Embed Size (px)
Citation preview
Transformational Leadership: Strategic Planning TL1EO Nursing’s mission, vision, values, and strategic plan align with the organization’s priorities to improve the organization’s performance. TL1EOa: Provide one example, with supporting evidence, of an initiative identified in the nursing strategic plan that resulted in an improvement in the nurse practice environment. Background/Problem Nursing & PCS Strategic Plan Every fall the Nursing & Patient Care Services (N&PCS) Executive Team participates in an all-day retreat to review the previous year’s accomplishment and identify strategic goals and tactics for the upcoming year. In October 10, 2013, the annual Nursing & Patient Care Services retreat was held which resulted in the articulation of the 2014 Nursing & Patient Care Services strategic plan (OOD 3). The proposed plan is vetted with leadership and staff throughout N&PCS so there’s opportunity for input and a shared awareness of the strategic priorities. In the 2014 N&PCS Strategic plan, Goal #1 reads, “Optimize the patient experience to ensure the coordinated, standardized and evidence-based delivery of care throughout the Patient Journey.” The tactic, “Enhance and sustain outcomes on Phase I, II and II Innovation Units through the effective use of education and resources” was a tactic that was pertinent to every unit. Innovation Units were launched in late 2012 and throughout 2013 across all the inpatient care units to ensure that the experience of every patient and family at goes smoothly from admission to discharge – that they know who is taking care of them and how they can be reached. And, when they’re ready to go home, everyone feels prepared. This was accomplished through the implementation of 15 tests of change/interventions including the role of the Attending Nurse who coordinate the delivery of patient care with the interdisciplinary team throughout the patient journey. The Annual Performance Measures for the 2014 N&PCS Strategic Plan include improvements in nursing sensitive indicators (attachment TL1EOa.a). One such indicator is central line-associated bloodstream infections (CLABSIs). CLABSIs are a serious type of Hospital Acquired Infection (HAI), with critically ill patients being at particular risk. CLABSIs in ICUs remain among the most deadly infections, with associated mortality rates between 12-25%. Improving CLABSI rates was also a stated strategic goal in the 2014 N&PCS Quality & Safety Strategic Plan: Participate in efforts to improve nursing sensitive indicators and reduce healthcare associated infections: Falls, Pressure Ulcers, CAUTI and CLABSI (attachment TL1EOa.b). Nurse Practice Environment The nurse practice environment is defined by Zelauskas and Howes (1992) as a system that empowers nurses by providing them with increased opportunities for autonomy,
accountability, and control over the care they provide and the environment in which they deliver that care. The Medical Intensive Care Unit (MICU) on Blake 7 is an 18-bed adult medical intensive care unit that cares for a variety of complex respiratory and medical patients. These patients may require complex treatments including Continuous Veno-Venous Hemofiltration and Extracorporeal Membrane Oxygenation.
Although the MICU was using recognized best practices for CLABSI prevention, CLABSI rates remained high. The staff of the MICU reviewed the Oct-Dec 2013 CLABSI rate of 1.62 and recognized the potential for improvement. They conducted a literature review which showed that other academic medical centers had achieved a decrease in CLABSI with unit-based initiatives. Northeastern University School of Engineering and MGH had just established a collaborative relationship, and the opportunity to partner on this initiative presented itself. This effort was also in alignment with the N&PCS 2014 Annual Performance Measure of improving nursing sensitive indicator performance.
Goal Statement(s)
The goal of this initiative was to reduce CLABSI per 1000 central line days in the Medical Intensive Care Unit on Blake 7 through improvements in the nurse practice environment.
Description of the Intervention(s)/Initiative(s)/Activity(ies)
In January 2014, the MICU (Blake 7) embarked on an initiative to reduce CLABSI. Working collaboratively with Northeastern University School of Engineering, clinical nurses applied systems engineering methods to existing CLABSI reduction strategies. Workflow observations, human factors analysis, and reliability design principals were used to better understand the unit culture in the MICU and to customize interventions to reduce chances for human error and to make processes more reliable. A number of strategies were implemented over a 6-month period (January - June of 2014) and included the following:
Engaged clinical nurses in reviewing data, identifying interventions, and redesigningprocesses. This included reviewing CLABSI performance of other comparablehospitals to reaffirm that a rate of zero was achievable.
Posted a CLABSI flip chart in the central corridor of the unit with large (6”x10”) digitsindicating “Weeks since last CLABSI”, where it was easily visible for staff, patients,and visitors. This visual display of the number of weeks since the last central lineinfection mimics signage found in the manufacturing industry indicating “Days sincelast accident”. This strategy have been used for decades in manufacturing plantsand studies show that they are effective in reducing accidents when combined withelements of staff feedback.
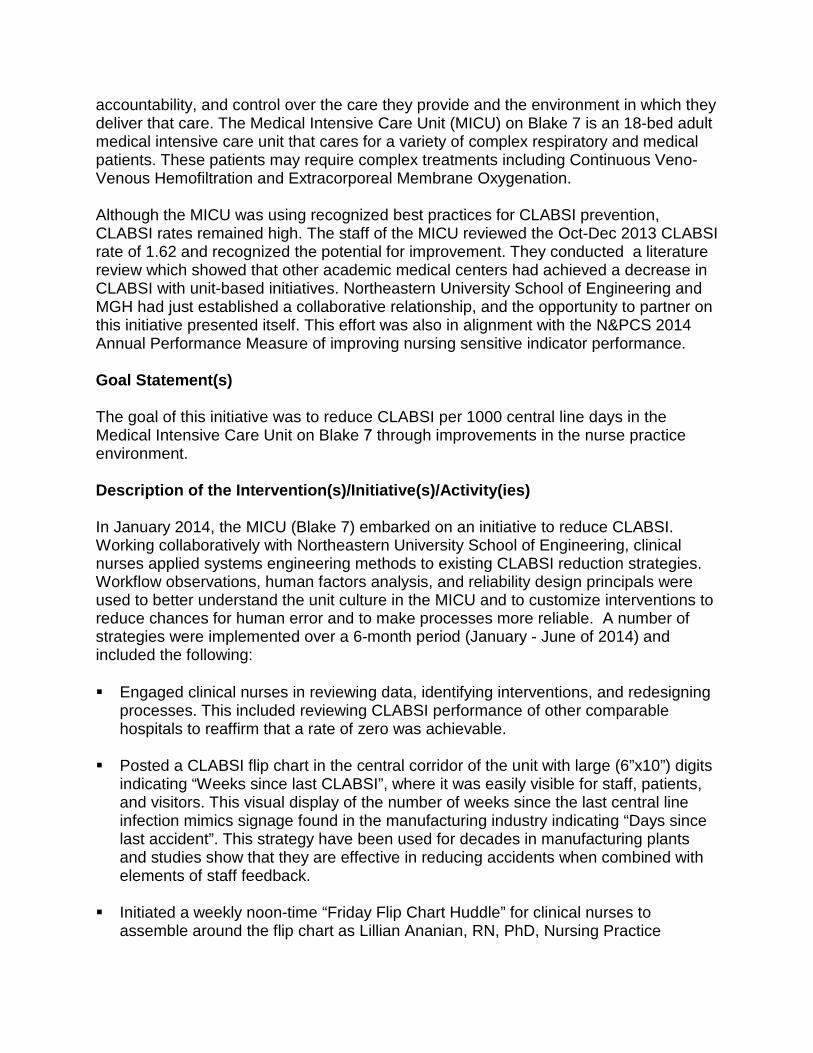
Initiated a weekly noon-time “Friday Flip Chart Huddle” for clinical nurses toassemble around the flip chart as Lillian Ananian, RN, PhD, Nursing Practice
Specialist (NPS), revealed whether the care team had achieved another week without infection. To make this a more reliable process, Ananian received an automated weekly email reminder to update the flip chart.
Created an electronic line-maintenance audit tool to enhance and sustain the audit process over time. Several clinical nurses volunteered to collect bi-weekly line maintenance data on all patients in the unit with central lines. The tool was based on a paper-version developed by Johns Hopkins Hospital and was created using a HIPAA compliant cloud-based survey service, capturing the type of line, tubing compliance, and dressing compliance, among other elements.
Provided weekly line maintenance feedback based on nursing-led audits that were shared during the Friday Flip Chart huddle, along with reinforcement of best maintenance practices.
Monitored/observed central line insertion procedures and halted providers from continuing the line insertion if clinical nurses saw sterility was compromised during the procedure.
Participated in daily patient rounds and prompted residents as needed to review/discuss the number of days a central line had been in place and why a line could or could not be removed.
These interventions showcase improvements in the nurse practice environment that empower clinical nurses to practice with autonomy and accountability and support
optimal patient outcomes by having control over the care they provide and the environment in which they practice. Participants: MICU CLABSI Reduction Workgroup
Name/Credential Title Department/Unit Lillian Ananian, RN, PhD Nursing Practice
Specialist Medical ICU (Blake 7)
Dominic Breuer, MS Industrial Engineer Northeastern University Ednan Bajwa, MD, MPH Medical Director Medical ICU (Blake 7) Paul Currier, MD Medical Director Respiratory Acute Care
(Bigelow 13 Jeanette Livelo, RN, DNP, NEA-BC Nursing Director Medical ICU (Blake 7) Richard Soria, RN, BSN, CCRN Clinical Nurse Medical ICU (Blake 7) Michael Tady, RN, BSN Clinical Nurse Medical ICU (Blake 7) Ryan Adams, RN, MSN Clinical Nurse Medical ICU (Blake 7) Elizabeth Mover, RN, BSN Clinical Nurse Medical ICU (Blake 7) Christine McCarthy, RN, BSN, CCRN Clinical Nurse Medical ICU (Blake 7) David Hooper, MD Chief Infection Control Unit Paula Wright, RN, BSN, CIC Project Manager Infection Control Unit Dolores Suslak, RN, MSN, CIC Director Infection Control Unit Elizabeth Mort, MD Senior Vice
President Quality & Safety
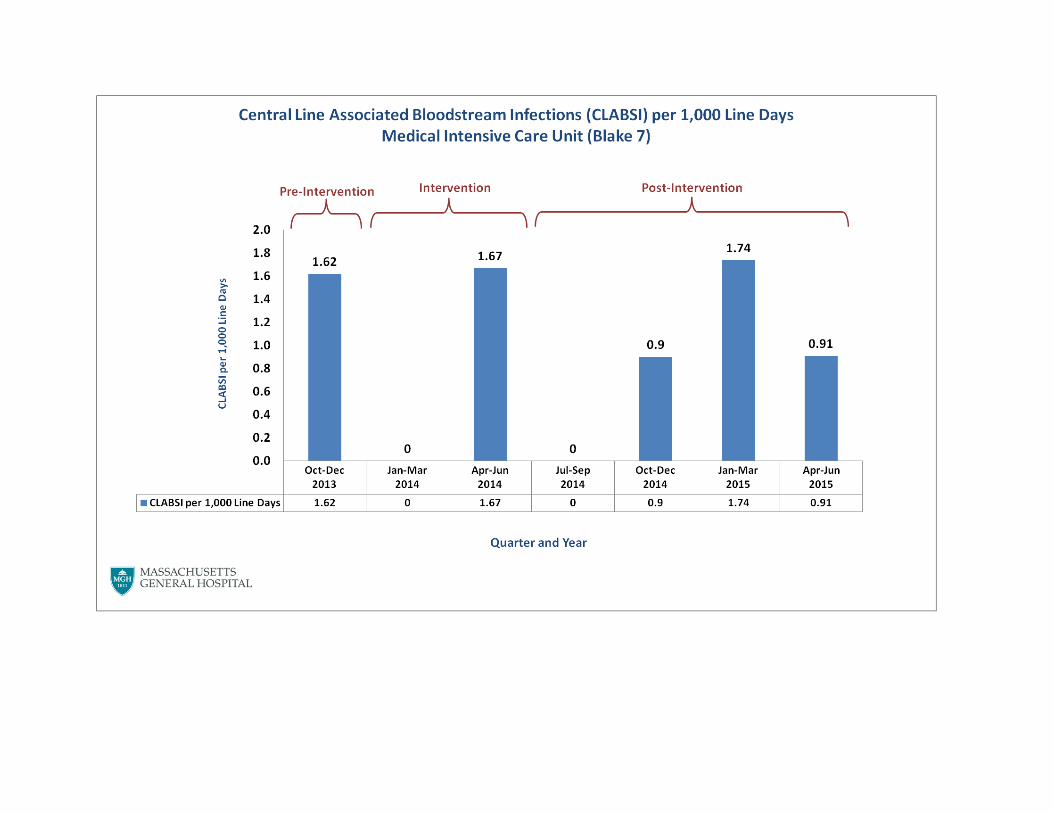
Outcome(s) The graph below shows that pre-intervention CLABSI per 1,000 line days was 1.62 and post-intervention 3 of 4 quarters between Oct 2014 - June 2015 showed a reduction ranging from 0 - 0.91. Three out of 4 quarters showing improvement is an indicator of sustained improvement. Well-documented best practices exist to reduce CLABSIs. One quarter (Jan-March 2015) showed an increase of 1.74 CLABSI per line days, which may indicate that interventions intended to prevent CLABSIs in the majority of patients, may not be effective for certain high risk patients, despite the best care. This initiative highlights the effectiveness of a systems approach to implementing interventions to enhance the nurse practice environment to promote CLABSI reduction in the MICU.

Massachusetts General Hospital Nursing & Patient Care Services
2014 Strategic Plan
January 2014
Excerpts from 2014 N & PCS Strategic Plan

Strategic Goals
Goal #1: Optimize the patient experience to ensure the coordinated, standardized and evidence-based delivery of care throughout the Patient Journey
Goal #2: Implement and evaluate consistent use of standardized documentation tools to support the processes that optimize the patient experience and outcomes
Goal #3: Create a welcoming, accessible environment that attracts, retains and develops a culturally competent workforce while embracing the diversity of our patients, their families, our employees, and the communities we serve
2014 Strategic Goals
Goals we will pursue to advance/support the organizational mission and our vision

2014 Strategic Goals
Goal #1: Optimize the patient experience to ensure the coordinated, standardized and evidence-based delivery of care throughout the Patient Journey
Tactics: Continue implementation and evaluation of Innovation Units
Enhance and sustain outcomes on Phase I, II, and III Innovation Units through effective use of education andresources. (Refer to Patient Journey Framework, Annual Performance Measures and Nursing SensitiveIndicators)
Identify and implement new interventions.
Develop a patient-journey framework for ambulatory and interventional practices (Phase IV).
Enhance systems to improve transitions in care through warm handovers using iPASS.
Align Innovation Unit initiative with:
Coordination of care with non-acute-care and home-care facilities.
Care re-design work
MGH/MGPO strategic plan.

Before During After
Admission process: ED, direct admits,
transfers
Patient stay; direct patient care; tests; treatments; procedures;
clinical support; operational support
Discharge process
Post-discharge
care
Pre-admission
care Inte
rven
tion
Inte
rven
tion
Inte
rven
tion
Inte
rven
tion
Innovations in Care Delivery “Patient Journey” Framework: Initial 15 Interventions
Relationship-based care ♦ The Attending Nurse role ♦ Hand-Over Rounding Checklist
Admission to Discharge Planning: -Est. discharge date
-Discharge disposition
- Welcome Packet (notebookand discharge envelope)
Admission to Discharge: - Domains of Practice
- Daily Interdisciplinary Team Rounds- Electronic Unit Whiteboards
- In-Room Whiteboards- Smart Phones
- Wireless laptop computers/tablets- Business cards- Hourly rounding
- Quiet hours
Post-Discharge: - Follow-up Call
Program
Goal: High-performing, inter-disciplinary teams that deliver safe, effective, timely, efficient, and equitable care that is patient- and family-centered
Copyright MGH 2012

Annual Performance Measures Including but not limited to:
Throughput and Efficiency Financial indicators- Case Mix Adjusted Cost per Discharge Workload Supply expenseAverage Length of StayAdmitting metricsEmergency Department metrics
External/Regulatory Successful Magnet Re-designation Successful Surveys and Visits Laboratory Joint Commission Laboratory Survey Successful Department of Public Health (DPH) Infection Control
Other System-Centered Metrics Environment of care surveys Safety culture survey Safety event reporting
Quality and Safety Nursing Sensitive Indicators* Readmissions
Infection Control Hospital Acquired Infections Nursing sensitive indicators* Urinary catheter device utilization ratio
Patient Experience Patient Satisfaction survey (HCAHPS) Follow-up Phone Calls (post-discharge) Patient Advocacy visits to patients Employee vacancy and turnover rates
Staff Satisfaction Staff Satisfaction (SPPPE and PES-NWI surveys) Clinical Recognition Advancement Certification and Formal Education Filled positions with focus on recruitment of diverse staff
*See next slide for detail.

Nursing Quality Indicators
• Pressure Ulcers• Falls with Injury• Physical Restraints• Pediatric Peripheral Infiltrations• Central Line Blood Stream
Infections• Catheter-Associated Urinary
Tract Infections• Time in Therapeutic Range• Completion of INRs in 28 days• Administration of Prophylactic
Antibiotics before SurgicalIncision
• Universal Protocol• Administration of Prophylactic
Antibiotic beforeCardiovascular ElectronicDevice Implementation
• DVT Prophylaxis +/- 24 hoursbefore Surgery
• Administration of ProphylacticAntibiotics before CesareanSection
• Administration of AppropriateDVT Prophylaxis beforeCesarean Section
• Human Papillomavirus Vaccine
• Influenza Vaccine with Asthma• Diabetes Self Management• Informed Consent• Completion of RN Machine Safety
Check Prior to Initiation of Dialysis• Pre-operative Fall Risk
Assessment• Successful First Attempts at
Peripheral Intravenous Insertions• Occlusion Rates in ICC Lines• Proportion of Infants in 22 to 29
Weeks Gestation Treated withSurfactant within 2 hours of birth
• Proportion of Infants in 22 to 29Weeks Gestation Screened forRetinopathy of Prematurity (ROP)
• Managing Post-operative CareCorrect Tray Set-up Protocol
• Vascular Access Time-Out• Door to IV rt-PA in 60 Minutes• Door to CT Scan (median time)• Acute Myocardial Infarction (AMI):
Primary PCI within 90 minutes ofArrival

Patient Care Services Office of Quality and Safety
2014 Strategic Plan Goals and Tactics
Excerpts from 2014 N & PCS Quality & Safety Strategic Plan

Goal #1: Support initiatives to improve the quality of the patient experience.
Tactics Sponsor OQ&S Staff
1.1 Continue to support the implementation and evaluation of Innovation Units • Data analytics: collecting and reporting of data to enhance
nursing intelligence • Support Innovation research efforts
PCS Colleen Snydeman Gennady Beyzarov Linda Akuamoah-Boateng
1.2 Participate in efforts to improve NSIs and reduce health care associated infections: Falls, Pressure Ulcers, Hand Hygiene, CAUTI & CLABSI • CAUTI workgroup initiatives • CLABSI efforts : Organizational, unit specific, Hopkins peer to peer
review, NU grant • Support hand hygiene initiatives as a primary means of reducing
health care associated infections
PCS IC CQS
Colleen Snydeman Linda Akuamoah-Boateng Gennady Beyzarov Judi Carr Deb Frost MaryAnn Walsh Patti Shanteler