Embed Size (px)
Citation preview

Transulnar AccessTransulnar Access
Ugo LimbrunoUgo Limbruno
Cardiovascular Department, ASL 6 Livorno, ItalyCardiovascular Department, ASL 6 Livorno, Italy

Why Transulnar?Why Transulnar?
Limitations of transradial access: rate
• Insufficient collateral circulation 5-10%
• Anatomic variations (radial loop, high take-off) 8-10%
• Technical failures 2-3%
• Radial artery occlusion 3-5%
• Radial artery as a graft conduit… -
Limitations of transradial access: rate
• Insufficient collateral circulation 5-10%
• Anatomic variations (radial loop, high take-off) 8-10%
• Technical failures 2-3%
• Radial artery occlusion 3-5%
• Radial artery as a graft conduit… -

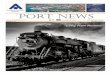
Diffuse narrowing of radial artery after repeat procedures
Diffuse narrowing of radial artery after repeat procedures
Yoo et al, Catheter Cardiovasc Interv 2003;58:301
Would you use it as a graft?Would you use it as a graft?

Transulnar: a Medline scanTransulnar: a Medline scan
Keywords: “transulnar” & “coronary”
• Terashima et alCatheter Cardiovasc Interv 2001;53:410-4
• Dashkoff et al Catheter Cardiovasc Interv 2002;55:93-6
• Limbruno et alCatheter Cardiovasc Interv 2004;61:56-9
• Lanspa et alCatheter Cardiovasc Interv 2004;61:211-3
Keywords: “transulnar” & “coronary”
• Terashima et alCatheter Cardiovasc Interv 2001;53:410-4
• Dashkoff et al Catheter Cardiovasc Interv 2002;55:93-6
• Limbruno et alCatheter Cardiovasc Interv 2004;61:56-9
• Lanspa et alCatheter Cardiovasc Interv 2004;61:211-3
9 coro
3 coro, 2 PCI
13 primary PCI
1 coro
9 coro
3 coro, 2 PCI
13 primary PCI
1 coro

Transulnar safety-feasibility:
a single-center prospective study
Transulnar safety-feasibility:
a single-center prospective study
• Site: Cardiovascular Dpt, Livorno, Italy.
• Population: 307 consecutive pts (224 M, 69±8 yrs) referred for elective coronary
angiography and/or PCI (April ’04 - Aug ‘04).
• Screening: 1) Modified Allen’s Test, bilateral2) Ulnar artery palpability, bilateral3) Reverse Modified Allen’s Test.
• Site: Cardiovascular Dpt, Livorno, Italy.
• Population: 307 consecutive pts (224 M, 69±8 yrs) referred for elective coronary
angiography and/or PCI (April ’04 - Aug ‘04).
• Screening: 1) Modified Allen’s Test, bilateral2) Ulnar artery palpability, bilateral3) Reverse Modified Allen’s Test.
Submitted

Transulnar feasibility: different strategies
Transulnar feasibility: different strategies
1. “1st CHOICE” STRATEGY: Transulnar in all patients with palpable ulnar artery and neg. reverse Allen test, regardless of the radial artery availability.
2. “2nd CHOICE” STRATEGY: Transulnar in patients with pos. Allen test, palpable ulnar artery and neg. reverse Allen test.
3. “CROSS-OVER” STRATEGY: Transulnar in case of transradial failure.
1. “1st CHOICE” STRATEGY: Transulnar in all patients with palpable ulnar artery and neg. reverse Allen test, regardless of the radial artery availability.
2. “2nd CHOICE” STRATEGY: Transulnar in patients with pos. Allen test, palpable ulnar artery and neg. reverse Allen test.
3. “CROSS-OVER” STRATEGY: Transulnar in case of transradial failure.

Transulnar feasibility: a prospective study
Transulnar feasibility: a prospective study
Two different strategies: Two different strategies:
• “1st choice” strategy (applied)
• “2nd choice” strategy (retrospective)

+ _
307 pts307 pts
Allen test(cut-off 7sec)Allen test(cut-off 7sec)
+ _
Ulnarpalpability
Ulnarpalpability
RadialRadialFemoralFemoral
ReverseAllen testReverse
Allen test_ +
UlnarUlnar
“2nd choice” strategy (retrospective)“2nd choice” strategy (retrospective)
12%12% 88%88%
5%5% 7%7%
5%5% 0%0%

_
307 pts307 pts
Ulnar palpableUlnar
palpable
+ _
ReverseAllen testReverse
Allen test
RadialRadialFemoral(radial control.)
Femoral(radial control.)
Ulnar accesssuccessful
Ulnar accesssuccessful
+ _
UlnarUlnar
60%60% 40%40%
59%59% 1%1%
48%48%
Allen test(cut-off 7sec)Allen test(cut-off 7sec)
+
_+ 36%36%16%16%
“1st choice” strategy (applied)“1st choice” strategy (applied)

Ulnar(n=181)
Radial(n=110)
6F/7F 141/6 97/4
Artery access rate 81% 98%
Aortic access 81% 95%
PCI 37% 39%
PCI procedural success 98% 98%
Transulnar feasibility: “1st choice” strategy
Transulnar feasibility: “1st choice” strategy
P<0.05 vs radial
* *
* *

0
2
4
6
8
10
12
14
Tim
e (
min
)
Sheathinsertion
Coronarycannulation
Fluoroscopy
Ulnar Radial
p<0.05p<0.05
Transulnar feasibility: time consumption
Transulnar feasibility: time consumption

Ulnar(n=181)
Radial(n=110)
AV fistulae/pseudoaneurism - -Nerve injury - -Hand ischemia - -Artery occlusion / flow reduction
11 (6%) 4(4%)
Severe hematoma 1(0,6%) -
Slight hematoma 10(5%) 3(3%)
Transulnar safetyTransulnar safety

Transulnar: technical issuesTransulnar: technical issues
• CORDIS Radial Kit (6F, 11cm) orTerumo Radifocus II
• Bare needle 21G (very mobile/deep artery!)
• 0.021 metal wire, in case of failure 0.014 “J-ed” coronary guidewire.
• Cocktail: verapamil 2,5 mg + heparin 5000 UI.
• CORDIS Radial Kit (6F, 11cm) orTerumo Radifocus II
• Bare needle 21G (very mobile/deep artery!)
• 0.021 metal wire, in case of failure 0.014 “J-ed” coronary guidewire.
• Cocktail: verapamil 2,5 mg + heparin 5000 UI.

81%success81%success
98%success
98%success
Transulnar: technical issuesTransulnar: technical issues

RARA
UAUAUAUA0%failure0%failure
3%failure
3%failure
RA anatomic variations: 9%RA anatomic variations: 9%RA-UA: similar size
Transulnar: technical issuesTransulnar: technical issues
recu
rrent R
A
recu
rrent R
A

Pts(n)
Accessrate
Occlusion
Nerve injury
A-VFistul
a
Hematoma
Sun et alTCT’04
40 100% 0 0 0 0
Aptecar et alTCT ‘04
186 94 % 2 % 0 0,5 % 0
Limbruno et alSubmitted
181 81% 6 % 0 0 0,6 %
Limbruno et alCCI 2003;61:56-9
13 77 % 0 0 0 0
Dashkoff et alCCI 2002;55:93-6
5 - - 0 0 0
Terashima et alCCI 2001;53:410-4
9 78 % 0 0 0 0
Total 434 88 % 3 % 0 0,2 % 0,2 %
Transulnar: a comprehensive overview
Transulnar: a comprehensive overview
Echo-selection for:•Radial anatomic
variations•Ulnar larger than radial

Transulnar: which strategy? (if any)Transulnar: which strategy? (if any)
1. “1st choice” strategy: might be of limited value due to a somewhat lower artery access rate with respect to transradial.
1. “1st choice” strategy: might be of limited value due to a somewhat lower artery access rate with respect to transradial.
3. “2nd choice” + Echo: as in #2, and in pts with unfavourable radial anatomic variations detected by a pre-procedural echo.
2. “2nd choice” strategy: might slightly increase the feasibility of wrist access in pts with inadequate Allen test.
2. “2nd choice” strategy: might slightly increase the feasibility of wrist access in pts with inadequate Allen test.
+4%+4%
Wrist accessWrist access
+6%?+6%?
-6%-6%