 174)
Turner NC, N
Engl J Med 2018;
379:1926-1936
Systemic anticancer therapies received as first, second, and third or greater lines of subsequent treatment by more than 10% of the patients in either trial group who discontinued the intervention.

0 6 12 18 24 30 36 42 48 54
Time (Month)
0
10
20
30
40
50
60
70
80
90
100T
ime t
o C
hem
oth
erap
y P
ro
bab
ilit
y (
%)
Palbociclib+Fulvestrant (N=347) Median TCT=17.6 months 95% CI (15.2, 19.7)Placebo+Fulvestrant (N=174)
Median TCT=8.8 months 95% CI (7.3, 12.7)
HR=0.58395% CI (0.468, 0.727)1-sided p<0.000001
347 254 182 133 99 78 56 41 6PAL+FUL174 91 58 40 22 16 13 10 1PBO+FUL
Number of patients at risk
Time From Randomization to post-progression Chemotherapy (TCT)
Cristofanilli, ESMO 2018

TEST=time to end of subsequent treatment.
0 6 12 18 24 30 36 42 48 54Time (Month)
0
10
20
30
40
50
60
70
80
90
100
Tim
e t
o E
nd
of
Next
Th
era
py P
rob
ab
ilit
y (
%)
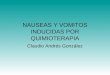
Palbociclib+Fulvestrant (N=347) Median TEST=18.8 months 95% CI (16.4, 20.5)Placebo+Fulvestrant (N=174) Median TEST=14.1 months 95% CI (12.0, 16.7)
HR=0.68495% CI (0.559, 0.836)1-sided p=0.0001
347 305 233 168 124 94 70 55 7PAL+FUL174 135 92 62 36 24 19 13 3PBO+FUL
Number of patients at risk
PFS1(inside trial) + PFS2 (first line post-progression)
Time From Randomization to END OF IMMEDIATE SUBSEQUENT LINE OF THERAPY POSTPROGRESSION (TEST)
Cristofanilli, ESMO 2018

0 5 10 15 20 25 30 35
Time (Month)
mPFS=11.2 mo
mPFS=4.6 mo
mOS=34.9 mo
mOS=28 mo
mTEST=18.8 mo
mTEST=14.1 mo
mTCT=17.6 mo
mTCT=8.8 mo
mTET=11.0 mo
mTET=4.6 mo
MAGNITUDE OF TREATMENT EFFECT WAS MAINTAINED ACROSS ENDPOINTS
6.6 months 6.9 months
PAL+FUL
PAL+FUL
PBO+FUL
PBO+FUL
mOS=median overall survival; mPFS=median progression-free survival.
OS
PFS
Cristofanilli, ESMO 2018

0 5 10 15 20 25 30 35
Time (Month)
mPFS=11.2 mo
mPFS=4.6 mo
mOS=34.9 mo
mOS=28 mo
mTEST=18.8 mo
mTEST=14.1 mo
mTCT=17.6 mo
mTCT=8.8 mo
mTET=11.0 mo
mTET=4.6 mo
MAGNITUDE OF TREATMENT EFFECT WAS MAINTAINED ACROSS ENDPOINTS
6.6 months 6.9 months
PAL+FUL
PAL+FUL
PAL+FUL
PAL+FUL
PBO+FUL
PBO+FUL
PBO+FUL
PBO+FUL
mTCT=median time from randomization to the start of postprogression chemotherapy; mTEST=median time from randomization to the end of the immediate subsequent line of postprogression therapy; mTET=median time from randomization to end of study treatment.
OS
TEST
TCT
PFS
TET
PAL+FUL
PBO+FUL
Cristofanilli, ESMO 2018

Phase III MONALEESA-7 Trial of Premenopausal Patients With
HR+/HER2− Advanced Breast Cancer Treated With Endocrine Therapy ±Ribociclib: Overall Survival Results
Hurvitz, etl al ASCO 2019Dr Sara Hurvitz
1906067504

Ribociclib + ET(n = 335)
Placebo + ET (n = 337)
Age (range), years 43 (25-58) 45 (29-58)
Race, n (%)WhiteAsianBlackOther/unknown
187 (56)99 (30)10 (3)
39 (12)
201 (60)99 (29)
9 (3)28 (8)
ECOG PS, n (%)a
012
245 (73)87 (26)
0
255 (76)78 (23)1 (< 1)
Previous neoadjuvant or adjuvant ET, n (%)NoYes
208 (62)127 (38)
196 (58)141 (42)
Previous chemotherapy for advanced disease, n (%)
47 (14) 47 (14)
Dr Sara Hurvitz
1906067504
Key Patient Baseline Characteristics
Hurvitz, etl al ASCO 2019

Dr Sara Hurvitz
Ribociclib + ET(n = 335)
Placebo + ET(n = 337)
Patients who discontinued study treatment, n
219 280
Any medication, n (%)a 151 (69) 205 (73)
Chemotherapy alone 49 (22) 80 (29)
Chemotherapy + hormone therapy/other
18 (8) 22 (8)
Hormone therapy alone
49 (22) 57 (20)
Hormone therapy + other
31 (14) 41 (15)
Other 4 (2) 5 (2)
• Receipt of any subsequent CDK4/6 inhibitors in patients who discontinued study treatment– Ribociclib arm: 22/219 patients
(10%) – Placebo arm: 52/280 (19%)
First Subsequent Therapy
1906067504
Subsequent Therapies After Treatment Discontinuation
Hurvitz, etl al ASCO 2019

Tripathy, NEJM 2019

Dr Sara Hurvitz
Ribociclib +
ETPlacebo + ET
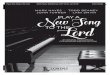
Events/n 95/335 139/337
Median time to
CT, monthsNot reached 36.9
HR (95% CI) 0.596 (0.459-0.774)
Kaplan-
Meier
Estimate
Ribociclib
+ ET
Placebo +
ET
36 months 67.2% 53.8%
42 months 65.8% 49.0%
Landmark Analysis
1906067504
Time to First Subsequent Chemotherapy
Hurvitz, etl al ASCO 2019

Dr Sara Hurvitz
Ribociclib +
ETPlacebo + ET
Events/n 126/335 161/337
Median PFS2,
moNot reached 32.3
HR (95% CI) 0.692 (0.548-0.875)
Kaplan-
Meier
Estimate
Ribociclib
+ ET
Placebo +
ET
36 months 58.4% 46.2%
42 months 54.6% 37.8%
PFS 2: time from randomization to progression on the next line of therapy or death
Landmark Analysis
1906067504
Progression-Free Survival 2
Hurvitz, etl al ASCO 2019

Tolaney, ASCO 2018

Tolaney, ASCO 2018

Time to First Post-discontinuation Chemotherapy
Tolaney, ASCO 2018

Time to the Second Disease Progression or Death
Tolaney, ASCO 2018

Tolaney, ASCO 2018

Tolaney, ASCO 2018

Real world data



QT: 4,6m ET 3,7m


Ciruelos E, Garcia-Saenz JA. SEOM, 2017
Radiografía en España de 1L de QT tras la terapia endocrina
Población Global(167)
Base: Total pacientes en 1ª L de QT tras HT en cada grupo; Unidad: Porcentaje
0,60%
10,…
35,90%
53,40%
Eribulina
Antraciclinas
QT Oral
Taxanos
Eribulina Antraciclinas QT Oral Taxanos
% Pacientes en tratamiento
80%
8,3%
11,7 %
capecitabina capebeva vinorelbina
QT ORAL
(60)
45%
31,5%
21,3%
2,2%
nab-paclitaxel Paclibeva paclitaxel docetaxel
TAX ANO
S
(89)
1L de QT tras terapia endocrina en España

Trials ongoing

• Locally advanced or
Met TNBC and HR+
• Block / 20 slides of
tumor tissue @recurrence
• Rec◆rrences at ≥ 12
months after last dose
of chemotherapy for
early BC
• No prior
Chemotherapy for
LA/MBC
• Candidate for taxane
therapy
• Measurable disease
• PIK3CA/AKT/PTEN-
altered tumor
Targeted Patient
Population
•(Neo)Adjuvant
chemotherapy (Y/N)
•PIK3CA/AKT1/PTEN
alteration status
•Region (APAC/EU/NA/RoW)
•(Neo)Adjuvant
chemotherapy (Y/N)
•Prior PI3K/mTOR
inhibitor (Y/N)
•Region (APAC/EU/NA/RoW)
Paclitaxel 80 mg/m2 (IV
weekly D1, D8 and D15)
+
Placebo (PO daily, D1-21 of
28-day)
(n~67)
Paclitaxel 80 mg/m2
(IV weekly, D1, D8 and D15)
+
Ipatasertib 400mg (PO daily,
D1-21 of 28-day)
(n~134)
Stratification
Factors
A
B
N= 249 TNBC pts
N= 201 HR+ pts
2
1
Randomization
2:1Treatments *
Paclitaxel 80 mg/m2 (IV
weekly D1, D8 and D15)
+
Placebo (PO daily, D1-21 of
28-day)
(n~83)
Paclitaxel 80 mg/m2
(IV weekly, D1, D8 and D15)
+
Ipatasertib 400mg (PO daily,
D1-21 of 28-day)
(n~166)
2
1
Dis
ease
Pro
gre
ssio
n
Post Treatment
Follow Up
• Survival
• Patient Reported
Outcome
• New anti-cancer
therapy + outcomes
• Disease follow-up
(as needed for PFS)
* All patients should receive loperamide (2 mg BID or 4 mg QD) as prophylaxis for diarrhea in the first
cycle, and investigators are encouraged to continue this dosing for the remainder of the study using
their discretion based on clinical judgments – if allowed by local guidance.
IPATUNITY

Targeting non-Luminal disease by PAM50 with Pembrolizumab + Paclitaxel in Hormone Receptor (HR)-positive/HER2-negative advanced/metastatic breast
cancer
TATEN
Primary endpoint
Advanced/metastatic
HR+/HER2-negative
Breast Cancer
HER2-E or Basal-like
(PAM50)
Progression after
CDKinh
1st CT line in
metastatic setting
Pembrolizumab
200mg/kg 3w
+
Paclitaxel 80mg/m2
d1,8,15/21d
Metastatic biopsy: PAM50, DNAseqand ctDNA
Blood samples: Baseline, C2D1, PD
N= 46 (184)
KEY SECONDARY
OBJECTIVES: ORR
according to PD1 expresión, CBR, PFS, DoR, TTP, OS,
Safety,
OR
R
PI: Dr. Aleix PratCo-PI: Dr. Eva Ciruelos
SOLTI: innovative breast cancer research

Conclusiones
• Tras tratamiento con inhibidores de cdk 4/6 laspacientes recibirán QT cuando exista crisis visceral ourgencia de respuesta.
• El tratamiento con inhibidores cdk 4/6 retrasa eltiempo al inicio de la QT.
• Valorar tipo QT en función de QTs previas recibidas,comorbilidades y preferencias de la paciente(capecitabina, paclitaxel).
• Valorar inclusión de pacientes en estudios clínicos.