Embed Size (px)
Citation preview
Transition to Value-Based Payment Models
Will Callicoat, (CFO if Value-Based Contracting is successful. If not, title changes to Barista.)
Our Vision: To Be The National Model for Patient Centered Care.
State of Reform
September 15, 2015
Agenda
I. Definitions
II. Why Value Based Care is important to Grays Harbor County
III. Implementation at SPMC
IV. The path forward
V. Provider compensation
VI. Value proposition
VII. Financial impact
VIII. Key considerations
IX. Timeline
1
"The existing systems do not reflect the relative value of health care services in important aspects of quality, such as clinical quality, patient-centeredness, and efficiency...nor recognize or reward care coordination...(in) prevention and the treatment of chronic conditions."
- IOM Report 2006
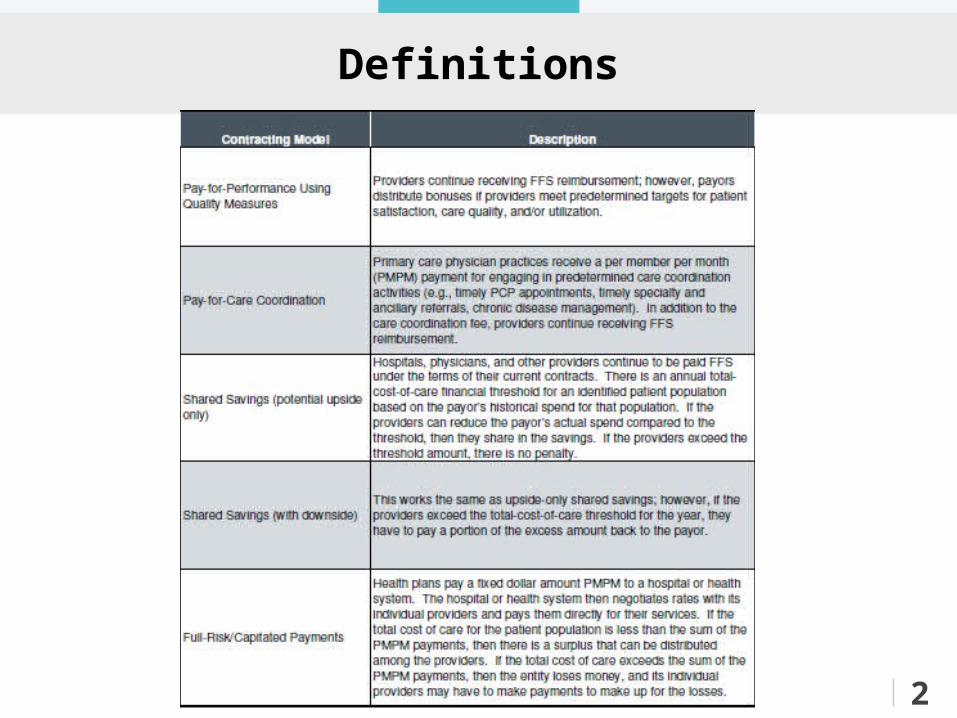
Definitions
2
4
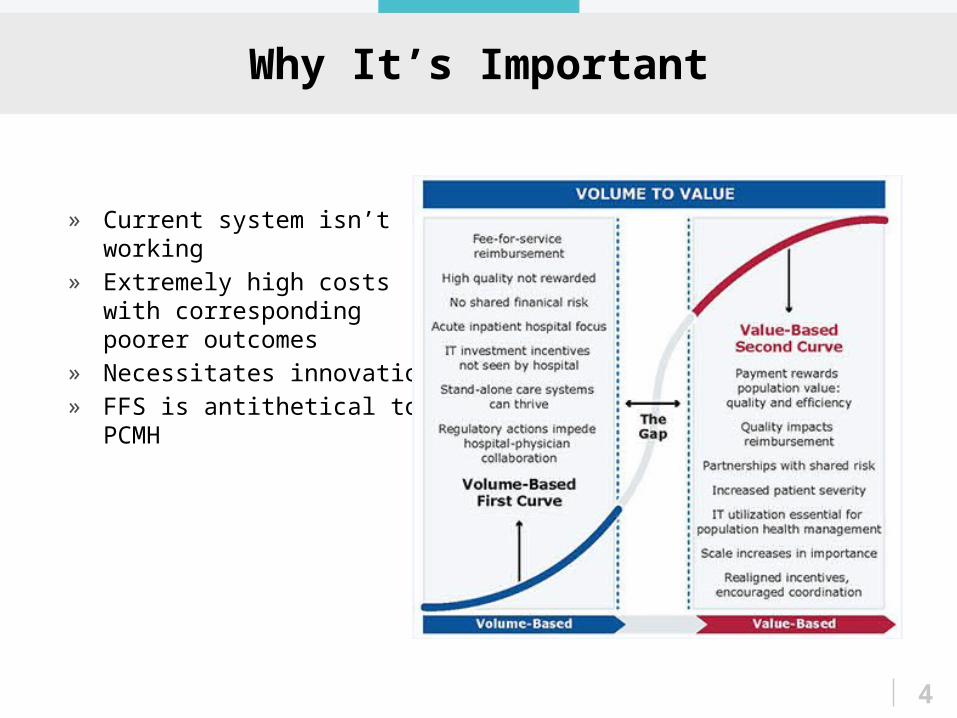
Why It’s Important
» Current system isn’t working» Extremely high costs with
corresponding poorer outcomes
» Necessitates innovation» FFS is antithetical to PCMH
5
Why It’s Important
Social environment• Life span in GH county is 3 years less than WA
avg. (Was 5 years less in 2000)• Higher drug use and smoking• Early instances of sexual activity• Less healthy eating and physical activity• In 2013, the unemployment rate was almost
double the state rate
Education and economics• 24% of county residents have a college or tech
degree vs. 42% in WA• GH County median income is $34,160. 42% less
than state median income of $58,585 (2013)Source: Grays Harbor County Community Health Needs Assessment
6
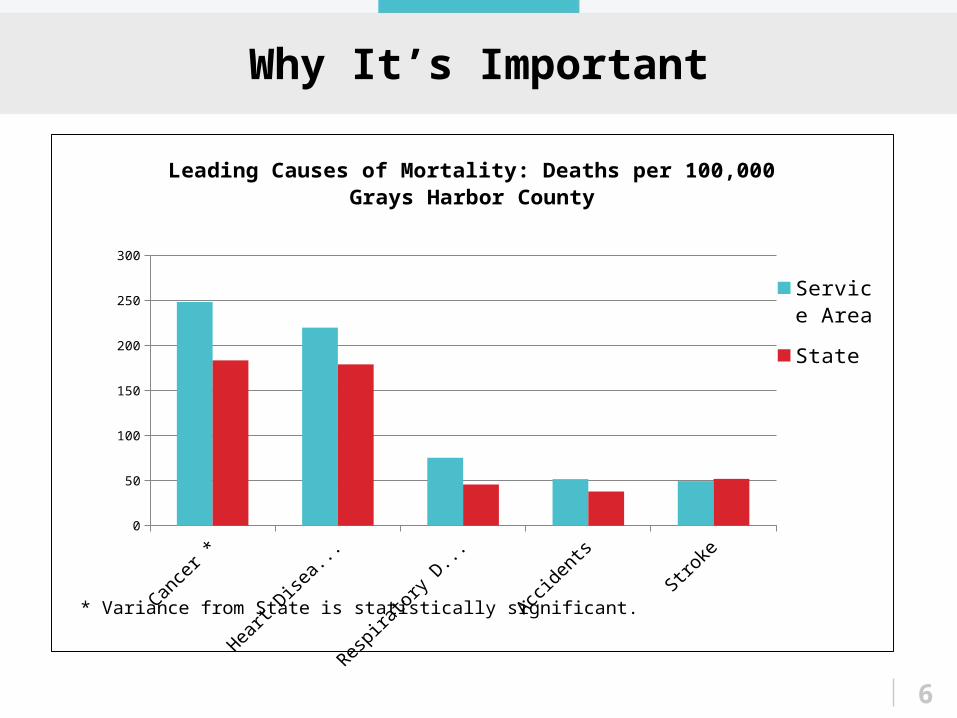
Why It’s Important
Cancer * Heart Disease * Respiratory Diseases
Accidents Stroke0
50
100
150
200
250
300
Leading Causes of Mortality: Deaths per 100,000 Grays Harbor County
Service Area
State
* Variance from State is statistically significant.
Implementation at SPMC
Summit Pacific Medical Center (SPMC)• Licensed for 24 beds, using 15• 13,000 ED visits per year• 3 Rural Health Clinics, including urgent
careo 30,000 visits per yearo 12 family medicine primary care
providerso Internal medicine hospitalists consult
3
Implementation at SPMC
1. Medicare Shared Savings Program / Accountable Care Organization 2015• Shared savings aligns the moral incentive
with the financial incentiveo Care Coordinationo Transitional Care Managemento Integrate mental healthcare into
primary careo Use internal medicine in-between
family medicine and specialty medicine 2. Data, data, data!!!
• If Medicare paid for it, you now know about ito High utilizerso high cost providers 3
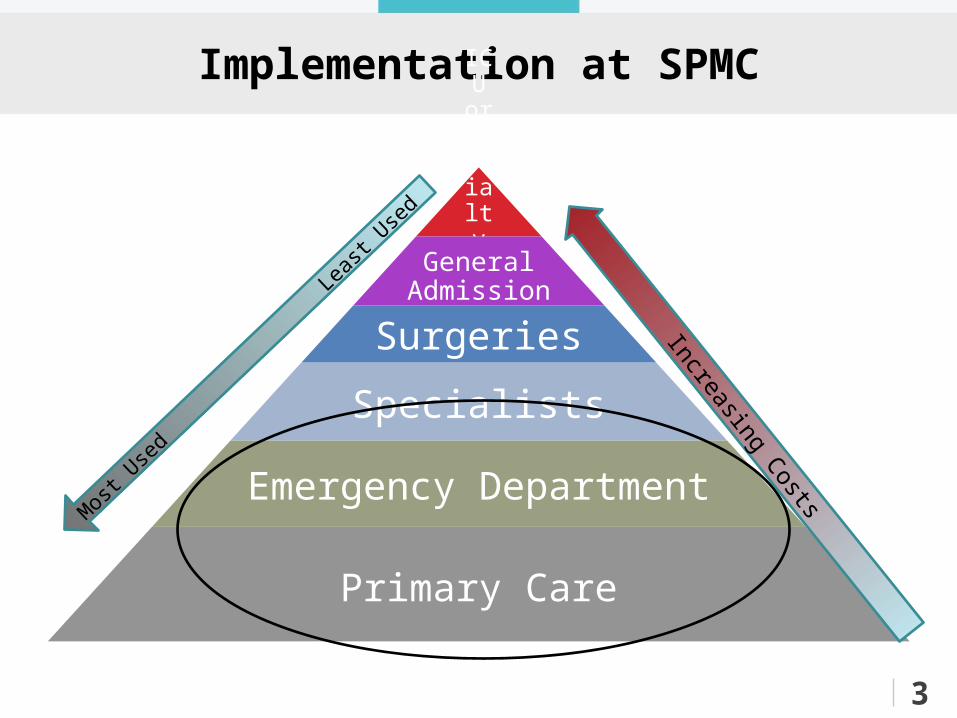
Implementation at SPMC
3
ICU or Specialty AdmissionGeneral
Admission
Surgeries
Specialists
Emergency Department
Primary Care
Increasing Costs
Mos
t Use
d
L
east
Used
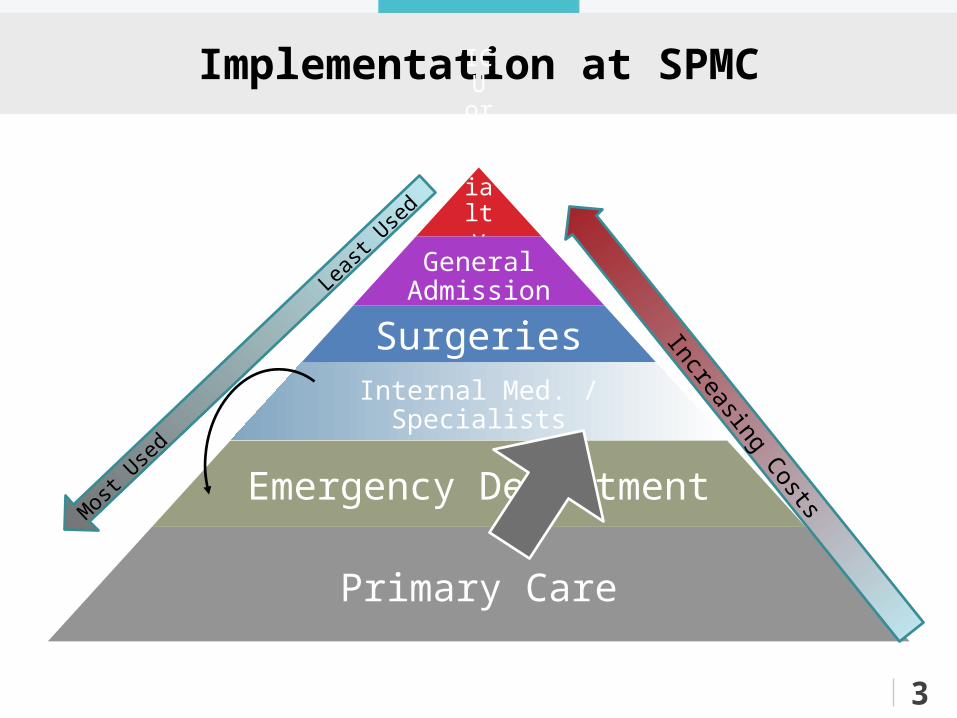
Implementation at SPMC
3
ICU or Specialty AdmissionGeneral
Admission
Surgeries
Internal Med. / Specialists
Emergency Department
Primary Care
Increasing Costs
Mos
t Use
d
L
east
Used
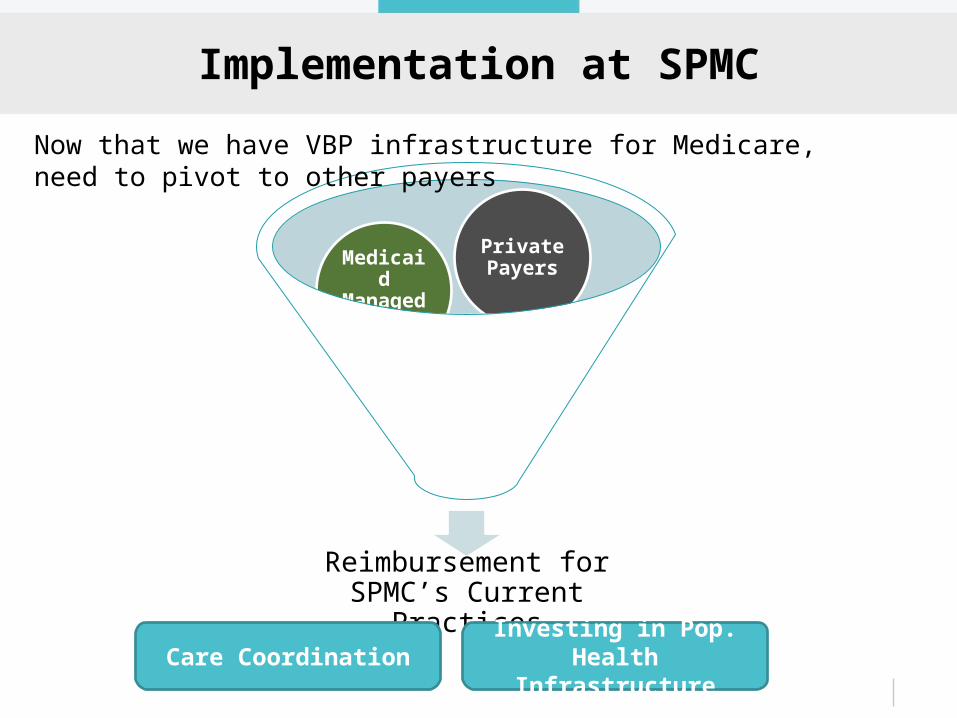
Implementation at SPMC
Reimbursement for SPMC’s Current Practices
ACO MSSP
Medicaid Managed
Care
Private Payers
Care CoordinationInvesting in Pop. Health
Infrastructure
Now that we have VBP infrastructure for Medicare, need to pivot to other payers
Implementation at SPMC
Organizational Readiness – pivot to other payers
• 2-hour Survey (built by ECG); completed with clinicians and operational leaders
• Identified organizational strengths and deficiencies in these categories:i. Care delivery transformationii. Comprehensive provider networkiii. Robust clinical informaticsiv. Effective payment modelsv. Strong organizational foundation
3
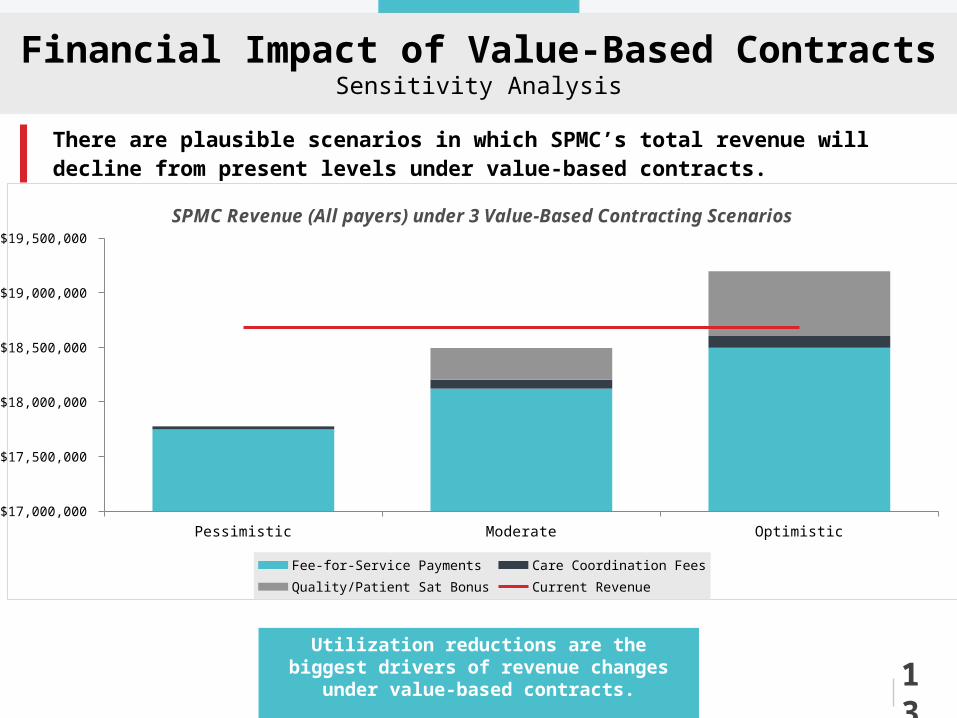
Financial Impact of Value-Based ContractsSensitivity Analysis
There are plausible scenarios in which SPMC’s total revenue will decline from present levels under value-based contracts.
Pessimistic Moderate Optimistic$17,000,000
$17,500,000
$18,000,000
$18,500,000
$19,000,000
$19,500,000
SPMC Revenue (All payers) under 3 Value-Based Contracting Scenarios
Fee-for-Service Payments Care Coordination Fees Quality/Patient Sat Bonus Current Revenue
Utilization reductions are the biggest drivers of revenue changes under value-based contracts.
13
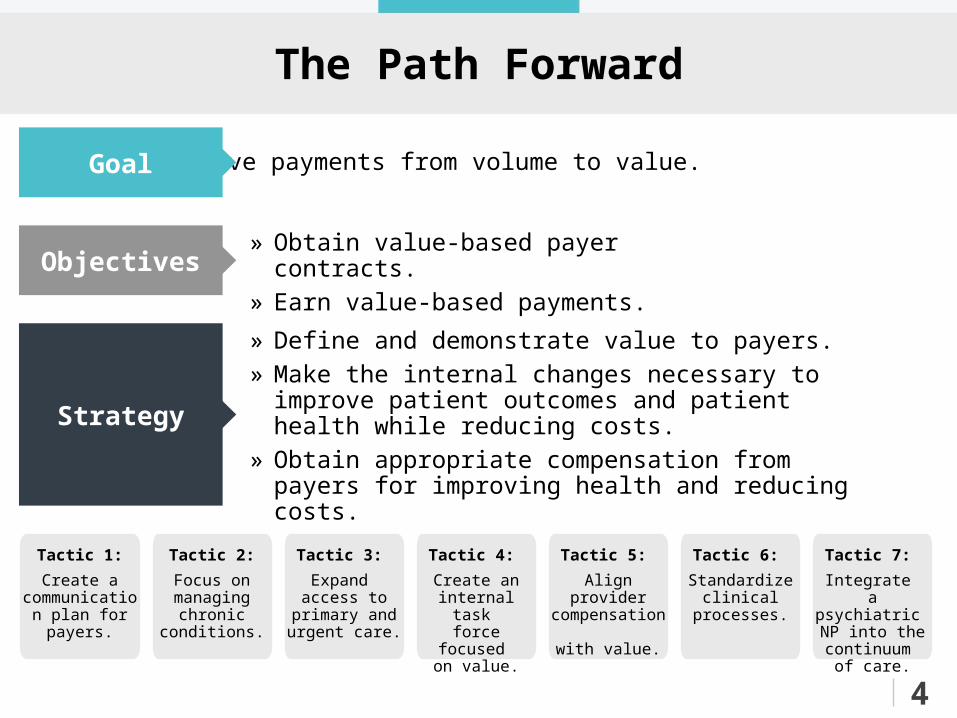
The Path Forward
Tactic 1:
Create a communication plan for payers.
Tactic 2:
Focus on managing
chronic conditions.
Tactic 3:
Expand access to
primary and urgent care.
Tactic 4:
Create an internal task
force focused on value.
Tactic 5:
Align provider compensation
with value.
Tactic 6:
Standardize clinical
processes.
Tactic 7:
Integrate a psychiatric NP into the continuum
of care.
Move payments from volume to value.
» Obtain value-based payer contracts.» Earn value-based payments.
» Define and demonstrate value to payers.» Make the internal changes necessary to improve patient
outcomes and patient health while reducing costs.» Obtain appropriate compensation from payers for
improving health and reducing costs.
Goal
Objectives
Strategy
4
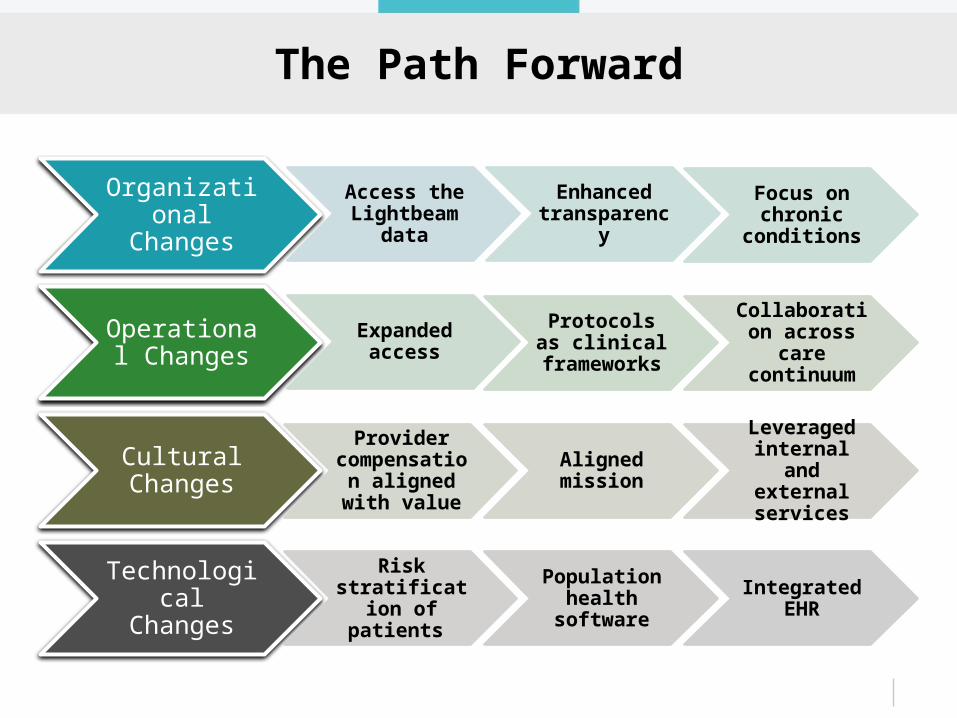
The Path Forward
Organizational Changes
Access the Lightbeam
data
Enhanced transparency
Focus on chronic
conditions
Operational Changes
Expanded access
Protocols as clinical
frameworks
Collaboration across care continuum
Cultural Changes
Provider compensation aligned with
value
Aligned mission
Leveraged internal and
external services
Technological Changes
Risk stratification of patients
Population health
software
Integrated EHR
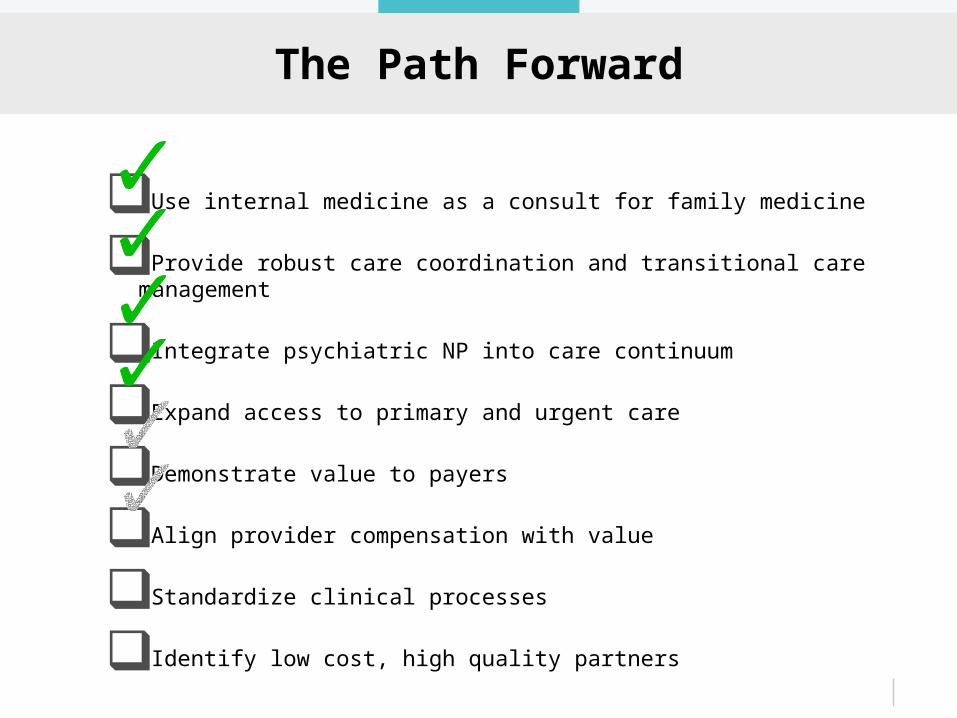
The Path Forward
Use internal medicine as a consult for family medicine
Provide robust care coordination and transitional care management
Integrate psychiatric NP into care continuum
Expand access to primary and urgent care
Demonstrate value to payers
Align provider compensation with value
Standardize clinical processes
Identify low cost, high quality partners
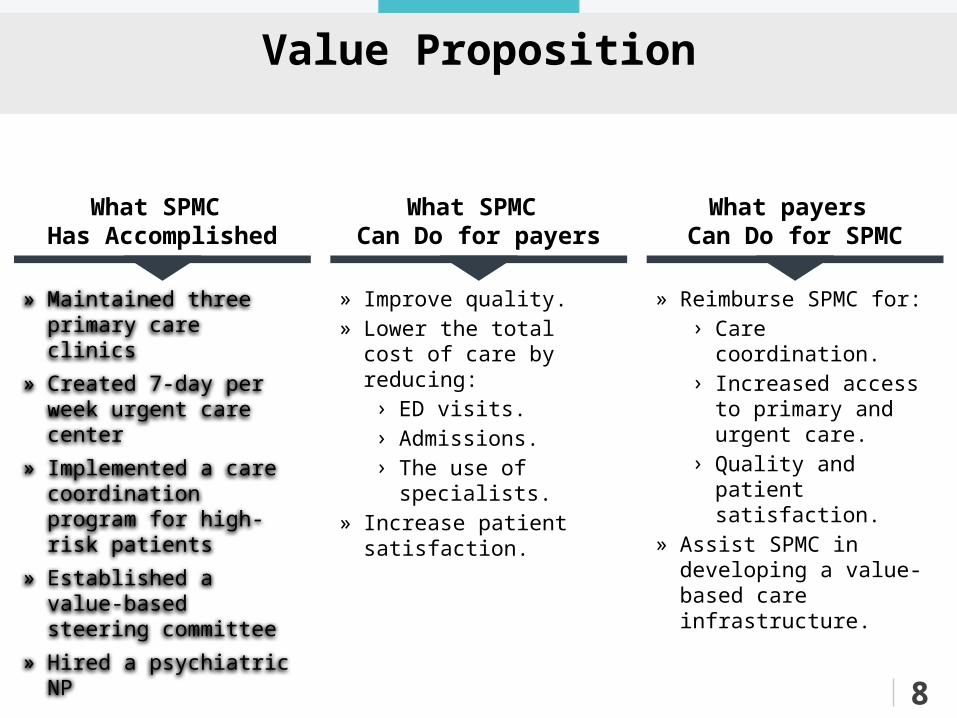
Value Proposition
» Maintained three primary care clinics
» Created 7-day per week urgent care center
» Implemented a care coordination program for high-risk patients
» Established a value-based steering committee
» Hired a psychiatric NP
» Improve quality.» Lower the total cost of
care by reducing:› ED visits.› Admissions.› The use of specialists.
» Increase patient satisfaction.
» Reimburse SPMC for:› Care coordination.› Increased access to
primary and urgent care.
› Quality and patient satisfaction.
» Assist SPMC in developing a value-based care infrastructure.
What SPMC Has Accomplished
What SPMC Can Do for payers
What payers Can Do for SPMC
8
Provider Compensation Tied to Quality
» 25-50% of annual goal bonuses tied to value by 2016› 2-3 month shadow period
» No penalty for not meeting measures
» Metrics will be “weighted”
» New technologies will support tracking
» Not as easy to tie provider comp to quality in a rural setting
Provider Compensation Tied to Quality
S.M.A.R.T. Specific, Measurable, Attainable, Relevant, and Timely
» Adherence to 6 process measures:1. Access to PCP Visits
2. Patients’ Rating of Provider
3. PHQ-2/PHQ-9 screening
4. HbA1C in Poor Control
5. Antibiotic Utilization
6. Medication Management and Reconciliation
» Accessory measures:1. ER utilization
2. 30-day Readmissions (AMI, PN, HF)
Key Considerations
SPMC must decide what to do next.
Payers» Without value-based contracts from some payers, will we begin to see disparate
results within our community?» Will our providers be able to provide care coordination to some patients but not
others? End Game» As costs decrease, the potential for future costs savings decreases
Bundled Payments» How will this impact rural hospitals that provide post-acute care (Swing bed and
therapies)
16
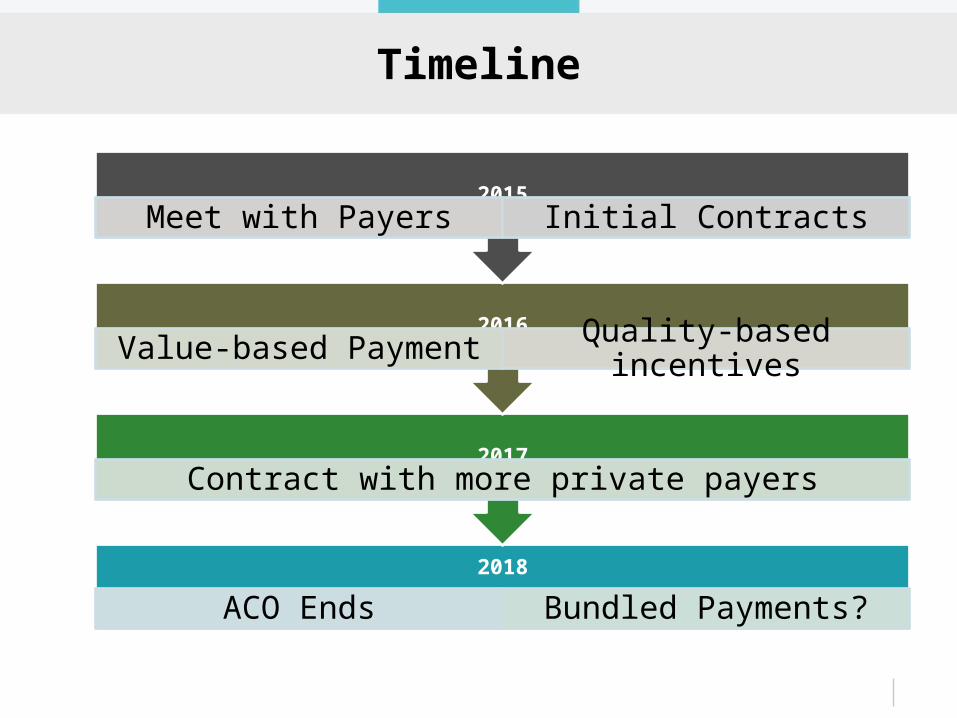
Timeline
2018
ACO Ends Bundled Payments?
2017Contract with more private payers
2016Value-based Payment Quality-based incentives
2015Meet with Payers Initial Contracts
Questions?
20
Thank you!
Does anyone know how to make a latte?
Contact information:[email protected](360) 346-2244





























