Embed Size (px)
Citation preview

Title
Transformational and Charismatic Leadership in Health Care
Sub-Title
A critical examination of the role of transformational and charismatic leadership in developing
health care services which are responsive to change and thus more likely to meet the needs of
patients, clients, other users, and those involved in the delivery of such services.
Abstract
This essay begins with an articulation of origins and developments of transformational leadership
theory and whilst supporting the assertion that charisma is an important component of
transformational leadership behaviour argues that it is not in itself a defining feature. The
cascading effect of transformational leadership is explored in relation to contemporary research
both within the US and UK and utilised to articulate the relationship between transactional and
transformational behaviours within health care settings which constitute an optimum change
profile. The nature of vision and charisma within the health care setting are critically evaluated
along with the relationship between transformational leadership and key outcomes such as felt
autonomy, job satisfaction, low staff turnover, service quality and the achievement of
organisational (cultural) change.
Key Words
Transformational Leadership, Transactional Leadership, Full Range Leadership Model,
Charisma, Idealised Influence, Inspirational Motivation, Intellectual Stimulation, Individual
Consideration, Contingent Reward, Management by Exception, Laissez-Faire, Empowerment,
Innovation, Creativity, System Perspective, Patient Directed Health Outcomes, Complexity,
Complexity of Need, Human Relations, Nursing Process, Redesign of Working Practices,
Process Redesign, Vision, Risk Taking, Management of Attention, Management of Meaning,
Management of Trust, Management of Self, Building Relationships, Teamwork, Physician

Integration, Sharing Experiences, Learning Organisation, Work Satisfaction, Job Satisfaction,
Staff Turnover, Occupational Health, Cascading Phenomenon, Leadership Practices Inventory,
LPI, Nursing Development Units, NDUs, NHS.

The concept of transformational leadership is described in a seminal work by the political
sociologist James MacGregor Burns entitled Leadership (1978). In his work, Burns attempts to
link the roles of leadership and followership. He describes leaders as those people who tap the
motives of followers.
Transactional leadership occurs when leaders set up relationships with followers that are based
on an exchange for some resource valued by the followers. Interactions between the
transactional leader and the followers appear to be episodic, short-lived and limited to that one
particular transaction. A transactional leader balances the demands of the organisation and the
requirements of the people within the organisation.
Transformational leadership is much more complex and happens when people are engaged
together in such a way that leaders and followers encourage one another to increase levels of
motivation and morality. In such situations the aspirations of leaders and followers merge to
become one, (Bass, 1998).
Similarly, (Northhouse, 2001; McKenna, 2000) distinguishes between two types of leadership
styles:
“Transactional leadership refers to the bulk of leadership models, which focus on
the exchange that occurs between leaders and their followers. Managers who
offer promotion to employees who surpass their goals are exhibiting transactional
leadership. The exchange dimension of transactional leadership is very common
and can be observed at many levels in the organisation." (Northhouse P, 2001,
p. 132)
"In transformational leadership the emphasis is on people of vision who are
creative, innovative, and capable of getting others to share their dreams while
playing down self-interest; and who are able to cooperate with others in reshaping
the strategies and tactics of the organisation…in response to a fast-changing
world (Tichy & Devanna, 1986)… to these qualities could be added the pursuit
Transformational & Charismatic Leadership in Health Care Page 1

of high standards, taking calculated risks, challenging and changing the existing
company structure, with even the potential for the display (when considered
appropriate) of directive tendencies. (Bass, 1990)” (McKenna, 2000, p.383)
Bass (1985, 1998) provides a more expanded and refined theory of transformational leadership
which develops the work of Burns (1978) and House (1977), by giving far more attention to the
behaviour and needs of followers than had previously been given. Bass (1985, 1998) argued that
the principles of transformational leadership could be equally applied to situations where the
outcomes were not positive than those where the opposite was true and describing transactional
and transformational leadership as a singe continuum rather than mutually independent continua.
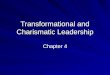
Bass (1985, 1998) identifies the main characteristics of transformational leadership as; charisma
idealised influence, intellectual stimulation and consideration of the emotional needs of each
follower, (Hunt, 1996).
Transformational Leadership ContinuumTransformational Leadership
Idealised Influence (Charisma)Inspirational MotivationIntellectual StimulationIndividual Consideration
Transactional Leadership
Contingent RewardManagement By Exception (Active)Management By Exception (Passive)
Laissez-fair Leadership
Non-transactional (non-leadership)
[Source: Adapted from Northouse P, 2001, p.136; Bass B, 1998, p.7-9]
In developing his model of transformational leadership Bass (1985) built upon earlier
charismatic literature and it is not surprising that House’s (1977) model of charismatic
leadership is often mistakenly identified as an archetype of transformational leadership. Weber
(1947) describes charisma as a special personality characteristic that gives a person superhuman
or exceptional powers and is reserved for a few, is of divine origin, and results in the person
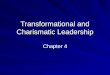
being treated as a leader. In addition to displaying certain personality characteristics, charismatic
leaders also demonstrate specific types of behaviours:
they are strong role models for the beliefs and values they want their followers to adopt,
Transformational & Charismatic Leadership in Health Care Page 2

they appear competent to their followers,
they articulate ideological goals which have moral overtones,
they communicate high expectations for followers, and they exhibit confidence in
follower’s abilities to meet these expectations. The impact of this behaviour is to
increase followers’ sense of competence and self-efficacy, which in turn increases their
performance,
they arouse task-relevant motives in followers that may include affiliation, power or
esteem.
Charismatic Leadership CharacteristicsPersonality Characteristics Behaviours Effects on FollowersDominantDesire to influence
ConfidentStrong Values
Sets strong role modelShows competence
Articulates goalsCommunicates high expectationsExpresses confidenceArouses motives
Trust in leader’s ideologyBelief similarity between leader and follower
Unquestioning acceptanceAffection towards leader
ObedienceIdentification with leaderEmotional involvementHeightened goalsIncreased confidence
[Source: Adapted from Northouse, 2001, p.133; Hunt 1996, p.189-190]
Hunt (1996) provides a clear synopsis of the differences between Bass’s (1985) theory of
transformational leadership and the earlier work of (Burns, 1978; House, 1977):
Bass (1985) emphasised an expansion of the followers’ portfolio of needs and wants with
a firm focus on the need for growth, development and self-actualisation,
Bass (1985) allowed for positive and negative transformations, that is transformations
that lead to organisational failure or ethically undesirable outcomes,
Bass (1985) unlike Burns (1978) does not view transformational and transactional
leadership as opposite ends of the same continuum, but views transformational leadership
as higher order (extraordinary) leadership which goes beyond the transactions found in
everyday management,
Bass (1985) considers that transformational leadership consists of four factors; idealised
influence (or charisma), individual consideration, inspirational motivation and intellectual
Transformational & Charismatic Leadership in Health Care Page 3

stimulation. Thus charisma is an important element of transformational leadership but
unlike House’s (1977) theory is not considered to be sufficient in itslef,
Bass (1985) considers that transactional leadership behaviours are based on two
dimensions namely, contingent reward and management-by-exception.
Contemporary health care settings are characterised by discontinuous change, increased
expectations from all service users, increased professional accountability and political pressure
for efficiency incorporating standardised easily measurable outcomes, technologically driven
change, an ageing population and an increase focus on the role of management and leadership
within clinical practice. Thus, despite the conceptual and operational liabilities often associated
with charismatic and transformational paradigms these have become increasingly attractive to
researchers and practitioners within health care and nursing contexts.
(Brown & Sofarelli, 1998) cite (Davidhizar R, 1993) in arguing that in today's changing and
chaotic health care arena the nurse leader needs to utilise the qualities of transformational
leadership which focus on people and solving problems in an ever-changing environment. They
go on to state that transformational nursing leadership actively embraces and encourages
innovation and change and provides the skills necessary for the profession to:
"… stretch its boundaries and be innovative in the way in which problems are
viewed and solved. This will become increasingly more important as nurses leave
the traditional hospital setting and expand their practises into the community. The
ability to find innovative solutions, to extend beyond their boundaries of comfort,
and to test new ways of doing old things, will move nursing further into the centre
of the arena of the new health care services." (Brown D & Sofarelli D, 1998,
p.203)
Trofino, (1995) claims that transformational leadership provides a mechanism for developing a
holistic, (bio-psycho-social), systemic perspective, which empowers nurses to make optimum
use of the enabling technologies to move “beyond even patient-centred health care to patient
directed health outcomes.” (Trofino, 1995, p.42)
Transformational & Charismatic Leadership in Health Care Page 4

(Davidhizar R, 1993) cites the work of Barker (1991) in arguing that; transformational
leadership in health care settings place less emphasis on hierarchical structures, logical decision
making and that rationality becomes less prominent, and that “this transition is appropriate as the
world has become a far more complex place” (Davidhizar R, 1993, p.675). Hence, scientific
approaches to leadership, (and presumably medically, scientifically orientated models of health
care), which do not take into account the complexity of individual need and the contingent
relationship of an ever changing environment are not likely to provide conceptual or practical
frameworks which underpin everyday actions. Davidhizar (1993) citing Barker (1991) argues:
“The new transformational paradigm is characterised by mutuality and affiliation,
acknowledging complexity and ambiguity, co-operation verses competition, and
emphasis on human relations, process versus task, acceptance of feelings,
networking verses hierarchy, and recognition of the value of intuition.”
(Davidhizar R, 1993, p.675).
According to Davidhizar (1993) the techniques of transformational leadership can enable nurse
leaders to design work environments, which satisfy the needs of their followers and enhance the
quality of care given to patients. She makes the important point that transformational leaders
combine a focus on nursing process (‘nursing heritage’) with redesigning the working practices
(process redesign) and the wider environment in order to facilitate team working and the
achievements of followers.
What is interesting about Davidhizar’s (1993) framework for transformational leadership in
nursing is the emphasis and importance she places on charisma (idealised influence) almost to
the exclusion of other transformational dimensions, and the lack of any guidance on how, (or
indeed if it is necessary), for nurse leaders to combine transformational and transactional
dimensions of leadership behaviour to achieve optimum influence. Davidhizar (1993) however,
does not attempt to provide a detailed definition of charisma beyond labelling it as a
“management quality that can empower employees and facilitate co-operation, creativity and
innovation” (Davidhizar R, 1993, p.675).
Transformational & Charismatic Leadership in Health Care Page 5

According to (Davidhizar R, 1993) charismatic leadership can ‘backfire’ in the following
conditions:
- Goals of the leaders are contrary to needs of the society: when followers and leaders are
bound by values which are not beneficial to society (and presumably patients) then such
leadership can be regarded as unethical as its effects are likely to be non-beneficial.
- Emotions become irrational: when emotional commitment to the leader becomes so intense
that a wider sense of rationality becomes lost. At which point followers will have developed
either a dependent or counter-dependent relationship with the leader to the exclusion of all
other influences.
- Leader is judged by exceptional standards: in such situation the strong desire amongst
followers to achieve personal identity with the leader may lead to unacceptable levels of
emotional and physical stress as followers attempt to emulate their leader’s exceptional
behaviour.
However, positive influences of charisma in transformational leadership are identified as:
- Self-esteem: having a positive self-regard is an important personal characteristic of
leadership, which is projected onto followers. Charismatic leaders are confident, highly
enthusiastic and have a high sense of self-worth. These characteristics are important
determinants of influence as subordinates (followers) are unlikely to follow a leader who
appears lacking in self-confidence, personal ability or has little understanding of
organisational goals and the wider environmental influences.
- Focus on People: Within the nursing profession the ability to relate to others members of the
team who are likely to possess high levels of interpersonal skills themselves is an important
determinant of effective leadership/influence. This is especially important given that the
ability to sustain and develop human relationships is an integral component of effective
practice. The charismatic/transformational nursing leader ensures that relationships with
Transformational & Charismatic Leadership in Health Care Page 6

colleagues are used to foster participation in problem solving and decision-making as a basis
for sustaining commitment to shared goals.
“Focus on people is one characteristic of charismatic leadership. In other words,
the leader who utilises a charismatic approach is orientated to people and visibly
focuses on human needs of followers. When subordinates present a concern, the
leader conducts an assessment to find the basis for concern.” (Davidhizar R,
1993, p.677).
- Vision: having a vision is an essential component of leadership for a leader who seeks to
lead with charisma. Having a vision for the development of practice, the ward/dept,
organisation, patient/clients and other stakeholders involves “knowing where the department,
unit or organisation is heading and how society will be served” (Davidhizar R, 1993, p.678).
A vision allows followers to reflect on the current state, identify its shortcomings and
become committed to a desirable future state, which is attainable and predicated on known
professional/ideological values.
“A vision allows individuals to see beyond the tedium of their present
predicament and to rise above the tedium of day-day events. A vision [if shared]
pulls people together in collective purpose and provides stimulation for extra
effort.” (Davidhizar R, 1993, p.678).
An Australian perspective on transformational nursing leadership provided by Sofarelli &
Brown (1998) citing (Davidhizar R, 1993) argues that:
“Transformational leadership is a style which is ideally suited to the present
climate of change because it actively embraces and encourages innovation and
change. A transformational leader [by encouraging and supporting reasonable
risk taking] will provide the skills for the profession to stretch its boundaries and
be innovative in the way in which problems are viewed an solved.” (Sofarelli &
Brown, 1998, p.203)
Transformational & Charismatic Leadership in Health Care Page 7

In defining the nature of transformational leadership within a nursing, health care setting they
cite the work of (Bennis 1986, 1990; Bennis & Nanus, 1985; McDaniel, 1997) in describing
four leadership competencies which they view as central to the provision of transformational
leadership in nursing/health care settings:
Management of Attention: management of attention is demonstrated by leaders who are able to
determine from events, patterns and relationships around them, what is relevant for the future
and then communicate this to followers. (Sofarelli & Brown, 1998) cite McBride (1994) who
states that “transformational leaders are those who have the ability to find meaning in piecemeal
actions and to make those connections for others so they can see the macro level while dealing
with the micro level” (McBride, 1994, p.284). Within contemporary health care systems the
transformational nursing leader will be constantly scanning their environment in order to use
relevant information in the formation and development of their vision.
“The transformational leader will ensure that their followers have all the
information that is required to work towards the shared vision, and will give them
the knowledge and support to enable them to develop the skills required to
analyse the information for themselves and to make decisions based upon that
information. [Thus, developing their followers ability to become transformational
leaders in their own right].” (Sofarelli & Brown, 1998, p.204)
The management of meaning is an essential prerequisite of individual, team and organisational
learning, as organisations strive through learning to achieve a symbiotic relationship with their
environments so that they are able to shape the environment as much as being shaped by in.
Management of Meaning: transformational leaders give meaning to their actions and those of the
organisation primarily through expressing their vision and modelling behaviours commensurate
with that vision. (Sofarelli & Brown, 1998) cite research by Dunham & Klafehn (1990, 1995)
into the transformational nature of leadership provided by nursing executives, in arguing that a
Transformational & Charismatic Leadership in Health Care Page 8

vision is a personal attribute and in order to align followers and the organisation to their vision
transformational nursing leaders must posses powerful communication skills.
“To be effective, a leader must fulfil many functions, but one of the most
important is the management of meaning and the effective articulation of their
dreams to their followers in order to inspire them to accept and be committed to
the vision. Effective transformational leaders are able to create a vision and
effectively communicate that vision to those people they lead, and throughout the
organisation. This required powerful and persuasive communication skills.”
(Sofarelli & Brown, 1998, p.204)
(Sofarelli & Brown, 1998) cite the work of Kets de Viries (1989) in arguing that
transformational leaders use language, ceremonies and symbols in order to reinforce the meaning
of their vision, they also know how and when to make use of humour, irony and colloquial
language which enhances meaning for their followers. They go on to argue, based on the work
of Dunham & Klafehn (1990) that a vision is not for the sole purpose of adding meaning to the
leader-follower relationship; effective transformational leaders can use a vision to revitalise a
whole organisation by giving people a meaning, purpose and a sense of higher value in their
work.
Management of Trust: is essential as leaders cannot empower with trust and trust is essential in
the transformational process. Trust is communicated to followers in many different ways but
one of the most important is through leadership visibility. Followers are not likely to trust a
leader who is often absent (behind closed doors), not prepared to do their share of the work,
avoids developing inter-personal relationships with followers, does not fulfil
commitments/promises and who does not model behaviour commensurate with their vision. The
successful development of trust is the foundation of transformational leadership in nursing as the
interrelationships that nurses develop with fellow professionals, patients/clients and the wider
community is built on an ethos of care and trust.
Transformational & Charismatic Leadership in Health Care Page 9

“Leaders must fulfil their commitments, keep promises, stay on course, live what
they say and be supportive when necessary; they need to be seen by people as
credible and trustworthy. (Kouzes & Posner, 1987) wrote that trust was at the
centre of human relationships and essential for organisational effectiveness.
Leaders within organisations can communicate trust to others by providing and
environment in which trust can develop.” (Sofarelli & Brown, 1998, p.205)
Management of Self: transformational leaders have a high personal self-regard, built on high
levels of self-awareness and self-esteem. They are able to communicate this to others and their
interrelationships with followers will as a consequence be built on positive reinforcement whilst
encouraging reasonable risk taking. They cite Bennis (1986) who states that “leaders know
themselves, they know what they are good at and they nurture those skills and competencies”
(Bennis, 1986, p.86) Transformational nursing leaders value learning, the gaining of knowledge
and the encouraging of others to view mistakes as an opportunity to learn and recognise that
there is no such thing as failure. They cite Kouzes & Posner (1987) who believe that:
“..the self-confidence that exceptional leaders gain through learning about
themselves; their skills, prejudices, talents and shortcomings .. [their] self
confidence develops as [they] build on strengths and overcome weaknesses.”
(Kouzes & Posner, 1987, p.277)
In conclusion Sofarelli & Brown (1998) argue that transformational leadership is ideally suited
to context of nursing, not least because it actively embraces change and innovation within an
ethical framework which complements values and beliefs of the profession.
“A transformational nursing leader will not only be able to achieve this [change]
but will also provide the skills and desires for other professionals to stretch their
boundaries and become innovative in the way that they view problems and their
solutions….the ability to find innovative solutions; to extend beyond their
boundaries of comfort; and to test new ways of doing old things will move
Transformational & Charismatic Leadership in Health Care Page 10

nursing further into the centre of the arena of the new health care services.”
(Sofarelli & Brown, 1998, p. 206)
They go on to argue that whilst traditional management skills, which emphasise transactional
components of leadership are an important and necessary dimensions of nursing leadership, it is
only when these are combined with transformational dimensions will nurses be able to deliver
the type of change and innovation so essential to today’s health care organisations. (Sofarelli &
Brown, 1998) cite Beyers (1995) in arguing that nurses are in an ideal position to influence
change within the health care settings, given that the profession is present in all context and that
nurses that nurse have a expert power base and a good, (holistic), insight into health problems;
“this places them in an ideal position to identify problems, to make recommendations and
implement new models of care” (Sofarelli & Brown, 1998, p. 206)
Dixon (1999) makes the important point that within today’s health care environments which are
characterised by “discontinuity leading to a fundamental shift in the ways in which patient care is
delivered” (Dixon, 1999, p.17). She goes on to argue that within such an environment
organisations need to balance so called soft issues of human relations with harder issues of
budget management. Key to such cultural change is the “metamorphosis of the leader’s ability to
put into action transformational leadership behaviours and characteristics” (Dixon, 1999, p.17).
“Leaders must posses the ability to help organisational players commit to what the
organisation stands for and how work is conducted. This is the foundation of
change. Without this, transformation is doomed to failure. Other key behaviours
include meaningful clear, consistent communication through multiple forms,
acting with integrity and being authentic; and treating people with respect and
dignity. These behaviours engender the trust building so central to teamwork.
Finally creating opportunities for innovation and risk taking provides the fuel that
propels the organisation to a new level of effectiveness.” (Dixon, 1999, p.17)
(Dixon, 1999) argues that:
Transformational & Charismatic Leadership in Health Care Page 11

- Building relationships: by ensuring visibility on shifts, active listening, challenging
traditional viewpoints whilst providing support required to explore new behaviours – new
ways of working,
- Creating a shared vision for the future: which emphasise a positive view of the future
whilst recognising the importance of professional values,
- Developing a strategy for implementing the vision: involving all organisational members
at all levels focussing on core values such as the recognition of expert resources,
conscientiousness, will/can-do attitude, sensitivity to internal and external customer
needs, and creative thinking,
- Recognising the value of teamwork:
- Developing a physician integration strategy:
- Communicating and sharing experiences:
- Creating a learning Organisation:
- Recognising Results Achieved:
In a survey by McDaniel & Wolf (1992) to determine the dimensions of leadership that result in
low turnover and work satisfaction, utilising Bass & Avolio’s (1985), Multi-Functional-
Leadership Questionnaire and Job Satisfaction Questionnaire from an earlier study by Hinshaw
(1987) aimed at developing ‘innovative retention strategies for nursing staff’, in a nursing
department comprising of 1 nurse executive (NCEO), 11 middle level administrators and 77
registered nurses was able to validate the following hypotheses:
Hypothesis 1: Leader self-assessment scores will be higher (p>0.05) than those of the respective followers;Hypothesis 2: Leader self-assessment scores will be higher than the follower’s assessment of the leaderHypothesis 3: (in a facility where leaders report a predominance of transformational behaviour, (as illustrated by their transformational scores), staff nurse work satisfaction will be average or above and correlated to staff’s leader- other scores andHypothesis 4: Staff turnover will be low.
Transformational & Charismatic Leadership in Health Care Page 12

The results derived from the MFLQ were as follows:
Transformational and Transactional Self Score of the Nursing Chief Executive Officer (NCEO) and Middle AdministratorsFactors NCEO Middle AdministratorsTransformational
Individual ConsiderationCharismaIntellectual Stimulation
TransactionalManagement by ExceptionContingent Rewards
3.43.13.73.32.52.52.4
3.0*2.73.23.02.22.02.3
*Statistically Significant P < 0.05 (McDaniel & Wolf, 1992, p.62)
Paired Scores Showing Self-Scores and Other Scores of NCEO, Middle Level Administrators, and RN StaffFactors NCEO Self NCEO by
AdminAdmin Self Admin by
RNsTransformational
Individual ConsiderationCharismaIntellectual Stimulation
TransactionalManagement by ExceptionContingent Rewards
3.43.13.73.3
2.52.52.4
2.6*2.72.32.7
2.0*1.82.1
3.02.73.23.0
2.22.02.3
2.4*2.32.72.3
2.11.92.2
*Statistically Significant P < 0.05 (McDaniel & Wolf, 1992, p.63)
The self-scores for the NCEO and Middle level administrators indicate that the nurse executives
had consistently higher self-assessment scores across all factors compared with those of middle
level administrators, (hypothesis 1). McDaniel and Wolf (1992) state that:
“The score validated the cascading or shared [leadership] phenomenon and were
comparable with those results obtained at similar levels of non-nurse
administrators and nurse executives. As one moves down the hierarchy, it is
anticipated that the transformational scores will decrease slightly, with a
concomitant emphasis on the transactional scoring representing the daily
management in an organisation.” (McDaniel & Wolf, 1992, p.62)
They go on to argue that the higher top echelon transformational scores suggested that more
attention was given to leadership interventions which directly related to the transformational
Transformational & Charismatic Leadership in Health Care Page 13

items on the MFLQ, such as developing an organisational vision or shared values of service
delivery. The declining transformational scores for middle grades may suggest that “an
increasing amount of attention would be given to the operational management of the service that
parallels the decline in administrative hierarchy.” (McDaniel & Wolf, 1992, p.62)
The paired scores show that the self-assessment scores of the administrators were higher than the
scores given to them by the registered nurses, these differences are consistent across all factors
and support hypothesis 2. The transactional scores of the administrators and registered nurses
were lower than the transformational scores which according to McDaniel & Wolf (1992) is a
desirable finding.
“This suggests that while these nurse administrators emphasise the
transformational components of their work, they also build on day to day
management [predicated primarily on transactional dimensions of leadership] to
encourage the nursing staff in their work and the accomplishment of their nursing
goals. The transformational leader would support a vision of nursing and enhance
the nursing staff to share that vision and to develop their perceptive positions.”
(McDaniel & Wolf, 1992, p.63)
The results from the job satisfaction survey supported hypothesis 3, that given the high levels of
transformational leadership practised by the nurse administrators that job satisfaction among the
nursing staff would be average or above. Data collecting relating to staff turnover supported
hypothesis 4.
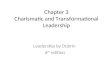
Research by Morrison et al., (1997) investigating the relationship between leadership style and
empowerment and its effect on job satisfaction amongst nursing staff in a regional medical centre
in the USA, using Bass & Avolio’s (1995) MFLQ to measure leadership and leadership style,
Warr’s et al., (1979) Job Satisfaction Questionnaire and Spreizer’s (1995) psychological
empowerment instrument, returning 275 useable questionnaires from an initial sample of n=442;
indicated that both transformational and transactional leadership were positively related to job
satisfaction with correlations of 0.64 and 0.35 respectively, with only transformational leadership
Transformational & Charismatic Leadership in Health Care Page 14

being positively correlated to empowerment 0.26. The higher positive correlation between job
satisfaction and transformational leadership compared with transactional leadership is argued by
Morrison et al (1997) to provide evidence of the Bass’s (1985) augmentation concept which
(Dixon 1999; McDaniel & Wolf, 1992) practically summarise in arguing that effective
transformational leaders build on the transactions found in everyday management.
Correlation Matrix for Leadership Style, Empowerment and job SatisfactionVariable 1 2 3 4Transformational Leadership -Transactional Leadership 0.54* -Empowerment 0.26* 0.08* -Job Satisfaction 0.64* 0.35* 0.41* -N= 275, *p < 0.05 [Source: Morrison et al, 1997, p.30]
Other studies by Laschinger & Havens (1997), Laschinger, Wong, Macmahon & Kaufmann
(1999) and McNeese-Smith (1997) indicate a causal relationship between transformational
leadership behaviour and perceptions of staff nurse empowerment, levels of occupational health
and organisational effectiveness.
Research in the UK by Bowles & Bowles (2000) using Kouzes & Posner’s (1988, 1995)
Leadership Practices Inventory (LPI) in a comparative study of transformational leadership in
nursing development units (NDUs) and conventional clinical settings, using a sample of 70
nurses comprising of two equally sized sub-groups drawn from NDU and Non-NDU settings.
The self-evaluations using the LPI showed little difference between the sub-groups. However,
the data indicated two differences in which leadership was perceived by followers
(observers/raters):
The observer (raters) score for non-NDU leaders were lower than those from NDU
leaders across each of the five practices of exemplary leadership.
Transformational & Charismatic Leadership in Health Care Page 15

The observer (raters) scores for non-NDU leaders are lower than the leaders’ self-
evaluations across each of the five practices. By contrast observer scores for NDU
leaders were higher than the leaders’ self-evaluations on four out of the five practices.
Mean Self-evaluations for each of the five practices of exemplary leadershipRole Challenge
the processInspire a shred Vision
Enable others to act
Model the way
Encourage the heart
Total Leadership Score
NDU Leader
24.14 23.14 25.29 24.14 25.29 121.43
Non-NDU Leader
24 22.14 25.36 24.57 25.29 121.86
Mean observer evaluations for each of the five practices of exemplary leadershipRole Challenge
the processInspire a shred Vision
Enable others to act
Model the way
Encourage the heart
Total Leadership Score
NDU Leader
25.71 25.25 25.64 24.71 25.21 125.75
Non-NDU Leader
22.92 21.29 24.64 23.82 23.32 115.57
[Source: Bowles & Bowles, 2000, p.73]
Bowles & Bowles (2000) state that
“NDU leaders were more highly evaluated by their observers than their non-NDU
counterparts. They demonstrated a higher level of congruence between their self-
evaluations and observer evaluation and more transformational leadership
behaviour than their counterparts.” (Bowles & Bowles, 2000, p.74)
A review of a sample of 2,013 managers from the NHS identified a far more complex model set
of behaviours than previous US research.
“The most obvious implications of these findings is the staggering complexity of
the role of leadership in the NHS. Another lesson is that the transactional
competencies of management, while crucial are simply not sufficient on their
own. […] what is clear is that existing us models of leadership do not encapsulate
this complexity. Typically, they place and overwhelming emphasis on charisma
Transformational & Charismatic Leadership in Health Care Page 16

and vision: on leaders acting primarily as the role model for their followers. Is
this the product of adopting research methodologies which focus solely on the
views of top managers, or researchers developing models from their own
observations?” (Alimo-metcalfe, 2001, p.40)
The qualities of leadership emerging as most important to staff to staff in NHS are characterised
by concern for others, followed by the ability to communicate and inspire.
Qualities of Leadership Perceived by NHS Staff to be Most ImportantAt the very top of the list of dimension for leadership came Genuine Concern for Others. This includes showing genuine interest in staff as individuals, seeing the world through their eyes, valuing their contributions, developing their strengths; coaching, mentoring and having positive expectations of what staff can achieve. The others, in order of importance, were followers.
Decisiveness, Determination, Readiness to take Reasonable Risks. Ability to clarify shared values and a sense of direction. This reflects a strong element of engaging with colleagues. This is another example of how the model differs from major US ones.
Inspirational Communicator, Networker and Achiever. This is essentially about communicating the vision of the organisation with passion and commitment. Unlike US models of ‘visionary and charismatic’ leadership, it stresses the need for partnership in engaging and extensive range of internal and external interested parties in the process by actively networking with them, gaining their confidence and support through sensitivity to their varying needs. It also about celebrating the accomplishments of the team, department or organisation.
Ability to Draw People Together with a Shared Vision. This relates to having a clear vision and strategic direction in which the ‘leader’ actively engages various internal and external stakeholders in developing; drawing others together in achieving the vision. It encapsulates some of the core values and attitudes exhorted by the government’s modernisation agenda.
Empowering others to lead. A manager who displays this dimension, trusts staff to take decisions/initiatives on important matter; delegates effectively and encourages staff to develop their leadership by providing opportunities to them to take on increased responsibilities.
Charisma. This is concerned with exceptional communication skills, ability to keep in close contact with others, encouraging others to join in.
Transparency. This relates to the aspect of integrity which is about honesty and consistency in behaviour, but also reflects the attitude of placing the good of the organisation before personal gain. It also involves humanity and humility and willingness to modify one’s views after listening to others.
Encouraging Challenges to the Status Quo. This includes clarifying the long term corporate direction while encouraging others to challenge the status quo, with respect to traditions and assumptions about what is being done, how problems are dealt with, and the quality of the service provided.
Accessibility, Approachability and Flexibility. This reflects a style which is not status-conscious, which places great importance on face-to-face, as opposed to distant leadership, and which attempts to ensure that staff at all levels feel comfortable and able to access the individual.
Supporting a Development Culture. This includes empowering individuals to challenge tradition, take risks and express dissatisfaction. In so doing the person presents a powerful role model for leadership.
Ability to Analyse and Think Creatively. Managing Change Sensitively and
Transformational & Charismatic Leadership in Health Care Page 17

This is sees as an essential dimension in the public sector leader. It involves the capacity to deal with a wide range of complex issues and the ability to utilise creativity in problem solving.
Skillfully. This includes being sensitive to the impact which changes in the external environment can have on the organisation; being aware of how these changes will differentially impact on parts of the organisation, being aware of the impact of one’s decisions, and having the wisdom to balance the need to change with some degree of stability.
(Source: Alimo-Metcalfe, 2001, p.41)
According to Lindholm & Sivberg (2000) managers within health care generally and nursing in
particular are increasing the pressure on their subordinates from board level downwards to
provide skilled and competent leadership which will empower their staff to meet the challenges
of providing patient/client focussed health care in the 21st century. Contemporary approaches to
leadership Bass & Avolio (1985, 1990), Burns (1978), Kouzes & Posner (1987), Tichy &
DeVanna (1986), Conger & Kunnungo (1987, 1999) present complex multi-dimensional
models of leadership which argue that change may be engendered though by combining the
judicious use of transformational behaviours with the less frequent use of transactional
behaviours.
“With regard to the turbulent arena of health care, Davidhizar (1993) and
Lafferty (1998) speak about utilising the qualities of transformational leadership,
which focuses on problem solving in a changing environment as the most
appropriate form of leadership. Burns (1978), who produced an early conception
of transformational leadership, argue that leaders and followers raise one another
to higher levels of motivation and morality rooted in common
values…..Transactional leadership by contrast is concerned with day-to-day
operations in an unchanged organisational system and has, according to Dunham
& Klafehn (1990) more of the characteristics of traditional leadership and
management…directed at organisational maintenance… Bass (1985) considers
transformational leadership and transactional leadership to be distinct but not
mutually exclusive processes, and declared that the same leader may use both
types of leadership at different times.” (Lindholm & Sivberg , 2000, p.328)
The key issues here is that the empowerment of nursing by leaders is likely to cascade down to
the community, and an empowered community will then be able to choose [within environmental
Transformational & Charismatic Leadership in Health Care Page 18

constraints] health services that are pertinent to the health needs of that community. These are
high ideals - but the key theme of empowerment through the leadership styles associated with the
4Is of transformation leadership are viewed as an important dimension of professional practice.
However, in order to gain and appreciation of the potential contribution that transformational
leadership theory can make to the development of contemporary health care systems through the
empowerment of nursing practice it is important to remember that:
such perspectives largely ignore the effect of contingent contextual variables such as the
inequitable or inadequate distribution of resources, quantum advances in supporting
technologies, the inherently irrational nature of the political environment etc.,
and as a study of the characteristics of executive nurse leadership by (Dunham &
Klafehn, 1995) clearly indicates, effective leadership in the health care arena is not
simply a case of utilising a transformational style at the expense of a transactional one,
but on employing critical thinking in ensuring that transformational behaviours augment
the transactions which are the foundations of everyday management in order that the
nursing profession and the organisation are able to respond to environmental variables
within an adaptive relationship of creative reinvention.
Transformational & Charismatic Leadership in Health Care Page 19

References
Alimo-Metcalfe, 1996, “The feedback revolution”. The Health Service Journal, June 13, p.26-38
Alimo-Metcalfe B, 1998, “The use of 360o feedback for developing leadership”, International Journal of Selection and Assessment, Vol 7(1)
Alimo-Metcalfe B, 1998, Effective Leadership, London: Local Government Management Board
Alimo-Metcalfe B, 2001, Haven Can Wait in Leadership in the NHS – HSJ Management Collections, London: EMP Public Sector Management
Alimo-Metcalfe B, Ch10 – Leadership Qualities in the NHS: What are the competencies and quality needed and how can they be developed in Mark A L & Dopson S (Eds), 2002, Organisational Behaviour in Health Care – the Research Agenda, London: Palgrave.
Barker A M, 1991, Emerging leadership paradigms, Nursing and Health Care, 12(4), p.204-207
Barker A M, 1992, Transformational Nursing Leadership, New York: National League for Nursing Press
Bass B M & Avolio B J, 1990, The implications of transactional and transformational leadership for individual, team and organisational development, Research in organisational change and development, 4, p.231-272
Bass B M & Avolio B J, 1993, Transformational leadership: A Response to critiques, In Chemmers M M & R Ayman (Eds), Leadership theory and research: Perspectives and directions, p.49-98, San Diego, CA: Academic Press
Bass B M & Avolio B J, 1994, Improving Organisational Effectiveness through Transformational Leadership, London: Sage Publications
Bass B M & Avolio B J, 1995, MFLQ Technical Report, Palo Alto, CA: MindGarden
Bass B M, 1985, Leadership and performance beyond expectations, New York: Free Press
Bass B M, 1990, From transactional to transformational leadership: Learning to share the vision, Organisational Dynamics, 18, p.19-31
Bass B M, 1990, Handbook of leadership: A survey of theory and research: New York: Free Press
Bass B M, 1995, The revised MFLQ 5X, Palo Alto, CA: MindGarden
Bass B M, 1996, A new paradigm of leadership: an inquiry into transformational leadership, Alexandria, VA: US Army Research Institute for the Behavioural and Social Sciences in Yukl G,
Transformational & Charismatic Leadership in Health Care Page 20

1999, An evaluation of conceptual weaknesses in transformational and charismatic leadership theories, Leadership Quarterly, Summer 99, 10(2), p.285
Bass B M, 1997, Does the transactional-transformational paradigm transcend organisational and national boundaries? American Psychologist, 52, p.130-139
Bass B M, 1998, Transformational Leadership, London: Lawrence Erlbaum Associates
Bass B M, 1999, Two decades of research and development in transformational leadership, European journal of work and organisational psychology, 8(1), p.9-32
Bennis W G & Nanus B, 1985, Leaders: The strategies for taking charge, New York: Harper Row
Bennis W G, 1986, The four traits of leadership, in Leader V Manager, Williamson J H (Ed), John Wiley & Sons, New York, p.79-80 in Sofarelli & Brown, 1998, The need for nursing leadership in uncertain times, Journal of Nursing Management, 6, p.201-207
Bennis W G, 1989, On Becoming a leader, London: Hutchinson Business Books Ltd
Bennis W G, 1990, Why leaders can’t lead, CA: San Francisco: Jossey-Bass Publishers
Beyers M, 1995, AONE’s officers on transformation, Journal of Nursing Administration, 25, p.8-9
Brown D & Soferelli D, 1998, The need for nursing leadership in uncertain times, Journal of Nursing Management, 6(4), July 1998, pp.201-201.
Burns J M, 1978, Leadership, New York: Harper Row
Conger J A & Kanungo R, 1987, Towards a Behavioural Theory of Charismatic Leadership in Organisational Settings, Academy of Management Review, 1987, Vol 12 No 4, p.637-647
Conger J A & Kanungo R, 1999, Charismatic Leadership in Organisations, Sage Publications, London
Davidhizar R, 1993, Leading with charisma, Journal of advanced nursing, 18, 675-679
Dixon D L, 1999, Achieving Results Through Transformational Leadership, Journal of Nursing Administration, Vol 29, No 12 - December 1999, p.17-21
Dunham J & Klafehn K, 1990, Transformational Leadership and the Nurse Executive, 1990, Journal of Nursing Adminstration, 20, p.28-33
Dunham J & Klafehn K, 1995, Identifying the best in nurse executive leadership, part 1, Journal of Nursing Administration, 1995, 25(6), p.68-70
Transformational & Charismatic Leadership in Health Care Page 21

Dunham J & Klafehn K, 1995, Identifying the best in nurse executive leadership, part 2, Journal of Nursing Administration, 1995, 25(7/8), p.24-31
Hinshaw A S, Smeltzer C, Atwood J, 1987, Innovative retention strategies for nursing staff, Journal of nursing administration, 17(2), p.18-24
House R J, 1977, A 1976 theory of charismatic leadership in Hunt J G & Larson L L (Eds), Leadership the cutting edge, Carbondale, IL: Southern Illinois University Press in Yukl G, 1998, Leadership in organisations, New York: Prentice Hall
Hunt J G, 1996, Leadership: A New synthesis, London: Sage Publications
Kets de Vires M F R, 1989, Prisoners of Leadership, New York: John Wiley & Sons in Sofarelli & Brown, 1998, the need for nursing leadership in uncertain time, Journal of Nursing Management, 6, p.201-207
Kouzes J & Posener B, 1987, The leadership challenge, San Francisco CA, Jossey Bass publishers
Kouzes J & Posener B, 1988, Leadership Practices Inventory II, San Francisco CA, Jossey Bass
Lafferty C L, 1998, Transformational leadership and the hospice, RN. case manager: a new critical pathway. Hospice Journal, 13, p.33-48
Laschinger H K S & Havens D S, 1997, The effect of work place empowerment on staff nurses’ occupational mental health and work effectiveness, Journal of Nursing Administration, 27(6), p.42-50
Laschinger H K S, Wong C, Macmahon L & Kaufmann C, 1999, Leader Behaviour Impact on Staff nurse Empowerment, Job Tension and Work Effectiveness, Journal of Nursing Administration, 29(5), p.28-39
Laurent C L, 2000, A nursing theory for nursing leadership, Journal of nursing management, 8, p.83-87
Lindholm M & Siverberg B, 2000, Leadership style among nurse managers in changing organisations, Journal of Nursing Management, 8, p.327-325
McBride A B, 1994, Transformational Leadership, Nursing Outlook, 42, p.284
McDaniel C & Wolf G A, 1992, Transformational Leadership in Nursing Service - A Test of Theory, Journal of Nursing Administration, Vol 22, No 2 - February 1992, p.60-65
McDaniel R R, 1997, Strategic Leadership: a view from quantum and chaos theories, Health Care Management Review, 22, p.21-37
Transformational & Charismatic Leadership in Health Care Page 22

McKenna E, 2000, Business Psychology and Organisational Behaviour: A Student’s Handbook, Hove: Lawrence Erlbaum Associates
McNeese-Smith D K, 1993, Leadership behaviour and employee effectiveness, nurse management, 25(4), p.38-39
McNeese-Smith D K, 1997, The influence of Manager Behaviour on Nurses’ Job Satisfaction, Productivity and Commitment, Journal of Nursing Administration, 27(9), p.47-55
Northouse P G, 1997, Leadership - Theory and Practice, London: Sage Publications
Northouse P G, 2001, Leadership Theory and Practice (2nd Ed), London: Sage Publications
Soferelli D & Brown D, 1998, The need for nursing leadership in uncertain times, Journal of Nursing Management, 6(4), July 1998, pp.201-201.
Spreitzer G M, 1995, Psychological Empowerment in the workplace: dimensions, measurement and validation, Academy of Management Journal, 38(5), p. 1442-1465
Tichy N M & Devanna M A, 1986, Transformational Leader, New York: Willey
Tichy N M & Devanna M A, 1990, Transformational Leader (2nd Ed), New York: Willey
Trofino J, 1995, Transformation leadership in health care, Nursing Management, 26, p.42-47
Warr P, Cook J & Wall T, 1979, Scales for the measurement of some work attitudes and aspects of psychological well-being, Journal of Occupational Psychology, 52, p.129-148 in Morrison R S, Jones L, Fuller B, 1997, The relation between leadership style and empowerment on job satisfaction of nurses,. Journal of Nursing Administration, 27(5), p.27-34
Weber M, 1947, The theory of social and economic organisations in Northhouse P G, 1997, Leadership - Theory and Practice, London: Sage Publications
Transformational & Charismatic Leadership in Health Care Page 23