Embed Size (px)
Citation preview

1 'RANSACTIONS OF THE OPHTHALMOLOGICAL SECTION
(Authors' abstracts). Edited by K . G. Pioman, Secretary.
OF T H E SWEDISH MEDlCAL ASSOCIATION 1929-1931')
14th Meeting, March lst, 1929. K. 0. Granstrom: A Case o f Kerafit is Pustuliformis Profunda.
Acta Ophthalm. Vol. VII, p. 330, 1929.
Gustaf Dohlman: Demonstration of an Apparafus f o r Optic Regi: stration o f the Vestibular Movements o f the Eye. (Demonstration eines Apparates zur optischen Registrierung der vestibularen Augens bewegungen. Vers. 0. G. Heidelberg, p. 459, 1928.)
Ernst Svensson: Review o f H. N o g u c h i ' s ,,The Etiology o f Tra: choma", J. of Exp. Mcd. Vol. XLVIII, 1928.
K. G. Ploman: Review o f A . S i e g r i s t's ,,Der graue Altersstar", Urban a. Schwarzenberg, 1928.
15th Meeting, June lst, 1929. The secretary announced that the desires of the section regarding
the qualifications requircd for heads of hospital ophthalmolgy der partmcnts havc in a petition to His Majesty of April 25, 1929, been formulated thus:
The time of training required for qualification as the head of an ophthalmology department to be placed at a minimum of 3 years, at least 2 of them at an eye clinic. h'o decisions to he made as to the type of training during the third year. Of the 2 years a t an eye clinic, at least 1 to be devoted to work in wards for the treatment of eye diseases.
16th Meeting, November 30th, 1929. Henrik Sjogren: A Case o f Sympathetic Choroidoretinitis (with
A boy agcd 8, with a perforating injury to the right eye incurred demonstration of the patient).
_-__-__ *) received Dec. 5th 1931.

404
May 6, 1929, Admitted t o the eye clinic of the Serafimer Hospital the same day. The eye was considerably irritated. From the vertex of the cornea up to a fcw millimeters above the margin there was a sharply cut lesion through which the iris had partially prolapsed. T h e lens was very cloudy.
Slow improvement until May 14, when the eye became more irris tated, the aqueous humour being considerably clouded, with hemor5 rhagic iritis, and the configuration of the iris blurred.
O n June 3, there were a few deposits on Deseemet’s membrane in the right eye. Left eye entirely normal. June 4, enucleation of the right eye. June 8, left eye not irritated. Fine light beam, no dcposits, no cloudiness of the vitreous body, normal papilla. T. 7/55. June 13, a few small deposits on Descemet’s membrane. July 12, fully developed sympathetic ophthalmia. V. 0.1. August 3, V. 4/50.
After this there was gradually progressing improvement with the vitreous humour clearing so that the fundus was visible on Aug. 28. Far out in the periphery a fairly large number of small orange spots could be seen, most of them round but a good many rather irregular in shape. There were no rings of pigment, but in the centres of several of these spots there were small accumulations of pigment. Thc size of these foci is estimated a t about the breadth of one or two retinal vessels.
The improvement continued gradually and the acuity of vision rose to 0.7. The choroideal foci remained unchanged the whole time and no enlargement or increased pigmentation could be found in them. No changes in the macula or otherwise in the posterior part of the eye.
V. G r a e f e appears to be the first to havc observed such foci in sympathetic ophthalmia. No more detailed clinical observation of them is to be found, however, until H i r s c h b e r g , and after him H a a b. The first to study them histologically was D a 1 C n, who found that these foci arc made up of a collection of lymphocytes and epitheloid cells within the lamina vitrea of the chorioid, with defects in thc overlying pigment epithelium. These foci of D a l C n have been pointed out by a number of authors as being the only patho. gnomic symptom of sympathetic ophthalmia. According to M e 11 e r, however, they are also present in septic endophthalmitis, and ac: cording to v. H i p p e 1 in tuberculous alteration of the chorioid.
C . G. Bostrom: Some Remarks on the Visual Requirements for Railway men.
On the authority of a >>Rapport sur I’Unification des Prescriptions Visuellesa made at the 13th Ophthalmological Congress a t Amsterdam and The Hague in 1929, the lecturer gives a summary of the requires ments of most countrics for different personnel groups; the Swedish requirements are dealt with in greater detail. T h e lecturer then emphasises the exceeding importance of making the first exas

4.05
mination with the greatest care. After reporting on the periodic cxamination of employees required in most countries, the lecturer sevcrely criticised the soscalled practical tests. Periodic examination is not yct made in Sweden; in the case of older employees, the railway directing board usually relaxes the visual requirements somewhat in individual cascs. The lccturer recommended the introduction of fres qucnt tests, saying that nthe absence of all control throughout the period of employment is equivalent to giving the certificate of visual normalcy a t thc time of engagement an unlimited validitya.
After a brief staterncnt of the development and present status of the problem of colour perception in Sweden, the lecturer pointed out the desirability of also resexamining the colour perception some time aftcr cngagement.
(This lecture has been published in Swedish in the N o r d i s k J a r n b a n e t i d s k r i f t, 1931.)
17th Meeting, February 22nd, 1930. Yngvar Lindblad: A Case of Schminke's Sarcoma. The patient was a man aged 36. Extreme exophthalmos, persisting
for the past two months, had induced the patient to seek an eye specialist, who found that the nasopharynx was filled with a tumorous mass which had already perforated the hard palate. Xsray treatment had no effect. The patient died after six weeks of general metas stasis. Photographs of the patient and of microscopic slides were demonstrated.
Sven Larsson: A Contribution to the Knowledge of Changes in the Fundus Oculi in Leucremia. (Zur Kenntnis der Augenhintergrundvers andcrungen bei Leukamic, Acta Ophthalm. Vol. 8, p. 22, 1930).
Henrik Sjogren: Keratoconjunctivitis Sicca. The paticnt was a woman aged SO. As a child she had had rheus
matic fever. There were no further joint symptoms after that until 1926, whcn quite suddenly there were again symptoms in several joints, especially those of the hands and feet. A t the same time a number of secretory anomalies appeared, such as pronounced dryness of the mouth and complete absence of perspiration. A t this time too the patient's eyes began to give her trouble. They began to smart, and there was a constant fccling of friction, great sensitiveness t o light and a feeling of dryness in them. The patient entirely lost the power of weeping, nor could the tears be elicited as a reflex by means of strong odours. The patient felt ,>dry all through".
Condition on examination: Neither eye was irritated. The cons junctivae wcre densely scattered with quantities of small, irregularly shaped crosions covering practically the entire surface. In addition

406
t o these, there were a number of old maculae. Staining with rose bengale also stained the conjunctivae bulbi within the region of thc rima. The sensibility was distinctly reduced in the cornea and the conjunctivae. No other disturbances of sensibility. From the cons junctivac there was a slight stringy secretion. The fundus and media were otherwise normal. V. O.S., 0.6(+ 2); 0. D., 0.4(+ 2). ’The ins traocular tension was much reduced, and ranged from 9/53 to 1215.5. T h e tear secretion proved with S c h i r m e r ’ s t e s t t o b e m u c h r e d u c e d .
O n extirpation of the lacrimal gland, pronounced dryness of the eycs will sometimes be observed. There will be a tough, stringy secretion and erosions of the cornea, with the looscned epithelium occasionally adhering like tiny threads. Similar changes have been found in children with congenital aplasia of thc secretory nerve pass sagcs and a consequent lack of tcars, or in acquired dryness through a n injury to the trigcminal or facial nerve. Another group is made up of cases described by F u c h s, S c h o n i n g e r, S c h e e r e r, B e t s c h, I s h i k o w i t z and others under the name of kcratitis filamentosa. In some of these cases there is occasionally reduction of the corneal sensibility. Since it has been thought that the main cause of the corncal affection was to be sought in the lack of lacrimal secretion, D u k eiE 1 d e r suggested the name of kcratitis sicca. The discase is practically limited to women a t the change of life and often appears in conjunction with endocrine arthritis, for which reason the ultimate cause is assumed t o be a disturbance of the ovarian function.
In our patient the symptoms most rescmblc those of kcratitis sicca. There are, however, two additional symptoms here. The one is that of erosions of the conjunctivae, which are doubtless present in other cases too, but arc not visible in them owing to the fact that staining is usually done with fluorescin, which conceals thesc erosions; thc other is that of hypotonicity. The latter can probably be explained in this case by a diminution of the xsecrctionu of the aqueous.
Lumbar puncture was made on the patient. After this she had for several days severe headaches which persisted for over a week as soon as the patient stood up, but disappeared again when she lay down. The pain also disappeared when the head was bent forward, since the lumbar pressure rises then. Since no leakage could be diss covered, it is probable tha t the production of new spinal fluid was delayed by the chorioid plexus. Ah analogous condition of the aques ous and the ciliary body seems likely.
K. 0. Granstrom: A n Unusual Case of Catarrh of the Conjunctiva (Published in collaboration with S v e n L a r S S O ~ under the title of uUn cas Ctrange de keratosconjonctivite - avec >Syndrome de Paris naudc - transmissible aux lapinsq Acta Ophthalm. Vol. 9, p. 94, 1931).

407
K. G. Ploman: The Pressure Curve in the Miotic Treatment of Glaucoma.
After giving a survey of the work of K o e l l n e r , H a g e n and L ii h 1 e i n, the author demonstrated a few caws in which the pressure had been measured five times a day, a t 8, 11, 2, 5 and 8.
C a s e 1. H. H., aged 69, a physician. Irritative glaucoma of the left eyc. Thc fundi were normal; there was a small, curved D j r r r u m scotoma, but otherwise the field of vision was normal. V. 1, T. 2 / 7 5 Right eye normal.
F i g . 1,
Fig. 1 shows that the pressurc is not regulatcd by pilocarpine. Without miotics the prcssure reached its highcst valuc, 38 mm. (on Nov. 28) a t 5 p.m., and already rcturned to normal, 20 mm., a t 8 p.m. Pilocarpine given at 7.30 and 10 a .m. reduces the value to about 25 mm., but even aftcr this, there is a maximum value of 28 mm. a t 5 p.m. Pilocarpinescserine given a t these same hours of the morning was also unable to prevent an increase a t 5 p.m.; this was not done until the second administration of the eyesdrops was moved forward to 1 p. m. (Dec. 12). Pilocarpine alone given a t this time was not found to be cqually effcctive (Dec. 17). Since no increase of pressure was found in the mornings, pilocarpine alone was givcn in the evenings.
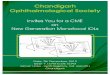
C a s e 2. K. E. H., aged 75, apothccary. Thc patient had been getting trcatment with pilocarpine for simple glaucoma since 1926. The pressure, which had at first been regulated by 1 pcr cent pilos carpine twice daily, rose in 1929, as can be secn from fig. 2, to a pathological value in spite of the administration of 2 per cent pilo5 carpinc three times daily.
The serial measurements (Fig. 2) without miotics showcd on Feb. 13, 1930 a distinct increase in pressurc which was regulated chiefly by the administration of pilocarpineseserine. However, the slightly too high

408
H Mn;
EE E E E E EE E E 1919.4.9 1930722 ?3.2 742 15.2 r9.2
F i g . 2.
morning pressure on Feb. 19 suggests that this therapy is inadequate- and must sooner or later give way to operative measures.
C a s e 3. G. A., aged 74, labourer. Absolute glaucoma of the right eye, incipient glaucoma of the left.
Condition on examination, Feb. 24, 1930. With the right eye, the patient sees motions of the hand temporally, T. is 1110. Left eye,. papilla and field of vision normal. V. 0.9, T. 3/10.
Hours Mm. Hg
90 80 70 60 50 40 30 20 10 0
fight Nqht Mghf Mght Night Mght &8 I1 ?4 17 20b8 77 I4 77 2d8 77 I4 77 2018 I? 74 I7 20'8 ? I 14 17 201
I I I I I I I I I I I I I I 1 1 1 1 1 1 1 1 1 ~ 1 1 I I I I I I I I I I I I 1 111 I I I I I I I I I I I I I I I I I I I I I I I 1 Mthoutmiotics P P P P P P FJ PP P
E E E E E E
Fig . 3.
Fig. 3 shows that the pressure, which is very high without miotics, can not be brought to normal by pilocarpineseserine even in the better eye, thus comprising a clear indication for operation.
These observations confirm the experience gaincd in other yuzrters, for instance that the conditions of pressure are essentially the same in both eyes even when there are pathological symptoms in only one of them, that the curve need not always be highest in the morning, etc. The repeated measurements give valuable information as to t h e

most suitable timc for administcring the miotics, and the kind of miotic to be used. Thcre is no doubt that they may aid in making an carly diagnosis possiblc in ambiguous cases and by disclosing transient increases in pressure explain dcterioration when the pressure has bcen normal a t occasional earlier measurements. The scrial measurements should be rcpeated at suitable intervals to makc surc that the prescribed miotics have not lost their efficiency. Such cxs tremely scrupulous observation makcs more effective treatment possible and undoubtedly in many cases allows of the safe postpones ment of operation, which is certainly not without valuc in vicw of thc fact that we havc no ideal operative trcatmcnt for this affcction.
18th Meeting, November 29th, 1930. Sven Larsson: A Successfully Operated Case of a Suprasellar Tumour.
H. Ahlbom: Demonstration o f a N e w Method o f Locating Foreign Bodies in the Eye. Distant X:ray exposures with the cornea made visible. (Ein ncucs Vcrfahren zur Lokalisation von Fremdkiirpern im Augc. Fcrnriintgenaufnahmen mit Sichtbarmachung der Hornhaut. A4cta Ophthalm. Vol. 9, p. 1, 1930.)
Yngvar Lindblad: A Case of Acute Blindness in Fat Embolism. The paticnt was a corpulent man, aged 39, who had been jammed
in an automobile collision. H c sustaincd a pelvic fracture and ex: hibitcd general symptoms of fat embolism. Ten hours after the acs cident, thc patient awoke from a few hours’ sleep to complete amaus rosis which pcrsisted until his death six days later. His pupils werc rigid but thcrc werc no unmistakable ophthalmoscopic findings, merely a suspicion of contracted arteries. A t the autopsy, there were found to be, in addition to a few fat cmboli in the peripheral organs, cx: tensivc areas of malacia close to the calcarine fissure in both hcmisphcrcs of the brain, though grossly not embracing all thc centres of vision. No fat cmboli werc found in the eyes (note: later, numbers of them werc found in the retina by another method). Photographs of the brain and microscopic slides were demonstrated.
A. DaIen: A Slight Modification of Diascleral Transillumination. A s we know, the diagnosis of an iniraocular tumour is sometimes
attended with certain difficulties, especially if the media are cloudy or the tumour is concealed by an extensive detachment of the retina. Undcr such conditions, diascleral transillumination is the most ims portnnt means of discovering it. This is as we know usually done in such a way that the transilluminating lamp is placed at differcnt points of thc wall of the eyeball and the examiner sees whether the pupil shines red or not. However, if thc tumour is situated at the posterior

pole of the eye, the lamp can not easily be placed on that part of the sclera which corresponds to the position of the tumour. In such cases 1 have hitherto introduced the small transilluminating lamp I described in Klin. Monatsbl. 1925 by an incision in the conjunctiva and inserted the lamp so far that the opening for the passage of light was opposite the suspccted point on the wall of the eyeball. I t is in this way often possiblc to diagnose a tumour situated a t the posterior pole of the cyc.
Lately, however, 1 have bcen using a method which gives a more reliable result. If a strong transillumination lamp is placed on the cornea opposite the pupil and the examiner iiispccts the wall of the eyeball, a tumour situated within the wall will be seen as a dark shadow on it. In this way a good imprcssion is gaincd of the position and extent of thc tumour. In order to inspect the posterior wall of the eyeball, I make a temporary incision through the tendon of the external rectus muscle, seize thc part of the tendon stump that is attached to the cyeball with a thumb forceps, and rotate the eyeball inwards; I then draw it nasally with a fcnestrated angular rctractor and a t the same time draw the rcst of the orbital contents temporally with anothcr hook. In this way, that part of the eyeball which is situated temporally to the optic nerve is acccssible to inspection, and I have found that even comparatively small tumours are quitc distinct under these circumstances. If the tumour is situated nasally to the optic nerve, it will probably be iieccssary to make a temporary ins cision through some onc of the other straight eye muscles in order to rotate the eycball so that the part of the wall desired is accessible. Howcvcr, I have not yct had occasion to test this method on any tumours situated thus.
Sven Larsson: Studies on Consensual Variations of the lntraocular Pressure. ( J s t bei traumatischer Schadigung eines Auges am anderen Auge kliniseh eine Keaktion des intraokularcn Druckes zu heobachs ten?<< Acta Ophthalm. Vol. 8, p. 261, 1930.)
19th Meeting, February 28th, 1931. Yngvar Lindblad: A Case of Uveo-Parotic Fever. The patient was a man of 46, treated for two months on an in.
dctinite diagnosis of fevcr and headaches, in the course of which he had bcen admitted to hospitals twice and thcre bcen subjected t o lumbar puncture (T. 190 cm., 90 cells). No signs of syphilis, Was$ scrmann negative in blood and spinal fluid. For some days, the pas tient had had pains under the chin and up toward thc cars, and lately he has been sensitive to light and had some asthenopic trouble.
Both eyes were pale and containcd quantities of fine deposits on Desccmet's membrane, '1 distinct lightkm-im and numbers ot fine

41 1
opacities in the vitreous. V. 0,9-1. After treatment with bismuth and potassium iodide, atropin and bathing the eyes, the patient’s geb neral condition was improved in a month, and the eyes were free of symptoms after two months.
Sven Larsson: Some Cases of Progressive, Familial Macular Dege: neration.
I. O f three brothers in a family, the two eldest, aged 12 and 15 respectively, exhibit macular degcncration. The disease appears to have given its first symptoms a t thc agc of twelve in both boys; the younger boy was not conscious of his defect. The parents arc cousins. In the father’s family there is pronounced colour blindness, but others wise there is nothing of interest in thc family history. T h e patients arc scnsitivc to light, thus making examination of the fundi rather difficult. The patients suffer from nyctalopia. The older brother’s acuity of vision is reduced to 0.2 on both eyes and has been stationary for a two years’ period of obscrvation; in the younger brothcr, the vision has in the course of the samc period dcteriorated from 0.7-0.8 to 0.5 on both eyes. There are smnll central scotomata, in the younger boy with comparatively free centres (ring scotoma). In the fundi, therc is a suggestion of cloudincss a t the edges of the papillac. In the macula therc is a fairly wellsdefined spot, about the size of a papilla, with a granular appearance and generally of a somer what deeper red shade than its surroundings. The normal reflcxcs are absent. In thc peripheral parts the fundi appcar to be slightly deficient in pigment. The vessels look normal. Thcre arc similar changes in both eyes.
11. Of five brothers in another family, 2 aged 23 and 28 respecs tively present symptoms fully identical with those of the two preceding cases. The family history is of no interest. The deterioration of vision was first observed a t the age of fifteen, but much earlier pros nounced coloilr blindness had been discovered in one of thc brothers. Both of them had nyctalopia and were very scnsitive to light. In the course of 2 or 3 years of observation, the vision had deteriorated from 0.5 to 0.2-0.3, about equally on both sides. Relative central scotomata. Thc papillae are blurred and the maculae have about the same aps pearance as in the previous cases. In addition the elder brothcr has numcrous small, palc foci lying deep in the retina or the chorioid and having about the appearance and distribution of circinate retinir tis, though the foci here are more scattered and less whitc. The Was; scrmann rcaction ncgative. (Demonstration of the elder brother.)
111. Man aged 25, one of five brothers and sisters, of whom one of the latter has poor eyesight owing to ,,unusual macular alterationsa (examined by another doctor). The family history is of 110 interest. Wcakness of vision was observcd a t the age of 17, followed by rapid deterioration for the first year, after which it remained stationary a t 0.1 on both cyes. In thc fundi, there are blurred papillar cdges,

412
typical macular alteration as in the foregoing cnscs and similar small, pale, more peripherally situated foci as in circinate retinitis.
There is no doubt that these cases belong to that group of macular degeneration which S t a r g a r d t has called progressive familial macular degcneration without psychic anomalies. The typical distur: bance of function and the ophthalmoscopic symptoms, thc bilatcral presence of the symptoms and the familial appearance of the discasc, beginning a t a definite agc in the same family and with a similar picture and course in the different members of it, thc slow progrcss and the absence of othcr signs of discasc all establish the diagnosis.
The etiology is unknown. The diseasc is ranged under the heredo: degenerations and has bcen considercd equivalent to retinitis pigmen: tosa (L e b c r, T r c a c h e r5C o 11 i n s ) . The children in consanguinc marriagcs arc thought to be more inclined to this disease ( N c t t- 1 e s h i p) but there is no typical heredity. Syphilis has been regarded as an etiological factor (M o r a x, S c h i f f, W c r t h e i m e r and T i 1 1 6 ) but this seems hardly likely. In the course of the diseasc there is frequently quite rapid progress a t first up to about the age of 20, after which the diseasc progresses more slowly or is stationary. There may be extreme reduction of vision, but not blindness as a rule. Narrowed retinal vcssels and pale papillae have bcen observcd (A 1 k i o, S t e y 11). N o pathosanatomical examinations appear to have been made. In one case of a possibly related form of macular de: generation (D o y n e), T r e a c h e r X o 11 i n s found the place of thc pigmcnt epithelium occupied by a hyalinoid mass between the retina and the lamina vitrea and destruction of the rod and conc cells and the nuclear layers of the retina.
The cloudiness of the papillae in all the cases rclated hcre is of interest. I t has been supposcd that the degcneration is preceded by hypertrophy of the neuroglia (S c h a 11). Another interesting fcaturc is the symptom complex, observed in 2 cases, resembling circinatc retinitis, which should probably be takcn to have the same origin as the simultaneous macular alteration. The pronounced sensibility to light is striking; it was particularly noticeable in these cases and hin.dercd examination by Gullstrand’s ophthalmoscope.
K. 0. Granstrom: A Simple Method of Measuring the Distance Between the Pupils.
The distance between thc pupils is usually measurcd in a simple manner by thc soacalled strabomcter, giving values which arc probably sufficiently exact for the testing of eye-glasses for example. Certain sources of error are, however, connected with this method, especially when thc distance betwcen the pupils is to be measured in distant focus, as most pcoplc find it difficult to avoid convergence when the strabometer is placcd closc before their cyes by an cxamincr standing very near them. Too small a value may in addition be obtained by the circumstancc that thc examiner is only a t arm’s length trom thc

413
patient and the strabometer naturally can not be held immediately in front of the pupils.
In order to avoid these sources of error, another method has been used to measure thc distance between the pupils.
The apparatus consists of a monocular glass adjusted to 3 or 4 m., and a pair of spectacles of windowsglass. O n each of the latter there is a distinctly visible vertical line with a distance of 60 mm. between the lines. T o both sides of these there arc somewhat shorter vertical lines a t intervals of 1 mm.
The measurement is extrerncly simple. The subject sits on a chair a n d focusses on a distant object. A little laterally to the direction of his glancc a t a distance of about 3 m. the examiner looks through t h e monocular and observes which line corresponds to the centre of the pupils, thus a t once obtaining the distance betwcen them.
The examining room should of coursc be well lighted, among other things so as to make the pupils myotic. Possible disturbing reflections from the lenses are easily avoided by a slight bending or turning of the subject’s head. I t is very easy to read off the values, and difs ferent examiners agree very well in their findings. Theoretically this method gives too short a distance between the pupils since the examiner is not in the distant focus of the subject, but a t a distancc of 3 m. this error is extremely slight and has no practical signis ficance.
This method has been tried with good effect in selecting lookcouts in the antisaircraft artillery. The measurement of distances here is made with stereoscopic instruments, and to obtain good and rapid adjustment each obscrver should know the exact distance between his pupils.
A similar principle of measuring the distance between the pupils of the eyes was suggested, according to G r a e f c ~ S i i m i s ch’s res ference book (sUntersuchungsmetliodenc), by E m m c r t in 1880, thc difference being merely that E m m e r t used only one vertical line o n each lcns and changed its position until i t crossed the centre of the pupil.
K. G. Ploman: A Case of Self=Mutilafion b y Tearing Several Ocular Muscles.
H. C., a w i d o w a g e d 6 4. The patient, who was a t a hospital for mental diseases, had in an unguarded moment of mentar confusion o n Dec. 23, 1923 mutilated both eyes with her right index finger. O n account of bleeding, the eyes were bandaged a t once.
L o c a l c o n d i t i o n D e c . 2 5 , 1923 . Right eye: the upper lid was slightly swollen and the eye protruding somewhat. In the cons junctiva, which is slightly congested, a sharply cut lesion can be seen running around the cornea a t a distance of 2 to 5 mm. from the limd bus. Tcmporally a strip of bloody tissue about 2 cm. long hung down from the wound. There was a minor erosion in the centre of the
11

414
cornea, the pupil was dilated and apparently rigid. Left eye: the lids were inconsiderably swollen. Nasally in the conjunctiva bulbi there was a vertical lesion, 1 cm. long and about 2 mm. from the limbus. The cornea and media were normal, as was the pupil also. E x a s m i n a t i o n u n d e r a n a e s t h e s i a . In the right eye, the external rectus muscle was torn off 2 cm. from its origin and the superior rectus about 1 cm. from its origin; on the upper side of the eyeball there was a long, torncoff tendon running under the conjunctiva toward the upper outer quadrant, belonging probably to the superior obliquus. The internal and inferior rectus and the inferior obliquus were intact. In the left eye the internal rectus was torn off to its origin. The muscles were sutured as well as possible.
There was an uneventful recovery. The right pupil which was very large a t first gradually diminished in size.
J a n. 2 4, 1 9 2 4. No exophthalmos. The right eye deviated nasally 10 to 15. The right pupil was larger than the left, and did not react directly, only consensually. The left pupil was normal. The right papilla was very pale and a t its nasal edge a slight hemorrhage could be seen; the fundus was otherwise normal. The left fundus oculi was also normal.
J a n . 2 8 , 1 9 3 1 . In spite of considerable negativism on the part of the patient it was possible to make a fairly complete examination. When the patient looks straight ahead the position of the eyes is normal. The right eye can not be abducted a t all and its upward movements are limited; the nasal and downward movements are normal. The pupil reacts, though somewhat sluggishly. The media are normal, the optic nerve pale. V. 0.1 (doubtful value). The left eye presents no objective changes and its motility is normal. V. 0.5 (4- 1.00
C o m m e n t. This is probably a rather unusual case. In the right orbit the finger must have been pushed very far in since the abs ducens had been torn off far to thc back, and the blanching of the optic nerve (and possibly also the hemorrhage close to the papillae) suggests a dircct lesion. The pupil rigidity is probably likewise to be regarded as an injury to the posterior ciliary nerves. It is remarks able that such violence produced no more serious infection and that the position of the right eye has been so little affected in spite of the extensive muscular injury.
f 1.00 c. 180").
20th Meeting, April 25th, 1931. Sven Larsson: A Case of Ablatio Retinae Successfully Operated b y
Electroendothermy.
K. 0. Granstrom: A Case of 0culo:Glandular Tularemia. To be published shortly in the Acta Ophthalm.

41 5
Maria He1lgren:Sjogren: A Case of a Thin=WaNed Traumatic Cys t in the Anterior Chamber.
The patient is a man aged 20. Four ycars earlier there had been a perforating injury to thc upper margin of the left cornea. Healed with the upper edge of the iris slightly drawn up and full retention of vision. After three years the patient noticed in the upper part of the iris a yellow spot which increased in size, and the vision detcriorated; a t times the eye was slightly reddened. After another halfsyear the patient came to the Serafimer Hospital (January 1931) and at that time prescnted the following condition:
Left eye slightly inflamed, with a dense granular lightsbeam and a suggestion of hypopyon; springing from the upper angle of the chamber there was a yellowish white, pea-sized cystoid formation, a posterior cortical cataract, and cloudiness of the vitreous body. Vision 4-5/60. T.norma1. Kight eye normal. SR in the blood normal, Wassermann negative. The cyst was punctured, and its purulent cons tents werc found on cultivation to give a small growth of pneumo; cocci. After operation, the remainder of the cyst shrank; after one month there was no further irritation of the eye and the vision was 0.1. The patient was discharged but returncd after a few wceks with the eye in about the same condition as before. Under atropin treat? mcnt the cyst spontaneously regressed almost entirely in thc course o f two months. Its anterior wall adheres to the completely trams parent cornea. The iris is partially drawn forward to its posterior wall. Only the upper part of the cyst contained an exudatc, the lower par t being entirely transparcnt. A thin lightsbeam remains. T h e lens is cloudier. V. 0.15160.
Fredrik Kugelberg (Tirupatur): 1ntra:Capsular Cataract Extraction- Swedish: Hygica, Vol. 93, p. 689, 1931.
21st Meeting, October 2nd, 1931. In response to a request of the central executive board of S v e;
r i g e s L a k a r f ii r h u n d (IJnited Physicians of Sweden) for an ex2 pression of opinion from the section on thc requircments for the right to advertisc as an eye specialist, the section agreed aftcr an animated discussion on the following statement:
,For the right to advertise as an eye specialist, three ycars’ training as a subordinate physician a t a hospital shall be required, at least two of these at an eyc clinic and a t least one of these two at an internal ward for eye diseases; the work done during the third year to rcmain a free ch0ice.n

416
22nd Meeting, November 28th, 1931. A. Dalkn: Invalidity Following Injuries to the Eye. The lecturer reviewed the formerly applied manner of cstirnating
invalidity following eye injuries in Sweden, and then reported on the scale on which such estimates are based a t present. According to this scale (see table), a visual acuity of 0.7 is regardcd as adequate for
Table.
~~
1-0,7 0 ~ 0
I _______- ~
25
I
25 ~ 32
a n able person. A reduction of the vision of one eye to 0.3 is taken as involving a 10 per cent invalidity, complcte loss of vision in one eye, a 20 per cent invalidity. If the injured eye has t o be enucleated, the compensation rises to 25 per cent, and the patient is in addition compensated for the purchase and renewal of the artificial eye. Total blindness is regarded as 100 per cent invalidity, but a person who has completely lost his eyesight by an accident usually gets a higher coms pensation than he would on an annuity calculated in the usual way on 100 per cent; this is on the legal basis that higher compensation is due persons whose physical condition demands special care. As

417
a rule the compcnsation is probably equivalent t o 75 or 80 per cent of thc injurcd person’s former salary.
This scale was elaborated on the samc principles as those on which the lccturer based the scale accompanying the >,inquiry into injuries of the eyen which he made in 1919 for the R i k s f o r s a k r i n g ss
a n s t a 1 t (Statc Insurance Bureau). When thc visual acuity falls below the value that is regarded as equivalent to fully adcquate for an able person, it is considered of no consequence how the visual reduction is distributed between the two eyes. A visual acuity of 0.7 in one eye and 0 in the other is therefore the same as 0.6 in the one and 0.1 in the other, or 0.5 in the one and 0.2 in the other, and so m. The lccturer considered this principle as on the whole the proper one as well a5 practically convenient, but he emphasised the fact that exccptions might have to be made in special cases according to the occupation of the injured person. Individual considerations might, in the lecturer’s opinion, otherwise also have to be made occasionally, since different occupations make different demands on the visual acuity. However, there are great practical difficulties hindering the classification of the insured persons into groups based on the visual acuity requircd b y their occupations, since within the same occupation there may be different kinds of work requiring very difs fcrent degrecs of visual acuity, and since many of the insurcd persons occasionally change their occupation or the specific work they are doing. In the lecturer’s opinion, i t is wisest to have a scale giving adequate compcnsation to the majority of the insured, and to raise this Compensation in individual cases in which this would be justified. Even if oiic or another case were to be over:compensated or possibly underscornpensated by such a system, a good deal of discontent and many complaints on the par t of the insured would no doubt thereby bc avoided.
If there has already been invalidity before an accident, that caused
by the accident is computed by the formula - I , in which I. rer
presents the invalidity after the accident and I, that before the acr cident. This calculation would in the lecturer’s opinion be correct if the injured person’s income sank in inverse proportion to his ins validity and if his annuity were in proportion to his total salary. Since, however, the annuity is calculated only on salaries of up to 3000 k r o n o r - a sum probably often carned evcn by partial ins valids - the result will be that a person who has had his vision reduced by two or more accidents, cach of which gives him the right to compensation, will receive a higher compensation than if the res duction of his vision had been causcd by only onc accident. This the lecturer regards as unreasonable.
According to the law, invalidity is compensated only in cases of accidents which have reduced the ability to work by a t least 10 pcr cent. A person who has had scveral succcssive accidents none of
10-1

418
which by itself has reduced hi5 ability by as much as 10 per ccnt may thus lose much of his sight, indeed become almost blind, without any claims to compensation. This is also unjust.
In unilateral aphakia, the lecturer is of the opinion that invalidity should be considered reduced by 5 per cent a t most if the visual acuity of thc aphakial eye is used in the calculation after correction. The suggcstion made in some quarters that the acuity value used should be halfway between that obtained with a glass and that without a glass leads to the illogical consequcncc that a person with a traumatic cataract and a vision of for instance 1/60 on one cyc, after a successful cataract operation with the vision, corrected by a glass, amounting possibly to 1, totally loses the fairly considerable invalidity compensation he enjoyed previously, although his ability to worh has hardly been improved by thc opcration.
The lecturer also emphasiscs his vicw that invalidity must not, naturally, be judged solely by the visional acuity, and that certain functional disturbances such as limitation of the field of vision, pa: ralysis of the eye muscles, etc. can not be treated uniformly, but must be judged individually. In addition, he points out the difficulties that in certain cases may attend the proper estimation of invalidity, for instance when the uninjured eye at the time of the accident is subject t o a progressive disease which has not yet essentially reduced the vision but will probably sooner or later lead to blindness.
A comparison between the invalidity compensation for eye injw ries in Sweden and the neighbouring countries proves that i t is higher in Swcden. It is, of course, possible that eye injuries under the scale in force in Sweden at present are somewhat ovcrscompensated, but if such is the case, the same is probably true as well - and perhaps to a greater extent - in certain other injuries not connected with the eyes.
Y. Lindblad: Demonstration of the Microscopic Slides of Two Cases of Fat Emboli in the Retina. T o bc published in full in a later number of the Acta Ophthalm.
Sten Tengroth: Statistics of Roentgen Therapy at the Eye Clinic of the Sabbatsberg Hospital (head, Dr. F o r s m a r k).
In the course of the last three years about 150 of the patients treated at the eye clinic and its outspatient dcpartment were given Roentgen treatment, chiefly those suffering from chronic uveitis (tus berculous), sclerokeratitis and parenchymatous kcratitis. The Xsray dosage was usually 1110-1/8 SUD (HED), repeated onc or more times, first a t intervals of one week, then of two to four weeks or longer, in other words a lower dose than S t o c k’s. More than 4 or 5 treatments were not willingly given. No complications were observed. Good results were obtained in something more than 50 per cent in chronic uveitis and sclerokeratitis. In parenchymatous keratitis, the treats

419
ment probably cut the process short and caused more perfect clearing up. In practically all the cases the subjective discomfort rapidly disappeared, which must be regarded as socially important. The re+ sults agree with what has been found at foreign clinics and encourage the further employment of roentgenotherapy in diseases of the eye.