Embed Size (px)
Citation preview

Pediatric Interventions
Transcatheter Closure of a Large Residual Shunt AfterDeployment of the Das-Angel Wings Device Using
the Amplatzer Septal Occluder
Wei Zhu, MD, Qi-Ling Cao, MD, and Ziyad M. Hijazi, *† MD
A 35-year-old female patient with a large residual shunt following transcatheter closure ofa large secundum atrial septal defect using the Das-Angel Wings device underwentsuccessful complete closure of the residual shunt using a 15-mm Amplatzer SeptalOccluder. Transesophageal (two- and three-dimensional) echocardiography was ofgreat help during the closure procedure. Cathet. Cardiovasc. Intervent. 48:184–187,1999. r 1999 Wiley-Liss, Inc.
Key words: catheter closure; ASD; residual shunt; Amplatzer
INTRODUCTION
The majority of secundum type of atrial septal defects(ASD) are amenable for transcatheter closure techniquesusing various investigational devices. However, a majordrawback of this form of therapy is the high incidence ofresidual shunt, especially after certain types of closuredevices. The Amplatzer septal occluder is a new self-centering device introduced over the last 2–3 years. Thisdevice combines certain characteristics to make it anideal closure device: high rate of complete closure, abilityto reposition or retrieve the device prior to release shoulda mistake in deployment is made without damaging theprosthesis itself, and the small introducer sheath requiredfor delivery [1,2]. There are few thousands of patientswho underwent catheter closure of their ASDs usingvarious investigational devices. Some of these patients(approximately 5%) ended with moderate to large re-sidual shunts requiring further management. We report ona patient who previously underwent catheter closure of amoderate to large ASD using the Das-Angel Wingsdevice. An Amplatzer septal occluder was used to closethe residual shunt successfully and completely. We be-lieve that this is the first case in the literature of closure ofa residual shunt after an Angel Wings using the Am-platzer.
CASE REPORT
K.M. is a 35-year-old female patient who was diag-nosed to have a large secundum ASD. She had dyspnea
on exertion and easy fatigability. She was referred for thepossibility of transcatheter closure. Her physical examina-tion revealed normal first heart sound, fixed splitting ofthe second heart sound, grade II/VI systolic ejectionmurmur heard best at the left upper sternal border, and adiastolic rumble. An electrocardiogram (EKG) revealednormal sinus rhythm, right axis deviation, and evidenceof right ventricle enlargement. Transthoracic echocardiog-raphy (TTE) revealed the presence of moderate to largesecundum ASD with left-to-right shunt, right ventricleenlargement with an end-diastolic dimension of 40 mm.After an informed consent was obtained, the patient under-went routine right and left heart catheterization with the intentto close the defect with an Angel Wings device. The Qp/Qsratio was 3:1. Transesophageal echocardiography (TEE)under general endotracheal anesthesia revealed the presenceof a large secundum ASD measuring 19–24 mm. There were
Division of Cardiology, Department of Pediatrics, Floating Hospi-tal for Children at New England Medical Center, Tufts UniversitySchool of Medicine, Boston, Massachusetts
†In accordance with the policy of the Journal, the designated authordiscloses a financial or other interest in the subject discussed in thisarticle.
*Correspondence to: Dr. Ziyad M. Hijazi, Division of Cardiology,Department of Pediatrics, The University of Chicago ChildrensHospital, 5841 S. Maryland Ave., MC4051 Chicago, IL 60637.E-mail: [email protected]
Received 22 January 1999; Revision accepted 8 April 1999
Catheterization and Cardiovascular Interventions 48:184–187 (1999)
r 1999 Wiley-Liss, Inc.

enough rims surrounding the defect. The balloon stretcheddiameter was 21 mm.A30-mm Das-Angel Wings device wasutilized for closure. The first attempt at releasing the devicefailed. However, after jerking the delivery catheter and devicetwice, the device was released uneventfully.
However, the superior-posterior corner of the left atrialdisk prolapsed through the septum into the right atrium.This resulted in a large residual shunt, which wasvalidated both by TEE and angiography (5 mm). Sincethe device was stable, it was opted not to do anythingelse, hoping that the residual shunt will decrease withtime. During a 2-year follow-up (patient refused surgicalintervention), she was receiving 81 mg per day of aspirinand no significant change in her symptoms with enlargedright ventricle (end-diastolic dimension 31 mm), indicat-ing continued significance of the residual shunt. There-fore, the patient was catheterized again with the intentionto close the residual shunt using the new Amplatzer. Rightand left heart catheterization revealed normal pulmonaryartery pressures and a Qp/Qs ratio of 2:1. Angiography
was performed in the right upper pulmonary vein, whichrevealed the presence of the residual shunt at the superiormargin of the Angel Wings device. Continuous TEEmonitoring was performed during the entire procedure.This revealed that the superior/posterior corner of theAngel Wings device protruded into the right atrium (Fig.1). There were enough rims around the residual shunt andthe size of residual shunt was 11 mm by color DopplerTEE. Three-dimensional (3D) reconstruction was alsoperformed with TomTec 3D reconstruction computersystem. The 3D imaging provided an optimal view toshow the detailed structure of the residual shunt and ofthe Angel Wings device (Fig. 2). The morphologicappearance of the prolapsed device was demonstrated andfrom the en face view we were also sure that there wasenough superior and posterior rims for the new device toanchor on. The balloon stretched diameter using Med-itech sizing balloon (Boston Scientific, Watertown, MA)was at least 25 mm (pulling the balloon from left to rightenlarged the residual shunt significantly).
Fig. 1. Two-dimensional Transesophageal echocardiographic(TEE) images in the long axis view (A and B) and in the short axisview (C and D) pre- and postclosure of the residual shunt. A: Thesuperior corner of the Das-Angel Wings device (double thinarrow) protrudes into the right atrium resulting in a largeresidual defect (small arrow). B: Postclosure with a 15-mmAmplatzer (thick arrow). The Angel Wings device (double thinarrow) is being sandwiched between the two disks of the
Amplatzer (sandwich view). C: The posterior corner of the AngelWings device protrudes into the right atrium (double thin arrow)resulting in a large residual defect (small arrow). D: Postclosurewith the Amplatzer (thick arrow). The Angel Wings (double thinarrow) is being sandwiched between the two disks of theAmplatzer. LA: left atrium; SVC: superior vena cava; RA: rightatrium; AO: aorta.
Catheter Closure of Residual Shunt 185
We believed if we used a smaller device, close to thesize of the defect by 2- and 3D TEE, it would have beensufficient. Therefore, a 15-mm Amplatzer septal occluderwas successfully deployed using a 7 Frdelivery systemwithout much difficulty. The left atrial disk of theAmplatzer was positioned in the left atrium, close to theresidual defect and then the right atrial disk was posi-tioned in a way to sandwich the prolapsed corner of theAngel Wings between the defect and the right atrial disk.Immediately after the Amplatzer was released, TEErevealed no residual shunt and the Amplatzer device wasin good position across the superior-posterior margin ofthe Angel-Wings device, mimicking the sandwich view(Fig. 1). Furthermore, there was no Doppler evidence ofobstruction to the blood flow in the superior vena cava(SVC) or in the mouth of the right upper pulmonary vein
(RUPV). Three-dimensional reconstruction was also doneto validate the position of the second device (Fig. 2).Hemostasis was achieved, and the patient was awakenedand allowed to recover overnight. At her 6-week follow-up, she reported improved symptoms evidenced byimprovement in her exercise capacity (workload im-proved from 112 to 122 watts), a decrease in the rightventricle size from 31 mm prior to closure to 22 mm.
DISCUSSION
Transcatheter closure has been regarded as an accept-able alternative treatment for patients with secundumASD. However, there still exist some drawbacks inimplanting various devices. The common drawback is theresidual shunt, which was reported to be as high as
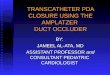
Fig. 2. Three-dimensional TEE en face views for the atrialseptum. A: From the right atrial side before deployment of theAmplatzer device demonstrating the prolapsed superior/poste-rior corner of the Angel Wings device (double thin arrow) andthe residual defect (small arrow). B: View from the left atrial sidedemonstrating the Angel Wings (double thin arrow) and theresidual defect (small arrow). C: View from right atrial side
postclosure with the Amplatzer (thick arrow) demonstrating theAngel Wings (double thin arrow) being sandwiched between theAmplatzer and the septum. D: View from the left atrial sidepostclosure demonstrating the Amplatzer device (thick arrow)and the Angel Wings device sandwiched between the Amplatzerand the septum. RA: right atrium; SVC: superior vena cava; IVC:inferior vena cava; AO: aorta; LA: left atrium.
186 Zhu et al.

20%–30% [3–6]. However, not all patients with residualshunt require further intervention. Only residual shunt ofclinical significance usually needs further intervention(surgical/catheter).
We believe that the new Amplatzer device has a uniquedesign allowing easy implantation and, more importantly,provides the ability to reposition or even retrieve thedevice prior to its release from the delivery cable. It is thisunique character that encouraged us to use the Amplatzerin this patient with a large residual shunt and a veryunusually prolapsed corner of the previous device. Onemay wander about the resultant profile of both devicestogether and the potential for obstruction to blood flow inthe SVC and the RUPV. We believe that having thepatient on aspirin therapy until the new device becomescompletely endothelialized (about 6 months) is of impor-tance to prevent small clots from developing. Further-more, we noticed that with time the profile of the devicetends to get much smaller secondary to the memoryproperty of the Nitinol metal and, So far, there has beenno Doppler evidence of obstruction to blood flow in theSVC or the RUPV.
This case shows that 2D TEE can demonstrate usefulinformation about the site of residual shunt and the rimsaround the margin of the device where the residual shuntoriginated. However, we need mental conceptualizationof the defect and device to understand it better. Therefore,3D TEE provided an en face view of the atrial septalstructure. From this view we not only knew the patho-logic morphology of the device but also its relationshipwith the surrounding structure. This is indispensable for asuccessful deployment of the device. We also learned that
as the left side of the device prolapsed into the rightatrium, the balloon sizing can easily overestimate the sizeof the residual shunt, whereas 3D TEE can help to selectappropriate size of the device.
We conclude that the new Amplatzer septal occluderdevice can be of use to close residual shunts, especially inpatients who wish to avoid open heart surgery altogether.
ACKNOWLEDGMENTS
We thank Drs. Hitendra Patel and Jonathan Rhodes fortheir invaluable help during the case.
REFERENCES
1. Masura J, Gavora P, Formanek A, Hijazi ZM. Transcatheter closureof secundum atrial septal defects using the new self-centeringAmplatzer septal occluder: initial human experience. Cathet Cardio-vasc Diagn 1997;42:388–393.
2. Thanopoulos B, Laskari C, Tsaousis GS, Zarayelyan A, Vekiou A,Papadopoulos GS. Closure of atrial septal defects with Amplatzerocclusion device: preliminary results. J Am Coll Cardiol 1998;31:1110–1116.
3. Rome JJ, Keane JF, Perry SB, Spevak PJ, Lock JE. Double-umbrella closure of atrial defects: initial clinical application.Circulation 1990;82:751–758.
4. Rao PS, Sideris SE, Housdorf G, et al. International experience withsecundum atrial septal defect occlusion by the buttoned device. AmHeart J 1994;128:1022–1135.
5. Hausdorf G, Schneider M, Franzbach B, Kampmann C, Kargus K,Goeldner B. Transcatheter closure of secundum atrial septal defectswith atrial septal defect occlusion system (ASDOS): initial experi-ence in children. Heart 1996;75:83–88.
6. Das GS, Hijazi ZM, O’Laughlin MP, Mendelsohn AM, for theInvestigators. Initial results of the U.S. PFO/ASD Closure Trial. JAm Coll Cardiol 1996;27(suppl A):119A.
Catheter Closure of Residual Shunt 187



![Post Traumatic Ventricular Septal Defect Closure Using an … · ensure survival [3].In this procedure, an Ampletzer VSD Occluder has usually been employed [4], or occasionally, an](https://img.pdfslide.us/doc/110x75/602593159134b37e87220abe/post-traumatic-ventricular-septal-defect-closure-using-an-ensure-survival-3in.jpg)