Embed Size (px)
Citation preview

Transforming Health Care Delivery in a Rural
SettingFebruary 12, 2013

Please note that the views expressed by the conference speakers do not necessarily reflect the views of the American Hospital Association and Health Forum.

OverviewLori Williams, Illinois Hospital AssociationVice President, Small & Rural Hospital
Affairs

Illinois Hospital Association
4
• Offices in Naperville, Springfield and Washington, D.C., an advocate for 200 hospitals and health systems
• 88 are considered Small & Rural
• 51 are Critical Access Hospitals

Hospitals as Leaders in Rural Communities
Small & Rural Hospitals in Illinois:
• Provide 65,380 direct and indirect jobs• 1 of the top 3 employers in most rural
counties• Contribute $9.9 billion to rural
economies• Leading health care transformation
5

6
Adopted by the Centers for Medicare and Medicaid (CMS), the goals of the Triple Aim are defined as:
• Improving Health Care• Patient Experience
• Quality
• Improving Health & Wellness
• Reducing cost
Meeting the Triple Aim

Building Value Based Systems in rural communities
Rural Hospitals:
• Expanding access to primary care• Focusing on Prevention & Wellness• Developing care coordination services• Using technology in new ways• Moving from inpatient to outpatient
services• Partnering with other health providers
7

Value-Based Care
Health Coaching
Health Screening & Assessment
Medical Home
DiseaseManagement
Stephanie McCutcheson and Associates, 2011
Compliance and Community
Support ServicesBetter Health! Lower Costs!

Integrated Health Advocacy Program®
Advocating for Superior Healthcare
Harry Wolin, Administrator/CEO
Mason District Hospital
Havana, Illinois
9

Integrated Health Advocacy Program®
IHAP is a disease management program that allows employers to reduce their healthcare costs, reduce future liabilities, and maximize the health of the highest utilizers in an organization.
10

11

Mason District Hospital
We exist to serve the health care needs of the community in a cost effective manner with a
constant striving for the highest quality care, to maintain a strict standard of professional and
ethical behavior, and to always place the patient at the center of our activities.

13
Service PopulationMason County• With 14,666 people, Mason County is
the 77th most populated county in the state of Illinois out of 102 counties.
• In 2010, the median household income of Mason County Residents was $42,461.
• 15.5% of Mason County residents live in poverty.
• The median age for Mason County residents is 44.0 years young.
• The largest Mason County racial/ethnic groups are White (97.5%) followed by two or more races (0.9 %) and Hispanic (0.8%). US Census Bureau, 2010 Census

Mason District Hospital is...
– 269 Employees: • 9 active medical staff members/physicians • 198 total physicians/allied health care providers • 55 volunteers
– $24,068,598 Annual Budget– 1,466 Annual Admissions– 14,370 Annual Ambulatory Clinic Visits– 24,338 Annual Hospital Outpatient Visits– Serves more than 18,000 people in west-central IL
14

The Burden of Healthcare
• Healthcare is the largest component of employee benefit costs
• 80% of healthcare dollars are used by 20% of benefit plan participants
• The largest amount of healthcare dollars are spent by those with multiple chronic illnesses or about 5% of people
• This 5% spends half of the healthcare dollars and incurs the largest claims each year
15

Anderson, G. (2010) Chronic Care: Making the Case for Ongoing Care. Robert Wood Johnson Foundation.

Anderson, G. (2010) Chronic Care: Making the Case for Ongoing Care. Robert Wood Johnson Foundation.

Anderson, G. (2010) Chronic Care: Making the Case for Ongoing Care. Robert Wood Johnson Foundation.

19
Unique Solution To A Growing Problem
Lowers risk future liabilities
ReducesHealthcare
Costs
Tested Strategy
with Sustained Outcomes
Improves Participants’Health
Educates andSupportsEmployees

The IHAP® “Core Team”
20
Primary Advocate /
Registered NursePrimary
Advocate
Psychosocial Advocate
Psychosocial Advocate/
Counselor, Psychologist or
Social Worker
Medical Advocate
Medical Advocate / Medical Doctor/Mid Level

Participant and Advocate Responsibilities
21
• Productive Participation
• Calendars/ Diaries• Regular Instruments
Participant
• Confidentiality• Education• Empowerment
Team to Participant • Cost Effectiveness
• Documented Progress
• Outcomes Reporting
Team to Plan

22
Projected ROI• Risk assumes the average of the minimum and
maximum potential claims liability of an identified group of high-risk individuals
• Cost is a calculation of Company ABC’s historical claims data (2008-2010) plus the cost for 36 months of the IHAP program (assuming 100% participation)
RiskCost + IHAP Costs for 36 Months = Projected
Return on Investment

23
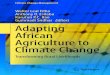
Mason District Hospital participant health care costs 2009-2011

What Have We Learned
24
Data supports the money saved:• Every $1 spend saved $4o Reinvested the money into
preventative care Positive Outcomes
• Decreased Absenteeism• Self Directive Testing• Patients feel better

Characteristics of IHAP® Participants
25
Length of employment 2 to 36 years
Number of current health problems 1 to 13
Current medications 2 to 17
Hours of sleep per night 3 to 12
Chronic health issues/conditions reported by IHAP Team
14 to 27

“A focus on a small population of intensive users could have the
potential for improving care for all.”
R. Blendon (Harvard School of Public Health), C. Shoen (The Commonwealth Fund), et. al.; Project Hope,
The People-to-People Health Foundation, Inc., 2003

What Our Customers Are Saying About IHAP®
“The program DOES change people’s lives and has proven to be replicable
across teams/organizations.”
“The program is helping people and the spirit of the program is aligned with our
values as an organization.”
“The philosophy, principles, and impact of the program make me proud to sponsor these teams.”
27

Thank You
28

MDH LifeSteps©McDonough District Hospital in Macomb, IL
Kenneth Boyd,Chief Executive Officer

McDonough District Hospital
Mission StatementThe mission of McDonough District Hospital, in partnership with its Medical Staff, is to provide health services with a personal approach to care that enhances the quality of life.
Vision StatementTo be your First Choice for First Class Health Services
Core Values
Honesty and Integrity, Respect, Exceptional Service, Commitment to Excellence and Teamwork

72 Staffed Bed General Medical Surgical Hospital
Hospital services include: behavioral health, cancer care, cardiopulmonary, diabetes education, home health, hospice, dialysis, laboratory, radiology, transitional care, food nutrition, emergency room, surgery, and wound management.
Outpatient rehab services include Physical Therapy, Speech-Language Pathology, Cardiac, Pulmonary, Industrial & Sports Rehab. Inpatient rehab services include physical, occupational & speech therapy.
McDonough District Hospital is...

620 Total Employees: • 38 active medical staff members/physicians, • 85 consulting medical staff, 48 telemed staff,
35 allied health providers for a total of 206 “providers” on staff
• 150 active volunteers Annual Budget - $143M gross/$71.8M Net 2,350 Annual Admissions 30,000 Visits to employed physician offices &
7,300 to our Convenient Care Clinic 48,000 Annual Hospital Outpatient Visits
McDonough District Hospital is...

The PSA has an estimated total population of 31,998 (2011) which has the following demographic characteristics:
Median age: 24.7 years Median household income: $34,990
Racial and ethnic distribution: 88% Caucasian, 5% African American, 3% Asian, 2% Hispanic of any race, 2% all other
The SSA has an estimated population of 16,769 (2011) which has the following demographic characteristics:
Median age: 44.0 years Median household income: $41,694 Racial and ethnic distribution: 97% Caucasian, 1% Hispanic
of any race, 2% all other
Primary & Secondary Population Information...

MDH has identified 68 zip codes surrounding the primary and secondary service areas as potential growth opportunities. Residents of this expanded service area (ESA) contribute 8% of the hospital’s inpatient admissions and 5% of its ER visits. The ESA has an estimated population of 104,356 (2011)
which has the following demographic characteristics:• Median age: 40.7• Median household income: $41,081• Racial and ethnic distribution: 90% Caucasian, 5%
Hispanic of any race, 4% African American, 1% all other
Expanded Service Area Information

MDH LifeSteps© Program
Voluntary Program rolled out to McDonough District Hospital Employees in August, 2012 Core components of MDH LifeSteps© Program:
1. Biometric Screening; Full Gamut of Laboratory Tests then 6 month screenings thereafter
2. Online Health Risk Assessment; Software Program Purchased with partnership Identifies top risk factors of population Participants receive access to patient portal
3. Online health resource library, monthly newsletters and challenges, and wellness activities
4. 3 Mayo Certified Wellness Coaches

MDH LifeSteps© Program
Summary Findings of First Cohort:
301 Active participants
Overall, participation rate of 53%; 65% of management staff
98% “Very Satisfied”
Top three modifiable risk factors; Physical activity, Weight Management; Osteoporosis risk
Goal: Reduction of top 3 modifiable by 30%; over three years

MDH LifeSteps© Program Incentives
Focusing on Life Style Choices – Health Improvement – Personal Responsibility
Cash Incentives for:• Annual Health Screenings• Flu Shots• Exercise Programs• Wellness Challenges• Full participation in MDH LifeSteps© program
= zero increase in employee out of pocket cost in health premium responsibility

What’s Next...
Trial partnerships with small to medium sized employers within MDH service area
McDonough Telephone Cooperative: secured Other identified partners for approach: City of Macomb,
McDonough County (Board and employees), McDonough County YMCA.
Allowing Business Partners reduced cost for trial as well as choice of program components
Analyzing Data Collection Development of company wellness plan specific to Business
Partner’s employee population & business model Opportunity to integrate MDH LifeSteps© with Business
Partner’s insurance carrier and health plan design

Questions for the Panel

Thank you!Contact Information:Harry Wolin, Administrator & CEOMason District [email protected] (309) 543-8575
Kenneth Boyd, Chief Executive OfficerMcDonough District [email protected] (309) 833-4101
Lori WilliamsV.P. Small & Rural Hospital AffairsIllinois Hospital [email protected](217) 541-1164