Embed Size (px)
Citation preview

B
C
Tr
Lc
CDL
a
b
c
B
RA
I
IdordgFsdr
JgJ
l
O
h1a
raz J Otorhinolaryngol. 2018;84(5):660---664
www.bjorl.org
Brazilian Journal of
OTORHINOLARYNGOLOGY
ASE REPORT
ransoral robotic supraglottic partial laryngectomy:eport of the first Brazilian case�
aringectomia parcial supraglótica transoral robótica: relato do primeiroaso brasileiro
laudio Roberto Cerneaa,b,∗, Leandro Luongo Matosa,∗,orival de Carlucci Juniora, Fernando Danelon Leonhardtc,eonardo Haddadc, Fernando Walderc
Universidade de São Paulo (USP), Faculdade de Medicina, Disciplina de Cirurgia de Cabeca e Pescoco, São Paulo, SP, BrazilHospital Israelita Albert Einstein, São Paulo, SP, BrazilUniversidade Federal de São Paulo (UNIFESP), Disciplina de Otorrinolaringologia - Cirurgia de Cabeca e Pescoco, São Paulo, SP,razil
teittaaaasq
pitu
eceived 14 December 2015; accepted 16 January 2016vailable online 3 May 2016
ntroduction
n the past decade, we have witnessed the introduction andissemination of transoral robotic surgery for the treatmentf tumors, mainly of the oropharynx and larynx. The use ofobotic surgery improves visualization of the operative fieldue to its three-dimensional image and enhances the sur-eon’s dexterity due to bimanual control of the robotic arms.urthermore, the assistant contributes with suction and tis-ue traction, which leads to the use of four instrumentsuring surgery, something impossible during a transoralesection through laryngoscopy, for instance.1 Therefore,
� Please cite this article as: Cernea CR, Matos LL, de Carlucciunior D, Leonhardt FD, Haddad L, Walder F. Transoral robotic supra-lottic partial laryngectomy: report of the first Brazilian case. Braz
Otorhinolaryngol. 2018;84:660---64.∗ Corresponding authors.
E-mails: [email protected] (C.R. Cernea),[email protected] (L.L. Matos).
Peer Review under the responsibility of Associacão Brasileira detorrinolaringologia e Cirurgia Cérvico-Facial.
C
Amsi
ttps://doi.org/10.1016/j.bjorl.2016.01.016808-8694/© 2016 Associacao Brasileira de Otorrinolaringologia e Cirurgiccess article under the CC BY license (http://creativecommons.org/lic
he technique makes the approach truly minimally invasive,specially in the case of supraglottic partial laryngectomy,n which the conventional open approach inevitably leadso protective tracheostomy and feeding tube use, some-imes for prolonged periods. The robotic access, however,llows for early feeding without the need of a tube, andlso eliminates the need for tracheostomy in many cases,s the rates of aspiration, fistulas, or other complicationsre significantly reduced when compared with conventionalurgery and with oncologic and functional results that areuite similar between the two techniques.2
Therefore, this study reports the first case of supraglotticartial laryngectomy performed by transoral robotic surgeryn Brazil, as well as documents the late oncologic and func-ional results (Approved by the Research Ethics Committeender No. 228/14).
ase report
57-year-old female patient was evaluated for a fouronth complaint of odynophagia; she was a long-term
moker (30 pack-years) and a non-alcoholic. Physical exam-nation revealed no lesions at the oroscopy and no palpable
a Cervico-Facial. Published by Elsevier Editora Ltda. This is an openenses/by/4.0/).
Robotic supraglottic laryngectomy 661
A B C
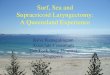
in the epiglottis and affecting the left aryepiglottic fold in the axial
A
B
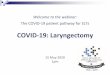
Figure 2 Intraoperative period. (A) Positioning of roboticas
trlpseaccbr
Figure 1 Computed tomography depicting a vegetative lesion(A), coronal (B), and sagittal (C) views.
cervical lymph nodes. The nasofibrolaryngoscopy identifieda large vegetating lesion affecting the entire epiglottis andextending to the left aryepiglottic fold, but not affecting thearytenoid fold or the left ventricular fold; both vocal foldswere still mobile.
An incisional biopsy revealed that the lesion was amoderately differentiated squamous cell carcinoma (SCC).Assessment by computed tomography (Fig. 1) showed thatthe lesion had limits compatible with the laryngoscopy, with-out pre-epiglottic space involvement and without cervicallymph nodes suggestive of metastases. There was no evi-dence of pulmonary metastases; the search for a secondprimary tumor through high digestive endoscopy with chro-moendoscopy was negative, and the cancer was staged asT2N0M0 (stage II).
The patient then underwent a transoral robotic supra-glottic partial laryngectomy using the daVinci SI SurgicalSystem® (Intuitive Surgical®; Sunnyvale, California, UnitedStates) equipment (Fig. 2). The procedure was uneventful,lasted 158 minutes, had a 50-mL blood loss and the resectionhad clear intraoperative frozen section margins. There wasno need for tracheostomy and the patient was extubated inthe operating room under endoscopic view. Also, the useof a parenteral feeding tube was not necessary, and thepatient received a thickened liquid diet on the second post-operative day, without evidence of aspiration. The lengthof hospital stay was three days. Definitive anatomopatho-logical analysis disclosed a moderately differentiated SCCwithout perineural or angiolymphatic invasion with marginsfree of tumor.
After 24 postoperative days, the patient underwentuneventful selective cervical dissection of levels II, III, andIV bilaterally and histopathological analysis found no metas-tases in 57 dissected lymph nodes; she was discharged within72 hours.
There was no indication for adjuvant treatment, and thepatient remains on outpatient follow-up, with no evidenceof disease, with a normal diet and no voice alterations at 42months of follow-up.
Discussion
Since the first published work by Weinstein in 20073 withthe description of the first three cases, other centers began
lt
u
rms and optical sensor; (B) surgical wound appearance afterupraglottic laryngectomy.
o perform supraglottic laryngectomy using the transoralobotic approach, but the number of reported cases is stillow. The largest series in the literature included 84 surgerieserformed in seven French services.1 The authors demon-trated that the mean time of parenteral tube use wasight days and 24% of patients resumed oral intake 24 hoursfter the procedure. Only 24% of patients required a tra-heostomy, but there was aspiration pneumonia in 23% ofases, including one death for that reason. Postoperativeleeding occurred in 15 patients and 51% of the patientsequired adjuvant radiotherapy due to the anatomopatho-
ogical findings, but there is no description in this study ofhe oncologic outcomes in these patients.Therefore, a systematic review in the Medline databasentil September 2015 (using the key words [‘‘laryngectomy’’

662 Cernea CR et al.
Table 1 Results of the systematic review of published cases of robotic supraglottic partial laryngectomy due to squamous cellcarcinoma.
Study n Age (years) Primary lesion cT cN NeckDissection
Margins
Weinstein20073
3 59 Supraglottic T2 N0 Yes Free59 T2 N0 Yes Free69 T3 N0 Yes Free
Alon 20124 7 72 Supraglottic T2 N1 Yes Free51 T1 N0 Yes Free45 T3 N0 Yes Free57 T2 N0 Yes Free67 T2 N2b Yes Free67 T1 N1 Yes Free71 T2 Yes Free
Ozer 201210 13 58 (mean) EP (100%) 1 T1 11 N0 Yes (all) Free (all)AEF (76.9%) 10 T2 2 N2bVF (23%) 2 T3BT (23%)EP (15.3%)PS (15.3%)
Ansarin20135
10 68 (mean) Supraglottic 2 T1 6 N0 40% Positive in40% ofpatients
6 T2 4 N+2 T3
Lallemant20138
10 64 EP/AEF T2 N2c Yes Free67 EP T2 N1 Yes Free75 EP T1 N0 Yes Free63 EP/AEF T1 N0 Yes Free60 EP/AEF/BT T2 N2b Yes Free50 VF T1 N0 Yes Free59 AEF T1 N0 Yes Positive60 AEF/VF/AT T2 N0 Yes Free67 AT/AEF T2 N0 Yes Free51 AEF/VF T2 N0 Yes Positive
Mendelsohn20139
18 ND Supraglottic 5 T3/4a 6 NDis Free in allcases13 T1/2 12 SL
Park 201311 16 66 (mean) 10 EP 7 T1 9 N0 Yes (No for 2cases of EPT1N0)
Positive in 2cases (12%)4 AEF 5 T2 3 N1
2 VF 4 T3 3 N2b3 N2c
Durmus 20146 1 45 EP/VF T2 N0 Yes ND
Kayhan 20147 13 60 (mean) Supraglottic 4 T1 9 N0 Yes (all) Free in allcases9 T2 3 N2c
1 N3
Perez-Mitchel201412
1 68 VF T2 N0 No Positive
Razafindranaly20151
84 59 (mean) Supraglottic 29 T1 54 N0 67 cases(80%)
Positive in 8cases (9.5%)46 T2 11 N1
9 T3 4 N2a9 N2b5 N2c1 N3

Robotic supraglottic laryngectomy 663
Table 1 (Continued )
Study Perioperativecomplications
TCT (days) ENS/GTM(days)
Hospitallength ofstay (days)
Adjuvanttreatment
Localrecurrence
Weinstein20073
No --- --- 3 --- NDNo --- --- 8 ---No --- --- 5 CT + RT
Alon 20124 No --- --- ND --- NoNo --- 56 --- NoBurning 4 38 --- NoNo 45 45 --- NoNo Dependent GTM RT RT NoNo --- --- --- NoNo --- GTM RT RT No
Ozer 201210 1 conversion to negativemargins
17 (1 case) 40 (1 case) 3.9 (mean) RT (2 casesN+)
No (medianof 6.8months)
Ansarin 20135 None in 10 cases 90% 70% (mean12 days)
13 ± 6 days(mean)
70% (5CT + RT; 1new surgeryfor freemargins; 1RT)
No (medianof 5 months)
Lallemant20138
No 4 5 ND CT+RT NoNo --- 2 years RT NoNo --- 21 --- NoNo --- --- --- NoNo --- 20 CT+RT NoBleeding --- --- --- NoNo --- 2 RT NoNo --- 8 --- NoNo 3 5 --- NoNo 3 4 --- No
Mendelsohn20139
None in 18 cases None 0% GTM(ENS: ND)
11 (median) 10 CT+RT No
Park 201311 None Yes (allcases; mean11.2 days)
Yes (allcases; mean8.3 days)
13.5 (mean) Yes in 8cases (RT 3cases,CT+RT 5cases)
No (mean of20.3months)
Durmus 20146 No --- --- ND --- NDKayhan 20147 2 cases of aspiration
pneumonia1 case Yes (all;
mean 21.3days)
Yes (all;mean 8days)
5 CT + RT (mean of14.1months)
Perez-Mitchel201412
No 3 (OTI) 14 5 --- No (medianof 30months)
Razafindranaly20151
1 conversion 24 cases(24%; mean8 days; 1casedependenton TCT)
64 cases(76%; meanof 8 days; 1case ofpermanentGTM)
15.1 (mean) CT+RT in 43cases (51%)
ND16 cases of bleeding19 cases of aspirationpneumonia1 pharyngocutaneousfistula
---, procedure not performed; AEF, aryepiglottic fold; AT, arytenoid; BT, base of tongue; CT, chemotherapy; ENS, Enteral nutrition support?;E.P, epiglottis; GTM, gastrostomy; NDis, neck dissection; ND, no data; OTI, orotracheal intubation; PS, pyriform sinus; RT, radiotherapy;SL, sentinel lymph node screening; TCT, tracheostomy; VF, ventricular fold; VF, vocal fold

6
aariIicbad
vaipi
C
Tlosr
C
T
R
1
1
64
nd ‘‘robotic surgery’’]) was performed, and it retrieved 11rticles,1,3---12 totaling 176 cases, in addition to the patienteported herein (Table 1). It was observed that most of thencluded patients had tumors at an early stage (stages I andI) and that the surgery was performed with free marginsn most cases, with few complications. The need for tra-heostomy and a parenteral feeding tube was variable, butrief, in most cases. The need for adjuvant therapy was lownd oncologic results showed no cases of local recurrence,emonstrating the safety of the method.
In this case, some aspects are noteworthy and were latererified by other studies summarized here: the patient hadn uneventful postoperative period, in addition to very sat-sfactory oncologic and functional results. The desire torovide the patient’s late follow-up status led to the delayn reporting the present case.
onclusion
his case describes the viability of supraglottic partialaryngectomy by transoral robotic approach, with good post-perative evolution and early rehabilitation. It is therefore aafe method, with very satisfactory oncologic and functionalesults.
onflicts of interest
he authors declare no conflicts of interest.
eferences
1. Razafindranaly V, Lallemant B, Aubry K, Moriniere S, VergezS, De Mones E, et al. Clinical outcomes with transoral roboticsurgery for supraglottic squamous cell carcinoma: experience
1
Cernea CR et al.
of a French evaluation cooperative subgroup of GETTEC. HeadNeck. 2015; Suppl. 24:37---43.
2. Silver CE, Beitler JJ, Shaha AR, Rinaldo A, Ferlito A. Cur-rent trends in initial management of laryngeal cancer: thedeclining use of open surgery. Eur Arch Otorhinolaryngol.2009;266:1333---52.
3. Weinstein GS, O’Malley BW Jr, Snyder W, Hockstein NG. Transo-ral robotic surgery: supraglottic partial laryngectomy. Ann OtolRhinol Laryngol. 2007;116:19---23.
4. Alon EE, Kasperbauer JL, Olsen KD, Moore EJ. Feasibility of tran-soral robotic-assisted supraglottic laryngectomy. Head Neck.2012;34:225---9.
5. Ansarin M, Zorzi S, Massaro MA, Tagliabue M, Proh M, GiuglianoG, et al. Transoral robotic surgery vs transoral laser micro-surgery for resection of supraglottic cancer: a pilot surgery. IntJ Med Robot. 2014;10:107---12.
6. Durmus K, Gokozan HN, Ozer E. Transoral robotic supra-glottic laryngectomy: surgical considerations. Head Neck.2015;37:125---6.
7. Kayhan FT, Kaya KH, Yilmazbayhan ED. Transoral roboticapproach for schwannoma of the larynx. J Craniofac Surg.2011;22:1000---2.
8. Lallemant B, Chambon G, Garrel R, Kacha S, Rupp D, Galy-Bernadoy C, et al. Transoral robotic surgery for the treatmentof T1-T2 carcinoma of the larynx: preliminary study. Laryngo-scope. 2013;123:2485---90.
9. Mendelsohn AH, Remacle M, Van Der Vorst S, Bachy V, LawsonG. Outcomes following transoral robotic surgery: supraglotticlaryngectomy. Laryngoscope. 2013;123:208---14.
0. Ozer E, Alvarez B, Kakarala K, Durmus K, Teknos TN, CarrauRL. Clinical outcomes of transoral robotic supraglottic laryn-gectomy. Head Neck. 2013;35:1158---61.
1. Park YM, Kim WS, Byeon HK, Lee SY, Kim SH. Surgical tech-niques and treatment outcomes of transoral robotic supraglottic
partial laryngectomy. Laryngoscope. 2013;123:670---7.2. Perez-Mitchell C, Acosta JA, Ferrer-Torres LE. Robotic-assisted salvage supraglottic laryngectomy. P R Health Sci J.2014;33:88---90.