Embed Size (px)
Citation preview

OPERATIVE NUANCES
TRANSCALLOSAL TRANSCHOROIDAL APPROACH TO
TUMORS OF THE THIRD VENTRICLE
Hahnah J. Kasowski, M.D.Department of Neurosurgery,Yale UniversitySchool of Medicine,New Haven, Connecticut
Brian V. Nahed, M.D.Department of Neurosurgery,Yale UniversitySchool of Medicine,New Haven, Connecticut
Joseph M. Piepmeier, M.D.Department of Neurosurgery,Yale UniversitySchool of Medicine,New Haven, Connecticut
Reprint requests:Joseph M. Piepmeier, M.D.,Department of Neurosurgery,Yale UniversitySchool of Medicine, TMP 4,333 Cedar Street,New Haven, CT 06510.Email: [email protected]
Received, January 16, 2004.
Accepted, May 19, 2005.
ALTHOUGH THE LITERATURE is rich with descriptions of the approach to the thirdventricle, surgeons remain cautiously reserved. In this report, we demonstrate that thetranscallosal approach can be easily performed provided that preoperative planning isadequate. Familiarity with the course of major cortical and deep draining veins grantsthe surgeon a wide exposure of the posterior third ventricle. We discuss the indica-tions, surgical technique, and pitfalls to this approach while providing an accompa-nying video mirroring our discussion.
KEY WORDS: Third ventricle tumor, Transcallosal, Transchoroidal
Neurosurgery 57[ONS Suppl 3]:ONS-361–ONS-366, 2005 DOI: 10.1227/01.NEU.0000176652.59747.40
We present the surgical treatment of atumor in the posterior third ventri-cle using a transcallosal approach.
Third ventricular tumors are relatively rare,and few neurosurgeons approach these tu-mors regularly, although much has been writ-ten on this topic (1–9). The transcallosal ap-proach provides excellent exposure to thirdventricular lesions, but careful preoperativeplanning and knowledge of the anatomy isnecessary to prevent complications. In partic-ular, care should be taken to understand andpredict the course of major cortical and deepdraining veins with preoperative imaging. Wediscuss the indications, surgical technique,and pitfalls to this approach.
PREOPERATIVE PLANNING
A clear understanding of venous anatomyis critical for the success of this operation.Adequate access to the corpus callosum andthird ventricle requires that the surgeon estab-lish an interhemispheric corridor that is 2 to 3cm in diameter. Because the location of majorcortical draining veins can limit this accessand dictate the side on which the craniotomyis based, a magnetic resonance venogram, inaddition to standard magnetic resonance im-aging (MRI) sequences, proves to be quite use-ful. Although we usually plan to approach theventricular system from the nondominanthemisphere, we may choose to enter on theopposite side if a wider corridor is available.
ILLUSTRATIVE CASE
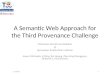
The patient was a 21-year-old woman who pre-sented with a history of progressive headaches overa period of 1 month. MRI demonstrated hydroceph-alus and a posterior third ventricular mass (Fig. 1).The patient initially underwent endoscopic thirdventriculostomy and tumor biopsy, which was di-agnostic of ependymoma. The third ventriculos-tomy was successful, and subsequent imaging dem-onstrated resolution of her hydrocephalus. Giventhe natural history of ependymoma, a complete ex-cision of the tumor was planned.
PATIENT POSITIONING
The patient was positioned supine, with theleft shoulder elevated by a shoulder roll. Thehead was then rotated such that the coronalsuture was oriented in the vertical plane andthe right hemisphere was inferior. We preferto have the right side down so that gravityaids in the retraction of the hemisphere. Thehead was fixed with a Mayfield frame, and alinear bicoronal incision was prepared anddraped.
CRANIOTOMY(see video at web site)
A bone flap that is centered two-thirds infront of and one-third behind the coronal su-ture is generally sufficient, but the bone flapmay need to be moved slightly more anteri-orly or posteriorly, depending on venousanatomy and location of the tumor (Fig. 2,
NEUROSURGERY VOLUME 57 | OPERATIVE NEUROSURGERY 4 | OCTOBER 2005 | ONS-361
inset). In this patient, because the tumor was located in theposterior third ventricle, our bone flap was made slightlymore anterior to provide better direct visualization of theposterior third ventricle. The bone flap should allow severalcentimeters of visualization of the right hemisphere and ex-tend just past the sagittal sinus on the left. To prevent damageto the sinus, we prefer to take the bone flap in two pieces: first,taking a bone flap over the right hemisphere that extends justto the right of midline; next, dissecting the sagittal sinus fromthe bone just medial to the previous bone flap. The bone overthe sagittal sinus is then removed.
It is critical that the dural opening provide exposure up tothe edge of the superior sagittal sinus. We begin opening thedura laterally and then carefully extend the opening towardthe midline where the dural flap is based. It is not uncommonto find that dominant frontal cortical veins enter the duralateral to the superior sagittal sinus. When this occurs, thedura can be incised on either side of the vein such that a duralroof is formed over the vein, sparing the vein. Dural tentingstitches are then placed such that the dura is carefully re-tracted across the midline to the sagittal sinus. Care must betaken not to place too much tension on the dural flap, becausethis can partially or completely occlude the sagittal sinus.
INTERHEMISPHERIC DISSECTION
Brain relaxation is critically important to minimizeretraction-induced injury and should occur before interhemi-spheric dissection. A combination of hyperventilation, osmoticdieresis, and ventricular drainage can be used. We routinely
give 0.5 g/kg of mannitol at skin incision and maintain theend-tidal CO2 in the range of 25 to 30 mm Hg. If the brain isnot adequately relaxed at this point, a ventricular drain can beplaced ipsilateral to the craniotomy. However, large tumorsmay necessitate placement of a contralateral ventriculostomy.
A self-retaining retractor system is brought onto the fieldand used to gently retract the right hemisphere. The operatingmicroscope is then brought in and used for the remainder ofthe operation. Both blunt and sharp dissecting instruments areused to develop the plane along the falx and then between thecingulate gyri. The pericallosal arteries must then be identi-fied. Once the surgeon is sure of their course, the corpuscallosum can be identified by its relative hypovascularity andpale white color.
FIGURE 1. Preoperative MRIimages (A, axial; B, sagittal; C,coronal).
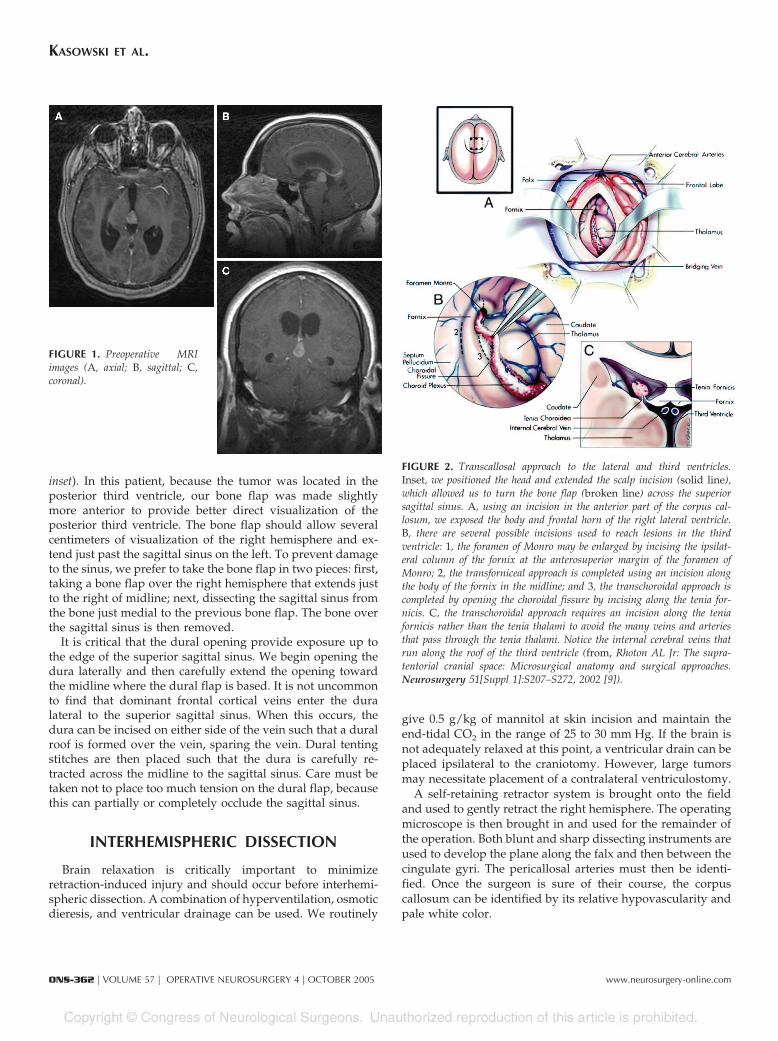
FIGURE 2. Transcallosal approach to the lateral and third ventricles.Inset, we positioned the head and extended the scalp incision (solid line),which allowed us to turn the bone flap (broken line) across the superiorsagittal sinus. A, using an incision in the anterior part of the corpus cal-losum, we exposed the body and frontal horn of the right lateral ventricle.B, there are several possible incisions used to reach lesions in the thirdventricle: 1, the foramen of Monro may be enlarged by incising the ipsilat-eral column of the fornix at the anterosuperior margin of the foramen ofMonro; 2, the transforniceal approach is completed using an incision alongthe body of the fornix in the midline; and 3, the transchoroidal approach iscompleted by opening the choroidal fissure by incising along the tenia for-nicis. C, the transchoroidal approach requires an incision along the teniafornicis rather than the tenia thalami to avoid the many veins and arteriesthat pass through the tenia thalami. Notice the internal cerebral veins thatrun along the roof of the third ventricle (from, Rhoton AL Jr: The supra-tentorial cranial space: Microsurgical anatomy and surgical approaches.Neurosurgery 51[Suppl 1]:S207–S272, 2002 [9]).
KASOWSKI ET AL.
ONS-362 | VOLUME 57 | OPERATIVE NEUROSURGERY 4 | OCTOBER 2005 www.neurosurgery-online.com

CALLOSOTOMY
The callosal incision is planned between the two anteriorcerebral arteries with the goal of entering the right lateralventricle. We suggest incising the callosum just beneath theright anterior cerebral artery, aiming slightly toward the righthemisphere. The surgeon should avoid dissecting toward theleft side because of the effect of the right-side-down headpositioning and the resultant shift of the right hemisphere.Both of these techniques will help to keep the callosum fromopening into the left ventricle or in line with the attachment ofthe septum pellucidum. Although this is not necessarily aproblem, it can cause unnecessary confusion.
The length and placement of the callosotomy is determinedby the location and size of the tumor. Our callosal incision inthis case measures approximately 2 cm in length and is madewith bipolar coagulation and suctioning with a 6-French suc-tion tip. The corpus callosum can be variable in thickness,depending on the underlying tumor mass and/or preexistinghydrocephalus, and can be stretched to just a few millimeters.In this patient, the corpus callosum was relatively thick, mea-suring approximately 1 cm. The exact placement of the callo-sotomy may vary, depending on the surgical window af-forded by the cortical draining veins. The preoperative MRIscan may be helpful in localizing the preferred distance of thecallosotomy from the genu of the corpus callosum. Theependymal lining is recognized by its deep gray coloring justbefore the ventricle is entered. Once the ventricle is opened, aself-retaining retractor blade can be advanced just into theventricle.
TRANSCHOROIDAL DISSECTION
Once the ventricle is opened, it is important to first establishnormal landmarks. The structure that is most obvious and easiestto identify is the choroid plexus, which can be followed anteri-orly to the foramen of Monro. Further identification of the septaland thalamostriate veins can be used to determine which ventri-cle has been opened (Fig. 2A). In the right lateral ventricle, thethalamostriate vein is to the right of the choroid plexus. If callosalsectioning has led to the contralateral ventricle, the septum pel-lucidum can be opened to gain access to the contralateral side.Should this occur, however, the surgeon must take care to pre-serve the fornices at the base of the septum.
Below the fornix, the roof of the third ventricle is composed oftwo layers of the tela choroidea and the velum interpositum, avascular space that is located between these layers. The internalcerebral veins and the medial posterior choroidal arteries runwithin the velum interpositum. Our approach was through thetela choroidea and velum interpositum into the third ventricle.
Dissection through the tela choroidea should be performedmedial to the choroidal fissure in the tenia fornicis rather than inthe tenia thalami, because the veins that drain the internal cap-sule and medial hemisphere pass through the tenia thalami andshould not be sectioned (Fig. 2, B and C). We prefer to begin thedissection by gently lifting the choroid plexus, coagulating it, and
then removing it along its insertion at the choroid fissure, allow-ing for visualization of the choroidal fissure. We begin our dis-section along the medial edge of the choroidal fissure whilegently elevating the adjacent fornix to avoid inadvertent damage.Once the tenia fornix is divided, the velum interpositum is en-tered and the internal cerebral veins and the medial posteriorchoroidal arteries are visualized. These vessels should be re-tracted laterally until the lower layer of tela is visualized, whichmay then also be divided (Fig. 3).
The choroid plexus of the third ventricle, the massa inter-media, and the floor of the third ventricle are now seen. Asmall portion of the tumor can also be seen below the massaintermedia. At this point, we encountered two anatomic struc-tures that limited our view and approach to the tumor. Thefirst was a large massa intermedia. This patient was knownfrom the preoperative imaging to have a large massa interme-dia, and as expected, the massa intermedia significantly ob-structed our view of the posterior third ventricle and tumor.As mentioned, this patient had had a previous endoscopicthird ventriculostomy, which alleviated her hydrocephalus.We suspect that if the patient had still had significant hydro-cephalus, the massa intermedia would have been significantlystretched and easier to work around. However, in this case, wewere forced to divide it so as to better visualize and resect thetumor, a maneuver that we have not previously had to per-form. Postoperatively, the patient experienced no appreciableneurological deficit from this maneuver.
After the massa intermedia was sectioned, our entry into thethird ventricle was also limited by two thalamostriate veins.We initially attempted to dissect the anterior vein from thelateral wall of the ventricle. However, when this proved dif-ficult, we thought that it was preferable to sacrifice the veinrather than risk its rupture. Rarely do we sacrifice drainingveins; however, when there is duplication of the venous drain-age, as in this patient, we have not had complications when asingle vein is sacrificed.
LESION EXCISION
Tumor resection is facilitated by maintaining the dissectionplane between the ependyma and the lesion. Because it is notuncommon for intraventricular tumors to grow slowly and be-come quite large, we often must first decompress the tumor andthen identify the space between the tumor edge and ependyma.
Determining the type of tumor is important in predictingthe blood supply. Papillomas and meningiomas, for example,receive their blood supply from the choroidal vessels. Withthese tumors, early identification and transection of thesevessels will significantly reduce bleeding. In contrast, tumorsthat arise from the ependymal surface and septum pelluci-dum, such as gliomas and neurocytomas, receive their bloodsupply from the small vessels of the ventricular walls. In thispatient, the blood supply was encountered after primary de-bulking. These vessels tend to be smaller and cause less bloodloss but still require meticulous dissection and goodvisualization.
TRANSCALLOSAL TRANSCHOROIDAL APPROACH TO THIRD VENTRICLE
NEUROSURGERY VOLUME 57 | OPERATIVE NEUROSURGERY 4 | OCTOBER 2005 | ONS-363
The tumor was small, and initial tumor removal was easilyaccomplished with suctioning. As the tumor was aspirated,the cerebral aqueduct was visualized. The previous third ven-triculostomy was also appreciated more anteriorly. As we
approached the posteriorpart of the tumor beneath theposterior commissure, manysmall tumor vessels were en-countered. Visualization ofthe most posterior portion ofthe tumor was limited by theoverlying posterior commis-sure. The resection continueduntil we felt that the risk offurther resection outweighedthe risk of some small resid-ual tumor. Although westrive for a complete tumorexcision, extending the resec-tion into the underlying mid-brain can be devastating andshould not be attempted ifthe tumor plane is unclear.
After tumor resection, it isimportant to ensure completehemostasis. To prevent ven-tricular obstruction and hy-drocephalus, blood that mayhave accumulated should begently irrigated out of theventricular system. The ven-tricles are then filled with sa-line to displace any air thatmay have become trapped. Aventricular catheter is left for24 to 48 hours to measureventricular pressure and todemonstrate that the ventric-ular system is patent. A com-puted tomographic or MRIscan is obtained on the firstpostoperative day to checkfor obstruction and to evalu-ate the resection. Postopera-tively, the patient was neuro-logically intact and did notexperience any complicationsrelated to the procedure.
LIMITATIONS OFTHIS APPROACH
This case demonstrates thatthe transcallosal approach iseasily performed, providedthat the surgeon is familiar
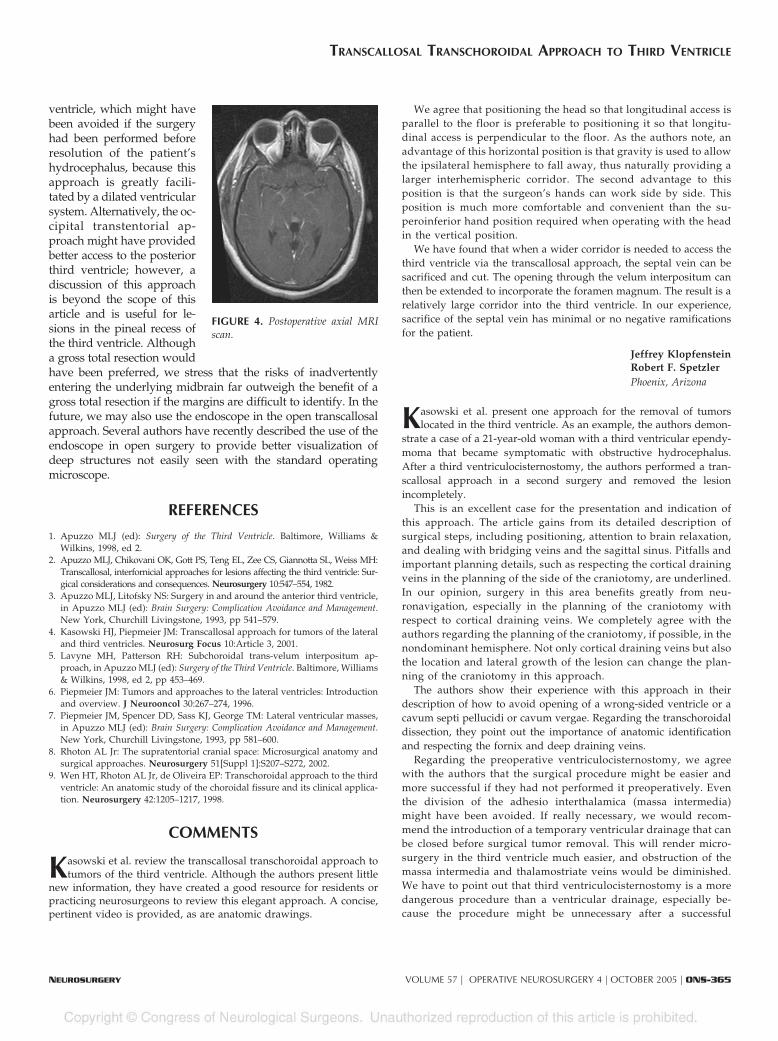
with the anatomy and achieves wide exposure of the posteriorthird ventricle. However, postoperative imaging revealed smallresidual tumor in the posterior third ventricle (Fig. 4). In thispatient, our exposure was limited in the pineal recess of the third
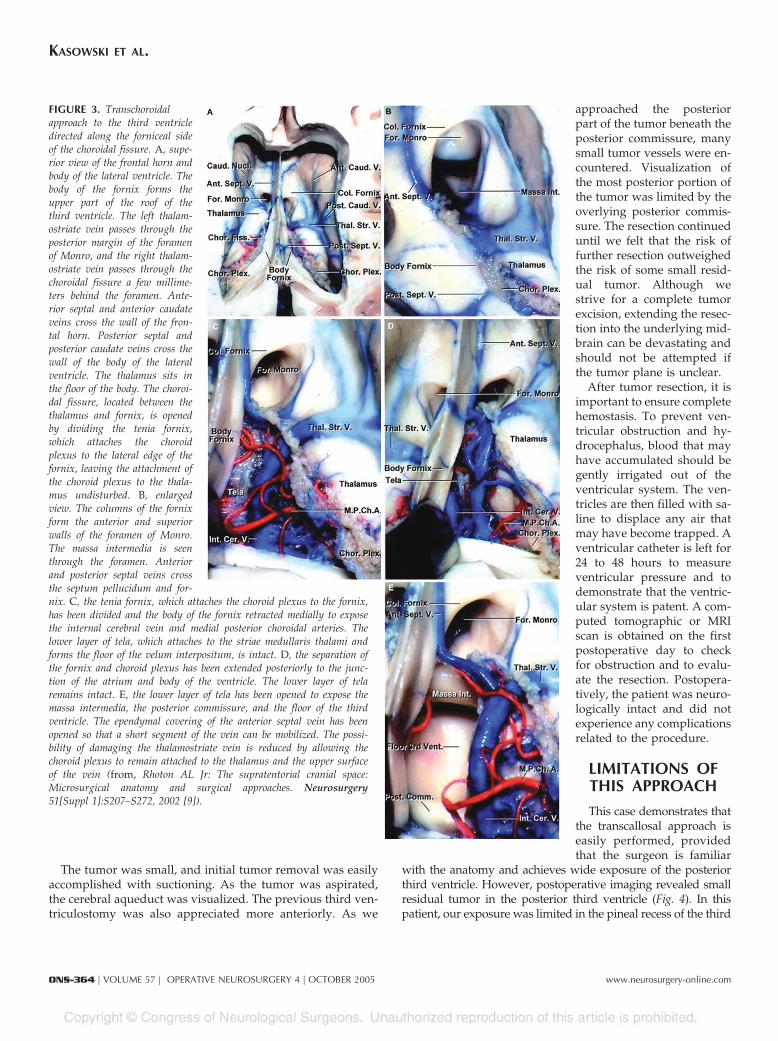
FIGURE 3. Transchoroidalapproach to the third ventricledirected along the forniceal sideof the choroidal fissure. A, supe-rior view of the frontal horn andbody of the lateral ventricle. Thebody of the fornix forms theupper part of the roof of thethird ventricle. The left thalam-ostriate vein passes through theposterior margin of the foramenof Monro, and the right thalam-ostriate vein passes through thechoroidal fissure a few millime-ters behind the foramen. Ante-rior septal and anterior caudateveins cross the wall of the fron-tal horn. Posterior septal andposterior caudate veins cross thewall of the body of the lateralventricle. The thalamus sits inthe floor of the body. The choroi-dal fissure, located between thethalamus and fornix, is openedby dividing the tenia fornix,which attaches the choroidplexus to the lateral edge of thefornix, leaving the attachment ofthe choroid plexus to the thala-mus undisturbed. B, enlargedview. The columns of the fornixform the anterior and superiorwalls of the foramen of Monro.The massa intermedia is seenthrough the foramen. Anteriorand posterior septal veins crossthe septum pellucidum and for-nix. C, the tenia fornix, which attaches the choroid plexus to the fornix,has been divided and the body of the fornix retracted medially to exposethe internal cerebral vein and medial posterior choroidal arteries. Thelower layer of tela, which attaches to the striae medullaris thalami andforms the floor of the velum interpositum, is intact. D, the separation ofthe fornix and choroid plexus has been extended posteriorly to the junc-tion of the atrium and body of the ventricle. The lower layer of telaremains intact. E, the lower layer of tela has been opened to expose themassa intermedia, the posterior commissure, and the floor of the thirdventricle. The ependymal covering of the anterior septal vein has beenopened so that a short segment of the vein can be mobilized. The possi-bility of damaging the thalamostriate vein is reduced by allowing thechoroid plexus to remain attached to the thalamus and the upper surfaceof the vein (from, Rhoton AL Jr: The supratentorial cranial space:Microsurgical anatomy and surgical approaches. Neurosurgery51[Suppl 1]:S207–S272, 2002 [9]).
KASOWSKI ET AL.
ONS-364 | VOLUME 57 | OPERATIVE NEUROSURGERY 4 | OCTOBER 2005 www.neurosurgery-online.com
ventricle, which might havebeen avoided if the surgeryhad been performed beforeresolution of the patient’shydrocephalus, because thisapproach is greatly facili-tated by a dilated ventricularsystem. Alternatively, the oc-cipital transtentorial ap-proach might have providedbetter access to the posteriorthird ventricle; however, adiscussion of this approachis beyond the scope of thisarticle and is useful for le-sions in the pineal recess ofthe third ventricle. Althougha gross total resection wouldhave been preferred, we stress that the risks of inadvertentlyentering the underlying midbrain far outweigh the benefit of agross total resection if the margins are difficult to identify. In thefuture, we may also use the endoscope in the open transcallosalapproach. Several authors have recently described the use of theendoscope in open surgery to provide better visualization ofdeep structures not easily seen with the standard operatingmicroscope.
REFERENCES
1. Apuzzo MLJ (ed): Surgery of the Third Ventricle. Baltimore, Williams &Wilkins, 1998, ed 2.
2. Apuzzo MLJ, Chikovani OK, Gott PS, Teng EL, Zee CS, Giannotta SL, Weiss MH:Transcallosal, interfornicial approaches for lesions affecting the third ventricle: Sur-gical considerations and consequences. Neurosurgery 10:547–554, 1982.
3. Apuzzo MLJ, Litofsky NS: Surgery in and around the anterior third ventricle,in Apuzzo MLJ (ed): Brain Surgery: Complication Avoidance and Management.New York, Churchill Livingstone, 1993, pp 541–579.
4. Kasowski HJ, Piepmeier JM: Transcallosal approach for tumors of the lateraland third ventricles. Neurosurg Focus 10:Article 3, 2001.
5. Lavyne MH, Patterson RH: Subchoroidal trans-velum interpositum ap-proach, in Apuzzo MLJ (ed): Surgery of the Third Ventricle. Baltimore, Williams& Wilkins, 1998, ed 2, pp 453–469.
6. Piepmeier JM: Tumors and approaches to the lateral ventricles: Introductionand overview. J Neurooncol 30:267–274, 1996.
7. Piepmeier JM, Spencer DD, Sass KJ, George TM: Lateral ventricular masses,in Apuzzo MLJ (ed): Brain Surgery: Complication Avoidance and Management.New York, Churchill Livingstone, 1993, pp 581–600.
8. Rhoton AL Jr: The supratentorial cranial space: Microsurgical anatomy andsurgical approaches. Neurosurgery 51[Suppl 1]:S207–S272, 2002.
9. Wen HT, Rhoton AL Jr, de Oliveira EP: Transchoroidal approach to the thirdventricle: An anatomic study of the choroidal fissure and its clinical applica-tion. Neurosurgery 42:1205–1217, 1998.
COMMENTS
Kasowski et al. review the transcallosal transchoroidal approach totumors of the third ventricle. Although the authors present little
new information, they have created a good resource for residents orpracticing neurosurgeons to review this elegant approach. A concise,pertinent video is provided, as are anatomic drawings.
We agree that positioning the head so that longitudinal access isparallel to the floor is preferable to positioning it so that longitu-dinal access is perpendicular to the floor. As the authors note, anadvantage of this horizontal position is that gravity is used to allowthe ipsilateral hemisphere to fall away, thus naturally providing alarger interhemispheric corridor. The second advantage to thisposition is that the surgeon’s hands can work side by side. Thisposition is much more comfortable and convenient than the su-peroinferior hand position required when operating with the headin the vertical position.
We have found that when a wider corridor is needed to access thethird ventricle via the transcallosal approach, the septal vein can besacrificed and cut. The opening through the velum interpositum canthen be extended to incorporate the foramen magnum. The result is arelatively large corridor into the third ventricle. In our experience,sacrifice of the septal vein has minimal or no negative ramificationsfor the patient.
Jeffrey KlopfensteinRobert F. SpetzlerPhoenix, Arizona
Kasowski et al. present one approach for the removal of tumorslocated in the third ventricle. As an example, the authors demon-
strate a case of a 21-year-old woman with a third ventricular ependy-moma that became symptomatic with obstructive hydrocephalus.After a third ventriculocisternostomy, the authors performed a tran-scallosal approach in a second surgery and removed the lesionincompletely.
This is an excellent case for the presentation and indication ofthis approach. The article gains from its detailed description ofsurgical steps, including positioning, attention to brain relaxation,and dealing with bridging veins and the sagittal sinus. Pitfalls andimportant planning details, such as respecting the cortical drainingveins in the planning of the side of the craniotomy, are underlined.In our opinion, surgery in this area benefits greatly from neu-ronavigation, especially in the planning of the craniotomy withrespect to cortical draining veins. We completely agree with theauthors regarding the planning of the craniotomy, if possible, in thenondominant hemisphere. Not only cortical draining veins but alsothe location and lateral growth of the lesion can change the plan-ning of the craniotomy in this approach.
The authors show their experience with this approach in theirdescription of how to avoid opening of a wrong-sided ventricle or acavum septi pellucidi or cavum vergae. Regarding the transchoroidaldissection, they point out the importance of anatomic identificationand respecting the fornix and deep draining veins.
Regarding the preoperative ventriculocisternostomy, we agreewith the authors that the surgical procedure might be easier andmore successful if they had not performed it preoperatively. Eventhe division of the adhesio interthalamica (massa intermedia)might have been avoided. If really necessary, we would recom-mend the introduction of a temporary ventricular drainage that canbe closed before surgical tumor removal. This will render micro-surgery in the third ventricle much easier, and obstruction of themassa intermedia and thalamostriate veins would be diminished.We have to point out that third ventriculocisternostomy is a moredangerous procedure than a ventricular drainage, especially be-cause the procedure might be unnecessary after a successful
FIGURE 4. Postoperative axial MRIscan.
TRANSCALLOSAL TRANSCHOROIDAL APPROACH TO THIRD VENTRICLE
NEUROSURGERY VOLUME 57 | OPERATIVE NEUROSURGERY 4 | OCTOBER 2005 | ONS-365
surgery. This article offers a lot of insight into the application andindications of this anatomically interesting approach.
Wolf LudemannMadjid SamiiHannover, Germany
This is a very nice description of the transchoroidal approach to thethird ventricle, with excellent illustrations. The advantage of this
technique is to spare the veins.The authors are very cautious in performing six burr holes for the
craniotomy in two flaps. One or two burr holes on the midline overthe sagittal sinus might be enough in young patients.
The transchoroidal approach is particularly suitable for tumors inthe midportion of the third ventricle. The tumor in the present patientis in the posterior third ventricle, and I would have preferred anoccipital transtentorial approach.
Nicholas de TriboletGeneva, Switzerland
The authors present their treatment of tumors involving the posteriorthird ventricle using a transcallosal approach. They emphasize that
the transcallosal approach provides excellent exposure when coupledwith diligent and careful preoperative planning. Knowledge of the sa-lient venous anatomy, variants of the choroidal fissure anatomy, andthree-dimensional relationships of the fissure to the pineal region andquadrigeminal plate cistern is requisite to prevent complications. Preop-erative understanding of midline draining veins is essential in tailoringthe approach to minimize venous sacrifice and compromise. The use of
gravity to aid in the retraction of the hemisphere is also an importantfactor. We use the three-quarter lateral position to maximize this. Inaddition, we prefer soft retraction with rolled patties placed at the ante-rior and posterior limits of the interhemispheric corridor.
Although the authors suggest an interhemispheric corridor that is 2to 3 cm in diameter, we have had good results with smaller ap-proaches, given that the anteroposterior dimension of the corridor ismore important than the lateral dimension (which only promotes thepotential for excessive retraction). We also prefer to take the flap as asingle piece and actually use the drill to place burr holes over themidline. We have not had a problem with sinus injury using thisapproach in children, given that the ability to separate the dura fromthe overlying bone is easier in younger children. In addition to duraltenting stitches, as noted, we also place dural sutures in the falx foradditional retraction. The use of ventricular drainage to allow forrelaxation of the brain cannot be overemphasized. A 2-cm callosalincision will usually allow for any approach in this region. In addition,as the authors note, the surgeon must take care to preserve thefornices at the base of the septum. It is also important that dissectionthrough the tela choroidea is performed medial to the choroidalfissure in the tenia fornicis rather than in the tenia thalami.
Finally, although complete excision is an appropriate goal, extend-ing the resection into the underlying midbrain can be devastating andshould not be attempted if the tumor plane is unclear. The only otherconsideration is the use of concurrent endoscopy, as initially describedby Perneczky, which is now common in a number of institutions.
Michael L. LevySan Diego, California
KASOWSKI ET AL.
ONS-366 | VOLUME 57 | OPERATIVE NEUROSURGERY 4 | OCTOBER 2005 www.neurosurgery-online.com


















![Introduction to MATLAB and SIMULINK a Project Approach Third Edition Engineering ]](https://img.pdfslide.us/doc/110x75/55cf9484550346f57ba287db/introduction-to-matlab-and-simulink-a-project-approach-third-edition-engineering.jpg)