Embed Size (px)
Citation preview

Transforming ClinicalNeurophysiology DiagnosticServices to Deliver 18 WeeksA Good Practice Guide

DH INFORMATION READER BOX
Policy EstatesHR/Workforce PerformanceManagement IM & TPlanning FinanceClinical Social Care/Partnership Working
Document purpose Best Practice Guidance
ROCR Ref: Gateway reference:8528
Title Improving Access to Clinical Neurophysiology Services
Author Department of Health
Publication date 23 Aug 2007
Target audience PCT CEs, NHS Trust CEs, SHA CEs, Foundation Trust CEs, MedicalDirectors, Directors of PH, Directors of Nursing, PCT PEC Chairs, NHS Trust Board Chairs, Special HA CEs, Directors of HR, Directors ofFinance, Allied Health Professionals, GPs, Communications Leads,Emergency Care Leads, Those collating data for the national diagnosticcensus
Circulation list
Description Clinical neurophysiology involves the diagnosis of a range of conditionsaffecting the central and peripheral nervous systems, for example,epilepsy and carpal tunnel syndrome. This document provides goodpractice and evidence to support the delivery of high quality, low waitneurophysiology services.
Cross reference N/A
Superseded documents N/A
Action required N/A
Timing N/A
Contact details Becky FarrenPhysiological Measurement Policy and Implementation18 Weeks - Commissioning Directorate4N14 Quarry HouseLeedsLS2 7UEhttp://www.18weeks.nhs.uk/public/default.aspx?main=true&load=ArticleViewer&Articleld=55
For recipient’s use

Transforming ClinicalNeurophysiology DiagnosticServices to Deliver 18 WeeksA Good Practice Guide
August 2007

2
Foreword
The NHS is currently being challenged toensure that patients move from referral totreatment in end to end clinical pathwayswithin a maximum of 18 weeks. This is atough challenge and puts significant pressureon diagnostic services where patients havepreviously experienced “hidden waits”.
Clinical neurophysiology diagnostics are anintegral part of many clinical pathways forpatients with problems and conditions thataffect the functioning of the brain, nervoussystem and muscles. The contribution ofclinical neurophysiology services in end to endpatient pathways has been poorly understoodto date and long waits have been uncovered,which are contributing to elongated patientpathways.
This document aims to provide commissionerswith information about where clinicalneurophysiology needs to fit into their local 18weeks strategy and providers with innovativeways in which services can be delivered inorder to meet the diagnostic milestones andthe December 2008 18 weeks targets. It setsout how the levers of health reform can bebrought be bear to improve quality, efficiencyand access to clinical neurophysiology services.
The models of service outlined in thisdocument have been developed by a smallgroup of experts. A national group is beingformed which will report in to the NationalPhysiological Measurement Programme Board,taking forward the implementation of thisdocument and the continued development ofservice improvement.
Overall, this document has been designed toboth stimulate discussion and to introduce newways of working aimed at reducing waits andincreasing access to clinical neurophysiologyservices. New ways of working will be essentialif sustainable improvements are to be deliveredand the patient’s experience enhanced.
Professor Sue Hill:Chief Scientific Officer; National Clinical Leadfor Physiological Measurement, Department of Health

Foreword 2
Executive summary 4
Vision and context for clinical neurophysiology services 5
How to achieve the vision and context 13
Systems and processes 13
Technology 20
Workforce 25
Symptom based pathways 31
Supporting commissioners and providers 36
Acknowledgements 38
Annex 1 Further information on Clinical Neurophysiology Tests 39
Annex 2 Complete references for incidence and prevalence Information in paragraph 9 40
Annex 3 Choose and Book referral screen for clinical neurophysiology 41
Annex 4 Royal Free referral form for one stop tingly fingers clinic 42
3
Contents

4
Clinical Neurophysiology involves the diagnosisof a wide range of conditions affecting thecentral and peripheral nervous systems. It isconcerned with testing the electrical functionof the brain, spinal cord and nerves in thelimbs and muscles. It is principally diagnostic,but can also be necessary for ongoingmanagement decisions, directly involvingtherapy for conditions.
Clinical neurophysiology services will play animportant part in the delivery of the 18-weekpatient pathway in a number of majorspecialties and are critical in the diagnosis andunderstanding of common diseases such asepilepsy, carpal tunnel syndrome, neuropathyand diabetes. Taking these conditions alonethere is a significant and increasing demand forclinical neurophysiology services.
This document provides good practice and theevidence to support the requirement for highquality, low wait clinical neurophysiologyservices and the mechanism for achievementand delivery using the three key componentsof systems and process, technology andworkforce together with new service modelssummarised as:
� System and process: enabling efficientclearance of historical backlogs;introducing effective booking andschedule management systems;reducing the number of DNAs, andincreasing the proactive use of availabledata to manage services.
� Technology: encouraging the use ofremote reporting, multifunctional
equipment, leading edge technologyand investment in IT support.
� Workforce: pioneering the developmentof multidisciplinary teams incorporatingthe development of the role of clinicalphysiologists and using existingresources more effectively by extensionof working hours and ensuring that theright staff are available for the righttask.
� New service models: introducing andmaking better use of one stop clinicsand providing diagnostics earlier in thepatient pathway associated with clearlydefined referral criteria.
It is critically important to ensure that effectiveleadership is in place at senior levels to drivethe management of large scale change.Change management success will be a majorcontribution to the delivery of 18-week patientpathways and a more effective and moderndiagnostic service for patients.
The levers and incentives introduced by thehealth reforms provide the opportunity formore effective commissioning and deliveryof clinical neurophysiology services includingthe use of local tariffs and practice basedcommissioning. This is a transformationaldocument to encourage each local clinicalneurophysiology service to become selfimproving and deliver a quality service whichresults in a better experience for patients.It will be of interest to providers andcommissioners alike.
Executive Summary

5
1. Clinical Neurophysiology is one of eightdiagnostic specialties recognised in theNational 18 Week PhysiologicalMeasurement Programme together with:
� Audiology
� Cardiac Physiology
� Gastrointestinal (GI) Physiology
� Ophthalmic and Vision Science
� Respiratory and Sleep Physiology
� Urodynamics
� Vascular Technology.
2. As outlined in the DH document ‘What isPhysiological Measurement?1’, the overallvision for the future of these diagnosticservices, is that they should:
� Be patient centred
� Realise the benefits of new technology
� Be streamlined and efficient withinReferral to Treatment (RTT) pathwaysof 18 weeks by December 2008
� Be delivered closer to home
� Provide excellent patient information
� Be accessible from primary as well assecondary care.
3. Understanding the role of diagnostics inthe future delivery of low-wait healthcareis essential if the rate, flow anddistribution of patients throughout theelective and non-elective systems is not tobe compromised. By utilising appropriatediagnostic tests, sequenced correctly (inprimary care if the quality of the test canbe maintained and if it is appropriate forpatients, or by making tests directlyaccessible and bookable by primary carepractitioners), there will be potential tomatch demand with real capacity.
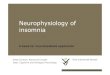
4. Clinical neurophysiology involves thediagnosis of a wide range of conditionsaffecting the central and peripheralnervous systems, with tests being utilisedin patient pathways for a variety ofspecialties including neurology,orthopaedics, paediatrics, ophthalmologyand rheumatology. The diagram in Figure1 shows the changing proportion ofworkload since 1990/91 attributable toeach referring specialty at Kent andCanterbury Hospital, which is typical of amedium sized District General Hospital(DGH).
Vision and context for clinicalneurophysiologyservices
1 ‘What is Physiological Measurement? A guide to the tests and procedures conducted by PhysiologicalMeasurement diagnostic services’ DH (May 2007) Located at www.18weeks.nhs.uk within the physiologicalmeasurement section.

5. The main tests undertaken in clinicalneurophysiology diagnostic services are2:
� EEG (Electroencephalography) is arecording of the electrical activity of thebrain and is used in the investigation ofvarious neurological conditions such asepilepsy, cerbrovascular disease,intracranial infections, metabolicdisorders, dementias and otherneurodegenerative disorders.
� Peripheral neurophysiology has twoaspects, which can be used together or independently to investigate, forexample, the presence or absence ofcarpal tunnel syndrome orneuropathies:
� Nerve Conduction Studies (NCS)involve electrical stimulation ofperipheral nerves with recording ofresponses from nerves and muscles.
Transforming Clinical Neurophysiology Diagnostic Services to Deliver 18 Weeks
6
2004
-05
2004
-05
2003
-04
2002
-03
2001
-02
2000
-01
1999
-00
1998
-99
1997
-98
1996
-97
1995
-96
1994
-95
1993
-94
1992
-93
1991
-92
1990
-91
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
GeneralPractice
Orthopaedics andRheumatology
Psychiatry
Ophthalmology
Paediatrics
Neurosciences
Other
Medicine
Figure 1: The changing contributions of referring specialties to clinical neurophysiology at Kentand Canterbury Hospital, a typical DGH. (Neurosciences include neurology, and may bereferred to by the latter term in other trusts). Numbers of tests have increased over the period,so a smaller proportion of referrals does not necessarily imply a reduction in number of tests.
2 Further details can be found in Annex 1

It is used to investigate, for example,focal neuropathies such as carpaltunnel syndrome, or generalisedneuropathies.
� Electromyography (EMG) is aninvasive procedure, involvinginsertion of a specialised needle intomuscle, which investigates the causesof muscle weakness and a variety ofdisorders affecting the nervoussystem.
� Evoked Potentials (EP) Visual,Brainstem Auditory and Somatosensoryare potentials produced by the brain inresponse to specific stimuli, for examplea flashing light, sound, or electrical
pulse. They are used to assess thefunction of nerve pathways, especiallyin some neurological disorders such asMultiple sclerosis and optic nervedisorders.
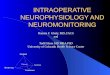
6. Clinical neurophysiology services arecommonly commissioned from the acutesector and most of the tests are providedfor outpatients, although some areprovided for patients from other Trustsand for patients directly referred fromprimary care, usually for suspected carpaltunnel syndrome. A range of services arealso provided for inpatients. A typicaldivision of workload is shown in Figure 2.
Transforming Clinical Neurophysiology Diagnostic Services to Deliver 18 Weeks
7
Inpatients20%
Primary Care15%
Outpatients65%
Figure 2: A diagram representing the division of workload in a typical clinical neurophysiologydepartment in a DGH.

7. Demand for EMG and NCS has beensteadily increasing over the past 10 years,whereas the number of requests for EEGand Evoked potentials has not changedsignificantly over the same period3.Currently there is variable accessibility toclinical neurophysiology services, evidenceof long patient waits and variableoutcomes.
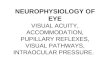
8. To transform clinical neurophysiologyservices, there is a need to improve timelyaccess to services of the highest quality,through innovative work practice in strongmultidisciplinary teams based in a range ofsettings for the tests listed. Figure 3 showsan illustration of the relationship betweenrequest, diagnostic test and workforce,which are all interdependent.
8
Figure 3: A diagram showing the relationship between requesting speciality, diagnostic testand workforce in a clinical neurophysiology department.
Neurology, Orthopaedics, General Practice etc.
EMG/NerveConduction
Delivered for the PATIENT by a
MULTIDISCIPLINARY TEAM (MDT)
comprised of:● Clinical Physiologist (Neurophysiology)
● Consultant Clinical Neurophysiologist● Administrative and Clerical Staff
Neurology, Paediatrics, General Practice etc. Neurology, Ophthalmology etc.
EvokedPotentialsEEG
3 Data and indications from a number of NHS clinical neurophysiology departments

Scale of the challenge
9. Clinical neurophysiology departments playa key role in the investigation ofpresenting symptoms in a number ofdisease areas and for a number ofdifferent specialities as outlined earlier.Details of incidence and prevalence ofcommon conditions where clinicalneurophysiology tests are utilised areshown in Figure 4 and imply that a totalof over 2 million people in England have acondition which could potentially benefitfrom investigation with approximately 400
new cases per 100,000 populationincident each year. Service providers andcommissioners should draw on thisinformation to develop an understandingof the needs of their local populations andto enable them to plan appropriately.References for this data in this table canbe found in Annex 2.
10. Although the demand for clinicalneurophysiology services has beenincreasing, the 2006-7 intervention rate(number of tests per 1,000 population) forperipheral neurophysiology in England is
Transforming Clinical Neurophysiology Diagnostic Services to Deliver 18 Weeks
9
Condition Incidence(New cases per year per100,000 population)
Prevalence (Cases per 100,000 ofpopulation)
Approximate TotalNumbers (UK)
Primary Test used forinvestigation ofcondition
Carpal TunnelSyndrome (1)
Women – 193Men – 88
7,000–15,000 600,000 NCS
Ulnar mono-neuropathy (1)
Men – 25Women – 19
N/A N/A NCS/EMG
Epilepsy (2,3) 49 500 182,750–425,000 EEG
Inherited Neuropathy(4)
N/A 40 23,600 NCS/EMG
Acquired Neuropathy(5,6)
69 2,400 N/A NCS/EMG
Motor NeuroneDisease (7,8)
1-2 4-6 4,000 NCS/EMG
Multiple Sclerosis (9) 3.4 95 52,000–62,000 EPs
NeurologicalSymptoms withoutdefined disease (10)
75 N/A 750,000 Any Test
Figure 4: A table showing the main drivers of demand for clinical neurophysiology services(references can be found in Annex 2).

only 2.74, with other countries reportingrates of between 4 and 10. The reasonfor the international rates being highercan be related to a number of factorsincluding a larger workforce in clinicalneurophysiology, a greater proportion ofprivate providers, the existence of a fee forservice system and greater historical use ofambulatory diagnostics. However, to meetthe changing prevalence and incidence ofconditions where the investigations mayplay a useful role the current interventionrates may need to increase, based on therequirements of local populations andcommissioning agreements.
Clinical neurophysiology and 18 weeks
11. The 18 week access target is differentfrom previous waiting time targets and willdirectly impact on clinical neurophysiologydepartments. Instead of focusing on asingle stage of treatment (such asoutpatients or inpatients), the 18 weekpathway addresses the whole patientpathway from referral to the start oftreatment. Diagnostic services in generaland clinical neurophysiology services inparticular have developed long waits andhave had less attention placed on them,but the 18-week patient pathway shines a
Transforming Clinical Neurophysiology Diagnostic Services to Deliver 18 Weeks
10
0
5,000
10,000
15,000
20,000
25,000
30,000
35,000
Sum of 26 + Weeks
Sum of 13 - 26 Weeks
Sum of 7 - 13 Weeks
Sum of 0 - 6 Weeks
May
-07
Apr-07
Mar-
07
Feb-
07
Jan-0
7
Dec-0
6
Nov-0
6
Oct-06
Sep-
06
Aug-0
6Ju
l-06
Jun-
06
Figure 5: A chart showing the change in the number of waiters for peripheral neurophysiologytests between June 2006 and May 20075.
4 Department of Health Diagnostics Census Data from 20065 Monthly Diagnostic Census from June 2006 to May 2007 – Department of Health

Transforming Clinical Neurophysiology Diagnostic Services to Deliver 18 Weeks
11
light on this so called “hidden wait”requiring service providers andcommissioners to think and act differently.
12. In January 2006 a monthly diagnostic datacollection was introduced for all peripheralneurophysiology tests (NCS and EMG)which revealed the extent of the waits.Over the last year, there has been areduction in the number of long waiters inclinical neurophysiology, but there remainover 20,000 people on waiting lists, with4,000 of those waiting over 26 weeks.Figure 5 shows the waiting list profileoverthe last year for peripheralneurophysiology tests, and Figure 6 breaksthe number of waiters in May 2007 down
by SHA, demonstrating the extent of thevariation across the country.
13. The quarterly diagnostic census alsocollects waiting time data on a greaterrange of clinical neurophysiology tests andreveals that there are also long waits inother parts of the service, particularly EEG(with 1,250 patients waiting over 6 weeksin March 2007).
14. The Operating Framework for the NHS for2007/08 set milestones for providerorganisations to achieve in advance of theDecember 2008 target, which re-emphasise the need for continued andsustained improvement in clinicalneurophysiology diagnostic services.
0
500
1,000
1,500
2,000
2,500
3,000
3,500
4,000Sum of 26 + Weeks
Sum of 13 - 26 Weeks
Sum of 7 - 13 Weeks
Sum of 0 - 6 Weeks
Yorkshireand
Humberside
WestMidlands
SouthWest
SouthEast
Coast
SouthCentral
NorthWest
NorthEast
LondonEast ofEngland
EastMidlands
Figure 6: A chart showing the regional variation, by SHA, in the number of waiters forperipheral neurophysiology tests in May 2007.

15. The key milestones to be achieved by theend of March 2008:
� >85% of pathways where patients areadmitted for hospital treatments shouldbe completed within 18 weeks
� 90% of pathways that do not end in anadmission should be completed within18 weeks
� 6 weeks maximum wait for alldiagnostic tests (whether as part of 18week pathways or provided as directaccess services).
16. These milestones will require a significantreduction in the current long waits in thesystem and are a significant challenge tothe NHS as a whole. Clinicalneurophysiology departments will need toundertake appropriate planning to makesure capacity is available both to clearcurrent backlogs and to operate asustainable low wait service in the future.
Purpose of this document
17. This good practice guidance document islargely based on the experiences of DHNHS Physiological MeasurementDevelopment Sites6 and other NHS sitesand services that have demonstratedimprovements and tested innovative
delivery models and solutions to improvingaccess and reducing waits for clinicalneurophysiology services during 2006/07,together with the work of a ClinicalNeurophysiology Leadership Group(CNLG)7.
18. Good practice in clinical neurophysiologyservices as outlined in this document will:
� Challenge existing practice andpathways so that patient outcomes andexperience are improved
� Maximise transformational changeopportunities within provider units sothat service meets patient needs
� Minimise risks to patients and staff intaking forward change
� Utilise service improvement techniques
� Support commissioners to deliver 18weeks across all care pathways.
19. Implementing good practice models willhelp to deliver a high quality service, inwhich staff are competent to undertakeinvestigations appropriately in differentialdiagnosis. Results are interpreted correctlyand the workforce is equipped andcompetent to deliver services in a varietyof settings, with clinical leadership drivinginnovation, redesign and sustainability.
Transforming Clinical Neurophysiology Diagnostic Services to Deliver 18 Weeks
12
6 A list of the Development Sites, the ideas they tested and sources of other ideas is provided in theAcknowledgements. Full case studies from each development site are available on the 18 weeks website.
7 A group of representatives from the British Society of Clinical Neurophysiology (BSCN) and theElectrophysiological Technologists Association (EPTA)

13
How toachieve thevision and context
20. Clinical neurophysiology services may betransformed by using existing knowledgeabout improving NHS systems andprocess, bringing together evidence aboutinnovative technology and providing thetraining to enable a competent productiveworkforce to deliver the right processes atthe right skill level (all shown in Figure 7).Each of these key themes is coveredseparately in the following paragraphs.
Systems and processes21. A substantial amount of additional
capacity can be realised by improvingsystems and processes within clinical
neurophysiology departments. Thefollowing paragraphs detail how benefitscan be gained from collecting data,understanding capacity, managingdemand, booking patients and carryingout lean analysis.
Collect data about clinicalneurophysiology services
22. Providers and commissioners are requiredto submit data to the Department ofHealth on a monthly basis for allperipheral neurophysiology tests8 and on aquarterly basis for all other clinicalneurophysiology tests9.
Matchingworkforce skills
and competencesto improving working
practices
Realising thebenefits of
new technology
Making systemsand processes
lean and efficient
Improving the patientexperience and providingbetter access to clinical
neurophysiology services
PATIENT
Figure 7: The key delivery levers for achieving the vision for clinical neurophysiology services.
8 Data can be accessed at http://www.performance.doh.gov.uk/diagnostics/index.htm 9 DH Review of Central Returns (ROCR) reference number: ROCR/OR/0168/FT6/001

23. Many clinical neurophysiologydepartments have poor data managementsystems and are not designed to capturethe information required to inform the 18week diagnostic collection. Improvementin this key area is likely to make asignificant difference to delivery and alsoto the ability of individual departments tounderstand their service and plan for thefuture, although relatively simple softwaresolutions can be introduced which wouldimprove the current situation.
24. In order to understand the scale of thechallenge for NHS services, commissionersshould work with providers to ensure they:
� Collect and analyse demand data,against agreed lists, in order todetermine the rate of referral, and to beaware of demand changes
� Maintain data sets, which record thetype of referral, referral source includingspeciality, referral date, appointmentdate, attendance record, and waiting/clearance times.
Understand capacity
25. Commissioners and providers should havean understanding of the capacity of theirdepartments. Choose and Book willrequire clinical neurophysiologydepartments to understand their
“production function” – i.e. the numberof tests they can theoretically carry out,related to specific numbers of slots in abooking schedule.
26. In order to fully understand a servicecapacity and how it relates to demand forclinical neurophysiology services, providersneed to:
� Understand demand for the service andwhere it comes from
� Know the number of diagnosticsessions and slots available for each test
� Utilise and analyse data to informservice redesign and models ofprovision to ensure that access isimproved and that patient flow isbalanced into and out of the service.
27. A Physiological Measurement 18 WeeksProductivity Tool10 has been madeavailable (a screenshot is shown in Figure8), which uses a number of simple inputsto allow an estimate to be made ofdepartmental capacity. It then calculatesclearance times based upon the services’current waiting list and an estimate ofpotential efficiency gains to be made. Thetool assists with the two stage process of:
� Clearance of current backlog
� Maintenance of a stable schedule for a“low wait” diagnostic service.
Transforming Clinical Neurophysiology Diagnostic Services to Deliver 18 Weeks
14
10 The tool can be found at:http://www.18weeks.nhs.uk/public/default.aspx?main=true&load=ArticleViewer&ArticleId=945

Transforming Clinical Neurophysiology Diagnostic Services to Deliver 18 Weeks
15
Figure 8: The Physiological Measurement 18 Weeks Productivity Tool: Simple inputs areentered regarding the length of each test and operational time available. Chart 1 shows thetheoretical throughput in terms of tests using this information. Chart 2 shows a percentageincrease from current activity. Both charts update automatically as inputs are altered, to modelhow extra capacity could be released.

28. If there is insufficient capacity to see therequired number of patients in the timeavailable, contingency measures may needto be implemented. These could include:
� Creating additional capacity byincreasing the hours of operation – thisis the most effective way of increasingcapacity for marginal cost and alsopotentially provides appointment slotswhen it is more convenient for patients(i.e. evenings and weekends)
� Validation to exclude duplicates e.g.those that have been seen, no longerneed care or have died
� Pooling of patients into single listswhere possible
� Agreements with neighbouring trusts
� Exploring options with the independentsector.
Manage demand, including introducingreferral criteria
29. Patients are likely to present to primarycare with a range of symptoms, whichmay suggest a possible condition thatcould be determined by carrying out aclinical neurophysiology test. The table inFigure 9 sets out a summary of commonpresentations and associated tests andmay be used by primary care practitioners
to inform patient assessment and referral.Standardised referral criteria across anetwork can assist with consistency andensuring best use of valuable resources.This could be built into local referraldocumentation which includes otherrelevant information relating to the patientwhich will further help to establish therange of tests that may need to beundertaken and the requirement for inputby different members of themultidisciplinary team in clinicalneurophysiology.
30. From the end of July 2007, primary careproviders are able to select clinicalneurophysiology tests via the Choose andBook Directory of Services. The Chooseand Book form for clinical neurophysiologyis included at Annex 3 and demonstratesthe type of information that can help tomake an effective referral. The forms canalso be found on the Choose and Bookwebsite11.
Transforming Clinical Neurophysiology Diagnostic Services to Deliver 18 Weeks
16
11 http://www.chooseandbook.nhs.uk/staff/implementation

* sf: Single Fibre** SSEP: Somatosensory Evoked Potential
Note. Patients’ present with symptom complexes [column 1]; diagnoses are made on the basisof the test as above and a clinical opinion
Figure 9: A table showing the usefulness of clinical neurophysiology for common symptomgroups to provide a guide for primary care.
Transforming Clinical Neurophysiology Diagnostic Services to Deliver 18 Weeks
17
PRESENTATION LIKELY CONDITIONS USEFULNESS OF CLINICALNEUROPHYSIOLOGY
APPPROPRIATE TESTS TOUSE
Tingly Fingers Carpal Tunnel Syndrome (CTS) High NCS
Ulnar Neuropathy High NCS/EMG
Radiculopathy Medium NCS/EMG
Sensory Loss Neuropathy High NCS/EMG
Inherited Neuropathy Medium/High NCS/EMG
Acquired Neuropathy High NCS/EMG
Elderly Patients Neuropathy Low/Medium NCS/EMG
Diabetic Patients Neuropathy Low NCS/EMG
Weakness Motor Neurone Disease High NCS/EMG
Myopathy High NCS/EMG
Myasthenia High EMG/sfEMG*
Spinal Disease Medium EMG/SSEP**
Disorders of Consciousness Epilepsy High EEG
Non-Epileptic Attack Disorder High EEG
Sleep Medium EEG
Coma Medium EEG
Migrane Low EEG
Syncope Low EEG

31. Most clinical neurophysiology diagnosticsare provided following an outpatientconsultation with a specialist within theacute Trust setting, and a significantamount of acute inpatient work alsooccurs on a daily basis. Improved access todiagnostic tests directly from primary careis also essential, assuming agreed referralcriteria are in place. Effective referralcriteria will support the management ofthese various sources of demand and are akey element of service transformationprocesses. They help to support not onlyequitable provision, but also ensure thatpatients with defined symptoms flow intothe most appropriate service.
32. The Royal Free Hampstead NHS Trusthave developed and implemented areferral protocol with local GPs,encouraging direct access into services, asdetailed in the following case study.
33. The information in the case study aboveshows what it is possible to achieve andneeds to be used with the existing referralcriteria developed for specific tests toensure the development of appropriatethresholds for referral into clinicalneurophysiology departments.
CASE STUDY: THE ROYAL FREEHAMPSTEAD NHS TRUST
“One stop clinic for ‘tingly fingers’”
The Royal Free Hampstead NHS Trustdeveloped, tested and agreed referralcriteria, with ten GP’s, which enablepatients with tingly fingers to be referredinto a one stop clinic. In the clinic, nerveconduction studies are performed by CPN’s,reported by the CCN and a treatment planmade. An appointment with an orthopaedicsurgeon in his outpatient clinic (moderateor severe CTS) or provision of splints (mildCTS) occurs on the same day as the test.
The key benefit of this model of care is thatpatients only have one appointment at thehospital instead of three, providing asuperior patient experience and lessadministration and a reduction in waitingtimes from 26 weeks to 13 weeks for theTrust, enabling more effective use ofcapacity and lower waiting times.
The referral form for this clinic isreproduced in Annex 4
Transforming Clinical Neurophysiology Diagnostic Services to Deliver 18 Weeks
18

Implement booking systems
34. Having built an understanding of capacityand demand and implemented clearreferral criteria, clinical neurophysiologydepartments may benefit fromimplementing booking systems, whichcould consist of:
� A booked in advance service tooutpatients, rather than an ad hoc ondemand service, which is an inefficientuse of staff time
� Improved management of DNAsthrough a clear and consistently appliedDNA policy and booking at short noticeinto cancelled slots
� Innovative ways of calling patients forappointment and reminding them ofthe date.
35. Effective booking will be achieved ifadequate patient information is includedon the referral form. This will help tospeed up processing and ensure any teststhat are required can be completedwithout delay, including reporting andinterpretation, to support informed clinicaldecision making.
36. Booking systems can also be improved by:
a) Reviewing existing internal paper-basedreferral systems and redesigning themto enable all bookings to be made
chronologically by date of referral andnot date received by the department
b) Validating all waiting lists to eliminateany duplicate entries, to free upcapacity which otherwise would be lost.
37. Scheduling or booking arrangementsshould be as efficient as possible and allavailable capacity appropriately managedand utilised where possible by dedicatedadministrative staff, as outlined in the casestudy below.
38. Clinical neurophysiology services areencouraged to introduce a patient trackinglist (PTL) to manage reductions in currentwaiting lists, and to work towards a
CASE STUDY: PENNINE ACUTE TRUST(NORTH MANCHESTER GENERALHOSPITAL)
“Use of administrative and clerical staff tomanage waiting lists on a day to day basisand drastically reduce DNA rates”
Pennine Acute Trust transferredresponsibility for waiting list managementfrom clinical physiologists to suitably trainedadministration staff; this allowed moreproductive use of clinical physiologist time.Partial booking and strict rules on DNAswere also introduced, which resulted in adecrease in the DNA rate from 18% tobetween 3-5%, and a measured increase inclinical capacity.
Transforming Clinical Neurophysiology Diagnostic Services to Deliver 18 Weeks
19

complete pathway approach from GPreferral to start of treatment. Guidance onthe implementation of PTLs is available onthe 18 weeks website12.
Implement lean solutions
39. There are advantages in the use of “Lean”process methodology. Lean is an approachto improve flow and eliminate waste thatwas developed by Toyota. Lean is aboutgetting the right things to the right place,at the right time, in the right quantities,while minimising waste and being flexibleand open to change. Service modelimprovement stems from adopting a leansystem design approach and fully usingthe resources that are available in clinicalneurophysiology departments. A majorway to achieve improved use of resourcesis to undertake a local process mappingexercise13. This could lead to improvedworkflow, better understanding and use ofpatient management systems and greaterefficiency of all staff, with better teamworking14.
40. Lean solutions may hinge on moreeffective ways of working, for example byimplementing measures to maximise useof clinician time, as illustrated in thefollowing case study.
Technology41. Embracing the benefits of new technology
is critically important in delivering servicesfor 21st century healthcare as highlightedby the Health Industries Taskforce15.
IT Solutions for Clinical Neurophysiology
42. Clinical neurophysiology departmentsutilise a range of IT systems and there isno consistent approach across sites. Somedepartments have developed innovativeapproaches to managing information, suchas in the case study below:
CASE STUDY: THE ROYAL FREEHAMPSTEAD NHS TRUST
“Process mapping of patient journeys forCarpal Tunnel Syndrome (CTS)”
The Royal Free Hampstead carried outprocess mapping of the patient journey forCTS. This enabled staff to identify wheredelays occurred and to improve bothadministration of appointments, referralcriteria and offer direct access to GP’s. Thepatient pathway was reduced to onehospital visit, including an outpatientconsultation with an orthopaedic surgeonand NCS for the investigation of CarpalTunnel Syndrome.
Transforming Clinical Neurophysiology Diagnostic Services to Deliver 18 Weeks
20
12 Full details about the PTL methodology can be found at http://www.18weeks.nhs.uk/public/default.aspx?load=ArticleViewer&ArticleId=947
13 Several development sites have undertaken this exercise14 http://www.institute.nhs.uk/ServiceTransformation/Lean+Thinking/15 DH Strategic Implementation Group, Health Industries Taskforce ‘Innovation for health: making a difference

Transforming Clinical Neurophysiology Diagnostic Services to Deliver 18 Weeks
21
CASE STUDY: EAST KENT HOSPITALS NHS TRUST
“Electronic diary and record keeping database”
The clinical neurophysiology department at Kent & Canterbury Hospital has developed andrun an electronic diary and record keeping database since 1989. In developing these, cleardistinctions were made between the two types of computer systems used in clinicalneurophysiology.
� Administrative system used for appointment scheduling, report writing, record storage,management audit and research
� Technical software embedded in the equipment which performs the tests.
The administrative system is the hub and links to other hospital IT systems and the equipmentin the department as illustrated in Figure 10, which shows the system links enabling allrecordings made in the department to be accessed directly from within the administrativedatabase (by loading whichever software is appropriate to the recording and retrieving theactual data from storage and passing it to the viewer software). The need for specialistsoftware, for the viewing of EEG for example, restricts the availability of this facility elsewherein the trust, though EEGSYS itself can be accessed from anywhere on the network by staffwith the appropriate rights.
Figure 10: Diagram to illustrate the electronic system in use in the clinical Neurophysiologydepartment at Kent and Canterbury Hospital and how this is linked to other systems.
E E G S YS
DOCUME NTMANAG E ME NT(NE UR OL OGY)
CT S S UR G E R Y(P R IMAR Y CAR E )
E E G S YS T E M 3(MICR OME D)
E MG S YS T E M(DANT E C)
WE B B AS E DB OOK ING
CHOOS E andB OOK ?
Func tional
Work ing but c ould be
enhanced
Under deve lopment
P ASE E G S YS T E M 1
(VIAS YS )
E E G S YS
DOCUME NTMANAGEME N T(NEU RO LOG Y)
CT S S UR G E R Y(PR IMAR Y CAR E )
E E G S YS T E M 3(M ICROMED)
E MG S YS T E M(DANT E C)
WE B B AS E DBOOKING
CHOOS E andBOOK ?
Func tional
Working but could be
enhanced
Under development
P ASE E G S YS T E M 1
(VIASYS )
EEG/EMG/EPSYSTEM (NIHON
KODEN)
Demographic data
Clinic letters/AppointmentsReports
Reports
Surgery notes
App
oint
men
ts
EEG re
cord
s
Test data
DemographicsTest Data

New technology
43. There are several areas where newtechnology has the potential to improveclinical neurophysiology services.
44. New multifunctional digital equipmentthat combines nerve conduction studies,electroencephalography and evokedpotentials allow distinct flexibility inservice. Each clinical neurophysiology test
requires a specific function from theequipment and an appropriately located orscreened room to undertake the test,therefore, only one investigation can beperformed at a time. The ability to carryout multiple investigations in the sameroom has the potential to increasethroughput and efficiency. Figure 11shows a combined NCS/EEG/EP system.
Transforming Clinical Neurophysiology Diagnostic Services to Deliver 18 Weeks
22
The benefits of this system include:
� Immediate access from the neurology clinic to clinical neurophysiology reports
� Clinical neurophysiology investigations can be requested directly from the clinic, anappointment offered, agreed with patient and a subsequent follow up appointmentmade
� The clinical neurophysiology department can access clinic letters if more clinicalinformation is needed at the time of the investigation
� Monitoring activity levels in department
� Referral management
� Service development
� Manpower planning
� Audit and research.
While this case study demonstrates the value of an IT hub for streamlining systems andprocesses, the diagram illustrates that more work is required to provide the functionality toenable test results to be directly obtained from the equipment it is generated on and for thisinformation to be uploaded in the form of a clinical and technical report for use in differentialdiagnosis.

Figure 11: An example of multifunctionalequipment used for NCS/EEG and EP.
45. Use of computer technology to record theresults of EEGs and video clips of clinicalevents have allowed the interpretation ofthe results at a remote site, enabling fasterinterpretation of results, leading tospeedier diagnosis and treatment for thepatient. Benefits of this technologyinclude:
� Faster reporting
� Records forwarded to competentneurophysiological interpreter ratherthan waiting for him/her to visitlocation
� Ability to audit across widerareas/regions
� Improved access for patients’ sinceEEGs can be recorded outside usualdepartments closer to patient.
46. The bandwidth requirements for thistechnology are significant, so it isnecessary to ensure that the appropriateprovision of IT hardware and support forusers and receivers are present.
47. The widespread use of inexpensive digitalvideo with EEG and the advent of cheapdigital storage for large volumes of datahave greatly aided the analysis of clinicalevents during recording. Some of thelatest advances include the introduction ofportable equipment built around a laptopcomputer. This equipment can be used ina variety of locations, including close tothe patient by appropriately trained andcompetent practitioners. An example of aninterface is shown in Figure 12.
Transforming Clinical Neurophysiology Diagnostic Services to Deliver 18 Weeks
23

48. There has been a distinct trend over pastyears for medical equipment to becomesmaller and more portable, increasing theease of use in community or mobile caresettings. Specifically in clinicalneurophysiology (particularly in the USA)several hand held devices for quick andsimple carpal tunnel testing have recently
been marketed. Some have been validatedagainst conventional NCS and givereasonable results16. However, they arelimited in the range of measurements theycan make, and their absolute accuracy andclinical utility is still being fully evaluated.The technology requires furtherassessment, but should be kept under
Transforming Clinical Neurophysiology Diagnostic Services to Deliver 18 Weeks
24
Figure 12: An example of a digital EEG interface.
16 Detail of the Mediracer device can be found in: Acta. Neurol. Scand 2007: 115: 390-397

review given its potential use in primarycare. For other types of equipment used inclinical neurophysiology there is likely tobe a limited improvement in portabilitydue to the technical complexity of theequipment involved.
Implementation of new technology
49. Challenges faced within organisationsinclude the need to break withtradition/culture and apply a way ofworking that continues to look for a betterway to deliver services to patients. Thismeans keeping abreast of changingtechnology, not only for its potential totransform patient care but also for theopportunities and challenges it raises forworkforce development. Associated withthe introduction of all new technology isthe need for standards and protocols fortests and reporting to ensure that highquality and safe services are provided forpatients. Specifications for clinicalneurophysiology tests will be published inthe near future on the 18 weeks website.
WorkforceClinical neurophysiology workforce profile
50. In every part of the NHS, the workforce iscritical in implementing effective serviceswith plans needing to be affordable andsupported by significant role redesign, skillmix and productivity gains. There is a largevariation in clinical neurophysiologystaffing per unit population and per unitproductivity. This leads to wide ranging
service models, with different levels ofcare for patients.
51. Clinical neurophysiology diagnostics areperformed by a small multidisciplinaryteam comprising of medical staff, clinicalphysiologists and support workers andadministrative and clerical staff withvariation in the level of staff whoundertake specific functions within anindividual department. There are variationsnationally in staffing levels and workforceprofiles and even departments with similarstaffing levels and case mix do not alldeliver the same level of activity.
52. Reducing waits in clinical neurophysiologyin a sustainable way to meet themilestones and achieve the access targetsfor 2008 will require a fundamentalchange in the way the multidisciplinaryteam work together. Multidisciplinaryworking in clinical neurophysiology hastraditionally involved Clinical Physiologistsin Neurophysiology [CP(N)s] performingEEGs and EPs, with Consultant ClinicalNeurophysiologists [CCNs] interpretingresults in relation to the clinical problem,as well as performing nerve conductionstudies and EMG
53. Opportunities for development of CP(N)sand other members of the non-medicalworkforce team in clinical neurophysiologyneed to be fully exploited in amultidisciplinary approach (whereCCNs are often the clinical lead) for anumber of reasons:
Transforming Clinical Neurophysiology Diagnostic Services to Deliver 18 Weeks
25

� CCNs are limited in number (with onlylow levels of growth expected in thecoming years), requiring their specialistskills to be used effectively.
� CP(N)s have extensive skills andknowledge that could be furtherdeveloped, enhancing their role and thetasks they can perform as part of amultidisciplinary team.
� Current capacity issues (and longwaiting times) in clinicalneurophysiology are often cited to beworkforce related rather than a lack ofsuitable equipment or clinic space.
New Roles
54. A range of new and extended workforceroles have emerged recently in clinicalneurophysiology, many of which havebeen tested within the development sitesand other hospitals to support innovativesolutions to address the long waits.These are summarised in Figure 13 andare related to some of the pathwaysdeveloped around peripheralneurophysiology but do not coverthe whole pathway. However theydemonstrate the use of developing andexpanding the roles of the workforce andutilising skill mix to achieve a morestreamlined service.
55. The introduction of assistant and associatepractitioner and other support roles meansCP(N)s can be freed up from routineduties to undertake other specialistprocedures such as ulnar nerveneuropathy and peripheral neuropathynerve conduction studies, and intra-operative monitoring (IOM).
CASE STUDY: IPSWICH HOSPITAL NHSTRUST
“Increase throughput by maximisingclinician time for NCS clinics”
To utilise Consultant time effectively staff atIpswich Hospital ran parallel clinics forperipheral neurophysiology with 2 CP(N)sperforming nerve conduction studies andone CCN supervising and performing EMGif indicated. One clinic was for CTSscreening and one clinic for complex NCV,which may need EMG. This allowed 10patients instead of 5 to be seen in asession. If the CCN was free, they reportedon EEG’s in any available time betweenpatients. This enabled maximum use ofvaluable but scarce CCN time in adepartment with no full time consultantcover.
Transforming Clinical Neurophysiology Diagnostic Services to Deliver 18 Weeks
26

Transforming Clinical Neurophysiology Diagnostic Services to Deliver 18 Weeks
27
Neu
roph
ysio
logi
cal
inve
stig
atio
n N
ew/e
xten
ded
role
Im
pact
Si
tes
test
ed
Oth
er s
ites
usi
ng
this
mod
el
Adm
inis
trat
ion
and
pati
ent
care
Adm
inis
trat
ion
& C
leric
al S
taff
Ass
ista
nt/S
enio
r A
ssis
tant
Clin
ical
Phy
siol
ogis
ts(N
euro
phys
iolo
gy)
Impr
oved
wai
ting
list
man
agem
ent
Rem
ovin
g ad
min
istr
atio
ndu
ties
from
mor
e se
nior
sta
ff
Prep
arin
g ro
oms
and
patie
nts
for
test
s
Patie
nt c
are
with
in d
ept
Nor
folk
& N
orw
ich
Uni
vers
ityH
ospi
tal N
HS
Trus
t
Penn
ine
Acu
te N
HS
Trus
t
Ipsw
ich
Hos
pita
l NH
S Tr
ust
NC
SC
arpa
l Tun
nel S
cree
ning
(C
TS)
Band
5 C
linic
al P
hysi
olog
ists
(Neu
roph
ysio
logi
sts)
Fo
cus
prov
isio
n of
CTS
NC
Sby
clin
ical
phy
siol
ogis
ts f
reei
ngup
tim
e fo
r th
e C
CN
Incr
ease
d ca
paci
ty
Dec
reas
e w
aitin
g tim
es
UH
B N
HS
Foun
datio
n H
ospi
tal
Trus
t
East
Ken
t H
ospi
tals
NH
S Tr
ust
Maj
ority
of
Clin
ical
Neu
roph
ysio
logy
dep
ts a
reno
w u
sing
thi
s m
odel
NC
SU
lnar
and
Per
iphe
ral n
erve
Scre
enin
g
Band
6/7
Clin
ical
Phy
siol
ogis
ts(N
euro
phys
iolo
gy)
In c
onju
ncti
on w
ith
CC
N
Focu
s pr
ovis
ion
of N
CS
bycl
inic
al p
hysi
olog
ists
CC
N in
volv
ed o
nly
if EM
Gre
quire
d
Incr
ease
d ca
paci
ty
Dec
reas
e w
aitin
g tim
es
Uni
vers
ity H
ospi
tal o
f N
orth
Staf
fs N
HS
Trus
t
Pool
e H
ospi
tal N
HS
Trus
t
e.g.
City
Hos
pita
l Birm
ingh
amH
amm
ersm
ith H
ospi
tal N
HS
Trus
t
EP a
nd I
OM
Inv
esti
gati
ons
Band
7/8
a C
linic
alPh
ysio
logi
sts
perf
orm
low
ris
kan
d ro
utin
e ca
ses
Free
ing
up t
ime
for
the
CC
Nto
foc
us o
n m
ore
com
plex
case
s
Nor
folk
& N
orw
ich
Uni
vers
ityH
ospi
tal N
HS
Trus
tR
oyal
Fre
e H
amps
tead
NH
STr
ust
Uni
vers
ity H
ospi
tal o
f N
orth
Staf
fs N
HS
Trus
t
Rep
orti
ng o
f EE
Gan
d N
CS
Band
7C
linic
al P
hysi
olog
ists
(Neu
roph
ysio
logi
sts)
In c
onju
ncti
on w
ith
CC
N
Prov
isio
n of
clin
ical
rep
orts
for
EEG
/EP’
s an
d N
CS
for
CTS
insi
mpl
e, r
outin
e ca
ses
Red
uced
wai
ting
times
for
rout
ine
repo
rts
Uni
vers
ity H
ospi
tal o
f N
orth
Staf
fs N
HS
Trus
te.
g.C
ity H
ospi
tal B
irmin
gham
Ham
mer
smith
Hos
pita
ls N
HS
Trus
t
Figu
re 1
3: T
able
sho
win
g ex
tend
ed r
oles
of
the
clin
ical
neu
roph
ysio
logy
wor
kfor
ce a
s te
sted
by
phys
iolo
gica
lm
easu
rem
ent
deve
lopm
ent
site
s.

56. The impact of developing extended rolesfor CP(N)s, for example in clinicalreporting of EEGs and carrying outperipheral neurophysiology examinations,can be clearly demonstrated in thefollowing two case studies:
57. Integral to these two case studies is theneed for CP(N)s to acquire the rightskills and competences via appropriateeducation and training that underpins theknowledge required and which progressesconsistent clinical governance. Thiseducation needs to be similar to the leveland type of training undertaken bymedical staff who may have traditionallyundertaken these roles.
CASE STUDY: UNIVERSITY HOSPITALS OFNORTH STAFFORDSHIRE NHS TRUST
“Introduction of new and extendedworkforce roles”
North Staffordshire Trust’s ClinicalGovernance Board approved CP(N) toautonomously report NCS carpal tunnelsyndrome studies, normal EEGs and evokedpotential (EP’s) investigations.
In addition a further extension to the CP(N)role is to perform NCS in ulnar neuropathiesand peripheral nerve studies. There is noroutine input from the consultant althoughclinical opinion is being provided by medicalstaff in the early stages of the project.
Use of Senior Assistant Clinical Physiologystaff since 2003/4 to manage bookings andday to day coordination of the departmentfurther releases specialist staff toconcentrate on more complex work and thedevelopment of extended role practitioners.CASE STUDY: POOLE HOSPITAL NHS
TRUST
“Clinical Physiologist (Neurophysiology)led ulnar neuropathy clinics”
Poole hospital has implemented a CP(N) ledulnar neuropathy clinic since July 2006 witha period of clinical physiologist trainingprovided by the consultant clinicalneurophysiologists. Standards are constantlymonitored with consultant re-examinationavailable if requested by the CP(N). Waitingtimes for a consultant led clinic droppedfrom a maximum of 26 weeks to 10 weeksover a 9 month period and waits for aCP(N) led ulnar clinic are now 6 weeks.
CASE STUDY: NORFOLK AND NORWICHUNIVERSITY HOSPITAL NHS Trust
“A review of workforce functions toincrease productivity”
At Norfolk and Norwich, generalhousekeeping duties, patient care andadministrative tasks are performed by anAssistant Clinical Physiologist (ACP) atAgenda for Change Band 2 or 3. Thisreleases time for other staff to carry outtests and has resulted in increasedthroughput of patients by 10 per week.
Transforming Clinical Neurophysiology Diagnostic Services to Deliver 18 Weeks
28

58. Extended and new roles for CP(N)s willneed to continually evolve and developfurther to include more complex peripheralneurophysiology as outlined in Figure 14.The skills to perform these extended roleswill require the attainment of thenecessary competencies developed incollaboration with CCNs who provide aclinical opinion based on both clinicalneurophysiological data and the patient’sclinical presentation. Through the creationof a truly multidisciplinary team, based onskills and comparable competences, therewill be the opportunity to deliver therequired range of tests and an enhanced,high quality service for patients.
59. Creative approaches to training anddevelopment will need to be developedin order to achieve flexibility in theworkforce, which may include use of e-based learning opportunities and anetwork wide approach to training.In addition, clinical supervision andgovernance arrangements need to beput in place for all levels of staff.
Leadership
60. There is strong evidence from theorganisations cited in this document thatone of the biggest success factors is dueto inspirational leadership and a ‘can-do’attitude. To achieve major change inworkforce transformation, strong clinicaland managerial leadership is essential.
61. Clinicians and managers play a key rolein discussing how the service can beprovided and it is important that allproviders are involved in discussionsrelating to future provision.
62. Senior departmental staff have anopportunity to shape the local agenda bycontributing to clinical neurophysiologynetwork diagnostic groups to share goodpractice and agree locally negotiatedsolutions to current and future challenges.
Transforming Clinical Neurophysiology Diagnostic Services to Deliver 18 Weeks
29

Transforming Clinical Neurophysiology Diagnostic Services to Deliver 18 Weeks
30
Figu
re 1
4: T
able
sho
win
g th
e cu
rren
t an
d po
tent
ial
role
s of
the
clin
ical
neu
roph
ysio
logy
wor
kfor
ce.
Proc
edur
eSt
age
of t
est
Ass
ocia
te C
linic
al P
hysi
olog
ists
Clin
ical
Phy
siol
ogis
ts,
CP(
N)s
Adv
ance
d Pr
acti
tion
er
Rou
tine
EEG
Test
and
ana
lysi
sro
utin
e pr
actic
ero
utin
e pr
actic
e
Clin
ical
opi
nion
deve
lopm
ent
oppo
rtun
ity
Prol
onge
d/co
mpl
ex E
EGTe
st a
nd a
naly
sis
deve
lopm
ent
oppo
rtun
ityro
utin
e pr
actic
e
Clin
ical
opi
nion
deve
lopm
ent
oppo
rtun
ity
Tele
met
ryTe
st a
nd a
naly
sis
rout
ine
prac
tice*
rout
ine
prac
tice*
Clin
ical
opi
nion
spec
ial i
nter
est
deve
lopm
ent
oppo
rtun
ity
Intr
aope
rati
vem
onit
orin
gTe
st a
nd a
naly
sis
deve
lopm
ent
oppo
rtun
ityro
utin
e pr
actic
e*
Clin
ical
opi
nion
spec
ial i
nter
est
deve
lopm
ent
oppo
rtun
ity
Evok
ed p
oten
tial
sTe
st a
nd a
naly
sis
deve
lopm
ent
oppo
rtun
ityro
utin
e pr
actic
e**
rout
ine
prac
tice*
**
Clin
ical
opi
nion
deve
lopm
ent
oppo
rtun
ityde
velo
pmen
t op
port
unity
NC
S (C
TS O
nly)
Test
and
ana
lysi
sde
velo
pmen
t op
port
unity
rout
ine
prac
tice
rout
ine
prac
tice
Clin
ical
opi
nion
deve
lopm
ent
oppo
rtun
ityro
utin
e pr
actic
e
NC
STe
st a
nd a
naly
sis
deve
lopm
ent
oppo
rtun
ityde
velo
pmen
t op
port
unity
Clin
ical
opi
nion
spec
ial i
nter
est
deve
lopm
ent
oppo
rtun
ity
NC
S/EM
GTe
st a
nd a
naly
sis
deve
lopm
ent
oppo
rtun
ity
Clin
ical
opi
nion
spec
ial i
nter
est
deve
lopm
ent
oppo
rtun
ity
*In
dep
artm
ents
tha
t ha
ve t
his
faci
lity
**Li
mite
d ra
nge
of t
ests
***
Com
plet
e ra
nge
of t
ests
Ass
ista
nt P
ract
ition
ers
perf
orm
a r
ange
of
task
s in
sup
port
of
othe
r pr
ofes
sion
als
incl
udin
g ch
aper
onin
g, c
lear
ing
up, e
lect
rode
car
e,or
gani
satio
n of
tra
nspo
rt a
nd s
o co
ntrib
utin
g to
the
pat
ient
exp
erie
nce.
CC
Ns
and
Spec
ialis
t R
egis
trar
s of
fer
clin
ical
opi
nons
on
test
s pe
rfor
med
by
CP(
N)s
(EE
Gs,
Evo
ked
Pote
ntia
ls a
nd N
CS)
as
wel
l as
perf
orm
ing
and
repo
rtin
g al
l asp
ects
of
perip
heria
l neu
roph
ysio
logy
tes
ts.

63. A number of symptom based 18 weekcommissioning flow pathways have beenpublished across a whole variety ofspecialties. All of these pathways areavailable to download from the 18 weekswebsite17. Pathways of relevance to clinicalneurophysiology include Blackouts; Pins &Needles and Numbness in Fingers.
64. Three additional pathways are presentedin Figures 15, 16 and 17, highlightingareas of particular concern for clinicalneurophysiology departments. A numberof service models that have beenillustrated earlier in this document formkey parts of these pathways. Theyhighlight the way forward for developinga more streamline approach for providingan efficient patient pathway within clinicalneurophysiology departments.
Key points in relation to each of thesepathways are:
� CTS pathway (Figure 15) is based on aone stop clinic to investigatepain/tingling/numbness in the hand ineither a primary or secondary caresetting and is practitioner led withreferrals directly to the clinicalneurophysiology department/provider
� Other Neurological Symptoms(Figure 16), this is similar to the CTSpathway but is adapted to offer a widerscreening service for other neurological
symptoms. Some of this may be relatedto peripheral neuropathies (in particularulnar entrapment at the elbow) andvarious types of peripheral neuropathy(i.e. diabetes), but up to 50% ofperipheral neurophysiology work canfall into categories outside these.Delivery could be in primary orsecondary locations although volumemay be restrictive and may need a CCNin addition to the CP(N)
� EEG pathway (Figure 17) provides aninitial route for the investigation ofblackouts/seizures, when a routine EEGwould be performed and, if results areequivocal, a sleep deprived appointmentoffered straight away. This could bearranged with the patient beforeleaving the department, cutting out areferral back to the specialist consultantuntil a second EEG has been done.
65. The three pathways highlight innovativeways of delivering care to patientsattending clinical neurophysiologydepartments. They emphasise a number ofkey changes that departments can maketo improve the flow of patients:
� Introduce effective referral protocols
� Provide clinical neurophysiologydiagnostic services that are tailoredfor specific groups of patients
31
Symptom based pathways
17 http://www.18weeks.nhs.uk/public/default.aspx?load=Pathways#

� Carry out assessments in advanceof specialist consultant care whereappropriate and perform further clinicalneurophysiology tests if appropriate
� Provide treatment, where possible, atthe same time as assessment.
These changes are covered in greater detail inparagraphs 66 to 69.
66. Introduce effective referral protocols:
� Referral protocols can be used toensure appropriateness of referral andstreamline patients with key conditionsincluding those with suspected carpeltunnel syndrome and suffering fromblackouts/seizures
Transforming Clinical Neurophysiology Diagnostic Services to Deliver 18 Weeks
32
CTS PathwayPrimary/Secondary Care
Symptom – Pain / tingling / numbness in hand
GP
Neurophysiology (Referralprotocol used)
Specialist Consultant insecondary care
NCS for CTS Screening
Results back toreferrer
Review byGP/Orthopaedics
Alternative pathologyFurther NCS/EMG
Results recommendations to referrerReview by GP/Orthopaedics
Further diagnostics
Mild CTS Moderate CTS Severe CTS
According to NCS results and clinical presentation:
Treatment PlanWhich includes1. No Treatment2. Splint (temporary)3. Injection (temporary)4. Surgery
Normal NCS Abnormal NCS (Not CTS) Abnormal NCS (CTS)
Figure 15: A diagram to illustrate a model pathway for CTS.

� By using the Choose and Book directoryof service referral form, primary carepractitioners should be able to identifythe pathway that the majority ofpatients will follow and choose theappropriate clinic slot.
67. Provision of clinical neurophysiologyservices that are tailored for specificgroups of patients:
� An effective model is to establish clinicsfor groups of patients. This ensures thatthe most appropriate workforce isavailable to deliver the services required
� An average of 50% of patients seen inclinical neurophysiology departmentsare attending for suspected CTS andthey can be seen in a focused clinic.This could also apply to routine EEGand be run in conjunction with aspecialist clinic (i.e. Neurology).
Transforming Clinical Neurophysiology Diagnostic Services to Deliver 18 Weeks
33
Other Neurological Symptoms PathwayPrimary/Secondary Care
Other Neurological Symptoms (NOT Tingly Fingers)
Patient referredfrom GP
Neurophysiology (Referralprotocol used)
Specialist Consultant insecondary care
Clinical Neurophysiology MedicalOpinion using appropriate test
(EMG, NCS, EEG etc.)
Referral to Neuroscience,Neurology or Neurosurgery
Results back toreferrer
Review bySpecialists
AppropriateTreatment
Clinical NeurophysiologyMedical Opinion using
appropriate test(EMG, NCS, EEG etc.)
Results back toreferrer
Review bySpecialists
Figure 16: A diagram to illustrate a model pathway for other Neurological Symptoms.

Transforming Clinical Neurophysiology Diagnostic Services to Deliver 18 Weeks
34
EEG
Pat
hway
Sym
ptom
– B
lack
outs
/ S
eizu
res
Patie
nt r
efer
red
from
GP
Neu
roph
ysio
logy
(R
efer
ral p
roto
col u
sed)
Rou
tine
EEG
Clin
ical
Rev
iew
of
Rou
tine
EEG
Res
ult
Non
-Spe
cifi
cEp
ilept
ifor
mab
norm
alit
ies
Slee
p D
epri
ved
EEG
Nor
mal
*- r
etur
nto
ref
erre
r
Nor
mal
Nor
mal
Non
spe
cifi
c ab
norm
alit
ies*
Sym
ptom
s co
ntin
ue.
Long
Ter
m E
EG m
onit
orin
g(t
o ca
ptur
e an
att
ack)
Res
ults
to
refe
rrer
for
rev
iew
Res
ults
to
refe
rrer
for
rev
iew
of
resu
lts a
nd c
linic
alhi
stor
y, t
reat
men
t an
d fu
rthe
r di
agno
stic
s
*Dep
endi
ng o
n lo
cal
Prac
tice
prog
ress
ion
toSl
eep
depr
ived
may
be
aut
omat
ic o
r no
t
Res
ults
to
refe
rrer
. Rev
iew
res
ults
and
clin
ical
his
tory
. Tre
atm
ent
or f
urth
erdi
agno
stic
s. M
ay n
eed
to r
epea
t EE
Gin
fut
ure
if cl
inic
ally
indi
cate
d
Supp
orts
dia
gnos
is o
f Ep
ileps
y.R
esul
ts b
ack
to r
efer
rer,
revi
eww
ith c
linic
al h
isto
ry. A
ppro
pria
tetr
eatm
ent
or f
urth
er d
iagn
ostic
s.M
ay n
eed
to r
epea
t in
fut
ure
ifcl
inic
ally
indi
cate
d.
Abn
orm
al
Abn
orm
al
Con
sulta
nt C
linic
–C
ardi
ac (
as p
er p
athw
ay)
(Neu
rolo
gy)
Figu
re 1
7: A
dia
gram
to
illus
trat
e a
mod
el p
athw
ay f
or E
EG.
This
pat
hway
ref
ers
to e
pile
psy,
fun
ny t
urns
and
fits
onl
y.

68. Carry out patient assessments in advanceof specialist consultant care whereappropriate:
� A step can be taken out of a patient’sjourney by carrying out an assessmentin a clinical neurophysiologydepartment in advance of a specialistconsultant appointment
� Patients on each of the pathwaysdetailed could benefit from a clinicalneurophysiology assessment as a firststep in their care pathway
� Further clinical neurophysiology testscan be carried out without the needto refer back to specialist referrer,effectively cutting the time to treatmentin some cases.
69. Provide treatment, where possible, at thesame time as assessment:
� Some pathways could end in clinicalneurophysiology without the need forfurther investigation or care
� For example, it will be appropriate to fitsome patients with tingly fingers with asplint at the same time as theirassessment which would be inconjunction with locally agreedprotocols.
Transforming Clinical Neurophysiology Diagnostic Services to Deliver 18 Weeks
35

70. Clinical neurophysiology can be providedand supported through a variety ofmodels in addition to the currentsecondary care based service. This includesservices in the community, includingoutreach sessions by clinical physiologistsfrom the local hospital, and independentsector providers.
71. Clinical neurophysiology services shouldbe commissioned to provide patients withservices that are responsive to their needsand that empower patients to be good
partners in achieving those needs. Criticalto this is ensuring that the guide tocommon symptoms investigated by clinicalneurophysiology in Figure 9 and moredetailed referral criteria are uniformlyimplemented across the main referralstreams.
72. As part of the PCT commissioning cycle,all current and potential providers ofclinical neurophysiology services (bothNHS and independent sector) should beconsulted in relation to adoption of thesuggested referral criteria and newpathways outlined in this document.
73. Clinical neurophysiology tests currentlydo not have a separate tariff but arebundled in the out patient tariff. Accessto tests and interpretation requires localagreement with a negotiated fee. PracticeBased Commissioning together with thedevelopment of a local tariff for highvolume tests, either by direct access to thehospital or providing the services in thecommunity, are key levers to demonstratethe value of clinical neurophysiologyservices and facilitate their futuredevelopment.
74. Development of a PCT and/or SHA widenetwork may be useful in helping toimplement these pathways, spreadinggood practice and making best use of allavailable capacity.
CASE STUDY: UNIVERSITY HOSPITALSBIRMINGHAM
“Provision of peripheral neurophysiologyservices in community outreach clinics”
One Birmingham PCT has funded theprovision of a peripheral neurophysiologyservice within community outreach clinics.A triage protocol was agreed with GPs,enabling clinics to be booked at the PCT,therefore saving time and shortening thepatient pathway. The service is provided byclinical physiologist practitioners of Agendafor Change Band 6 or above, fortnightly, inconjunction with a GP with a special interestin orthopaedics. Waiting lists reduced as220 patients were seen in the first year,therefore helping the Trust to meet the 18week target. Funding has now been securedto continue this service for 2 more years.
36
Supporting commissionersand providers

75. Questions to ask when commissioningclinical neurophysiology diagnosticservices include:
� Do we know that this service willprovide the tests that we require?
� Does the service provider have a goodclinical governance structure?
� How will quality assurance be carriedout?
� Will there be a regular audit?
� How will the provider communicatewith the referrer?
� Is there a way to ensure that the testreport follows the patient on theirpathway?
76. Suggested actions for SHA/18 weekleads include:
� Understand the demand for localservices (paragraphs 9 and 10 of thisdocument can be used as a startingpoint)
� Know what the current gaps are inclinical neurophysiology for deliveryof 18 weeks and the diagnosticmilestones, for sustainable provisionand to support organisations to closethe gaps
� Commission education and trainingprovision to deliver a workforce fit forthe future to deliver the 18 weekpathway.
77. Suggested actions forPCTs/Commissioners:
� Understand the demand in the localpopulation to direct the right level ofservice to meet those needs
� Develop a clinical neurophysiologynetwork to enable the sharing of ideas,development of standards for datacollection and to support active clinicalengagement in commissioning decisions
� Develop a robust quality governanceframework for provision of clinicalneurophysiology, including thecommunity and independent sector
� Put mechanisms in place to commissionappropriate workforce, including robustworkforce planning for the future todeliver new models of care
� Provide a combination of serviceredesign and adequate capacity forthe delivery of 18 weeks.
78. The models of service outlined in thisdocument have been developed by asmall group of experts. They have beendesigned both to stimulate discussion andto introduce new ways of working aimedat reducing waits and increasing accessto clinical neurophysiology services.
Transforming Clinical Neurophysiology Diagnostic Services to Deliver 18 Weeks
37

Clinical NeurophysiologyCaroline Dunn, National Project Lead forNeurophysiology
Paul White, Independent HealthcareConsultant (Health Horizons Ltd)
Nick Kane, Frenchay Hospital, Bristol
Jonathan Cole, Poole Hospital
Evadne Cookman, Hammersmith HospitalsNHS Trust
Anne Burge, Birmingham City Hospital
Robin Kennett, John Radcliffe Hospital, Oxford
Louis Merton, St Mary’s Hospital, Portsmouth
Shelagh Smith, National Hospital forNeurology and Neurosurgery
Andrew Weir, Institute of NeurologicalSciences, Glasgow
Peter Heath, University Hospital of NorthStaffordshire
David Allen, Southampton General Hospital
Jeremy Bland, Kent and Canterbury Hospital
The list below includes the PhysiologicalMeasurement Development Sites and ideasthey tested, together with other organisationsthat have trialled best practice ideas.
East Kent Hospitals NHS TrustCommitting to continuous service improvement
Norfolk & Norwich University HospitalNHS TrustManaging the clinical commitment to IOMsurgery
Royal Devon & Exeter NHS Foundation TrustExtending the technologist/clinical physiologistrole
Royal Free Hampstead NHS TrustIntroducing direct access referral from primarycare for patients with suspected carpal tunnelsyndrome
Issuing splints directly to patients with mildcarpal tunnel syndrome
University Hospital Birmingham NHSFoundation TrustProviding a peripheral neurophysiology servicein primary care
University Hospital of North StaffordshireNHS TrustIntroduce new and extended workforce roles
Other sites:
� Leeds Teaching Hospital NHS Trust
� Pennine Hospitals Acute NHS Trust
� Poole Hospital NHS Trust
� Ipswich Hospital NHS Trust
� Hammersmith Hospitals NHS Trust
38
Acknowledgements

Overview ofElectroencephalography (EEG)The electrical activity of the brain (the EEG)can be recorded using either scalp (surface) or,in special circumstances, intracranial electrodes.The majority of studies are undertaken on anoutpatient basis using scalp electrodes.Recordings may last from a half to severalhours, particularly if a period of sleep isincluded. The principal indication for EEG is inthe investigation and management of epilepsyand other disorders of consciousness. Since it israre for brief recordings to capture a clinicalattack, these EEGs are usually referred to asinterictal recordings. Interictal EEG is used tosupport a clinical diagnosis of epilepsy and toclassify the type of seizures and epilepsysyndrome, and include photic stimulation andhyperventilation with informed consent. EEG isalso used in the diagnosis and management ofother conditions such as coma, encephalitisand Creutzfelt Jacob disease (CJD).
Specialised EEG investigations includeambulatory EEG and video EEG (telemetry)monitoring. These studies monitor the EEG forseveral days or weeks in an attempt to capturea clinical attack and characterise the associatedEEG. Some patients, particularly those beingconsidered for surgical treatment of intractableepilepsy, may require intracranial electrodes(depth or sub-dural electrodes) as part of videoEEG studies.
Overview of Nerve ConductionStudies and Electromyography(NCS/EMG)The electrical activity of nerves and musclescan be recorded to assess their function, as adirect extension of the clinical history andneuromuscular examination. NCS/EMG studiesprovide useful information in the evaluation ofmotor and sensory nerves, from their nerveroots, through the brachial and lumbosacralplexi to the peripheral nerves, and in thecase of motor nerves to the neuromuscularjunction and muscles. The majority of NCSexaminations are undertaken on an outpatientbasis using surface stimulating and recordingelectrodes, whilst muscles are examined withinvasive needle EMG electrodes. Recordingsmay last from a half to several hours. Theprincipal indication for NCS/EMG is in theinvestigation of sensory symptoms (numbness,paresthesias and pain), weakness, muscleatrophy and fatigability. NCS/EMG studies aregenerally not helpful when such symptomsarise from disorders of the Central NervousSystem, or when pain results from disease orinjury that does not affect peripheral nerves.
39
Annex 1: Further information onClinical NeurophysiologyTests

1. Latinovic R, Glliford, MC, Hughes RAC.Incidence of common compressiveneuropathies in primary care. JNNP2006;77:263-265.
2. Hauser WA, Kurland LT. The epidemiologyof epilepsy in Rochester, Minnesota, 1935through 1967. Epilepsia 1975;16:1-66.
3. Bell GS, Sander JW. The epidemiology ofepilepsy: the size of the problem. Seizure2001;10:306-316.
4. Reilly MM, Hanna MG. GeneticNeuromuscular disease. JNNP 2002;73(Suppl II): ii12-ii21.
5. MacDonald BK, Cockerell OC, SanderJWAS, Shorvon SD. The incidence andlifetime prevalence of neurologicaldisorders in a prospective communitybased study in the UK. Brain 2000; 123:665-676.
6. England JD, Asbury AK. PeripheralNeuropathy. Lancet 2004; 363: 2151-61.
7. Leigh PN, Ray-Chaudhuri K. MotorNeuron disease. JNNP 1994; 57: 886-896.
8. Logroscino G et al. Incidence ifamyotrophic lateral sclerosis in southernItaly: population based study. JNNP 2005;76:1094-1098.
9. Hader WJ, Elliot M, Ebers GC.Epidemiology of multiple sclerosis inLondon and the Middlesex County,Ontario, Canada. Neurology 1988:38:617-621
10. Kurtzke. The current neurologic burden ofillness and injury in the United States.Neurology 1982; 32: 1207-14).
40
Annex 2:Complete references forincidence and prevalenceInformation in paragraph 9

Choose and Book Neurophysiology Service Request Form(N.B. Choose and Book referrals accompanied by incomplete forms may be rejected)
SECTION 1: PATIENT DEMOGRAPHIC DETAILS
Patient NHS number: UBRN:
Patient first names: Patient last name:
Date of Birth (DD/MM/YY): Gender: Male Female
Patient address (1st line):
Patient town / city: Patient postcode:
Patient contact number: Patient contact number 2:
SECTION 2: REFERRER INFORMATION
First name: Last name:
Referrer role: GP On behalf of GP
GP Practice Code: Referrer contact no:
GMC Registration No: Referrer e-mail address:
SECTION 3: TEST SERVICE REQUEST
Priority: Routine Urgent
Is the patient currently on any medication?
If yes, provide full details.
Yes No
Does the patient have an infection or do they pose aninfection risk to others?
No Yes
Test requested: (please tick one only)
EEG
Nerve Conduction Studies Please complete Section 4
EMG Please complete Section 4
Provisional diagnosis (or symptoms and signs):
Reason for request:
Relevant clinical history:
SECTION 4: COMPLETE FOR ALL NERVE CONDUCTION SCREENING OR EMG REQUESTS
Does the patient have a cardiac pacemaker? No Yes
Is the patient on Warfarin or any anti-coagulation medication? No Yes
If you have answered ‘yes’ to any of the questions above, please ensure that you include any relevant information inthe clinical history section.
41
Annex 3: Choose and Book referralscreen for clinicalneurophysiology

ROYAL FREE HOSPITAL: REFERRAL FORM FOR ONE STOP CLINIC FOR TINGLY FINGERS
FAX DIRECTLY TO: [Phone #] [For attention of CP(N)]
Royal Free Hampstead NHS Trust
Department of Clinical Neurophysiology Tel: [Phone #]
Referral Form – For Nerve Conduction Studies on Patients with Suspected Carpal Tunnel Syndrome
Patient’s Name DOB: Phone number: (Home)
Address Hospital Number (Mobile)
Do you suspect that the patient is suffering from?
Referral form completed. Please sign and date. Fax directly to dept. [Fax #]
1. Carpal Tunnel syndrome? Go to question 5
2. Ulnar neuropathy at the elbow? Refer patient in the usual way
3. Generalised large fibre peripheral neuropathy? Refer patient in the usual way
4. Is your referral for an alternative reason? Refer patient in the usual way
5. Does the patient suffer from tingling/numbness of the whole hand(s),
all the fingers or predominantly the outside of the hand?
6. Is the tingling/numbness worse, or does it or wake the patient,
during the night?
7. Is the tingling eased by shaking the hand or by hanging it down?
8. Does the patient have neck symptoms?
9. Does the patient have permanent sensory loss or muscle wasting?
10. Does the patient have neurological symptoms other than in the hand?
11. Does the patient think that their occupation is responsible for
their symptoms?
12. Does the patient have Hand Arm Vibration Syndrome?
13. Has the patient had an arm fracture in the past 6 months?
14. Which hand is most affected?
42
Annex 4: Royal Free referral form for one stoptingly fingers clinic




© Crown Copyright 2007
282820 1p 1K Aug07 (ESP)Produced by COI for the Department of Health
If you require further copies of this title quote 282820 and contact:
DH Publications OrderlinePO Box 777, London SE1 6XHEmail: [email protected]
Tel: 08701 555 455Fax: 01623 724 524Textphone: 08700 102 870 (8am to 6pm Monday to Friday)
282820/Transforming Clinical Neurophysiology Diagnostic Services to Deliver 18 Weekscan also be made available on request in braille, in audio, on disk and in large print.
www.dh.gov.uk/publications