Embed Size (px)
Citation preview

Sagar Lonial, MD, FACPWinship Cancer InstituteEmory University School of MedicineAtlanta, Georgia
Course Director
Participate in interactive questions, download activity slides, and obtain your instant CME/CE credit online.
This CME/CE activity is jointly provided by Penn State College of Medicine and PVI, PeerView Institute for Medical Education; this activity is also co-provided by Medical Learning Institute, Inc.
CME/CE
Translating Therapeutic Innovations Into the Management of Multiple Myeloma: Insights on Modern Practice Across Disease Settings
What’s Inside
3
9
Tailoring Care in Newly Diagnosed Multiple Myeloma
New Developments in Pretreated Multiple Myeloma: Early Relapse
Novel Agents in Heavily Pretreated or Refractory Multiple Myeloma15
www.peerviewpress.com/SGC900

2 Go online to complete the post-test and evaluation for CME/CE credit
Activity Information
Activity Description and Educational ObjectivesIn this activity, a hematologic oncology expert takes you on a tour of key data and clinical considerations in the modern management of patients with multiple myeloma. Topics covered include the most recent developments on novel agent classes and next-generation therapeutics for myeloma, as well as perspectives on individualizing care in both newly-diagnosed and relapsed/refractory disease—how do age, eligibility for stem-cell transplantation, high-risk features or comorbid illnesses, or need for maintenance therapy affect treatment selection? Best practices for managing treatment-related adverse events in patients with myeloma receiving novel therapies are also reviewed.
Upon completion of this activity, participants will be able to:• Discuss updated clinical data on the treatment role, efficacy, and safety of novel agent
classes and next-generation therapeutics in myeloma, including proteasome inhibitors, immunomodulatory drugs, immunotherapies, and epigenetic agents, among others
• Recommend individualized treatment regimens in newly-diagnosed myeloma, including for elderly patients, individuals eligible or ineligible for stem-cell transplantation, and those requiring continuous/maintenance therapy
• Select individualized regimens for patients with relapsed/refractory myeloma, including individuals with early relapse or treatment-refractory disease
• Manage treatment-related adverse events in patients with myeloma, including those receiving regimens that contain novel components
Target AudienceThis activity has been designed to meet the educational needs of hematologists, hematologist-oncologists, medical oncologists, advanced practice nurses, and other clinicians involved in the care of patients with multiple myeloma.
Nursing Education Purpose StatementThe purpose of this activity is to improve knowledge and competence of nurses concerning the treatment of multiple myeloma.
Requirements for Successful CompletionIn order to receive credit, participants must view the activity and complete the post-test and evaluation form. A score of 80% or higher is needed to obtain CME credit and 70% or higher to obtain CE credit. There are no pre-requisites and there is no fee to participate in this activity or to receive CME/CE credit. Statements of Credit are awarded upon successful completion of the post-test and evaluation form.
Media: Enduring MaterialRelease and Expiration Dates: August 24, 2017 - August 23, 2018Time to Complete: 60 minutes
Faculty & Disclosure / Conflict of Interest Policy Before the activity, all faculty and anyone who is in a position to have control over the content of this activity and their spouse/life partner will disclose the existence of any financial interest and/or relationship(s) they might have with any commercial interest producing healthcare goods/services to be discussed during their presentation(s): honoraria, expenses, grants, consulting roles, speakers bureau membership, stock ownership, or other special relationships. Presenters will inform participants of any off-label discussions. All identified conflicts of interest are thoroughly vetted by Penn State College of Medicine and Medical Learning Institute, Inc. for fair balance, scientific objectivity of studies mentioned in the materials or used as the basis for content, and appropriateness of patient care recommendations.
Course DirectorSagar Lonial, MD, FACPChair and ProfessorDepartment of Hematology and Medical OncologyChief Medical OfficerWinship Cancer InstituteEmory University School of MedicineAtlanta, Georgia
Sagar Lonial, MD, FACP, has a financial interest/relationship or affiliation in the form of:Consultant for Amgen, Inc.; Bristol-Myers Squibb; Celgene Corporation; GlaxoSmithKline; Janssen Pharmaceuticals, Inc.; Merck & Co., Inc.; Millennium (Takeda Oncology); Novartis Pharmaceuticals Corporation; and Onyx Pharmaceuticals Inc.Grant/Research Support from Bristol-Myers Squibb; Celgene Corporation; and Takeda Pharmaceuticals U.S.A., Inc.
Sagar Lonial, MD, FACP, does intend to discuss either non–FDA-approved or investigational use for the following products/devices: next-generation agents such as proteasome inhibitors, IMiDs, antibodies, and other innovative therapeutics.
Nurse ReviewerPamela Ash, RN, MSN, CBCNSupportive Care Nurse ClinicianMary Babb Randolph Cancer Center ClinicWest Virginia UniversityMorgantown, West Virginia
Pamela Ash, RN, MSN, CBCN, has no financial interests/relationships or affiliations in relation to this activity.
Medical DirectorsAarati Ranganathan, PhDPVI, PeerView Institute for Medical Education
Aarati Ranganathan, PhD, has no financial interests/relationships or affiliations in relation to this activity.
Carmine DeLucaPVI, PeerView Institute for Medical Education
Carmine DeLuca has no financial interests/relationships or affiliations in relation to this activity.
Other PVI staff who may potentially review content for this activity have disclosed no relevant financial relationships.
Penn State College of Medicine staff and faculty involved in the development and review of this activity have disclosed no relevant financial relationships.
The associates of Medical Learning Institute, Inc. do not have any financial relationships or relationships to products or devices with any commercial interest.
DisclaimerThe information provided at this CME/CE activity is for continuing education purposes only and is not meant to substitute for the independent medical judgment of a healthcare provider relative to diagnostic and treatment options of a specific patient’s medical condition. Recommendations for the use of particular therapeutic agents are based on the best available scientific evidence and current clinical guidelines. No bias towards or promotion for any agent discussed in this program should be inferred.
Providership, Credit & SupportPhysiciansThis activity has been planned and implemented in accordance with the accreditation requirements and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint providership of Penn State College of Medicine and PVI, PeerView Institute for Medical Education. Penn State College of Medicine is accredited by the ACCME to provide continuing medical education for physicians.
The Penn State College of Medicine designates this enduring material for a maximum of 1.0 AMA PRA Category 1 CreditTM. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Information about CME credit for this activity is available by contacting Penn State at 717-531-6483 or [email protected]. Reference course # G6171-18-T.
NursesMedical Learning Institute, Inc. Provider approved by the California Board of Registered Nursing, Provider Number 15106, for 1.0 contact hour(s).
ProvidershipThis CME/CE activity is jointly provided by Penn State College of Medicine and PVI, PeerView Institute for Medical Education; this activity is also co-provided by Medical Learning Institute, Inc.
SupportThis activity is supported by educational grants from Celgene Corporation, Merck & Co., Inc., and Takeda Oncology.
Disclosure of Unlabeled UseThe faculty of this educational activity may include discussions of products or devices that are not currently labeled for use by the FDA. Faculty members have been advised to disclose to the audience any reference to an unlabeled or investigational use.
No endorsement of unapproved products or uses is made or implied by coverage of these products or uses in our reports. No responsibility is taken for errors or omissions in reports.
Please refer to the official prescribing information for each product for discussion of approved indications, contraindications and warnings.
The materials presented here are used with the permission of the authors and/or other sources. These materials do not necessarily reflect the views of PeerView Press or any of its partners, providers, and/or supporters.
www.peerviewpress.com/SGC900

3
Translating Therapeutic Innovations Into the Management of Multiple Myeloma: Insights on Modern Practice Across Disease Settings
Dr. Lonial: Hello. This is Dr. Sagar Lonial from the Winship Cancer Institute of Emory University in Atlanta, Georgia. Welcome to this educational activity on translating some of the recent developments in myeloma care into practice.
2005-2011 Novel platforms based on agents such as bortezomib or lenalidomide
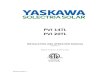
Since 2012, a Wave of Next-Generation Agents in Multiple Myeloma
Novel antibodies Next-generation PI Next-generation IMiD HDAC inhibitor
2012, 2015 Carfilzomib
2015 Panobinostat
2015
2013, 2015 Pomalidomide
2015 Daratumumab
2015 Elotuzumab + lenalidomide/
dexamethasone platform
2015 Ixazomib
2016
2016 Daratumumab + IMiD and PI platforms
2017 and Beyond Immunotherapy: PD-1 inhibitors BCMA CAR T cell Novel Targeted Agents: XPO1 and Bcl-2 inhibitors
Let’s start off talking about the revolution that’s occurred in the management of patients with myeloma over the last decade or so.
Since 2012, we’ve seen a huge wave of second-generation agents come into myeloma, including monoclonal antibodies such as daratumumab and elotuzumab; second-generation proteasome inhibitors such as carfilzomib and ixazomib; and third-generation IMiDs such as pomalidomide; and new classes of drugs such as HDAC inhibitors, including panobinostat.
And on the future horizon, we’re going to talk about some of the new agents and new drugs that will hopefully help us to shape the future of myeloma therapy, as well.
Tailoring Care in Newly Diagnosed Multiple Myeloma
Evolution of Initial Therapy in Multiple Myeloma
What are the recent data that support preferential use of triplet therapy?
VAd or dexamethasone
KTd RVd
KCd + Daratumumab?
KTd VTd
VCd
Td
Vd
Rd
So let’s talk a little bit about tailoring care in newly diagnosed multiple myeloma. We know that the evolution of initial therapy for multiple myeloma has included multiple agents that usually were used as doublets. It was either VAd [vincristine/doxorubicin/dexamethasone] or dexamethasone [dex], thalidomide/dex, lenalidomide/dex, bortezomib/dex, which then evolved into triplet-based therapies with IMiDs and proteasome inhibitors or proteasome inhibitors in combination with cyclophosphamide. And we’re now starting to go to third-level combinations that include second-generation proteasome inhibitors and monoclonal antibodies. So how do we use this information to guide what we’re initially doing right now?
SWOG S0777 (N = 525): RVd Versus Rd1
• Initial therapy: RVd for eight 21-day cycles vs Rd for six 28-day cycles in patients not intending to proceed to transplant, followed by Rd in both arms
1. Durie B et al. Lancet. 2017;389:519-527.

4 Go online to complete the post-test and evaluation for CME/CE credit
Translating Therapeutic Innovations Into the Management of Multiple Myeloma: Insights on Modern Practice Across Disease Settings
Well, in the SWOG triple-7 study, a triplet of RVd [lenalidomide/bortezomib/dexamethasone] was compared against a doublet. And there’s no question and no surprise that the progression-free survival was better in the triplet compared to the doublet. What was a surprise was that there was a big difference in overall survival favoring the use of RVd over lenalidomide and dexamethasone.
Now, what was unique about this trial is that most patients actually did not go on to have a transplant, and none of them had a transplant as part of their initial therapy. So this speaks to both a transplant-eligible and transplant-ineligible patient population, suggesting that RVd has now become a standard of care for suitable patients.
IFM2009: RVd Alone Vs RVd + ASCT1
RVd 1 Lenalidomide 12 mo
RVd 2-3 → PBSC collection → RVd 4-8
RVd 2-3 → PBSC collection → ASCT → RVd 4-5
1. Attal M et al. N Engl J Med. 2017;376:1311-1320.
Now, when you go further on, what we begin to evaluate is the role of RVd as initial induction therapy with or without stem cell transplantation. And these are data that were published by the IFM really evaluating the use of RVd with or without high-dose therapy.
The progression-free survival is clearly superior for the group that received RVd with a transplant compared to delayed transplant, but with a short follow-up, there was no difference in overall survival.
IFM2009: Response1
Outcome RVd-Alone
Group (n = 350)
Transplantation Group
(n = 350)
Adjusted Pa
Best response during study, n (%) CR VGPR PR SD
169 (48) 101 (29) 70 (20) 10 (3)
205 (59) 102 (29) 37 (11) 6 (2)
.02
CR, n (%) 169 (48) 205 (59) .003
CR or VGPR, n (%) 270 (77) 307 (88) .001
Minimal disease not detected during study, n/total n with CR or VGPR (%)b 171/265 (65) 220/278 (79) < .001
a P values were adjusted for multiplicity with the use of the Holm procedure to control the family-wise error rate at 0.05. b MRD was detected by means of flow cytometry. As a result of decisions made by the patient or the investigator, 5 patients in the RVd-alone group and 29 patients in the transplantation group were not tested. 1. Attal M et al. N Engl J Med. 2017;376:1311-1320.
However, I would argue that progression-free survival is in fact quite important, and if you begin to look at the fraction of patients that achieved MRD [minimal residual disease] negativity, two-thirds of those patients did so with a transplant, whereas only one-third did it without a transplant—again, supporting the idea that if your goal is to try and give patients a treatment that may give them the highest likelihood of achieving MRD negativity, high-dose therapy continues to have an important role in those patients.
There is a 26% reduction in risk of death, representing an estimated 2.5-year increase in median survivala
Lenalidomide Maintenance: Meta-Analysis1
Median OS (95% CI), mo
HR (95% CI) P
Len maintenance
NR (NR-NR) 0.74 (0.62-0.89)
.001 Placebo/ observation
86.0 (79.8-96.0)
a Log-rank test and Cox model stratified by study to assess impact of Len maintenance on OS. Median for len treatment arm was extrapolated to be 115 mo based on median of control arm and HR (median, 86 mo; HR = 0.74). 1. Attal M et al. 2016 American Society of Clinical Oncology Annual Meeting (ASCO 2016). Abstract 8001.
Len maintenance 605 578 555 509 474 431 385 282 200 95 20 1 0 Placebo/observation 604 569 542 505 458 425 350 271 174 71 10 0
No. at Risk
0.2
1.0
0.8
0.6
0.4
0
OS
Prob
abili
ty
0 10 20 30 40 50 60 70 80 90 100 110 120
Months
7-y OS
62%
50%
Now, the next phase of therapy for newly diagnosed myeloma patients is the role of lenalidomide maintenance.
And what I think you can see very clearly from this large meta-analysis presented at ASCO in 2016 is that with a median follow-up of somewhere around 7 years, there’s a big difference in overall survival favoring patients who have received lenalidomide maintenance, with a 26% reduction in risk of death and an estimated 2.5-year median increase in progression-free survival.
www.peerviewpress.com/SGC900

5
Translating Therapeutic Innovations Into the Management of Multiple Myeloma: Insights on Modern Practice Across Disease Settings
So this suggests that an IMiD–PI triplet has become standard; the use of high-dose therapy in transplantation continues to remain a standard; and the use of maintenance therapy—and in our hands, for standard-risk patients—also becomes a standard, as well.
• In addition to RVd (SWOG0777), VMP is an option to consider in older patients/nontransplant candidates
What About Elderly Patients? Standard Options Include Triplet …
1. San Miguel JF et al. J Clin Oncol. 2013;31:448-455.
VMP vs MP1
Now, what about looking at older transplant-ineligible patient populations? And it’s always important to realize that these data are somewhat skewed, particularly when they come from Europe, because these include patients who were 65 years old, and in the United States they’re likely eligible for high-dose therapy and autologous transplant.
We know that triplets are better than doublets, which we’ve seen from the San Miguel paper of VMP [bortezomib/melphalan/prednisone] versus melphalan and prednisone, and we’ve now seen from the SWOG study that RVd is clearly superior to Rd in terms of progression-free and overall survival.
… As Well as Doublets (FIRST Trial)
Continuous Rd Effective in High-Risk Subgroup2 Rd vs MPT1
1. Benboubker L et al. N Engl J Med. 2014;371:906-917. 2. Avet-Loiseau H et al. 57th American Society of Hematology Annual Meeting and Exhibition (ASH 2015). Abstract 730.
ORR
77 ORR
67 ORR
68
Now, the largest trial we have with a doublet in the context of transplant-ineligible patients is the FIRST trial. And this was a trial comparing MPT [melphalan/prednisone/thalidomide] versus len/dex 18 versus len/dex continuous.
And what we saw was no real difference in overall survival between those groups, but a much higher overall response rate and progression-free survival favoring the len/dex continuous therapy. And we know with lenalidomide and dexamethasone, even in the maintenance setting now, that we do continue therapy until progression.
And the FIRST trial continues to support that, at least from a progression-free survival endpoint. But again, I think that the outcomes for the RVd from the SWOG study that we talked about at the very beginning for patients who did not have a transplant appear to be somewhat superior to what we see even in the FIRST trial.
I think we have to put this in the context of what we now know. Triplets are clearly superior to doublets even in the older patient population. And there may be patients who cannot tolerate a triplet, in which case the doublet of len/dex continuous certainly is a reasonable opportunity. But certainly, for high-risk patients or patients who can tolerate triplet-based therapy, I think that the RVd SWOG study does continue to say that triplets remain the standard.
35-Day Cycle Lenalidomide •15 mg/d on days 1-21
Bortezomib •1.3 mg/m2 once weekly subQ on days 1, 8, 15, and 22
Dexamethasone •20 mg on days 1, 2, 8, 9, 15, 16, 22, and 23 for patients aged ≤75 y, and days 1, 8, 15, and 22 for patients aged >75 y
How to Modify Upfront Therapy: RVd-Lite1
Response After 4 Cycles (N = 30) n (%) ORR (≥PR) 27 (90.0) CR 5 (16.7) VGPR 11 (36.7) PR 11 (36.7) SD 3 (10.0) ≥VGPR 16 (53.3)
1. O'Donnell EK et al. ASH 2014. Abstract 4217.
Now, many have talked about trying to take the RVd triplet regimen and modify it into an easier regimen for older, frailer patients. And that gave rise to the RVd-lite regimen. These data use a lower dose of lenalidomide, use weekly subcutaneous bortezomib, and use lower doses of dexamethasone, as well.
The overall response rate in this phase 1/2 trial was about 90%. About 15% of patients achieved a complete remission, suggesting this was an active regimen. And very few patients had to come off, because this dose and schedule was better tolerated in a frailer patient and allowed patients to stay on therapy for a longer period of time.

6 Go online to complete the post-test and evaluation for CME/CE credit
Translating Therapeutic Innovations Into the Management of Multiple Myeloma: Insights on Modern Practice Across Disease Settings
1. Demo SD, et al. Cancer Res. 2007; 67:6383-6391. 2. Kirk CJ, et al, Blood. 2008;112:abstract 2765. 3. Siegel DS, et al. Blood 2012:120:2817-2825.
Next-Generation Proteasome Inhibitors1-4
Oral and next-generation
PIs
Carfilzomib Highly selective
and irreversible; IV
Oprozomib Oral; selective and
irreversible
Izaxomib Oral; selective
Rapid integration into front-line
regimens
1. Demo SD et al. Cancer Res. 2007;67:6383-6391. 2. Siegel DS et al. Blood. 2012;120:2817-2825. 3. Chauhan D et al. Clin Cancer Res. 2011;17:5311-521. 4. Parameswaran N et al. ASH 2014. Abstract 3453.
Now, as we continue to move forward, what are the next directions in upfront therapy with second-generation agents as well as antibody-based therapy?
So we know we’ve got other proteasome inhibitors that are in development or approved. Those include carfilzomib and ixazomib, both of which are approved, as well as the oral epoxyketone oprozomib, which is an oral version of carfilzomib that is not approved and is in clinical trials.
Extended Therapy With KRd in Newly Diagnosed Myeloma1
Newly diagnosed MM, ASCT
eligible
KRd (4 cycles)
ASCT
No ASCT
KRd (4 cycles)
KRd (10 cycles)
MRD MRD MRD
• KRd plus ASCT shows high rates of deep responses in newly diagnosed MM, with higher rates of sCR compared with KRd without ASCT
• High rates of MRD-negative disease, up to 97% by MFC and 71% by NGS, which appear higher than with KRd without ASCT
• Deep responses with KRd plus ASCT are associated with high rates of PFS and OS
• KRd regimen is generally well tolerated, and ASCT does not appear to add significant toxicity
• Randomized studies needed to confirm results
Induction Consolidation Maintenance
1. Zimmerman T et al. ASH 2016. Abstract 675.
These are data presented by the group from Chicago looking at KRd—carfilzomib in combination with len/dex—followed by transplantation, followed by KRd consolidation, followed by KRd maintenance for an additional 10 cycles.
And what Dr. Zimmerman and his group very nicely demonstrated from this trial was that patients could have very deep responses and that those responses could in fact be quite durable.
• Compared with standard intensive program with RVd regimen, time to response is rapid, with 78% of patients in VGPR or better at time of transplant (vs 50%)
• At the completion of consolidation, 70% of patients achieved MRD negativity by flow that is similar to RVd regimen
• Safety: Although no PN, 4 patients did not receive transplant because of toxicities; mechanisms of cardiovascular events need to be evaluated
Phase 2 IFM: KRd in Newly Diagnosed Myeloma1
Endpoint (N = 46), n
After Induction
After ASCT
End of Consolidation
Best Response, n (%)
sCR 9 15 26 32 (70) sCR + CR 11 19 28 35 (76) VGPR 25 18 11 7 (15) ≥VGPR 36 37 39 42 (91) PR 6 3 2 – ORR 42 40 41 46 (100) PD 1 1 1 –
KRd Followed by ASCT, KRd Consolidation, and Lenalidomide Maintenance
1. Roussel M et al. ASH 2016. Abstract 1142.
And if we look at the depth of response and stringent CR rate over time, what we see is that the CR rate after induction, after transplant, and at the end of consolidation continues to go up, and suggests that it may be better than what we saw with RVd, although again, it’s not been compared head to head as yet.
Cardiovascular Events: Summary
• Phase 2 IFM study: 30 of 45 patients experienced serious AEs, including cardiac and vascular issues in 8 patients1
• FORTE trial: Higher ORR rate, including more CRs, with KRd vs KCd; KRd more toxic but manageable and reversible with dose reductions2
Cardiac toxicity
1. Monitor patients for clinical signs or symptoms of cardiac failure or
cardiac ischemia
2. Withhold for Grade 3/4 cardiac AEs until recovery
Consider whether to restart at 1 dose level reduction based on a
benefit/risk assessment
Evaluate promptly if cardiac toxicity is suspected
Suggestions for Managing Cardiovascular Events With Carfilzomiba
Hydration required, though monitor for signs of volume overload; adjust total fluid intake as clinically appropriate in patients with
baseline cardiac failure or who are at risk for cardiac failure
a In patients aged ≥75 y, the risk of cardiac failure is increased compared to patients aged ˂75 y. 1. Roussel M et al. ASH 2016. Abstract 1142. 2. Gay F et al. ASCO 2017. Abstract 8003.
Now, one of the challenges that the French group brought up about KRd was about potential cardiovascular events. And if you look at that very small study, 30 of the 45 patients experienced serious adverse events, including cardiac and vascular issues in eight patients.
Many of those patients experienced thrombosis or phlebitis as a complication, as well as shortness of breath and congestive heart failure.
If you look at the FORTE trial, there was clearly a higher overall response rate for KRd versus the combination of carfilzomib with cyclophosphamide and dexamethasone. There were unique toxicities to either KRd or KCd [carfilzomib/cyclophosphamide/dexamethasone] that were managed for the most part through dose modifications and dose reductions.
www.peerviewpress.com/SGC900

7
Translating Therapeutic Innovations Into the Management of Multiple Myeloma: Insights on Modern Practice Across Disease Settings
So I think we don’t know the answer on the cardiovascular issues. They do occur relatively rarely, but they can occur even in the induction therapy setting and certainly are worthy of additional study before we make this a standard upfront recommendation for patients across the board.
IRd in Newly Diagnosed Myeloma1
CR plus stringent response VGPR PR
100
80
60
40
20
0 Cycle 3 (85%)
90
70
50
30
10
Patie
nts,
%
Cycle 6 (90%)
Cycle 9 (90%)
Cycle 12 (90%)
Time of Response Assessment
48 42 32 28
35
27
33
25
25
23
33
4
1. Kumar SK et al. Lancet Oncol. 2014;15:1503-1512.
Now, what about looking at ixazomib? These are data presented by Dr. Kumar and published in Lancet Oncology a couple of years ago looking at ixazomib, lenalidomide, and dexamethasone, or IRd, in newly diagnosed myeloma. You can see the VGPR or better rate at cycle 6 was about 50%, suggesting again that this is a very active and potent regimen for patients as they go forward.
IRd Before/After ASCT → Ixazomib Maintenance1
• IRd, 3 cycles of 28 days – Ixazomib 4 mg on days 1, 8, and 15 – Lenalidomide 25 mg on days 1 to 21 – Dexamethasone 40 mg on days 1, 8, 15, and 22
Induction
• Mobilization: Cyclophosphamide 3 g/m2 and G-CSF 5 mcg/kg PBSC harvest
• Melphalan 200 mg/m2 Peripheral SCT
• IRd, 2 cycles of 28 days Early consolidation
• IR (without dexamethasone), 6 cycles of 28 days Late consolidation
• Ixazomib 4 mg on days 1, 8, and 15 of each 28-day cycle
Maintenance therapy for 1 year
1. Moreau P et al. ASH 2016. Abstract 674.
And there are now trials from the French group again looking at IRd [ixazomib/lenalidomide/dexamethasone] with or without transplantation, particularly in this pilot, focusing on three cycles of IRd followed by [cyclophosphamide] mobilization, melphalan 200 mg/m2 and transplant, two cycles of IRd consolidation, then six cycles of ixa/lenalidomide without dexamethasone, and then ixazomib maintenance. And those data have been reported on and showed responses.
IRd Induction/Consolidation → Ixazomib Maintenance Responses Per Protocol1
Response, % Post-Induction (n = 42)
Post-ASCT (n = 37)
Post–Early Consolidation
(n = 37)
Post–Late Consolidation
(n = 34) sCR 2.4 9.5 23.8 38.2 CR 9.5 7.1 4.8 5.9
VGPR 23.8 45.2 38.1 32.4
PR 42.9 21.4 19 17.6
SD 14.3 4.8 0 0
PD 4.8 0 2.4 5.9
NE 2.4 11.9 11.9 0
>PR 81 83.3 85.7 94.1
>VGPR 38.1 61.9 66.7 76.5
>CR 11.9 16.7 28.6 44.1
1. Moreau P et al. ASH 2016. Abstract 674.
The CR rate was about 38% post–late consolidation. The VGPR or better rate was about 32% post–late consolidation, suggesting that, at least from this analysis from the French group, the depth of response with the weekly dose of ixazomib may not have been quite as deep as they would have liked. But certainly, they are continuing to pursue this now with a twice-a-week ixazomib induction in the original induction therapy cycles.
IRd Safety Summary and Example for AE Management1,2
Hematologic Events • Thrombocytopenia • Neutropenia
Nonhematologic Events Also Noted •Skin and subcutaneous tissue disorders •Peripheral neuropathy •Cardiac issues—atrial fibrillation •Thrombosis
Example: Managing Hematologic Events (Thrombocytopenia) in Pts on IRd Withhold ixazomib and lenalidomide until platelet count is ≥30,000/mm3 Post-recovery: Resume lenalidomide at next lower dose; resume ixazomib at
most recent dose If platelet count falls to <30,000/mm3 again, withhold regimen until platelet
count ≥30,000/mm3 Post-recovery: Resume ixazomib at next lower dose, resume lenalidomide at
most recent dosea
a For additional occurrences, alternate dose modification of lenalidomide and ixazomib. 1. Kumar SK et al. Lancet Oncol. 2014;15:1503-1512. 2. Moreau P et al. ASH 2016. Abstract 674.
Now, when you begin to look at adverse events, most of them are hematologic, with neutropenia and thrombocytopenia. Similar to bortezomib, peripheral neuropathy was noted, although it was seen in a low percentage of patients. And there were some skin rashes that were noted as well. Again, most of them were manageable and did not appear to be a significant issue beyond cycle 1 of therapy.

8 Go online to complete the post-test and evaluation for CME/CE credit
Translating Therapeutic Innovations Into the Management of Multiple Myeloma: Insights on Modern Practice Across Disease Settings
Ixazomib in Patients Not Proceeding to Transplant1
Patients with newly diagnosed MM
N = 65; cohort of 42 that did not proceed to
SCT
Weekly ixazomib (4 mg) plus Rd
Patients continuing on to receive single-agent
ixazomib (n = 25)
After Induction • ORR: 80% • CR + VGPR: 63% • CR: 32% • Median OS: NR • 4-y OS: 82%
After Maintenance • Increased depth of response
noted with ixazomib maintenance
• 32% of patients improved their response during maintenance
1. Kumar SJ et al. The 22nd European Hematology Association Congress (EHA 2017). Abstract S408.
Changed not reached to NR in Median OS
Now, what about looking at ixazomib and not proceeding to transplant? These are data presented by Dr. Kumar where he began to look at patients with newly diagnosed myeloma, 42 of whom did not proceed onto transplantation.
They received weekly ixazomib plus len/dex and showed an overall response rate of about 80%, VGPR or better rate of 63%, 32% CR, median overall survival not reached, with 82% still alive at 4 years, again, suggesting that for frail older patients, perhaps RVd-lite may not be the way to go. Replacing bortezomib with ixazomib, an oral agent, may be a kinder, gentler way to achieve the PI–IMiD combination for these patients in an all-oral regimen.
Efficacy of Antibody Therapy in Newly Diagnosed Myeloma: Daratumumab Regimens in MMY10011,2
0
1
2
3
4
5
6
VD +DARA(n = 6)
VMP +DARA (n
= 6)
VTD +DARA (n
= 6)
POM-D +DARA (n
= 6)
Patie
nts,
n
PD
MR
PR
VGPR
sCR
Daratumumab-KRd in Newly Diagnosed MM
12-mo PFS 94%
1. Mateos MV et al. ASH 2014. Abstract 176. 2. Jakubowiak A et al. ASCO 2017. Abstract 8000.
Best Response
Vd + Dara
(n = 6)
VMP + Dara
(n = 6)
VTd + Dara
(n = 6)
Pom/Dex + Dara (n = 6)
ORR was 100% in newly diagnosed group, 50% in the relapsed group
Now, everybody’s very excited about the use of daratumumab and other monoclonal antibodies in the induction therapy setting. At ASH and at ASCO and EHA, we did see data presented on daratumumab as part of the upfront regimen. This was a carfilzomib/len/dex/daratumumab in newly diagnosed myeloma.
The overall response rate was about 100%. Ninety-one percent achieved a VGPR or better, and the 12-month PFS was at about 94%. This was a very small abstract, about 21 patients, but certainly suggests that the addition of monoclonal antibodies to newly diagnosed myeloma is a very exciting new potential opportunity, and we just need longer follow-up and more patients to understand how to use this in our treatment approach.
Efficacy of Antibody Therapy in Newly Diagnosed Myeloma: Phase 2a RVd + Elotuzumab1
1. Laubach J et al. ASCO 2016. Abstract 8002.
• Longer follow-up needed in more patients to determine whether infections are attributable to addition of antibody
•
Response After 4 Cycles
82
95
70
Now, at the same time, Jacob Laubach presented data also on elotuzumab plus RVd. And this was another phase 2 study, again, with relatively short follow-up.
And what Jacob very nicely showed was an overall response rate of about 82%; among patients who went on to transplant, 95%; no transplant, it was about 70%. And patients appeared to tolerate this treatment relatively well, although there were two deaths in this study, one of which was likely associated with infectious complications.
We know infections in newly diagnosed myeloma are an issue. Whether those are attributable to the addition of the antibody or not I think is certainly difficult to understand right now. But I think it’s important for us, again, to also get longer follow-up in more patients treated with this combination to better understand how to use it.
www.peerviewpress.com/SGC900

9
Translating Therapeutic Innovations Into the Management of Multiple Myeloma: Insights on Modern Practice Across Disease Settings
• No prospective studies; patients can have an indolent course
Restarting Therapy and Prognostic Factors in Relapsed Myeloma1
Indications to Start Therapy
• CRAB features • Rapid rise in M protein • High levels of free light
chain with renal presentation
• High-risk cytogenetics with biochemical progression
Prognostic Factors
• Duration of initial response
• Acquisition of new abnormalities (1qamp, del17p)
• ISS/RISS • Performance status • Presence of EMD • Circulating plasma cells
1. http://imwg.myeloma.org/management-of-relapsed-multiple-myeloma-recommendations-of-the-international-myeloma-working-group/. Accessed July 18, 2017.
Dr. Lonial: So let’s switch gears a little bit and talk about management of early relapse. Unfortunately, as good as we are in the induction therapy and consolidation therapy approach, many patients will in fact relapse.
So when do we restart therapy? I think it’s important to understand that the Myeloma Working Group continues to suggest that patients with biochemical relapse do not necessarily need to start a salvage therapy immediately, and in fact, in many of them, they can be watched.
You can look at progression to CRAB features [calcium (elevated), renal failure, anemia, and bone lesions], although things that might push you to treat patients earlier are high levels of free light chain proteinuria or high levels of free light chain that may result in renal complications, high-risk genetics, performance status, circulating plasma cells, or a rapid rise in the M protein. These were all features that might suggest one needs to start therapy before the development of symptomatic myeloma.
New Developments in Pretreated Multiple Myeloma: Early Relapse
• Triplets preferred: RVd, VCd, or KRd, but at reduced doses; IRd, all oral regimen
• Doublets only in frail patients: Rd or Vd at reduced doses
Transplant Candidates (several cycles)
Transplant Ineligible (until progression)
• Triplets preferred: RVd or VCd; KRd if neuropathy
• Doublets: Rarely used (ie, Vd to improve renal dysfunction, then add lenalidomide)
• Maintenance: Lenalidomide in standard-risk patients; bortezomib or RV in high-risk patients
Summary of Initial Therapy for Newly Diagnosed Myeloma
So, in summary, for the newly diagnosed approach, I think it’s pretty clear that triplets represent the standard approach for almost all patients now. The RVd IMiD–PI combination has likely become the standard. VCd, or cyclophosphamide in combination with bortezomib and dexamethasone, is likely a suboptimal option. If RVd is not something that you want to be able to use or you can’t use because of access, VTd [bortezomib/thalidomide/dexamethasone] might be an alternative approach.
The use of carfilzomib and lenalidomide and dexamethasone is being evaluated in ongoing studies, and there are in fact randomized phase 3 trials looking at carfilzomib/len/dex versus bortezomib/len/dex in a phase 3 trial through the ECOG group.
Doublets are rarely used. Maintenance therapy continues to be an important part of treatment. Lenalidomide for standard risk; more complicated, either bortezomib or bortezomib/lenalidomide in high-risk patients is important.
Then again, for transplant-ineligible, triplets again are the primary choice. But if they can’t be delivered, then doublets with treatment until progression are important.

10 Go online to complete the post-test and evaluation for CME/CE credit
Translating Therapeutic Innovations Into the Management of Multiple Myeloma: Insights on Modern Practice Across Disease Settings
New Wave of Therapies Recognized by the NCCN (Early Relapse)1
Category 1 Recommendation in Previously Treated Myeloma for Next-Generation Therapies
Indication
Carfilzomib + dexamethasone Carfilzomib + lenalidomide/dexamethasone Patients receiving 1-3 prior therapies
Daratumumab + boretezomib or lenalidomide and dexamethasone
Patients with MM who have received ≥1 prior therapy
Elotuzumab + lenalidomide/dexamethasone Patients receiving 1-3 prior therapies
Ixazomib + lenalidomide/dexamethasone Patients with MM who have received ≥1 prior therapy
Pomalidomide + dexamethasone
Patients receiving ≥2 prior therapies including lenalidomide and a PI with
disease progression on or within 60 days of completion of the last therapy
1. National Comprehensive Cancer Network (NCCN) Clinical Oncology Guidelines. Multiple Myeloma. Version 3.2017.
And as you can see, there is a new wave of treatments available for patients in the early relapse setting, including carfilzomib, daratumumab, elotuzumab, ixazomib, and pomalidomide, as well as combinations with many of these other regimens going forward.
Pomalidomide-Based Doublets: Phase 3 MM-003 Trial1
Primary Endpoint: PFS Safety and MM-003 Summary
• Most common grade 3/4 events: neutropenia, anemia, and thrombocytopenia
• ≥ Grade 3 PN in 15% with pom/LD dexamethasone vs 11% with HD dexamethasone
• Pom/LD dexamethasone is an option for advanced RRMM, including in patients who have failed bortezomib and lenalidomide
Median PFS Pom/LD dex: 4.0 mo HD dex: 1.9 mo HR = 0.48 (P < .0001)
100
80
60
40
20
0
Patie
nts,
%
Months
1. San Miguel J et al. Lancet Oncol. 2013;14:1055-1066.
0 2 4 6 8 10 12 14 16 18 1 3 5 7 9 11 13 15 17
Now, what are the data that gave us pomalidomide-based doublets? This was the MM-003 trial. This was pom/dex versus dexamethasone, a trial that could not be done in the United States, and demonstrated a significant improvement in PFS as well as overall survival, favoring the use of pomalidomide in the relapse setting.
• Early recognition, management to avoid infections and treatment interruption
Managing IMiD-Related Myelosuppression
Example: Neutropenia Management in Myeloma Pts Receiving Pomalidomide1
1. Pomalyst (pomalidomide) Prescribing Information. http://www.pomalystrems.com/pdf/POM_Full_PI.pdf. Accessed June 30, 2017.
When Neutrophils Recommendation
Fall to <500 per mcL or febrile neutropenia (fever ≥38.5˚ C and ANC <1,000 per mcL) ANC return to ≥500 per mcL
Interrupt treatment, follow CBC weekly Resume treatment at 3 mg/d
For each subsequent drop to <500 per mcL Return to ≥500 per mcL
Interrupt treatment Resume treatment at 1 mg < previous dose
Now, what about management of some of the adverse events associated with pomalidomide? Myelosuppression is likely the most common one that we see, and management of myelosuppression is recommended in the package insert for pomalidomide. These are relatively standard. The use of either dose reduction or growth factor support I think represents alternative ways to get to this endpoint [ie, improvement in ANC to normal limits].
ENDEAVOR: Carfilzomib/Dexamethasone Versus Bortezomib/Dexamethasone1
464 144 0 41 4 331 No. at Risk Carfilzomib grp Bortezomib grp 465 81 0 12 1 252
0
100
80
60
20
40
0 12 30 18
PFS,
%
24 6
Carfilzomib group Bortezomib group
HR = 0.53 (95% CI, 0.44-0.65) P < .0001
a Used a higher dose of carfilzomib (56 mg/m2). 1. Dimopoulos MA et al. Lancet Oncol. 2016;17:27-38.
Carfilzomib Groupa
(n = 464) Bortezomib Group
(n = 465) Median PFS (95% CI), mo 18.7 (15.6-NE) 9.4 (8.4-10.4)
Months
The ENDEAVOR trial was a large randomized phase 3 trial comparing carfilzomib and dexamethasone versus bortezomib and dexamethasone. And while this was bortezomib/dex at standard dosing, this was car/dex at 56 mg/m2. This is a higher dose of carfilzomib, and in fact, this higher dose is clearly more potent than bortezomib, as evidenced by a pretty significant improvement in progression-free survival.
www.peerviewpress.com/SGC900

11
Translating Therapeutic Innovations Into the Management of Multiple Myeloma: Insights on Modern Practice Across Disease Settings
ASPIRE: KRd1
0
0.2
0.4
0.6
0.8
1.0
48 0 6 12 24 30 36 42 Months Since Randomization
Prop
ortio
n Su
rviv
ing
W
ithou
t Pro
gres
sion
18
HR = 0.69 (0.57-0.83)
0
0.2
0.4
0.6
0.8
1.0
48 0 6 12 24 30 36 42 Months Since Randomization
Prop
ortio
n Su
rviv
ing
18
HR = 0.79 (0.63-0.99) P = .04 P = .0001
Median PFS KRd: 26.3 mo Placebo/Rd: 14.7 mo
1. Stewart AK et al. N Engl J Med. 2015;372:142-152.
KRd Placebo/Rd
Now, if you begin to look at the triplet versus doublet question, Keith Stewart published this paper a few years ago, the ASPIRE trial, looking at carfilzomib/len/dex versus len/dex. And again, as you can see here, median PFS is 26.3 months versus 14.7 months, a significant difference. And if you begin to look at survival, there are suggestions that the survival curves are disparate. We don’t know that for certain, although hopefully in the next year or so we will see longer follow-up and understand whether those survival curves did in fact differentiate and continue to stay separate over time.
Ixazomib/Dexamethasone1
≥100
50
0
-100
-50
At least 25% increase
At least 25% decrease
Perc
ent C
hang
e
Arm A—4 mg (n = 35)
Arm B—5.5 mg (n = 35)
ORR, % 31 54 Median EFS, mo 8.4 7.8 Median DOR, mo 16.7 16.3 Median time to response, mo 1.1 1.0
1. Kumar SK et al. Blood. 2016;128:2415-2422.
These were data from the early trials in phase 1 in relapsed and refractory myeloma showing waterfall plots of the single-agent activity or the activity of ixazomib in combination with dexamethasone.
TOURMALINE-MM1: IRd PFS Summary1
1.0
0.8
0.6
0.4
0.2
0 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
Prob
abili
ty o
f PFS
Months Since Randomization
Log rank P = .012 HR = 0.742 (95% CI, 0.587-0.939) No. of events: IRd = 129; placebo/Rd = 157
Median follow-up: ~15 mo
Median PFS IRd: 20.6 mo Placebo/Rd: 14.7 mo
1. Moreau P et al. Blood. 2015;126:727.
And this then gave rise to the TOURMALINE-MM1 trial. This is ixazomib/len/dex versus lenalidomide and dexamethasone, showing a significant improvement in progression-free survival—20 months versus 14 months—for the group randomized to ixazomib.
TOURMALINE: PFS Stratified by Risk1
Patients by Cytogenetic Status
Median PFS, mo HR
IRd Placebo/Rd All (N = 722) 20.6 14.7 0.742 Standard risk (n = 145) 20.6 15.6 0.640 High risk (n = 137) 21.4 9.7 0.543 Del(17p)a 21.4 9.7 0.596 t(4;14) alone (n = 61) 18.5 12.0 0.645
a Alone or in combination with t(4;14) and/or t(14;16). 1. Richardson PG et al. ASCO 2016. Abstract 8018.
PFS in High- and Standard-Risk Patients PFS in High
And more importantly, it suggested that in patients with high-risk cytogenetics, the addition of ixazomib could overcome almost completely that negative impact on progression-free survival. If we begin again to look at stratified PFS by risk, you can see across the board the PFS is between 20 and 21 months for the group randomized to ixazomib.
This I think is really important and does in fact suggest that the use of ixazomib, similar to what we know about bortezomib and carfilzomib, is a reasonable strategy for high-risk myeloma.

12 Go online to complete the post-test and evaluation for CME/CE credit
Translating Therapeutic Innovations Into the Management of Multiple Myeloma: Insights on Modern Practice Across Disease Settings
Phase 3 Studies of Daratumumab Combinations in Patients Receiving ≥1 Prior Line of Therapy1
DRd (n = 286) Daratumumab 16 mg/kg IV • Every week: cycles 1-2 • Every 2 weeks: cycles 3-6 • Every 4 weeks until PD Lenalidomide 25 mg PO (similar to Rd
alone) Dexamethasone 40 mg
Rd (n = 283) Lenalidomide 25 mg PO • Days 1-21 of each cycle until PD Dexamethasone 40 mg weekly until PD
R A N D OM I Z E
POLLUX DVd (n = 251)
Daratumumab 16 mg/kg IV • Every week: cycles 1-3 • Every 3 weeks: cycles 4-8 • Every 4 weeks: cycles 9+ Bortezomib 1.3 mg/m2 subQ (similar to
Vd alone) Dexamethasone 20 mg
Vd (n = 247) Bortezomib 1.3 mg/m2 subQ on days 1,
4, 8, and 11 for 8 cycles Dexamethasone 20 mg on days 1, 2, 4,
5, 8, 9, 11, and 12 for 8 cycles
CASTOR
R A N D OM I Z E
MRD Assessments • At suspected CR • 3 and 6 mo after CR
MRD Assessments • At suspected CR • 6 and 12 mo after first study dose
Patient Characteristics • Median (range) prior lines: 1 (1-11) • Prior bortezomib: 84% • Prior lenalidomide: 18%
Patient Characteristics • Median (range) prior lines: 2 (1-10) • Prior bortezomib: 66% • Prior lenalidomide: 42%
1. Avet-Loiseau H et al. 58th American Society of Hematology Annual Meeting and Exhibition (ASH 2016). Abstract 246.
Next we’ll talk about monoclonal antibodies: the phase 3 studies of daratumumab in combination with either len/dex in the POLLUX trial or bortezomib/dex in the CASTOR trial. Again, the trial designs were almost identical between the two. And these are the trials that led to the FDA approval of bortezomib and lenalidomide in combination with daratumumab.
n Median PFS, mo DRd group 286 NE
Rd group 283 18.4
Efficacy and safety in elderly patients was similar to that of the overall population in both trials3
POLLUX and CASTOR: PFS
POLLUX: 12-mo PFS1
0
20
40
60
80
100
21 0 3 6 9 12 15 18 Months
PFS,
% 83.2 (95% CI, 78.3-87.2)
DRd group
Rd group
60.1 (95% CI, 54.0-65.7) HR for progression or death = 0.37 (95% CI, 0.27-0.52) P < .001
1. Dimopoulos MA et al. N Engl J Med. 2016;375:1319-1331. 2. Lentzsch S et al. ASCO 2017. Abstract 8036. 3. Mateos MV et al. ASCO 2017. Abstract 8033.
Median PFS, mo DVd Group (n = 251)
Vd Group (n = 247)
All patients 16.7 7.1 1 prior therapy NE 7.9 2-3 prior therapies 9.8 6.3
CASTOR: 18-mo PFS2 CASTOR: 18-mo PFS2
And what we see is a significant improvement in PFS for both treatment arms. With longer follow-up, the difference in progression-free survival is not going away. In fact, it does appear that that PFS is being maintained in the daratumumab arm, and it suggests that this is actually really important for patients not just in the short term, but also in the long term.
• Percent of MRD-negative patients among those who achieved ≥CR
MRD Negativity in Daratumumab Combination Studies1
CASTOR
ITT
Popu
latio
n, %
0
5
10
15
25
20
DVd Vd 10-4
DVd Vd DVd Vd 10-5 10-6
60
35
37
22 16
9
b
MRD negative MRD positive
POLLUX
ITT
Popu
latio
n, %
0
10
20
30
40
DRd Rd 10-4
MRD negative MRD positive
DRd Rd DRd Rd 10-5 10-6
65
42
52
27 26
13
a b a
a P < .005. b P < .05. 1. Avet-Loiseau H et al. ASH 2016. Abstract 246.
If we begin to look at the fraction of patients that could even begin to achieve MRD negativity—in the center of both of those figures 10-5 and to the right side 10-6—those are the two MRD endpoints that I think are meaningful. A majority of patients that achieve these levels of MRD negativity did so with the addition of daratumumab. Very rarely did it occur with lenalidomide and dexamethasone alone.
Daratumumab + Pomalidomide/Dexamethasone in Relapsed/Refractory Myeloma: EQUULEUS1
• N = 103 patients with MM and prior treatment with a PI and an IMiD
• Median age = 64 y; 8% of patients ≥75 y
Patients in pomalidomide/
dexamethasone arm
• Daratumumab at 16 mg/kg combined with pomalidomide/dexamethasone Dose
Response %
VGPR 28
CR 6
sCR 8
June 2017 Daratumumab approved for use in combination with pomalidomide and dexamethasone for patients with MM who have received ≥2 prior therapies, including a PI and lenalidomide
1. Chari A et al. Blood. 2017 Jun 21. [Epub ahead of print].
Now, just in the last few months, we’ve seen data on the daratumumab plus pomalidomide trial, with a VGPR or better rate of 28%, CR rate of 6%, stringent CR rate of 8%. This has been presented by Dr. Chari and is now in press in Blood.
But more importantly, the FDA identified these data in 103 patients and actually approved pomalidomide in combination with daratumumab based on this very exciting and encouraging phase 2 clinical trial—suggesting that for patients who have been exposed to lenalidomide, as in the POLLUX trial, replacing lenalidomide with pomalidomide and adding in daratumumab might be a reasonable salvage regimen.
www.peerviewpress.com/SGC900

13
Translating Therapeutic Innovations Into the Management of Multiple Myeloma: Insights on Modern Practice Across Disease Settings
ELOQUENT-2: Phase 3 Study of ERd in Previously Treated Myeloma1
1. Lonial S et al. ASCO 2017. Abstract 8028.
HR = 0.71 (95 % CI, 0.59-0.86)
P = .0004
ERd Rd Median PFS 19.4 mo 14.9 mo
95% CI 16.6-22.3 12.1-17.3
4-Year Update: PFS in All Randomized Patients
No. at Risk ERd 321 304 280 260 233 216 196 180 160 147 132 125 111 103 94 91 79 70 63 60 55 52 49 46 36 31 24 17 13 6 2 0 Rd 325 295 249 216 192 173 158 141 124 108 91 76 68 64 61 54 47 41 39 37 33 31 30 27 22 13 19 6 3 1 1 0
Median PFS95% CI
No. at Risk
So let’s look at the other monoclonal antibody that’s in the approval window. That’s elotuzumab. This was an update with the 4-year data that I presented at ASCO this year. Three-year, 4-year follow-up with median progression-free survival continuing to favor the group that received elo/len/dex versus lenalidomide and dexamethasone, with the same magnitude of difference that we saw at the initial 2-year follow-up.
ELOQUENT-2: Response and Survival Outcomes1
ERd Rd
Median OS 48.3 mo 39.6 mo
95% CI 40.3-54.4 33.3-45.4
HR = 0.78 (95% CI, 0.63-0.96)
ERd Rd Median DOR 21.2 mo 16.8 mo
95% CI 18.4-25.8 14.9-19.4
HR = 0.77 (95% CI, 0.62-0.95) P = .0176
a OS analysis was not prespecified at 4-y follow-up. 1. Lonial S et al. ASCO 2017. Abstract 8028.
ORR and Best Overall Response
Overall Survival
No. at Risk ERd 321 316 308 303 296 288 283 270 264 250 242 236 224 221 210 197 192 187 181 178 170 163 155 150 132 93 64 42 24 10 4 2 0 Rd 325 312 298 287 278 264 255 243 237 228 222 213 208 202 193 184 174 164 158 154 147 141 137 128 109 80 53 30 13 7 3 0 0
ORR and Best Overall Response
No. at RiskERd 321 316 308 303 296 288 283 270 264 250 242 236 224 221 210 197 192 187 181 178 170 163 155 150 132 93 64 42 24 10 4 2 0
The response rate continues to be superior. And in fact, if you look at the survival curve, the hazard ratio is 0.78, favoring the group that received elo/len/dex. We don’t have a P value on that difference as yet, but we’re hoping to have a P value in the next 12 to 24 months that will show us that what we’re seeing in terms of PFS is in fact bearing out, and is likely very important.
• ASCO 2017: Isatuximab in combination with pom/dex, ORR of 67%2
• Phase 3 isatuximab plus pom/dex planned (ICARIA-MM, NCT02990338)
Isatuximab: Anti-CD38 Monoclonal Antibody
Modes of Action of Isatuximab1
1. Richardson P et al. ASH 2016. Abstract 2123. 2. Mikhael J et al. ASCO 2017. Abstract 8007.
Now, there are other CD38 antibodies that are in development. The one that I want to spend just a moment talking about is isatuximab. This is another anti-CD38 monoclonal antibody that has similar mechanisms of action to what you see with daratumumab, and in fact has a similar mechanism and response rate when combined with pomalidomide and dexamethasone. Those data were presented at ASCO this year.
Daratumumab Combinations: Similar Safety Profile Across Phase 3 Trials
POLLUX (+ Lenalidomide/Dexamethasone)1
Most common grade 3/4 AEs included: • Neutropenia (51.9% vs 37.0%) • Thrombocytopenia (2.7% vs 13.5%) • Anemia (12.4% vs 19.6%) Daratumumab-associated infusion-related reactions occurred in 47.7% (mostly grade 1 or 2)
CASTOR (+ Bortezomib/Dexamethasone)2
Most common grade 3/4 AEs included: • Thrombocytopenia (45.3% and
32.9%) • Anemia (14.4% and 16.0%) • Neutropenia (12.8% and 4.2%)
Infusion-related reactions in 45.3% of the patients in the daratumumab group (mostly grade 1 or 2)
1. Dimopoulos MA et al. N Engl J Med. 2016;375:1319-1331. 2. Palumbo A et al. N Engl J Med. 2016;375:754-776.
Now, what about safety profiles for daratumumab? This is a similar safety profile across phase 3 trials. You can see the frequency of infusion-related reactions, which really is the major issue that seems to come up, is relatively low and tends to occur in the first two doses of daratumumab, mostly grade 1/grade 2. It does occur in about 45% of patients across the board.

14 Go online to complete the post-test and evaluation for CME/CE credit
Translating Therapeutic Innovations Into the Management of Multiple Myeloma: Insights on Modern Practice Across Disease Settings
• Daratumumab can bind to RBCs and interfere with allo-antibody screening for transfusion by causing positive indirect anti-globulin testing1
Daratumumab and Blood Compatibility Testing
DTT abolishes the binding of daratumumab to RBCs2
International effort underway to validate the
use of DTT for daratumumab-treated
patients globally3
1. Hoffmeister CC, Lonial S. J Clin Oncol. 2016;34:4421-4430. 2. Chapuy CI et al. Transfusion. 2015;55:1545-1554. 3. Chapuy CI et al. ASH 2015. Abstract 3567.
The other thing to be aware of with daratumumab is issues with blood compatibility testing. Daratumumab—because there is CD38 expression on red blood cells—does bind red blood cells and can cause a false-positive indirect Coombs test. There is a DTT assay that can be done to eliminate the daratumumab from the red blood cells in the blood bank to allow for typing and crossing to occur in an efficient manner, but your blood bank needs to know that this is coming.
So we’ve recommended now that most folks let their blood bank know and do a type and screen prior to the first dose of daratumumab, and then let them know that if the patient needs blood anytime in the future to be sure to use the DTT assay to mitigate the complications associated with that.
Managing Infusion Reactions With Antibody Therapy in Myeloma1
Acetaminophen 325 mg Diphenhydramine 25 mg Dexamethasone 20 mg IV
Montelukast 10 mg PO Famotidine 20 mg IV
Acetaminophen 325 mg Dexamethasone 20 mg IV
Diphenhydramine 25 mg IV
Acetaminophen 650 mg Diphenhydramine 50 mg Dexamethasone 20 mg IV
Famotidine 20 mg IV
Daratumumab 16 mg/kg (in 500 mL) starting at
100 mL/h and increasing by 50 mL/h to a maximum
of 200 mL/h
Elotuzumab 10 mg/kg (in 250 mL) starting at
30 mL/h up to a maximum of 120 mL/h
Daratumumab 16 mg/kg (in 1,000 mL) starting
at 50 mL/h and increasing by 50 mL/h to a maximum of 200 mL/h
Daratumumab Elotuzumab
All infusions First Infusions Subsequent Infusions
1. Hoffmeister CC, Lonial S. J Clin Oncol. 2016;34:4421-4430.
What about managing infusion reactions with antibody therapy in myeloma? This is a nice little table from a paper that Craig Hoffmeister and I wrote in the Journal of Clinical Oncology about a year ago where we show our recommendations.
Again, you can see, these are relatively straightforward. We’ve found at our center that the use of montelukast, a leukotriene inhibitor, does have a significant impact on reducing the risk of infusion reactions over time.
www.peerviewpress.com/SGC900

15
Translating Therapeutic Innovations Into the Management of Multiple Myeloma: Insights on Modern Practice Across Disease Settings
Novel Agents in Heavily Pretreated or Refractory Multiple Myeloma
…including in patients exposed to multiple novel therapies?
What Agent Classes Have Shown Activity in Heavily Pretreated or Refractory Myeloma…
Anti-CD38 antibodies (daratumumab)
HDAC inhibitors (panobinostat)
Immune checkpoint inhibitors (pembrolizumab); CAR T cell
XPO1 inhibitors (selinexor)
Looking at novel agents in heavily pretreated or refractory multiple myeloma, again we have CD38 antibodies, daratumumab; HDAC inhibitors, panobinostat; immune checkpoint inhibitors, such as pembrolizumab, as well as other targets, including BCMA and CAR T cells; and finally XPO1, or selinexor.
18%
10%
1% 2%
0
5
10
15
20
25
30
35
16 mg/kg
OR
R, %
sCRCRVGPRPR
ORR = 31%
Daratumumab: SIRIUS and GEN501 Pooled Analysis1
13% VGPR or better
n (%) Overall response rate (sCR + CR + VGPR + PR) 46 (31)
Best response sCR CR VGPR PR MR
3 (2) 2 (1)
14 (10) 27 (18) 9 (6)
VGPR or better (sCR + CR + VGPR) 19 (13)
CR or better (sCR + CR) 5 (3)
• N = 148
1. Usmani SZ et al. Blood. 2016;128:37-44. 2. Nooka A et al. 58th American Society of Hematology Annual Meeting and Exhibition (ASH 2016). Abstract 492.
Consider using daratumumab in combinations, particularly with IMiDs, as the IMiD may augment the antimyeloma efficacy of daratumumab2
So if we look at the pooled analysis of daratumumab from the SIRIUS trial as well as the GEN501 trial, we can see that the overall response rate in refractory myeloma is about 31%, with about 13% of those patients achieving VGPR or better.
Now, those are data that we know about and have been used for a long period of time. But many patients are continuing to receive daratumumab as a single agent. But as I would encourage you to do, use daratumumab in combinations, particularly with IMiDs, because even if a patient is resistant to an IMiD, the IMiD may augment the antimyeloma efficacy of daratumumab.
HDAC Inhibitors: Panobinostat Regimens in Myeloma1
Panobinostat Bortezomib
Dexamethasone
Patients who have received ≥2 prior regimens, including
bortezomib and an IMiD
Panobinostat Carfilzomib
Panobinostat Cyclophosphamide
Dexamethasone
Patients who have received ≥2 prior
regimens, including IMiD and a PI, and who have disease progression on or
within 60 days of completion of
last therapy
1. National Comprehensive Cancer Network (NCCN) Clinical Oncology Guidelines. Multiple Myeloma. Version 3.2017.
Now, what about HDAC inhibitors? We know that panobinostat has been tested with bortezomib. There are also data with panobinostat with carfilzomib, and data with panobinostat and cyclophosphamide and dexamethasone.
Panobinostat in Double-Refractory Disease1
1. Richardson PG et al. Blood. 2016;127:713-721.
Events Median PFS (95% CI), mo
HR (95% CI)
Pan-Vd 44/73 12.5 (7.3-14.0) 0.47 (0.31-0.72) Placebo-Vd 54/75 4.7 (3.7-6.1)
PFS Among Patients Who Received ≥2 Prior Regimens Including Bortezomib and an IMiD Agent
Events Median PFS (95% CI), mo
HR (95% CI)
Pan-Vd 44/73 12.5 (7.3-14.0) 0.47(0.31-0.72)Placebo-Vd 54/75 4.7 (3.7-6.1)
These are the data that led to the FDA approval for panobinostat in combination with bortezomib and dex, particularly in a highly relapsed and refractory patient population, showing a more than tripling of the PFS with panobinostat/bortezomib/dex versus bortezomib and dexamethasone.
From a practical perspective, sometimes that regimen can be more challenging to give. We find that in many situations, partnering with carfilzomib is a little bit easier, as the GI toxicity seems to be a little bit lower.

16 Go online to complete the post-test and evaluation for CME/CE credit
Translating Therapeutic Innovations Into the Management of Multiple Myeloma: Insights on Modern Practice Across Disease Settings
Rationale for PD-1 Blockade in Myeloma1
1. Sznol M and Chen L. Clin Cancer Res. 2013;19:1021-1034.
PD-1 + IMiDs likely restore MM-specific
cytotoxic T cells, resulting in clinically relevant responses
PD-1 + IMiDs likely restore MM-specific
cytotoxic T cells, resulting in clinically relevant responses
Now, what about PD-1 in myeloma? We know that PD-1 alone does not have a significant efficacy signal, but as we’ve learned in pretty much every other disease in cancer, PD-1 certainly is important as we begin to think about immunotherapy in patients with myeloma. So, while PD-1 alone may not be the answer, combining PD-1 may certainly be important. And the best partner for PD-1, from what we know so far, is the IMiD molecules, likely because the IMiDs activate T cells, activate NK cells, and generally rev up immune function.
Pembrolizumab + Pomalidomide/Dexamethasone in Relapsed/Refractory Myeloma1
Pembrolizumab 200 mg IV First 6 patients treated on day 1 only
Dexamethasone 40 mg orally 20 mg for patients aged >70 y
Pomalidomide 4 mg orally
Day 1 Day 21 Day 14 Day 7
Response Evaluable (n = 45)
Double Refractory (n = 32)
High-Risk Cytogenetics (n = 27)
ORR, n (%) 29 (65) 22 (68) 15 (56)
Clinical benefit, n (%) 32 (72) 23 (69) 16 (60)
sCR, % 7 3 7
CR, % 2 3 4
sCR + CR + VGPR, % 29 24 15
1. Badros AZ et al. ASH 2016. Abstract 490.
Now, Ashraf Badros presented and has now published, in Blood, data combining pembrolizumab with pomalidomide and dexamethasone in relapsed and refractory myeloma. What he showed very nicely was an overall response rate of about 65%, clinical benefit rate of about 72%, VGPR or better rate of about 29%. These were all patients who were pomalidomide sensitive.
• Median PFS: ~17 mo
Duration of Response With Pembrolizumab + Pomalidomide/Dexamethasone1
1. Badros AZ et al. ASH 2016. Abstract 490.
Some of those patients could actually go on to be on treatment for a long period of time. And in fact, in this trial, the median progression-free survival was almost 17 months. And that 17 months is much longer than you’d expect with pom/dex in that same indication where the median PFS would be about 3 months.
So 17 months suggests that there clearly are some immune-mediated effects that are occurring, both with the pomalidomide and the PD-1–targeting agent pembrolizumab.
Pembrolizumab + Pomalidomide/Dexamethasone in Relapsed/Refractory Myeloma1
Safety summary: frequent but manageable
1. Badros AZ et al. ASH 2016. Abstract 490.
Safety summary: frequent but manageable
1. Badros AZ et al. ASH 2016. Abstract 490.
And we know that’s also the case, because if you begin to look at adverse events, we did see some PD-1–related adverse events, including rash, pneumonitis, and diarrhea.
Now, most of the pneumonitis was in similar frequency to what’s been seen in other PD-1–based trials. Many of the patients who were thought to have pneumonitis may have had infectious pneumonia, and in fact, one of the patients who had grade 3 pneumonitis actually continued on pembrolizumab. And we know, from our lung cancer colleagues, that patients who develop grade 3 pneumonitis that’s true autoimmune in nature have to discontinue pembrolizumab.
www.peerviewpress.com/SGC900

17
Translating Therapeutic Innovations Into the Management of Multiple Myeloma: Insights on Modern Practice Across Disease Settings
So some of this may have been the effect of infections that we know are an issue in myeloma, but there likely were some autoimmune phenomena as well.
Response, n (%) Evaluable (n = 17)
Lenalidomide Refractory
(n = 9) ORR 13 (76) 5 (56) VGPR 4 (24) 2 (22) PR 9 (53) 3 (33)
Pembrolizumab + Lenalidomide Combinations Also Explored in Relapsed/Refractory Myeloma1
KEYNOTE-023: Activity of Pembrolizumab + Rd in RRMM
• Multiple trials are assessing agents targeting the PD-1 axis in MM; recently, two phase 3 studies evaluating the combination of pembrolizumab and IMiDs were placed on hold due to safety concerns2
1. San Miguel J et al. ASH 2015. Abstract 505. 2. http://www.ascopost.com/News/57813. Accessed August 14, 2017.
Now, there were also data presented by the Spanish group on pembrolizumab in combination with lenalidomide. And again, you can see the overall response rate of about 76%.
But what was unique about this trial was they treated len-refractory patients as well. And what they demonstrated was that about a third to a half of len-refractory patients would respond to len plus pembrolizumab, suggesting again that the IMiD–PI combination is very powerful, even if the patient’s myeloma is resistant to an IMiD. So these combinations are being tested in phase 3 trials.
Narrator: Recently, the pembrolizumab–IMiD combination trials were put on hold by the US FDA due to safety concerns, and further analyses are pending. Trials combining an IMiD with another PD-1 inhibitor, nivolumab, are ongoing, but no signals have been noted to date.
• AEs manageable; ocular toxicity
most frequent reason for dose modifications
• 66.7% ORR including a stringent CR observed at higher doses of GSK2857916 in this refractory population
• 3.4 mg/kg selected as the dose to investigate in the expansion phase of current study
Targeting BCMA in Myeloma With Antibody–Drug Conjugates1
GSK2857916: Humanized, afucosylated IgG1 anti-BCMA antibody recently tested in relapsed/refractory myeloma
1. Cohen AD et al. ASH 2016. Abstract 1148.
• Target specific • Enhanced ADCC
Fc region of
antibody
• Stable in circulation Linker
• MMAF (non–cell permeable, highly potent auristatin)
Drug
toxicity frequent reason for dose
stringent CR observed at higher doses of GSK2857916 in this
as the dose to investigate in the expansion
GSK2857916: Humanized, afucosylated IgG1 BCMA antibody recently tested in
relapsed/refractory myeloma
• Target specific• Enhanced ADCC
Fc region Fc region of of of
antibodyantibodyantibodyantibody
• Stable in circulationcirculationLinkerLinker
Dr. Lonial: Now, what about BCMA? We know that BCMA makes a lot of sense as a target. It’s probably the most narrowly defined target in myeloma, present almost only on plasma cells. And we know that there are many ways to get to BCMA.
What we have interesting data on at this time point is the anti-BCMA antibody–drug conjugate, which were presented by Adam Cohen at ASCO. And what he demonstrated quite nicely was that there were responses seen at the highest dose level of about 60%, suggesting this was an active drug. And many patients are looking forward to trying to get onto that drug as we go forward.
bb2121 Survival and Tumor Clearance in MM Mice2
bb2121: Anti-BCMA Chimeric Antigen Receptor T-Cell Product Candidate1,2
Autologous T cells transduced with a lentiviral vector encoding a novel anti-BCMA CAR • 4-1BB co-signaling motif
selected to promote proliferation and persistence
• Construct demonstrated potent preclinical in vivo activity with low tonic signaling
a No dose-limiting toxicities yet identified, and dose escalation continues. 1. Berdeja J et al. European Organisation for Research and Treatment of Cancer, the National Cancer Institute, and the American Association for Cancer Research 2016 Symposium (EORTC-AACR-NCI 2016). Abstract 14LBA. 2. Morgan LM et al. 24th Anniversary Congress of the European Society of Gene and Cell Therapy (ESGCT 2016).
• bb2121 demonstrated substantial anti-tumor activity in heavily pretreated patients with MM – ORR of 100% (15/15) in patients treated at 3 highest dosing levels (doses >50 x 106)
• bb2121 was well tolerated, with mild to moderate CRS reported to datea • Dosing escalation and expansion will continue to identify recommended phase 2 dose
0
Tum
or V
olum
e, m
m3
1,000
0
2,000
3,000
4,000
20 40 60 80 Days
Surv
ival
, %
20
0
40
80
100
20 40 60 100
60
80 0 Days
Anti-BCMA CAR Bortezomib Control CAR T Vehicle
We also know that the anti-BCMA CAR T cell is also very exciting. There were data presented at ASCO and EHA on a couple of different BCMA and anti-CAR T cells.
bb2121 is probably the one with the most data. And what we know about bb2121 is that there were significant responses. Fifteen of 15 patients at the highest dose level had a response. It appeared to be tolerated relatively well, with rare cytokine release syndrome. And expansion cohorts are currently ongoing.
But there are three or four other BCMA-targeted CAR T-cell programs that are currently in existence. And whether this represents the answer, or it’s part of the answer, at this time point I think remains unclear, but the data certainly look very encouraging.

18 Go online to complete the post-test and evaluation for CME/CE credit
Translating Therapeutic Innovations Into the Management of Multiple Myeloma: Insights on Modern Practice Across Disease Settings
• AEs included nausea, anorexia, GI events; manageable with supportive care measures (eg, antiemetics, appetite stimulants, GFS, thrombopoietin receptor agonists, salt supplementation)
Selinexor (XPO1 Inhibitor) in Heavily Pretreated Myeloma1
Category, n (%) n ORR CBR VGPR PR MR
Overall 78 16 (21) 26 (33) 4 (5) 12 (15) 10 (13)
Quad refractory 48 10 (21) 14 (29) 2 (4) 8 (17) 4 (8)
Penta refractory 30 6 (20) 12 (40) 2 (7) 4 (13) 6 (20)
6 doses/mo 51 10 (20) 15 (29) 3 (6) 7 (14) 5 (10)
8 doses/mo 27 6 (22) 11 (41) 1 (4) 5 (19) 5 (19)
Tested in Phase 2 STORM Trial Plus Low-Dose Dexamethasone for Heavily Pretreated Patients With MM Refractory to Most Recent Treatment
1. Vogl DT et al. ASH 2016. Abstract 491.
Selinexor is a first-in-class XPO1 inhibitor that works through a new mechanism. Data were presented at ASH this year from Dan Vogl, where he began to look at selinexor in quad- and penta-refractory patients. And basically, those are patients that have seen all the approved new drugs in myeloma. And what he demonstrated quite nicely was that the response rate in quad- and penta-refractory patients was about 20% PR or better. If you begin to look at clinical benefit or better, it goes up to 29% and 40% in quad- and penta-refractory.
In this patient population that was studied, that represents a pretty significant improvement in progression-free survival. And combinations of selinexor with dexamethasone, as well as selinexor in combination with bortezomib and/or carfilzomib, also represent future treatment options going forward.
Venetoclax (Bcl-2 Inhibitor): Efficacy1
0 2 4 6 8 10 12 14 16 18 20 22 24 0
25
50
75
100
Months Since First Dose
t(11;14) Non-t(11;14)
Time to Progression
All patients
Not
Pro
gres
sed,
%
Patie
nts,
%
0
10
20
30
40 sCR CR
3 4
8
6
4
10
13
13 3 3
VGPR PR
50
All Patients (N = 66)
t(11;14) (n = 30)
Non-t(11;14) (n = 36)
ORR 21%
ORR 40%
ORR 6%
• Phase 3 study of venetoclax plus bortezomib and dexamethasone in relapsed/refractory myeloma is ongoing2
1. Kumar S et al. ASH 2016. Abstract 488. 2. https://clinicaltrials.gov/ct2/show/NCT02755597. Accessed June 30, 2017.
No. at Risk 66 33 27 20 16 9 3 1 1 1 1 1 30 20 19 17 13 7 2 1 1 1 1 1 36 13 8 3 3 2 1
Now, the last of the new drugs I want to talk about is venetoclax. And for those of you who have been using venetoclax in CLL [chronic lymphocytic leukemia] and follicular lymphoma, this is not new information. But in myeloma, certainly, it does represent new information, because we may actually have a biomarker to predict who has a higher sensitivity for response.
Patients who are 11;14 translocation positive appear to have a much higher overall response rate than non-11;14. And if you look at this trial presented by Dr. Kumar at ASH, again, you can see an overall response rate of about 40% in the 11;14 group, and it’s only 6% in the non-11;14 group.
And this has gone on to a larger phase 2 study, suggesting that venetoclax plus dex has a very high overall response rate in the 11;14 group, and venetoclax plus bortezomib/dex has a very high overall response rate across all patients, whether or not they are 11;14 positive. And these data are now being tested in a randomized phase 3 trial.
• More options than ever before to treat myeloma patients
Summing Up the State of Therapy in Myeloma
Next-generation PIs/IMiDs rapidly moving into front-line care; antibodies are next
Triplet therapy
Antibodies (daratumumab); XPO1 inhibitors (selinexor); Bcl-2 inhibitors (venetoclax); checkpoint inhibitors (pembrolizumab); and CAR T cell immunotherapy
Novel classes
Doublets and triplets based on carfilzomib, ixazomib, pomalidomide, daratumumab, and elotuzumab
Newer therapeutics
In summary, it’s very clear that there are lots and lots of options, lots of treatment choices. It can in fact be confusing to decide what to do at any given point. There are a few benchmarks that I think all patients should try and achieve. And the first is, they should likely receive a triplet-based induction with an IMiD and a PI.
I would argue that RVd [lenalidomide/bortezomib/dexamethasone] is likely that standard, but there are others who would suggest KRd [carfilzomib/lenalidomide/dexamethasone] based on the encouraging data we’ve seen in phase 2 trials, or IRd [ixazomib/lenalidomide/dexamethasone] based on other encouraging data from phase 2 trials.
Transplant continues to have a role, as does maintenance therapy. Newer drugs, such as carfilzomib, ixazomib, daratumumab, elotuzumab, and pomalidomide are all important partners as we begin to think about early salvage therapy.
And finally, new targets, such as XPO1 inhibitors, checkpoint inhibitors, BCMA-targeted antibodies and CAR T cells and venetoclax all represent new targets for patients across the board as we begin to think about improving outcomes for patients in the long term. Thank you.
www.peerviewpress.com/SGC900

19
Translating Therapeutic Innovations Into the Management of Multiple Myeloma: Insights on Modern Practice Across Disease Settings

CME/CE
Translating Therapeutic Innovations Into the Management of Multiple Myeloma: Insights on Modern Practice Across Disease Settings
www.peerviewpress.com/SGC900
Sign up for e-mail alerts on new clinical advances and educational activities in your specialty: www.peerviewpress.com/signup
Copyright © 2000-2017, PeerView Press
This CME/CE activity is jointly provided by Penn State College of Medicine and PVI, PeerView Institute for Medical Education; this activity is also co-provided by Medical Learning Institute, Inc.
This activity is supported by educational grants from Celgene Corporation, Merck & Co., Inc. and Takeda Oncology.
PVI, PeerView Institute for Medical Education, Penn State College of Medicine, and Medical Learning Institute, Inc. are responsible for the selection of this activity's topics, the preparation of editorial content, and the distribution of this activity. The preparation of PeerView activities is supported by educational grants subject to written agreements that clearly stipulate and enforce the editorial independence of PVI, Penn State College of Medicine, and Medical Learning Institute, Inc. Our activities may contain references to unapproved products or uses of these products in certain jurisdictions. For approved prescribing information, please consult the manufacturer's product labeling. No endorsement of unapproved products or uses is made or implied by coverage of these products or uses in our activities. No responsibility is taken for errors or omissions in activities.
New and improved sourcefor free CME/CE
Expert commentary is based on data from recent medical literature. The materials presented here are used with the permission of the authors and/or other sources. These materials do not necessarily reflect the views of PeerView Press or any of its partners, providers, and/or supporters.

![pvicollective.compvicollective.com/.../uploads/2012/09/pvi-annual-report-2… · Web viewpvi. collective: [performance] [video] [intervention][] pvi. pvi. collective. collective](https://img.pdfslide.us/doc/110x75/5aadeb937f8b9a5d0a8b7182/web-viewpvi-collective-performance-video-intervention-pvi-pvi-collective.jpg)