Embed Size (px)
Citation preview
Trachs and Tubes and Shunts, Oh My!
2016 Vermont Healthcare and EMS Preparedness Conference
Disclaimer I have no actual or potential
conflict of interest in relation to this presentation.
Children with special health care needs (CSHCN)
• 12 million children (18% of the population) have special health care needs. 1
• Approximately 25% of all children seen in Pediatric E.D.’s have special needs. 2
Who are CSHCN ? • Premature infants
• Infants and children with congenital heart/lung disease
• Infants and children with neurologic abnormalities
• Technology-dependent – Ventilator, Pacemaker, etc.
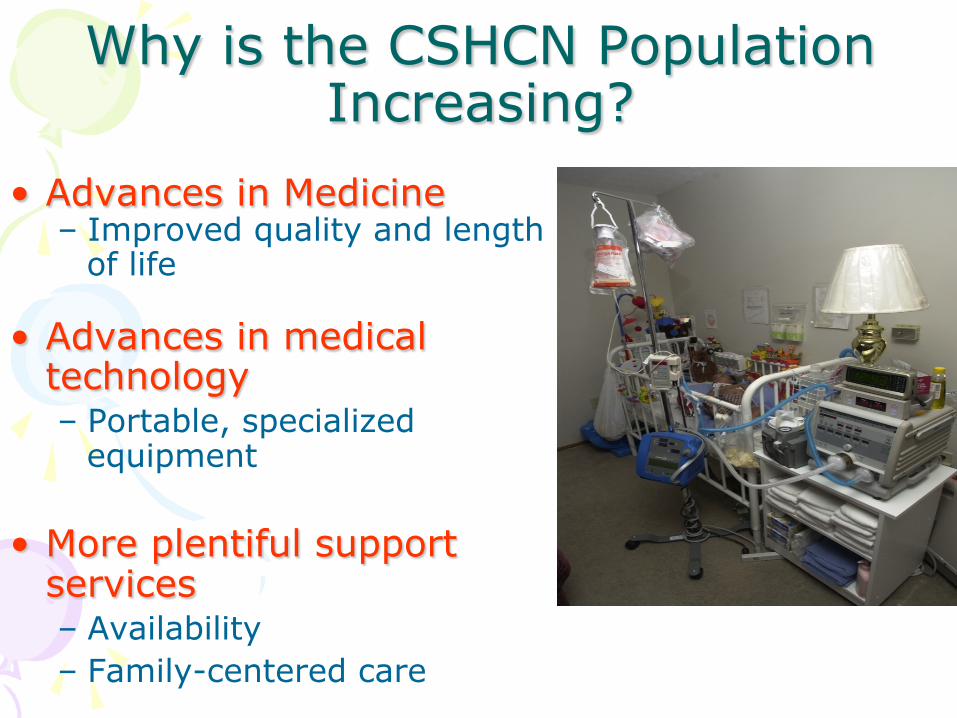
Why is the CSHCN Population Increasing?
• Advances in Medicine – Improved quality and length
of life
• Advances in medical technology – Portable, specialized
equipment
• More plentiful support services – Availability – Family-centered care

Tracheostomy
Tracheostomy A surgical opening into the trachea through which a tracheostomy tube
can be passed. The child then breathes through this opening.
Tracheostomy Tubes
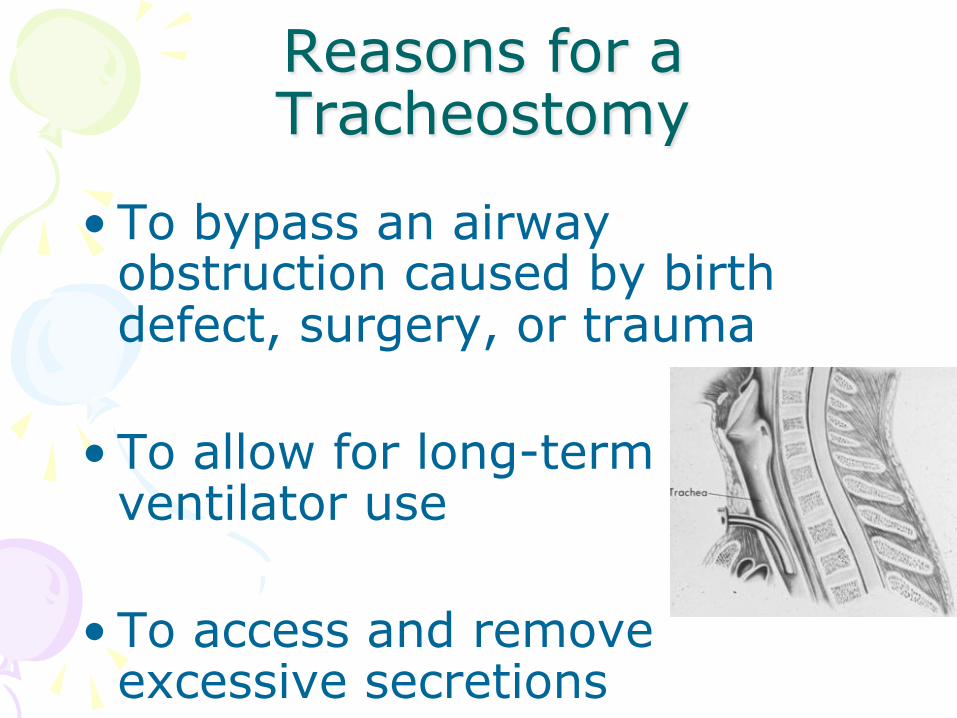
Reasons for a Tracheostomy
• To bypass an airway obstruction caused by birth defect, surgery, or trauma
• To allow for long-term ventilator use
• To access and remove excessive secretions
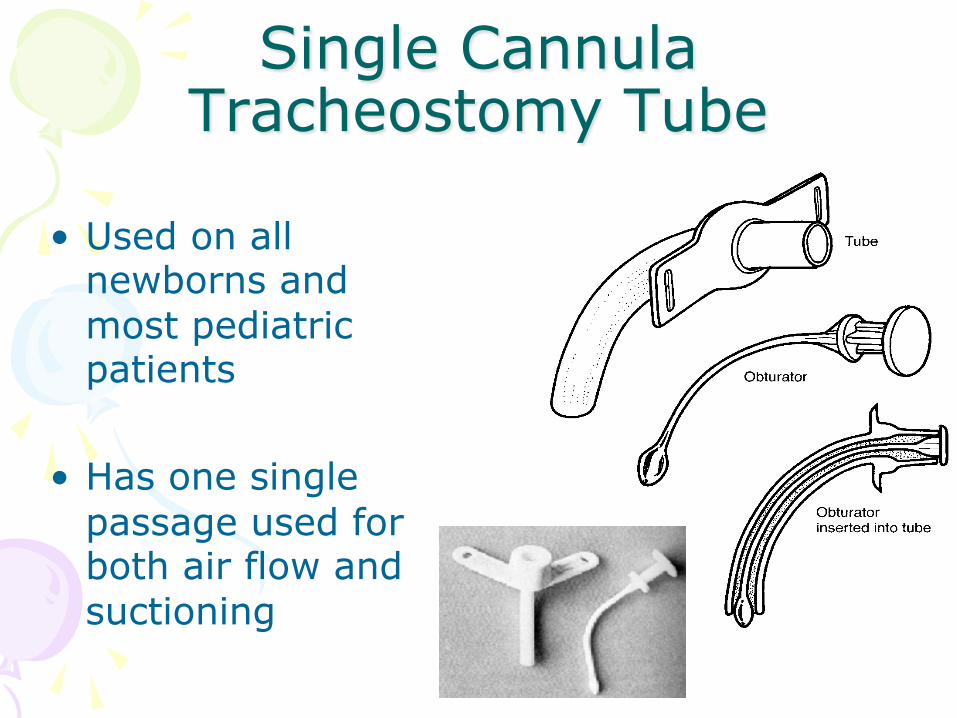
Single Cannula Tracheostomy Tube
• Used on all newborns and most pediatric patients
• Has one single passage used for both air flow and suctioning
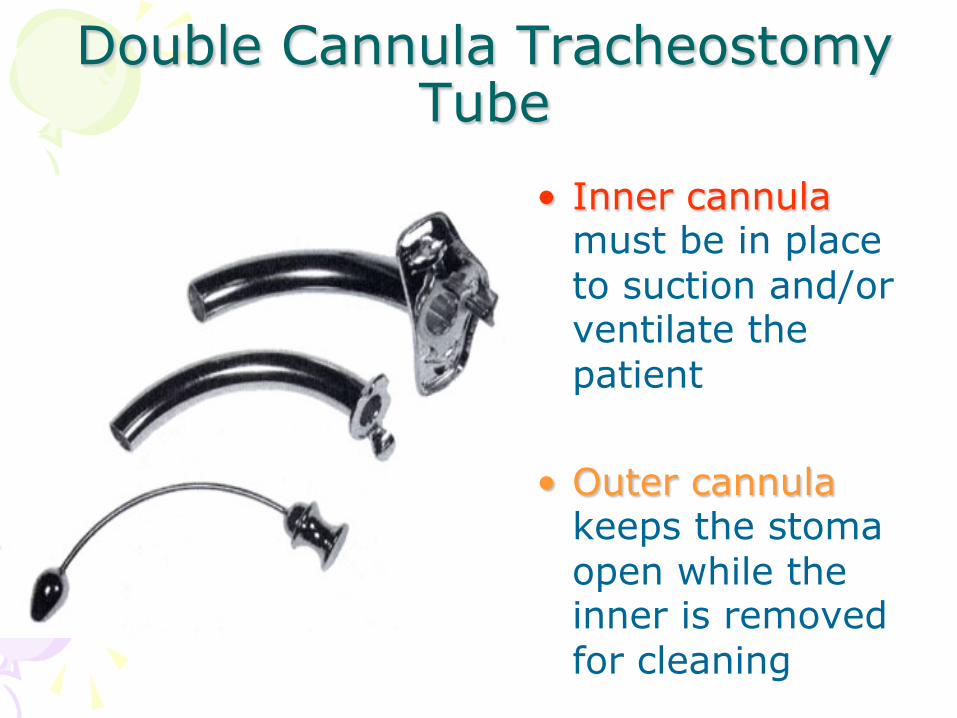
Double Cannula Tracheostomy Tube
• Inner cannula must be in place to suction and/or ventilate the patient
• Outer cannula keeps the stoma open while the inner is removed for cleaning
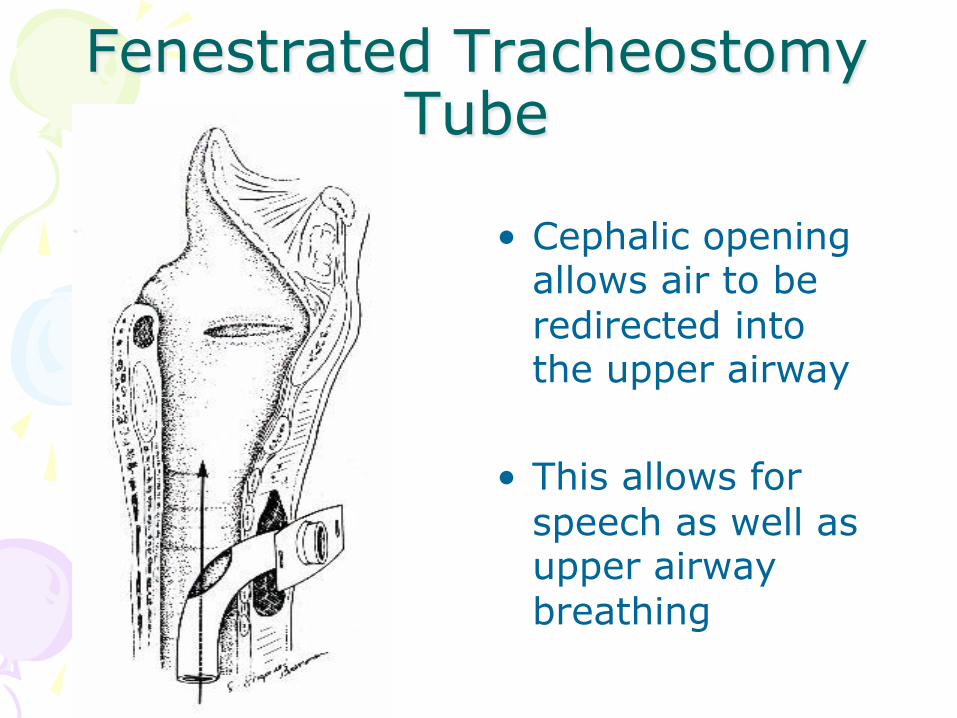
Fenestrated Tracheostomy Tube
• Cephalic opening allows air to be redirected into the upper airway
• This allows for speech as well as upper airway breathing
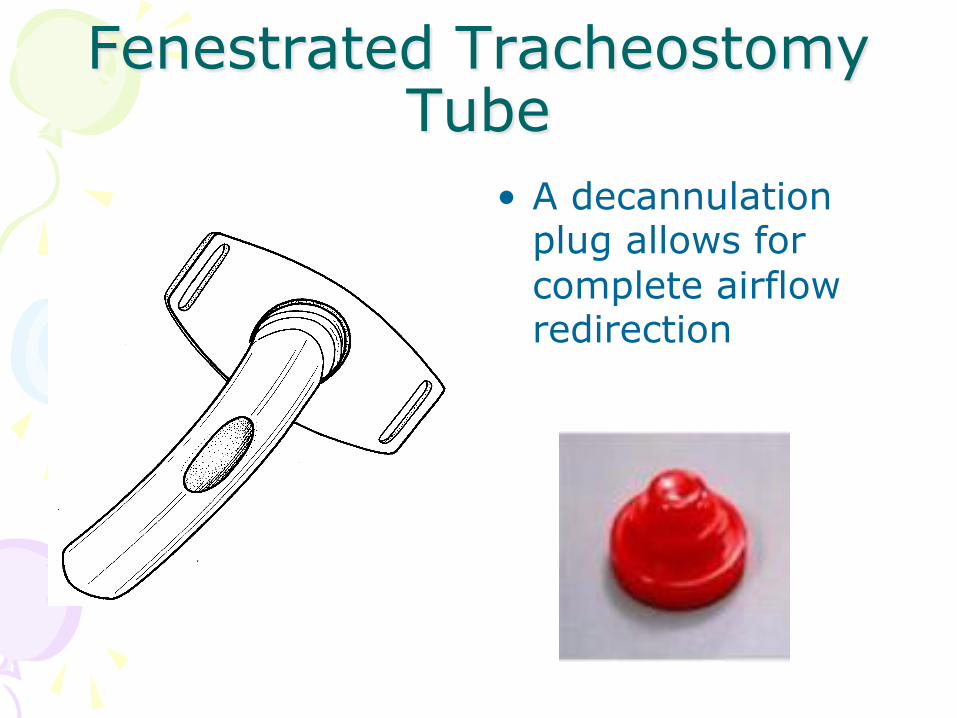
Fenestrated Tracheostomy Tube
• A decannulation plug allows for complete airflow redirection
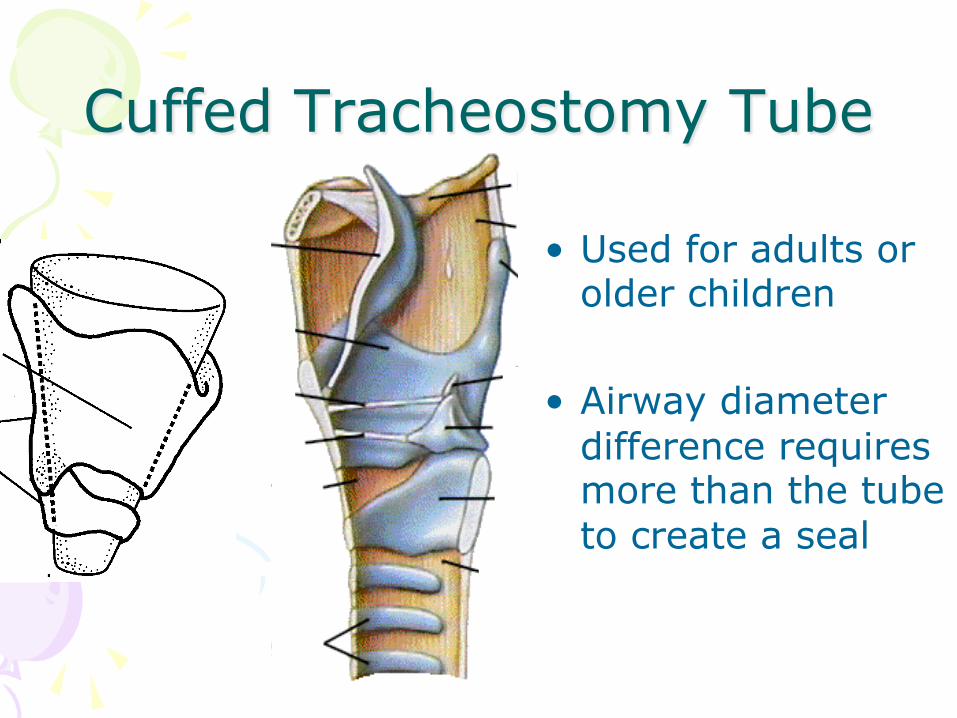
Cuffed Tracheostomy Tube
• Used for adults or older children
• Airway diameter difference requires more than the tube to create a seal
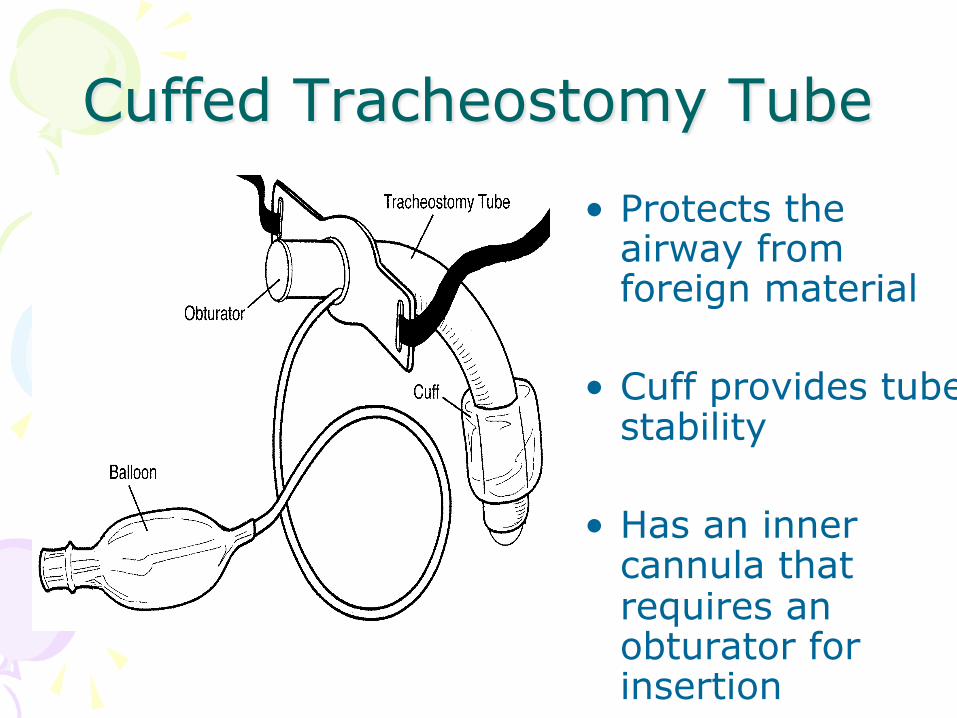
Cuffed Tracheostomy Tube
• Protects the airway from foreign material
• Cuff provides tube stability
• Has an inner cannula that requires an obturator for insertion
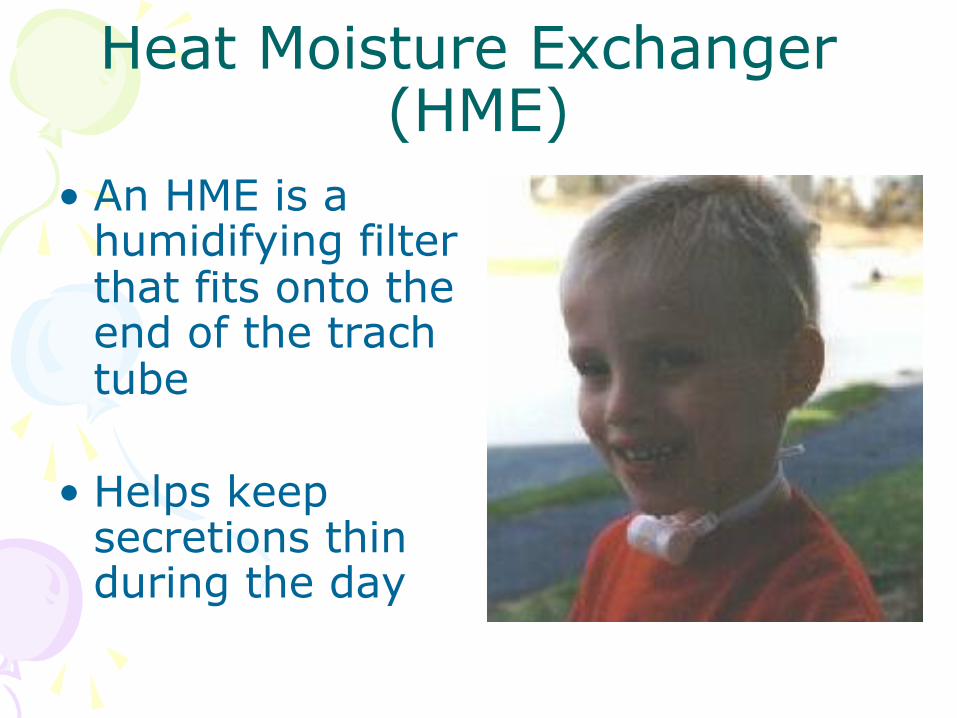
Heat Moisture Exchanger (HME)
• An HME is a humidifying filter that fits onto the end of the trach tube
• Helps keep secretions thin during the day
Tracheostomy Emergencies • Obstruction of the tube
– Accumulated dry secretions – Improper airway positioning – Incorrect insertion – Tracheal stenosis
• Hemorrhage from the stoma site
– Tracheal necrosis/fistula development
• Displacement of the tube
Tracheostomy - Management
• Place a rolled towel under the child’s shoulders
• Make sure the tracheostomy tube is properly seated
• Make sure obturator/ decannulation plug has been removed
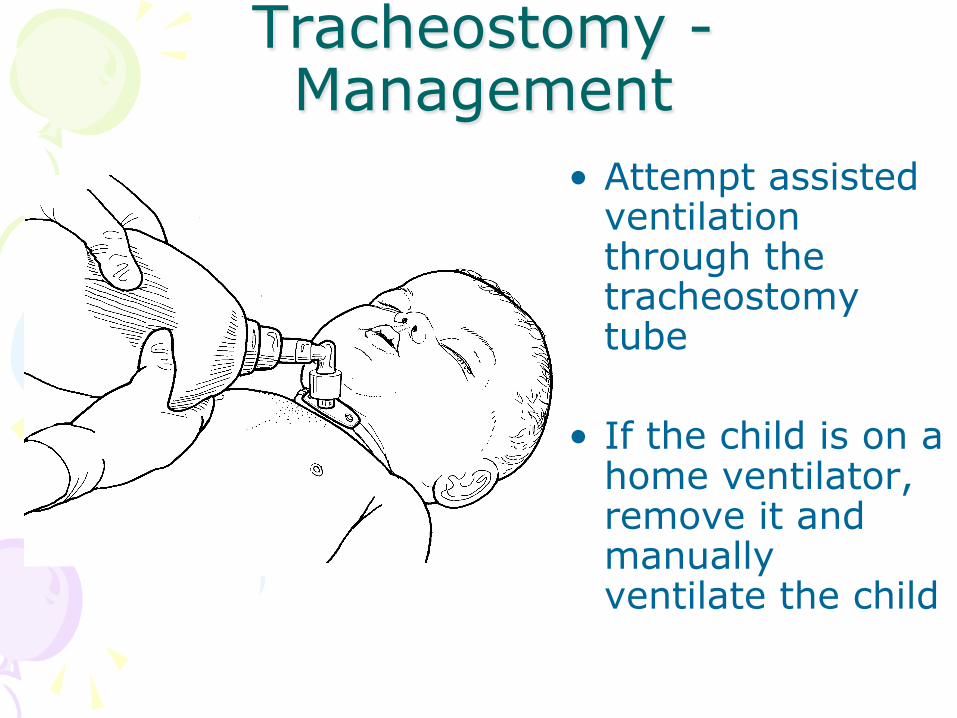
Tracheostomy - Management
• Attempt assisted ventilation through the tracheostomy tube
• If the child is on a home ventilator, remove it and manually ventilate the child
Tracheostomy - Management
• Pre-oxygenate the patient
• Loosen secretions with normal saline
• Suction for no more than 5-10 seconds while removing the catheter
• Re-assess pulse and mental status
4
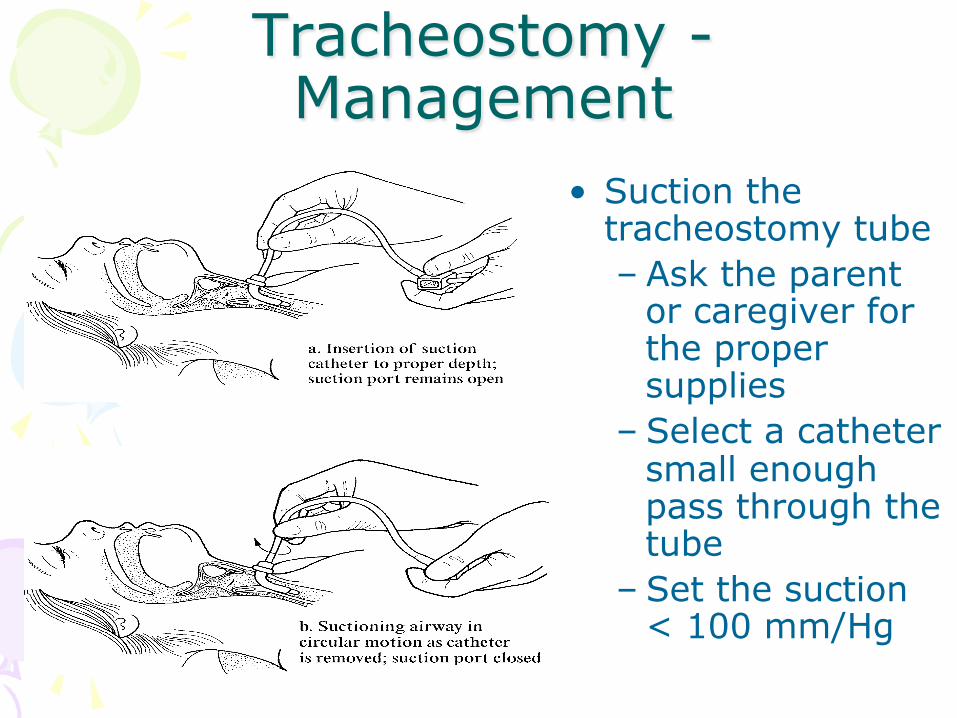
Tracheostomy - Management
• Suction the tracheostomy tube – Ask the parent
or caregiver for the proper supplies
– Select a catheter small enough pass through the tube
– Set the suction < 100 mm/Hg
Tracheostomy - Management
• There are times when the patient’s tracheostomy tube may need to be replaced – Tube has been dislodged – Tube cannot be cleared by suctioning
• Follow your protocol !
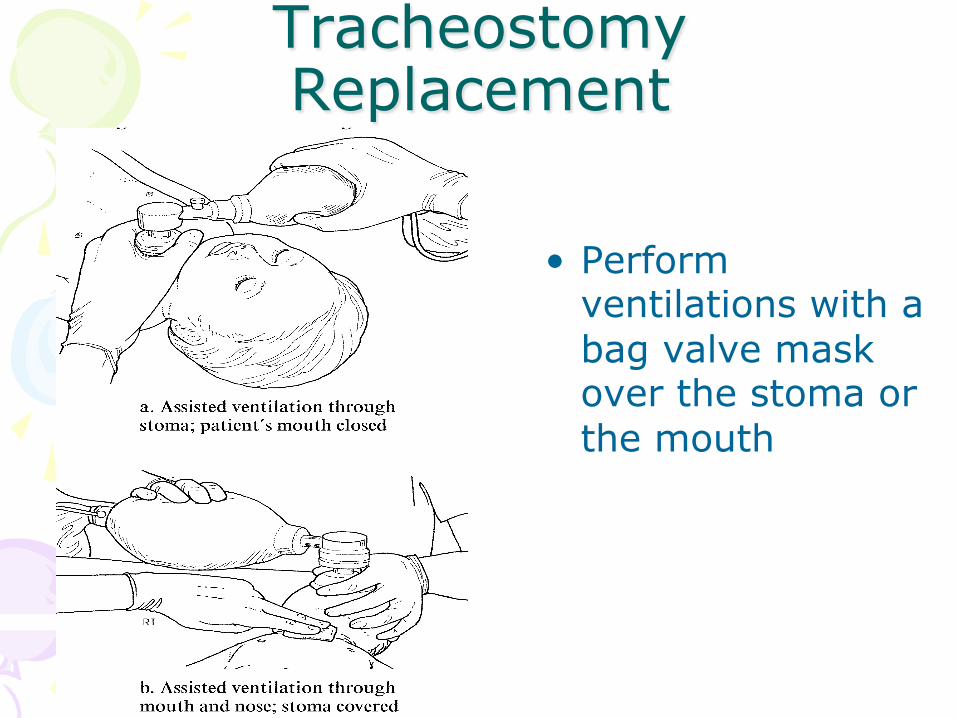
Tracheostomy Replacement
• Perform ventilations with a bag valve mask over the stoma or the mouth
4
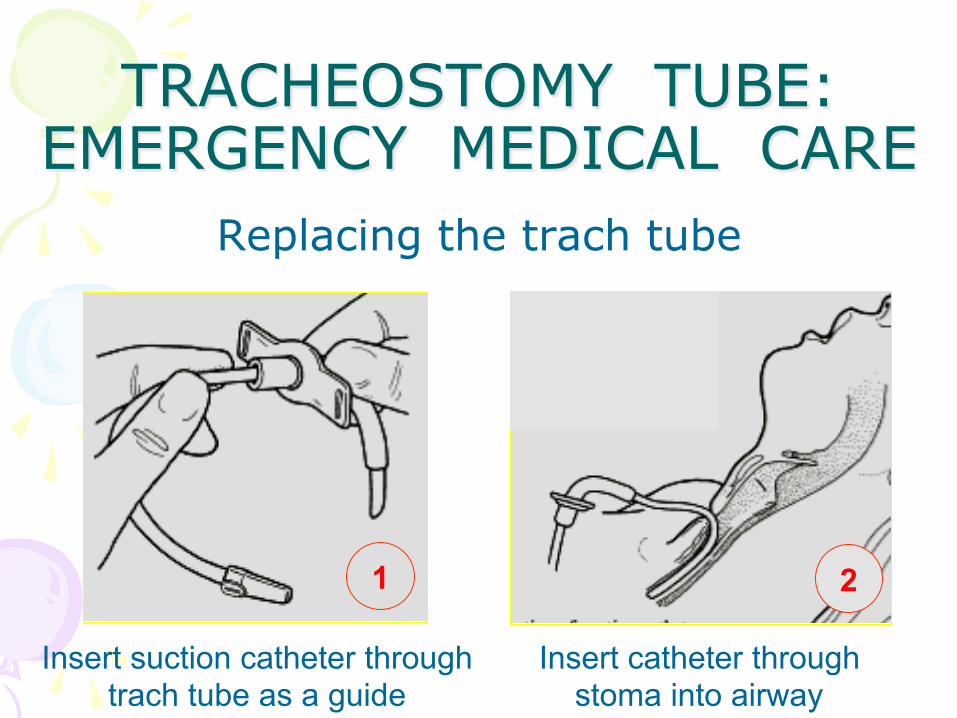
TRACHEOSTOMY TUBE: EMERGENCY MEDICAL CARE
Replacing the trach tube
Insert suction catheter through trach tube as a guide
1
Insert catheter through stoma into airway
2
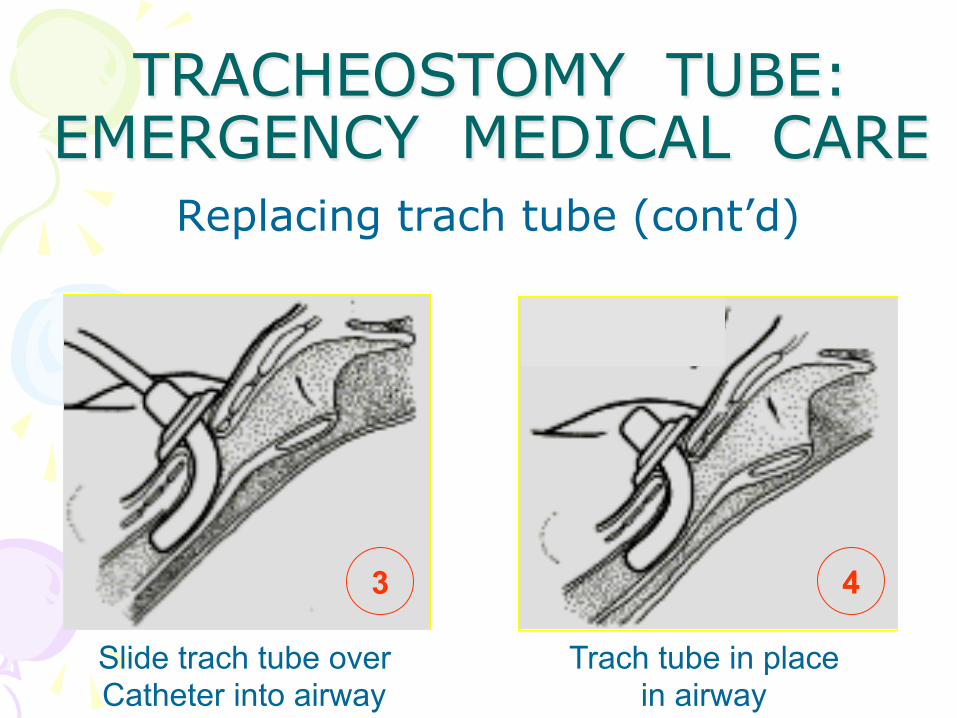
TRACHEOSTOMY TUBE: EMERGENCY MEDICAL CARE
Replacing trach tube (cont’d)
Slide trach tube over Catheter into airway
3
Trach tube in place in airway
4
Tracheostomy Replacement • Confirm proper placement
– Equal chest rise – Equal B.S. – No sign of sub-Q air – Improvement of pulse, color and mental status

Feeding Catheters
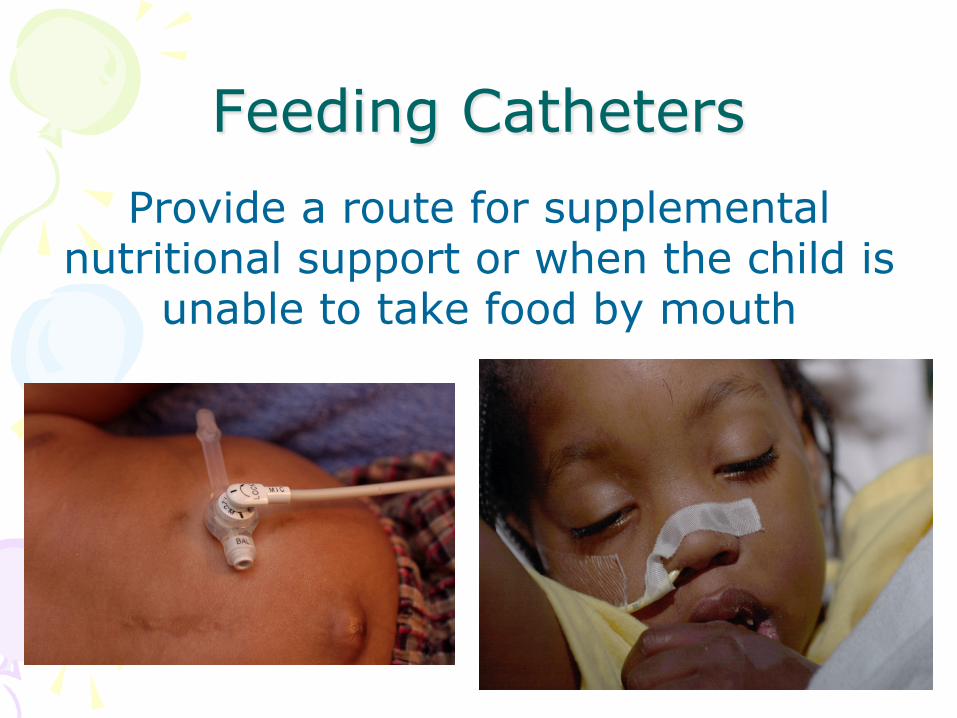
Feeding Catheters Provide a route for supplemental
nutritional support or when the child is unable to take food by mouth
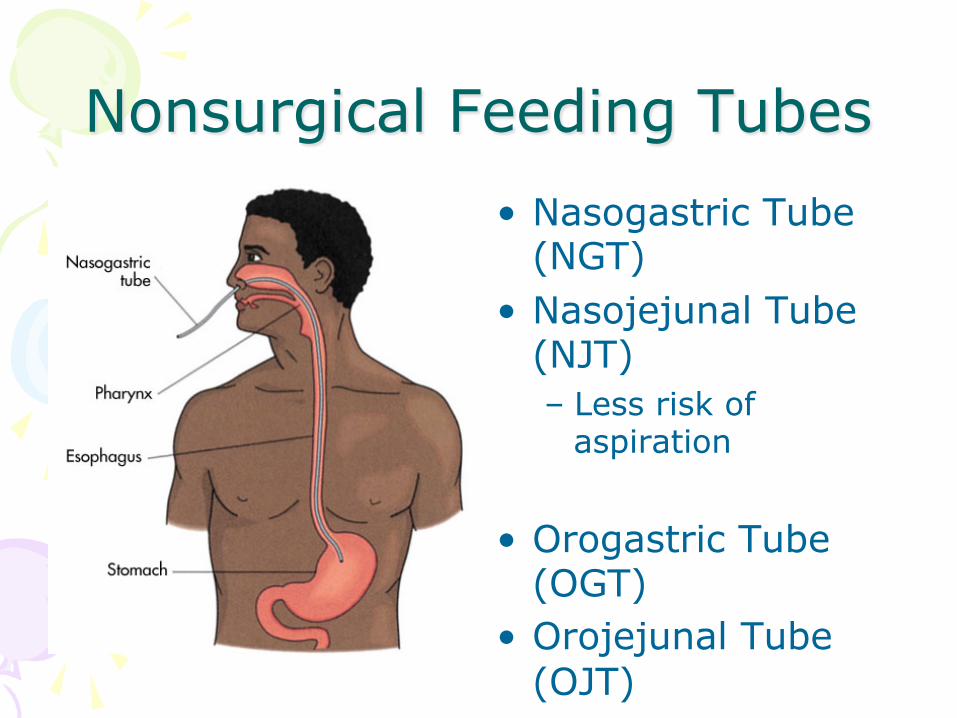
Nonsurgical Feeding Tubes • Nasogastric Tube
(NGT) • Nasojejunal Tube
(NJT) – Less risk of
aspiration
• Orogastric Tube (OGT)
• Orojejunal Tube (OJT)
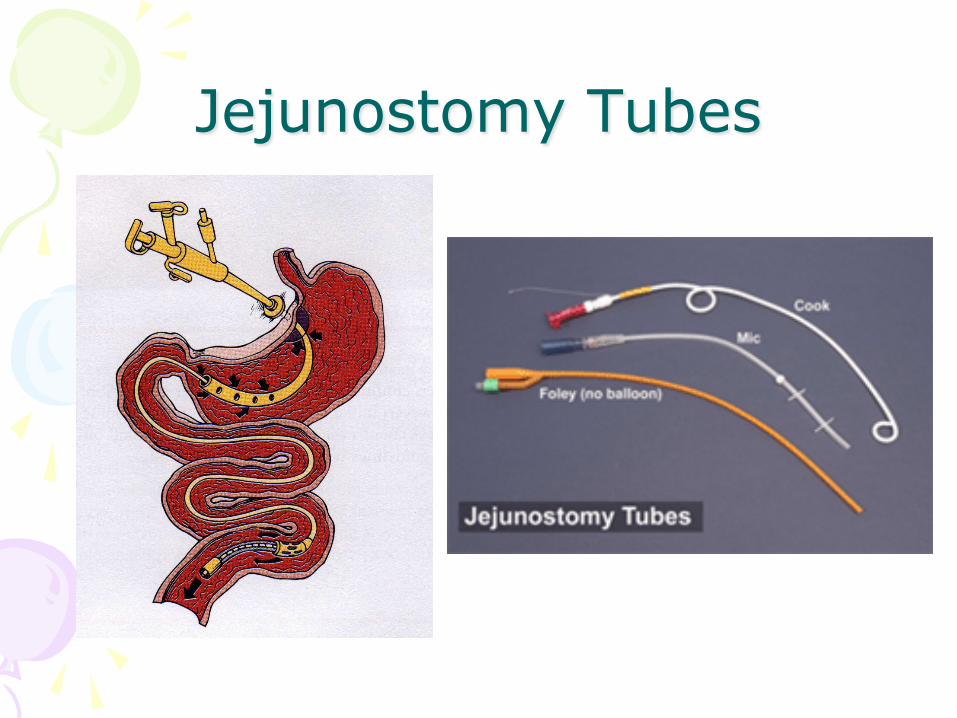
Jejunostomy Tubes
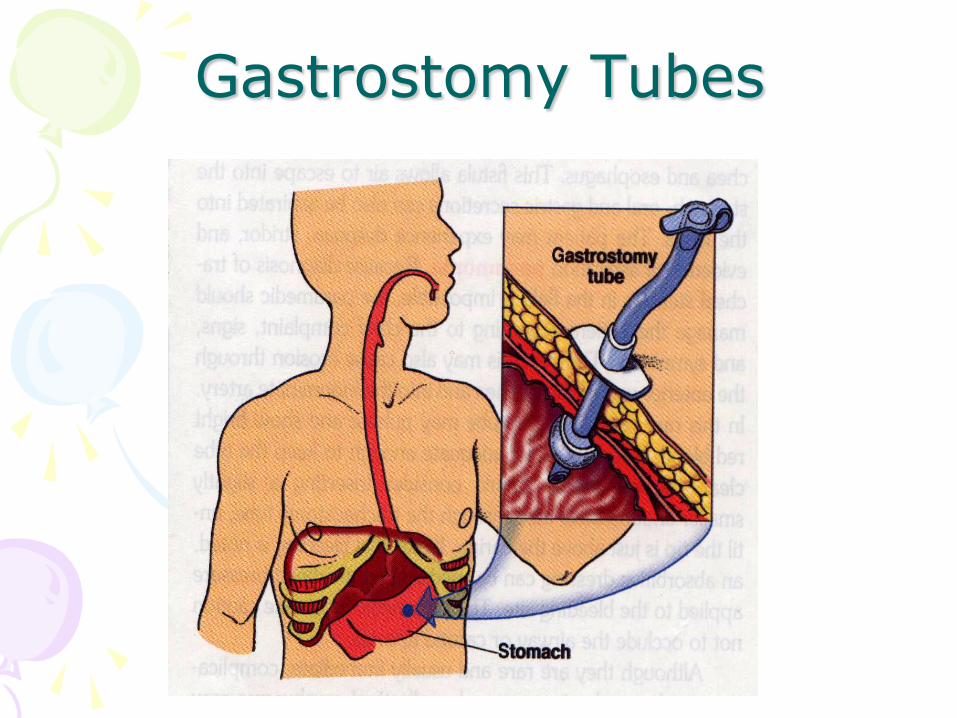
Gastrostomy Tubes
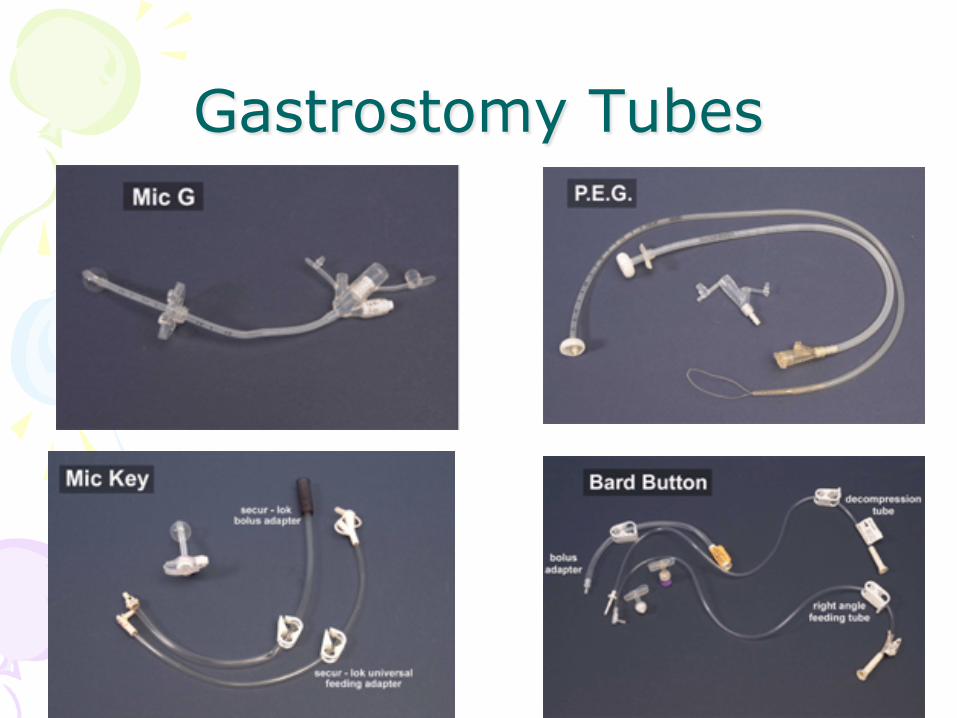
Gastrostomy Tubes
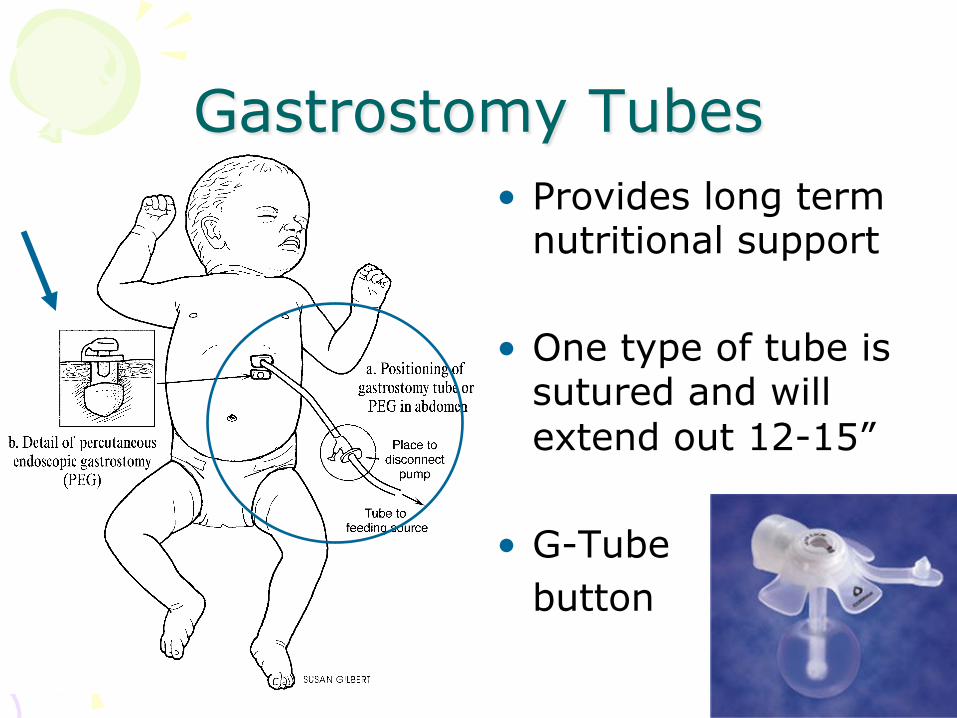
Gastrostomy Tubes • Provides long term
nutritional support
• One type of tube is sutured and will extend out 12-15”
• G-Tube button

4
Feeding Tubes - Complications
• Site Bleeding
• Infection
• Broken
• Dislodged
• Respiratory distress – Aspiration
Management Considerations • Be alert for changes in mental status
• Consider hypoglycemia in a diabetic pt. that can’t be fed
• Control bleeding at site with sterile dressings
• With extended ventilation time, watch for gastric distention

4
4
Management Considerations • Follow all local protocols before performing
any non-standard procedures
• Let the caregiver help you with flushing the tube
• Bring any dislodged/broken tubing with you
• Transport is usually required if your assessment reveals any complications present a danger to the patient

Shunts
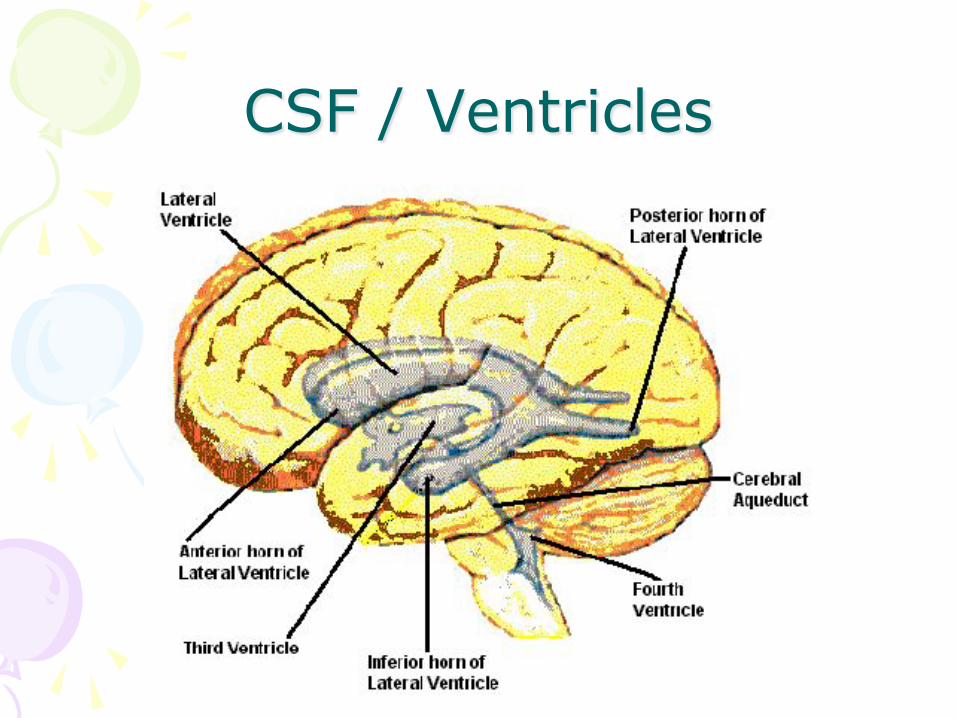
CSF / Ventricles
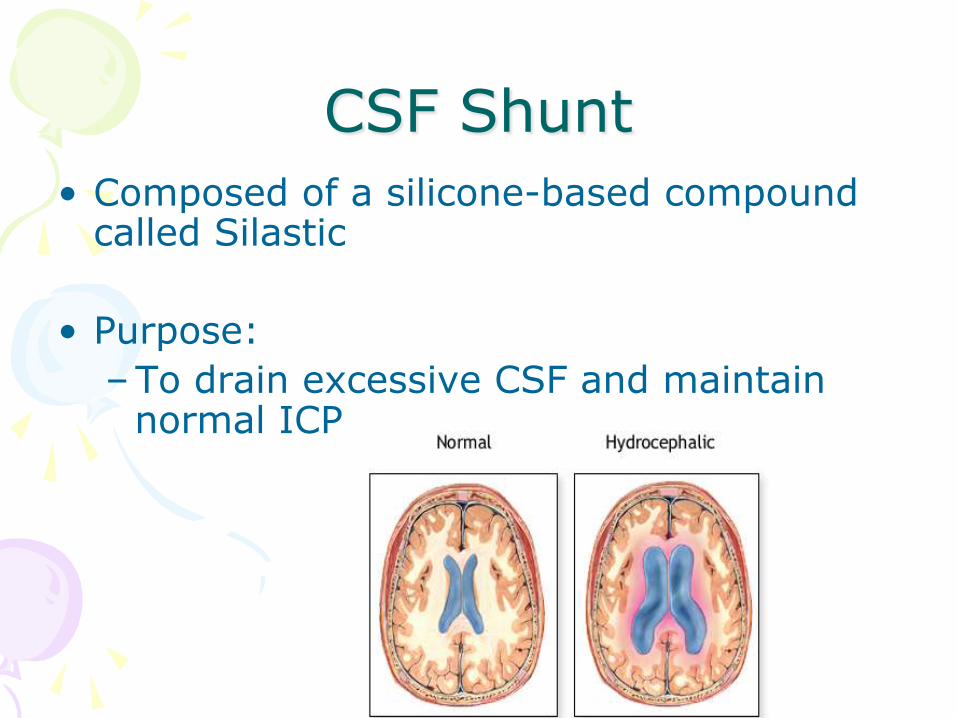
CSF Shunt • Composed of a silicone-based compound
called Silastic
• Purpose: – To drain excessive CSF and maintain
normal ICP
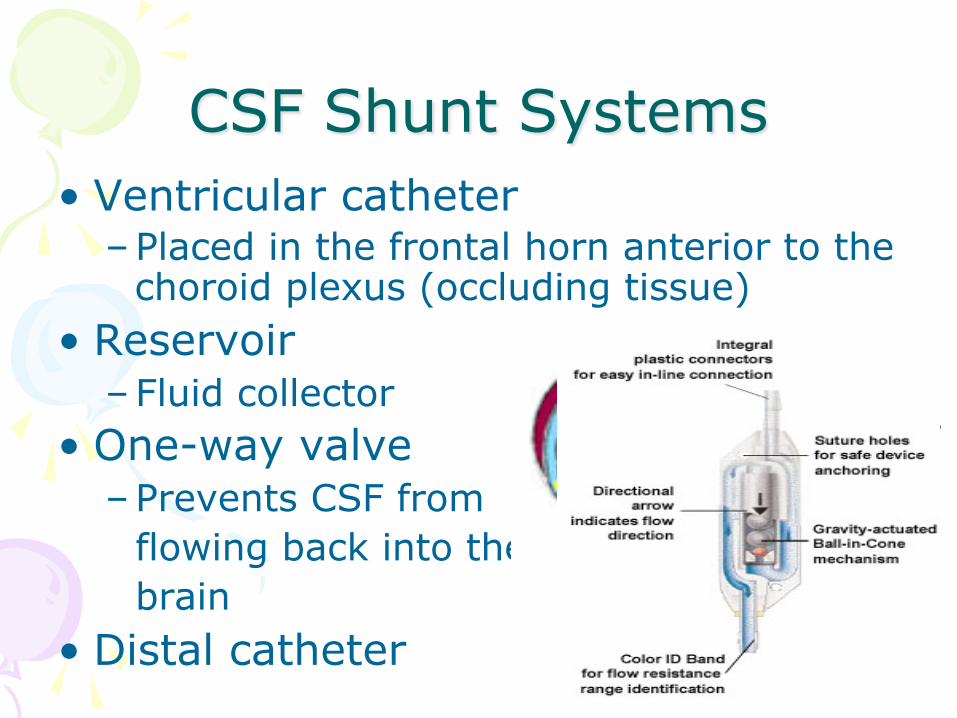
CSF Shunt Systems • Ventricular catheter
– Placed in the frontal horn anterior to the choroid plexus (occluding tissue)
• Reservoir – Fluid collector
• One-way valve – Prevents CSF from flowing back into the brain
• Distal catheter

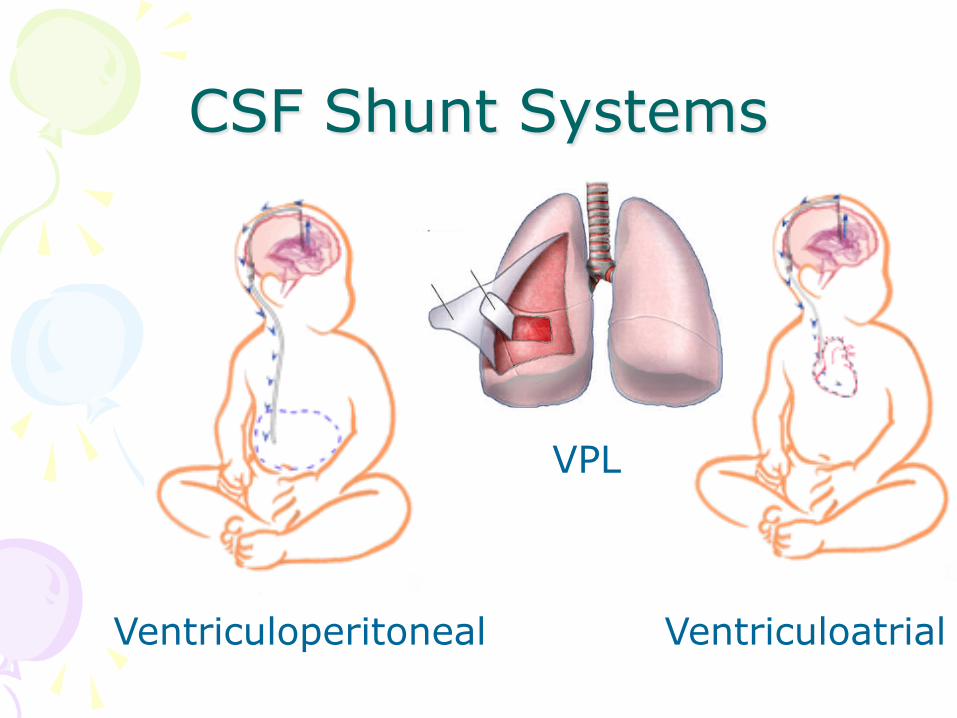
CSF Shunt Systems
Ventriculoatrial
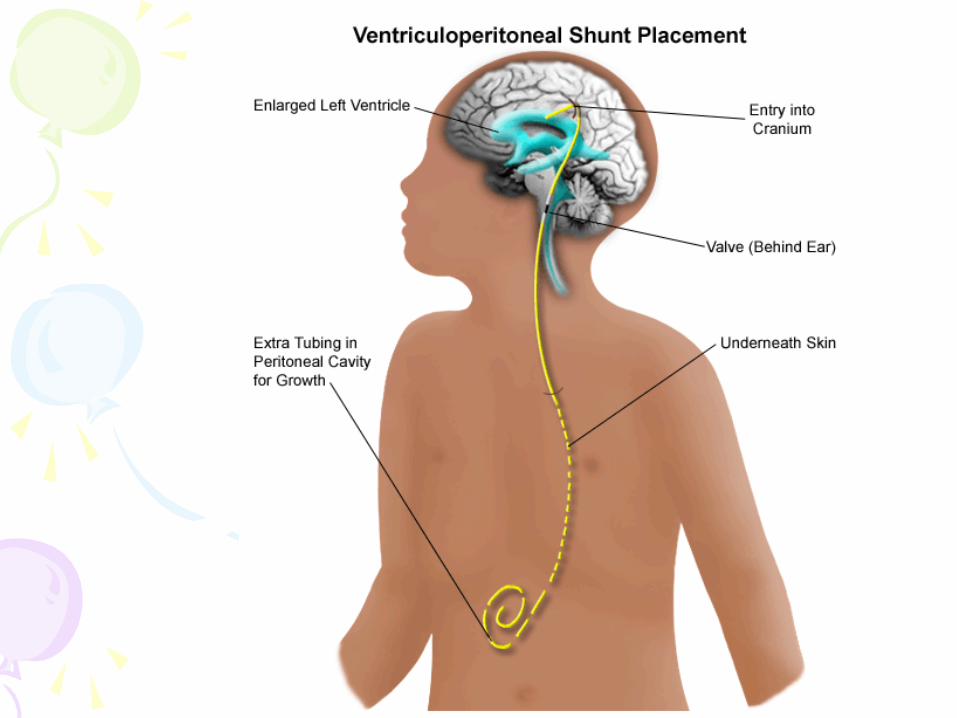
Ventriculoperitoneal
VPL
Shunt Complications • The risk of shunt occlusion is
greatest in the first few months following placement, ranging from 25-40% in the first year.5
• By 5 years following initial
placement, 50% of shunts will fail and require revision.5
Shunt Complications • Shunt obstruction
– Proximal end most common
– VA: thrombus – VP: peritonitis
• Shunt disconnection/fracture
• Infection
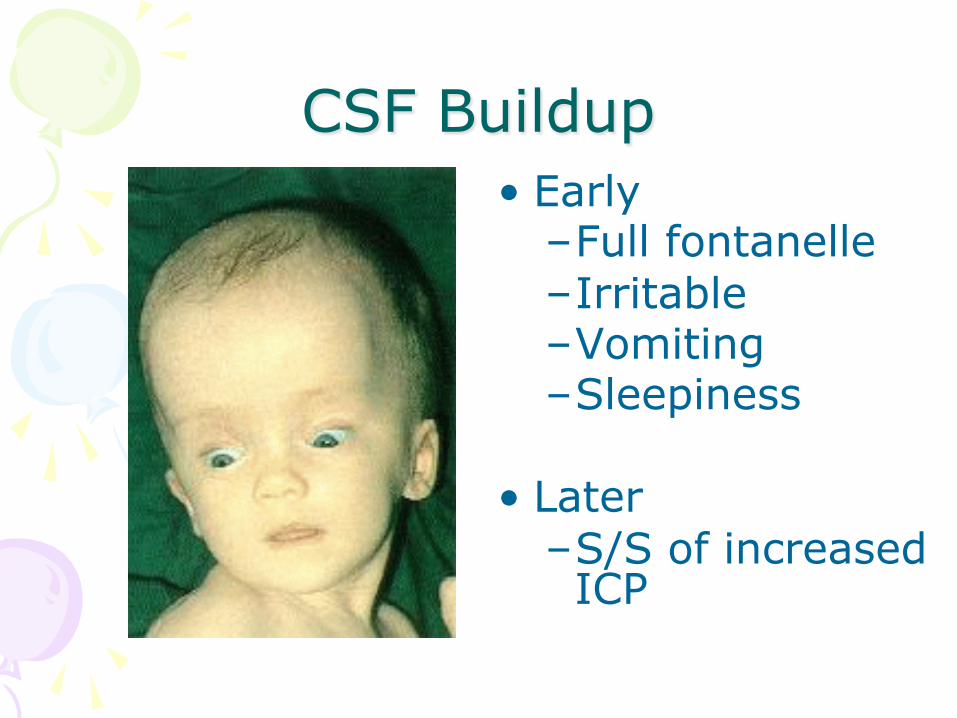
CSF Buildup • Early
– Full fontanelle – Irritable – Vomiting – Sleepiness
• Later – S/S of increased ICP
All children with shunts that present
with vomiting or decreasing LOC are
considered to have a shunt dysfunction
until proven otherwise by
radiologic evidence!
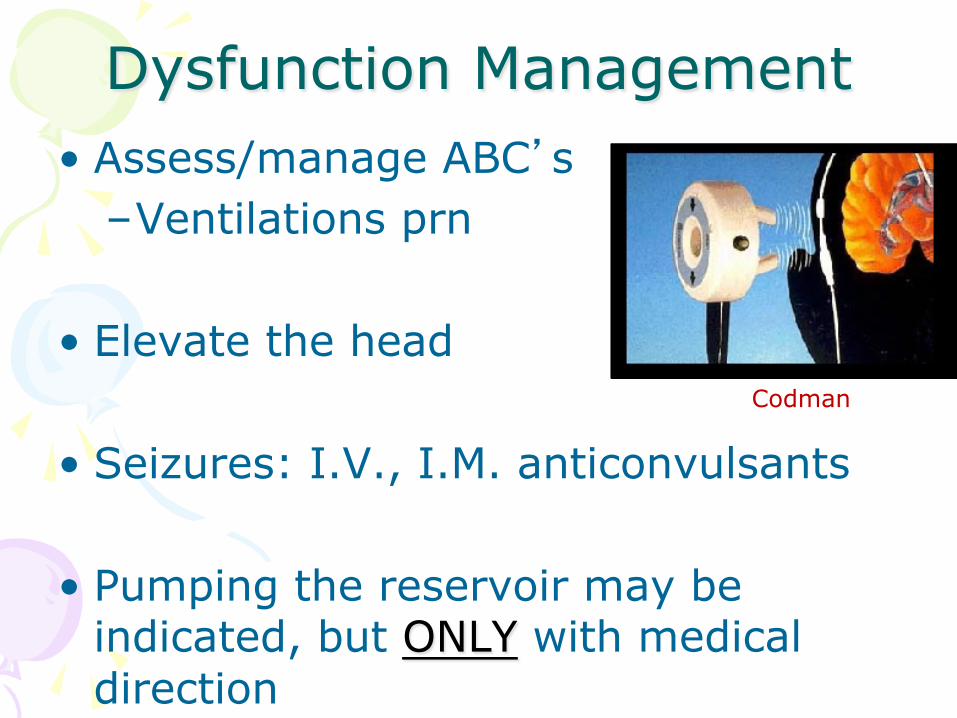
Dysfunction Management • Assess/manage ABC’s
– Ventilations prn
• Elevate the head
• Seizures: I.V., I.M. anticonvulsants
• Pumping the reservoir may be indicated, but ONLY with medical direction
Codman
Central Intravenous
Catheters
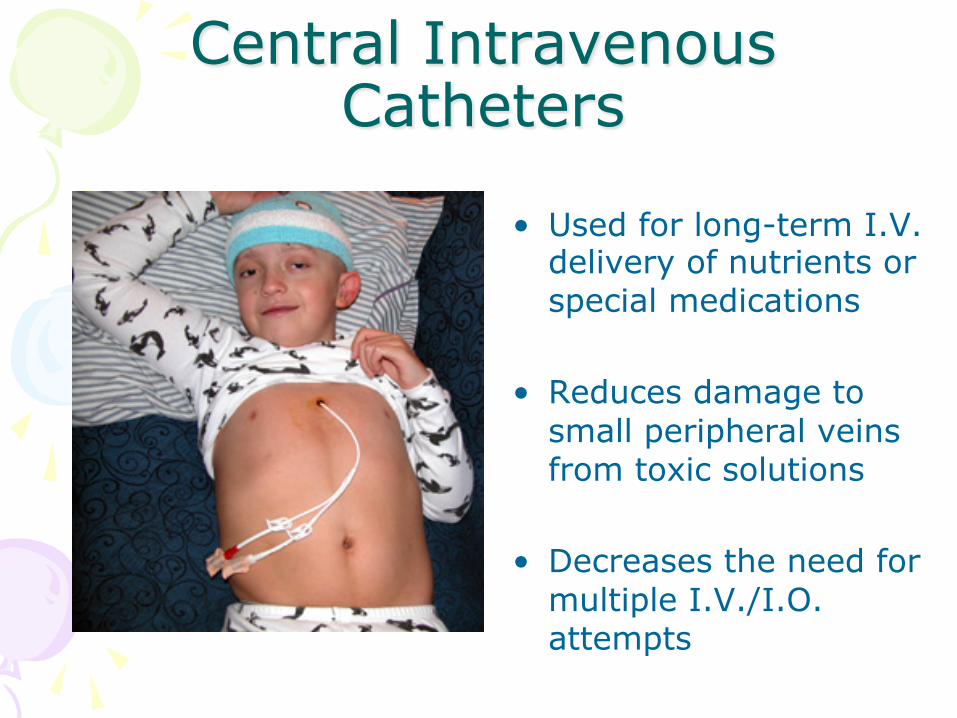
Central Intravenous Catheters
• Used for long-term I.V. delivery of nutrients or special medications
• Reduces damage to small peripheral veins from toxic solutions
• Decreases the need for multiple I.V./I.O. attempts
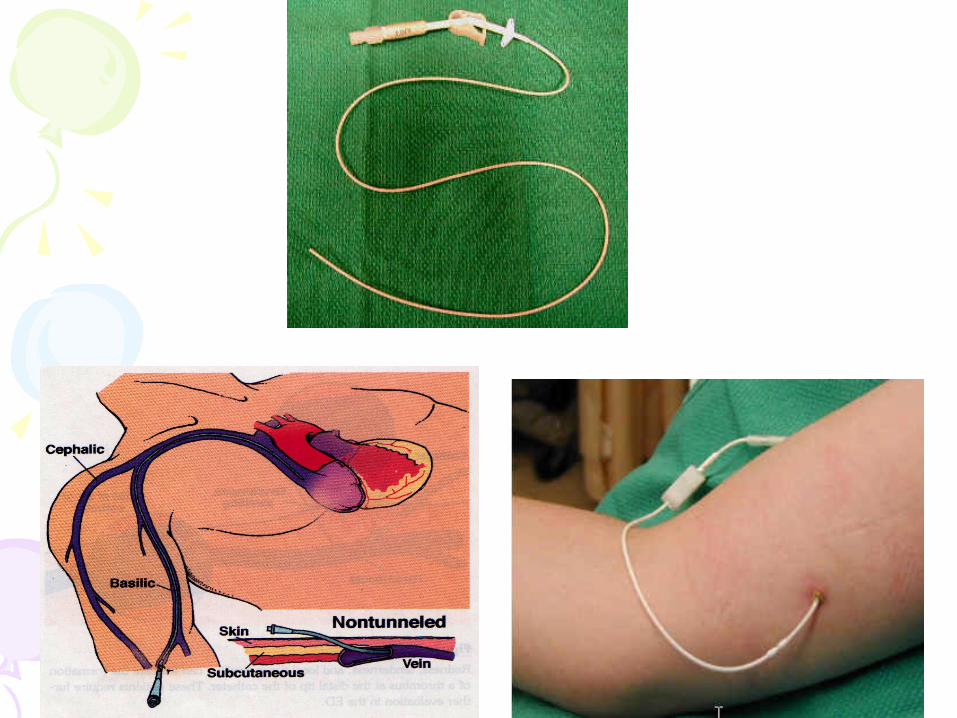
Peripherally Inserted Central Catheters
• Small flexible catheter inserted into a peripheral vein then threaded so that its tip is positioned in a central location
• Best suited for treatments lasting from several weeks to 6 months requiring frequent access to veins
• Flushed once/day with heparin
PICC Considerations • Do not use a tourniquet or B.P. cuff
on same arm
• If needed, clamp the extension tubing, not the PICC tubing
• If you have to flush or aspirate, use at least a 10 ml syringe
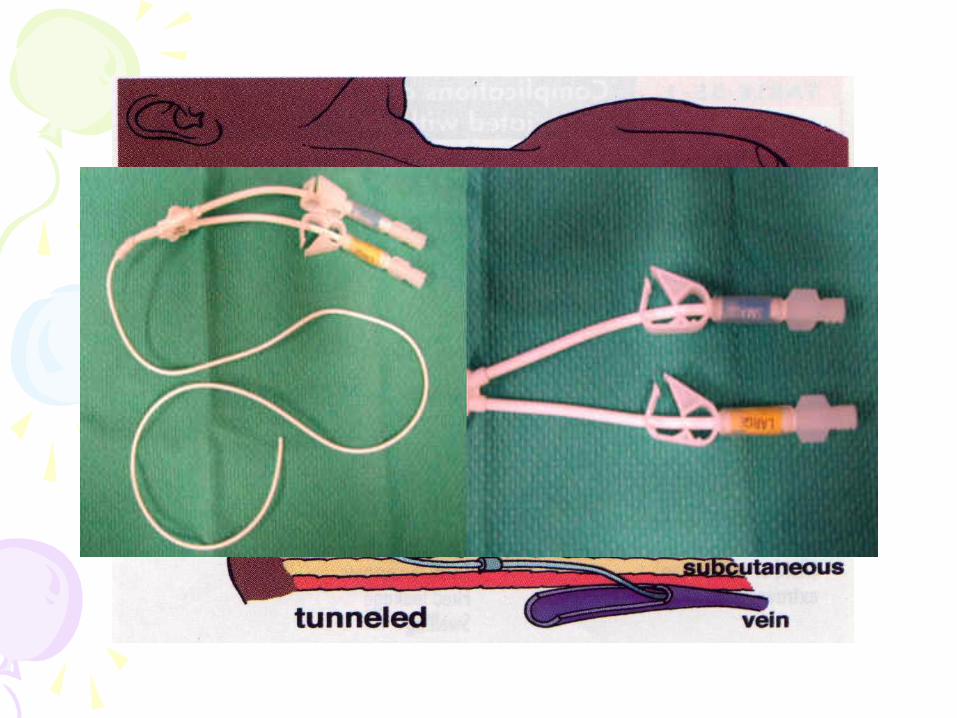
Partially-Implanted CVC’s • Single/Multiple Lumen Catheter
(HickmanTM or BroviacTM ) – Very common – Heparin is used to keep the line patent – Has a clamp that is closed when CVC is
not in use – Multiple lumen devices
• Incompatible medications • Can access any port
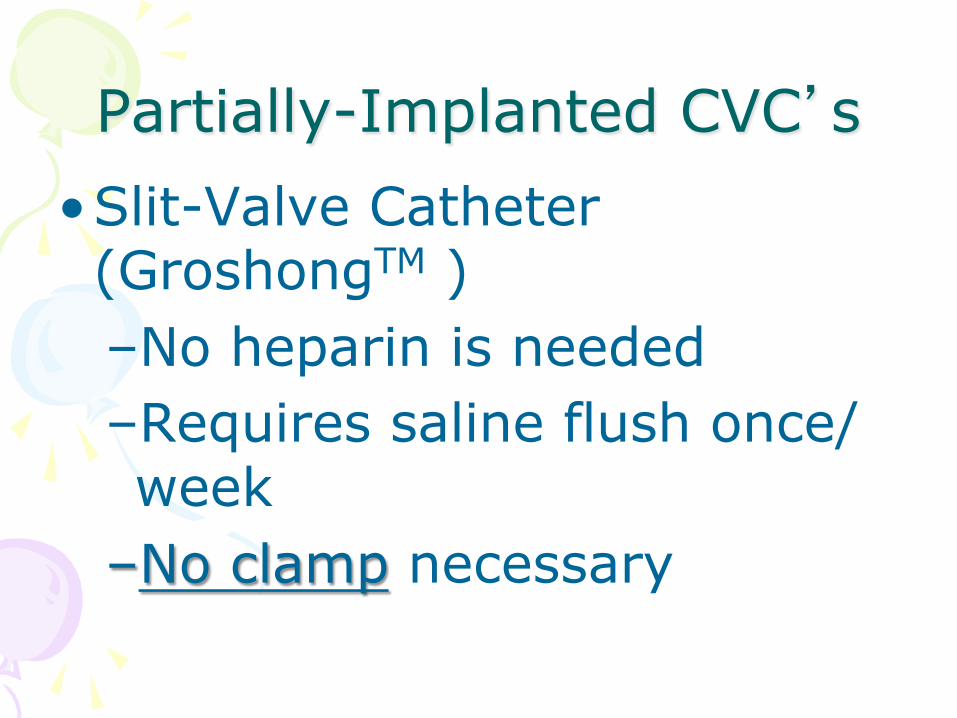
Partially-Implanted CVC’s • Slit-Valve Catheter (GroshongTM ) – No heparin is needed – Requires saline flush once/week
– No clamp necessary
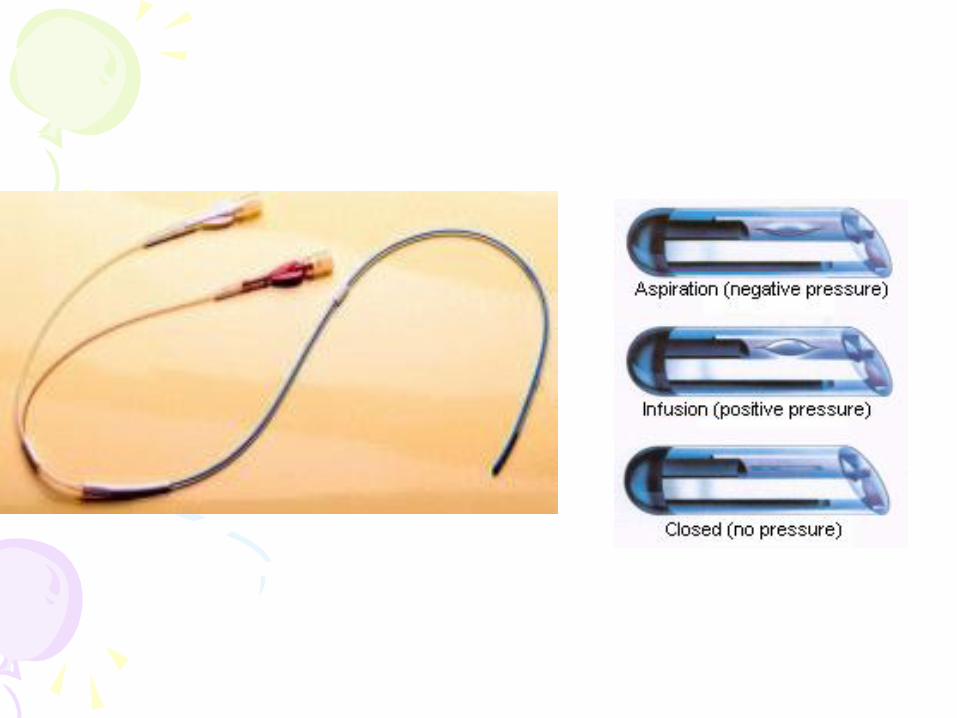
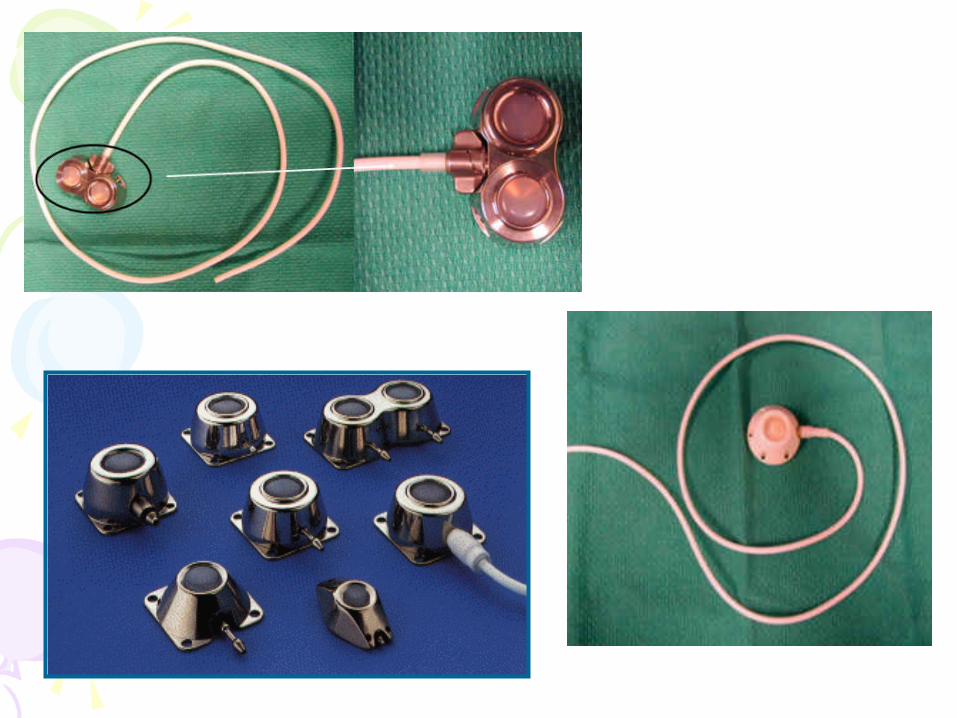
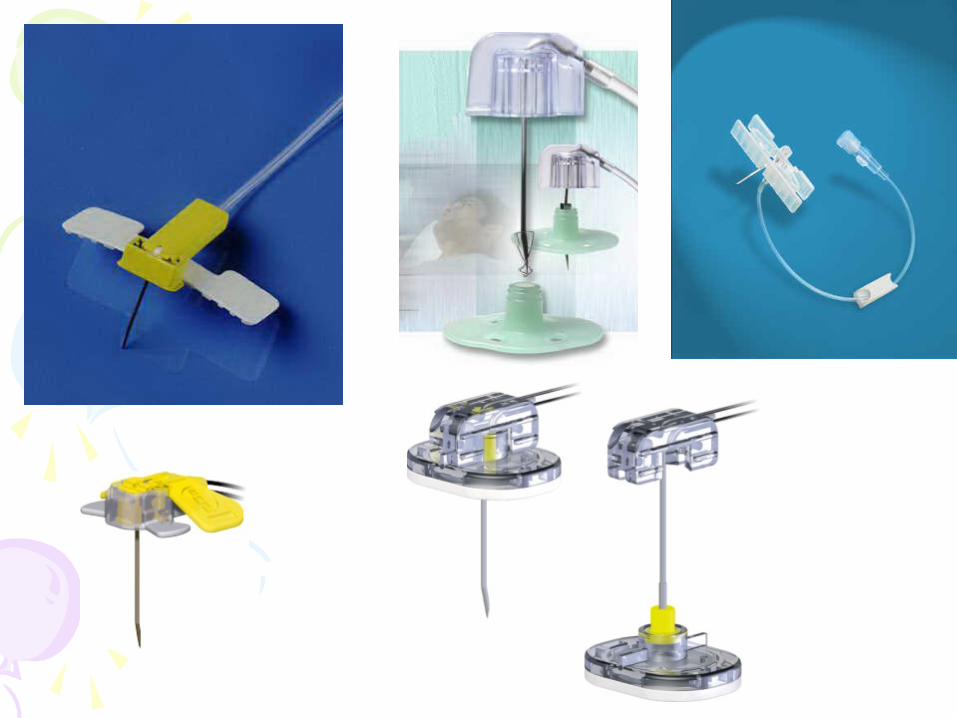
Implanted Vascular Access Ports
• Port-a CathTM MediPortTM PASPortTM
• Totally-implanted under the skin • Has a self-sealing heparinized
reservior • Accessed by Huber needle
4
CVC General Assessment • Use sterile dressings whenever possible
• Check the catheter site/bleeding
• Look for local infection
• Inspect the external portion of the catheter/air embolism
• Evaluate for dehydration/lack of flow

Thank You, Florida !
Christopher Ebright B. Ed., NRP
EMS Education Coordinator
National EMS Academy Covington, LA
@chrisebright69
Resources 1. Reynolds S, Desguin B, Uyeda A, et al. Children with chronic
conditions in a pediatric emergency department. Pediatr Emerg Care. 1996;12:166-8
2. Newacheck P, McManus M, Fox H, Hung Y, Halfon N. Access to health care for children with special health care needs. Pediatrics. 2000;105:760-6.
3. McPherson M, Arango P, Fox H, et al. A new definition of children with special health care needs. Pediatrics. 1998;102:137-40
4. Seng, M., Karriker, K. Meeting the Challenge: Improving Emergency Medical Care for Children with Special Health Care Needs, The University of Arizona College of Medicine, Tuscon, AZ, 1999
5. Hudgins, R.J., Boydston, W.R., Introduction to Shunt Complications. Childrens Healthcare of Atlanta, 2007; www.choa.org/
Resources • http://www.health.state.ny.us/nysdoh/ems/
ppcctoc.htm • http://www.cpem.org/html/giflist.html • http://www.tracheostomy.com/images/trach1.gif • http://www.fsma.org/equiplist/250.jpg • http://www.tracheostomy.com/misc/bipap.htm • http://stevenbell.blogspot.com/images/steven-
hickman.jpg • http://www.cvtoolbox.com/cvtoolbox2/
card_proced/supports/aicd.jpg • http://www.clevelandclinic.org/heartcenter/pub/
guide/disease/congenital/pfo.htm • http://www.kumc.edu/instruction/medicine/
pedcard/cardiology/pedcardio/pdadiagram.gif • http://www.sinoaf.co.ug/images/l-images/s_catheter.jpg
Resources • http://www.unverse.com/WizardOz.html • http://www.lessonsfromoz.com/images/gallery/
tin-man.jpg • http://blogs.zdnet.com/images/scarecrow.jpg • http://www.choa.org/default.aspx?id=909 • http://www.dcyf.ri.gov/special_foster_care.php • http://www.flare.net/specialhealth/ryan.jpg • http://www.cincinnatichildrens.org/svc/alpha/c/
special-needs/resources/technology.htm • http://www.azdhs.gov/phs/ocshcn/
education_advocacy/medicalhome_az.htm • http://www.standingdani.com/images/
boyanddog.jpg • http://www.p2p-co.org/images/liam2b.jpg
Resources • http://www.travelblog.org/Photos/274216.html • http://jkmoore.ath.cx/weblog/images/
funny_faces_both_kids.jpg • http://www.ahoffman.com/humor/images/A0000011.jpg • http://www.mirarr.net/gallery/kids/kids4-big.jpg • http://www.greenhill.org/evergreen/images/Story
%20Images/2005-2006/September/Special%20Section/kids-learn-play-ease-stress.jpg
• http://www.wpcv.com/images/kids-will-play.gif • http://www.nwpublichealth.org/docs/wph/needs.html • http://www.cerebromente.org.br/n02/fundamentos/
ventriculos_i.htm • http://www.pennhealth.com/health_info/Surgery/
ventriperishunt_2.html • http://www.tracheostomy.com/surgery/tracheostomy/
trach5.jpg
Resources • http://images.webmd.com/images/hw/media69/medical/
hw/nr551434.jpg • http://www.cardiva.biz/products/p067-1.gif • http://www.drexelmed.edu/documents/neurosurgery/ped/
Spina_Bifida/sld017.htm • http://www.braintumor.org/pservices/images/shunt.jpg • http://www.bcchildrens.ca/Services/SurgeryAndSurgSuites/
GeneralSurgery/TubeFeeding/TypesOfTubes/ • http://www.isips.org/Safety_Huber_Needle.html • http://rds.yahoo.com/
_ylt=A9ibyGaSDOdFrFYBm3CjzbkF;_ylu=X3oDMTBsMW5yM3VoBHNlYwNwcm9mBHZ0aWQDSTA2Nl84OA--/SIG=11rpjo9cs/EXP=1172856338/**http%3A//www.picclines-sat.com/serv01.htm
• http://www.aftonmedical.com/trach_masks.htm • www.tracheostomy.com