Embed Size (px)
Citation preview
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 1
publiziert bei:
AWMF-Register Nr. 182/001 Klasse: S2e
In-flight Cardiopulmonary Resuscitation during Commercial Air Transport: Consensus statement and Supplementary Guideline from the German
Society of Aerospace Medicine (DGLRM)
Jochen Hinkelbein 1,2,3, * Lennert Böhm 1
Stefan Braunecker 1,2,4 Harald V. Genzwürker 5
Steffen Kalina 2,3
Fabrizio Cirillo 3,6 Matthieu Komorowski 7
Andreas Hohn 3 Jörg Siedenburg 8
Michael Bernhard 9 Ilse Janicke 2,10
Christoph Adler 11 Stefanie Jansen 12
Eckard Glaser 1,2,13 Pawel Krawczyk 14
Mirko Miesen 15 Janusz Andres 14
Edoardo De Robertis 6 Christopher Neuhaus 1,2,16
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 2
Affiliations
* Chairman of the task force 1 Working group “guidelines, recommendations, and statements”, German Society of Aviation and Space Medicine, Munich, Germany 2 Working group “emergency medicine and air rescue”, German Society of Aviation and Space Medicine, Munich, Germany 3 Department of Anaesthesiology and Intensive Care Medicine, University Hospital Cologne, Cologne, Germany 4 Department of Critical Care, King's College Hospital, London, UK 5 Department of Anaesthesiology, Neckar-Odenwald-Kliniken, Buchen & Mosbach,
Germany 6 Department of Neurosciences, Reproductive and Odontostomatological Sciences,
University of Naples “Federico II”, Via S. Pansini, 5 – 80131 Napoli, Italy 7 Department of Surgery and Cancer, Faculty of Medicine, Imperial College London, UK 8 Uetersen, Germany 9 Emergency Department, University of Leipzig, Germany 10 Department for Cardiology and Angiology, Heart Center Duisburg, Evangelisches Klinikum Niederrhein, Duisburg, Germany 11 Department of Internal Medicine III, Heart Center of the University of Cologne, Cologne, Germany 12 Department of Otorhinolaryngology, Head and Neck Surgery, University of Cologne, Cologne, Germany 13 Gerbrunn, Germany 14 Department of Anaesthesiology and Intensive Therapy, Jagiellonian University,
Cracow, Poland 15 YourCockpit Flight Simulator, Cologne, Germany 16 Department of Anaesthesiology, University Hospital Heidelberg, Heidelberg, Germany
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 3
Corresponding author:
Jochen Hinkelbein, MD, DESA, EDIC, FAsMA Department of Anaesthesiology and Intensive Care Medicine
University Hospital Cologne 51149 Cologne
Germany Phone: +49 171 8231385
E-Mail: [email protected]
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 4
Abstract
Background: Approximately 3 billion people worldwide will travel by commercial air
transport in 2016. A calculation based on the number of passengers transported shows that between 1 out of 14,000 to 1 out of 50,000 passengers will experience
acute medical problems during a flight. Cardiac arrest accounts for 0.3% of all in-flight medical emergencies, yet it is responsible for 86% of in-flight events resulting
in death. So far, no guideline for in-flight cardiac arrest (IFCA) does exist providing specific treatment recommendations.
Methods: A task force was created to develop a guideline for the treatment of in-flight cardiac arrest based on clinical and investigational expertise in this area. By
using a systematic literature search including GRADE, RAND, and DELPHI methods, specific recommendations for the treatment of IFCA have been created.
Results and conclusions: Several main recommendations have been developed:
emergency equipment location as well as content should be mentioned in the pre-flight safety announcement; ECG should be available for patients with cardiac arrest,
it is very important to request help by an on-board announcement after identification of a patient with cardiac arrest; two-person CPR is considered optimum and should
be performed if possible; the crew should be trained regularly in basic life support – ideally with a focus on CPR in aircraft; a diversion should immediately be performed
if the patient has a return of spontaneous circulation.
Key-words:
CPR; cardio-pulmonary resuscitation; cardiac arrest; airplane; in-flight medical emergencies; BLS; AED
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 5
Background
In 2016, approximately 3 billion people worldwide will travel by commercial air transport 1 including more than 1 billion tourists 2. Although air travel is safe in
general, passenger demographics and pre-existing medical conditions as well as the number of passengers aboard larger aircraft (e.g. Airbus A380) and flights over very
long distances 3 raise the probability of in-flight emergencies per flight. Therefore, medical issues during air travel of passengers have attracted increasing interest in
recent years 2, 4. Depending on the destination, 22 to 64% of travellers report some illness 2.
Although in-flight medical emergencies frequently occur in commercial airline operations, detailed data on incidence, causes, and consequences still remain limited 5-7. This area of emergency medicine is rarely investigated scientifically, or even published so far 4, 8, 9. A calculation based on the number of passengers transported
shows that between 1 out of 14,000 to 1 out of 50,000 passengers will experience
acute medical problems during a flight 5-7. However, most emergencies are mild, self-limited and can be treated effectively and definitively on board with little or no
equipment and without interruption of the flight 10. Severe disorders occur infrequently and fatalities are very rare 11. However, diversions and unplanned
landings are quite expensive and require sophisticated management of the remaining passengers.
Sudden cardiac arrest remains a leading cause of death throughout the world 12. In a recent study, Nable et al. 13 found that cardiac arrest accounts for only 0.3% of all
in-flight medical emergencies, yet it is responsible for 86% of in-flight events resulting in death 11. Unfortunately, cardiac events during commercial aviation are
not that infrequent 8, and result in a high percentage of in-flight mortality 14, 15. Cardiac arrest on board has an incidence of 1 per 5-10 million passenger flights with
about 1,000 persons deaths annually aboard International Airlines Transport Association (IATA) carriers 16, 17.
Current cardiopulmonary resuscitation (CPR) guidelines by the American Heart Association (AHA) 18 and the European Resuscitation Council (ERC) 17, 19 only provide
general recommendations for cardiac arrests in transportation vehicles and in-flight
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 6
medical emergencies aboard airplanes. However, these guidelines are for general
purpose and do not consider the specificities of the aviation-/airplane-related setting. Furthermore, aviation-specific management of cardiac arrest during flight is not
sufficiently addressed in the published literature.
Despite a few previous studies on this topic 20 and some recommendations in the
current ERC 17 or AHA 18 guidelines for CPR no sound or extensive recommendations are available yet how to handle patients with an in-flight cardiac arrest (IFCA).
The objective of this consensus statement and supplemental guideline is to analyse published literature and to derive evidence-based and expert-opinion
recommendations addressing specifically in-flight cardiopulmonary resuscitation after sudden cardiac arrest in (commercial) airplanes.
Methods
Literature evaluation strategy
A task force was created to develop a guideline on the treatment of in-flight cardiac arrest based on clinical and investigational expertise in this area. A set of questions
and keywords was prepared by the taskforce to guide the literature search. These were first drafted and then validated by the chairmen of the taskforce and literature
reviewers.
The chairmen of the taskforce also established the inclusion criteria for the studies
according to the search terms listed in table 1. This process was started in January 2015 and completed in September 2015. The final literature search was conducted
between September 2015 and December 2015. A broad filter for cardiac arrest in airplanes was applied in conjunction with a study type filter and a specific subgroup
filter based on the questions and keywords. MEDLINE, EMBASE and Cochrane Library were searched from January to December 2015 for normalized and free-text terms
such as “cardiac arrest” etc. (search strategy: table 1). A total of 2,387 records were identified. Articles identified went through a two round selection process described
below.
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 7
First, title and abstract screening removed duplicates and papers selected according
to the inclusion criteria defined previously. This process was conducted by a systematic screening and, when in doubt, checked by a second reviewer. Systematic
reviews, randomized controlled trials, cohort studies, case control studies, and cross sectional surveys were included. Existing guidelines were identified and considered
separately. Narrative reviews, editorials, case series or case reports were excluded. Only publications in English were included.
Full-text versions of the remaining articles were obtained and divided amongst the authors for further screening using the aforementioned criteria. The articles were
checked individually for risk of bias, applicability and significance. In the final set of articles, evidence gathered was critically appraised using the GRADE methodology 21.
As GRADE was used to assess the quality of the evidence, the following features were assessed for each outcome. GRADE was based on study design limitations
(selection, performance, detection, attrition and reporting bias), effect consistency
and size, directness, precision, publication bias, dose response effect and presence of antagonistic bias. The GRADE system has not standardized this decision-making
process of the expert panel. In an effort to standardize this evidence processing, the methodology committee of this working group selected the Rand Appropriateness
Method (RAM) 22.
For consensus, when strong evidence was lacking, a three round Delphi method was
used 23. Voting was performed by e-voting for the first, second, and third rounds. The experts formulated draft recommendations before each conference to serve as a
foundation for subsequent discussion and evaluation. The expert panel was updated through short presentations about the literature search results and subsequent
interpretation for drafting of the proposed recommendations. After a single round of face-to-face debating, anonymous voting rounds were conducted, followed
subsequently by internet-based voting rounds. This process provided a structured and validated method for expert panel activities.
In addition, it standardized statistical methodology for determining the degree of agreement to serve as a foundation for deciding about the recommendation grade
(weak, intermediate, and strong consensus). A strong consensus was defined as an
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 8
agreement of >90%, an intermediate consensus with 70-90% agreement, a weak
consensus with 50-70% agreement, and no consensus as <50%. After preparation of the final manuscript with all recommendations included, it was
sent to the board of the society (DGLRM) for approval. This guideline is based on a consensus of an expert group corresponding to level S2e of the classification levels
of the Association of the Scientific Medical Societies in Germany (AWMF, Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften e. V.,
see www.awmf.org) with the identification number #182-001.
Guidelines for IFCA Background
According to the International Civil Aviation Organization (ICAO) and other sources of information, in the year 2016 approximately 3.2 billion people worldwide travel by air 1, 3, 11, 24. Although this mode of transportation is quite safe from a technical point of
view, passengers with all their pre-existing individual health issues (e.g., age, pre-existing diseases, obesity, or the onset of new acute issues) are increasingly at risk
of becoming a patient during flight.
In-flight cardiac arrest (IFCA) is a rare phenomenon (0.3% of in-flight medical
emergencies) during commercial air travel, but represents a relevant cause of in-flight medical emergencies 16 and is a major contributor to in-flight deaths. It has an
incidence of 1 per 5-10 million passenger flights 17 and each year, about 1,000 persons die aboard International Airlines Transport Association (IATA) carriers 16, 17.
Irrespective of the cause of cardiac arrest, early recognition and calling for help, treatment including appropriate management of the deteriorating patient, early
defibrillation, high-quality cardiopulmonary resuscitation (CPR) with minimal interruption of chest compressions and treatment of reversible causes, are the most
important interventions 17, 18. Especially in the remote environment of an aircraft, these guidelines require adaption, modification, and supplementation to ensure the
best possible outcome for patients. Current CPR guidelines by the American Heart Association (AHA) 18 and the European Resuscitation Council (ERC) 17, 19 are for
general purpose and do not consider the particular aviation-/airplane-related setting.
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 9
The present consensus statement and guideline from the German Society for
Aerospace Medicine (DGLRM) addresses aviation-specific management of in-flight cardiac arrest patients. Recommendations are displayed condensed as a summary in
table 2.
General recommendations Emergency equipment location as well as major content has to be
mentioned in the pre-flight safety announcement (strong consensus, Level of Evidence low, Grade of Recommendation A).
Information on the location of emergency medical equipment as well as
brief information on how to act in case of a cardiac arrest must be printed
on the seat pocket Safety Instructions card (strong consensus, Level of Evidence high, Grade of Recommendation A).
Several considerations are important to improve the access to both equipment and
patients available to reduce no-flow-time and improve outcome of patients suffering from an IFCA.
Infrastructure and fast access to emergency equipment can reduce the time lag to adequate therapeutic attempts and decrease no-flow-time significantly. Since all
passengers and crew members on-board are potential bystanders, all should know exactly where emergency equipment and crew are located. Besides some general
information in the pocket safety cards, the location of emergency equipment should be mentioned in the pre-flight safety announcement.
It is of crucial importance that (professional) help is requested by an on-
board announcement after identification of a patient with cardiac arrest (strong consensus, Level of Evidence low, Grade of Recommendation A).
In the event of a passenger medical incident, there can be delays of more than 20
minutes to several hours before expert assistance is available and the availability of
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 10
medically trained persons on-board cannot be entirely relied upon 25. Many crew
members as well as health care providers may require additional support or help to decide on complex cases or in exceptional circumstances.
Teleconsultation should be available during the flight (intermediate
consensus, Level of Evidence low, Grade of Recommendation B).
Teleconsultation consists of a well-trained specialist on ground that could be called in case of any problems via satellite phone, video or radio communication. This service
should be available 24/7 and is usually offered by airlines or affiliated companies. Especially for severe cases in remote locations teleconsultation has advantages.
Besides giving advice, telephone-CPR could also be performed. Recent studies showed that this service is beneficial throughout the world and can save lives 26-28.
Medical consultation or teleconsultation should likely be obtained once a perfusing
rhythm has been established or in cases of prolonged resuscitation 12.
It is important that a standardized documentation form is available (strong consensus, Level of Evidence low, Grade of Recommendation A).
Data recently published on in-flight medical events are based mainly on figures
gathered by individual airline companies and had been collected retrospectively 3, 29-
31. These results are often limited and might be biased due to the relatively small
number of transportations per airline. Furthermore, most of the published data are based on retrospective analyses and no valid data on the worldwide incidence are
available. Data from prospective studies remains to be published 5. Studies on emergency medical equipment show a clear inconsistency in the medical
equipment 6, 7. However, these data may only be interpreted thoroughly if the incidence and nature of in-flight medical emergencies are taken into account.
Therefore, a valid database on world-wide in-flight medical emergency is essential but does not exist yet, unfortunately. Another challenging problem besides the lack
of standardized documentation during or after an international in-flight medical emergency, is the absence of denominator data, e.g. to calculate incidences or rates 32. Analysing absolute numbers only, severely limits data interpretation 5.
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 11
Without having sound numerator data and valid denominators 32 progress in this field
is very limited 5. Therefore, there is a clear necessity to achieve more accurate scientific results in this field by gathering conclusive data and to document findings in
a standardized form. The DGLRM provides a standardized documentation form 33.
CPR- and other emergency medical data can be registered in a standardized international data base (weak consensus, Level of Evidence
low, Grade of Recommendation B)
Besides data documentation in a standardized form, data collection in an (international) data base is of utmost importance to produce high numbers and to
facilitate benchmarking, data analyses and international comparisons as well. For the time being no data-base or registry exist 5. All flight services should be committed to
report their proper data sets to this international registry.
Emergency equipment For commercial airline transport, legal requirements define required emergency
medical equipment on-board aircraft. A minimum standard for medical emergency material is defined by national or international regulations 34. Therefore, all
commercial aircraft have to be equipped with a first aid kit (FAK) that all cabin crew members are trained to use. The FAK is suited to cover most minor illnesses, e.g.,
nausea, headache, or dyspepsia. In addition, aircraft equipped with more than 30 seats, must be equipped with a
(special) medical kit which can be used by competent personnel (e.g., health care providers, physicians; i.e., doctor’s kit, DK) 4. In these kits, besides equipment and
medication, generally recommended the contents may be chosen by special requirements of the companies or by suggestions from their medical advisors.
Intravenous medication as well as material required for intravenous access is often provided in a doctor’s kit. Unfortunately, the contents of these additional kits vary
significantly throughout Europe 6-9, 35.
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 12
Since data on in-flight emergencies is rarely published, it is not possible to
adequately assess the usefulness of the material provided 3, 5, 6, 24. However, both supplementary material/devices as well as drugs may be necessary for proper patient
management. It is of utmost importance that all medical equipment must be certified for storage as
well as fully operational at the ambient conditions experienced on-board aircraft at the highest altitude the aircraft is certified to operate at or at the actual cabin
pressure resulting during flight.
An ECG should be available for patients with cardiac arrest (strong consensus, Level of Evidence moderate, Grade of Recommendation A).
Measurement of blood pressure by non-invasive devices (NIBP) as well as continuous
electrocardiography (ECG) is considered a minimal requirement for emergency
patients. Although there is a lack of randomized controlled trial (RCT) literature to underscore this statement, it is supported by the working group and several other
non-RCT publications. As an alternative to an ECG, an automatic external defibrillator (AED) with monitoring function on-board the aircraft is considered adequate,
especially for patients suffering from an IFCA.
A defibrillator (e.g. AED) is considered essential and should be available during the flight (strong consensus, Level of Evidence moderate, Grade of
Recommendation B).
Early defibrillation including the early use of AEDs by both emergency responders and trained health care providers improved outcome of resuscitated patients 12. Many
airlines have recognized that survival of cardiac arrest depends on early access to CPR and defibrillation and therefore have placed AEDs on board long-haul aircraft 25.
Furthermore, the Federal Aviation Administration (FAA) mandated as part of its 2001 safety guidelines that by 2004 all commercial airlines carry AEDs and train personnel
in their use 12. According to the ERC guidelines for CPR, an AED and a first aid kit should be
requested immediately from cabin crew 17, 19. Since time to defibrillation is one of the
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 13
most important factors for survival after cardiac arrest 16, basic life support should,
therefore, be performed as soon as possible 19. Furthermore, the Federal Aviation Administration require all airlines flying into the United States to carry Automated
External Defibrillators 25. According to EASA regulations the carriage of an AED is subject to the risk assessment of the pertinent airline. The needs of the pertinent
operations should be taken into account 36. A shockable rhythm is present in 25-31% of patients and the in-flight use of an AED
can result in an increased overall survival rate (33-50% survival to hospital discharge) 12, 17. However, recently published data shows that an AED was used
rarely (in only in 0.4% of patients having an in-flight medical problem) 37. Per se, AED use is possible during flight but crew and pilots should be informed 38.
The use of the AED aboard commercial aircraft is effective, with an excellent rate of survival to discharge from the hospital after conversion of ventricular fibrillation 39.
There are not likely to be complications when the device is used as a monitor in the
absence of ventricular fibrillation 39.
An intravenous access is considered essential and should be available during the flight (strong consensus, Level of Evidence low, Grade of
Recommendation B).
An intravenous access is standard for drug application and adrenaline injection during CPR 6, 7 and is usually provided in the doctor´s kit 19. However, according to
EASA regulations, intravenous access should be carried within the Emergency Medical Kit 36.
Providing intraosseous access may be necessary and the device must be
available (consensus, Level of Evidence low, Grade of Recommendation A).
In cases when an i.v.-line cannot be placed timely or within a few attempts, the intraosseous (i.o.) route is an appropriate alternative 19. For intraosseous access
specific needles are required. Whereas semi-automatic drilling needles are standard in most EMS systems, the devices are heavy and the use of lithium ion batteries
being extremely problematic in an airplane. Automatic needles have the risk of failure
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 14
and injury. Therefore, a “cook needle” is the best alternative in this very special
setting for intraosseous access.
For CPR, epinephrine (adrenaline), amiodarone, lignocaine (lidocain), glucose, and midazolam must be available (strong consensus, Level of
Evidence moderate, Grade of Recommendation A).
For CPR, and resulting arrhythmias it is of utmost importance to have required drugs in an intravenous formulation available for injection. As in current CPR guidelines
recommended 19, the following drugs should be available on-board (e.g., in the
doctor´s kit): epinephrine (adrenaline) [at least 5x 1mg], amiodarone [at least 3x
150 mg], glucose [at least 10 g], and midazolam [at least 2x 5 mg]. Alternatively to
amiodarone, lignocaine (lidocain) [at least 100 mg] can be used.
Mechanical CPR devices may facilitate CPR in special situations, but are
considered inappropriate during flight (strong consensus, Level of Evidence low, Grade of Recommendation C).
Mechanical devices for CPR are standard in many EMS systems and can be used in
special circumstances, e.g., long transportation during CPR. However, the weight of these devices is high and their use on-board an aircraft may be extremely rare.
Therefore, it is considered not useful to have such devices on-board commercial aircrafts.
Pulse oximetry is considered standard (“basic monitoring”) and should be
available for treatment (strong consensus, Level of Evidence B, Grade of Recommendation B). Non-invasive blood pressure measurement devices
are considered standard (“basic monitoring”) and must be available for treatment (strong consensus, Level of Evidence moderate, Grade of
Recommendation A).
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 15
In addition to NIBP and ECG, pulse oximetry is also considered as a minimal standard
for emergency patients. Pulse oximetry (SpO2) monitoring and oxygen supplementation are used to detect and correct hypoxemia in emergency patients.
Since improvements were made in pulse oximetry technology by Takuo Aoyagi, it has become a standard monitoring technique in emergency medical treatment of
severely ill or injured patients 40, 41. Pulse oximetry can enhance patient safety due to its ability to detect hypoxia earlier than other methods 40, 42. There are mainly three
sensor sites used (finger, toe, ear) all with a comparable accuracy 40. However, regarding pulse oximetry, it should be recognized that some influencing
factors may lead to false measurements. Influencing factors such as changes in the measurement kinetics or perfusion can lead to an aberration of the pulse wave signal
and therefore inaccurate readings 42.
The use of capnometry/capnography is marginally important during an in-
flight cardiac arrest. At the minimum a (simple) qualitative capnometer should be available (weak consensus, Level of Evidence low, Grade of
Recommendation B).
Monitoring of end-tidal carbon dioxide (etCO2) levels is standard care for cardiac arrest patients after endotracheal intubation and in spontaneous breathing patients 19. The use of capnometry/capnography can reduce the risk of undetected oesophageal intubation and reflect the quality of the CPR. Since the incidence of
endotracheal intubation during flight is low, a quantitative measurement is often not necessary. However, at least qualitative measurements should be available since
they are easy, cheap, and light-weight.
Using a glucometer for glucose measurements is important during/after CPR and the device must be available (weak consensus, Level of Evidence
moderate, Grade of Recommendation A).
During and after CPR, serum glucose levels may vary substantially. To prevent severe hypoglycemia and hyperglycemia, blood glucose levels should be measured
during and after CPR.
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 16
CPR strategies Bystander CPR enhances the survival rate significantly and should be performed as soon as possible 18, 19. If a cardiac arrest is recognized, professional help should also
be sought immediately. Crew is sometimes reluctant to use on-board announcements requesting a healthcare provider for an emergency, since this may disturb
passengers and produce unwanted attention. However, in the event of a cardiac arrest, all help should be gathered as soon as possible. The easiest and most
effective way is an on-board announcement.
Two-person CPR is considered optimum (strong consensus, Level of Evidence moderate, Grade of Recommendation A).
Ideally, CPR (both BLS and ALS) is performed by at least two people according to the current CPR guidelines 18, 19. Every 2 minutes a rotation between bystanders/crew
should be performed to prevent exhaustion and reduced effectiveness 18, 19, 43.
Overhead-CPR and telephone-CPR may be performed during resuscitation (weak consensus, Level of Evidence low, Grade of Recommendation C).
Chest compression during transportation seems to be feasible and efficient 44.
However, infrastructure and environmental factors can substantially interfere with the execution of CPR procedure 45. For example, in the confined space of an aircraft,
access to the patient may be reduced or nearly impossible. There are situations when cardiac arrest may occur in a confined space, making it difficult to kneel by the
side of the patient 46 (fig. 1). In the confines of an aircraft aisle, it may be difficult to perform standard CPR with one or two rescuers kneeling at the side of the patient 46.
There is a paucity of data on this topic, e.g. in helicopters during flight, and quality of chest compressions is inferior to other emergency scenarios if applied during flight 44,
45. Havel et al. 44 demonstrated that closed chest compression can generally be applied during transport but there may be at least some differences in effectiveness.
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 17
Optimally, the rescuer should be positioned in front of one of the aisle seats in the
kneeling position for performance of chest compressions, and a second rescuer in front of the opposite aisle seat performing ventilation or applying the AED to the
patient. The limitations would be the small space for either rescuer to perform their tasks 16.
In situations where it is not possible to perform standard CPR according to the CPR guidelines 19, over-the-head-CPR (OTH-CPR) may be considered as a suitable
alternative 47 (fig. 2). The ERC guidelines recommend considering an over-the-head technique for CPR if access precludes conventional CPR 17. Guidelines for basic life
support (BLS) describe this technique for manual chest compression 46. Over-the-head chest compression was combined in one previous study with bag-
valve-mask ventilation. This resulted in CPR that conformed closely to ERC guidelines 46. However, for OTH the average compression depth was significantly less than for
the standard position (P=0.0149) and there were more compressions of incorrect
depth (P=0.0400) 46. Handley et al. 46 also showed that for one-man CPR (which is presumably less frequently used than two-man CPR in the aeroplane cardiac arrest
setting), standard CPR is superior to an over-the-head (OTH) technique. However, this study was limited by small numbers and the fact that it did not actually simulate
real-life conditions, as it was carried out on mannequins in simulated flight cabins and not in moving airplanes. In congruency, Perkins et al. 47 also demonstrated that
OTH-CPR is possible but associated with lower quality of CPR. Laying the collapsed person on the seats (if the arm-rests can be folded back promptly) and initiating CPR
is the fastest option and allows initiation of essential life-saving procedures with the least interruption to precious time after cardiac arrest 16.
The optimum place for CPR is the galley, but may depend on the aircraft
model (strong consensus, Level of Evidence C, Grade of Recommendation B). Also, CPR in the aisle of the aircraft is considered possible
(intermediate consensus, Level of Evidence moderate, Grade of Recommendation C).
Environment
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 18
The confined environment of the aircraft cabin may also interfere with the on-board
management of patients suffering a cardiac arrest, as treatment may be hampered by poor access, restricted space, interference from noise, and vibration that makes it
difficult to assess pulse and breathing for CPR 16. Additionally, the quality of CPR may be low 14, 46.
In the challenging setting of an aircraft cabin in flight, the potential interventions are limited owing to confined and restricted space for patient care and less-than-
appropriate positioning of the patient, limited personnel with the appropriate skill set, and limited supplies 13. It is most important to gain access to the patient, even if the
patient has to be transferred several meters, e.g., to the galley. Also, the current guidelines for CPR recommend transferring the patient after cardiac arrest to a
suitable location, e.g., galley or exit area 17. The provision of CPR on-board airplanes is limited by the closed, confined spaces
that rescuers are forced to operate in 16. The lack of space may make it difficult for
rescuers to kneel comfortably by the side of the patient to perform standard CPR 16.
CPR should ideally be performed/supervised by a health care provider (strong consensus, Level of Evidence C, Grade of Recommendation B) – if
present. However, aircraft crew, trained in BLS-AED or CPR, or a layperson with corresponding training should also be recruited to perform chest
compressions (strong consensus, Level of Evidence low, Grade of Recommendation B).
During flight, the most appropriate and probably the only possible approach to the
management of cardiac arrest is a basic approach. Thus, recognition of cardiac arrest, compression-only CPR and defibrillation with the use of an AED represent the
interventions that the volunteer physician should consider applying 13.
For airway management during in-flight CPR, the use of a supraglottic airway (e.g., laryngeal mask or laryngeal tube) may be superior to face
mask ventilation or endotracheal intubation (ETI) (strong consensus, Level of Evidence low, Grade of Recommendation B).
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 19
Airway management While endotracheal intubation is considered the „optimal method“ of providing and maintaining a clear secure airway 19, it must be taken into account that the success
rate for in-flight endotracheal intubation (ETI) is significantly lower as compared to elective intubation in hospitals (by a factor of 8.7) or emergency intubations at scene
(by a factor of 2.3) 48. Today, supraglottic airway devices (SGA) have in partly eliminated the need for
early routine endotracheal intubation in many medical fields 49. Over the last years several manufacturers presented improved and new types of SGA. Newer generation
devices have multiple advantages such as gastric access and a higher leak pressure. Insertion of a supraglottic airway devices is usually easier (no laryngoscope needed),
faster (no muscle relaxation needed), and safer (no risk of oesophageal intubation) when compared with tracheal intubation. Furthermore, ETI requires
substantially more training 50, 51. Therefore and adapted to the aircraft environment,
the use of SGA may be superior for airway management.
Cabin crew must be trained initially and once per year in CPR (strong consensus, Level of Evidence B, Grade of Recommendation A) and should
be re-trained in CPR every six months (strong consensus, Level of Evidence moderate, Grade of Recommendation B).
Crew qualification In the event of a passenger medical incident, delays ranging from 20 minutes to several hours before expert assistance is available and the potential lack of
medically-trained persons on board must be taken into consideration 25. Therefore, sufficient and regular training of the aircraft crew in CPR and emergency medical
treatment is of utmost importance. Cabin crew have an essential role in aviation safety and require appropriate recurrent training 25.
Recent literature indicated that a training interval in cabin crew of 12 months is too long and practical skills degrade over this period 25. The optimal frequency and type
of recurrent training which maintains skills and knowledge at an appropriate level needs still to be determined for this occupational group 25.
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 20
The crew should be trained regularly in basic life support – ideally with a
focus on CPR in aircraft (strong consensus, Level of Evidence low, Grade of Recommendation A).
A gradual decline in CPR and AED skills following training has been demonstrated in
laypersons and medically trained persons 52, 53 and has been associated with the types of instructional techniques of employees 54, variations in programme delivery 55
and the time interval between training and re-assessment 25, 56, 57. In a recent study, most cabin crew members failed to deliver CPR correctly, showing
wide variations in hand positioning, compression depth and rate, which is all critical for survival following cardiac arrest 25. Recent literature has confirmed that a short
(15 minute) BLS refresher course was sufficient to maintain the skills 58. Especially for lay rescuers and non-medical rescuers, having a flow chart available can improve
quality of CPR 59.
A standardized course in advanced life support (ALS) or immediate life support (ILS) is also helpful, but due to the complexity not necessary. A first-aid course is not
considered sufficient for management of IFCA.
A diversion should immediately be undertaken if the patient has a return of spontaneous circulation (ROSC) (strong consensus, Level of Evidence
low, Grade of Recommendation B). Diversion One strategy for the management of cardiac arrest patients in flight is the immediate
diversion to the closest airport 12. However, evidence suggests that at the current time diversion for patients presenting with non-shockable rhythms may be futile and
aircraft diversion includes additional risks: emergent landings, potential need to dump fuel, landing with overweight aircraft, altered flight patterns, landing in poor
weather, high costs, and landing in unfamiliar conditions 12. Prior to 1990, it was standard airline practice to divert aeroplanes to the nearest
major airport if there was a cardiac arrested subject on board 16. The ERC guidelines recommend to request an immediate flight diversion to the nearest appropriate
airport 17, but do not give any details when to request (if cardiac arrest is detected or
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 21
if return of spontaneous circulation (ROSC) is achieved). However, according to
these guidelines, death on board can only be confirmed legally by a physician 17. If a dead person is found, or CPR has been terminated (see ethics of resuscitation and
end-of-life decisions), flight diversion is not recommended 60. In a recent study, an emergency diversion was performed in 22/1,312 cases (i.e.,
1.7%) 37. This percentage is low and in the range of previous research (1.1-13.0%) 11, 30, 61-63. If the patient has been successfully resuscitated, diversion and emergency
landing are probably the most appropriate recommendations to be made to the captain of the aircraft 13.
If a return of spontaneous circulation is not achieved within 20 to 30 minutes in the absence of a reversible cause, it is appropriate to consider cessation of resuscitation
efforts 13.
CPR should be continued during emergency diversion (strong consensus,
Level of Evidence low, Grade of Recommendation A).
The decision for diversion is typically made after ROSC of the patient. However, scenarios are possible where an emergency diversion is performed before ROSC. For
example, when leaving land and expecting a flight over open water during an ongoing CPR, a diversion may be performed before ROSC. In that case – considering
on-board safety issues – CPR should not be interrupted during landing at the diversion airport. However, this approach should be discussed with the cabin crew
and the pilots.
Post-resuscitation care Fixation devices are considered marginally important and can help to fixate the patient after ROSC (weak consensus, Level of Evidence low,
Grade of Recommendation C). After ROSC, patients can move or might be agitated. Therefore, sufficient fixation or immobilization devices may be helpful, especially to assure flight safety. There are no
data or studies available on this topic.
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 22
Due to reduced ambient pressure in the aircraft cabin, oxygen should be used even after ROSC to compensate for a reduced oxygen partial pressure
in the blood (strong consensus, Level of Evidence low, Grade of Recommendation B).
Oxygen toxicity and a worse outcome of resuscitated patients with hyperoxia have
been described in the medical literature 18, 19, 64, 65. However, environmental factors in the aircraft cabin are not comparable to the setting on ground. During flight on
cruising altitude, cabin pressure is approximately 850 hPa resulting in an oxygen saturation in healthy adults of approximately 90-92% 66. Since current guidelines on
CPR (on the ground) recommend not to use oxygen but target a range of 94-98% of oxygen saturation 18, 19, supplementary oxygen by face masks 67, 68 in spontaneously
breathing patients could be beneficial. By applying 2-3 litres oxygen per minute,
oxygen saturation can be adjusted to the target range when using oxygen masks 67,
68.
It is important to induce targeted temperature management as soon as
possible after ROSC (weak consensus, Level of Evidence low, Grade of Recommendation B).
A few case reports confirmed the feasibility of Targeted Temperature Management
(TTM) using cold i.v.-fluids and chemical cooling packs during air transport 69. Also, current ERC guidelines recommend temperature control (at least avoiding a body
core temperature higher than 36°C 70) as early as possible but not using cold saline 19. In summary, avoiding post-ROSC fever may have the largest benefit 70, 71.
To reduce patient temperature after ROSC, several methods are usually available in a commercial airplane. Due to convection and the large amount of air passing the
aircraft cabin, removing clothing and not covering patients with a sheet may decrease body core temperature significantly. Whereas cold (infusion) fluids are
usually not available and must be cooled before application, their use has been associated with worse outcome 72. However, crushed ice is available in large
amounts in most airliners and can be used, e.g., for cooling the head, neck, armpits,
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 23
or the groin. It should be taken into account that using ice for cooling patients can
have obvious drawbacks (e.g., obstacle for further treatment, delay in procedures, or frostbites) 73.
Acknowledgements The manuscript was prepared by the working group “guidelines, recommendations,
and statements” of the German Society of Aerospace Medicine and reviewed by the board of the German Society of Aerospace Medicine (DGLRM). The authors thank
Prof. Douglas Boyd (University of Texas) sincerely for his critical comments, language editing, and improving the quality of this manuscript.
Disclosures
C.N. is Treasurer of the German Society for Aviation and Space Medicine (DGLRM).
E.D.R. received honorarium form MSD.
E.G. is CEO of the German Academy for Aviation- and Travel Medicine (DAFR). H.G. received travel reimbursement for presentations from Ambu and VBM,
Germany.
J.H. is Vice President of the German Society for Aviation and Space Medicine (DGLRM) and Treasurer of the European Society of Aerospace Medicine
(ESAM); no other conflicts of interest do apply for J.H. J.S. is employed at Lufthansa.
C.A., A.H., M.B., S.J., J.A., P.K., F.C., I.J., and M.K. have no conflicts of
interest.
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 24
References
1. Association IAT.
http://www.iata.org/pressroom/facts_figures/fact_sheets/Documents/fact-sheet-industry-facts.pdf (online, July 20, 2016). 2016.
2. Freedman D, Chen L, Kozarsky P. Medical Considerations before International Travel. N Engl J Med. 2016;375:247-260.
3. Graf J, Stüben U, Pump S. In-flight medical emergencies. Dtsch Aerztebl Int. 2012;109(37):591-602.
4. Qureshi A, Porter K. Emergencies in the air. Emerg Med J. 2005;22:658-659. 5. Hinkelbein J. Significant More Research Required: No Further Progress
Without Sound Medical Data and Valid Denominators for In-Flight Medical Emergencies. J Travel Med. 2015;22(6):355-356.
6. Hinkelbein J, Neuhaus C, Wetsch W, Spelten O, Picker S, Böttiger B, Gathof B.
Emergency medical equipment on board German airliners. J Travel Med. 2014;21(5):318-323.
7. Hinkelbein J, Spelten O, Wetsch W, Schier R, Neuhaus C. Emergencies in the sky: In-flight medical emergencies during commercial air transport. Trends in Anaesthesia and Critical Care (online first). DOI: 10.1016/j.tacc.2013.03.001. 2013.
8. Sand M, Bechara F, Sand D, Mann B. Surgical and medical emergencies on board European aircraft: a retrospective study of 10189 cases. Crit Care. 2009;13:R3.
9. Sand M, Bechara F, Sand D, Mann B. In-flight medical emergencies. Lancet. 2009;374:1062-1063.
10. Siedenburg J. Epidemiology of “In-flight Emergencies”. In: Siedenburg J,
Küpper T (eds): Moderne Flugmedizin. Gentner Verlag, Stuttgart: 653 – 655. 2015.
11. Peterson D, Martin-Gill C, Guyette F, Tobias A, McCarthy C, Harrington S, Delbridge T, Yealy D. Outcomes of medical emergencies on commercial airline
flights. N Engl J Med. 2013;368(22):2075-2083.
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 25
12. Brown A, Rittenberger J, Ammon C, Harrington S, Guyette F. In-flight
automated external defibrillator use and consultation patterns. Prehosp Emerg Care. 2010;14(2):235-239.
13. Nable J, Tupe C, Gehle B, Brady W. In-Flight Medical Emergencies during Commercial Travel. N Engl J Med. 2015;373(10):939-945.
14. Fischer H, Neuhold S, Hochbrugger E, Steinlechner B, Koinig H, Milosevic L, Havel C, Frantal S, Greif R. Quality of resuscitation: Flight attendants in an
airplane simulator use a new mechanical resuscitation device - A randomized simulation study. Resuscitation. 2011;82:459-463.
15. Cocks R, Liew M. Commercial aviation in-flight emergencies and the physician. Emerg Med Australas. 2007;19(1):1-8.
16. Charles R. Cardiac arrest in the skies. Singapore Med J. 2011;52(8):582-585. 17. Truhlář A, Deakin C, Soar J, Khalifa G, Alfonzo A, Bierens J, Brattebø G,
Brugger H, Dunning J, Hunyadi-Antičević S, Koster R, Lockey D, Lott C, Paal P,
Perkins G, Sandroni C, Thies K, Zideman D, Nolan J. European Resuscitation Council Guidelines for Resuscitation 2015: Section 4. Cardiac arrest in special
circumstances. Resuscitation. 2015;95:148-201. 18. Neumar R, Shuster M, Callaway C, Gent L, Atkins D, Bhanji F, Brooks S, Caen
Ad, Donnino M, Ferrer J, Kleinman M, Kronick S, Lavonas E, Link M, Mancini M, Morrison L, O’Connor R, Samson R, Schexnayder S, Singletary E, Sinz E,
Travers A, Wyckoff M, Hazinski M. 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular
Care. Circulation. 2015;132:S315-S367. 19. Monsieurs K, Nolan J, Bossaert L, Greif R, Maconochie I, Nikolaou N, Perkins
D, Soar J, Truhlář A, Wyllie J, Zideman D. European Resuscitation Council Guidelines for Resuscitation 2015: Section 1. Executive summary.
Resuscitation. 2015;95:1-80. 20. Chalkias A, Georgiou M, Böttiger B, Monsieurs K, Svavarsdóttir H, Raffay V,
Iacovidou N, Xanthos T. Recommendations for resuscitation after ascent to high altitude and in aircrafts. Int J Cardiol. 2013;167(5):1703-1711.
21. Guyatt G, Oxman A, Schünemann H, Tugwell P, Knottnerus A. GRADE guidelines: A new series of articles in the Journal of Clinical Epidemiology.
Journal of Clinical Epidemiology. 2011;64:380-382.
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 26
22. Fitch K, Bernstein S, Aguilar M, Burnand B, LaCalle J, Lazaro P, Loo Mvh,
McDonnell J, Vader J, Kahan J. The RAND/UCLA Appropriateness Method User's Manual. Santa Monica, CA: RAND Corporation, 2001.
http://www.rand.org/pubs/monograph_reports/MR1269.html. 2001. 23. Fink A, Kosecoff J, Chassin M, Brook R. Consensus methods: charcteristics and
guidelines for use. Am J Public Health. 1984;74(9):979-983. 24. Silverman D, Gendreau M. Medical issues associated with commercial flights.
Lancet. 2009;373:1067-2077. 25. Mahony P, Griffiths R, Larsen P, Powell D. Retention of knowledge and skills in
first aid and resuscitation by airline cabin crew. Resuscitation. 2008;76(3):413-418.
26. Bolle SR, Johnsen E, Gilbert M. Video calls for dispatcher-assisted cardiopulmonary resuscitation can improve the confidence of lay rescuers--
surveys after simulated cardiac arrest. J Telemed Telecare.17(2):88-92.
27. Panczyk M, McNally BF, Bobrow BJ. Telephone CPR: saving lives around the world. New program will help dispatchers and track vital data. EMS World. 2013;42(9):35-36, 39.
28. Spelten O, Warnecke T, Wetsch WA, Schier R, Bottiger BW, Hinkelbein J.
Dispatcher-assisted compression-only cardiopulmonary resuscitation provides best quality cardiopulmonary resuscitation by laypersons: A randomised
controlled single-blinded manikin trial. Eur J Anaesthesiol.33(8):575-580. 29. Valani R, Cornacchia M, Kube D. Flight diversions due to onboard medical
emergencies on an international commercial airline. Aviat Space Environ Med. 2010;81(11):1037-1040.
30. Chandra A, Conry S. In-flight Medical Emergencies. West J Emerg Med. 2013;14(5):499-504.
31. Hung K, Chan E, Cocks R, Ong R, Rainer T, Graham C. Predictors of flight diversions and deaths for in-flight medical emergencies in commercial
aviation. Arch Intern Med. 2010;170(15):1401-1402. 32. Hinkelbein J, Dambier M, Schwalbe M, Glaser E, Neuhaus C. Lack of
Denominator Data in Aviation Accident Analysis. Aviat Space Environ Med. 2010;81(1):77.
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 27
33. Hinkelbein J, Kalina S, Braunecker S, Böhm L, Glaser E, Neuhaus C.
Standardisiertes Erfassungsprotokoll der DGLRM für Notfälle an Bord von Luftfahrzeugen. Flugmed Tropenmed Reisemed. 2016;23(1):19-22.
34. Europäische U. VERORDNUNG (EG) Nr. 859/2008 DER KOMMISSION vom 20. August 2008 zur Änderung der Verordnung (EWG) Nr. 3922/91 des Rates in
Bezug auf gemeinsame technische Vorschriften und Verwaltungsverfahren für den gewerblichen Luftverkehr mit Flächenflugzeugen. Amtsblatt der Europäischen Union. 20.9.2008;L254:1-238.
35. Sand M, Gambichler T, Sand D, Thrandorf C, Altmeyer P, Bechara F.
Emergency medical kits on board commercial aircraft: a comparative study. Travel Med Infect Dis. 2010;8(6):388-394.
36. (EASA) EAaSA. Acceptable Means of Compliance (AMC) and Guidance Material (GM) to Part-CAT. Decision 2014/015/R. 2014.
37. Akyol C, Kesapli M, Gungor F, Janitzky-Akyol A, Soydam-Guven D, Kaya G.
Inflight Emergencies During Euroasian Flights. J Travel Med. 2015;22(6):361-367.
38. Harve H, Hämäläinen O, Kurola J, Silfvast T. AED use in a passenger during a long-haul flight: repeated defibrillation with a successful outcome. Aviat Space Environ Med. 2009;80(4):405-408.
39. Page R, Joglar J, Kowal R, Zagrodzky J, Nelson L, Ramaswamy K, Barbera S,
Hamdan M, McKenas D. Use of automated external defibrillators by a U.S. airline. N Engl J Med. 2000;343(1210-1216).
40. Hinkelbein J, Hose D, Fiedler F. Comparison of Three Different Sensor Sites for Pulse Oximetry in Critically Ill Patients. Int J Intensive Care. 2005;12(4):159-
163. 41. Aoyagi T, Kishi M, Yamaguchi K, Watanabe S. Improvement of the earpiece
oximeter. Abstracts of the 13th annual meeting of the Japanese Society of Medical Electronics and Biological Engeneering. 1974: 90–91 (Jap).
42. Pedersen T, Moller A, Pedersen B. Pulse oximetry for perioperative monitoring: systematic review of randomized, controlled trials. Anesth Analg. 2003;96:426–431.
43. Ochoa F, Ramalle-Gómara E, Lisa V, Saralegui I. The effect of rescuer fatigue
on the quality of chest compressions. Resuscitation. 1998;37(3):149-152.
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 28
44. Havel C, Schreiber W, Riedmuller W, Haugk M, Richling N, Trimmel H, Malzer
R, Sterz F, Herkner H. Quality of closed chest compression in ambulance vehicles, flying helicopters and at the scene. Resuscitation. 2007;73:264—270.
45. Thomas S, Stone C, Bryan-Berge D. The ability to perform closed chest compressions in helicopters. Am J Emerg Med. 1994;12(3):296-298.
46. Handley A, Handley J. Performing chest compressions in a confined space. Resuscitation. 2004;61:55-61.
47. Perkins G, Stephenson B, Smith C, Gao F. A comparison between over-the-head and standard cardiopulmonary resuscitation. Resuscitation. 2004;61(2):155-161.
48. McIntosh S, Swanson E, McKeone A, Barton E. Location of airway
management in air medical transport. Prehosp Emerg Care. 2008;12(4):438-442.
49. Das A, Majumdar S, Mukherjee A, Mitra T, Kundu R, Hajra B, Mukherjee D,
Das B. i-gel in Ambulatory Surgery: A Comparison with LMA-ProSeal in Paralyzed Anaesthetized Patients. J Clin Diagn Res. 2014;8(3):80-84.
50. Bernhard M, Mohr S, Weigand M, Martin E, Walther A. Developing the skill of endotracheal intubation: implication for emergency medicine. Acta Anaesthesiol Scand. 2012;56(2):164-171.
51. Mohr S, Weigand M, Hofer S, Martin E, Gries A, Walther A, Bernhard M.
Developing the skill of laryngeal mask insertion. Anaesthesist. 2013;62:447-452.
52. Berden H, Bierens J, Willems F, Hendrick J, Pijls N, Knape J. Resuscitation skills of lay public after recent training. Ann Intern Med. 1994;23(5):1003-
1008. 53. Abella B, Sandbro N, Vassilatos P, et a. Chest compression rates during
cardiopulmonary resuscitation are suboptimal — a prospective study during in-hospital cardiac arrest. Circulation. 2005;111(428-434).
54. Kaye W, Rallis S, Mancini M, et a. The problem of poor retention of cardiopulmonary resuscitation skills may lie with the instructor, not the learner
of the curriculum. Resuscitation. 1991;21(1):67-87. 55. Parnell M, Larsen P. Poor quality teaching in lay person CPR courses.
Resuscitation.73:271-278.
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 29
56. Kaye W, Wynne G, Marteau T, et a. An advanced resuscitation course for pre-
registration house officers. J R Coll Phys Lond. 1990;24(1):51-54. 57. Eisenberger P, Safar P. Life supporting first aid training of the public-review
and recommendations. Resuscitation. 1994;4(1):3-18. 58. Nishiyama C, Iwami T, Murakami Y, Kitamura T, Okamoto Y, Marukawa S,
Sakamoto T, Kawamura T. Effectiveness of simplified 15-min refresher BLS training program: A randomized controlled trial. Resuscitation. 2015;90:56-60.
59. Rössler B, Ziegler M, Hüpfl M, Fleischhackl R, Krychtiuk K, Schebesta K. Can a flowchart improve the quality of bystander cardiopulmonary resuscitation?
Resuscitation. 2013;84(7):982-986. 60. Bossaert L, Perkins G, Askitopoulou H, et a. European Resuscitation Council
Guidelines for Resuscitation 2015 Section 11. Resuscitation. 2015;95:301-310. 61. Delaune Er, Lucas R, Illig P. In-flight medical events and aircraft diversions:
one airline´s experience. Aviat Space Environ Med. 2003;74(1):62-68.
62. Cummins R, Schubach J. Frequency and types of medical emergencies among commercial air travellers. J Am Med Assoc. 1989;261:1295-1299.
63. Weinlich M, Nieuwkamp N, Stueben U, Marzi I, Walcher F. Telemedical assistance for in-flight emergencies on intercontinental commercial aircraft. J Telemed Telecare. 2009;15(8):409-413.
64. Kilgannon J, Jones A, Parrillo J, Dellinger R, Milcarek B, Hunter K, Shapiro N,
Trzeciak S. Relationship Between Supranormal Oxygen Tension and Outcome After Resuscitation From Cardiac Arrest. Circulation. 2011;123:2717-2722.
65. Kilgannon J, Jones A, Shapiro N, Angelos M, Milcarek B, Hunter K, Parrillo J, Trzeciak S. Association Between Arterial Hyperoxia Following Resuscitation
From Cardiac Arrest and In-Hospital Mortality. J Am Med Assoc. 2010;303(21):2165-2171.
66. Hinkelbein J, Glaser E, eds. Flugmedizin. 1 ed: UniMed Science, Bremen; 2007.
67. Hinkelbein J, Glaser E. Evaluation of two oxygen face masks with special regard to inspiratory oxygen fraction (FiO2) for emergency use in rescue
helicopters. Air Med J. 2008;27(2):86-90.
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 30
68. Hinkelbein J, Glaser E, Doerrstein J, Genzwuerker H. Oxygen delivery
comparison of two constant-flow masks during flight to 6863 m. Aviat Space Environ Med. 2006;77(5):540-544.
69. Lyon R, Cowan G, Janossy K, Adams R, Corfield A, Hearns S. In-flight cooling after out-of-hospital cardiac arrest. Resuscitation. 2010;81:1041-1042.
70. Nielsen N, Wetterslev J, Cronberg T, Erlinge D, Gasche Y, Hassager C, Horn J, Hovdenes J, Kjaergaard J, Kuiper M, Pellis T, Stammet P, Wanscher M, Wise
M, Åneman A, Al-Subaie N, Boesgaard S, Bro-Jeppesen J, Brunetti I, Bugge J, Hingston C, Juffermans N, Koopmans M, Køber L, Langørgen J, Lilja G, Møller
J, Rundgren M, Rylander C, Smid O, Werer C, Winkel P, Friberg H, Investigators. TT. Targeted temperature management at 33°C versus 36°C
after cardiac arrest. N Engl J Med. 2013. 71. Bro-Jeppesen J, Hassager C, Wanscher M, et a. Post-hypothermia fever is
associated with increased mortality after out-of-hospital cardiac arrest.
Resuscitation. 2013;84(1734-1740). 72. Kim F, Nichol G, Maynard C, Hallstrom A, Kudenchuk P, Rea T, Copass M,
Carlbom D, Deem S, Longstreth JW, Olsufka M, Cobb L. Effect of prehospital induction of mild hypothermia on survival and neurological status among
adults with cardiac arrest: a randomized clinical trial. J Am Med Assoc. 2014;311(1):45-52.
73. Lampe J, Becker L. Rapid cooling for saving lives: a bioengineering opportunity. Expert Rev Med Devices. 2007;4(4):441-446.
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 31
Figure Legends
Fig. 1: CPR in confined space from the side in an aircraft. Whereas the patient lies in the aisle, the rescuer is placed sideward in the
leg area.
Fig. 2: Over the head (OTH) CPR in the aisle of an aircraft.
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 32
Tables
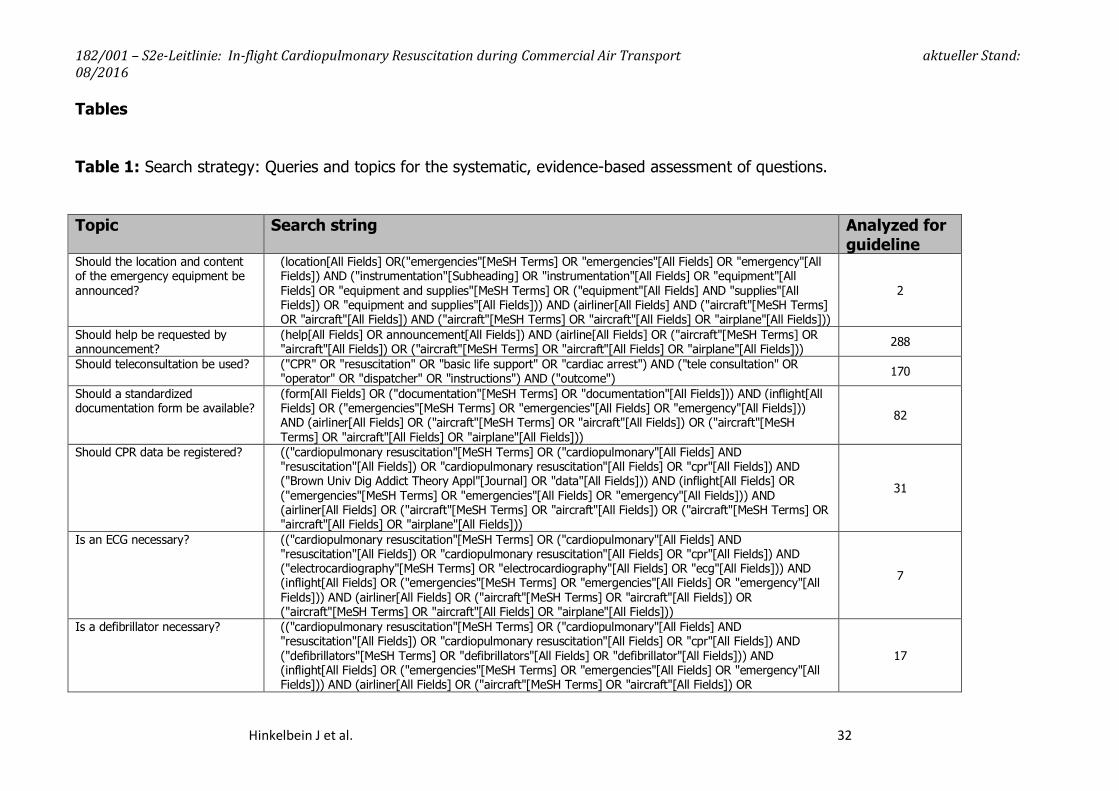
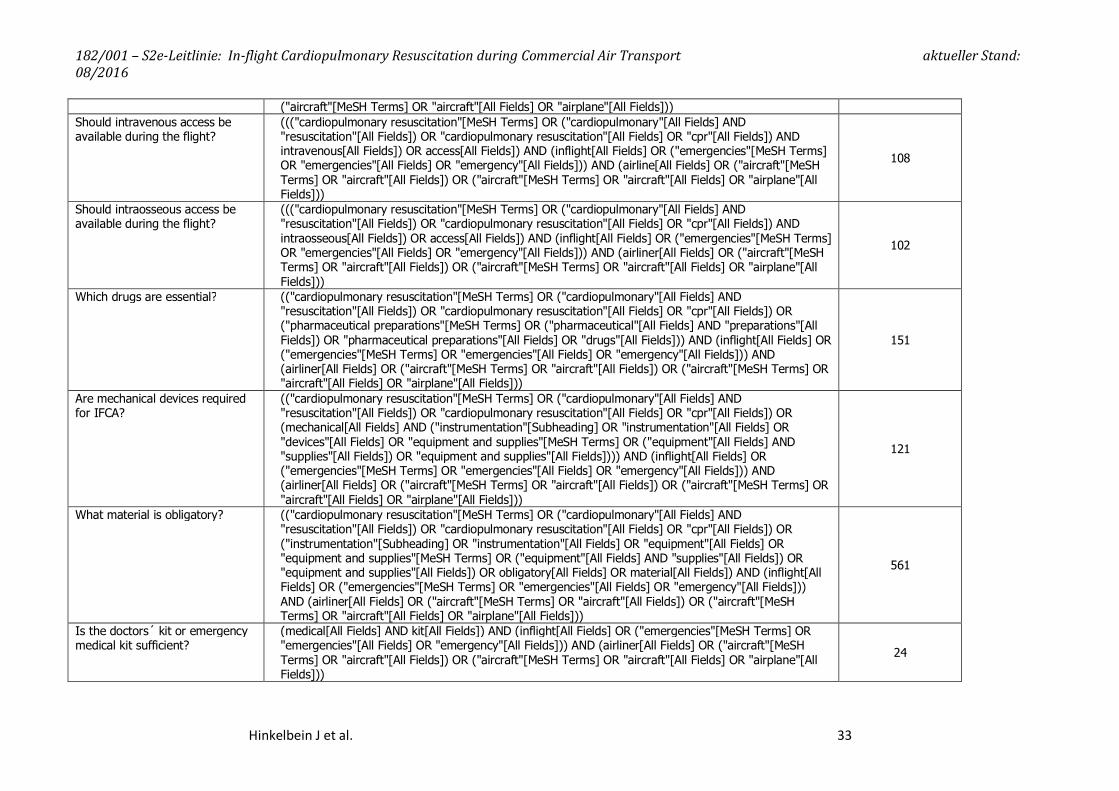
Table 1: Search strategy: Queries and topics for the systematic, evidence-based assessment of questions.
Topic Search string Analyzed for guideline
Should the location and content of the emergency equipment be announced?
(location[All Fields] OR("emergencies"[MeSH Terms] OR "emergencies"[All Fields] OR "emergency"[All Fields]) AND ("instrumentation"[Subheading] OR "instrumentation"[All Fields] OR "equipment"[All Fields] OR "equipment and supplies"[MeSH Terms] OR ("equipment"[All Fields] AND "supplies"[All Fields]) OR "equipment and supplies"[All Fields])) AND (airliner[All Fields] AND ("aircraft"[MeSH Terms] OR "aircraft"[All Fields]) AND ("aircraft"[MeSH Terms] OR "aircraft"[All Fields] OR "airplane"[All Fields]))
2
Should help be requested by announcement?
(help[All Fields] OR announcement[All Fields]) AND (airline[All Fields] OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields]) OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields] OR "airplane"[All Fields])) 288
Should teleconsultation be used? ("CPR" OR "resuscitation" OR "basic life support" OR "cardiac arrest") AND ("tele consultation" OR "operator" OR "dispatcher" OR "instructions") AND ("outcome") 170
Should a standardized documentation form be available?
(form[All Fields] OR ("documentation"[MeSH Terms] OR "documentation"[All Fields])) AND (inflight[All Fields] OR ("emergencies"[MeSH Terms] OR "emergencies"[All Fields] OR "emergency"[All Fields])) AND (airliner[All Fields] OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields]) OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields] OR "airplane"[All Fields]))
82
Should CPR data be registered? (("cardiopulmonary resuscitation"[MeSH Terms] OR ("cardiopulmonary"[All Fields] AND "resuscitation"[All Fields]) OR "cardiopulmonary resuscitation"[All Fields] OR "cpr"[All Fields]) AND ("Brown Univ Dig Addict Theory Appl"[Journal] OR "data"[All Fields])) AND (inflight[All Fields] OR ("emergencies"[MeSH Terms] OR "emergencies"[All Fields] OR "emergency"[All Fields])) AND (airliner[All Fields] OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields]) OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields] OR "airplane"[All Fields]))
31
Is an ECG necessary? (("cardiopulmonary resuscitation"[MeSH Terms] OR ("cardiopulmonary"[All Fields] AND "resuscitation"[All Fields]) OR "cardiopulmonary resuscitation"[All Fields] OR "cpr"[All Fields]) AND ("electrocardiography"[MeSH Terms] OR "electrocardiography"[All Fields] OR "ecg"[All Fields])) AND (inflight[All Fields] OR ("emergencies"[MeSH Terms] OR "emergencies"[All Fields] OR "emergency"[All Fields])) AND (airliner[All Fields] OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields]) OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields] OR "airplane"[All Fields]))
7
Is a defibrillator necessary? (("cardiopulmonary resuscitation"[MeSH Terms] OR ("cardiopulmonary"[All Fields] AND "resuscitation"[All Fields]) OR "cardiopulmonary resuscitation"[All Fields] OR "cpr"[All Fields]) AND ("defibrillators"[MeSH Terms] OR "defibrillators"[All Fields] OR "defibrillator"[All Fields])) AND (inflight[All Fields] OR ("emergencies"[MeSH Terms] OR "emergencies"[All Fields] OR "emergency"[All Fields])) AND (airliner[All Fields] OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields]) OR
17
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 33
("aircraft"[MeSH Terms] OR "aircraft"[All Fields] OR "airplane"[All Fields])) Should intravenous access be available during the flight?
((("cardiopulmonary resuscitation"[MeSH Terms] OR ("cardiopulmonary"[All Fields] AND "resuscitation"[All Fields]) OR "cardiopulmonary resuscitation"[All Fields] OR "cpr"[All Fields]) AND intravenous[All Fields]) OR access[All Fields]) AND (inflight[All Fields] OR ("emergencies"[MeSH Terms] OR "emergencies"[All Fields] OR "emergency"[All Fields])) AND (airline[All Fields] OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields]) OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields] OR "airplane"[All Fields]))
108
Should intraosseous access be available during the flight?
((("cardiopulmonary resuscitation"[MeSH Terms] OR ("cardiopulmonary"[All Fields] AND "resuscitation"[All Fields]) OR "cardiopulmonary resuscitation"[All Fields] OR "cpr"[All Fields]) AND intraosseous[All Fields]) OR access[All Fields]) AND (inflight[All Fields] OR ("emergencies"[MeSH Terms] OR "emergencies"[All Fields] OR "emergency"[All Fields])) AND (airliner[All Fields] OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields]) OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields] OR "airplane"[All Fields]))
102
Which drugs are essential? (("cardiopulmonary resuscitation"[MeSH Terms] OR ("cardiopulmonary"[All Fields] AND "resuscitation"[All Fields]) OR "cardiopulmonary resuscitation"[All Fields] OR "cpr"[All Fields]) OR ("pharmaceutical preparations"[MeSH Terms] OR ("pharmaceutical"[All Fields] AND "preparations"[All Fields]) OR "pharmaceutical preparations"[All Fields] OR "drugs"[All Fields])) AND (inflight[All Fields] OR ("emergencies"[MeSH Terms] OR "emergencies"[All Fields] OR "emergency"[All Fields])) AND (airliner[All Fields] OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields]) OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields] OR "airplane"[All Fields]))
151
Are mechanical devices required for IFCA?
(("cardiopulmonary resuscitation"[MeSH Terms] OR ("cardiopulmonary"[All Fields] AND "resuscitation"[All Fields]) OR "cardiopulmonary resuscitation"[All Fields] OR "cpr"[All Fields]) OR (mechanical[All Fields] AND ("instrumentation"[Subheading] OR "instrumentation"[All Fields] OR "devices"[All Fields] OR "equipment and supplies"[MeSH Terms] OR ("equipment"[All Fields] AND "supplies"[All Fields]) OR "equipment and supplies"[All Fields]))) AND (inflight[All Fields] OR ("emergencies"[MeSH Terms] OR "emergencies"[All Fields] OR "emergency"[All Fields])) AND (airliner[All Fields] OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields]) OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields] OR "airplane"[All Fields]))
121
What material is obligatory? (("cardiopulmonary resuscitation"[MeSH Terms] OR ("cardiopulmonary"[All Fields] AND "resuscitation"[All Fields]) OR "cardiopulmonary resuscitation"[All Fields] OR "cpr"[All Fields]) OR ("instrumentation"[Subheading] OR "instrumentation"[All Fields] OR "equipment"[All Fields] OR "equipment and supplies"[MeSH Terms] OR ("equipment"[All Fields] AND "supplies"[All Fields]) OR "equipment and supplies"[All Fields]) OR obligatory[All Fields] OR material[All Fields]) AND (inflight[All Fields] OR ("emergencies"[MeSH Terms] OR "emergencies"[All Fields] OR "emergency"[All Fields])) AND (airliner[All Fields] OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields]) OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields] OR "airplane"[All Fields]))
561
Is the doctors´ kit or emergency medical kit sufficient?
(medical[All Fields] AND kit[All Fields]) AND (inflight[All Fields] OR ("emergencies"[MeSH Terms] OR "emergencies"[All Fields] OR "emergency"[All Fields])) AND (airliner[All Fields] OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields]) OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields] OR "airplane"[All Fields]))
24
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 34
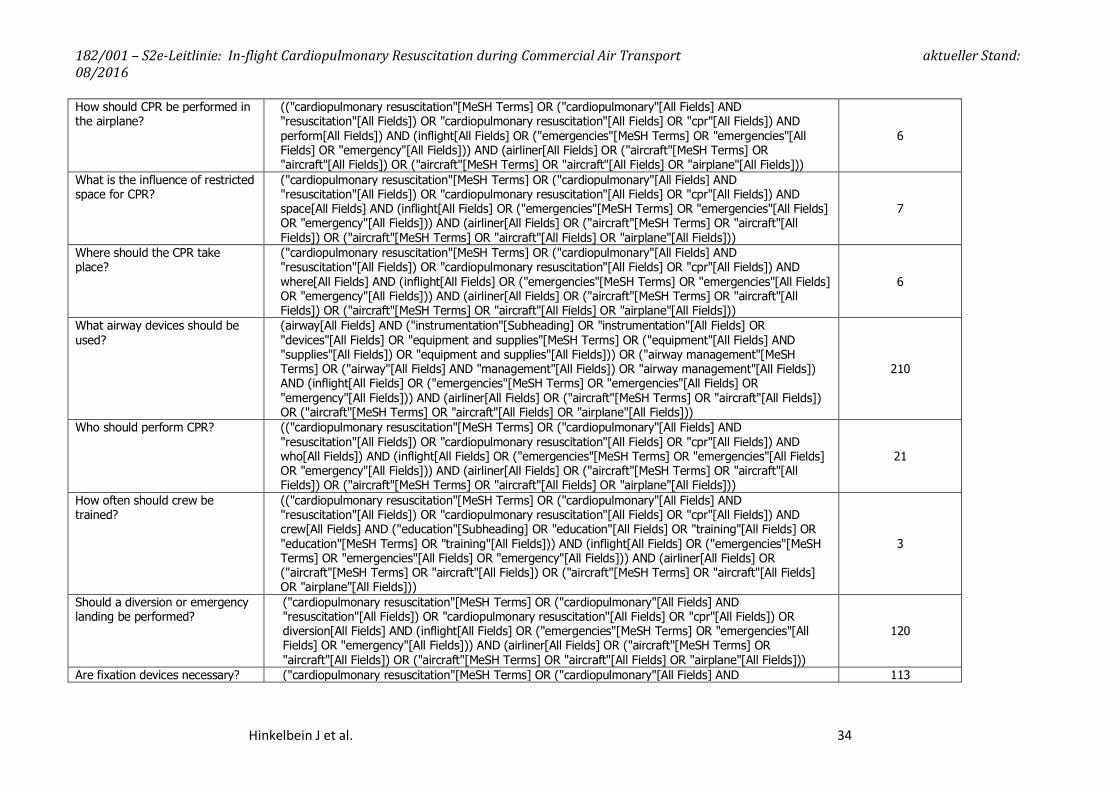
How should CPR be performed in the airplane?
(("cardiopulmonary resuscitation"[MeSH Terms] OR ("cardiopulmonary"[All Fields] AND "resuscitation"[All Fields]) OR "cardiopulmonary resuscitation"[All Fields] OR "cpr"[All Fields]) AND perform[All Fields]) AND (inflight[All Fields] OR ("emergencies"[MeSH Terms] OR "emergencies"[All Fields] OR "emergency"[All Fields])) AND (airliner[All Fields] OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields]) OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields] OR "airplane"[All Fields]))
6
What is the influence of restricted space for CPR?
("cardiopulmonary resuscitation"[MeSH Terms] OR ("cardiopulmonary"[All Fields] AND "resuscitation"[All Fields]) OR "cardiopulmonary resuscitation"[All Fields] OR "cpr"[All Fields]) AND space[All Fields] AND (inflight[All Fields] OR ("emergencies"[MeSH Terms] OR "emergencies"[All Fields] OR "emergency"[All Fields])) AND (airliner[All Fields] OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields]) OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields] OR "airplane"[All Fields]))
7
Where should the CPR take place?
("cardiopulmonary resuscitation"[MeSH Terms] OR ("cardiopulmonary"[All Fields] AND "resuscitation"[All Fields]) OR "cardiopulmonary resuscitation"[All Fields] OR "cpr"[All Fields]) AND where[All Fields] AND (inflight[All Fields] OR ("emergencies"[MeSH Terms] OR "emergencies"[All Fields] OR "emergency"[All Fields])) AND (airliner[All Fields] OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields]) OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields] OR "airplane"[All Fields]))
6
What airway devices should be used?
(airway[All Fields] AND ("instrumentation"[Subheading] OR "instrumentation"[All Fields] OR "devices"[All Fields] OR "equipment and supplies"[MeSH Terms] OR ("equipment"[All Fields] AND "supplies"[All Fields]) OR "equipment and supplies"[All Fields])) OR ("airway management"[MeSH Terms] OR ("airway"[All Fields] AND "management"[All Fields]) OR "airway management"[All Fields]) AND (inflight[All Fields] OR ("emergencies"[MeSH Terms] OR "emergencies"[All Fields] OR "emergency"[All Fields])) AND (airliner[All Fields] OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields]) OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields] OR "airplane"[All Fields]))
210
Who should perform CPR? (("cardiopulmonary resuscitation"[MeSH Terms] OR ("cardiopulmonary"[All Fields] AND "resuscitation"[All Fields]) OR "cardiopulmonary resuscitation"[All Fields] OR "cpr"[All Fields]) AND who[All Fields]) AND (inflight[All Fields] OR ("emergencies"[MeSH Terms] OR "emergencies"[All Fields] OR "emergency"[All Fields])) AND (airliner[All Fields] OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields]) OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields] OR "airplane"[All Fields]))
21
How often should crew be trained?
(("cardiopulmonary resuscitation"[MeSH Terms] OR ("cardiopulmonary"[All Fields] AND "resuscitation"[All Fields]) OR "cardiopulmonary resuscitation"[All Fields] OR "cpr"[All Fields]) AND crew[All Fields] AND ("education"[Subheading] OR "education"[All Fields] OR "training"[All Fields] OR "education"[MeSH Terms] OR "training"[All Fields])) AND (inflight[All Fields] OR ("emergencies"[MeSH Terms] OR "emergencies"[All Fields] OR "emergency"[All Fields])) AND (airliner[All Fields] OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields]) OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields] OR "airplane"[All Fields]))
3
Should a diversion or emergency landing be performed?
("cardiopulmonary resuscitation"[MeSH Terms] OR ("cardiopulmonary"[All Fields] AND "resuscitation"[All Fields]) OR "cardiopulmonary resuscitation"[All Fields] OR "cpr"[All Fields]) OR diversion[All Fields] AND (inflight[All Fields] OR ("emergencies"[MeSH Terms] OR "emergencies"[All Fields] OR "emergency"[All Fields])) AND (airliner[All Fields] OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields]) OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields] OR "airplane"[All Fields]))
120
Are fixation devices necessary? ("cardiopulmonary resuscitation"[MeSH Terms] OR ("cardiopulmonary"[All Fields] AND 113
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 35
"resuscitation"[All Fields]) OR "cardiopulmonary resuscitation"[All Fields] OR "cpr"[All Fields]) OR fixation[All Fields] AND (inflight[All Fields] OR ("emergencies"[MeSH Terms] OR "emergencies"[All Fields] OR "emergency"[All Fields])) AND (airliner[All Fields] OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields]) OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields] OR "airplane"[All Fields]))
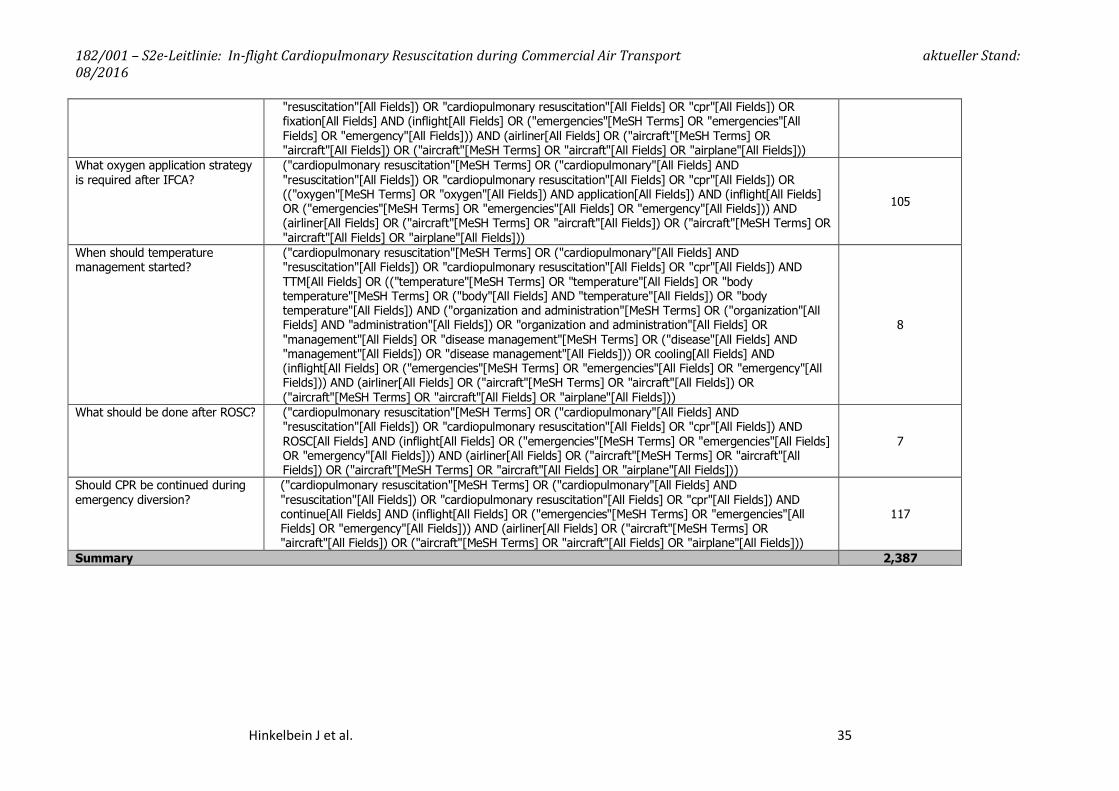
What oxygen application strategy is required after IFCA?
("cardiopulmonary resuscitation"[MeSH Terms] OR ("cardiopulmonary"[All Fields] AND "resuscitation"[All Fields]) OR "cardiopulmonary resuscitation"[All Fields] OR "cpr"[All Fields]) OR (("oxygen"[MeSH Terms] OR "oxygen"[All Fields]) AND application[All Fields]) AND (inflight[All Fields] OR ("emergencies"[MeSH Terms] OR "emergencies"[All Fields] OR "emergency"[All Fields])) AND (airliner[All Fields] OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields]) OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields] OR "airplane"[All Fields]))
105
When should temperature management started?
("cardiopulmonary resuscitation"[MeSH Terms] OR ("cardiopulmonary"[All Fields] AND "resuscitation"[All Fields]) OR "cardiopulmonary resuscitation"[All Fields] OR "cpr"[All Fields]) AND TTM[All Fields] OR (("temperature"[MeSH Terms] OR "temperature"[All Fields] OR "body temperature"[MeSH Terms] OR ("body"[All Fields] AND "temperature"[All Fields]) OR "body temperature"[All Fields]) AND ("organization and administration"[MeSH Terms] OR ("organization"[All Fields] AND "administration"[All Fields]) OR "organization and administration"[All Fields] OR "management"[All Fields] OR "disease management"[MeSH Terms] OR ("disease"[All Fields] AND "management"[All Fields]) OR "disease management"[All Fields])) OR cooling[All Fields] AND (inflight[All Fields] OR ("emergencies"[MeSH Terms] OR "emergencies"[All Fields] OR "emergency"[All Fields])) AND (airliner[All Fields] OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields]) OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields] OR "airplane"[All Fields]))
8
What should be done after ROSC? ("cardiopulmonary resuscitation"[MeSH Terms] OR ("cardiopulmonary"[All Fields] AND "resuscitation"[All Fields]) OR "cardiopulmonary resuscitation"[All Fields] OR "cpr"[All Fields]) AND ROSC[All Fields] AND (inflight[All Fields] OR ("emergencies"[MeSH Terms] OR "emergencies"[All Fields] OR "emergency"[All Fields])) AND (airliner[All Fields] OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields]) OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields] OR "airplane"[All Fields]))
7
Should CPR be continued during emergency diversion?
("cardiopulmonary resuscitation"[MeSH Terms] OR ("cardiopulmonary"[All Fields] AND "resuscitation"[All Fields]) OR "cardiopulmonary resuscitation"[All Fields] OR "cpr"[All Fields]) AND continue[All Fields] AND (inflight[All Fields] OR ("emergencies"[MeSH Terms] OR "emergencies"[All Fields] OR "emergency"[All Fields])) AND (airliner[All Fields] OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields]) OR ("aircraft"[MeSH Terms] OR "aircraft"[All Fields] OR "airplane"[All Fields]))
117
Summary 2,387
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 36
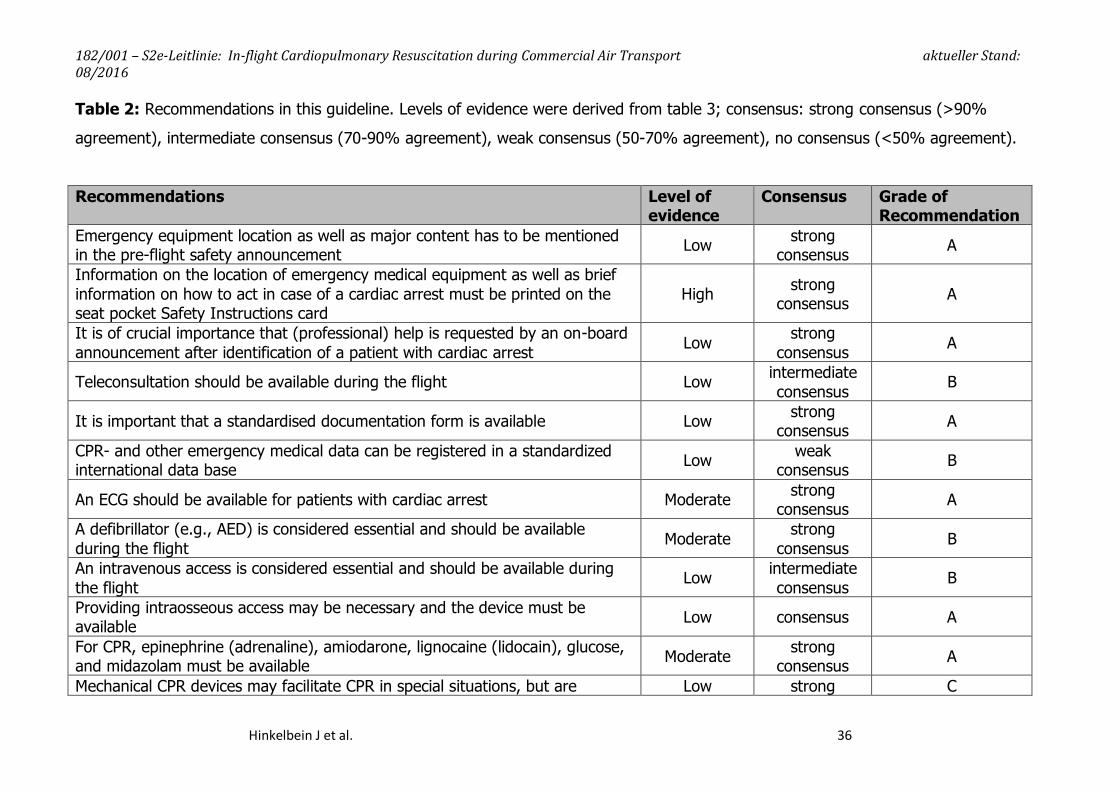
Table 2: Recommendations in this guideline. Levels of evidence were derived from table 3; consensus: strong consensus (>90%
agreement), intermediate consensus (70-90% agreement), weak consensus (50-70% agreement), no consensus (<50% agreement).
Recommendations Level of evidence
Consensus Grade of Recommendation
Emergency equipment location as well as major content has to be mentioned in the pre-flight safety announcement Low strong
consensus A
Information on the location of emergency medical equipment as well as brief information on how to act in case of a cardiac arrest must be printed on the seat pocket Safety Instructions card
High strong consensus A
It is of crucial importance that (professional) help is requested by an on-board announcement after identification of a patient with cardiac arrest Low strong
consensus A
Teleconsultation should be available during the flight Low intermediate consensus B
It is important that a standardised documentation form is available Low strong consensus A
CPR- and other emergency medical data can be registered in a standardized international data base Low weak
consensus B
An ECG should be available for patients with cardiac arrest Moderate strong consensus A
A defibrillator (e.g., AED) is considered essential and should be available during the flight Moderate strong
consensus B
An intravenous access is considered essential and should be available during the flight Low intermediate
consensus B
Providing intraosseous access may be necessary and the device must be available Low consensus A
For CPR, epinephrine (adrenaline), amiodarone, lignocaine (lidocain), glucose, and midazolam must be available Moderate strong
consensus A
Mechanical CPR devices may facilitate CPR in special situations, but are Low strong C
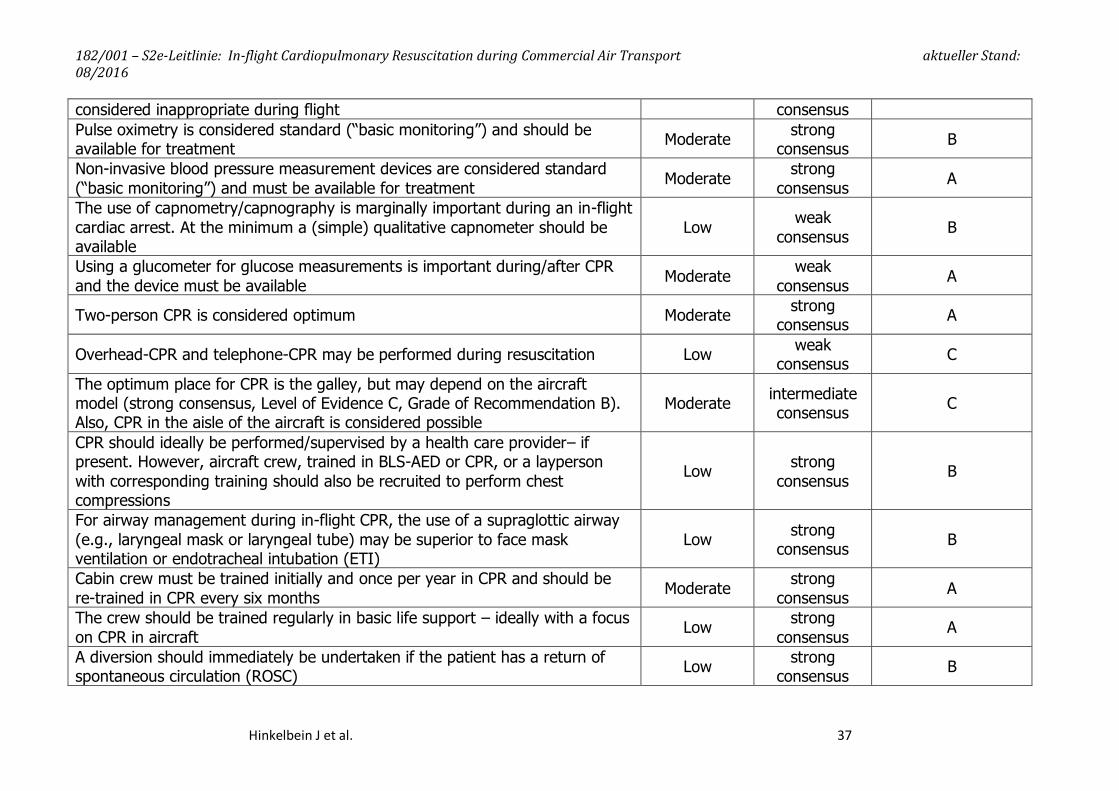
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 37
considered inappropriate during flight consensus Pulse oximetry is considered standard (“basic monitoring”) and should be available for treatment Moderate strong
consensus B
Non-invasive blood pressure measurement devices are considered standard (“basic monitoring”) and must be available for treatment Moderate strong
consensus A
The use of capnometry/capnography is marginally important during an in-flight cardiac arrest. At the minimum a (simple) qualitative capnometer should be available
Low weak consensus B
Using a glucometer for glucose measurements is important during/after CPR and the device must be available Moderate weak
consensus A
Two-person CPR is considered optimum Moderate strong consensus A
Overhead-CPR and telephone-CPR may be performed during resuscitation Low weak consensus C
The optimum place for CPR is the galley, but may depend on the aircraft model (strong consensus, Level of Evidence C, Grade of Recommendation B). Also, CPR in the aisle of the aircraft is considered possible
Moderate intermediate consensus C
CPR should ideally be performed/supervised by a health care provider– if present. However, aircraft crew, trained in BLS-AED or CPR, or a layperson with corresponding training should also be recruited to perform chest compressions
Low strong consensus B
For airway management during in-flight CPR, the use of a supraglottic airway (e.g., laryngeal mask or laryngeal tube) may be superior to face mask ventilation or endotracheal intubation (ETI)
Low strong consensus B
Cabin crew must be trained initially and once per year in CPR and should be re-trained in CPR every six months Moderate strong
consensus A
The crew should be trained regularly in basic life support – ideally with a focus on CPR in aircraft Low strong
consensus A
A diversion should immediately be undertaken if the patient has a return of spontaneous circulation (ROSC) Low strong
consensus B
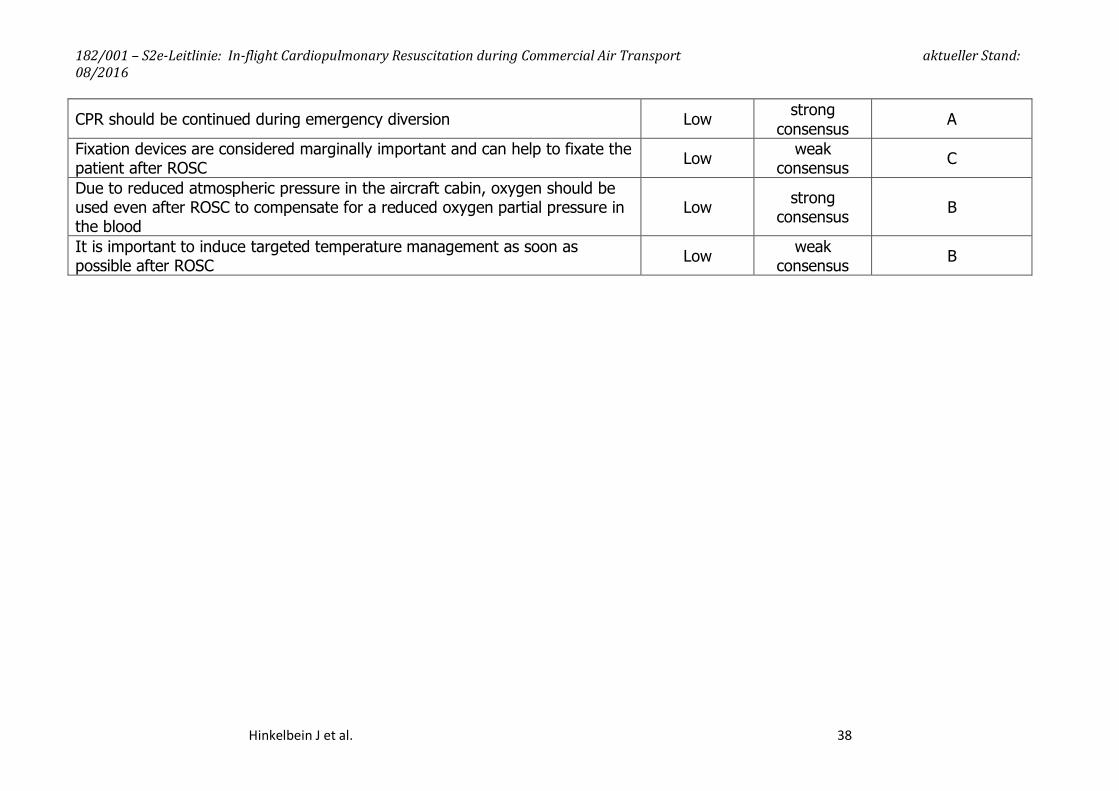
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 38
CPR should be continued during emergency diversion Low strong consensus A
Fixation devices are considered marginally important and can help to fixate the patient after ROSC Low weak
consensus C
Due to reduced atmospheric pressure in the aircraft cabin, oxygen should be used even after ROSC to compensate for a reduced oxygen partial pressure in the blood
Low strong consensus B
It is important to induce targeted temperature management as soon as possible after ROSC Low weak
consensus B
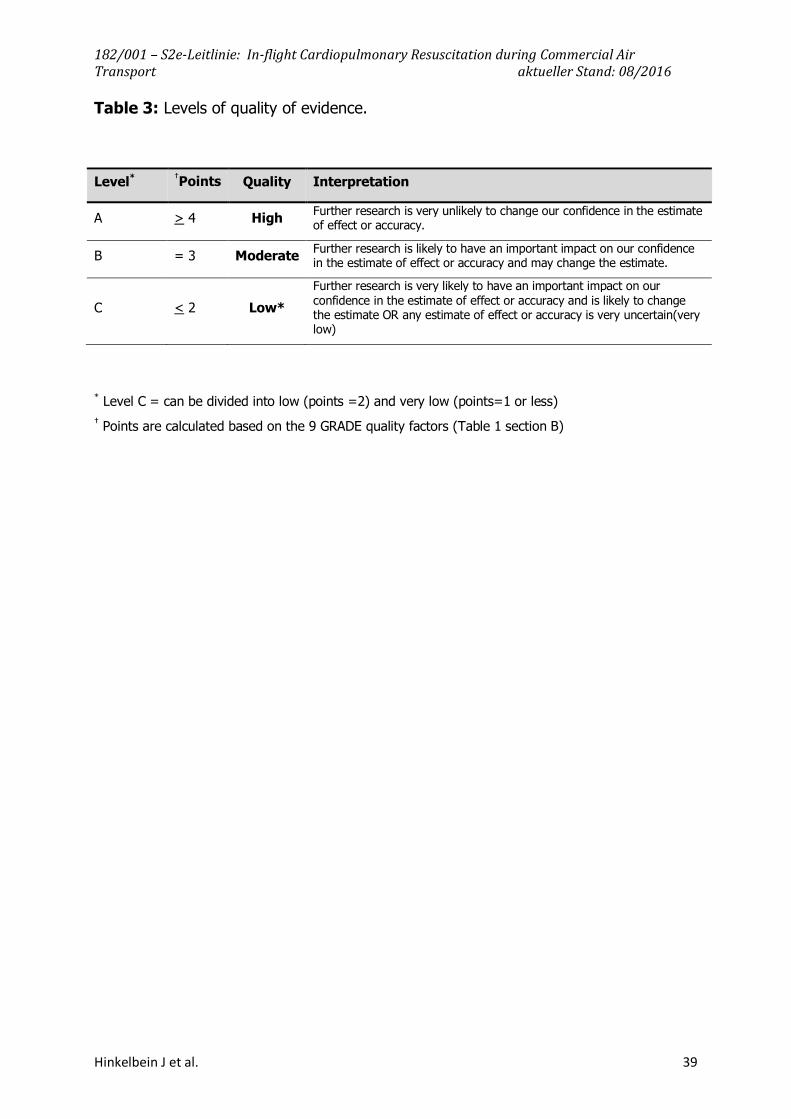
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 39
Table 3: Levels of quality of evidence.
* Level C = can be divided into low (points =2) and very low (points=1 or less) † Points are calculated based on the 9 GRADE quality factors (Table 1 section B)
Level* †Points Quality Interpretation
A > 4 High Further research is very unlikely to change our confidence in the estimate of effect or accuracy.
B = 3 Moderate Further research is likely to have an important impact on our confidence in the estimate of effect or accuracy and may change the estimate.
C < 2 Low* Further research is very likely to have an important impact on our confidence in the estimate of effect or accuracy and is likely to change the estimate OR any estimate of effect or accuracy is very uncertain(very low)
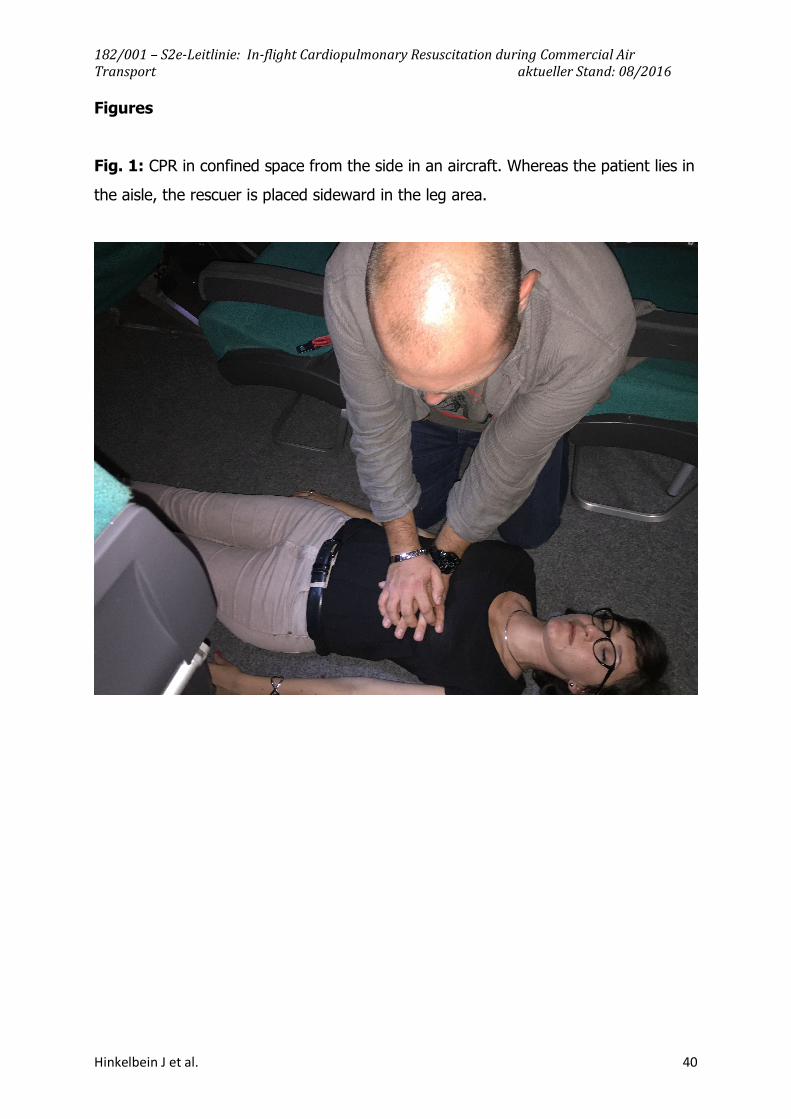
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 40
Figures
Fig. 1: CPR in confined space from the side in an aircraft. Whereas the patient lies in
the aisle, the rescuer is placed sideward in the leg area.
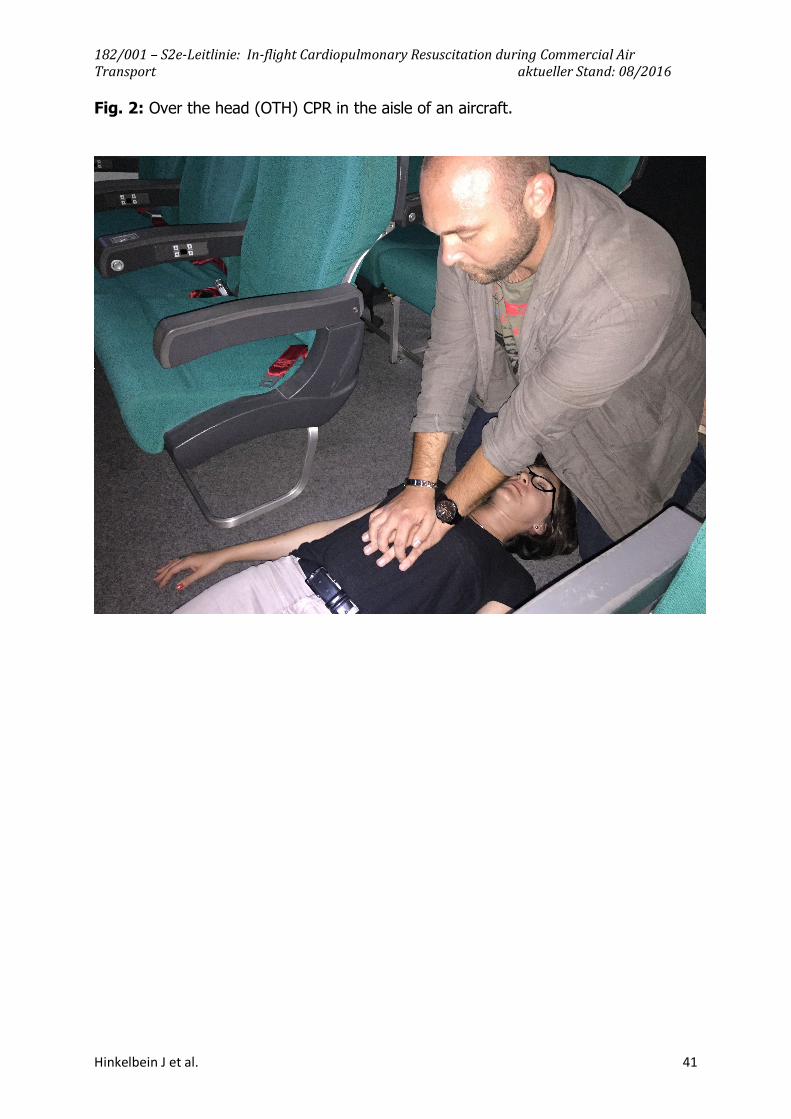
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 41
Fig. 2: Over the head (OTH) CPR in the aisle of an aircraft.
182/001 – S2e-Leitlinie: In-flight Cardiopulmonary Resuscitation during Commercial Air Transport aktueller Stand: 08/2016
Hinkelbein J et al. 42
Erstellungsdatum: 08/2016 Nächste Überprüfung geplant: 08/2021
Die "Leitlinien" der Wissenschaftlichen Medizinischen Fachgesellschaften sind systematisch entwickelte Hilfen für Ärzte zur Entscheidungsfindung in spezifischen Situationen. Sie beruhen auf aktuellen wissenschaftlichen Erkenntnissen und in der Praxis bewährten Verfahren und sorgen für mehr Sicherheit in der Medizin, sollen aber auch ökonomische Aspekte berücksichtigen. Die "Leitlinien" sind für Ärzte rechtlich nicht bindend und haben daher weder haftungsbegründende noch haftungsbefreiende Wirkung. Die AWMF erfasst und publiziert die Leitlinien der Fachgesellschaften mit größtmöglicher Sorgfalt - dennoch kann die AWMF für die Richtigkeit des Inhalts keine Verantwortung übernehmen. Insbesondere bei Dosierungsangaben sind stets die Angaben der Hersteller zu beachten!
© Deutsche Gesellschaft für Luft- und Raumfahrtmedizin Autorisiert für elektronische Publikation: AWMF online





























