Embed Size (px)
Citation preview

Transplantation Immunology

Transplantation Immunology rqd background understanding
MHC
antigen processing and presentation
MHC restriction
T cell differentiation
thymic selection
T cell activation
Chapters 4&5 Janeway

Transplantation
Tolerance
Rejection
Immunosuppression

Reading
• Pgs 644-650 : Janeway 7th Edition
• Starzl T, Zinkernagel R. Transplantation tolerance from a
historical perspective. Nature Reviews 2001;1:233-239

Transplantation
• Blood cell malignancies
• Organ failure
• Autoimmune disease

Transplantation
• Cornea
• Bone marrow
• Kidney
• Liver
• Heart
• Lungs
• Intestine
• Stem Cells



Graft Rejection: normal immune
response
• specific recipient immune response.
T-cell mediated :
New born mice do not reject grafts
Nude Mice.
rejection can be transferred by T-cells
•memory
.

Figure 5-17

Klein, J. et. al. N Engl J Med 2000;343:702-709
Location and Organization of the HLA Complex on Chromosome 6









Major Historical Events 1

Major Historical Events 2

T Cells Reject Graft/Genes Matter
• Autograft
• Syngeneic
• Allogeneic

Importance of HLA Matching

MHC polymorphisms affect TCR
interaction with the peptide–MHC
surface.

Figure 5-17


BM Transplantation/Tolerance

Classic Graft vs Host Disease

Organ Tx/Immunosuppression

MHC Restriction/T Cell Recognition

Figure 7-14

Thymic selection eliminates the most-
reactive and least-reactive TCRs.

Novel Tolerogenic Mechanisms
• Second signal (CD80/86)
• T regulatory cells
• Myeloid derived suppressor cells (MDSCs)
• NK Cells
– Kill DCs in donor organ
– Hepatic NK cells kill infiltrating T cells


1
Chapter 7
The Skeletal System:
Bone Tissue
2
INTRODUCTION
• Bone is made up of several different tissues
working together: bone tissue, cartilage, dense
connective tissue, epithelium, blood forming
tissues, adipose tissue, and nervous tissue
• Each individual bone is an organ
• Dynamic and ever-changing throughout life
• The bones, along with their cartilages, make up the
skeletal system
3
Functions of Bone
• Supporting & protecting soft tissues
• Attachment site for muscles making
movement possible
• Storage of the minerals, calcium &
phosphate -- mineral homeostasis
• Blood cell production occurs in red bone
marrow (hemopoiesis)
• Energy storage in yellow bone marrow
4
Anatomy of a Long
Bone
• diaphysis = shaft
• epiphysis = one end of a
long bone
• metaphyses are the
areas between the
epiphysis and diaphysis
and include the
epiphyseal plate in
growing bones.
• Articular cartilage over
joint surfaces acts as
friction reducer & shock
absorber
• Medullary cavity =
marrow cavity

5
Anatomy of a Long
Bone
• Endosteum = liningof marrow cavity
• Periosteum = toughmembrane coveringbone but not thecartilage
– fibrous layer =dense irregularCT
– osteogenic layer =bone cells & bloodvessels thatnourish or helpwith repairs
6
Histology of
Bone• A type of
connective tissue
as seen by widely
spaced cells
separated by
matrix
• Matrix of 25%
water, 25%
collagen fibers &
50% crystalized
mineral salts
• 4 types of cells in
bone tissue
7
Histology of Bone Tissue
• Bone (osseous) tissue consists of widely separated cells
surrounded by large amounts of matrix.
• The matrix of bone contains inorganic salts, primarily
hydroxyapatite and some calcium carbonate, and collagen
fibers.
• These and a few other salts are deposited in a framework of
collagen fibers, by a process called calcification.
– The process of calcification occurs only in the presence
of collagen fibers.
– Mineral salts confer hardness on bone while collagen
fibers give bone its great tensile strength.
8
Four Types of Bone Cells
• Osteoprogenitor (osteogenic) cells -- undifferentiated cells
– can divide to replace themselves & can become osteoblasts
– found in inner layer of periosteum and endosteum
• Osteoblasts -- form matrix & collagen fibers but can’t divide
• Osteocytes -- the principal cells of bone tissue.
– mature cells that no longer secrete matrix
• Osteoclasts -- huge cells from fused monocytes (WBC)
– serve to break down bone tissue
– function in bone resorption at surfaces such as endosteum

9
Matrix of Bone
• Inorganic mineral salts provide bone’s hardness
– hydroxyapatite (calcium phosphate) & calcium carbonate
• Organic collagen fibers provide bone’s flexibility
– their tensile strength resists being stretched or torn
• Remove minerals with acid & rubbery structure
results
• Denature collagen by heating and bones become
brittle
• Bone is not completely solid since it has small spaces
for vessels and red bone marrow
– spongy bone has many such spaces
– compact bone has very few such spaces
10
Compact Bone
• Compact bone is arranged in units called osteons
or Haversian systems
• Osteons contain blood vessels, lymphatic vessels,
nerves, and osteocytes along with the calcified
matrix.
• Osteons are aligned in the same direction along
lines of stress. These lines can slowly change as
the stresses on the bone changes.
11
Compact or
Dense Bone
• Looks like solid hard layer of bone
• Makes up the shaft of long bones and theexternal layer of all bones
• Resists stresses produced by weight andmovement
12
Histology of Compact Bone
• Osteon is concentric rings (lamellae) of calcified matrix
surrounding a vertically oriented blood vessel
• Osteocytes are found in spaces called lacunae
• Osteocytes communicate through canaliculi filled with
extracellular fluid that connect one cell to the next cell

13
Spongy Bone
• Spongy (cancellous) bone does not contain
osteons. It consists of trabeculae surrounding
many red marrow filled spaces
• It forms most of the structure of short, flat, and
irregular bones, and the epiphyses of long bones
• Spongy bone tissue is light and supports and
protects the red bone marrow
14
The Trabeculae of Spongy Bone
• Latticework of thin plates of bone called trabeculae oriented
along lines of stress
• Spaces in between these struts are filled with red marrow
where blood cells develop
No true Osteons.
15
Blood Supply of Bone
• Periosteal arteries
– supply periosteum
• Nutrient arteries
– enter through nutrient
foramen
– supplies compact bone
of diaphysis & red
marrow
• Metaphyseal & epiphyseal
arteries
– supply red marrow &
bone tissue of
epiphyses
16
BONE FORMATION
• All embryonic connective tissue begins as
mesenchyme
• Bone formation is termed osteogenesis or
ossification
• Two types of ossification occur
– Intramembranous ossification is the formation of bone
directly from fibrous connective tissue membranes
(dermis)
– Endochondral ossification is the formation of bone from
hyaline cartilage models

17
Intramembranous Bone Formation
• Intramembranous ossification forms the flat bones
of the skull and the mandible
– An ossification center forms from mesenchymal cells as
they convert to osteoblasts and lay down osteoid matrix.
– The matrix surrounds the cell and then calcifies as the
osteoblast becomes an osteocyte.
– The calcifying matrix centers join to form bridges of
trabeculae that constitute spongy bone with red marrow
between.
– On the periphery the mesenchyme condenses and
develops into the periosteum.
18
Intramembranous Bone
Formation
19
Endochondral Bone Formation
• Endochondral ossification involves replacement of
cartilage by bone and forms most of the bones of
the body
• The first step in endochondral ossification is the
development of the cartilage model
20
Endochondral Bone Formation
• Development and Growth of
Cartilage Model
– mesenchymal cells form a
cartilage model
– interstitial growth in length occurs
by chondrocyte cell division and
matrix formation
– appositional growth in width occurs
by formation of new matrix on the
periphery by new chondroblasts
from the perichondrium
– cells in midregion burst and
change pH triggering calcification
and chondrocyte death

21
Endochondral Bone Formation
• Development of Primary
Ossification Center
– nutrient artery penetrates center
of cartilage model
– cells in perichondrium
differentiate into osteoblasts and
start forming bone
– osteoblasts and osteoclasts
migrate to center of cartilage
model
– osteoblasts deposit bone matrix
over calcified cartilage forming
spongy bone trabeculae
– Osteoclasts form medullary cavity
22
Endochondral Bone Formation
• Development of Secondary Ossification Center
– blood vessels enter the epiphyses around time of birth
– spongy bone is formed but no medullary cavity
– cartilage on ends of bone remains as articular cartilage
23
Bone Growth in Length
• Bones grow in length at the epiphyseal (growth) plate
• The epiphyseal plate consists of four zones:
– zone of resting cartilage
– zone of proliferating cartilage
– zone of hypertrophic cartilage
– zone of calcified cartilage
• Activity at the epiphyseal plate is the only means by which
the diaphysis can increase in length
24
Zones of Growth in
Epiphyseal Plate• Zone of resting cartilage
– anchors growth plate to bone
• Zone of proliferating cartilage
– rapid cell division (stacked
coins)
• Zone of hypertrophic cartilage
– cells enlarged & remain in
columns
• Zone of calcified cartilage
– thin zone, cells mostly dead
since matrix calcified
– osteoclasts removing matrix
– osteoblasts & capillaries move
in to create bone over calcified
cartilage

25
Bone Growth in Length
• Between ages 18 to 25, epiphyseal
plates close
– cartilage cells stop dividing and
bone replaces the cartilage
(epiphyseal line)
• Growth in length stops by age 25
26
Bone Growth in Thickness
• Only by appositional growth at the bone’s surface
• Periosteal cells differentiate into osteoblasts and form bonyridges and then a tunnel around periosteal blood vessel
• Concentric lamellae fill in the tunnel to form an osteon
27
Factors Affecting Bone Growth
• Nutrition
– adequate levels of minerals and vitamins
• calcium and phosphorus for bone growth
• vitamin C for collagen formation
• vitamins K and B12 for protein synthesis
• Sufficient levels of specific hormones
– during childhood need insulin-like growth factor
• promotes cell division at epiphyseal plate
• need hGH (growth), thyroid (T3 & T4) and insulin
– at puberty the sex hormones, estrogen and testosterone,
stimulate sudden growth and modifications of the
skeleton to create the male and female forms
28
Hormonal Abnormalities
• Oversecretion of hGH (human growth hormone)
during childhood produces giantism
• Undersecretion of hGH or thyroid hormone during
childhood produces dwarfism
• Both men or women that lack estrogen receptors
on cells grow taller than normal
– estrogen is responsible for closure of growth
plate

29
Bone Remodeling
• Remodeling is the ongoing replacement of old bone
tissue by new bone tissue
– Old bone is constantly destroyed by osteoclasts, whereas
new bone is constructed by osteoblasts
– In orthodontics teeth are moved by braces. This places
stress on bone in the sockets causing osteoclasts and
osteablasts to remodel the sockets so that the teeth can
be properly aligned
– Several hormones and calcitriol control bone growth and
bone remodeling
30
Bone Remodeling
• Ongoing since osteoclasts carve out small tunnels
and osteoblasts rebuild osteons.
– osteoclasts form leak-proof seal around cell edges
– secrete enzymes and acids beneath themselves
– release calcium and phosphorus into interstitial fluid
– osteoblasts take over bone rebuilding
• Continual redistribution of bone matrix along lines
of mechanical stress
– distal femur is fully remodeled every 4 months
31
Fracture & Repair of Bone
• A fracture is any break in a bone
• Healing is faster in bone than in cartilage due
to lack of blood vessels in cartilage
• Healing of bone is still slow process due to
vessel damage
• Clinical treatment
– closed reduction = restore pieces to normal
position by manipulation
– open reduction = realignment during surgery
32
Fractures
• Named for shape or position of fracture line
• Common types of fracture
– greenstick -- partial fracture
– impacted -- one side of fracture driven into the
interior of other side

33
Fractures
• Common types of fracture
– closed -- no break in skin
– open fracture --skin broken
– comminuted -- broken ends of bones are
fragmented
34
Fractures
• Common types of fracture
– Pott’s -- distal fracture of fibula and/or tibia
– Colles’s -- distal fracture of radius and/or ulna
– stress fracture -- microscopic fissures from
repeated strenuous activities
35
Repair of a Fracture
• Formation of fracture hematoma
– damaged blood vessels produce clot in 6-8 hours, bone cells die
– inflammation brings in phagocytic cells for clean-up duty
– new capillaries grow into damaged area
• Formation of fibrocartilagenous (soft) callus
– fibroblasts invade & lay down collagen fibers
– chondroblasts produce fibrocartilage to span the broken ends of the
bone
36
Repair of a Fracture
• Formation of bony (hard) callus
– osteoblasts secrete spongy bone that joins 2 broken ends of
bone
– lasts 3-4 months
• Bone remodeling
– compact bone replaces the spongy bone in the bony callus
– surface is remodeled back to normal shape

37
Calcium Homeostasis & Bone Tissue
• Skeleton is a reservoir of calcium & phosphate
• Calcium ions involved with many body systems
– nerve & muscle cell function
– blood clotting
– enzyme function in many biochemical reactions
• Small changes in blood levels of Ca+2 can be
deadly
– plasma level maintained 9-11 mg/100mL
– cardiac arrest if too high
– respiratory arrest if too low
38
Hormonal Influences
• Parathyroid hormone (PTH) is
secreted if Ca+2 levels fall
– osteoclast activity increased,
kidney retains Ca+2 and
produces calcitriol
• Calcitonin hormone is
secreted from parafollicular
cells in thyroid if Ca+2 blood
levels get too high
– inhibits osteoclast activity
– increases bone formation by
osteoblasts
39
EXERCISE AND BONE TISSUE
• Bone has the ability to alter its strength in response to
mechanical stress by increasing deposition of mineral salts
and production of collagen fibers
– Removal of mechanical stress leads to weakening of
bone through demineralization and collagen reduction
• reduced activity while in a cast
• astronauts in weightless environment
• bedridden person
– Weight-bearing activities, such as walking or weightlifting,
help build and retain bone mass
40
AGING AND BONE TISSUE
• Of two principal effects of aging on bone, the first is the loss
of calcium and other minerals from bone matrix, which may
result in osteoporosis.
– very rapid in women 40-45 as estrogens levels decrease
– in males, begins after age 60
• The second principal effect of aging on the skeletal system
is a decreased rate of protein synthesis
– decrease in collagen production which gives bone its
tensile strength
– decrease in growth hormone
– bone becomes brittle & susceptible to fracture

41
Osteoporosis
• Decreased bone mass resulting in porous bones
• Those at risk
– white, thin, menopausal, smoking, drinking, female with
family history
– athletes who are not menstruating due to decreased body
fat & decreased estrogen levels
– people allergic to milk or with eating disorders whose intake
of calcium is too low
• Prevention or decrease in severity
– adequate diet, weight-bearing exercise, & estrogen
replacement therapy (for menopausal women)
– behavior when young may be most important factor
42
Disorders of Bone Ossification
• Rickets
• calcium salts are not deposited properly
• bones of growing children are soft
• bowed legs, skull, rib cage, and pelvic deformities
result
• Osteomalacia
• “adult rickets”
• new adult bone produced during remodeling fails
to ossify
• hip fractures are common
• Caused by vitamin D deficiency

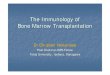
hematopoietic stem cell An immature cell that can develop into all types of blood cells, including white blood cells, red blood cells, and platelets. Hematopoietic stem cells are found in the peripheral blood and the bone marrow. Also called blood stem cell.
ENLARGE
Blood cell development. A blood stem cell goes through several steps to become a red blood cell, platelet, or white blood cell.

1. 1. What is Liver Transplantation? 2. 2. Liver transplantation is surgery to remove a diseased liver and
replace it with a healthy one. This kind of surgery has been done for more than 38 years. Many people have had liver transplants and now lead normal lives. When a patient receives a liver transplant, his or her entire liver is removed. It is then replaced by either a complete new liver or a portion of a healthy liver.
3. 3. What are the reasons for needing a Liver Transplant? 4. 4. Liver transplantation is needed for patients who are likely to die
because of liver failure. Many diseases can cause liver failure. The most common is cirrhosis which is the scarring and death of liver cells. Cirrhosis caused by hepatitis C is the most common reason for liver transplants.
5. 5. Other conditions that may ultimately require a liver transplant include: - Diseases of the bile ducts, including biliary atresia, primary biliary cirrhosis and primary sclorosing (PSC), which can cause liver failure if there is a backup of bile in the liver. - Some inherited diseases, such as Wilson Disease in which dangerous levels of copper build up in the body, and hemochromatosis, where the liver is overwhelmed by iron. - Primary liver cancer or cancer that affects only the liver - Alcoholism which can cause cirrhosis
6. 6. In adults, the most common reason for liver transplantation is cirrhosis. Cirrhosis: - is caused by many different types of liver injuries that destroy healthy liver cells and replace them with scar tissue. - can be caused by viruses such as hepatitis B and C, alcohol, autoimmune liver diseases, buildup of fat in the liver, and hereditary liver diseases. In children, the most common reason for liver transplantation is biliary atresia. Bile ducts: - which are tubes that carry bile out of the liver, are missing or damaged in this disease, and obstructed bile causes cirrhosis. Bile helps digest food. - Other reasons for transplantation are liver cancer, benign liver tumors, and hereditary diseases. Sometimes the cause of liver disease is not known.
7. 7. Liver transplants can help adults and children. 8. 8. What is the donor operation like? 9. 9. The donor operation is done through an incision in the upper
abdomen. If the LDLT recipient is a child, only a portion of the left part of the liver is removed from the donor: about 25% of the donor's total liver.
10. 10. If the LDLT recipient is an adult, a larger portion of the liver needs to be removed from the donor, usually the right portion of the liver: about 60% of the donor's total liver.
11. 11. The blood vessels supplying the portion of the liver to be removed are separated out, the liver itself is divided, and the portion

to be transplanted is removed. This portion is brought into a separate operating room for the recipient, where the transplant is then performed. The donor operation takes 6 to 8 hours.
12. 12. Liver Transplant Symptoms : People who have liver disease may have many of the following problems: - Jaundice - Yellowing of the skin or eyes - Itching - Dark, tea-colored urine - Gray- or clay-colored blood movements - Ascites - An abnormal buildup of fluid in the abdomen - Vomiting of blood - Tendency to bleed - Mental confusion, forgetfulness
13. 13. Where Does a Liver for a Transplant Come From? There are two types of liver transplantation options: living donor transplantation and cadaveric transplantation.
14. 14. Living donor - Living donor liver transplants are an option for some patients with end-stage liver disease. This involves removing a segment of liver from a healthy living donor and implanting it into a recipient. Both the donor and recipient liver segments will grow to normal size in a few weeks. - The donor, who may be a blood relative, spouse or friend, will have extensive medical and psychological evaluations to ensure the lowest possible risk. Blood type and body size are critical factors in determining who is an appropriate donor. - Recipients for the living donor transplantation must be active on the transplant waiting list. Their health must also be stable enough to undergo transplantation with excellent chances of success.
15. 15. Cadaver In cadaveric liver transplantation, the donor may be a victim of an accident or head injury. The donors heart is still beating, but the brain has stopped functioning. Such a person is considered legally dead, because his or her brain has permanently and irreversibly stopped working. The heart continues to beat because the donor is attached to a respirator. The respirator delivers an adequate supply of oxygen to all vital organs. At this point, the donor is in an intensive-care unit. The identity of a cadaveric donor and circumstances surrounding the person's death are kept confidential.
16. 16. Which Tests Are Required Before Getting a Liver Transplant? You will need to bring all of your previous doctor records, X-rays, liver biopsy slides and a record of medications to your pre-evaluation. To complement and to update previous tests, some or all of the following diagnostic studies are generally performed during your evaluation. If specific problems are identified, additional tests may be ordered. - Computed tomography, which uses X-rays and a computer to generate pictures of the liver, showing its size and shape. - Doppler ultrasound to determine if the blood vessels to and from your liver are open. - Echocardiogram to help evaluate your

heart. - Pulmonary function studies to determine your lungs' ability to exchange oxygen and carbon dioxide. Blood tests to determine blood type, clotting ability, and biochemical status of blood and to gauge liver function. AIDS testing and hepatitis screening are also
17. 17. What Happens When They Find a Match? When an organ has been identified for you, a transplant coordinator will contact you by telephone or by pager. Make sure that you do not eat or drink anything once you have been called to the hospital. The transplant coordinator will notify you of any additional instructions. When you arrive at the hospital, additional blood tests, an Electrocardiogram and a chest X-ray will generally be taken before the operation. You also may meet with the anesthesiologist and a surgical resident. If the donor liver is found to be acceptable you will proceed with the transplant. If not, you will be sent home to continue waiting.
18. 18. During Surgery: Liver transplant surgery takes between six and 12 hours. During the operation, doctors remove the diseased liver and replace it with the donated liver. Most patients stay in the hospital for up to three weeks after surgery. The surgeon will disconnect your diseased liver from your bile ducts and blood vessels before removing it. The blood that flows into your liver will be blocked or sent through a machine to return to the rest of your body. The surgeon will put the healthy liver in place and reconnect it to your bile ducts and blood vessels. Your blood will then flow into your new liver.
19. 20. After Surgery: - You will stay in the hospital for an average of 1 to 3 weeks to be sure your new liver is working. You will take medicines to prevent rejection of your new liver and to prevent infections. Your doctor will check for bleeding, infections, and rejection. During this time you will start to learn how to take care of yourself and use your medicines to protect your new liver after you go home. - In the hospital, you will slowly start eating again. You will start with clear liquids, then switch to solid food as your new liver starts to work. - Liver transplants are performed in many centers across the country. The healthy liver is obtained from a donor who has not suffered liver injury. The healthy liver is transported in a cooled saline solution that preserves the organ for up to 8 hours. This time allows for testing to determine if the blood and tissue of the donor match the recipient. The diseased liver is removed through an incision in the upper abdomen. The new liver is put in place and attached to the patient's blood vessels and bile ducts. The operation can take up to 12 hours and may require blood transfusions.
20. 21. - Patients require hospital care for 1 to 4 weeks after liver transplant, depending on the degree of illness. After liver transplantation, patients must take immunosuppressive medications

for the rest of their lives to prevent immune rejection of the transplanted organ.
21. 22. What Complications Are Associated With Liver Transplantation? - Two of the most common complications following liver transplantation are rejection and infection.
22. 23. Rejection: Your immune system works to destroy foreign substances that invade your body. The immune system, however, cannot distinguish between your transplanted liver and unwanted invaders, such as viruses and bacteria. Therefore, your immune system may attempt to attack and destroy your new liver. This is called a rejection episode. About 70% of all liver-transplant patients have some degree of organ rejection prior to discharge. Antirejection medications are given to ward off the immune attack.
23. 24. Infection: Because antirejection drugs that suppress your immune system are needed to prevent the liver from being rejected, you are at increased risk for infections. This problem diminishes as time passes. Not all patients have problems with infections, and most infections can be treated successfully as they occur.
24. 25. What are the side effects of a liver transplant? The most common side effects are caused by the drugs that treat or prevent rejection. These side effects can include: - fluid retention - raised blood pressure - headaches - diarrhea - nausea
25. 26. Blood tests will show if the new liver is being rejected. 26. 27. Eating a healthy diet and taking the medications are part of
taking care of your new liver. 27. 28. Indications: Liver transplantation is potentially applicable to
any acute or chronic condition resulting in irreversible liver dysfunction, provided that the recipient does not have other conditions that will preclude a successful transplant. Metastatic cancer outside liver, active drug or alcohol abuse and active septic infections are absolute contraindications. This has been changing recently. Advanced age and serious heart, pulmonary or other disease may also prevent transplantation. Most liver transplants are performed for chronic liver diseases that lead to irreversible scarring of the liver.

BRIEFING NOTES ON HUMAN STEM CELLS
What are stem cells? Stem cells are cells which can generate new copies of themselves, and can turn into the more specialised
cells (e.g. red blood cells) that perform functions in the body.
There are different types of stem cells, some of which can turn into any cell in the body (pluripotent) and
some of which can only turn into certain cells in one type of tissue (tissue specific).
Adult and foetal stem cells are tissue specific: they only turn into certain types of specialised cells.
- We all have adult stem cells in many of our tissues which repair and replenish damaged cells.
Embryonic stem cells exist only briefly after fertilisation, well before the embryo becomes a foetus, and
can turn into any cells in the body. This is why they are so important scientifically.
- Scientists can create induced pluripotent stem cells (iPS cells) which act like embryonic cells.
How do we get stem cells? Human embryonic stem cells are obtained from very early stage embryos, within 5-6 days of fertilisation.
- Most embryos used in stem cell research were initially created for use in IVF and are donated by parents.
- The cells isolated from the embryo give rise to one cell line which can produce an infinite number of cells
iPS cells do not occur naturally, but any adult cell could potentially be manipulated to become an iPS cell.
- There are various different te h i ues fo ep og a i g adult cells into iPS cells, though it is not yet
known whether any iPS cells can exactly mimic embryonic cells.
Adult and foetal stem cells can be isolated from specific tissues, where they are naturally small in number.
What are stem cells used for? Stem cell research does not just focus on medical treatments that put cells into patients: all types of stem
cell are used in basic research to understand how our bodies work and develop, and to understand disease.
- Studying disease at the cellular level provides an alternative to animal based models of drug discovery
Two distinct approaches exist for using stem cells in medical treatments, both the subject of research
1. Cell replacement therapies where cells are transplanted to integrate with the od s e isti g tissue
- Not all cell replacement therapies use stem cells, some use specialised cells
2. Using stem cells for the substances they release which encourage the body to repair itself
What stem cell-based treatments exist? There are only a few widely available stem cell-based treatments all of which use adult stem cells; there
are no current stem cell-based treatments that use embryonic or iPS stem cells.
- Blood stem cells have a long history of use in treating blood disorders
- Stem cells can be used to grow sheets of skin for use in skin grafts and wound healing
Cell replacement therapies for various conditions, including eye diseases, spinal cord injuries and stroke are
in clinical trials, but are not yet available outside trials.
Stem cell treatments that encourage natural repair, making use of substances that stem cells release, are in
early development for a range of neurological conditions as well as heart disease and diabetes.
Where does the scientific community stand? The majority of scientists think research on all stem cell types, including embryonic stem cells, is necessary
because of their obvious potential for the effective treatment of all sorts of conditions.
There is not enough evidence to say whether iPS cells can completely replace embryonic stem cells, though
there is a minority of scientists who have ethical reservations about embryonic stem cells.

What are the issues around stem cells?
Ethics
Some religious groups like the Catholic Church object to using human embryonic stem cells since they view the
destruction of very early stage embryos as the destruction of a human life; likewise they object to research on
human embryos and IVF treatment. There is an argument that iPS cells could, in theory, produce human life so
they do not answer these objections. Ethi al a d legal de ates est o he a e o gai s pe so hood , though this is a not a question the science alone can answer.
Patenting life: Some groups, including Greenpeace, have objected to the patenting of stem cells on
the basis that application of intellectual property rights to anything that represents a life should not be
allowed. One possible alternative is the patenting of technologies used to carry out stem cell research.
Stem cell tourism
Dramatic claims about the pote tial of ste ells to p o ide a u e fo e e thi g ha e prompted people to
travel to countries with unregulated clinics offering stem cell treatments for a huge range of conditions.
Primarily advertised on the web, such treatments tend to use stem cells for the beneficial substances they
produce, though patients may be wilfully deceived into believing they are receiving cell replacement therapies.
Even though there are numerous legitimate clinical trials taking place for treatments which use stem cells for
their beneficial products, most advertised treatments are not properly tested.
Why have we not seen more treatments?
Regenerative medicine is a very new field compared to traditional medicine, and to some extent the science is
running ahead of the regulatory system. Testing regenerative treatments is a challenge and our ability to
develop new treatments is limited by the fact that stem cell behaviour is not yet fully understood.
Clinical trials: The usual model for a clinical trial is hard to apply to regenerative medicine and
benefits of cell therapies are more likely to be seen at safety testing. However, benefits seen in safety
trials should not be interpreted as eakth ough u es as the e pe i e ts a e designed to assess
safety, not to look at how effective the treatments are.
Safety and side-effects
Concerns exist over the safety of using cells that can reproduce indefinitely in medical treatments. These
concerns are addressed when treatments go through proper clinical trials, but this is not the case for
unregulated treatments (see Stem cell tourism’).
Rejection: Treatments that transplant stem cells have a risk of rejection as the body recognises
differences in the DNA of transplanted cells. Therapies have been developed that use patient-derived
adult stem cells which avoid this problem, though we are far from making these commercially viable.
Cord blood and stem cell banking
Blood from the umbilical cord, which is rich in stem cells, can be stored indefinitely for use in later life. Cord
blood can be donated to public banks, or private companies offer storage for use by the baby or his/her
relatives in later life. Storage of fat tissue (adipose cells) and dental tissue is also possible. There is some
controversy over the logic of private stem cell banking since the likelihood of the donor needing their own cells
is small, and future scientific developments may make the stored tissue obsolete.

Links/Further Information
EuroStemCell is a Europe-wide collaboration of research centres aimed at public engagement. Great resource
for information including fact sheets and FAQs spanning all topics
www.eurostemcell.org/
Wellcome Trust resources on stem cell, including succinct information on research and medical potential
http://www.wellcome.ac.uk/About-us/Policy/Spotlight-issues/Human-Fertilisation-and-Embryology-Act/Stem-
cell-basics/index.htm
Stem cell science - Hope not hype pu li atio Biotechnology and Biological Sciences Research Council
http://www.bbsrc.ac.uk/web/FILES/Publications/hope_not_hype.pdf
BioNews provides timely news and comment on embryo/stem cell research and related topics
www.bionews.org.uk
The UK Stem Cell Bank provides a repository of human embryonic, foetal and adult stem cell lines as part of the
UK governance for the use of human embryos for research
http://www.ukstemcellbank.org.uk/
Scientific Opinion Paper on Umbilical Cord Blood Banking from the Royal College of Obstetricians and
Gynaecologists
www.rcog.org.uk/womens-health/clinical-guidance/umbilical-cord-blood-banking
The International Society for Stem Cell Research (ISSCR) has become the voice of the stem cell research
community
www.isscr.org/
These Briefing Notes have been written by the Science Media Centre in consultation with a number of
scientists, science press officers and broadcast journalists. They are not intended as a comprehensive
summary on a subject, but rather a snapshot of the basics, of points of controversy and a pointer towards
sources of more detailed information. They are subject to change and will be updated as and when the
science moves on.
For more information about our Briefing Notes, please contact the Science Media Centre on 020 7611 8300
or email [email protected].
Science Media Centre is a registered charity (no. 1140827) and a company limited by guarantee (no. 7560997).
Registered in England and Wales. Registered address: 215 Euston Road, London, NW1 2BE.

1

2

3

4

5

6

7

8

9

10

11

12

13

14

15

16

17

18

19

20

21

22

23

24

25

26

27

28

29


Roles in the BodyRoles in the Body
(and fibrocartilage)
Joint Capsule
http: / /adam.about.com/encyclopedia/19089.htm

DescriptionDescription
Soft connective tissue composed of Soft connective tissue composed of
densely packed collagen fibersdensely packed collagen fibersWhiteWhiteRelatively inelastic Relatively inelastic
Mechanical properties vary with shape and Mechanical properties vary with shape and
structural organizationstructural organization
Simon, SR. Simon, SR. Orthopaedic Basic ScienceOrthopaedic Basic Science. Ohio: American Academy of Orthopaedic Surgeons; 1994.. Ohio: American Academy of Orthopaedic Surgeons; 1994.

StructureStructure
Connective tissues are characterized by Connective tissues are characterized by sparse cellularity distributed within an sparse cellularity distributed within an extracellularextracellular matrixmatrix
Cells in tendons and ligaments are Cells in tendons and ligaments are called called fibroblastsfibroblasts

ComparisonComparison
LigamentsLigaments TendonsTendons
% of collagen% of collagen LowerLower HigherHigher
% of ground % of ground substancesubstance
HigherHigher LowerLower
OrganizationOrganization More randomMore random OrganizedOrganized
OrientationOrientationWeaving Weaving patternpattern
Long axis Long axis directiondirection
Simon, SR. Simon, SR. Orthopaedic Basic ScienceOrthopaedic Basic Science. Ohio: American Academy of Orthopaedic Surgeons; 1994.. Ohio: American Academy of Orthopaedic Surgeons; 1994.

CompositionComposition
COMPONENTCOMPONENT LI GAMENTLI GAMENT TENDONTENDON
Cellular Materials:Cellular Materials:
FibroblastsFibroblasts 20%20% 20%20%
ExtracellularExtracellular::
WaterWater 6060--80%80% 6060--80%80%
SolidsSolids 2020--40%40% 2020--40%40%
CollagenCollagen 7070--80%80% Slightly higherSlightly higher
TypeType II 90%90% 9595--99%99%
TypeType I I II I I 10%10% 11--5%5%
GroundGroundsubstancesubstance
2020--30%30% Slightly lesserSlightly lesser
ElastinElastin Up to 2X collagenUp to 2X collagen ScarceScarce

StrengthStrength
LigamentLigament TendonTendon
Tensile Tensile StrengthStrength
Less than Tendon; Varies Less than Tendon; Varies 50 to 150 50 to 150 MPaMPa
Elastic Elastic ModulusModulus
MeniscofemoralMeniscofemoral (355 (355 ±± 234 234 MPaMPa
AnterolateralAnterolateral bundle of PCL (294 bundle of PCL (294 ±± 115MPa)115MPa)
Posterior bundle of PCL (150 Posterior bundle of PCL (150 ±± 69MPa)69MPa)
1,200 1,200 –– 1,800 1,800 MPaMPa
* Wide ranges of mechanical properties are largely due to locatio* Wide ranges of mechanical properties are largely due to location and agen and age
http: / / ttb.eng.wayne.edu/~ grimm/BME5370/Lect5Out.html
http: / /dahweb.engr.ucdavis.edu/dahweb/126site/chp5.pdf

Biomechanical BehaviorBiomechanical Behavior
Measured material property values vary Measured material property values vary due to:due to:
LocationLocation
Varying degrees of crimpVarying degrees of crimp
Use: Mobilization/ ImmobilizationUse: Mobilization/ Immobilization
AgingAging
PregnancyPregnancy
DiabetesDiabetes
NSAID useNSAID use
HemodialysisHemodialysis

ViscoelasticViscoelastic ResponsesResponses
Tissue response to load dependent on:Tissue response to load dependent on:Magnitude of loadMagnitude of load
Duration of loadDuration of load
Prior loadingPrior loading
Affected by movement of waterAffected by movement of waterResistance to compressive force due to water trapped Resistance to compressive force due to water trapped in in proteoglycansproteoglycans
Contributes to sustained or cyclic responses to stressContributes to sustained or cyclic responses to stress
Types of ResponseTypes of ResponseCreepCreep
StressStress--RelaxationRelaxation
HysteresisHysteresishttp: / /www.tendinosis.org/ injury.html

CreepCreep
Time dependent elongation of Time dependent elongation of a tissue when subjected to a a tissue when subjected to a constant stressconstant stress
Example:Example:
Tendons: in an isometric Tendons: in an isometric contraction, the tendon will contraction, the tendon will lengthen slightly and more lengthen slightly and more muscle fibers will be recruited in muscle fibers will be recruited in order to maintain the position of order to maintain the position of the limbthe limb
Ligaments: joints will loosen Ligaments: joints will loosen with time, decreasing the with time, decreasing the possibility of injurypossibility of injury
http: / / ttb.eng.wayne.edu/~ grimm/ME518/L5A3.html
http: / /www.orthoteers.co.uk/Nrujp~ ij33lm/Orthconntiss.htm

StressStress--RelaxationRelaxation
Time dependent decrease in Time dependent decrease in applied stress required to applied stress required to maintain a constant elongationmaintain a constant elongation
Example:Example:
Tendons: in an isotonic Tendons: in an isotonic contraction, the stress will contraction, the stress will decrease with timedecrease with time
Ligaments: joints will loosen Ligaments: joints will loosen with time, decreasing the with time, decreasing the possibility of injurypossibility of injury
http: / / ttb.eng.wayne.edu/~ grimm/ME518/L5A3.html
http: / /www.orthoteers.co.uk/Nrujp~ ij33lm/Orthconntiss.htm

HysteresisHysteresis
Energy lost within the tissue between Energy lost within the tissue between loading and unloadingloading and unloading
Response of tissue becomes more repeatableResponse of tissue becomes more repeatable
Subsequent use of same force results in Subsequent use of same force results in greater deformationgreater deformation

Ligaments
silver.neep.wisc.edu/ ~ lakes/ linksLec3.html

Anterior Cruciate Posterior Cruciate Ligament
Ligament
Lateral CollateralMedial Collateral LigamentLigament
Anterior View of KneeAnterior View of Knee

Posterior View of KneePosterior View of Knee
Posterior View: Right knee in extension
www.ma.psu.edu/ ~ pt/ re nee384/ anatomy.htm
Lateral meniscus
Anterior cruciate ligament
Medial meniscus
Posterior cruciate ligament
Click for more detail

Superior View of KneeSuperior View of Knee
Posterior cruciate ligament
Medial meniscus
Lateral meniscus
Anterior cruciate ligament

StructureStructure
No molecular bonds between No molecular bonds between fasciclesfascicles
Free to slide relative to each Free to slide relative to each otherother
Orientations:Orientations:
Branching & InterwovenBranching & InterwovenSpirally wound: Ex ACLSpirally wound: Ex ACL
ParallelParallelDirect connection between Direct connection between bones: Ex Collateral bones: Ex Collateral LigamentsLigaments
Smaller diameter fibers than in Smaller diameter fibers than in tendonstendons
http: / /dahweb.engr.ucdavis.edu/dahweb/126site/chp4.pdf http: / / silver.neep.wisc.edu/~ lakes/BME601Fr.html
Simon, SR. Simon, SR. Orthopaedic Basic ScienceOrthopaedic Basic Science. Ohio: American Academy of Orthopaedic Surgeons; 1994.. Ohio: American Academy of Orthopaedic Surgeons; 1994.

CrimpingCrimpingOrientation of collagen in ligamentsOrientation of collagen in ligamentsAllows elongation of fibers before tensile stresses are experienAllows elongation of fibers before tensile stresses are experiencedced


FunctionsFunctions
Transmit loadTransmit load from bone to bonefrom bone to bone
Hold the skeleton togetherHold the skeleton together
Flexible but plasticFlexible but plastic
Provide stability at jointsProvide stability at jointsMaintain joint congruency Maintain joint congruency
Limit freedom of movementLimit freedom of movementPrevent excessive motion by being a static restraintPrevent excessive motion by being a static restraintOccasionally act as a positional bend/strain sensorOccasionally act as a positional bend/strain sensor
Mediate motions between opposing Mediate motions between opposing fibrocartilagefibrocartilage surfacessurfaces

Degrees of FreedomDegrees of Freedom
Potentially 6 degrees of freedom in all jointsPotentially 6 degrees of freedom in all joints33--plane rotationplane rotation
oo FlexionFlexion--extensionextension
oo AbductionAbduction--adductionadduction
oo InternalInternal--externalexternal
3 3 --plane translationplane translationoo MedialMedial-- laterallateral
oo CompressionCompression--distraction distraction
oo AnteriorAnterior--posteriorposterior

Primary Restraint*Primary Restraint*
Knee FlexKnee Flex Maximal StretchMaximal Stretch@Knee flexion @Knee flexion
of (of ( °° ))
Anterior CruciateAnterior Cruciateanterior anterior tibialtibialtranslationtranslation
30 30 -- 4545
Posterior CruciatePosterior Cruciateanterior anterior tibialtibialtranslationtranslation
9090
Medial CollateralMedial CollateralValgusValgus forces forces
internal tibia rotationinternal tibia rotation
00
1010--6060
Lateral CollateralLateral Collateral varusvarus forcesforces 00
* No peer* No peer--reviewed documentation to support this informationreviewed documentation to support this information

Mec
han
ical
Beh
avi
or
Mec
han
ical
Beh
avi
or H
um
an c
adav
eric
AC
L in
kn
ee j
oin
t
3a

Tensile Response CurveTensile Response Curve
Region 1Region 1““ToeToe””
Crimp: low stiffness; change in slope as Crimp: low stiffness; change in slope as collegencollegen fibers fibers straighten; ligaments become more stiff as more fibers straighten; ligaments become more stiff as more fibers are recruitedare recruited
Region 2Region 2Linear Region: slope = stiffness/Elastic Modulus Linear Region: slope = stiffness/Elastic Modulus
Elastic: higher stiffnessElastic: higher stiffness
Region 3Region 3Less linear behavior; deformation is permanent Less linear behavior; deformation is permanent (tearing, stretch); Area of (tearing, stretch); Area of MicrofailureMicrofailure;;Ultimate Load: where failure occurs (N)Ultimate Load: where failure occurs (N)
Region 3aRegion 3aEnergy absorbed to failure: area under the curve Energy absorbed to failure: area under the curve ((NmmNmm))
Region 4Region 4 Ligament rupturesLigament ruptures
Region 5Region 5Ligament may appear intact; Fibers to slide under low Ligament may appear intact; Fibers to slide under low loadsloads

Stress Vs. StrainStress Vs. StrainMore relevant method of expressing Force vs. More relevant method of expressing Force vs. Deformation behaviorDeformation behavior
Region descriptions same as Force vs. Deformation curveRegion descriptions same as Force vs. Deformation curve
Stress (N/mmStress (N/mm22) = load per cross) = load per cross--sectional area of sectional area of samplesample
Strain = percentage change in lengthStrain = percentage change in length

InjuriesInjuriesOccur most frequently during athletic activitiesOccur most frequently during athletic activities
Knee injuriesKnee injuriesACLACL
Partial or complete tear of ligament caused by quick changes in Partial or complete tear of ligament caused by quick changes in direction, direction, slowing down while running, landing a jump, direct contactslowing down while running, landing a jump, direct contact
Symptoms include delayed pain and swellingSymptoms include delayed pain and swelling
PCLPCLSprain of ligament due to overstretching, impact to the front ofSprain of ligament due to overstretching, impact to the front of the knee, the knee, misstepmisstep
MCLMCL
DiagnosisDiagnosisPress gently at knee cap to feel for fluid at the jointPress gently at knee cap to feel for fluid at the joint
XX--rayray
MRIMRI
http: / /http: / / orthoinfo.aaos.org/ fact/ thr_report.cfm?Thread_IDorthoinfo.aaos.org/ fact/ thr_report.cfm?Thread_ID= 157&topcategory= Knee= 157&topcategory= Knee
http: / /hcd2.bupa.co.uk/ fact_sheets/mosby_factsheets/Knee_ligamenhttp: / /hcd2.bupa.co.uk/ fact_sheets/mosby_factsheets/Knee_ligament_injuries.htmlt_injuries.html

HealingHealing
RICERICERest, Ice, Compression, ElevationRest, Ice, Compression, Elevation
Physical therapyPhysical therapyStrengthening exercisesStrengthening exercises
Range of motion testsRange of motion tests
BracesBraces
CrutchesCrutches
SurgerySurgery
http: / /http: / / orthoinfo.aaos.org/ fact/ thr_report.cfm?Thread_IDorthoinfo.aaos.org/ fact/ thr_report.cfm?Thread_ID= 157&topcategory= Knee= 157&topcategory= Knee
http: / /hcd2.bupa.co.uk/ fact_sheets/mosby_factsheets/Knee_ligamenhttp: / /hcd2.bupa.co.uk/ fact_sheets/mosby_factsheets/Knee_ligament_injuries.htmlt_injuries.html

http:/ /12.31.13.115/hwdb/ images/hwstd/medical/orthoped/n5550876.jpg

StructureStructure
Long cylindrical structures Long cylindrical structures Tightly packed longitudinally running collagen Tightly packed longitudinally running collagen fibersfibers
Nuclei and sparse cytoplasm of fibrocytes Nuclei and sparse cytoplasm of fibrocytes compressed almost flat between them compressed almost flat between them
Relatively avascularRelatively avascular
Slow to heal from trauma injuriesSlow to heal from trauma injuries
http: / /adam.about.com/encyclopedia/19089.htmhttp: / /adam.about.com/encyclopedia/19089.htm

AttachmentAttachment
Each muscle has two tendons:Each muscle has two tendons:
Proximal:Proximal: MyotendinousMyotendinous JunctionJunction (MTJ)(MTJ)The point of union with a muscle: origin The point of union with a muscle: origin
Distal:Distal: OsteotendinousOsteotendinous JunctionJunction (OTJ)(OTJ)The point of union with a bone: insertionThe point of union with a bone: insertion

FunctionFunction
Force transmission between muscle and boneForce transmission between muscle and boneSustain high tensile stressesSustain high tensile stresses
Conserve substantial muscular energy during Conserve substantial muscular energy during locomotionlocomotion
Energy storage capacityEnergy storage capacity
Enables the muscle belly to be at a convenient Enables the muscle belly to be at a convenient
distance from joint distance from joint
Satisfies kinematic and damping requirementsSatisfies kinematic and damping requirements

FunctionFunctionWithstand tensile forces while retaining Withstand tensile forces while retaining flexibilityflexibility

StructureStructure
Orientations:Orientations:
Parallel to direction of tensile forceParallel to direction of tensile force
Larger collagen fibers than in ligamentsLarger collagen fibers than in ligaments

Structure of TendonsStructure of Tendons

Collagen Fibers

In Vitro Tensile TestIn Vitro Tensile Test
Tissue is elongated to failureTissue is elongated to failurePrescribed ratePrescribed rate
Changes in force are recordedChanges in force are recorded
The force is plotted against timeThe force is plotted against time
Time axis is proportional to elongationTime axis is proportional to elongation
Constant strain rate Constant strain rate

Response to Tensile ForcesResponse to Tensile Forces
Highest tensile strength of any soft tissueHighest tensile strength of any soft tissue
Schematic loadSchematic load--elongation curve with 3 distinct elongation curve with 3 distinct regions of response to tensile loading:regions of response to tensile loading:

Mechanical BehaviorMechanical Behavior
Energy absorbed to failure: area under the curve

Mechanical BehaviorMechanical BehaviorRegion 1: Region 1: ““ToeToe”” RegionRegion
Collagen fibers straighten (less prominent than in ligaments Collagen fibers straighten (less prominent than in ligaments because fibers begin more aligned); Continued elongation stiffenbecause fibers begin more aligned); Continued elongation stiffens s tissuetissue
Region 2:Region 2:
Linear Linear ResponseResponse
Region 3Region 3
Region 4:Region 4:
Macroscopic Macroscopic FailureFailure
Slope represents stiffness; Micro failure occurs at the end;Slope represents stiffness; Micro failure occurs at the end;
Elastic recovery at stresses less than 4%Elastic recovery at stresses less than 4%
Corresponds to strains of 3Corresponds to strains of 3--8%8%
CrosslinksCrosslinks fail; Collagen fibers slide past one another; irreversible fail; Collagen fibers slide past one another; irreversible changes such as tearing or permanent stretching occurschanges such as tearing or permanent stretching occurs
Tensile failure of the fibersTensile failure of the fibers
Shear failure between the fibersShear failure between the fibers
Once maximum load is surpassedOnce maximum load is surpassed
Complete failure occurs rapidlyComplete failure occurs rapidly
Fibers recoil and blossomFibers recoil and blossom
Tangled bud at ruptured endTangled bud at ruptured end
Loses Load supporting abilityLoses Load supporting ability

Mechanical Properties (ContMechanical Properties (Cont’’d)d)
Greater crossGreater cross--sectional areasectional areaLarger loads can be applied prior to failureLarger loads can be applied prior to failure
Increased tissue strengthIncreased tissue strength
Increased StiffnessIncreased Stiffness
Longer tissue fibersLonger tissue fibersGreater fiber elongation before failureGreater fiber elongation before failure
Decreased tissue stiffnessDecreased tissue stiffness
Unaltered tissue strengthUnaltered tissue strength

InjuriesInjuries
OveruseOveruse
Spontaneous RuptureSpontaneous Rupture
DislocationDislocation
Thermal InjuriesThermal Injuries
Other InjuriesOther Injuries

HealingHealing
RegenerationRegenerationNew tissue identical to normal tissueNew tissue identical to normal tissue
StructurallyStructurallyFunctionallyFunctionally
Soft tissue injury healingSoft tissue injury healing
Scar repairScar repairRepair by connective tissueRepair by connective tissue
Inferior structural propertiesInferior structural propertiesInferior functional propertiesInferior functional properties
Or by their combinationOr by their combination

Healing ProcessHealing Process
Inflammation phase Inflammation phase From the first day of injury to the fourth From the first day of injury to the fourth through seventh daythrough seventh day
Proliferative phase Proliferative phase From the seventh through twentyFrom the seventh through twenty--first dayfirst day
Maturation or remodeling phase Maturation or remodeling phase From three weeks to one year From three weeks to one year

The End

Anterior Cruciate LigamentAnterior Cruciate Ligament

ACL: LocationACL: Location

ACL: FlexionACL: Flexion
AA-- AA’’ –– AnteromedialAnteromedial bandbandBB-- BB’’ –– I ntermediate componentI ntermediate componentCC-- CC’’ –– PosterolateralPosterolateral aspect of ligamentaspect of ligament

ACLACL
Located between the femur and tibia at the Located between the femur and tibia at the center of the kneecenter of the knee
Origin from lateral femoral condyleOrigin from lateral femoral condyleInsert into the surface of tibial plateauInsert into the surface of tibial plateauIntracapsularIntracapsularExtrasynovialExtrasynovial
Consists of two bundlesConsists of two bundlesAnteromedialAnteromedialPosterolateralPosterolateral
Blood supply originates primarily from femoral Blood supply originates primarily from femoral sideside
http: / /www.amershamhealth.com/medcyclopaedia/medical/ volume% 20I I I% 201/CRUCIATE% 20LIGAMENT.ASP

Posterior Cruciate Ligament:Posterior Cruciate Ligament:
LocationLocation

PCL: FlexionPCL: Flexion
AA-- AA’’ –– Small bandSmall bandBB-- BB’’ –– Bulk of the ligamentBulk of the ligamentCC-- CC’’ –– Anterior Anterior meniscofemoralmeniscofemoral ligamentligament

PCLPCLLocationLocation
Origin: Medial femoral condyleOrigin: Medial femoral condyle
Insert: Posterior cortical surface of tibia in the sagittal Insert: Posterior cortical surface of tibia in the sagittal midlinemidline
Intimately associated with posterior capsuleIntimately associated with posterior capsuleCovered by SynoviumCovered by Synovium
Less susceptible to vascular injury than ACLLess susceptible to vascular injury than ACL
Blood supply comes from middle geniculate Blood supply comes from middle geniculate arteryartery
Spiral shape permits tibiofemoral rotationSpiral shape permits tibiofemoral rotation

Medial Collateral LigamentMedial Collateral Ligament

MCLMCL
Primary stabilizer of the medial aspectPrimary stabilizer of the medial aspect
LocationLocationOrigin: Medial femoral Origin: Medial femoral condylecondyle at the at the adductor tubercleadductor tubercle
Fans out in anterior and posterior directionsFans out in anterior and posterior directions
Insert: Medial side of tibiaInsert: Medial side of tibia
Has both superficial and deep layerHas both superficial and deep layer
Visually appears like a sailboatVisually appears like a sailboat

MCL (ContMCL (Cont’’d)d)
Deep LayerDeep LayerOriginates at adductor tubercleOriginates at adductor tubercle
Separates distallySeparates distally
Above the joint line Above the joint line Inserts into the medial meniscusInserts into the medial meniscus
Holds the fibro cartilage in placeHolds the fibro cartilage in place
Along the inferior meniscal margin Along the inferior meniscal margin Blends into superficial layerBlends into superficial layer
Inserts into the medial tibial diaphysisInserts into the medial tibial diaphysis
Has generous blood supplyHas generous blood supply

Lateral Collateral LigamentLateral Collateral Ligament


Ligament of HumphreyLigament of Humphrey

Ligament of Ligament of WrisbergWrisberg




Other InjuriesOther Injuries
Tendon AvulsionsTendon AvulsionsTendon StrainsTendon StrainsPartial Tendon rupturesPartial Tendon rupturesLacerationsLacerationsTendon divisionTendon divisionForeign bodies in TendonsForeign bodies in TendonsBite Injuries and Bite Injuries and AcupuntureAcupunture induced induced complicationscomplications

Ten
don
Com
pos
itio
n

Joint Rotations

Knee Translations

FibrocartilageFibrocartilage
Fibrocartilage Fibrocartilage (n.)(n.) A kind of A kind of cartilage with a cartilage with a fibrous matrix and fibrous matrix and approaching fibrous approaching fibrous connective tissue in connective tissue in structure structure
http: / /www.kumc.edu/ instruction/medicine/anatomy/histoweb/cart/ cart12.htm
http: / /www.brainydictionary.com/words/ fi/ fibrocartilage164589.html

FibroblastsFibroblasts
Any cell or corpuscle from which connective Any cell or corpuscle from which connective tissue is developedtissue is developed
Oriented longitudinally with respect to tissueOriented longitudinally with respect to tissueOvoid or spindle shapedOvoid or spindle shaped
http: / /www.digitalnaturopath.com/cond/C136641.html

FibroblastsFibroblasts
Secrete and absorb matrix Secrete and absorb matrix elementselements
Components: Components: CollagenCollagenProteoglycansProteoglycansElastinElastin (recoil) (recoil) FibronectinFibronectin (cell(cell-- toto--cell cell
adhesion and migration)adhesion and migration)

Joint CapsuleJoint CapsuleFluid sac at joints that holds joints togetherFluid sac at joints that holds joints together
Creates skeletal system for Creates skeletal system for synovialsynovial membranemembraneLigaments or tendons thicken the exteriorLigaments or tendons thicken the exteriorProtects cartilage, muscles, connective tissueProtects cartilage, muscles, connective tissue
Difficult to identify ligaments and tendons from capsule Difficult to identify ligaments and tendons from capsule in the bodyin the body
http://physicaltherapy.about.com/cs/disabilities/l/aa111700f.htmhttp://web1.tch.harvard.edu/cfapps/A2ZtopicDisplay.cfm?Topic=Anatomy%20of%20a%20Joint

CollagenCollagen
Different Types: Different Types: I> > > I I I> > V,VI ,X,XI II> > > I I I> > V,VI ,X,XI I
Collagen Type I is Collagen Type I is fibrillarfibrillarMade up of three Made up of three polypeptide chainspolypeptide chains
22αα11
11αα22
Chains are leftChains are left --handed handed helixes but are wound helixes but are wound together in a righttogether in a right --handed handed helixhelix
http: / /www.accessexcellence.org/RC/VL/GG/collagen_Elastin.htmlhttp: / / en.wikipedia.org/wiki/Collagen

CollagenCollagen
Hydrogen bonds form Hydrogen bonds form between between glycinesglycines(( interchaininterchain) and ) and prolinesprolinesand and hydroxyprolineshydroxyprolines(( interchaininterchain))
CrossCross-- links between links between collagen molecules collagen molecules ““headhead--toto--tailtail”” and staggered in and staggered in parallelparallel

CollagenCollagen
Hydrogen bonds and Hydrogen bonds and crosscross-- links contribute links contribute to the stability of to the stability of each molecule and each molecule and aggregation at the aggregation at the fibril levelfibril level
Result: Structures Result: Structures extremely resistant extremely resistant to tensile forcesto tensile forces
http: / /www.orthoteers.co.uk/Nrujp~ ij33lm/Orthconntiss.htm

Additional PicturesAdditional Pictures