Embed Size (px)
Citation preview

Transforming Medicine: The Latest in Breast Cancer Clinical Trials
Antoinette R. Tan, MD, MHSc
Chief of Breast Medical Oncology

Metastatic Breast Cancer
• Metastatic breast cancer is a heterogeneous disease
• Goals of treatment
• Extend life
• Reduce cancer-related symptoms
• Optimize quality of life
• Balance toxicities of treatment with benefit

Factors that Influence Treatment Choices
Combination
vs.
single agents
Prior adjuvant
therapy
Cumulative dose
of anthracyclines
Prior exposure to
anti-HER2 therapy
Prior history
of taxanes
ER, PR, HER2
of tumor
Disease-free
interval
Disease
characteristics
Sites of
metastases
Tumor
biology
Tumor
burden
Patient
characteristics
Age
Performance
status
Side effects,
schedule
Medical conditions
i.e, diabetes, impaired
heart function
Trial vs.
“standard”
Cazzaniga et al, 2004.
PIK3CA
BRCA status

Systemic Treatment for Metastatic Breast Cancer
Evaluation for systemic treatment
Endocrine
Therapy
Chemotherapy
Immunotherapy
PARP Inhibitors
HR Positive Triple-negative
HER2-Targeted
Therapy
+
Endocrine
Therapy
HER-2+ HR+ and HER2+
BIOPSY
HER2-Targeted
Therapy

The Role of Clinical Trials
• Clinical trials are designed to build on the current standard of care
• Phases of a clinical trial• Phase I: Determines what dose is safe and test new drugs or new combinations of old
drugs
• Phase II: If the drug or intervention has an effect on the cancer
• Phase III: How the new treatment compares with the current standard
• Without clinical trials we cannot develop better treatments for the future

Metastatic breast cancer
2–5 prior chemotherapies
Progression ≤ 6 mos of
last chemotherapy
Neuropathy ≤ grade 2
ECOG PS ≤ 2
Eribulin Mesylate
N = 508
1.4 mg/m2, 2–5 mins IV
Day 1, 8 q21days
Treatment of Physician Choice
N = 254
Any monotherapy (chemotherapy,
hormonal, biological)a or supportive care
onlyb
Randomization 2:1 Progression-free survival
Overall response rate
Safety
Overall Survival
Primary
End Point
Secondary
End Points
Patients (N = 762)
− ≥ 2 for advanced disease
− Prior anthracycline and
taxane
aApproved for treatment of cancer.bPalliative treatment or radiotherapy administered according to local practice, if applicable.
ECOG = Eastern Cooperative Oncology Group; PS = performance status; IV = intravenous
EMBRACE Phase III Study Design
Cortes J et al. Lancet. 2011;377:914-923; Eribulin prescribing information, 2010.

Overall survival (months)
0.0
0.2
0.4
0.6
0.8
1.0
0 282624222018161412108642
Su
rviv
al
pro
bab
ilit
y
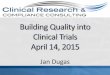
EMBRACE Trial: Overall Survival
EribulinMedian 13.12 months
TPCMedian 10.65 months
HR* 0.81 (95% CI 0.66, 0.99)p-value†=0.041
2.47 months
TPC (n=254)
Eribulin (n=508) 53.9%
1 year survival
43.7%
ITT population; *HR Cox model including geographic region, HER2/neu status, and prior capecitabine therapy as strata†p value from stratified log-rank test (pre-defined primary analysis); HR, hazard ratio; CI, confidence intervals
Cortes J et al. Lancet. 2011;377:914-923

Trastuzumab and Pertuzumab Bind to Different Regions on the HER2 Receptor
Courtesy of Dr. Swain, 2019
HER2Trastuzumab Pertuzumab
Subdomain IV of HER2
− Trastuzumab does not inhibit HER2 dimerization, thus blocking HER2:HER3
− Trastuzumab prevents HER2 receptor shedding
− Trastuzumab HER2 signalling and flags cells for destruction by the immune system
− Pertuzumab inhibits HER2 from forming dimer pairs
− Flags cells for destruction by the immune system
− Pertuzumab does not prevent HER2 receptor shedding
Dimerization domain of HER2
HER3

CLEOPATRA: Study Design
Swain, SM et al. N Engl J Med 2012;366:109-119
*< 6 cycles allowed for unacceptable toxicity or PD; > 6 cycles allowed at investigator discretion.
HER2, human epidermal growth factor receptor 2; MBC, metastatic breast cancer; PD, progressive disease.
HER2-positive metastatic breast
cancer(N = 808)
Placebo + trastuzumab
1:1
Docetaxel*≥ 6 cycles
n = 406
n = 402
Pertuzumab + trastuzumab
Docetaxel*≥ 6 cycles
PD
PD
• Study dosing every 3 weeks:
– Pertuzumab/placebo: 840 mg loading → 420 mg maintenance
– Trastuzumab: 8 mg/kg loading → 6 mg/kg maintenance
– Docetaxel: 75 mg/m2 → 100 mg/m2 escalation if tolerated

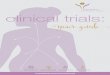
Number at risk
P + H + D 402 371 318 269 228 188 165 150 137 120 71 20 0 0
Pla + H + D 406 350 289 230 181 149 115 96 88 75 44 11 1 0
0
10
20
30
40
50
60
70
80
90
100
0 10 20 30 40 50 60 70 80 90 100 110 120 130
OS
(%
)
Time (mo)
8 years
HR 0.69 (95% CI = 0.58, 0.82)
Median OS: 40.8 mo (Pla) v 57.1 mo (P)
Landmark OS: 37%
Events: 235 (58.5%)
Landmark OS: 23%
Events: 280 (69.0%)
CLEOPATRA: Overall Survival*
Swain SM, et al. ASCO 2019
* Crossover pts were analyzed in the Pla arm.
OS was compared between arms using the log-rank test, stratified by prior treatment status and geographic region.
The Kaplan–Meier approach was used to estimate median OS, and a stratified Cox proportional hazards model
was used to estimate the HR and 95% CIs.
37%
23%

FDA Approvals of Targeted Therapy for Metastastic Breast Cancer, 2015 – 2019
• Cyclin Dependent Kinase Inhibitors
• Palbociclib (Ibrance®), 2/3/15
• Ribociclib (Kisqali®), 3/13/17
• Abemaciclib (Verzenio), 9/28/17
• PARP Inhibitors
• Olaparib (Lynparza®), 1/12/18
• Talazoparib (Talzenna), 10/16/18

Growth factorssuch as estrogen
G1
SG2
MCyclin DCdk4/6
Growth factor receptorsuch as the estrogen receptor (ER)
Target of CDK4/6 inhibitors
Inhibits progression from G1
to S phase of cell cycle
CDK4/6 inhibitors arrest the cell cycle at G1
by selective inhibition of CDK4/6
Rb p p
CDK 4/6 Inhibitors: Mechanism of Action
Adapted from Boer. Oncol Targets Ther. 2016;9:6119-6125.

FDA Approvals:CDK 4/6 Inhibitors in ER+ Breast Cancer
CDK, cyclin-dependent kinase; FDA, Food and Drug Administration; HER2−, human epidermal growth factor receptor 2 negative;
HR+, hormone receptor positive; NDA, New Drug Application; PFS, progression-free survival.
FDA News Release, 2015, 2016, 2017, 2018.
First Line After Disease Progression Following Endocrine Therapy
Palbociclib FDA accelerated approval 2/3/15
with letrozole first-line in postmenopausal HR+/HER2-
metastatic disease
FDA regular approval 3/31/17
for HR+/HER2- advanced/metastatic breast cancer in
combination with an aromatase inhibitor as initial endocrine
based therapy in postmenopausal women
FDA approval 2/19/16
with fulvestrant in HR+/HER2- advanced/metastatic disease
with progression following endocrine therapy
Ribociclib FDA approval 3/13/17
with an aromatase inhibitor as initial endocrine-based
therapy for postmenopausal women with HR+/HER2-
advanced/metastatic breast cancer
FDA approval 7/18/18
with an aromatase inhibitor as initial endocrine-based
therapy for pre/perimenopausal women with HR+/HER2-
advanced/metastatic breast cancer
with fulvestrant for the treatment of postmenopausal women
with HR+/HER2- advanced/metastatic breast cancer
FDA approval 7/18/18
with fulvestrant for the treatment of postmenopausal women
with HR+/HER2- advanced/metastatic breast cancer
Abemaciclib FDA approval 2/26/18
with an aromatase inhibitor as initial endocrine-based
therapy for postmenopausal women with HR+/HER2
advanced or metastatic breast cancer
FDA approval 9/28/17
in combination with fulvestrant for women with HR+/HER2-
advanced/metastatic breast cancer with disease progression
following endocrine therapy
as monotherapy for women and men with HR+/HER2-
advanced/metastatic breast cancer with disease progression
following endocrine therapy and prior chemotherapy in the
metastatic setting

New Drugs to Treat Metastatic Breast Cancer
• PARP (poly ADP-ribose polymerase) Inhibitors• Type of biological therapy
• It blocks an enzyme called PARP that cancer cells need to repair themselves.
• Healthy cells in the body can repair themselves if they get damaged.
• A change in one of the BRCA genes means that the cells in cancer have problems repairing damage.
• The hope is that the drug will stop PARP from working, any cancer cells still in one’s body after treatment will not be able to repair themselves and will die.

Olparib (Lynparza®)
• FDA approved: January 12, 2018
• Classification: an inhibitor of PARP
(poly-ADP-ribose polymerase inhibitor)
• Indication: In pts with BRCA-mutation, HER2-negative metastatic breast cancer treated with chemotherapy in the neoadjuvant, adjuvant or metastatic setting. In pts with HR-positive breast cancer treated with prior endocrine therapy
• Regimen: Olaparib 300 mg orally twice a day with or without food

Talazoparib (Talzenna)
• FDA approved: October 16, 2018
• Classification: an inhibitor of PARP
(poly-ADP-ribose polymerase inhibitor)
• Indication: For the treatment of adult pts with deleterious or suspected germline BRCA-mutated HER2-negative metastatic breast cancer
• Regimen: Talazoparib 1 mg capsule orally once daily with or without food

FDA Approvals of Targeted Therapy for Metastatic Breast Cancer, 2015 – 2019
• Immunotherapy
• Atezolizumab (Tecentriq®) and nab-Paclitaxel, 3/8/19
• PI3-Kinase Inhibitor
• Alpelisib (Piqray®), 5/24/19

Atezolizumab (Tecentriq®)
• FDA approved: March 8, 2019
• Classification: PD-L1 checkpoint inhibitor (programmed death receptor ligand 1)
• Indication: In combination with paclitaxel protein-bound for adult patients with unresectable locally advanced or metastatic triple-negative breast cancer (TNBC) whose tumors express PD-L1, as determined by an FDA-approved test.
• Regimen: Atezolizumab 840 mg administered as an intravenous infusion over 60 minutes, followed by 100 mg/m2 paclitaxel protein-bound. For each 28-day cycle, atezolizumab is administered on days 1 and 15, and paclitaxel protein-bound is administered on days 1, 8, and 15

Alpelisib (Piqray®)
• FDA approved: May 24, 2019
• Classification: an inhibitor of PI3 kinase
(phosphatidyl inositol -3- kinase)
• Indication: In combination with fulvestrant for the treatment of postmenopausal women, men, with HR+HER2-negative, PIK3CA mutated metastatic breast cancer as detected by an FDA-approved test following progression on or after endocrine-based regimen
• Regimen: Alpelisib 300 mg (two 150 mg tablets) orally daily with food and fulvestrant IM injection monthly

Biomarkers to Test
• Estrogen receptor
• Progesterone receptor
• HER2 (human epidermal growth factor receptor type 2)
_________________________________________________
• PIK3CA mutation – if tumor is hormone receptor-positive, HER2-negative
• PD-L1 status- if tumor is triple-negative
• BRCA mutation in the blood

New Paradigm in Breast Cancer Treatment
Neratinib ⭢⭢
Alpelisib ⭢⭢

Methods of Testing for Targets
• Germline testing
• To look for inherited mutations such as BRCA1/2 gene
• Next generation sequencing (NGS)
• To look for mutations in tumor tissue (tumor’s molecular make up)
• Expression of proteins
• To look for expression of nuclear hormone receptors or cell surface receptors
• Circulating tumor DNA (ctDNA)
• To look for mutations in blood

Molecular Analysis: Tumor vs Blood (Circulating Tumor (ct) DNA or “Liquid Biopsies”
• Tumor biopsy and testing is standard but invasive and represents
single time and location• Tumors are heterogeneous
• Tumors shed DNA (ctDNA) into the bloodstream• Represents all tumors in the body and all cells in the tumor
• Tumor heterogeneity represented in one sample

Research Vision of the Breast Program at LCI
• Active program of clinical research for breast cancer patients who present
with any stage of disease
• Goal is to have clinical trial portfolio offering
• Targets specific breast cancer subtypes, i.e. Triple-negative breast cancer
• Trials that have the potential to change the standard of care
• Evaluate newer techniques to tailor therapy, i.e. molecular profiling, circulating tumor
cells
• Phase I clinical trials (2 locations, LCI Charlotte and LCI Concord)
• Patients access to novel treatments, i.e. immunotherapy, antibody drug conjugates

TNBC Diagnosed by Core Needle Biopsy with Palpable Breast Mass 2.0 cm
RANDOMIZATION
Arm 1
Carbo q3wk x 4 + WP x 12 + Placebo
AC X 4 + Placebo
Arm 2
Carbo q3wk x 4 + WP x 12 + Atezolizumab
AC x 4 + Atezolizumab
SURGERY
(lumpectomy or mastectomy) and axillary staging
NSABP B-59/GBG 96-GeparDouzeA Randomized, Double-Blind, Phase III Clinical Trial of Neoadjuvant Chemotherapy with
Atezolizumab or Placebo in Patients with Triple-Negative Breast Cancer Followed by Adjuvant Continuation of Atezolizumab or Placebo
Arm 1
Placebo to complete 1 year
Arm 2
Atezolizumab to complete 1 year

LCI-BRE-H2N-PEPP-001 A Pilot Study of Paclitaxel Plus
Pembrolizumab in Patients with Metastatic Her2-negative Breast
Cancer (The PePPy trial)
Cohort A, n = 20Phased Regimen
Paclitaxel
Paclitaxel + Pembrolizumab
Cohort B, n = 20 Concurrent Regimen
Paclitaxel + Pembrolizumab
Cohort A: phased regimen of pembrolizumab in which paclitaxel is given alone for Cycles 1 and 2; then pembrolizumab is added starting with Cycle 3 Day 1
Cohort B: concurrent regimen of paclitaxel plus pembrolizumab (both drugs starting with Cycle 1 Day 1)

Antibody Drug Conjugates
1. Monoclonal antibody specific for a tumor antigen with little/no expression on normal cells
2. Linker that is stable in circulation but releases the chemotherapy in target cells
3. Potent chemotherapy drug to target cancer cells when internalized and released

DS-8201
FDA granted
breakthrough
therapy designation
August 2017
Sekiguchi, ESMO 2017
DS-8201a T-DM1
Antibody Anti-HER2 Ab Trastuzumab
MOATopoisomerase IBystander effect
Tubulin
Drug-to-antibody ratio 7-8 3.5

DESTINY-Breast U301: Phase 3 Study Design
ClinicalTrials.gov Identifier: NCT03523585.
Investigator’s choice*(n=200)
DS-8201(n=400)
T-DM1
treated
HER2+ MBCR
2:1
*trastuzumab + capecitabine or lapanitib + capecitabine
Primary Endpoints: Progression-free survival and overall survival

Tucatinib, Selective HER2 Tyrosine Kinase Inhibitor
Hamilton, SABCS, 2016

HER2CLIMB: Study Design
ClinicalTrials.gov Identifier: NCT02614794
Capecitabine +
Trastuzumab +
Tucatinib
Capecitabine +
Trastuzumab +
Placebo
N = 480
Patient Population
- HER2+ mBC patients with
progression after pertuzumab,
trastuzumab, a taxane, and TDM-1
- Patients w/ or w/o brain metastases
(stratified)
2:1

Pros and Cons of a Clinical Trial
• Pros• Access to newer promising therapies before they are approved• Help to move the field forward• Further the knowledge base that helps improve breast cancer care• Potentially help future cancer patients
• Cons• No guarantee trial treatment is better• There may be unexpected side effects• There is additional time needed as a participant, additional visits,
blood draws, and biopsies

How can I find out about clinical trials in my area?
• Treating oncologist
• ClinicalTrials.gov
• Clinical trials at the Clinical Center of the National Institutes of Health (NIH) in Bethesda, MD are free of charge to those who are eligible to join and willing to get treatment there. For more information, visit the NIH clinical center website or call 1-800-4CANCER.

How can I find out about clinical trials in my area?
Susan G. Komen® Breast Cancer Clinical Trial Information Helpline
If you or a loved one needs information or resources about clinical trials, call our Clinical
Trial Information Helpline at 1-877 GO KOMEN (1-877- 465- 6636) or email
Metastatic Breast Cancer Alliance
MBC Connect 2.0
https://www.mbcconnect.org/
The Metastatic Breast Cancer Alliance has developed a patient registry that matches users to clinical
trials they may be eligible for. Users must enter their treatment history to facilitate a possible match.

Future of Breast Cancer Research
• The identification and clinical application of molecular testing is evolving
• Developments in our understanding of therapy demonstrate progress towards individualizing treatment: “personalized medicine”
• Advances in the development and use of novel targeted agents are promising

“I’m just so
happy that I’m on
the right track.”
“I have hope.”
CURE magazine