Embed Size (px)
Citation preview

C H A P T E R
14
Bone Marrow Fat and Bone MassMasanobu Kawai 1, Clifford J. Rosen 2
1Osaka Medical Center and Research Institute for Maternal and Child Health, Osaka, Japan2Maine Medical Center Research Institute, Scarborough, ME, USA
INTRODUCTION
For a century adipocytes have been noted in the bonemarrow of mammals. And although fat cells have beenconsidered an integral part of the bone marrow micro-environment, few believed these cells were physiologi-cally active. However, the developmental, mechanical,and physiological components of adipogenesis withinthe trabecular niche have recently become the focus ofinvestigation by several groups. Coincident with thatattention, significant progress has been made in under-standing the differentiation programs of osteoblastsand adipocytes, as well as their common ancestor, themesenchymal stem cell. This review will center on ourcurrent knowledge of the interaction between marrowfat and the skeleton. We will focus on mouse and humanmodels, although our conclusions may extend to othervertebrates.
HISTORICAL VIGNETTE
Marrow adipocytes were recognized in pathologichuman specimens as early as the 19th century as “largecells in the bone marrow,” although their function wasunknown. Neumann was the first to describe fromautopsy samples that red marrow was replaced bymarrow giant cells in the peripheral skeleton with ageand then advanced the theorem that with advancingage, hematopoietic elements within the marrow arereplaced by large yellow cells. Subsequently, from anal-yses of patients with arsenic toxicity, marrow “giant”cells were shown to have unique characteristics thatresembled fat globules. In line with these observations,marrow adipocytes were recognized as a constant andunique feature of bone marrow aspirates and biopsies,and numerous studies identified the absence of marrowfat in some hematopoietic disorders or enhanced
167Translational Endocrinology of Bone
DOI: http://dx.doi.org/10.1016/B978-0-12-415784-2.00014-2
marrow adiposity in aplastic anemia due to chemicalsor radiation. In 1936 Huggins and Blocksom reportedthat tail vertebrae from rodents were laden with marrowfat in contrast to more anterior vertebrae [1]. In 1971,Meunier et al. first reported that osteoporotic elderlywomen had abundant marrow fat, which was directlyrelated to age and negatively correlated with trabecularbone volume [2]. Several reports followed whichdemonstrated that the increase in marrow adipositywas age dependent, but with gender, ethnic, and agevariation. By the 1990s, MRI emerged as a means toimage and quantitate marrow fat by spectroscopy [3].Phenotyping mice for marrow adiposity has advancedrecently with the use of high-field MRI and mCT withosmium staining. Future technological advances suchas MRI with PET scanning promise to further definefunctional aspects of marrow adiposity.
MOLECULAR AND CELLULAR ASPECTSOF MARROW ADIPOGENESIS
Transcriptional Control of Adipogenesis
Adipogenesis is a complex and integrated process inwhich several transcription factors come into play ina context-specific manner [4e6]. The molecular andcellular mechanisms of adipocyte differentiation havebeen widely and extensively studied using in vitroand in vivo models. The initial step of adipogenesis isthe lineage commitment of mesenchymal stem cells(MSCs) into preadipocytes. This occurs in the stromalvascular fraction of adipose depots and in the bonemarrow. Following the expansion of preadipocytes,MSCs differentiate into mature adipocytes under thetight control of multiple transcription factors includingC/EBPb/d and PPARg. Among these, PPARg, a nuclearreceptor and transcription factor, plays a central role in
� 2013 Elsevier Inc. All rights reserved.

14. BONE MARROW FAT AND BONE MASS168
adipogenesis as evidenced by the fact that the loss ofPparg in mouse embryonic fibroblasts leads toa complete absence of adipogenic capacity [7]. In vitro,multiple transcription factors and co-regulators havebeen implicated as modulators of the expression andfunction of PPARg. For example, differentiation of3T3-L1 cells, a well-recognized cell line that is used torecapitulate adipogenesis in vitro, is regulated by theintegration of several transcription factors includingthe C/EBP family, C/EBPb and d. These factors stimu-late Pparg transcription by directly binding to thepromoter region [8]. Increased expression of Pparg acti-vates the expression of another member of the C/EBPfamily, C/EBPa, which in turn enhances the expressionof PPARg. Partial loss of function of C/EBPa results ina mouse (A-Zip) with very little adipose tissueincluding virtually none in the bone marrow. Thus,the C/EBP family is critical for the induction of PPARgin vitro. However, in vivo adipogenesis is much morecomplex and requires other transcriptional and co-factors for PPARg regulation in part because PPARgexpression is maintained in adipose tissue of micelacking C/EBPb and/or d [9].
The Central Role of Peroxisome Proliferator-activated Receptor-gamma (PPARg)
Peroxisome proliferator-activated receptor-gamma(PPARg) is a member of the PPAR family of transcrip-tional factors, which has multiple roles not only in cellfate determination, but in lipid biosynthesis, mitochon-drial biogenesis, inflammation, neoplastic growth, andinsulin sensitivity [10,11]. PPARg is composed of fourvariants including PPARg1 and 2, the two major formsof PPARg protein, which are produced by differentialusage of promoters and alternative splicing. PPARg1 iswidely expressed in many tissues including the liver,skeletal muscle, adipose tissue, and bone, while expres-sion of PPARg2, which possesses 30 additional aminoacids in its N-terminus compared to PPARg1, isrestricted to adipogenic cells. Importantly, several linesof evidence demonstrate the existence of PPARg2 inmarrow stromal cells prior to their differentiation intoadipocytes [10,12,13]. PPARg dimerizes with the retinoicX receptor (RXR) alpha, and activates transcription oftarget genes, although a number of transcription factorsand co-activators are also involved in the regulation ofPparg expression and function. As described earlier,the C/EBP family, C/EBPa, b, and d, plays a pivotalrole in adipogenesis in cooperation with PPARg. PPARgexpression and function are also regulated by othertranscription factors during adipogenesis includingSrebp-1c, KLF5, KLF15, Zfp423, and early B cell factor(Ebf1), while KLF-2 and GATA2/3 negatively regulatesPPARg expression [4,14e18].
Naturally occurring substances such as fatty acidsand metabolites of arachidonic acids are potentialin vivo candidates for PPARg liagnds [19,20].15-Deoxy-D12,14-prostaglandin J2 (15d-PGJ2) is onesuch endogenous PPARg ligand which is derived fromarachidonic acid, although it still remains to be clarifiedwhether 15d-PGJ2 is functional in terms of activatingPPARg in vivo [21,22]. In addition to these, a syntheticclass of compounds, the thiazolidinediones (TZDs), arepotent exogenous ligands for PPARg and have beenwidely used in the treatment of diabetes [23e27].
PPARg transcriptional activity is regulated by histonemodification as well as ligand availability. In the absenceof ligands, co-repressors such as NCoR and SMRT aswell as histone deacetylases (HDAC) are recruited tothe protein complex of PPARg, thereby forcing PPARgto be transcriptionally silent [28]. In contrast, whenligands are available, these proteins are dissociatedfrom PPARg protein complex machinery and co-activa-tors such as CBP and histone acetyltransferase (HAT)are recruited. Another level of regulation is created bythe histone methylation by histone methyltransferase.Non-canonical Wnt pathways activated by Wnt5a havebeen shown to suppress PPARg transcriptional activa-tion through the histone methyltransferase, SETDB1(SET domain bifurcated 1) [29].
Posttranscriptional modifications of PPARg are alsoimportant components in regulating PPARg activity.PPARg2 has been shown to be phosphorylated at serine112 by secretory factors including EGF and PDGF, result-ing in the impairment of PPARg2 transcriptional activity[30e32]. On the other hand, phosphorylation at serine273 by Cdk5 enhances adipogenesis and has been linkedto greater fat deposition and suppression of adiponectin[33,34]. Agents that block Cdk5 phosphorylationincluding rosiglitazone have been demonstrated toenhance insulin sensitivity through this mechanism.Newer compounds that block Cdk5 phosphorylationbut do not have transcriptional activity have recentlybeen described as pure insulin sensitizers [33,34]. Inaddition to phosphorylation, sumoylation and ubiquiti-nation confer a different level of posttranscriptionalPPARg regulation [35e37]. In sum the importance ofthis nuclear receptor and transcriptional factor forcellular metabolic fate cannot be overstated. Hence thereare multiple layers of regulatory control over PPARgactivity.
PPARg and the Skeleton
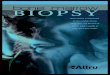
Osteoblasts and adipocytes share a commonprecursor (i.e. the mesenchymal stem cell, MSC), whichalso serves as a source of progenitors for marrowfibroblasts, chondrocytes, and supporting stromafor hematopoietic cells [38e40] (Fig. 14.1). Lineage

RANKL
PPARgamma
OPG
Mesenchymal stem cells
HSCs
Pre-adipocytesPre-osteoblasts
AdipocytesOsteoblasts
C/EBPsRunx2Osterix
Osteoclasts
FIGURE 14.1 PPARg regulates the cell fate decision of mesen-
chymal stem cells (MSCs) toward the adipogenic or osteogenic
lineage. The role of PPARg in osteoclast differentiation is stillcontroversial and needs to be clarified. Marrow adipocytes producea number of secretory factors and PPARg regulates the expression ofthese genes. PPARg: peroxisome proliferator-activated receptor-gamma. C/EBP: CCAAT enhancer binding protein. Runx2: runt-related transcription factor 2. Msx2: muscle segment homeoboxhomologue of 2. Please see color plate section.
DEVELOPMENT OF MARROW FAT 169
allocation of marrow MSCs towards either adipocytesor osteoblasts is a finely tuned event in which lineage-specific transcription factors (such as Runx2 andOsterix for osteoblasts and PPARg2 for adipocytes)play critical roles. Importantly, in some but not all situ-ations lineage allocation of MSCs towards either ofthese cell types is considered to be mutually exclusive;i.e. activation of PPARg leads to enhanced adipogenesisat the expense of osteoblastogenesis and is associatedwith reduced expression and function of osteogenictranscription factors such as Dlx5, Msx2, Runx2, andOsterix [41e44]. In line with this, suppression ofPPARg is reported to stimulate osteoblastogenesisand represses adipogenesis [45]. These observationsare also consistent with the findings of aged micemodels where marrow adiposity is increased andbone mass is reduced, associated with enhancedPPARg2 expression [46]. Similarly, haploinsufficiencyor a hypomorphic mutation of Pparg has been reportedto have increased bone mass and reduced marrowadiposity associated with increased osteoblast numberand bone formation [47,48]. In addition to the pivotalrole of PPARg in lineage allocation of MSCs, mountingevidence indicates the involvement of PPARg in osteo-clast differentiation as well. For example, PPARg acti-vation has been shown to activate bone resorption inpart through enhancing osteoclast differentiation byrecruitment of another co-activator of PPARg,PGC-1beta [49e52]. Furthermore, the effect of PPARgactivation on osteoclastogenesis could be in partmediated by the increased expression of Rankl in an
age-dependent manner [53]; however, the exact role ofPPARg in osteoclastogenesis is still controversial andneeds to be determined [54,55]. Additionally, werecently observed that conditional deletion of PPARgin differentiated adipocytes using the aP2 promoterresulted in lipodystrophy by 26 weeks accompaniedby high bone mass (Rosen CJ, personal observation).Interestingly, these mice exhibit increased osteoclastactivity suggesting that the phenotypic effects ofPPARg are highly context specific with temporal effectsfrom PPARg deletion varying with the timing ofinactivation.
DEVELOPMENT OF MARROW FAT
Marrow adipogenesis has recently gained attentionamong researchers because of its possible role asa modulator of physiological and pathological condi-tions. Marrow adipocytes have long been thought toresult from a default pathway for MSCs during differ-entiation. In support of that tenet, the compositionalratio in bone marrow adipocytes relative to hematopoi-etic element changes with age. For example, in neonatalmammals, adipocytes are all but absent in the bonemarrow and hematopoietic cells primarily occupy themarrow cavity at this stage. During pubertal growth,there is gradual but significant infiltration of marrowfrom the long bones with adipocytes. However, withadvancing age, the number of adipocytes in the bonemarrow increases dramatically, resulting in the appear-ance of fatty marrow. In humans, most of the femoralcavity is occupied by fat in the third decade of life,whereas in the vertebrae this does not occur until the7th or 8th decade. Importantly, these age-relatedchanges in marrow adiposity are associated with boneloss, although this does not necessarily imply causeand effect. On the other hand, marrow adipocytes arefound in abundance in states such as aplastic ormyelophthisic diseases, suggesting that adipogenesiscould either be inhibitory to hematopoiesis or mightoccupy the marrow space in lieu of hematopoieticelements [56].
The process of marrow adipogenesis is likely gov-erned by the same transcriptional cascades as observedin white adipocyte differentiation and hence PPARg iscertain to play a pivotal role. Streptozoticin-inducedtype 1 diabetic model mice exhibit massive develop-ment of marrow adiposity, which is antagonized bythe treatment with the PPARg inhibitor bisphenolA diglycidyl ether (BADGE) [57]. In the same vein,BADGE also suppresses the marrow adipogenesisfollowing irradiation in mice [56]. Treatment withTZDs affects bone mass and marrow adiposity, furthersubstantiating a role for PPARg in marrow fat

14. BONE MARROW FAT AND BONE MASS170
generation. These lines of evidence indicate that devel-opment of marrow adiposity is age specific and activa-tion of PPARg is likely central to the development ofmarrow adipocytes.
THE FUNCTION OF MARROW FAT
Some studies have suggested that marrow adipo-cytes, under most physiologically conditions, are meta-bolically inert. This process is often thought of asa default mechanism whereby MSCs enter the fatlineage because of their inability to differentiate intomore complex cells such as osteoblasts or chondrocytes.Although this hypothesis can be considered tenable inlight of several studies showing an inverse relationshipbetween marrow fat and bone volume, there are mousemodels to suggest this may not always be operative.Other studies suggest that marrow adipocytes may beself-promotive such that existing marrow adipocytescan induce differentiation of more MSCs into adipo-cytes, thereby preventing lineage allocation into othercell types [10,11]. Finally, we and others have shownthat mouse adipocytes from certain depots can suppressosteoblastogenesis when co-cultured with bone marrowstromal cells, suggesting that these cells could be meta-bolically active and inhibit osteoblastogenesis throughparacrine secretory factors (Rosen CJ, unpublishedobservation).
Marrow adipocyte infiltration is often associatedwith bone loss, but there is also evidence of a positivecorrelation between marrow adiposity and bone massin human and animal models. For example, C3H/HeJmouse exhibits high bone mass associated withincreased marrow adiposity compared to C57BL/6Jbackground [58]. In humans, marrow adiposityrobustly increases during puberty when skeletal acqui-sition is maximized [59]. These indirect lines ofevidence suggest that in physiological situationsmarrow adipocytes have a distinctly different rolefrom adipocytes found in pathogenic conditions. Inthat same vein, leptin expression in the bone marrowincreases at the time of puberty in mice when maximalbone mass is acquired and decreases with age, indi-cating that leptin could be one possible factor producedby marrow adipocytes that influences skeletal accrual(Rosen CJ, unpublished observation). In addition,mice with a global deletion of Ebf1 (an early B cell tran-scription factor) demonstrate a substantial increase inmarrow adiposity that is accompanied by an increasein osteoblasts [60], suggesting that this nuclear factormay have a role in enhancing lineage allocationbetween adipocytes and osteoblasts. Thus, marrowadipocytes may be an important component of thebone marrow niche and establish a favorable skeletal
micro-environment for osteoblast differentiation. Thiscould occur through the secretion of paracrine factorsor by release of free fatty acids that might be utilizedby osteoblasts.
Adipocytes in the bone marrow have been thoughtto be inhibitors of active hematopoiesis althoughfurther studies are required at different skeletal sites[56]. Interestingly, the appearance of adipogenesis inthe femoral bone marrow after transplantation or injurymay serve not as a true antagonist for hematopoiesisbut rather as a “place-holder” to maintain hematopoi-etic progenitors in a stem cell state awaiting signalsthat permit entrance of those cells into their differenti-ation scheme. Alternatively, marrow adipogenesismay serve as a functional reservoir to re-establish theniche. For example, in C57BL6 mice that are lethallyirradiated and then undergo marrow transplantation,the bone cavity fills with adipocytes between days5 and 10 but those cells subsequently disappear 3 weeksafter marrow transplantation. Moreover, in 1936 Hug-gins and Blocksom reported that when tail vertebraethat contain virtually all marrow fat and no red marroware implanted into the peritoneal cavity there wasa conversion of marrow adipocytes to hematopoieticmarrow suggesting that temperature plays a key rolein the switch from red to yellow marrow [1]. Indeed,this observation is very consistent with the distributionof marrow adipocytes in different skeletal sites withenhanced marrow adiposity noted in the extremitieswhere the ambient temperature is lower than withinthe body cavity. Currently, the optimal temperaturefor hematopoiesis and osteogenesis within the marrowis not known.
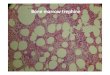
Interestingly, expression analysis reveals the exis-tence of genes involved in thermogenesis and lipidmetabolism in marrow adipocytes, suggesting thatmarrow adipocytes could be metabolically active [61](Rosen CJ, unpublished observation). In line with this,marrow adipocytes isolated from rabbit long bonesare more responsive (i.e. increases in glycerol and fattyacid release) to external stimuli such as beta adrenergicand cyclic AMP analogs than adipocytes from gonadalor intra-abdominal depots (Rosen CJ, unpublishedobservation). Furthermore, comparative studies of fattyacid depots in the marrow, interscapular brownadipose tissue (BAT) and mesenteric sites using NMRspectroscopy reveal a saturated: unsaturated fattyacid ratio in the marrow identical to that seen in BAT.Similarly, mice treated with rosiglitazone haveenhanced marrow adiposity that has spectroscopiccharacteristics identical to BAT. These observationsindicate that marrow adipocytes may represent a meta-bolic tissue involved in the maintenance of the marrowmicro-environment although further studies areneeded (Fig. 14.2).

PathologicalPhysiological
PubertyC3H/HeJ mice vsC57BL/6 mice etc.
Carorie restrictionAnorexia NervosalipodystrophyGH deficiencyAging, diabetes etc.
Positive association
with bone mass
Positive secretory factors :IGF-I, Leptin etc.
Negative secretory factors:Inflammatory cytokinesFree fatty acids etc.
Marrow adipocytes
Osteoblasts
Negative association
with bone mass
# Metabolic characteristics:Responsiveness to external stimuli
# Brown adipocyte-like phenotype :Expression of Ucp1
FIGURE 14.2 Marrow adipocytes produce a number of secretory
factors. Such factors could have a significant role in osteoblastdifferentiation and/or function. In pathogenic conditions, thesedeterminants could impact osteoblasts in a negative direction,whereas in physiological conditions these factors may have a differentrole from the one observed in the pathogenic conditions. There is alsoevidence that marrow fat is metabolically active and that genes whichare characteristics to brown adipocytes are expressed in marrowadipocytes. Please see color plate section.
MOUSE MODELS TO STUDY MARROW ADIPOCYTES 171
MOUSE MODELS TO STUDYMARROW ADIPOCYTES
Insulin Resistance Models
Clinical evidence demonstrates that type I diabetes isa significant risk factor for low bone mass and theincreased incidence of fractures although the underlyingmechanisms are not fully understood [62,63]. To under-stand the pathogenesis of low bone mass in diabeticpatients, some animal models have been introducedand these have shown that accompanying insulin defi-ciency profoundly increases marrow adiposity. The twomost commons strains are the spontaneous diabeticNOD mouse and C57BL6 mice in which diabetes isinduced by streptozotocin [64,65]. In both of thesemodels of type I diabetes, pro-adipocytic genes such asPPARg and aP2 (FABP4) were found to be increased inlong bones and this was correlated with decreasedexpression of osteocalcin [64,65]. Importantly, treatmentwith BADGE, a PPARg antagonist, decreased themarrow adiposity observed in streptozotocin-induceddiabetic models although skeletal loss was not reversedby the BADGE treatment. Thus, it is still unclear whethermarrow adipocyte infiltration in diabetic patients playsa central role to the development of bone loss.
TZD-induced Mouse Models
Activation of PPARg is associated with increasedmarrow adiposity as well as bone loss in rodent modelsalthough the effect of PPARg agonists on increased
marrow adiposity is strain and drug specific [66].Troglitazone has been shown to increase marrowadiposity in the Apoe�/� strain, but no changes inbone mass were observed [67]. Darglitazone is 20 timesmore potent than rosiglitazone and 150 times morepotent than pioglitazone [68]. A dose of darglitazone,10mg/kg/day, to 8-month-old male mice resulted ina profound decrease in both trabecular and corticalbone [49], but the effect of this TZD onmarrow adipositywas not reported. Netoglitazone, a relatively weak TZD,was found to decrease whole body bone mineral content(BMC), but did not affect trabecular bone volume orwhole body areal BMD in C57BL/6 mice, but this TZDalso increasedmarrow adiposity [69]. Importantly, agingis a key factor determining susceptibility to TZD-induced bone loss because PPARg has been shown tobe activated with aging in the bone marrow. Consistentwith these findings, rosiglitazone-induced bone loss ismuch more pronounced in older female C57BL/6Jmice, and is associated with significant infiltration ofthe marrow with large adipocytes. Histomorphometricindices in these mice reveal a marked suppression inbone formation and increases in bone resorption consis-tent with a profound imbalance in bone remodeling. Notsurprisingly, this effect is strain specific, such that somemice show only increased marrow adipogenesis but nobone loss (e.g. C3H/HeJ), while others display no skel-etal or marrow effects from rosiglitazone [66].
Calorie Restriction
Not surprisingly, nutritional status is a pivotal factorregulating the number of marrow adipocytes. Contraryto peripheral fat depots, i.e. subcutaneous and abdom-inal fat depots, a diet containing excess amounts of fattyacid is not a strong inducer of marrow adipocytes. Onthe other hand, there is evidence that calorie restrictionin young animals induces adipocytes in the bonemarrow accompanied by decreased bone mass [70].This effect appears to be time dependent as older miceon a 30% calorie restriction diet show enhanced bonemass but no evidence of increased marrow adiposity.In line with the findings observed in mouse models,patients with anorexia nervosa exhibit a massive infiltra-tion of adipocytes in bone marrow despite minimalsubcutaneous or peripheral fat, and a concomitantdecrease in bone mass [71,72]. The remodeling changesare remarkable and include a reduction in bone forma-tion and an increase in bone resorption. Induction ofPPARg could be in part responsible for the developmentof marrow adiposity, but the mechanism of how calorierestriction triggers the development of marrow adipo-cytes still remain to be elucidated. One possibility isthat there is a systemic signal, either released centrallyor locally, that triggers a hormonal response to induce

14. BONE MARROW FAT AND BONE MASS172
marrow adipogenesis. One such candidate is theorixogenic hormone ghrelin which has also been shownto induce marrow adipogenesis in experimentalanimals [73].
Leptin-deficient Model
Leptin is a secretory factor produced by adipocytesthat regulates body composition, fertility, appetite, andbone and energy metabolism. In addition, emergingevidence indicates the critical role of leptin in skeletalmetabolism by relaying an adipokine signal at the hypo-thalamus [74e76]. The ob/ob (obese) strain of mice, firstdescribed in 1950 by Ingalls et al., carries a spontaneousnon-sense mutation at codon 105 of the leptin gene thatresults in a complete loss of leptin protein [77,78]. As thename of this strain suggests, these mice are extremelyobese: exhibiting profound hyperphagy, glucose intoler-ance, and hyperinsulinemia [78,79]. In the femur, ob/obmice have increased marrow adipocytes and peripheraladministration of leptin corrects the marrow adiposityphenotype seen in the femur of these mice [80e84].Both long bones and axial skeleton of ob/ob mice showvery high bone mass, despite absence of gonadalsteroids and this is associated with decreased marrowadiposity [75,76,80], establishing the inverse relation-ship between marrow adiposity and bone mass ina compartment-specific manner.
TABLE 14.1 Marrow Adiposity among Different Strains of Mice
IRS-1-deficient Mice
Insulin is a key factor in adipogenesis and fat storage.The IRKO mouse, which has global absence of theinsulin receptor but in which expression of IR has beenrestored in pancreas, liver, and brain, but not muscleor fat, has extremely low numbers of marrow adipo-cytes, with normal trabecular BMD [64]. Similarly, wenoted that in a spontaneous mutant, small, which hasa homozygous recessive mutation in the intact IRS-1molecule, there is a virtual absence of marrow fatdespite very low bone mass during neonatal and adultlife. As noted previously, bone loss, diabetes, andmarrow adiposity have been described in several othermouse models all of which show reduced osteocalcinexpression [65,85]. Furthermore, as was noted in ob/obmice, the increase in marrow adipocytes appears limitedto the calvaria and long bones and not the vertebrae [64].
Strain Number of adipocytes/high-power field
C57BL/6J 31 þ/� 4.8
C3H/HeJ 17.8 þ/� 7.2
A/J 14 þ/� 4.6
DBA/2J 30.6 þ/� 9.9
Adapted from Rosen CJ et al. Crit Rev Eukaryot Gene Expr. 2009;19(2):109e24.
Growth Hormone Deficiency
Growth hormone (GH) is produced and secretedfrom somatotrophs in the anterior pituitary and regu-lates linear growth, body composition, and lipid andglucose metabolism both in an IGF-I dependent andindependent manner. GH is well known to induce
lipolysis in adipose tissue and patients with GH defi-ciency have been shown to acquire more fat than normalcontrols, leading to the development of obesity-relatedmetabolic complications. In bone, GH has been shownto have both direct effects on long bone growth andindirect effects via IGF-I. The dw/dwmutation is a spon-taneous mutation that arose in the Lewis strain of rat.These rats are dwarfs as a result of GH deficiency, andhave a profound increase in both adipocyte numberand adipocyte size in the marrow of the long bones,compared to wild-type controls [86]. Treatment withGH results in a decrease in adipocyte number, whereastreatment with IGF-I results in a decrease in adipocytevolume [87]. Recently, Turner and colleagues demon-strated that acute pituitary insufficiency due to hypoph-ysectomy resulted in significant marrow adiposity thatcan be reversed by GH, but not by IGF-I, estrogen, orcortisol [88]. Interestingly, LID mice, in which hepaticIGF-I is deleted, have very high GH levels andlow IGF-I, but do not have marrow adiposity. On theother hand, little mice with a spontaneous mutation ofthe growth hormone releasing hormone receptorhave significant marrow fat [88]. Thus, abnormalitiesin the GHeIGF-I axis are associated with marrowadipogenesis.
Inbred Strains
Inbred strains of mice are powerful tools for use in thestudy of the genetics of complex disease, since eachmouse of a given strain represents essentially an iden-tical twin of all other mice in that strain. As a result,phenotypic measures such as bone mineral density(BMD) or serum HDL levels remain relatively constantwithin a strain, but may vary greatly between strains(see http://www.jax.org/phenome). In a pilot study ofmarrow adipocyte numbers in the distal femur (immedi-ately proximal to the growth plate) of four inbred strainsof mice, we found that the number of marrow adipo-cytes per unit area varied greatly between strains(Table 14.1). Interestingly, BV/TV% was only found tobe significantly correlated with marrow adipocytenumber for the DBA/2J mice (R¼ 0.78, p¼ 0.04). More-over, vBMD of the femur (which is principally a cortical

MARROW FAT IN HUMANS 173
bone phenotype) did not correlate with marrowadipocyte number for any of the strains suggestingthat the relationship between bone mass and marrowadiposity is not a simple inverse correlation.
Aging
In rodents and humans, aging is associated witha significant increase in marrow adiposity. C57BL6 isthe most frequent strain studied, and in both malesand females, mice older than 20 months accumulatemarrow adipocytes in the distal femur and proximaltibia but not in the lumbar vertebrae. As noted this isassociated with the age-related decline in trabecularbone mass but not with cortical bone density. Ovariec-tomy, a model of accelerated aging, also enhancesadipocyte infiltration in the bone marrow and this isgreater in older retired breeders than younger mice.
MARROW FAT IN HUMANS
Physiology
The physiologic role of adipocytes in human bonemarrow is largely unknown. Marrow fat had longbeen regarded as “a filler” for space vacated by trabec-ular bone loss, which is often seen in aged people andpatients with osteoporosis [89e92]. However, with anextensive revision of our understanding of fat tissue asan endocrine organ, a novel concept that marrow adipo-cytes possess similar metabolic characteristics as someperipheral or brown fat depots has emerged. Moreover,the juxtaposition of adipose tissue within the bonemarrow milieu suggests that its presence may haveconsequences for the skeleton. Two theories are mostprevalent as to the consequences of marrow adiposity.First, since the total bone marrow cavity is sharedamong adipose, bone, and hematopoietic tissues, fatoverload would displace functional hematopoieticand/or osteogenic cells from the marrow cavity [93],therefore making it a negative determinant of bonemass. Second, a balanced bone marrow microenviron-ment including marrow adipocytes is essential fornormal hematopoiesis and osteogenesis because of theirstrong energy needs [40,94]. Indeed, increased produc-tion of fat-related factors, such as fatty acids, couldpositively or negatively affect metabolism in the bonemarrow depending on the nature of the fatty acidand the type of receptor activation such as the GPR120 receptor on MSCs [95]. In addition, adipokines,steroids, and cytokines [96e98] can exert profoundeffects on neighboring marrow cells, sustaining hemato-poietic and osteogenic processes [90,92,97,98]. Finally, ifadipocytes generate heat as brown-like cells, this could
theoretically enhance or depress bone remodeling[61,99]. These possibilities require further testing butsupport the thesis that marrow adipocytes are a criticalcomponent of the bone marrow niche and influencethe establishment of bone marrow environment.
Developmental of Marrow Fat in Humans
As described above, in newborns there is no marrowfat at any skeletal site; however, adipocyte numberincreases with age such that for individuals older than30 years of age, most of the femoral cavity is occupiedby adipose tissue. Indeed, recent studies have shownthat in the appendicular skeleton of adults more than70% of the marrow space is occupied by fat. This age-related increase in marrow adiposity is known to beassociated with age-related bone loss and BMD,establishing the widely accepted tenet of the inverse cor-relationship between these two parameters. Thisconcept is largely true especially in the case of patho-logic conditions including osteoporosis, drug use, andmalnutrition. However, in physiological conditions thislong-standing tenet may not be true. For example, theconversion from red to “yellow” marrow occurs aroundthe time of peak bone acquisition, supporting thealternative hypothesis that marrow adipocytes createa favorable skeletal microenvironment for osteoblasto-genesis, thereby maximizing bone accrual duringpuberty.
The development of marrow adipocytes is affected bythe nutritional status. Despite the similarities in terms ofsets of transcriptional machinery used in the develop-ment of marrow adipocytes as noted in white adipocytedevelopment, the trigger for marrow adipocyte forma-tion could be different from white adipose tissue.In fact, marrow adipocyte infiltration is often observedin the clinical conditions called “fat redistribution,” inwhich marrow fat infiltration is associated witha decrease in peripheral adipose depot. For example,HIV-related lipodystrophy causes a significant decreasein peripheral adipose tissue whereas marrow adiposityis enhanced. In that same vein, states of malnutritionincluding anorexia nervosa lead to an increase inmarrow adiposity while there is concurrent peripheralloss of adipose depots. Importantly, overnutrition isnot a contributor to the development of marrowadiposity, suggesting that amount of peripheral fatdepots is not correlated with marrow adiposity. In fact,in a recent work by Gilsanz and colleagues, adolescentsand young adults had significant marrow adiposity inthe appendicular skeleton, but this was not related tosubcutaneous or visceral fat depots, nor with markersof cardiovascular risk [100]. However, this tenet has tobe clarified and might be compartment specific becausethere is also evidence of a positive correlation between

14. BONE MARROW FAT AND BONE MASS174
vertebral marrow adiposity and visceral fat mass insome scenarios [101].
The issue of whether fat is detrimental or agonistic toskeletal remodeling is not easily resolvable. Currentmethods including MRI with and without spectroscopy,CT, and histology do not provide functional informationabout the type of adipocyte and its role in the marrow.Recent work by Li et al. demonstrated that individualswith fractures, whether they were diabetic or not, hadincreased saturated fat relative to unsaturated fat,a pattern also seen in brown adipose tissue (see ASBMRAbstract FR0049 Patsch, 2011). These data plus evidencein experimental animals that brown-like adipogenicgenes are expressed in the marrow of older animals rai-ses the intriguing possibility that there is a dynamicaround marrow adiposity such that white adipocytescould become “brown-like” under the influence ofneurogenic, endocrine, or paracrine factors.
Clinical Implications
Aging
Age-related bone loss occurs universally in allmammals and unlike postmenopausal bone loss affectsindividuals regardless of sex steroid status. Becausemaintenance of bone homeostasis relies on the balanceof bone remodeling, any factors which disturb this crit-ical balance will lead to bone loss. The characteristicfeature of age-related bone loss is the uncoupling offormation from resorption leading to a net loss of bonemass. The etiology of this uncoupling is multi-factorialand includes changes in endogenous gonadal steroids,increased reactive oxygen species, and a global declinein local growth factors that promote osteoblastic differ-entiation [2,102,103]. In addition, aging is also relatedto the alteration in lineage commitment of MSCs. Forinstance, it has been observed in humans that thenumber of MSCs committed to the adipocytic lineageincreases with age, while those committed to the osteo-blastic lineage decrease. There is increasing evidenceof lineage allocation of MSC fate away from osteoblastswith aging and towards pre-adipocytes. This couldresult from increased activity of PPARg2, orthe decreased expression of the TGF-b/BMP, Wnt/b-catenin, and IGF-I signaling pathways [46]. Thesechanges could easily lead to reduced osteoblast differen-tiation, while the formation of new adipocytes isenhanced. In addition, an increase in marrow adipocyteswould result in greater secretory factors which could bedeleterious to bone formation, establishing a viciousloop which would accelerate bone loss. In addition tothe alteration in cell fate determination, phenotypicchanges of MSCs during the aging process could alsobe responsible for age-related bone loss. For example,impairment of cell proliferation and differentiation, as
well as chromosomal instabilities of MSCs, has beenimplicated in long-term cell culture models [104].
It has been reported that an increase in marrowadiposity is characterized not only by greater numbersof marrow adipocytes but also an increase in their size[93]. In a cross-sectional study of post-mortem iliac crestbiopsies adipose tissue volume increased from 15 to 60%between 20 and 65 years old, while trabecular bonevolume decreased from 26 to 16% [2]. More recently,Justesen et al. found that marrow adipose tissueincreased from 40% at age 30 to 68% at 100 years old,while bone volume decreased to 12% [105]. Finally, inosteopenic bone it was observed that, in addition tothe age-related inverse correlation between adiposeand bone tissues, the hematopoietic tissue was replacedby fat [106]. Other conditions such as osteoporosis[2,105], immobilization [92,107,108], microgravity [109],ovariectomy [110], diabetes [111], or glucocorticoidtreatment [112] also show an increase in the content ofmarrow adipose tissue and decreased bone volume.
TZDs
In the context of PPARg activity, treatment of rodentsor humans with rosiglitazone causes bone loss andstructural fragility, in part due to impaired bone forma-tion [113]. This phenotype resembles the process ofaging in mammalian bone, which is also characterizedby significant marrow adiposity, reduced trabecularbone volume fraction and increased bone resorption.Postmenopausal females tend to be the most sensitiveto the bone loss by the thiazolidinediones [113]. In onereport, older women lost more than 2% of their bonedensity after only 14 weeks of rosiglitazone treatment[113]. In several large randomized trials of rosiglitazoneand pioglitazone, peripheral fractures were reported tobe twice as likely in diabetic women treated witha TZD compared to those administered metformin,insulin, or sulfonylureas [114]. It still needs to be clari-fied whether TZDs can induce marrow adiposity inhuman populations as observed in rodent models,although in one prospective human study bone losscaused by TZDs is not associated with marrow fat infil-tration [115]. Thus, it still remains unclear whethermarrow adiposity occurs in humans as it does in miceafter exposure to TZDs. However, biochemical markersof bone turnover in patients on TZDs reveal uncouplingwith enhanced bone resorption and suppressed boneformation that are consistent with experimental findingsin mice. Furthermore, the predisposition of postmeno-pausal women to the skeletal effects of TZDs suggestthat an altered bone remodeling state due to greaterrates of resorption than formation enhances the suscep-tibility to TZD-induced bone loss. Interestingly, theskeletal sites most frequently reported to fracture indiabetics are those that are predominantly cortical in

FUTURE DIRECTION 175
nature rather than trabecular [114]. This would implythat drug-induced changes in metabolic factors such asadipokines may play a systemic role in TZD-inducedbone loss, independent of changes in the trabecularcompartment that is more directly related to enhancedmarrow adiposity.
Other Clinical Scenarios
Thirty-five years ago Meunier reported that osteopo-rotic women had more marrow fat than controls [2].Nearly a quarter of a century ago, Klibanski andcolleagues noted an enhanced marrow fat signal inanorexic women who were osteoporotic (Klibanski,personal communication). Abella reported that onbone marrow biopsy, anorexia nervosa was associatedwith significant marrow adiposity [116]. Subsequently,Wehlri and colleagues noted by MRI that marrow fatin the vertebrae was inversely associated with bonemass [117]. Yeung et al. and Griffith et al. reporteda similar negative correlation between marrow fat byspectroscopy and areal bone mass [3,118]. And veryrecently, this group reported that marrow adipositywas associated with reduced vascularity in the femoralhead [119]. Hence, emerging evidence suggests that inhuman conditions, marrow fat may invade spaces previ-ously occupied by trabecular bone. However, we do notknow whether this is a primary or secondary event, orwhether struggling osteoblasts require adjacent adipo-cytes for energy. Clinical scenarios provide some cluesas to marrow fat function relative to bone.
Osteoporosis
Those who are suffering from osteoporosis, whetherof primary or secondary origin, have more marrowadipocytes than age-matched controls. It has beenshown that bone marrow stroma cells isolated from oste-oporotic patients have enhanced adipogenic capacityeither basally or during early cell differentiationcompared to control subjects [38,98,120,121]. Forinstance, the proliferation rate and the mitogenicresponse to IGF-1 are significantly diminished, whilethe pERK/ERK ratio is increased in osteoporoticMSCs, compared with control MSCs [121,122]. In othercell types, activation of the MEK/ERK signalingpathway has been shown to enhance the activity of adi-pogenic transcription factors [123]. On the other hand,MSCs derived from osteoporotic donors have dimin-ished alkaline phosphatase activity and less calciumdeposition under osteogenic differentiation conditions,in agreement with their reduced capability to producemature forming bone cells. In addition to the intrinsiccharacteristic of MSCs involved in cell commitmentand differentiation, it is recognized that locallyproduced factors like leptin, estrogens, fatty acids, and
growth factors may be important in regulating neigh-boring osteoblasts. For example, in vitro studiesconfirmed that bone marrow MSCs were responsive toleptin, both through enhanced proliferation and differ-entiation into the osteoblastic lineage [124e126], aswell as inhibition of MSCs into adipocytes [125,127].
After menopause, decreased endogenous estradiolenhances bone turnover. This is accompanied by a shiftin the adipocyte to osteoblast ratio, favoring fat accumu-lation in the bone marrow [105,128]. A direct effect ofestrogen on the skeleton has been underlined by devel-opmental failure of bone in males with deficientestrogen activity [129,130]. The skeletal response tofalling estrogen levels has also been demonstratedin vitro and in vivo. In the former, in human MSCs recip-rocal estrogen regulation of osteogenic and adipogenicdifferentiation has been reported [131,132]. In the latter,bone biopsy samples from postmenopausal womenrevealed that estrogen replacement was associatedwith markedly reduced adipocytes compared to womenwithout estrogen replacement (Khosla, personalcommunication). The observation that aromatase(the enzyme responsible for estrogen biosynthesis) andother enzymes implicated in sex metabolism are foundin extra gonadal organs, including adipose and bonetissues [133e136], has strengthened the concept thatlocally generated androgens and estrogens can exertregulatory action on bone marrow cells. In fact, aroma-tase expression was found in MSCs [132], in osteoblasts,and osteoblast-like cells [133,134,137,138]. Studiesduring MSCs differentiation point to the potentialimportance of local estrogen production and action forosteogenic and adipogenic commitment [132,134], andas a negative regulator for adipogenesis [139,140]. Allthese observations support the hypothesis of a thresholdestradiol level for normal skeletal remodeling [141,142],which could be attained by both appropriate endoge-nous aromatase activity and estrogenic precursors.
FUTURE DIRECTION
One of the most important questions to be answeredis the function of adipose tissue within the marrowniche. Clearly, the infiltration of adipocytes is a dynamicprocess controlled at the progenitor level although notalways at the expense of osteogenesis. As a corollaryto the issue of function another question arises; i.e. ifthese adipocytes are “brown-like” do they generateheat, and is this important for optimal bone acquisition?In preliminary data from the Li laboratory at UCSF inB6 mice, the degree of saturation of marrow fat felldramatically from 3 weeks of age to 16 weeks, aninterval during and after peak bone acquisition. Simi-larly, one could ask whether the characteristics of

14. BONE MARROW FAT AND BONE MASS176
marrow fat change with age; i.e. do aging mice andhumans still have the capacity to generate “brown-like” adipocytes or is the marrow infiltration of agingpurely a “filler” for empty marrow space. Regardlessof the mechanism, the consequences of marrowadiposity as it relates to structural integrity still needto be defined before its magnitude can be defined asa risk factor for subsequent fractures. Finally, it is essen-tial that we understand the afferent signals from themarrow and bone that influence the appearance ofadipocytes. With newer cell and tissue functionalstudies, the possibilities of answering these questionsare enhanced.
References
[1] Huggins C, Blocksom BH. Changes in bone marrow accompa-nying a local increase of temperature within physiologicallimits. J Exp Med 1936:1e26.
[2] Meunier P, Aaron J, Edouard C, Vignon G. Osteoporosis and thereplacement of cell populations of the marrow by adiposetissue. A quantitative study of 84 iliac bone biopsies. ClinOrthop Relat Res 1971;80:147e54.
[3] Griffith JF, Yeung DK, Antonio GE, Wong SY, Kwok TC, Woo J,et al. Vertebral marrow fat content and diffusion and perfusionindexes in women with varying bone density: MR evaluation.Radiology 2006;241:831e8.
[4] Rosen ED, MacDougald OA. Adipocyte differentiation from theinside out. Nat Rev Mol Cell Biol 2006;7:885e96.
[5] Kawai M, Sousa KM, MacDougald OA, Rosen CJ. The manyfacets of PPARgamma: novel insights for the skeleton. Am JPhysiol Endocrinol Metab 2010;299:E3e9.
[6] Rosen ED, Spiegelman BM. Molecular regulation of adipo-genesis. Annu Rev Cell Dev Biol 2000;16:145e71.
[7] Kubota N, Terauchi Y, Miki H, Tamemoto H, Yamauchi T,Komeda K, et al. PPAR gamma mediates high-fat diet-inducedadipocyte hypertrophy and insulin resistance. Mol Cell1999;4:597e609.
[8] Darlington GJ, Ross SE, MacDougald OA. The role of C/EBPgenes in adipocyte differentiation. J Biol Chem 1998;273:30057e60.
[9] Tanaka T, Yoshida N, Kishimoto T, Akira S. Defective adipocytedifferentiation in mice lacking the C/EBPbeta and/or C/EBP-delta gene. EMBO J 1997;16:7432e43.
[10] Tontonoz P, Spiegelman BM. Fat and beyond: the diversebiology of PPARgamma. Annu Rev Biochem 2008;77:289e312.
[11] Kawai M, Rosen CJ. PPARgamma: a circadian transcriptionfactor in adipogenesis and osteogenesis. Nat Rev Endocrinol2010;6:629e36.
[12] Braissant O, Foufelle F, Scotto C, Dauca M, Wahli W. Differentialexpression of peroxisome proliferator-activated receptors(PPARs): tissue distribution of PPAR-alpha, -beta, and -gammain the adult rat. Endocrinology 1996;137:354e66.
[13] Tontonoz P, Hu E, Graves RA, Budavari AI, Spiegelman BM.mPPAR gamma 2: tissue-specific regulator of an adipocyteenhancer. Genes Dev 1994;8:1224e34.
[14] Mori T, Sakaue H, Iguchi H, Gomi H, Okada Y, Takashima Y,et al. Role of Kruppel-like factor 15 (KLF15) in transcriptionalregulation of adipogenesis. J Biol Chem 2005;280:12867e75.
[15] Oishi Y, Manabe I, Tobe K, Tsushima K, Shindo T, Fujiu K, et al.Kruppel-like transcription factor KLF5 is a key regulator ofadipocyte differentiation. Cell Metab 2005;1:27e39.
[16] Gupta RK, Arany Z, Seale P, Mepani RJ, Ye L, Conroe HM, et al.Transcriptional control of preadipocyte determination byZfp423. Nature 464:619e23.
[17] Banerjee SS, Feinberg MW, Watanabe M, Gray S, Haspel RL,Denkinger DJ, et al. The Kruppel-like factor KLF2 inhibitsperoxisome proliferator-activated receptor-gamma expressionand adipogenesis. J Biol Chem 2003;278:2581e4.
[18] Tong Q, Tsai J, Tan G, Dalgin G, Hotamisligil GS. Interactionbetween GATA and the C/EBP family of transcription factors iscritical in GATA-mediated suppression of adipocyte differenti-ation. Mol Cell Biol 2005;25:706e15.
[19] Kawai M, Sousa KM, MacDougald OA, Rosen CJ. The manyfacets of PPARgamma: novel insights for the skeleton. Am JPhysiol Endocrinol Metab 2010;299:E3e9.
[20] Kawai M, Rosen CJ. PPARgamma: a circadian transcriptionfactor in adipogenesis and osteogenesis. Nat Rev Endocrinol2010;6:629e36.
[21] Forman BM, Tontonoz P, Chen J, Brun RP, Spiegelman BM,Evans RM. 15-Deoxy-delta 12, 14-prostaglandin J2 is a ligandfor the adipocyte determination factor PPAR gamma. Cell1995;83:803e12.
[22] Bell-Parikh LC, Ide T, Lawson JA, McNamara P, Reilly M,FitzGerald GA. Biosynthesis of 15-deoxy-delta12,14-PGJ2and the ligation of PPARgamma. J Clin Invest 2003;112:945e55.
[23] Ciaraldi TP, Gilmore A, Olefsky JM, Goldberg M,Heidenreich KA. In vitro studies on the action of CS-045, a newantidiabetic agent. Metabolism 1990;39:1056e62.
[24] Fujiwara T, Yoshioka S, Yoshioka T, Ushiyama I, Horikoshi H.Characterization of new oral antidiabetic agent CS-045. Studiesin KK and ob/ob mice and Zucker fatty rats. Diabetes1988;37:1549e58.
[25] Iwamoto Y, Kuzuya T, Matsuda A, Awata T, Kumakura S,Inooka G, et al. Effect of new oral antidiabetic agent CS-045 onglucose tolerance and insulin secretion in patients withNIDDM. Diabetes Care 1991;14:1083e6.
[26] Nolan JJ, Ludvik B, Beerdsen P, Joyce M, Olefsky J. Improve-ment in glucose tolerance and insulin resistance in obesesubjects treated with troglitazone. N Engl J Med 1994;331:1188e93.
[27] Suter SL, Nolan JJ, Wallace P, Gumbiner B, Olefsky JM. Meta-bolic effects of new oral hypoglycemic agent CS-045 in NIDDMsubjects. Diabetes Care 1992;15:193e203.
[28] Guan HP, Ishizuka T, Chui PC, Lehrke M, Lazar MA. Core-pressors selectively control the transcriptional activity ofPPARgamma in adipocytes. Genes Dev 2005;19:453e61.
[29] Takada I, Mihara M, Suzawa M, Ohtake F, Kobayashi S,Igarashi M, et al. A histone lysine methyltransferase activatedby non-canonical Wnt signalling suppresses PPAR-gammatransactivation. Nat Cell Biol 2007;9:1273e85.
[30] Camp HS, Tafuri SR. Regulation of peroxisome proliferator-activated receptor gamma activity by mitogen-activated proteinkinase. J Biol Chem 1997;272:10811e6.
[31] Hosooka T, Noguchi T, Kotani K, Nakamura T, Sakaue H,Inoue H, et al. Dok1 mediates high-fat diet-induced adipocytehypertrophy and obesity through modulation of PPAR-gammaphosphorylation. Nat Med 2008;14:188e93.
[32] Hu E, Kim JB, Sarraf P, Spiegelman BM. Inhibition of adipo-genesis through MAP kinase-mediated phosphorylation ofPPARgamma. Science 1996;274:2100e3.
[33] Choi JH, Banks AS, Estall JL, Kajimura S, Bostrom P, Laznik D,et al. Anti-diabetic drugs inhibit obesity-linked phosphoryla-tion of PPARgamma by Cdk5. Nature 2010;466:451e6.
[34] Choi JH, Banks AS, Kamenecka TM, Busby SA, Chalmers MJ,Kumar N, et al. Antidiabetic actions of a non-agonist

REFERENCES 177
PPARgamma ligand blocking Cdk5-mediated phosphorylation.Nature 2011;477:477e81.
[35] Floyd ZE, Stephens JM. Interferon-gamma-mediated activationand ubiquitin-proteasome-dependent degradation of PPAR-gamma in adipocytes. J Biol Chem 2002;277:4062e8.
[36] Hauser S, Adelmant G, Sarraf P, Wright HM, Mueller E,Spiegelman BM. Degradation of the peroxisome proliferator-activated receptor gamma is linked to ligand-dependent acti-vation. J Biol Chem 2000;275:18527e33.
[37] Yamashita D, Yamaguchi T, Shimizu M, Nakata N, Hirose F,Osumi T. The transactivating function of peroxisome pro-liferator-activated receptor gamma is negatively regulated bySUMO conjugation in the amino-terminal domain. Genes Cells2004;9:1017e29.
[38] Bianco P, Riminucci M, Gronthos S, Robey PG. Bone marrowstromal stem cells: nature, biology, and potential applications.Stem Cells 2001;19:180e92.
[39] Jiang Y, Jahagirdar BN, Reinhardt RL, Schwartz RE, Keene CD,Ortiz-Gonzalez XR, et al. Pluripotency of mesenchymal stemcells derived from adult marrow. Nature 2002;418:41e9.
[40] Minguell JJ, Erices A, Conget P. Mesenchymal stem cells. ExpBiol Med (Maywood) 2001;226:507e20.
[41] Shockley KR, Lazarenko OP, Czernik PJ, Rosen CJ,Churchill GA, Lecka-Czernik B. PPARgamma2 nuclear receptorcontrols multiple regulatory pathways of osteoblast differenti-ation from marrow mesenchymal stem cells. J Cell Biochem2009;106:232e46.
[42] Lecka-Czernik B, Gubrij I, Moerman EJ, Kajkenova O,Lipschitz DA, Manolagas SC, et al. Inhibition of Osf2/Cbfa1expression and terminal osteoblast differentiation by PPAR-gamma2. J Cell Biochem 1999;74:357e71.
[43] Cheng SL, Shao JS, Charlton-Kachigian N, Loewy AP,Towler DA. MSX2 promotes osteogenesis and suppresses adi-pogenic differentiation of multipotent mesenchymal progeni-tors. J Biol Chem 2003;278:45969e77.
[44] Ichida F, Nishimura R, Hata K, Matsubara T, Ikeda F, Hisada K,et al. Reciprocal roles of MSX2 in regulation of osteoblast andadipocyte differentiation. J Biol Chem 2004;279:34015e22.
[45] Kang S, Bennett CN, Gerin I, Rapp LA, Hankenson KD,Macdougald OA. Wnt signaling stimulates osteoblastogenesisof mesenchymal precursors by suppressing CCAAT/enhancer-binding protein alpha and peroxisome proliferator-activatedreceptor gamma. J Biol Chem 2007;282:14515e24.
[46] Moerman EJ, Teng K, Lipschitz DA, Lecka-Czernik B. Agingactivates adipogenic and suppresses osteogenic programs inmesenchymal marrow stroma/stem cells: the role of PPAR-gamma2 transcription factor and TGF-beta/BMP signalingpathways. Aging Cell 2004;3:379e89.
[47] Akune T, Ohba S, Kamekura S, Yamaguchi M, Chung UI,Kubota N, et al. PPARgamma insufficiency enhances osteo-genesis through osteoblast formation from bone marrowprogenitors. J Clin Invest 2004;113:846e55.
[48] Cock TA, Back J, Elefteriou F, Karsenty G, Kastner P, Chan S,Auwerx J. Enhanced bone formation in lipodystrophic PPAR-gamma(hyp/hyp) mice relocates haematopoiesis to the spleen.EMBO Rep 2004;5:1007e12.
[49] Li M, Pan LC, Simmons HA, Li Y, Healy DR, Robinson BS, et al.Surface-specific effects of a PPARgamma agonist, darglitazone,on bone in mice. Bone 2006;39:796e806.
[50] Sottile V, Seuwen K, Kneissel M. Enhanced marrow adipo-genesis and bone resorption in estrogen-deprived rats treatedwith the PPARgamma agonist BRL49653 (rosiglitazone). CalcifTissue Int 2004;75:329e37.
[51] Wan Y, Chong LW, Evans RM. PPAR-gamma regulates osteo-clastogenesis in mice. Nat Med 2007;13:1496e503.
[52] Wei W, Wang X, Yang M, Smith LC, Dechow PC, Wan Y.PGC1beta mediates PPARgamma activation of osteoclasto-genesis and rosiglitazone-induced bone loss. Cell Metab11:503e16.
[53] Lazarenko OP, Rzonca SO, Hogue WR, Swain FL, Suva LJ,Lecka-Czernik B. Rosiglitazone induces decreases in bone massand strength that are reminiscent of aged bone. Endocrinology2007;148:2669e80.
[54] Bendixen AC, Shevde NK, Dienger KM, Willson TM, Funk CD,Pike JW. IL-4 inhibits osteoclast formation through a directaction on osteoclast precursors via peroxisome proliferator-activated receptor gamma 1. Proc Natl Acad Sci USA2001;98:2443e8.
[55] Hounoki H, Sugiyama E, Mohamed SG, Shinoda K, Taki H,Abdel-Aziz HO, et al. Activation of peroxisome proliferator-activated receptor gamma inhibits TNF-alpha-mediated osteo-clast differentiation in human peripheral monocytes in part viasuppression of monocyte chemoattractant protein-1 expression.Bone 2008;42:765e74.
[56] Naveiras O, Nardi V, Wenzel PL, Hauschka PV, Fahey F,Daley GQ. Bone-marrow adipocytes as negative regulators ofthe haematopoietic microenvironment. Nature 2009;460:259e63.
[57] Botolin S, McCabe LR. Inhibition of PPARgamma prevents typeI diabetic bone marrow adiposity but not bone loss. J CellPhysiol 2006;209:967e76.
[58] Sheng MH, Baylink DJ, Beamer WG, Donahue LR, Rosen CJ,Lau KH, et al. Histomorphometric studies show that boneformation and bone mineral apposition rates are greater inC3H/HeJ (high-density) than C57BL/6J (low-density) miceduring growth. Bone 1999;25:421e9.
[59] Kawai M, Rosen CJ. Insulin-like growth factor-I and bone:lessons from mice and men. Pediatr Nephrol 2009;24:1277e85.
[60] Horowitz MC, Bothwell AL, Hesslein DG, Pflugh DL,Schatz DG. B cells and osteoblast and osteoclast development.Immunol Rev 2005;208:141e53.
[61] Krings A, Rahman S, Huang S, Lu Y, Czernik PJ, Lecka-Czernik B. Bone marrow fat has brown adipose tissue charac-teristics, which are attenuated with aging and diabetes. Bone2012 Feb;50(2):546e52. Epub 2011 Jun 24.
[62] Vestergaard P. Discrepancies in bone mineral density andfracture risk in patients with type 1 and type 2 diabetesdameta-analysis. Osteoporos Int 2007;18:427e44.
[63] McCabe LR. Understanding the pathology and mechanismsof type I diabetic bone loss. J Cell Biochem 2007;102:1343e57.
[64] Botolin S, Faugere MC, Malluche H, Orth M, Meyer R,McCabe LR. Increased bone adiposity and peroxisomal pro-liferator-activated receptor-gamma2 expression in type I dia-betic mice. Endocrinology 2005;146:3622e31.
[65] Botolin S, McCabe LR. Bone loss and increased bone adiposityin spontaneous and pharmacologically induced diabetic mice.Endocrinology 2007;148:198e205.
[66] Ackert-Bicknell CL, Shockley KR, Horton LG, Lecka-Czernik B,Churchill GA, Rosen CJ. Strain-specific effects of rosiglitazoneon bone mass, body composition, and serum insulin-likegrowth factor-I. Endocrinology 2009;150:1330e40.
[67] Tornvig L, Mosekilde LI, Justesen J, Falk E, Kassem M. Trogli-tazone treatment increases bone marrow adipose tissue volumebut does not affect trabecular bone volume in mice. CalcifTissue Int 2001;69:46e50.
[68] Aleo MD, Lundeen GR, Blackwell DK, Smith WM,Coleman GL, Stadnicki SW, et al. Mechanism and implicationsof brown adipose tissue proliferation in rats and monkeystreated with the thiazolidinedione darglitazone, a potent

14. BONE MARROW FAT AND BONE MASS178
peroxisome proliferator-activated receptor-gamma agonist. JPharmacol Exp Ther 2003;305:1173e82.
[69] Lazarenko OP, Rzonca SO, Suva LJ, Lecka-Czernik B. Netogli-tazone is a PPAR-gamma ligand with selective effects on boneand fat. Bone 2006;38:74e84.
[70] Devlin MJ, Cloutier AM, Thomas NA, Panus DA, Lotinun S,Pinz I, et al. Caloric restriction leads to high marrow adiposityand low bone mass in growing mice. J Bone Miner Res2010;25:2078e88.
[71] Bredella MA, Fazeli PK, Miller KK, Misra M, Torriani M,Thomas BJ, et al. Increased bone marrow fat in anorexia nerv-osa. J Clin Endocrinol Metab 2009;94:2129e36.
[72] Fazeli PK, Bredella MA, Misra M, Meenaghan E, Rosen CJ,Clemmons DR, et al. Preadipocyte factor-1 is associated withmarrow adiposity and bone mineral density in women withanorexia nervosa. J Clin Endocrinol Metab 2010;95:407e13.
[73] Thompson NM, Gill DA, Davies R, Loveridge N, Houston PA,Robinson IC, et al. Ghrelin and des-octanoyl ghrelin promoteadipogenesis directly in vivo by a mechanism independent ofthe type 1a growth hormone secretagogue receptor. Endocri-nology 2004;145:234e42.
[74] Elefteriou F, Ahn JD, Takeda S, Starbuck M, Yang X, Liu X, et al.Leptin regulation of bone resorption by the sympatheticnervous system and CART. Nature 2005;434:514e20.
[75] Takeda S, Elefteriou F, Levasseur R, Liu X, Zhao L, Parker KL,et al. Leptin regulates bone formation via the sympatheticnervous system. Cell 2002;111:305e17.
[76] Ducy P, Amling M, Takeda S, Priemel M, Schilling AF, Beil FT,et al. Leptin inhibits bone formation through a hypothalamicrelay: a central control of bone mass. Cell 2000;100:197e207.
[77] Ingalls AM, Dickie MM, Snell GD. Obese, a new mutation in thehouse mouse. J Hered 1950;41:317e8.
[78] Zhang Y, Proenca R, Maffei M, Barone M, Leopold L,Friedman JM. Positional cloning of the mouse obese gene andits human homologue. Nature 1994;372:425e32.
[79] Charlton HM. Mouse mutants as models in endocrine research.Q J Exp Physiol 1984;69:655e76.
[80] Hamrick MW, Pennington C, Newton D, Xie D, Isales C. Leptindeficiency produces contrasting phenotypes in bones of thelimb and spine. Bone 2004;34:376e83.
[81] Bartell SM, Rayalam S, Ambati S, Gaddam DR, Hartzell DL,Hamrick M, et al. Central (ICV) leptin injection increases boneformation, bone mineral density, muscle mass, serum IGF-1,and the expression of osteogenic genes in leptin-deficient ob/obmice. J Bone Miner Res 2011;26:1710e20.
[82] Gryglewski RJ. Prostacyclin among prostanoids. PharmacolRep 2008;60:3e11.
[83] Iwaniec UT, Boghossian S, Trevisiol CH, Wronski TJ, Turner RT,Kalra SP. Hypothalamic leptin gene therapy prevents weightgain without long-term detrimental effects on bone in growingand skeletally mature female rats. J Bone Miner Res2011;26:1506e16.
[84] Williams GA, Callon KE, Watson M, Costa JL, Ding Y,Dickinson M, et al. Skeletal phenotype of the leptin receptor-deficient db/db mouse. J Bone Miner Res 2011;26:1698e709.
[85] MartinLM,McCabeLR.Type Idiabetic bonephenotype is locationbut not gender dependent. Histochem Cell Biol 2007;128:125e33.
[86] Charlton HM, Clark RG, Robinson IC, Goff AE, Cox BS,Bugnon C, et al. Growth hormone-deficient dwarfism in the rat:a new mutation. J Endocrinol 1988;119:51e8.
[87] Gevers EF, Loveridge N, Robinson IC. Bone marrow adipocytes:a neglected target tissue for growth hormone. Endocrinology2002;143:4065e73.
[88] Menagh PJ, Turner RT, Jump DB, Wong CP, Lowry MB, Yakar S,et al. Growth hormone regulates the balance between bone
formation and bone marrow adiposity. J Bone Miner Res2010;25:757e68.
[89] Gimble JM. The function of adipocytes in the bone marrowstroma. New Biol 1990;2:304e12.
[90] Tavassoli M. Marrow adipose cells and hemopoiesis: an inter-pretative review. Exp Hematol 1984;12:139e46.
[91] Gimble JM, Robinson CE, Wu X, Kelly KA. The function ofadipocytes in the bone marrow stroma: an update. Bone1996;19:421e8.
[92] Payne MW, Uhthoff HK, Trudel G. Anemia of immobility:caused by adipocyte accumulation in bone marrow. MedHypotheses 2007;69:778e86.
[93] Rozman C, Feliu E, Berga L, Reverter JC, Climent C, Ferran MJ.Age-related variations of fat tissue fraction in normal humanbone marrow depend both on size and number of adipocytes:a stereological study. Exp Hematol 1989;17:34e7.
[94] Dazzi F, Ramasamy R, Glennie S, Jones SP, Roberts I. The role ofmesenchymal stem cells in haemopoiesis. Blood Rev2006;20:161e71.
[95] Cornish J, MacGibbon A, Lin JM, Watson M, Callon KE,Tong PC, et al. Modulation of osteoclastogenesis by fatty acids.Endocrinology 2008;149:5688e95.
[96] Aghaloo TL, Felsenfeld AL, Tetradis S. Osteonecrosis of the jawin a patient on Denosumab. J Oral Maxillofac Surg 68:959e63.
[97] Gimble JM, Zvonic S, Floyd ZE, KassemM, Nuttall ME. Playingwith bone and fat. J Cell Biochem 2006;98:251e66.
[98] Nuttall ME, Gimble JM. Controlling the balance betweenosteoblastogenesis and adipogenesis and the consequent ther-apeutic implications. Curr Opin Pharmacol 2004;4:290e4.
[99] Lecka-Czernik B. Marrow fat metabolism is linked to thesystemic energy metabolism. Bone 2012 Feb;50(2):534e9. Epub2011 Jul 4. Review.
[100] Di Iorgi N, Mittelman SD, Gilsanz V. Differential effect ofmarrow adiposity and visceral and subcutaneous fat oncardiovascular risk in young, healthy adults. Int J Obes (Lond)2008;32:1854e60.
[101] Bredella MA, Torriani M, Ghomi RH, Thomas BJ, Brick DJ,Gerweck AV, et al. Vertebral bone marrow fat is positivelyassociated with visceral fat and inversely associated with IGF-1in obese women. Obesity (Silver Spring) 2011;19:49e53.
[102] Manolagas SC. Cellular and molecular mechanisms of osteo-porosis. Aging (Milano) 1998;10:182e90.
[103] Manolagas SC. From estrogen-centric to aging and oxidativestress: a revised perspective of the pathogenesis of osteoporosis.Endocr Rev 31:266e300.
[104] Wagner W, Bork S, Lepperdinger G, Joussen S, Ma N, Strunk D,et al. How to track cellular aging of mesenchymal stromal cells?Aging (Albany NY) 2010;2:224e30.
[105] Justesen J, Stenderup K, Ebbesen EN, Mosekilde L, Steiniche T,Kassem M. Adipocyte tissue volume in bone marrow isincreased with aging and in patients with osteoporosis. Bio-gerontology 2001;2:165e71.
[106] Burkhardt R, Kettner G, Bohm W, Schmidmeier M, Schlag R,Frisch B, et al. Changes in trabecular bone, hematopoiesis andbone marrow vessels in aplastic anemia, primary osteoporosis,and old age: a comparative histomorphometric study. Bone1987;8:157e64.
[107] Minaire P, Edouard C, Arlot M, Meunier PJ. Marrow changes inparaplegic patients. Calcif Tissue Int 1984;36:338e40.
[108] Belin de Chantemele E, Blanc S, Pellet N, Duvareille M,Ferretti G, Gauquelin-Koch G, et al. Does resistance exerciseprevent body fluid changes after a 90-day bed rest? Eur J ApplPhysiol 2004;92:555e64.
[109] LeBlanc A, Schneider V, Shackelford L, West S, Oganov V,Bakulin A, et al. Bone mineral and lean tissue loss after long

REFERENCES 179
duration space flight. J Musculoskelet Neuronal Interact 2000;1:157e60.
[110] Wronski TJ, Walsh CC, Ignaszewski LA. Histologic evidence forosteopenia and increased bone turnover in ovariectomized rats.Bone 1986;7:119e23.
[111] Forsen L, Meyer HE, Midthjell K, Edna TH. Diabetes mellitusand the incidence of hip fracture: results from the Nord-Tron-delag Health Survey. Diabetologia 1999;42:920e5.
[112] Vande Berg BC, Malghem J, Lecouvet FE, Devogelaer JP,Maldague B, Houssiau FA. Fat conversion of femoral marrow inglucocorticoid-treated patients: a cross-sectional and longitu-dinal study with magnetic resonance imaging. Arthritis Rheum1999 Jul;42(7):1405e11.
[113] Grey A, Bolland M, Gamble G, Wattie D, Horne A, Davidson J,Reid IR. The peroxisome proliferator-activated receptor-gammaagonist rosiglitazone decreases bone formation and bonemineral density in healthy postmenopausal women: a random-ized, controlled trial. J Clin Endocrinol Metab 2007;92:1305e10.
[114] Habib ZA, Havstad SL, Wells K, Divine G, Pladevall M, Wil-liams LK. Thiazolidinedione use and the longitudinal risk offractures in patients with type 2 diabetes mellitus. J ClinEndocrinol Metab 95:592e600.
[115] Harslof T, Wamberg L, Moller L, Stodkilde-Jorgensen H,Ringgaard S, Pedersen SB, et al. Rosiglitazone decreases bonemass and bone marrow fat. J Clin Endocrinol Metab 2011;96:1541e8.
[116] Abella E, Feliu E, Granada I, Milla F, Oriol A, Ribera JM, et al.Bone marrow changes in anorexia nervosa are correlated withthe amount of weight loss and not with other clinical findings.Am J Clin Pathol 2002;118:582e8.
[117] Wehrli FW, Hopkins JA, Hwang SN, Song HK, Snyder PJ,Haddad JG. Cross-sectional study of osteopenia with quanti-tative MR imaging and bone densitometry. Radiology2000;217:527e38.
[118] Yeung DK, Griffith JF, Antonio GE, Lee FK, Woo J, Leung PC.Osteoporosis is associated with increased marrow fat contentand decreased marrow fat unsaturation: a proton MR spec-troscopy study. J Magn Reson Imaging 2005;22:279e85.
[119] Griffith JF, Yeung DK, Tsang PH, Choi KC, Kwok TC, Ahuja AT,et al. Compromised bone marrow perfusion in osteoporosis. JBone Miner Res 2008;23:1068e75.
[120] Gimble JM, Robinson CE, Wu X, Kelly KA, Rodriguez BR,Kliewer SA, et al. Peroxisome proliferator-activated recep-tor-gamma activation by thiazolidinediones induces adipo-genesis in bone marrow stromal cells. Mol Pharmacol 1996;50:1087e94.
[121] Rodriguez JP, Garat S, Gajardo H, Pino AM, Seitz G. Abnormalosteogenesis in osteoporotic patients is reflected by alteredmesenchymal stem cells dynamics. J Cell Biochem 1999;75:414e23.
[122] Rodriguez JP, Rios S, Fernandez M, Santibanez JF. Differentialactivation of ERK1,2 MAP kinase signaling pathway inmesenchymal stem cell from control and osteoporotic post-menopausal women. J Cell Biochem 2004;92:745e54.
[123] Prusty D, Park BH, Davis KE, Farmer SR. Activation of MEK/ERK signaling promotes adipogenesis by enhancing peroxi-some proliferator-activated receptor gamma (PPARgamma) andC/EBPalpha gene expression during the differentiation of 3T3-L1 preadipocytes. J Biol Chem 2002;277:46226e32.
[124] Takahashi Y, Okimura Y, Mizuno I, Iida K, Takahashi T, Kaji H,et al. Leptin induces mitogen-activated protein kinase-dependentproliferation of C3H10T1/2 cells. J Biol Chem 1997;272:12897e900.
[125] Thomas T, Gori F, Khosla S, Jensen MD, Burguera B, Riggs BL.Leptin acts on human marrow stromal cells to enhance
differentiation to osteoblasts and to inhibit differentiation toadipocytes. Endocrinology 1999;140:1630e8.
[126] Reseland JE, Syversen U, Bakke I, Qvigstad G, Eide LG,Hjertner O, et al. Leptin is expressed in and secreted fromprimary cultures of human osteoblasts and promotes bonemineralization. J Bone Miner Res 2001;16:1426e33.
[127] Hess R, Pino AM, Rios S, Fernandez M, Rodriguez JP. Highaffinity leptin receptors are present in human mesenchymalstem cells (MSCs) derived from control and osteoporoticdonors. J Cell Biochem 2005;94:50e7.
[128] Gambacciani M, Ciaponi M, Cappagli B, Piaggesi L, DeSimone L, Orlandi R, et al. Body weight, body fat distribution,and hormonal replacement therapy in early postmenopausalwomen. J Clin Endocrinol Metab 1997;82:414e7.
[129] Smith EP, Boyd J, Frank GR, Takahashi H, Cohen RM,Specker B, et al. Estrogen resistance caused by a mutation in theestrogen-receptor gene in a man. N Engl J Med 1994;331:1056e61.
[130] Morishima A, Grumbach MM, Simpson ER, Fisher C, Qin K.Aromatase deficiency in male and female siblings caused bya novel mutation and the physiological role of estrogens. J ClinEndocrinol Metab 1995;80:3689e98.
[131] Pino AM, Rodriguez JM, Rios S, Astudillo P, Leiva L, Seitz G,et al. Aromatase activity of human mesenchymal stem cells isstimulated by early differentiation, vitamin D and leptin. JEndocrinol 2006;191:715e25.
[132] Heim M, Frank O, Kampmann G, Sochocky N, Pennimpede T,Fuchs P, et al. The phytoestrogen genistein enhances osteo-genesis and represses adipogenic differentiation of humanprimary bone marrow stromal cells. Endocrinology 2004;145:848e59.
[133] Schweikert HU, Wolf L, Romalo G. Oestrogen formation fromandrostenedione in human bone. Clin Endocrinol (Oxf) 1995;43:37e42.
[134] Janssen JM, Bland R, Hewison M, Coughtrie MW, Sharp S,Arts J, et al. Estradiol formation by human osteoblasts viamultiple pathways: relation with osteoblast function. J CellBiochem 1999;75:528e37.
[135] Compston J. Local biosynthesis of sex steroids in bone. J ClinEndocrinol Metab 2002;87:5398e400.
[136] Issa S, Schnabel D, Feix M, Wolf L, Schaefer HE, Russell DW,et al. Human osteoblast-like cells express predominantly steroid5alpha-reductase type 1. J Clin Endocrinol Metab 2002;87:5401e7.
[137] Tanaka S, Haji M, Nishi Y, Yanase T, Takayanagi R, Nawata H.Aromatase activity in human osteoblast-like osteosarcoma cell.Calcif Tissue Int 1993;52:107e9.
[138] Sasano H, Uzuki M, Sawai T, Nagura H, Matsunaga G,Kashimoto O, et al. Aromatase in human bone tissue. J BoneMiner Res 1997;12:1416e23.
[139] Heine PA, Taylor JA, Iwamoto GA, Lubahn DB, Cooke PS.Increased adipose tissue in male and female estrogen recep-tor-alpha knockout mice. Proc Natl Acad Sci USA 2000;97:12729e34.
[140] Okazaki R, Inoue D, Shibata M, Saika M, Kido S, Ooka H, et al.Estrogen promotes early osteoblast differentiation and inhibitsadipocyte differentiation in mouse bone marrow stromal celllines that express estrogen receptor (ER) alpha or beta. Endo-crinology 2002;143:2349e56.
[141] Riggs BL, Khosla S, Melton 3rd LJ. Sex steroids and theconstruction and conservation of the adult skeleton. Endocr Rev2002;23:279e302.
[142] Gennari L, Nuti R, Bilezikian JP. Aromatase activity and bonehomeostasis in men. J Clin Endocrinol Metab 2004;89:5898e907.