Embed Size (px)
Citation preview

Accepted Manuscript
Title: Transcranial direct current stimulation for motorrecovery of upper limb function after stroke
Author: Jitka Podubecka Kathrin Bosl Sandra RothhardtGeert Verheyden Dennis Alexander Nowak
PII: S0149-7634(14)00187-0DOI: http://dx.doi.org/doi:10.1016/j.neubiorev.2014.07.022Reference: NBR 1999
To appear in:
Received date: 10-2-2014Revised date: 25-7-2014Accepted date: 28-7-2014
Please cite this article as: Podubecka, J., Bosl, K., Rothhardt, S., Verheyden,G., Nowak, D.A.,Transcranial direct current stimulation for motor recovery ofupper limb function after stroke, Neuroscience and Biobehavioral Reviews (2014),http://dx.doi.org/10.1016/j.neubiorev.2014.07.022
This is a PDF file of an unedited manuscript that has been accepted for publication.As a service to our customers we are providing this early version of the manuscript.The manuscript will undergo copyediting, typesetting, and review of the resulting proofbefore it is published in its final form. Please note that during the production processerrors may be discovered which could affect the content, and all legal disclaimers thatapply to the journal pertain.

Page 1 of 32
Accep
ted
Man
uscr
ipt
Transcranial direct current stimulation for motor recovery of upper
limb function after stroke
1Jitka Podubecká, 1Kathrin Bösl, 1Sandra Rothhardt, 2Geert Verheyden, 1,3Dennis Alexander
Nowak
1Neurologische Fachklinik Kipfenberg, Kipfenberg, Germany
2Department of Rehabilitation Sciences, KU Leuven, Belgium
3Department of Neurology, University Hospital, Philipps-University, Marburg, Germany
Jitka Lüdemann-Podubecká
Klinik Kipfenberg
Neurologische Fachklinik
Kindinger Strasse 13
D-85110 Kipfenberg
Tel.: 0049 (0)8465-175-66131
Fax: 0049 (0)8465-175-184
E-mail: [email protected]
Abstract: Backround: Changes in neural processing after stroke have been postulated to impede recovery from stroke. Transcranial direct current stimulation has the potential to alter cortico‐spinal excitability and thereby might be beneficial in stroke recovery. Methods: We review the pertinent literature prior to 30/09/2013 on transcranial direct current stimulation in promoting motor recovery of the affected upper limb after stroke. Results: We found overall 23 trials (they included 523 participants). All stimulation protocols pride on interhemispheric imbalance model. In a comparative approach, methodology and effectiveness of (a) facilitation of the affected hemisphere, (b) inhibition of the unaffected hemisphere and (c) combined application of transcranial direct current stimulation over the affected and unaffected hemispheres to treat impaired hand function after stroke are presented. Conclusions: Transcranial direct current stimulation is associated with improvement of the affected upper limb after stroke, but current evidence does not support its routine use.
Keywords: transcranial direct current stimulation, stroke, motor recovery, upper limb

Page 2 of 32
Accep
ted
Man
uscr
ipt
Introduction
Stroke is the leading cause of permanent disability in Europe and the United States
(Kolominsky-Rabas et al., 2001; Taylor et al., 1996). More than 50% of stroke victims retain
severe neurological impairments, most often those affecting motor function. Among these
patients, about 80% will retain some grasping deficits linked to upper limb impairments
(Jørgensen et al., 1995a, 1995b).
The better understanding of the stroke-induced remodelling of neural processing following
stroke have contributed to the development of novel targeted therapies that are thought to
promote neuroplasticity, among those non-invasive methods, such as repetitive transcranial
magnetic stimulation (rTMS) and transcranial direct current stimulation (tDCS) (Nowak et al.,
2010; Madhavan and Shah, 2012). TDCS and rTMS change cortico-spinal excitability for
several minutes outlasting the stimulation period (Lang and Siebner, 2007; Nitsche and
Paulus, 2007), induce remote changes within the cortical motor system and thereby may
improve motor function of the affected upper limb after stroke.
In the past few years, there has been a rapid increase in the application of non-invasive brain
stimulation to study brain-behaviour relations and to enhance the effectiveness of neuro-
rehabilitation. This paper summarizes the current knowledge of the effectiveness of tDCS to
enhance recovery of motor function of the affected upper limb after stroke.
Neural plasticity following stroke
Focal brain ischemia releases a complex cascade of metabolic and cytotoxic reactions causing
a loss of functional and structural integrity of neural tissue (Schallert et al., 2000) often
accompanied by typical changes in behaviour. Neuroplasticity is the ability of the brain to
adjust its functional capacities to novel situations. Compensation for damage of neural tissue
proceeds in effect by reorganizing and forming new connections between intact neurons
causing alterations of movement-related neural activation within peri-lesional and more
distant brain areas of both the ipsi- and contralesional hemisphere (Loubinoux et al., 2003).
“Positive” plasticity means modulation within the remaining intact motor network to optimize
neural resources for recovery of function. But one important finding is the notion that
plasticity is not always adaptive:
Several studies described a bilateral neural activation within motor areas of both hemispheres
during movements of the affected hand after stroke which cannot be found in healthy subjects
or when patients move the unaffected hand. E.g. one of the first longitudinal studies in

Page 3 of 32
Accep
ted
Man
uscr
ipt
recovering stroke patients compared fMRI motor activation patterns obtained in the first days
after stroke with those acquired 3 to 6 months post-stroke and described a stronger
bilateralization of neural activity in sensorimotor areas during the acute phase of stroke,
which returned to a more physiological, lateralized activation pattern 3 to 6 months post-
stroke (Marshall et al., 2000).
Neuroimaging analyses (PET, fMRI) of stroke subjects have noted enhanced task-related
neural activation in the contralesional primary motor cortex (M1), contralesional premotor
cortex, ipsilesional cerebellum, bilateral supplementary motor area and parietal cortex for
movements of the affected hand (Grefkes and Ward, 2014; Nowak et al., 2010; Rehme et al.,
2012). Importantly, enhanced recruiting of motor and non-motor areas in the unaffected
hemisphere was often associated with poor motor outcome of the affected hand: Stroke
victims with good functional outcome exhibited more lateralized neural activation within the
ipsilesional hemisphere for movements of the affected hand, while patients whose motor
deficit remained more severe recruited motor areas in both the ipsi- and contralesional
hemispheres (Grefkes and Ward, 2014; Nowak et al., 2010; Rehme et al., 2012).
These observations have helped the formulation of the interhemispheric imbalance model,
which assigns the increased neural activation of the non-lesioned hemisphere unambiguously,
playing a negative role on motor recovery of the affected hand. This model describes the brain
remodelling changes following stroke as “disruption of the balance” between the lesioned and
non-lesioned hemisphere (this phenomen is likely to be related to interhemispheric inhibition
between motor areas exerted via transcallosal connections) with the “shift balance” towards
the non-lesioned hemisphere being detrimental for the lesioned hemisphere (Nowak et al.,
2009, 2010). The increased activity within motor areas in the non-lesioned hemisphere and
the inhibitory influence towards the motor areas of the lesioned hemisphere affect negatively
the recovery of the affected upper limb.
Recent studies have questioned the general validity of the interhemispheric imbalance model.
The key findings from neuroimaging studies suggest, that the role of the contralesional motor
areas for recovery of motor function depends on several various factors such time since
stroke, lesion location or dimension of motor deficit (Grefkes and Ward, 2014; Rehme et al.,
2012): E.g. one fMRI study shows no significant difference of motor-related neural activity
between patients with mild motor impairments and healthy controls. In contrast, patients with
initially severe motor deficits featured a general reduction of motor-related neural activity in

Page 4 of 32
Accep
ted
Man
uscr
ipt
the first 1 to 3 days after stroke, which in the ensuing 10 days gradually increased in both
hemispheres. Increases in neural activity correlated with better motor recovery (Rehme et al.,
2011). Present data illustrate inter-individual differences in the evolution of neural activity
changes after stroke, which on the severity of the motor deficit and are probably linked to
inter-individual differences in the role of contralesional motor areas for motor recovery. The
increased neural activity within contralesional motor areas may have a supportive role on
motor recovery in patients with a severe deficit of the affected hand (at least during some
period since stroke). This does not apply to patients with a mild motor deficit.
Collectively, all these data described the relationship between localization of neural activity
and a dimension of motor recovery after stroke. Additionally, functional neuroimaging allows
us to compute how activity in one region is releated to activity in another region. These
relations are referred to as “functional” and “effective” connectivity (Grefkes and Ward,
2014; Grefkes and Fink, 2014).
Functional connectivity refers to a correlation of the neural activation between two (or more)
brain regions, without direction or causal interaction and can be probed in absence of a
structured task (resting-state) using fMRI. The recovery from motor deficits is typically
associated with a steady increase of resting-state connectivity, particularly between the
ipsilesional M1 and contralesional areas (Grefkes and Fink, 2014). Numerous studies showed
also reduced functional connectivity between ipsilesional M1 and contralesional M1, which
was correlated with the amount of motor impairment (Carter et al., 2012; Park et al., 2011;
Wang et al., 2010). Moreover, it was found that the contralesional premotor and posterior
parietal cortices have reduced functional connectivity with the ispilesional M1 (Wang et al.,
2010) whereas and that stronger functional connectivity between ipsiläsional M1 and other
brain areas in the early subacute phase post stroke is associated with a better motor recovery 6
months later (Park et al., 2011). These findings certify the association between disruption of
the physiological relationship between both hemispheres and an unfavourable motor outcome
of the affected upper limb, according to task-related neuroimaging studies (Grefkes and Ward,
2014; Nowak et al., 2010; Rehme et al., 2012). Additional, these findings illustrate a key-role
of functional connectivity of ipsilesional M1 with other brain areas (especially with
contralesional M1) for motor recovery after stroke.
The effective connectivity describes the influence that one region exerts onto the activity of
another and can be probed either by using of fMRI (during a voluntary motor task) or by
transcranial magnetic stimulation (TMS) paradigms. Dynamic causal modeling applied to

Page 5 of 32
Accep
ted
Man
uscr
ipt
fMRI data obtained from healthy individuals suggests that the movements of the hand lead to
an increase of excitatory effects from premotor areas exerted on the contralateral M1 activity,
whereas ipsilateral M1 activity is suppressed (Grefkes et al. 2008). In patients with stroke the
excitatory influence of the lesioned hemisphere is reduced (Grefkes and Fink, 2014).
Importantly, some patients show an additional negative influence exerted from the
contralesional M1 on the ipsilesional M1, which correlates with the degree of motor
impairment (Grefkes et al. 2008). The more impaired a subject is, the more the contralesional
M1 exerts an inhibitory influence on the ipsilesional M1, which further reduces the motor
output of the lesioned hemisphere beyond that which could be due only to the anatomical
damage (Grefkes and Fink, 2014).
Interestingly, the connectivity between motor areas within one hemisphere, as well as the
connectivity between both hemispheres vary during different stages of stroke (Grefkes and
Fink, 2014). A longitudinal study in acute stroke subjects showed reduced positive coupling
of ipsilesional SMA and dPMC with ipsilesional M1. Coupling parameters among these areas
increased with recovery and predicted a better outcome. Likewise, negative influences from
ipsilesional areas to contralesional M1 were attenuated. In subacute stroke, contralesional M1
exerted a positive influence on ipsilesional M1. Negative influences from ipsilesional areas on
contralesional M1 subsequently normalized, but patients with poorer outcome in the chronic
stage now showed enhanced negative coupling from contralesional upon ipsilesional M1
(Rehme et al. 2011). Another study showed a reduced interhemispheric inhibition in severly
impaired chronic stroke patients, which correlated strongly with reduced ipsilesional motor
cortex excitability (Volz et al. 2014).
Pertinent data indicate that the plastic changes in neural processing and their impact on motor
recovery after stroke are more complex than the simple interhemispheric imbalance model
may suggest. In summary, the best part of these studies favours the hypothesis that the poor
motor function and/ or motor recovery is associated with a disruption of the physiological
balance between motor areas of both hemispheres as well as with reduced positive coupling
between motor areas of ipsilesional hemisphere.
Transcranial direct current stimulation and modulation of neural plasticity for motor
recovery after stroke
The increasing interest in the application of tDSC in stroke rehabilitation is based on the fact

Page 6 of 32
Accep
ted
Man
uscr
ipt
that tDCS modulates cortical excitability thereby and allows direct interaction with potential
maladaptive neural plasticity. TDCS consists of applying a low-intensity current between two
electrodes (anode and cathode) placed on the scalp. Depending on electrode polarity placed
over M1 cortical excitability of M1 will be increased (anodal stimulation) or decreased
(cathodal stimulation). The amount and the duration of the changes in cortical excitability
depend on current density and stimulation duration (Nitsche and Paulus, 2007). To induce
changes in motor cortex excitability that outlast the stimulation period current intensities of at
least 0.6 mA and stimulation durations of at least 3 min. are needed. TDCS stimulation with a
current intensity of 1 mA and a stimulation duration of 5 or 7 minutes induce short-term
changes of cortical excitability that last for 10-15 minutes the stimulation itself. For long-term
changes in motor cortex excitability (one hour or more) a current intensity of 1 mA should be
administered for at least 11 minutes (Nitsche and Paulus, 2000).
A stable long-term effect of tDCS is relevant for its application in rehabilitation. Numerous
studies demonstrated stabilizing of long-term behavioral effect of tDCS. However, any
electrophysiologic effect of these stimulation-protocols they are missing. Therefore, studies to
explore the optimal stimulation-protocol and intersession interval for stabilizing of long-term
electropysiologic effect of tDCS are needed (Nitsche et al., 2008).
The current application of tDCS in rehabilitation of upper limb dysfunction after stroke is
mainly based on the concept of interhemispheric imbalance (Nowak et al., 2009, 2010).
Published studies until today illustrate three ways of neuromodulation within this concept: 1.
increase cortical excitability within the ipsilesional M1 (anodal tDCS to ipsilesional M1), 2.
decrease cortical excitability of contralesional M1 (cathodal tDCS to contralesional M1) or 3.
“bihemispheric stimulation” with the anode placed over ipsilesional M1 and the cathode over
contralesional M1.
In the pertinent literature no relevant side effects of currently used tDCS protocols have been
described. However, knowledge about the safe limits of duration and intensity of tDCS is still
limited (Nitsche et al., 2008). For safety reasons most researchers do not apply tDCS on
humans with implanted brain devices (e.g. deep brain stimulation) that may interfere with the
induced current flow. Also history of epilepsy, or pregnancy are widely held to be a
contraindication for tDCS application.
Methods The PubMed research database was reviewed for relevant articles upon the use of tDCS for
rehabilitation of impaired hand function after stroke up to 30/09/2013. The terms “transcranial

Page 7 of 32
Accep
ted
Man
uscr
ipt
direct current stimulation” and “stroke” were used. Studies were selected if they met the
following inclusion criteria: 1. study on humans, 2. diagnosis of stroke, 3. tDCS used as an
intervention, 4. motor assessment of the affected upper limb before and after the intervention,
5. Placebo-controlled study-design or study design with at least two experimental groups, 6.
three randomized patients at least.
Results 23 studies were identified that corresponded with the inclusion criteria. These studies included
a total of 523 stroke subjects. The studies showed a large variability of the study population,
the time from stroke when the intervention was performed, the number of the tDCS sessions,
the type of motor assessment performed and the methodological quality.
For sake of simplicity, studies were sub-categorized according to the stimulation protocol: 1.
increase of excitability of motor areas within the ipsilesional hemisphere, 2. decrease of
excitability of motor areas within the contralesional hemisphere, 3. decrease of excitability of
motor areas within the contralesional hemisphere compared to increase excitability motor
areas within the ipsilesional hemisphere, 4. decrease of excitability of motor areas within the
contralesional hemisphere and simultaneous increase of excitability of motor areas within the
ipsilesional hemisphere (bilateral stimulation). Tables 1,2,3, and 4 summarize studies sub-
categorized in each of these categories. The effectiveness of tDCS was calculated as the
percentage change of the outcome measure after the intervention in relation to the baseline
measurement.
Increase of excitability motor areas within the ipsilesional hemisphere
6 placebo-controlled human studies (n=91) investigated the effect of anodal tDCS over
ipsilesional M1 on motor function of the affected upper limb after stroke (Ang et al., 2012;
Hummel et al., 2005, 2006; Kim et al., 2008; Madhavan et al., 2011; Rossi et al., 2013).
Table 1 summarizes these studies.
INSERT TABLE 1 ABOUT HERE
Stimulation-parameters: All studies placed the anode over the ipsilesional M1 and the
cathode over the contralesional supraorbital region (Figure 1). Most of the studies applied
anodal tDCS at an intensity of 1mA tDCS over 20 minutes (Ang et al., 2012; Hummel et al.,
2005, 2006; Kim et al., 2008). Only two studies applied another stimulation protocols: 0,5

Page 8 of 32
Accep
ted
Man
uscr
ipt
mA over 15 minutes (Madhavan et al., 2011) and 2 mA over 20 minutes (Rossi et al., 2013).
Relevant side effects were not reported.
INSERT FIGURE 1 ABOUT HERE
Study-design: Most of the studies applied an crossover design with 2-3 experimental
treatments (any treatment 1 session) (Hummel et al., 2005, 2006; Kim et al., 2008; Madhavan
et al., 2011). Two studies investigated the effectiveness of tDCS applied over 5 (Rossi et al.,
2013) and 10 (Ang et al., 2012) days within a study-design including two parallel-groups
(experimental- and control-group). Only two studies included a follow-up test after 1 hour
(Kim et al., 2008) and 3 months (Rossi et al., 2013).
Adjunct therapies: One trial instructed participants to perform tracking movements with the
affected hand during the tDCS-session (Madhavan et al., 2011).
Stroke-aetiology: The majority of studies enrolled patients with ischemic stroke (Hummel et
al., 2005, 2006; Madhavan et al., 2011; Rossi et al. 2013). One study (Kim et al., 2008)
included patients with ischemic and haemorrhagic stroke.
Lesion location: Most studies included patients with subcortical and cortical lesion (Kim et
al., 2008; Madhavan et al., 2011; Rossi et al. 2013). Only two studies (Hummel et al., 2005,
2006) included only patients with a subcortical lesion.
Time after stroke: One study included patients with acute stroke (Rossi et al. 2013). The
remaining studies included patients with chronic stroke (Hummel et al., 2005, 2006; Kim et
al., 2008; Madhavan et al., 2011), and one of them also included patients with subacute stroke
(Kim et al., 2008).
Severity of upper limb impairment: All studies tested the efficiency of tDCS in patients
with moderate to mild sensory-motor impairment of the affected upper limb.
Missing data: One article (Ang et al., 2012) did not specify the aetiology of stroke, lesion
location, time from stroke and degree of impairment of the affected upper limb.
Effectiveness: 5 studies (n=41) reported a positive effect of anodal tDCS on motor function
of the affected upper limb after stroke (Ang et al., 2012; Hummel et al., 2005, 2006; Kim et
al., 2008; Madhavan et al., 2011). All results, but one (Ang et al., 2012), were statistically
significant. One study (Kim et al., 2008) showed a significant lasting tDCS-effect over a
follow-up of 60 minutes. All studies reporting a positive effect of anodal tDCS over
ipsilesional M1 tested chronic stroke patients.

Page 9 of 32
Accep
ted
Man
uscr
ipt
Only one study (n=50) reported a non-significant negative effect of anodal tDCS (Rossi et al.
2013). The Follow up of this study shows no lasting effect over 3 months.
The effect size of functional improvement was highly variable (percentage improvement
ranging between 19%-67%). On average the sensory-motor function of the affected hand
improved by 25% from baseline.
Summary: The best evidence, for the positive effect of the anodal tDCS on motor recovery of
the affected upper limb after stroke, exists currently for patients with a chronic stroke. There
are no data for patients within subacute stroke. For patients with acute stroke exists currently
only evidence for the negative effect of the anodal tDCS on motor recovery of the affected
hand.
Future studies should investigate the effect of anodal tDCS over ipsilesional M1 applied over
several days in combination with motor trainings, and how long the effect lasts after the
intervention. It is still unclear if anodal tDCS over ipsilesional M1 is effective to improve
hand function in subacute stroke. It is still unclear if anodal tDCS over ipsilesional M1 is
effective to improve hand function in haemorrhagic stroke.
Decrease of excitability of motor areas within the contralesional hemisphere
Three placebo-controlled studies (n=116) tested if cathodal tDCS over contralesional M1
improved motor function of the affecter upper limb after stroke (Nair et al., 2011; Wu et al.,
2013; Zimerman et al., 2012). Table 2 summarizes these studies.
INSERT TABLE 2 ABOUT HERE
Stimulation-parameters: The cathode was placed over the contralesional M1 in all studies
(Figure 2). In two studies the anode was placed over the contralesional supraorbital region
(Nair et al., 2011; Zimerman et al., 2012), in one study (Wu et al., 2013) the anode was placed
over the unaffected shoulder. Two studies tested the effect of 1mA tDCS applied over 20
(Zimerman et al., 2012) and 30 (Nair et al., 2011) minutes. One study tested tDCS at an
intensity of 1.2mA over 20 minutes (Wu et al., 2013). Relevant side effects were not reported.
INSERT FIGURE 2 ABOUT HERE
Study-design: One trial applied a crossover-design with one session of cathodal tDCS and
one session of placebo condition (Zimerman et al., 2012). Two studies probed the

Page 10 of 32
Accep
ted
Man
uscr
ipt
effectiveness of serial sessions of cathodal tDCS over 5 days (Nair et al., 2011) and 4 weeks
(Wu et al., 2013) on a study-design with two parallel-groups (cathodal tDCS, sham tDCS).
All studies included a follow-up investigation over 1 day to 4 weeks.
Adjunct therapies: Two studies integrated an occupation therapy (Nair et al., 2011) or motor
training (Zimerman et al., 2012) for the affected hand during the tDCS-session.
Stroke-aetiology: Two studies (Nair et al., 2011; Zimerman et al., 2012) enrolled only
patients with an ischemic insult, one study (n=90) included also patients with haemorrhagic
stroke (Wu et al., 2013).
Lesion location: One study selected only patients with a subcortical lesion (Zimerman et al.,
2012), one study included patients with cortical and subcortical lesions (Nair et al., 2011).
Time after stroke: All trials included primarily patients with chronic stroke.
Severity of upper limb impairment: One study investigated patients with a moderate to mild
impairment of the affected upper limb (Zimerman et al., 2012), two studies tested patients
with a moderate to severe upper limb impairment (Nair et al., 2011; Wu et al., 2013).
Missing data: One study did not specify lesion location (Wu et al., 2013).
Effectiveness: Two studies (Wu et al., 2013; Zimerman et al., 2012) reported a significant
positive effect, one study a positive effect without statistical significance (Nair et al., 2011) of
cathodal tDCS over contralesional M1 on upper limb motor recovery after stroke. Follow-up
shows a significant preservation of the tDCS-effect one day to 4 weeks after the intervention.
The effect size varied between 15%-58% percentage improvement of hand function (average
improvement in relation to baseline: 45%). These results inferred a higher efficiency by
cathodal tDCS, than by anodal tDCS.
Summary: Cathodal tDCS over the contralesional M1 is beneficial for motor recovery of the
moderately to severely impaired upper limb in chronic stroke. Future studies should
investigate the effect in acute and subacute stroke.
Comparison of decrease of excitability of motor areas within the contralesional
hemisphere and increase of excitability of motor areas within the ipsilesional
hemisphere
7 trials (n=204) compared the effectiveness of anodal tDCS over ipsilesional M1 with
cathodal tDCS over contralesional M1 to improve motor recovery of the affected hand after
stroke (Boggio et al., 2007; Fregni et al., 2005; Hesse et al., 2011; Khedr et al., 2013; Kim et
al., 2010; Ochi et al., 2013; Stagg et al., 2012). All but one study (Ochi et al., 2013) were
placebo-controlled.

Page 11 of 32
Accep
ted
Man
uscr
ipt
Table 3 summarizes these studies.
INCLUDE TABLE 3 ABOUT HERE
Stimulation-parameters: All studies placed the active electrode over the M1 (anodal tDCS
over the ipsiläsional M1/ cathodal tDCS over the contralesional M1) and the reference
electrode over the contralateral supraorbital area. Four studies used a stimulation intensity of
1mA over 10-20 minutes (Boggio et al., 2007; Fregni et al., 2005; Ochi et al., 2013; Stagg et
al., 2012), three studies used a stimulation intensity of 2mA over 20-25 minutes (Hesse et al.,
2011; Khedr et al., 2013; Kim et al., 2010). Significant side effects were not described.
Study-design: With the exception of one study (Ochi et al., 2013) with 2 experimental-groups
(anodal tDCS, cathodal tDCS), three experimental-treatments were performed (anodal tDCS,
cathodal tDCS, sham tDCS) (Boggio et al., 2007; Fregni et al., 2005; Hesse et al., 2011;
Khedr et al., 2013; Kim et al., 2010; Stagg et al., 2012). 4 studies investigated the efficiency
of tDSC on a crossover-design with a treatment over one day to 4 weeks (Boggio et al., 2007;
Fregni et al., 2005; Ochi et al., 2013; Stagg et al., 2012), 3 studies used a study-design with 3
parallel-groups (Hesse et al., 2011; Khedr et al., 2013; Kim et al., 2010) and a treatment over
6 days to 6 weeks. 3 studies implemented a follow-up investigation after 3 to 6 months (Hesse
et al., 2011; Khedr et al., 2013; Kim et al., 2010).
Adjunct therapies: Two studies combined the tDCS-stimulation sessions with robot-assisted
training for the affected upper limb (Hesse et al., 2011; Ochi et al., 2013).
Stroke-aetiology: Most of the studies enrolled patients with ischemic stroke (Hesse et al.,
2011; Khedr et al., 2013; Kim et al., 2010; Stagg et al., 2012). One study (Ochi et al., 2013)
included both ischemic and haemorrhagic stroke aetiologies.
Lesion location: All studies included patients with subcortical and cortical lesions.
Time after stroke: 4 trials tested patients with a chronic stroke (Boggio et al., 2007; Fregni et
al., 2005; Ochi et al., 2013; Stagg et al., 2012), 3 trials patients with an acute stroke (Hesse et
al., 2011; Khedr et al., 2013; Kim et al., 2010).
Severity of upper limb impairment: Two studies (Hesse et al., 2011; Ochi et al., 2013)
tested patients with severe and moderate hand dysfunction. Five studies (Boggio et al., 2007;
Fregni et al., 2005; Khedr et al., 2013; Kim et al., 2010; Stagg et al., 2012) tested the
efficiency of tDCS in patients with moderate to mild impairment of one upper limb.
Missing data: Two studies did not specify stroke-aetiology and lesion location (Boggio et al.,
2007; Fregni et al., 2005).

Page 12 of 32
Accep
ted
Man
uscr
ipt
Effectiveness: One study (n=96) reported a positive effect (no significant) only for cathodal
tDCS (Hesse et al., 2011). All others placebo-controlled trials (n=95) reported a positive
effect for both cathodal tDCS and anodal tDCS (Boggio et al., 2007; Fregni et al., 2005;
Khedr et al., 2013; Kim et al., 2010; Ochi et al., 2013; Stagg et al., 2012). Two trials (n=58)
of them did not report statistical significances for either intervention (Khedr et al., 2013; Kim
et al., 2010). Both these studies included patients with acute stroke as well as the study
without a positive effect by anodal tDCS (Hesse et al., 2011).
Follow-up measures (Hesse et al., 2011; Khedr et al., 2013; Kim et al., 2010) showed a
preservation of the effect of tDCS over three to six months after intervention.
Effect size of tDCS showed a high variability: Anodal tDCS varied between 46%-78% (on
average 15%) improvement of hand function in relation to baseline, cathodal varied between
5-103% (on average 40%) improvement of hand function in relation to baseline, without
apparent differences between different assessments.
Summary: In a comparative approach cathodal tDCS shows a greater efficiency upon
improvement of hand function in comparison to anodal tDCS.
Decrease of excitability of motor areas within the contralesional hemisphere and
simultaneous increase of excitability within motor areas on the ipsilesional hemisphere
(bilateral tDCS stimulation)
7 trials (n=112) investigated the efficiency of bilateral tDCS for motor recovery of the upper
limb after stroke (Bolognini et al., 2011; Fusco et al., 2013; Lefebvre et al., 2012; Lindenberg
et al., 2010; Mahmoudi et al., 2011; O'Shea et al., 2014; Takeuchi et al., 2012). All studies but
one (Takeuchi et al., 2012) were placebo-controlled. Table 4 summarizes these studies.
INSERT TABLE 4 ABOUT HERE
Stimulation-parameters: With the exception of one study (which combined faciliatory tDCS
and inhibitory rTMS) (Takeuchi et al., 2012)), all studies applied bilateral stimulation with the
anode placed over the ipsilesional M1 and the cathode placed over the contralesional M1
(Figure 3). 5 studies used a stimulation intensity of 1mA (over 20-30 minutes) (Lefebvre et
al., 2012; Lindenberg et al., 2010; Mahmoudi et al., 2011; O'Shea et al., 2014; Takeuchi et al.,
2012). One study used a stimulation intensity of 1.5mA (over 15 minutes) (Fusco et al., 2013)
and one study 2mA (over 40 minutes) (Bolognini et al., 2011). Negative side effects of the
bilateral stimulation were not described.

Page 13 of 32
Accep
ted
Man
uscr
ipt
INSERT FIGURE 3 ABOUT HERE
Study-design: 3 placebo-controlled trials tested the efficiency of bilateral tDCS within a
study-design with two experimental conditions (bilateral tDCS and sham tDCS) (Bolognini et
al., 2011; Lefebvre et al., 2012; Lindenberg et al., 2010). 3 placebo-controlled trials used a
study-design with 4-5 experimental conditions (anodal tDCS, anodal tDCS, bilateral tDCS,
sham tDCS) (Fusco et al., 2013; Mahmoudi et al., 2011; Takeuchi et al., 2012). One trial
(without placebo-control) compared the efficiency of bilateral tDCS, cathodal tDCS and
anodal tDCS (O'Shea et al., 2014).
4 trials tested the efficiency of bilateral tDCS on a crossover-design with 2-5 experimental
conditions and stimulation sessions over 1-2 days (Fusco et al., 2013; Lefebvre et al., 2012;
Mahmoudi et al., 2011; O'Shea et al., 2014). 3 trials included 2-3 experimental groups with a
treatment over 1-10 days (Bolognini et al., 2011; Lindenberg et al., 2010; Takeuchi et al.,
2012). 4 trials included a follow-up investigation after 1-4 weeks (Bolognini et al., 2011;
Lefebvre et al., 2012; Lindenberg et al., 2010; Takeuchi et al., 2012).
Adjunct therapies: Two studies combined tDCS-stimulation with constrained induced
movement therapy (Bolognini et al., 2011) or motor training for the affected hand (Lefebvre
et al., 2012).
Stroke-aetiology: 2 trials tested only patients with an ischemic insult (Lindenberg et al.,
2010; Mahmoudi et al., 2011), 4 trials included also patients with haemorrhagic stroke
(Bolognini et al., 2011; Fusco et al., 2013; Lefebvre et al., 2012; Takeuchi et al., 2012).
Lesion location: 4 trials included patients with subcortical and those with a cortical lesion
(Bolognini et al., 2011; Fusco et al., 2013; Lefebvre et al., 2012; Takeuchi et al., 2012), 2
trials included only patients with subcortical lesions (Lindenberg et al., 2010; Mahmoudi et
al., 2011).
Time after stroke: Most of the trials included patients with a chronic stroke (Bolognini et al.,
2011; Lefebvre et al., 2012; Lindenberg et al., 2010; Takeuchi et al., 2012), one trial included
patients with subacute and chronic stroke (Mahmoudi et al., 2011) and one trial included
patients with subacute and acute stroke (Fusco et al., 2013).
Severity of upper limb impairment: All trials included patients with a moderate to mild
impairment of one upper limb.
Missing data: One article did not specify stroke-aetiology, lesion location and time after
stroke (O'Shea et al., 2014).

Page 14 of 32
Accep
ted
Man
uscr
ipt
Effectivness: All placebo-controlled trials (n=102) reported a positive effect of bilateral tDCS
on motor recovery of the affected upper limb after stroke (Bolognini et al., 2011; Fusco et al.,
2013; Lefebvre et al., 2012; Lindenberg et al., 2010; Mahmoudi et al., 2011; O'Shea et al.,
2014), but two of them (n=29) were without statistical significance (Fusco et al., 2013;
Lindenberg et al., 2010).
Follow-up tests (Bolognini et al., 2011; Lefebvre et al., 2012; Lindenberg et al., 2010;
Takeuchi et al., 2012) showed a lasting effect of tDCS over six days to four weeks after the
intervention.
There was no significant difference between bilateral, anodal or cathodal tDCS on motor
recovery of the affected hand after stroke.
The effect size showed a high variability: bilateral tDCS improved hand function between -
7%-47% from baseline (on average 17%), facilitatory tDCS improved hand function between
0%-35% (on average 12%) and inhibitory tDCS improved hand function by 7%-20% (on
average 12%).
Summary: Bilateral tDCS seems to be more efficient than anodal tDCS or cathodal tDCS.
Future studies should prove the efficiency of the bilateral tDCS and compare it to facilitatory
and inhibitory tDCS within bigger study cohorts. Also its long-term effects should be further
evaluated.
Discussion This review included data from 23 articles including 523 stroke patients. In summary, the
pertinent literature suggests a positive effect of tDCS on motor recovery of the affected hand
after stroke.
Table 5 compares the effectiveness of the cathodal tDCS, anodal tDCS and the bilateral tDCS
to improve hand function after stroke in placebo-controlled trials. There was a large
heterogeneity in between studies regarding patient characteristics, intervention parameters,
outcome measures used and study designs.
INSERT TABLE 5 ABOUT HERE
Differential effectiveness of various tDCS protocols
Based on the current data cathodal tDCS over contralesional M1 is more effective than anodal
tDCS over ipsilesional M1.

Page 15 of 32
Accep
ted
Man
uscr
ipt
Cathodal tDCS was associated with an improvement in hand function in all patients tested,
but a significant effect was achieved in only 42% of them. Follow-up tests showed a lasting
effectiveness of cathodal tDCS for up to 6 months in all patients (but this effect was
statistically significant in only 43% (Table 5)).
Anodal tDCS was, by contrast, successful in 53% of tested patients. However, the effect
reached statistical significance in only 30% of them. Follow-up tests showed that in only 41%
of patients there was a lasting effect of tDCS over 6 months, which was statistically
significant in only 14% of those (Table 5).
A direct comparison of the amount of motor improvement to be achieved by cathodal tDCS
and anodal tDCS showed similar results: cathodal tDCS caused a 40% improvement of the
affected upper limb, anodal tDCS, by contrast, only a 20% improvement.
On the basis of the pertinent literature bilateral tDCS appears to be a highly effective protocol
to improve upper limb disability after stroke.
Bilateral tDCS improved hand motor function in all patients, but improvement reached the
level of statistical significance in about 75% of these. Follow-up investigation revealed a
lasting effect of bilateral tDCS for up to four weeks in all patients tested, but this effect was
statistically significant in only 62% of them (Table 5). In addition, bilateral tDCS caused
greater effect sizes than facilitatory tDCS and inhibitory tDCS alone.
Two-thirds of studies investigating the effectivity of tDCS on motor recovery of the affected
upper limb after stroke used a stimulation intensity of 1mA. Other stimulation intensities
(2mA, 1,5mA, 1,2mA, 0,5mA) were less widely applied. However current findings indicate a
smaller beneficial effect of 2mA tDCS compared with 1mA tDCS.
Patients characteristic dependent efficiency
Most studies tested patients with an ischemic stroke. Only recently researchers also included
more and more patients with haemorrhagic stroke aetiology. These studies showed a
comparable efficiency of tDCS to improve upper limb function in ischemic and haemorrhagic
stroke. Future studies should test the efficiency of tDCS on the motor recovery in larger study
cohorts of stroke patients with either stroke aetiology.
The majority of studies included patients with subcortical and cortical lesion. Some studies
tested only patients with subcortical lesions. The current data do not show any significant
difference in the efficiency of tDCS on upper limb improvement in patients with subcortical

Page 16 of 32
Accep
ted
Man
uscr
ipt
and cortical lesions. However, more data on larger study populations are needed before
definitive conclusions upon the differential effectiveness of various stimulation protocols in
subcortical and cortical stroke locations can be drawn.
At present the best positive evidence of the effect of the tDCS on motor recovery after stroke
exists mainly for patients with a chronic stroke. For patients with a subacute stroke, there are
hardly any data. There are some studies which tested the patients with acute stroke. These
studies show (compared with studies on patients with a chronic stroke) a smaller efficiency of
the tDCS on motor recovery. The facilitatory tDCS brought in patients with acute stroke even
further negative effect.
Most trials investigated the efficiency of tDCS in patients with a moderate to mild impairment
of the affected upper limb. Patients with a more severe motor impairment were much less
under investigation. Despite the fact that studies on the efficiency of tDCS in severely
affected stroke survivors are scarce, this should not be interpreted that tDCS is not effective in
this subpopulation. Again, more data on larger study cohorts are needed to underpin this
assumption. For example, a recent study indicated that inhibitory tDCS improved selective
proximal upper limb control for mildly impaired patients and worsened it for moderate to
severely impaired patients (Brandnam et al., 2012).
Conclusion This review implies that tDCS is safe and effective to support motor recovery of the affected
hand after stroke, however, data are to limited upon today to support its routine use.
The best evidence for the positive effect exists presently on patients with a chronic stroke
suffering from moderate to mild impairment of one upper limb. In contrast, current findings
imply small beneficial effect for patients with acute stroke. Moreover, present fMRI and
connectivity studies show that the neural plasticity and their impact on motor recovery after
stroke are much more complex than the interhemispheric imbalance model represent and not
completely understanding. Consequently, novel hypothetical concepts and surrogate markers
should be developed to predict the potential effectiveness of tDCS in an individual stroke
patient depending on lesion location, distribution, time from stroke and severity of motor
disability among other factors.
acute stroke <1 month after symptom onset
subacute stroke 1-6 months after symptom onset
chronic stroke >6 months after symptom onset

Page 17 of 32
Accep
ted
Man
uscr
ipt
References
Ang, K.K., Guan, C., Phua, K.S., Wang, C., The, I., Chen, C.W., Chew, E., 2012 Transcranial
direct current stimulation and EEG-based motor imagery BCI for upper limb stroke
rehabilitation. Conference proceedings: ....Annual International Conference of the IEEE
Engineering in Medicine and Biology Society. Conference. 2012, 4128-4131.
Bestmann, S., Swayne, O., Blankenburg, F., Ruff, C.C., Teo, J., Weiskopf, N., Driver, J.,
Rothwell, J.C., Ward, N.S., 2010. The role of contralesional dorsal premotor cortex after
stroke as studied with concurrent TMS-fMRI. The Journal of Neuroscience. 30, 11926-11937.
Boggio, P.S., Nunes, A., Rigonatti, S.P., Nitsche, M.A., Pascual-Leone, A., Fregni, F., 2007.
Repeated sessions of noninvasive brain DC stimulation is associated with motor function
improvement in stroke patients. Restorative neurology and neuroscience. 25, 123-129.
Bolognini, N., Vallar, G., Casati, C., Latif, L.A., El-Nazer, R., Williams, J., Banco, E., Macea,
D.D., Tesio, L., Chessa, C., Fregni, F., 2011. Neurophysiological and behavioral effects of
tDCS combined with constraint-induced movement therapy in poststroke patients.
Neurorehabilitation and neural repair. 25, 819-829.
Brandnam, L.V., Stimear, C.M., Barber, P.A, Byblow, W.D., 2012. Contralesional
hemisphere control of the proximal paretic upper limb following stroke. Cerebral Cortex. 22,
2662-2671.
Carter, A.R., Patel, K.R., Astafiev, S.V., Snyder, A.Z., Rengachary, J., Strube, M.J., Pope, A.,
Shimony, J.S., Lang, C.E., Shulman, G.L., Corbetta, M., 2012. Upstream dysfunction of
somatomotor functional connectivity after corticospinal damage in stroke. Neurorehabilitation
and Neural Repair. 26, 7-19.
Fregni, F., Boggio, P.S., Mansur, C.G., Wagner, T., Ferreira, M.J., Lima, M.C., Rigonatti,
S.P., Marcolin, M.A., Freedman, S.D., Nitsche, M.A., Pascual-Leone, A., 2005. Transcranial
direct current stimulation of the unaffected hemisphere in stroke patients. Neuroreport. 16,
1551-1555.

Page 18 of 32
Accep
ted
Man
uscr
ipt
Fusco, A., De Angelis, D., Morone, G., Maglione, L., Paolucci, T., Bragoni, M., Venturiero,
V., 2013. The ABC of tDCS: Effects of Anodal, Bilateral and Cathodal Montages of
Transcranial Direct Current Stimulation in Patients with Stroke-A Pilot Study. Stroke research
and treatment. 2013, 837595.
Grefkes, C., Eickhoff S.B., Nowak, D.A., Dafotakis, M., Fink, G.R., 2008. Dynamic intra-
and interhemispheric interactions during unilateral and bilateral hand movements assessed
with fMRI and DCM. Neuroimage. 41, 1382-1394.
Grefkes, C., Fink G.R., 2014. Connectivity-based approaches in stroke and recovery of
function. The Lacent Neurology. 13, 206-216.
Grefkes, C., Nowak, D.A., Eickhoff, S.B., Dafotakis, M,, Küst, J., Karbe, H., Fink, G.R.,
2008. Cortical connectivity after subcortical stroke assessed with functional magnetic
resonance imaging. Annals of neurology, 63, 236-246
Grefkes, C., Ward, N.S., 2014. Cortical Reorganization After Stroke: How Much and How
Functional? The Neuroscientist. 20, 56-70.
Hesse, S., Waldner, A., Mehrholz, J., Tomelleri, C., Pohl, M., Werner, C., 2011. Combined
transcranial direct current stimulation and robot-assisted arm training in subacute stroke
patients: an exploratory, randomized multicenter trial. Neurorehabilitation and neural repair.
25, 838-846.
Hummel, F., Celnik, P., Giraux, P., Floel, A., Wu, W.H., Gerloff, C., Cohen, L.G., 2005.
Effects of non-invasive cortical stimulation on skilled motor function in chronic stroke. Brain.
128, 490-499.
Hummel, F.C., Voller, B., Celnik, P., Floel, A., Giraux, P., Gerloff, C., Cohen, L.G., 2006.
Effects of brain polarization on reaction times and pinch force in chronic stroke. BMC
neuroscience. 7, 73.
Jørgensen, H.S., Nakayama, H., Raaschou, H.O., Vive-Larsen, J., Støier, M., Olsen, T,S.,
1995. Part I: Outcome. The Copenhagen Stroke Study. Archives of Physical Medicine and
Rehabilitation. 76, 399-405.

Page 19 of 32
Accep
ted
Man
uscr
ipt
Jørgensen, H.S., Nakayama, H., Raaschou, H.O., Vive-Larsen, J., Støier, M., Olsen, T,S.,
1995. Outcome and time course of recovery in stroke. Part II: Time course of recovery. The
Copenhagen Stroke Study. Archives of Physical Medicine and Rehabilitation. 76, 406-412.
Khedr, E.M., Shawky, O.A., El-Hammady, D.H., Rothwell, J.C., Darwish, E.S., Mostafa,
O.M., Tohamy, A.M., 2013. Effect of Anodal Versus Cathodal Transcranial Direct Current
Stimulation on Stroke Rehabilitation: A Pilot Randomized Controlled Trial.
Neurorehabilitation and neural repair. 27, 592-601.
Kim, D.Y., Lim, J.Y., Kang, E.K., You, D.S., Oh, M.K., Oh, B.M., Paik, N.J., 2010. Effect of
transcranial direct current stimulation on motor recovery in patients with subacute stroke.
American journal of physical medicine & rehabilitation/ Association of Academis Physiatrits.
89, 879-886.
Kim, D.Y., Ohn, S.H., Yang, E.J., Park, C.I., Jung, K.J., 2009. Enhancing motor performance
by anodal transcranial direct current stimulation in subacute stroke patients. American journal
of physical medicine & rehabilitation/ Association of Academis Physiatrits. 88, 829-836.
Kolominsky-Rabas, P.L., Weber, M., Gefeller, O., Neundoerfer, B., Heuschmann, P.U., 2001.
Epidemiology of ischemic stroke subtypes according to the TOAST criteria: incidence,
recurrence, and long-term survival in ischemic stroke subtypes: a population-based study.
Stroke. 32, 2735-2740.
Lang, N., Siebner, H.R., 2007. Repetitive transkranielle Magnetstimulation, in: Siebner, H.R.,
Ziemann, U. Das rTMS Buch. Heidelberg, pp. 499-513.
Lefebvre, S., Laloux, P., Peeters, A., Desfontaines, P., Jamart, J., Vandermeeren, Y., 2012.
Dual-tDCS Enhances Online Motor Skill Learning and Long-Term Retention in Chronic
Stroke Patients. Frontiers in human neuroscience. 6, 343.
Lindenberg, R., Renga, V., Zhu, L.L., Nair, D., Schlaug, G., 2010. Bihemispheric brain
stimulation facilitates motor recovery in chronic stroke patients. Neurology. 75, 2176-2184.
Loubinoux, I., Carel, C., Pariente, J., Dechaumont, S., Albucher, J.F., Marque, P., Manelfe,
C., Chollet, F., 2003. Correlation between cerebral reorganization and motor recovery after
subcortical infarcts. NeuroImage. 20, 2166-2180.

Page 20 of 32
Accep
ted
Man
uscr
ipt
Madhavan, S., Shah, B., 2012. Enhancing motor skill learning with transcranial direct current
stimulation - a concise review with applications to stroke. Frontiers in psychiatry. 3, 66.
Madhavan, S., Weber, K.A. 2nd, Stinear, J.W., 2011. Non-invasive brain stimulation
enhances fine motor control of the hemiparetic ankle: implications for rehabilitation.
Experimental brain research. 209, 9-17.
Mahmoudi, H., Borhani Haghighi, A., Petramfar, P., Jahanshahi, S., Salehi, Z., Fregni, F.,
2011. Transcranial direct current stimulation: electrode montage in stroke. Disability and
rehabilitation. 33, 1383-1388.
Marshall, R.S., Perera, G.M., Lazar, R.M., Krakauer, J.W., Constantine, R.C., DeLaPaz, R.L.,
2000. Evolution of cortical activation during recovery from corticospinal tract infarction.
Stroke. 31, 656-661.
Nair, D.G., Renga, V., Lindenberg, R., Zhu, L., Schlaug, G., 2011. Optimizing recovery
potential through simultaneous occupational therapy and non-invasive brain-stimulation using
tDCS. Restorative neurology and neuroscience. 29, 411-420.
Nitsche, M.A., Cohen, L.G., Wassermann, E.M., Priori, A., Lang, N., Antal, A., Paulus, W.,
Hummel, F., Boggio, P.S., Fregni, F., Pascual-Leone, A., 2008; Transcranial direct current
stimulation: State of the art 2008. Brain Stimulation. 1, 206-23.
Nitsche, M.A., Paulus, W., 2000. Excitability changes induced in the human motor cortex by
weak transcranial direct current stimulation. The Journal of physiology. 3, 633-639.
Nitsche, M.A., Paulus, W., 2007. Transkranielle Gleichstromstimulation, in: Siebner, H.R.,
Ziemann, U. Das rTMS Buch. Heidelberg, pp. 533-542.
Nowak, D.A., Bösl, K., Podubeckà, J., Carey, J.R., 2010. Noninvasive brain stimulation and
motor recovery after stroke. Restorative Neurology and Neuroscience. 28, 531-544.
Nowak, D.A., Grefkes, C., Ameli, M., Fink, G.R., 2009. Interhemispheric competition after
stroke: brain stimulation to enhance recovery of function of the affected hand.
Neurorehabilitation and neural repair. 23, 641-656.

Page 21 of 32
Accep
ted
Man
uscr
ipt
Ochi, M., Saeki, S., Oda, T., Matsushima, Y., Hachisuka, K., 2013. Effects of anodal and
cathodal transcranial direct current stimulation combined with robotic therapy on severely
affected arms in chronic stroke patients. Journal of rehabilitation medicine. 45, 137-140.
O'Shea, J., Boudrias, M.H., Stagg, C.J., Bachtiar, V., Kischka, U., Blicher, J.U., Johansen-
Berg, H., 2014. Predicting behavioural response to TDCS in chronic motor stroke.
NeuroImage. 85, 924-933.
Park, C.H., Chang, W.H., Ohn, S.H., Kim, S.T., Bang, O.Y., Pascual-Leone, A., Kim, Y.H.,
2011. Longitudinal changes of resting-state functional connectivity during motor recovery
after stroke. Stroke. 42, 1357-1362.
Rehme, A.K., Eickhoff, S.B., Rottschy, C., Fink, G.R., Grefkes, C., 2012. Activation
likelihood estimation meta-analysis of motor-related neural activity after stroke. NeuroImage.
59, 2771-2782.
Rehme, A.K., Eickhoff S.B., Wang L.E., Fink G.R., Grefkes C., 2011. Dynamic causal
modeling of cortical excitability from the acute to the chronic stage after stroke. Neuroimage.
55, 1147-1158.
Rehme, A.K., Fink, G.R., von Cramon, D.Y., Grefkes, C., 2011. The role of the contralesional
motor cortex for motor recovery in the early days after stroke assessed with longitudinal
FMRI. Cerebral Cortex. 21, 756-768.
Rossi, C., Sallustio, F., Di Legge, S., Stanzione, P., Koch, G., 2013. Transcranial direct
current stimulation of the affected hemisphere does not accelerate recovery of acute stroke
patients. European journal of neurology. 20, 202-204.
Schallert, T., Leasure, J.L., Kolb, B., 2000. Experience-associated structural events,
subependymal cellular proliferative activity, and functional recovery after injury to the central
nervous system. Journal of Cerebral Blood Flow & Metabolism. 20, 1513-1528.
Stagg CJ, Bachtiar V, O'Shea J, et al. Cortical activation changes underlying stimulation-
induced behavioural gains in chronic stroke. Brain 2012; 135:276-284.
Takeuchi, N., Tada, T., Matsuo, Y., Ikoma, K., 2012. Low-frequency repetitive TMS plus
anodal transcranial DCS prevents transient decline in bimanual movement induced by

Page 22 of 32
Accep
ted
Man
uscr
ipt
contralesional inhibitory rTMS after stroke. Neurorehabilitation and neural repair. 26, 988-
998.
Taylor, T.N., Davis, P.H., Torner, J.C. Holmes, J., Meyer, J.W., Jacobson, M.F., 1996.
Lifetime cost of stroke in the United States. Stroke. 27, 1459-1466.
Volz, L.J., Sarfeld A.S., Diekhoff S., Rehme A.K., Pool E.M., Eickhoff S.B., Fink G.R.,
Grefkes C., 2014. Motor cortex excitability and connectivity in chronic stroke: a multimodal
model of functional reorganization. Brain structure & function. Epub ahead of print
Wang, L., Yu, C., Chen, H., Qin, W., He, Y., Fan, F., Zhang, Y., Wang, M., Li, K., Zang, Y.,
Woodward, T.S., Zhu, C., 2010. Dynamic functional reorganization of the motor execution
network after stroke. Brain. 133, 1224-1238.
Wu, D., Qian, L., Zorowitz, R.D., Zhang, L., Qu, Y., Yuan, Y., 2013. Effects on decreasing
upper-limb poststroke muscle tone using transcranial direct current stimulation: a randomized
sham-controlled study. Archives of physical medicine and rehabilitation. 94, 1-8.
Zimerman, M., Heise, K.F., Hoppe, J., Cohen, L.G., Gerloff, C., Hummel, F.C., 2012. Modulation of training by single-session transcranial direct current stimulation to the intact motor cortex enhances motor skill acquisition of the paretic hand. Stroke. 43, 2185-219.

Page 23 of 32
Accep
ted
Man
uscr
ipt
‐ Highlights
‐ We review the literature on tDCS in rehabiliation of the affected hand after stroke.
‐ We found overall 23 placebo‐controlled trials.
‐ All stimulation protocols pride on interhemispheric imbalance model.
‐ TDCS is associated with improvement of the affected upper limb after stroke.
‐ Current evidence does not support its routine use.

Page 24 of 32
Accep
ted
Man
uscr
ipt
Intensity Duration
20 min 1 JTHF 9% (*) -3% na na 2
1 mA 20 min 1 reaction time 6% (*) -5% - - 2
pinch force 4% -3% - -
1 mA 20 min 1 BBT 21% (*) 3% 18% (*) 3% 2
finger
acceleration
67% (*) 0% 42% (*) -15%
0,5
mA
15 min 1 tDCS
les
tDCS
non-les
tDCS
sham1
tracking
accuracy
18% (**) -1% (*) 7% - -
MEPipsiles 29% 8% 11% - -
MEPcontrales -12% 13% 4% - -
2 mA 20 min 5 FM(UL) 83% 101% 2
5 participants; age: na; time
from stroke: na; lesion
location: na; stroke
epidemiology: na; upper limb
impairment: na
1 mA 20 min 10 randomized;
parallel-
group; sham-
controlled
2 experimental
groups: tDCSreal
+ MP (n=3),
tDCSsham + MP
(n=2)
accuracies of
detecting
motor imagery
2% -20% - - 2
50 participants; age 68,2±13,9
years; 1 day after the stroke;
ischemic corical (n=38) and
subcortical (n=12) stroke;
moderate to mild motor
impairment of upper limb
1 mA double-blind;
crossover;
sham-
controlled;
longitudinal
randomized;
parallel-
group;
double-blind;
sham-
controlled;
longitudinal
tDCS
sham
Patients charakteristics Study
description
Assesment Follow upStimulation
232%
tDCS
real
OG
SC
Study
design
Outcome
2 experimental
groups: tDCSreal,
tDCSsham; 3
months after
stroke follow up
2 experimental
sessions:
tDCSanodal,
tDCSsham; 10
days follow up
2 experimental
sessions:
tDCSanodal,
tDCSsham
Table 1. Facilitatory tDCS in promoting motor recovery of the affected hand after stroke
10 participants; age 62,8±12,5
years; 6,4±3 months after the
stroke; ischemic (n=8) and
hamorrhagic (n=2), subcortical
(n=9) and cortical (n=1) stroke;
moderate to mild impairment of
upper limb
single-blind;
crossower;
sham-
controlled
2 experimental
sessions:
tDCSreal,
tDCSsham; 60
mitutes follow up
6 participants; age 62,2±7,56
years; 3,7±1,1 years after the
stroke; ischemic subcortical
stroke; moderate to mild motor
impairment of upper limb
Number
section
tDCS
real
tDCS
sham
11 participants; age 57±16
years; 41,8±26,4 months after
the stroke; ischemic
subcortical stroke; moderate to
mild motor impairment of
upper limb
pseudo-
randomized;
double-blind;
crossover;
sham-
controlled
9 participants; age 65,4±13,2
years; 10,9±6,7 years after the
stroke; ischemic cortical (n=2)
and subcortical (n=7) stroke;
moderate to mild motor
impairment of upper limb
crossover;
sham-
controlled
3 experimental
sessions:
tDCSreal over
lesioned M1 +
TM, tDCSreal
over non-lesioned
M1 + TM,
tDCSsham + TM
Table(s)

Page 25 of 32
Accep
ted
Man
uscr
ipt
Patients charakteristics Study
description
Assesment
1 mA 30 min 5 FM(UL) na na 14% (*) 6% 3
ROM 16% 1% 16% (*) 4%
1,2 mA 20 min 20 FM(UL) 83% (**) 25% #### (**) 88% 4
MAS elbow 50% (**) 0% 50% (**) -50%
MAS wrist 50% (**) 0% 50% (**) -50%
1 mA 20 min 1
finger
movement
task
56% (*) 17% na (*) na 5
MEPipsiles -29% (*) na na na
SICIipsiles na (*) na na na
SICIcontrales na (*) na na na
Duration
14 participants; age
58,5±13,5 years; 30,5±24
months after the stroke;
ischemic cortical (n=9) and
subcortical (n=5) stroke;
moderate to severe motor
impairment of upper limb
randomized;
paralle-group;
double-blind;
sham-
controlled;
longitudinal
2 experimental
groups:
tDCSreal+OT;
tDCSsham+OT; 7
days follow up
correlation between FM(UL)-improvement and
decreased activation in the contralesional motor
cortex (FMRI)
Table 2. Inhibitory tDCS in promoting motor recovery of the affected hand after stroke
Stimulation Study design Outcome Follow up
Number
section OG
SC
Intensity
correlation between finger movement task-
improvement and SICIipsiles-change (r2=0,63)
tDCS
sham
2 experimental
sessions:
tDCSreal+MT,
tDCSsham+MT;
90min, 24 hours
and 90 days (5
participants)
follow up
tDCS
real
tDCS
sham
tDCS
real
90 participants; age
47,6±11,9 years; 4,9±3,0
months after the stroke;
lesion location: na; ischemic
(n=53) and hemorrhagic
(n=37) stroke, moderate to
severe motor impairment of
upper limb
cathode over M1
ipsilesional, anode over
the unaffected shoulder
randomized;
parallel-group;
double-blind;
sham-
controlled;
longitudinal
5 block á 3 minutes
with 2 minutes breaks
double-blind;
crossover;
sham-controlled
12 participants; age
58,3±13,3 years; 33,4±15,8
months after the stroke;
subcortical ischemic stroke;
moderate to mild motor
impairment of upper limb
2 experimental
groups:
tDCSreal+PT,
tDCSsham+PT; 4
weeks follow up
24 hours
Table(s)

Page 26 of 32
Accep
ted
Man
uscr
ipt
6 participants; age 53,7
years; 27,1 months after
the stroke; lesion location:
na; mild to moderate
motor impairment of
upper limb
1 mA 20 min 1 randomized;
crossover;
double-blind;
sham-
controlled
3 experimental
sessions:
tDCScathodal,
tDCSanodal,
tDCSsham
JTHF 6,8% (*) 11,7% (*) 4% - - - 3 Fregni et
al. 2005
9 participants; age
57,4±12,9 years; 40,9
months after the stroke;
subcortical stroke;
etiology of stroke: na;
mild to moderate motor
impairment of upper limb
1 mA 20 min 20 double-blind;
crossover;
sham-
controlled
3 experimental
treatments:
tDCSanodal,
tDCScathodal,
tDCS sham
JTHF 7,3% (*) 9,5% (*) na - - - 2 Boggio et
al. 2007
18 participants; age
57,8±13,0 years;
25,6±16,7 days after the
stroke; ischemic cortical
(n=5), corticosubcortical
(n=4) and subcortical
(n=9) stroke; moderate to
mild motor impairment of
upper limb
2mA 20 min 10 randomized;
parallel-
group;
double-blind;
sham-
controlled;
longitudinal
3 experimental
groups:
tDCSanodal,
tDCScathodal,
tDCSsham; 6
months follow
up
FM(UL) 45% 35% 20% 85% 53% 2% 5 Kim et al.
2010
2mA 20 min 30 FM(UL) 145% 139% 134% 197% 197% 174% 5
BBT na na na na na na
MRC 240% 372% 277% 234% 366% 297%
MAS 106% 250% 150% 125% 250% 171%
1 mA 20 min
10 min
1 response time
task (exp. 1)
5% (*) 0% (*) -7% - - - 1 Stagg et
al. 2012
grip force task na na na - - -
response time
task (exp. 2)
10% (*) -2% -10% - - -
MRI ipsiles 85% 10% - - -
MRI contrales 45% 5% - - -
1 mA 10 min 5 FM(UL) 6% 4% - - - - 2
MAS Elbow 12% 20% - - - -
MAS Wrist 20% 17% - - - -
MAS Finger 17% 28% (*) - - - -
MAL 6% 6% - - - -
hand grip
strenght
120% 79% 50% 193% 132% 125%
shoulder
abduction
88% 113% 10% 147% 175% 75%
rMTcontrales -2% -4% -3%
rMTipsiles "-20% (**) "-14%
(*)
"-6% (*)
aMTcontrales -1% -1% -4%
aMTipsiles "-21% (**) "-14%
(*)
"-8% (*)
3 months 5 Khedr et
al. 2013
correlation between the change in MT and increase in grip
strength
2mA 25 min 6 randomized;
paralell-
group;
double-blind;
sham-
controlled;
18 participants; age 61,1
years; 4,4 years after the
stroke; ischemic (n=7)
and hemorrhagic (n=11);
subcortical and cortical
stroke; moderate to
severe motor impairment
of upper limb
randomized;
double-blind;
crossover
2 experimental
treatments:
tDCSanodal+R
AAT,
tDCScathodal+
RAAT
Ochi et al.
2013
the patients with right hemispheric lesion improved significantly
larger with DCScathodal then with tDCSanodal
tDCSanodal - a negative correlation between decreases in
response time and increases in task-related cortical activation
in the ipsilesional M1
17 participants; age 63,5
years; 38 months after
the stroke; ischemic
(n=16) and hemorrhagic
(n=1), subcortical (n=10)
and cortical (n=7) stroke;
moderate to mild motor
impairment of upper limb
randomized;
crossover;
sham-
controlled;
crossover
3 experimental
sessions:
tDCSanodal,
tDCScathodal,
tDCSsham
96 participants; age
65,0±9,8 years; 3,1±1,6
weeks after the stroke;
ischemic subcortical and
cortical stroke; severe
motor impairment of
upper limb
randomized;
parallel-
group;
double-blind;
sham-
controlled;
multicenter;
longitudinal
3 experimental
groups:
tDCSanodal +
BRT,
tDCScathodal +
BRT,
tDCSsham +
BRT; 3 months
follow up
OG
SCAssesment
Number
section
Intensity Duration
Patients charakteristics Study
description
tDCScathodal - the patients with a subcortical lesion improved
significantly larger then those patients with a cortical
involvement
Outcome
tDCS
anodal
tDCS
cathodal
tDCS sham
Follow up
40 participants; age
58,4±8,9 years; 12,9±4,9
days after the stroke;
subcortical (n=14) and
cortical (n=26) ischemic
stroke; moderate to mild
motor impairment of
upper limb
3 experimental
groups:
tDCSanodal,
tDCScathodal,
tDCSsham; 1, 2,
and 3 months
follow up
Table 3. Facilitatory and inhibitory tDCS in promoting motor recovery of the affected hand after stroke
tDCS
anodal
tDCS
cathodal
tDCS
sham
Refere
nce
Stimulation Study
design
Hesse et
al. 2011
Table(s)

Page 27 of 32
Accep
ted
Man
uscr
ipt
1 mA 30 min 5 FM(UL) 15.0% 3.0% 16.0% 3.0% 4
WMFT 15.0% 5.0% 16.0% 6.0%
2 mA 40 min 10 3JTHF 33% (*) 3% 29% (*) 9%
Handgrip
Strenght
33% (*) -14% 48% (*) -6%
FM(UE) 25% (*) 7% 31% (*) 4%
MAL 75% 42% 75% 59%
MEP ipsiles 21% (*) -9%
TI ipsiles 34% (*) 14%
TI contrales 0% 1%
1mA 20 min 1 JTHF 15% (*) A: 11% (*) 8% (*) 1% 2
B: 4%
rTMS+ tDCS tDCS rTMS rTMS+
tDCS
tDCS rTMS
pinch force 14% (**) -1% 9% (*) 24% (**) 5% 19% (*)
acceleration 22% 10% 22% 26% 11% 22%
bimanual
coordination
5% 7% 24% (**) 8% 6% 8%
MEPcontrales "-24% (**) -3% "-21% (**) 0% -1% 3%
MEP ipsiles 24% (**) 20% (**) 22% (*) -2% -3% 3%
TCI contrales -14% -9% "-24% 1% 1% 1%
TCI ipiles 16% -2% 2% -1% 2% -1%
TCI ratio "-25% (**) -3% "-26% (**) 5% 1% 5%
correlation between bimanual coordination- and TCI contrales-changes (r=-0,486)
1 NHPT 14% 34% 19% "-1%-11% - - - - 1
grip force -7% 0% 13% 0% - - - -
30 min 1 4
PPT 19% 0% 13% (*) 3%
grip force -1% -4% 0% 5%
learning index na na 44% 4%
correlation between pinch force- and TIC ratio-changes (r=-0,477)
9 participants; age
53,5±20,7 years;
28,3±10,4 days after
the stroke; ischemic
(n=8) and
hemorrhagic (n=1),
cortical and
subcortical stroke;
upper limb
impairment: na
1,5mA 15 min single-
blind;
sham-
controlled;
crossover
3 experimental
groups:
tDCSanodal
(n=3),
tDCScathodal
(n=3),
tDCSbilateral
(n=3)
20 min 1 longitudinal
; parallel-
group
3 experimental
groups:
tDCSanodal,
rTMSinhibitory,
DCSanodal+rT
MSinhibitory; 1
session; 30min
and 7days
follow up
07 days
Table 4. Bilateral tDCS in promoting motor recovery of the affected hand after stroke
tDCS anodal tDCS
anodal
tDCS
sham
Stimulation Study
design
Assesment
OG
SC
tDCS
bilateral
tDCS
cathodal
Follow up
tDCSbilateral - correlation between WMFT- and precentral gyrus
activation laterality- changes
tDCSbilateral - stronger activation of intact ipsilesional motor regions
during paced movements of the affected limb then tDCSsham
correlation between TI ipsiles- and JTHF- changes (r=-0,55)
patients with subcortical lesion: the effect after tDCSbilateral was
almost twice as large compared with tDCS cathodal and tDCSanodal
correlation between MEP ipsiles- und FM(UE)- changes (r=0,67)
4 weeks
Outcome
tDCS bilateral tDCS
cathodal
5 experimental
sessions:
tDCSbilateral,
tDCScathodal,
tDCSanodalA
(cathode over
contralateral
supraorbital
area),
tDCSanodalB
(cathode on
contralateral
deltoid muscle),
tDCSsham
tDCS
sham
double-
blind;
parallel-
group;
sham-
controlled;
longitudinal
2 experimental
groups:
tDCSbilateral +
CIMT,
tDCSsham +
CIMT; 2 and 4
weaks follow up
double-
blind;
parallel-
group;
sham-
controlled;
longitudinal
2 experimantal
groups:
tDCSbilateral,
tDCSsham; 3
and 7 days
follow up
19 participants; age
61±9 years; 2,6±1,5
years after the stroke;
ischemic (n=16) and
hemorrhagic (n=2),
subcortical (n=7) and
cortical (n=11) stroke;
moderate to mild
motor impairment of
upper limb
Intensity Duration Number
section
20 participants; age
58,8±13,8 years;
35,4±22,4 months
after the stroke;
ischemic subcortical
stroke; moderate to
mild motor impairment
of upper limb
10 participants; age
60,8±14,1 years;
8,3±5,5 months after
the stroke; ischemic
cortical (n=7),
subcortical (n=2) and
brainstem (n=1)
stroke; morderate to
mild motor impairment
of upper limb
Patients
charakteristics
14 participants; age
46,7±13,6 years;
35,2±25,5 months
after the stroke;
ischemic (n=12) and
hemorrhagic (n=2);
subcortical (=5) and
cortical (n=9) stroke;
moderate to mild
motor impairment of
upper limb
27 participants; age
61,5±7,6 years;
67,1±48,4 months
after the stroke;
ischemic and
hemorrhagic
subcortical stroke;
moderate to mild
motor impairment of
upper limb
1 mA
tDCS
1Hz
rTMS
90%
rMT
Study
description
randomized
; double-
blind; sham-
controlled;
crossover;
longitudinal
2 experimental
sessions:
tDCSbilateral+
MT,
tDCSsham+MT;
30min, 60min
and 1 weak
follow up
1 mA 1 Woche
(**)
(**) (**)
double-
blind; sham-
controlled,
randomized
; crossover
Table(s)

Page 28 of 32
Accep
ted
Man
uscr
ipt
Study
description
1mA 20 min 1 reaction
time
2%(*) 6%(*) 0%(*) -7% - - - - 0
MI-BCI motor imagery Brain-Computer Interface RAAT robot-assisted arm training
JTHF Jebsen Taylor Hand Function Test MAL Motor Activity Log
na not available aMT active motor treshold
PNS peripheral nerve stimulation rMT resting motor treshold
BBT Box and Block Test PT physical therapy
TM Tracking movements WMFT Wolf Motor Function Test
FM(UL) Flugl-Meyer (upper limb) TI Transcallosal inhibition
MP motor practise NHPT Nine-Hole-Peg-Test
OT occupational therapy PPT Purdue Pegboard Test
ROM Range-Of-Motion (*) (**) along a numeral a significant time-effect for this group but not for the control group
MAS Modified Ashworth Scale (*) (**) between two numerals a significant between-groups-difference
MT motor training
SICI Short Interval Intracortical Inhibition
MRC Medical Research Counsil
MAS Modified Ashworth-Summenscore
BRT bilateral robot training
BBT Box and Block Test
Table 4. (continued) bilateral tDCS in promoting motor recovery of the affected hand after stroke
Follow up
OG
SC Refere
ncetDCS
sham
tDCS
bilateral
tDCS
sham
OutcomePatients charakteristics
13 participants; age 66 years;
time after stroke: na; lesion
location: na; etiology of stroke:
na; moderate to mild
impairment of upper limb
sham-
controlled;
crossover
4 experimental
sessions:
tDCSbilateral,
tDCSanodal,
tDCScathodal,
tDCSsham
Number
section
tDCS
cathodal
tDCS
bilateral
tDCS
anodal
tDCS
cathodal
tDCS
anodal
O´Shea et
al. 2013
correlation between the effects of anodal and cathodal tDCS (r= 0,6)
and between cathodal and bilateral tDCS (r=0,65)
Stimulation Study
design
Assesm
entIntensity Duration
Table(s)

Page 29 of 32
Accep
ted
Man
uscr
ipt
facilitatory tDCS inhibitory tDCS bilateral tDCS
placebocontrolled trials 15 (n=309) 12 (n=304) 6 (n=112)
placebocontrolled trials with a positive
effect
13 (n=163)
9 (n=91)
of this with a statistical
significance
12 (n=304)
7 (n=127)
of this with a statistical
significance
6 (n=112)
4 (n=83)
of this with a statistical
significance
placebocontrolled trials without a
positive effect2 (n=146) 0 (n=0) 0 (n=0)
placebocontrolled trials with follow up 5 (n=214) 6 (n=270) 3 (n=53)
placebocontrolled trials with a positive
effect by follow up
3 (n=88)
1 (n=30)
of this with a statistical
significance
6 (n=270)
3 (n=116)
of this with a statistical
significance
3 (n=53)
2 (n=33)
of this with a statistical
significance
placebocontrolled trials without a
positive effect by follow up2 (n=146) 0 (n=0) 0 (n=0)
Tab. 5 The review of the trials, which investigated the efect of the facilitatory tDCS, the inhibitory tDCS and the bilateral
tDCS for motor recovery of the affected upper limb after stroke
Table(s)

Page 30 of 32
Accep
ted
Man
uscr
ipt
Figure 1: Increase of cortical excitability within the ipsilesional M1 by facilitatory (anodal)
tDCS. The anodal electrode (+) is placed over standard scalp coordinates for ipsilesional M1,
the cathodal electrode (-) over the contralesional supraorbital rige.
Figure

Page 31 of 32
Accep
ted
Man
uscr
ipt
Figure 2: Decrease of cortical excitability within the contralesional M1 (thereby reducing the
transcallosal inhibition drive towards ipsilesional M1) by means of inhibitory (cathodal)
tDCS. The cathodal electrode (-) is placed over standard scalp coordinates for contralesional
M1, the anodal electrode (+) over the ipsilesional supraorbital rige.
Figure

Page 32 of 32
Accep
ted
Man
uscr
ipt
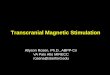
Figure 3: Increase of cortical excitability within ipsilesional M1 by stimultaneous bilateral
tDCS. The anodal electrode (+) is placed over standard scalp coordinates for ipsilesional M1,
the cathodal electrode (-) over standard scalp coordinates for contralesional M1.
Figure