Embed Size (px)
Citation preview

294 Surg Neurol 1991;35:294-9
Transcranial Stab Wounds: Morbidity and Medicolegal Awareness
Nabil Khalil, M.D., Mohammed Nagy Elwany, M.D., and Jimmy D. Miller, M.D.
University of Suez Canal, Suez, University of Alexandria, Alexandria, Egypt, and University of Mississippi, Jackson, Mississippi
Kahlil N, Elwany MN, Miller JD. Transcranial stab wounds: morbidity and medicolegal awareness. Surg Neurol 1991;35:294-9.
In this series of eight patients with transcranial stab wounds, the importance of classifications of such wounds as a separate traumatic entity is stressed. The mechanisms of neuronal and vascular damage in these wounds are discussed and are found to be specific from other head injuries. Cerebral injury by stabbing is largely restricted to the wound tract. Frontal stabs (two cases) are accompa- nied by the least morbidity and mortality, while temporal stabs (four cases) are more commonly fatal. In transorbital stabs (two cases) carotid-cavernous fistulae resulted. Early recognition, administration of antitetanus serum and anti- biotics, and debridement may minimize complications.
KEY WORDS: Head injury; Trauma; Stab wounds
In the 20th century, stab wounds of the skull and brain have become extremely uncommon. Most of the series reported have come from South Africa [3-5,8,9]. These studies draw attention to the pathology, anatomical fea- tures, and treatment of transcranial stabs. Unlike crani- ocerebral missile injuries, low-velocity penetrating stab wounds damage a focal area along the tract [2]. Thus, the mechanisms of neuronal and vascular damage differ from other types of head injuries. The present study highlights the importance of distinguishing these wounds as an entity.
Case R e p o r t s
Eight patients with transcranial stabs were admitted dur- ing the last 4 years to the neurosurgery departments of the Suez Canal and Alexandria universities and the University of Mississippi Medical Center (Table 1).
Address reprint request~ t0:Jimmy D. Miller, M.D., Department of Neurosurgery, University of Mississippi Medical Center, 2500 North State Street, Jackson, Mississippi 39216-4505.
Received May 29,1990; accepted August 20, 1990.
Case 1
A 20-year-old man was admitted to the casualty depart- ment of Port Foad, Suez Canal University Hospital. The patient had quarreled and received a right frontal stab wound by a sharp screwdriver that had been driven into the frontal lobe and withdrawn. On admission the patient received an antitetanus serum and intravenous antibiot- ics. The patient was fully conscious and normotensive, with a 1-cm scalp wound. Neurological examination re- vealed no deficits. Skull x-ray films showed a right frontal slot fracture. A computed tomography (CT) head scan revealed a short, narrow tract of lacerated cerebral tissue of 3 cm depth, passing from the right frontal eminence obliquely toward the lateral ventricle. Surgical explora- tion, debridement, and dural closure were performed. The patient was discharged after 10 days with no neuro- logical deficits. Follow-up at 6 months revealed no com- plications.
Case 2
A 19-year-old man was admitted to the University of Mississippi Medical Center after having been stabbed in the left frontal area. The penetrating instrument was not present and could not be identified. Physical examina- tion was remarkable for a 7-mm left frontal scalp wound. The patient was fully conscious and neurologically intact. A C T head scan confirmed a brain laceration in the left frontal lobe with no associated hematoma (Figure 1). The patient underwent emergency surgery for debridement and dural repair. He was maintained on antibiotics for 7 days following surgery and was discharged on the eighth postoperative day with no neurological deficits.
Case 3
A 23-year-old man was attacked with a pointed metal bar, receiving a left temporal stab. The patient was admit- ted to Suez Canal University 4 hours after the injury with the weapon embedded in his head. H e was deeply comatose with pinpoint pupils and positive Babinski re- flexes. Antitetanus serum, corticosteroids, and antibiot- ics were administered. On the lateral skull x-ray film
© 1991 by Elsevier Science Publishing Co., Inc. 0090-3019/91/$3.50

Transcranial Stab Wound Surg Neurol 295 1991;35:294-9
T a b l e 1. Summary of Cases
Sex/ Case age Neurologic Vascular Significant no. Site (yr) GCS deficits complications radiologic data Surgery Outcome
1 Right M/20 15 None None CTconfirmed right frontal Debridement Recovered; frontal traumatic tract no deficits
2 Left M/19 15 None None Left traumatic tract on CT Debridement & Recovered; frontal repair no deficits
3 Left M/23 3 Pinpoint pupils, None Plain x-ray film showed Removal of Died; postmortem temporal extensor plantar the retained pointed retained showed
hypertonia metal bar penetrating instrument lacerated deeply into the brain diencephalon
4 Right M/45 10 Left hemiparesis & - - CT revealed lacerated - - Recovered; temporal dysphagia temporal tract & right hemiparetic
ventricular hemorrhage 5 Left M/22
temporal
6 Left M/22 temporal
7 Right M/12 orbit
8 Left M/79 orbit
3 Pupil mid position & fixed, oculocephalic reflex absent
13 Slight facial palsy
13 None Right carotid cavernous fistulae
15 Impaired Left carotid extraocular cavernous movements in all fistulae direction of gaze
Plain x-ray film showed penetrating knife confirmed by CT
Angiography confirmed right carotid cavernous fistulae
Angiography confirmed left carotid cavernous fistulae
Removal of knife, debridement & repair
Muscle embolization
Detachable balloon catheter
Died; postmortem revealed severance of pons & basilar arteries
Recovered; no deficits
Proptosis improved
Recovered; no deficits. Died 1 month after discharge from unrelated pulmonary insufficiency, pneumonia, and heart failure
Abbreviations: CT, computed tomography; GCS, Glasgow Coma Scale: M, male.
the tip of the bar was above the dorsum sella, and on anteroposterior x-ray film, reached the midline. Craniot- omy and removal of the retained metal bar were per- formed immediately. A C T scan on the first postopera- tive day showed the lacerated tract reaching the diencephalon but no hematoma or midline shift. The patient died 2 days after admission. An autopsy docu- mented laceration of the diencephalon.
Case 4
A 45-year-old man was stabbed in the right temporal bone with a screwdriver that was withdrawn immediately by the assailant. Upon admission through the emergency room of Alexandria University Hospital, an initial neu- rological examination revealed a stuporous but arousable patient with equal and reactive pupils and a left hemipa- resis. A CT head scan revealed a right intraventricular hemorrhage and a small, localized, periventricular hema- toma. The stab wound could be visualized from the site
of entrance, traversing the internal capsule to reach the lateral ventricle. Carotid angiography detected no vascu- lar injury. The patient received antitetanus serum, antibi- otics, and corticosteroids. No surgical procedure was performed. The patient became fully conscious within 2 weeks but remained hemiparetic. A C T scan performed 1 month after the injury showed complete absorption of the hemorrhage. The patient was discharged for rehabili- tation and could walk with assistance 3 months after his injury.
Case 5
A 22-year-old man was admitted to Alexandria Univer- sity Hospital after sustaining a left temporal stab wound with a knife that was withdrawn by the assailant. He was deeply comatose and hypotensive (blood pressure 90/60 mm Hg). His pupils were mid position and fixed, and oculocephalic reflexes were absent. The patient died 2

296 Surg Neurol Khalil et al 1991;35:294-9
dent. The patient was stuporous (Glasgow Coma Scale score of 13) with periorbital swelling but no focal neuro- logical deficits. A C T head scan was normal. The patient improved and vision in the right eye was normal. How- ever, there was progressive proptosis of the right eye. Carotid angiography 2 weeks following the injury con- firmed the presence of a right carotid-cavernous fistula. The proptosis improved following muscle embolization via the cervical carotid, and the patient was discharged. Follow-up 2 years after his accident revealed slight pro- ptosis and a partial sixth nerve palsy.
Figure 1. Case 2." CT scan follouing a /eft frontal stab and weapon withdrawal demonstrates a skull fracture with an in-driren fragment and pneumocephalus. There is minimal hemorrhage along the tract.
hours after admission. Postmortem examination demon- strated laceration of the ports and basilar artery.
Case 6
A 22-year-old man was admitted to the University of Mississippi University Medical Center after he had been stabbed with a hunting knife. On initial examination, the knife was embedded in the left temporal region. He was lethargic but arousable, with very slight right facial palsy. There was no dysphasia. Skull x-ray films (Figure 2 A and B) confirmed intracranial penetration of the knife. A C T head scan showed intracranial involvement with associated subarachnoid hemorrhage in the left sylvian fissure (Figure 2 C). Emergency surgery was performed to remove the knife, debride the wound, and repair the lacerated dura mater. The patient had an unremarkable postoperative course and was discharged on the fourth postoperative day. The facial paresis gradually cleared.
C a s e 7
A 12-year-old boy was admitted to Port Foad University Hospital after having been stabbed in the medial canthus of the right orbit with a 25-cm metal rod from a bicycle wheel. The rod was withdrawn at the scene of the acci-
C a s e 8
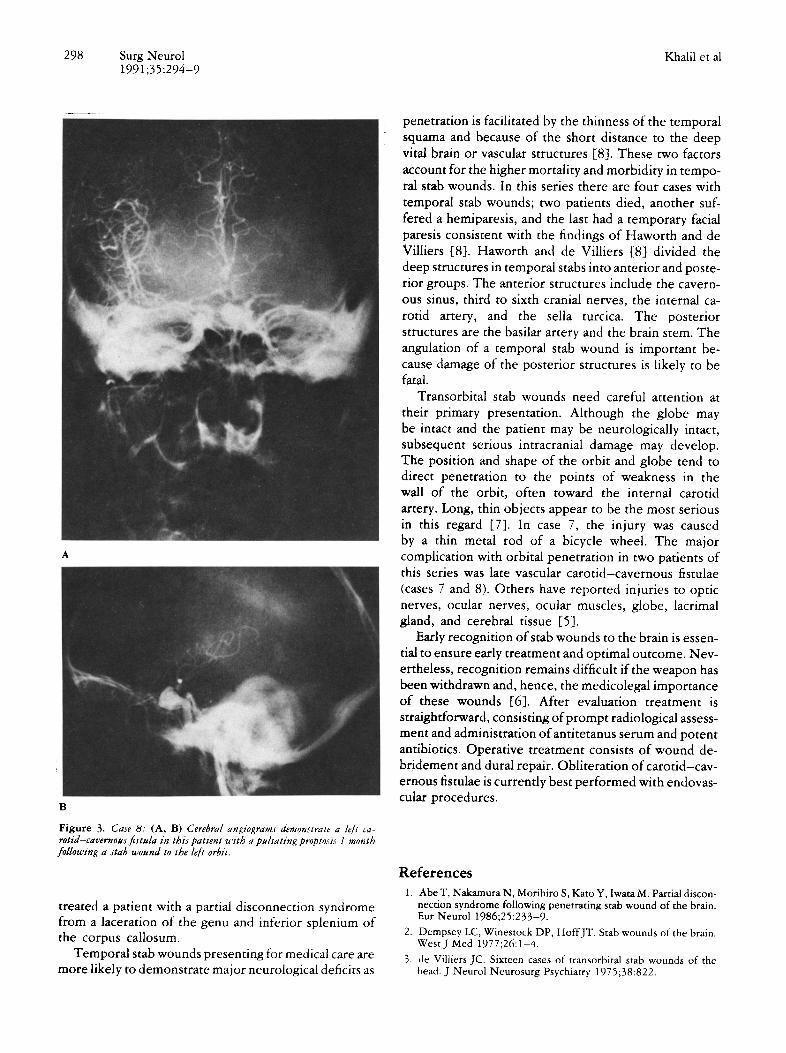
A 79-year-old man was stabbed in his left upper eyelid near the inner canthus. He was referred to the University of Mississippi Medical Center 1 month following the trauma. On admission the patient was fully conscious with a left pulsating proptosis. Vision in the left eye was not affected. Carotid angiography (Figure 3 A and B) documented the presence of a left carotid cavernous fistula. A detachable balloon catheter was introduced through the left cervical common carotid to occlude the fistula. Complete fistula closure could be achieved only by occlusion of the internal carotid artery. A Crutchfield clamp was placed on the common carotid artery in the neck and gradually closed over 3 days. Postoperative angiography showed complete closure of the fistula and the patient was discharged neurologically intact. He died 1 month after discharge from unrelated pulmonary insuf- ficiency, pneumonia, and heart failure.
Discussion
Transcranial stab wounds have their own mechanism of injury to the neuronal and vascular structures. They differ from missile or gunshot injuries, as there is no concentric zone of coagulative necrosis [2]. Unlike motor vehicle accidents, there is no diffuse injury to the brain. The instrument strikes the bone, producing a small slot fracture. Unless there is an associated hematoma or vascular occlusion, the brain damage is restricted to the wound tract [7,10]. In the absence of direct injury to the brain stem or laceration of a major intradural vessel, the prognosis of recovery is good (cases 1, 2, 7, and 8). The number of patients dying prior to presentation is unknown; however, of those presenting for medical care, the seriousness of the injury depends mainly upon the site and depth of the stab. In frontal stab wounds the patient may often be without deficits (cases 1 and 2) because the large frontal lobe prevents the instrument from reaching the deep vital structures. However , a unique syndrome has been reported from frontal stabs. Abe et al [1]

Surg Neurol 297 1991;35:294-9
C
A
Figure 2. Case 6: (A, B) Skull x-ray films show intracranial penetration of retained knife following an altercation. (C) CT scan is marred by artifact from the knife but reveals an absence of significant mass from intracranial hemorrhage.
B
298 Surg Neurol Khalil et al 1991;35:294-9
i ¸
. . . . . . . . . . . I
Figure 3. Case 8: (A, B) Cerebral angiograms demonstrate a left ca- rotid-cavernous fistula in this patient with a pulsating proptosis 1 month following a stab wound to the left orbit.
treated a patient with a partial disconnection syndrome from a laceration of the genu and inferior splenium of the corpus callosum.
Temporal stab wounds presenting for medical care are more likely to demonstrate major neurological deficits as
penetration is facilitated by the thinness of the temporal squama and because of the short distance to the deep vital brain or vascular structures [8]. These two factors account for the higher mortality and morbidity in tempo- ral stab wounds. In this series there are four cases with temporal stab wounds; two patients died, another suf- fered a hemiparesis, and the last had a temporary facial paresis consistent with the findings of Haworth and de Villiers [8]. Haworth and de Villiers [8] divided the deep structures in temporal stabs into anterior and poste- rior groups. The anterior structures include the cavern- ous sinus, third to sixth cranial nerves, the internal ca- rotid artery, and the sella turcica. The posterior structures are the basilar artery and the brain stem. The angulation of a temporal stab wound is important be- cause damage of the posterior structures is likely to be fatal.
Transorbital stab wounds need careful attention at their primary presentation. Although the globe may be intact and the patient may be neurologically intact, subsequent serious intracranial damage may develop. The position and shape of the orbit and globe tend to direct penetration to the points of weakness in the wall of the orbit, often toward the internal carotid artery. Long, thin objects appear to be the most serious in this regard [7]. In case 7, the injury was caused by a thin metal rod of a bicycle wheel. The major complication with orbital penetration in two patients of this series was late vascular carotid-cavernous fistulae (cases 7 and 8). Others have reported injuries to optic nerves, ocular nerves, ocular muscles, globe, lacrimal gland, and cerebral tissue [5].
Early recognition of stab wounds to the brain is essen- tial to ensure early treatment and optimal outcome. Nev- ertheless, recognition remains difficult if the weapon has been withdrawn and, hence, the medicolegal importance of these wounds [6]. After evaluation treatment is straightforward, consisting of prompt radiological assess- ment and administration of antitetanus serum and potent antibiotics. Operative treatment consists of wound de- bridement and dural repair. Obliteration of carotid-cav- ernous fistulae is currently best performed with endovas- cular procedures.
References 1. Abe T, Nakamura N, Morihiro S, Kato Y, Iwata M. Partial discon-
nection syndrome following penetrating stab wound of the brain. Eur Neurol 1986;25:233-9.
2. Dempsey LC, Winestock DP, HoffJT. Stab wounds of the brain. West J Med 1977;26:1-4.
3. de Villiers JC. Sixteen cases of transorbital stab wounds of the head. J Neurol Neurosurg Psychiatry 1975;38:822.

Transcranial Stab W o u n d Surg N e u r o l 299 1 9 9 1 ; 3 5 : 2 9 4 - 9
4. de VilliersJC, Grant AR, Chir B. Stab wounds at the craniocervical junction. Neurosurgery 1985;17:930-6.
5. de Villiers JC, Sevel D. Intracranial complications of transorbital stab wounds. Br J Ophthalmol 1975;59:52-6.
6. Di Maio VJM, Di Maio DJ. An unsuspected stab wound of the brain: case report. Milit Med 1972;137:434-5.
7. Duffy GP, Bhandari YS. Intracranial complications following transorbital penetrating injuries. Br J Surg 1969;56:685-8.
8. Haworth CS, de Villiers JC. Stab wounds to the temporal fossa. Neurosurgery 1988;23:431-5.
9. Kieck CF, de Villiers JC. Vascular lesions due to transcranial stab wounds. J Neurosurg 1984;60:42-6.
10. Lindenberg R. Trauma of meninges and brain. In: Minckler J, ed. Pathology of the nervous system. Vol 2. New York: McGraw- Hill, 1971:1721.





























