Embed Size (px)
Citation preview
Towards universal, comprehensive and equitable National Health Systems: The 20 Years Brasilian Experience in its context
Dr. Armando De Negri [email protected]
PHM – Brasil / World Social Forum on Health / International Society for Equity on Health
Cairo IPHU Short Training Course – March 23, 2008

People - Human Rights - Centered Health Systems
X
Market driven health services – (systems?)

The basis of the political debate around the human rights approach for health, generating a
political movement and its conquests…The indivisible triad for the right to health: • Universality means for every person during the entire life• Comprehensive means all individual and social needs all
life long – means to achieve the integral / full answer to the needs derived from the interdependent rights understood as a system / all necessary to make rights real
• Equity means social justice achieved trough the warranty of all people rights on time for their needs, with no differences to who have the same needs. It implies the equity on the access to the resources on policies, its financing, its services, quality of care and the health and social results of its application.

EQUITY…• The equity approach does not establish the
“minimum” but generates the tension between the the necessary (what is fair, just, the right) for everybody and the already possible for some individuals or groups (the privileges)…
• The very illustrative example of the crossed subsides and the per capita inequities…
• Inequities as the distance of each group in relation to the desirable fair / right, and the intolerable differences between groups in relation to the desired standard of the rights achievement

The good, for all, the fair, the desirable as an expression of the logic and doctrine of the social and human rights – “the reasonable”
A
B
C
Distance towards what is good, fair, desirable
Inequities among groups
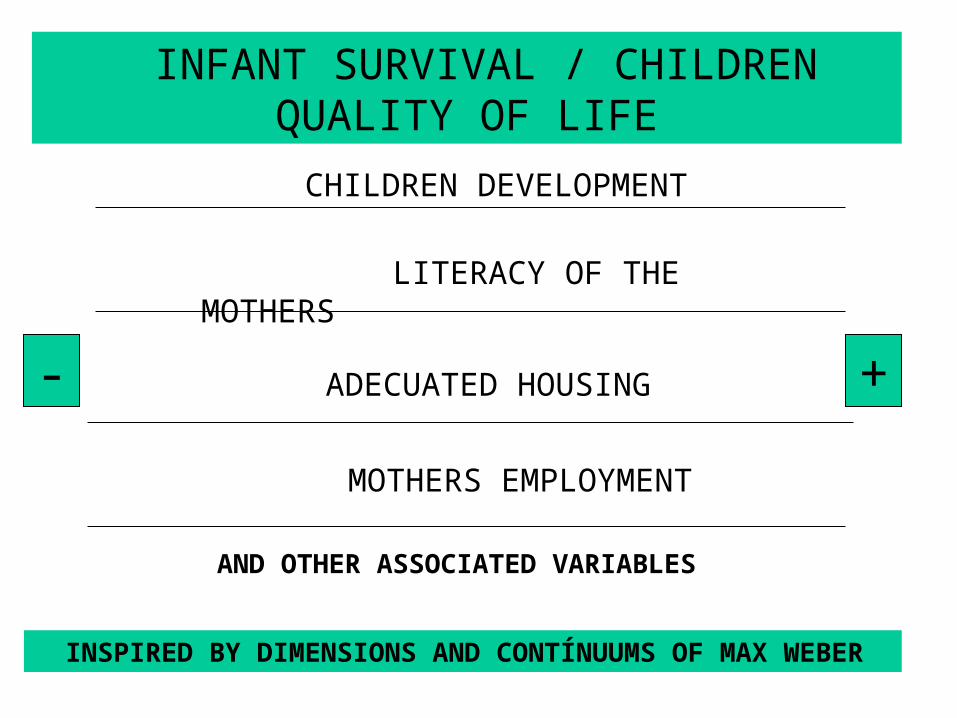
CHILDREN DEVELOPMENT
LITERACY OF THE MOTHERS
ADECUATED HOUSING
MOTHERS EMPLOYMENT
+-- +
INSPIRED BY DIMENSIONS AND CONTÍNUUMS OF MAX WEBER
INFANT SURVIVAL / CHILDREN QUALITY OF LIFE
AND OTHER ASSOCIATED VARIABLES
0
0,5
1
1,5
2
2,5
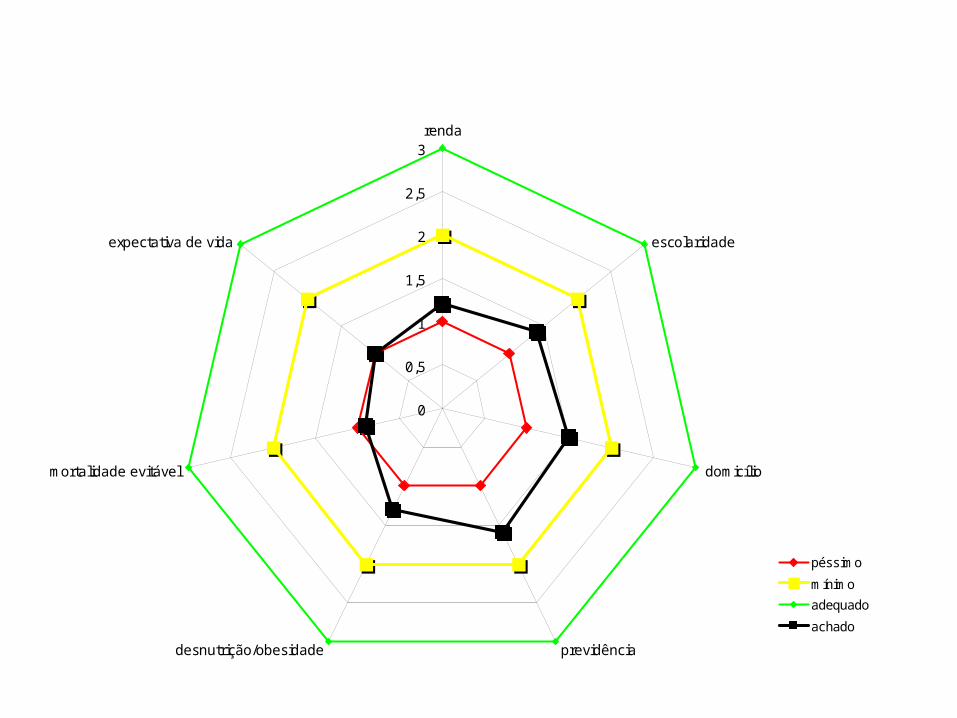
3renda
escolaridade
domicílio
previdênciadesnutrição/obesidade
mortalidade evitável
expectativa de vida
péssimo
mínimo
adequado
achado
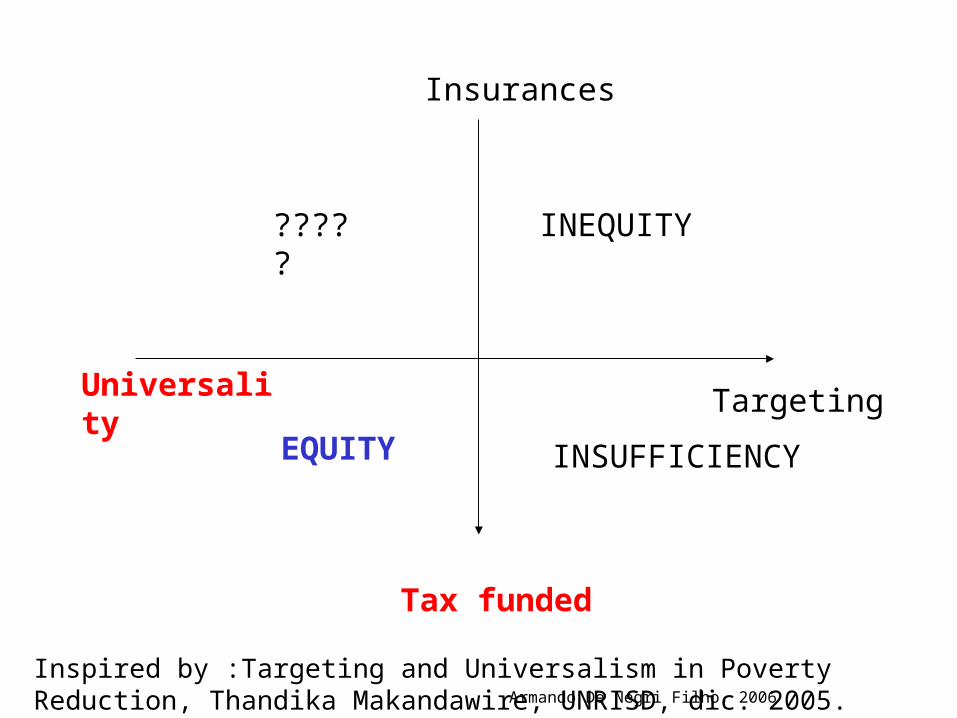
Tax funded
Universality Targeting
Insurances
INEQUITY
EQUITY
Inspired by :Targeting and Universalism in Poverty Reduction, Thandika Makandawire, UNRISD, dic. 2005.
INSUFFICIENCY
?????
Armando De Negri Filho, 2006
• According to Dr. Tandika the concern with “efficiency” of the public systems increased at the same time that the redistributive justice and social development concerns are reduced or disappeared.
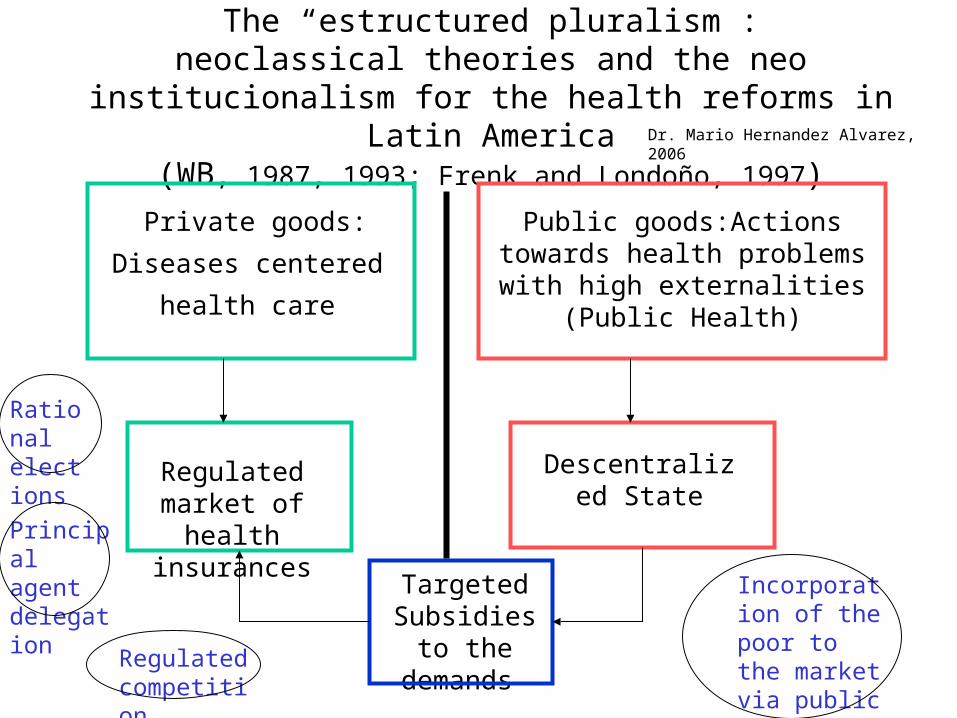
The “estructured pluralism”:neoclassical theories and the neo institucionalism for the health
reforms in Latin America(WB, 1987, 1993; Frenk and Londoño, 1997)
Private goods:
Diseases centered
health care
Public goods:Actions towards health problems with high
externalities (Public Health)
Regulated market of health
insurances
Descentralized State
Targeted Subsidies to the demands
Rational electionsPrincipal agent delegation
Regulated competition
Incorporation of the poor to the market via public / state assistance
Dr. Mario Hernandez Alvarez, 2006
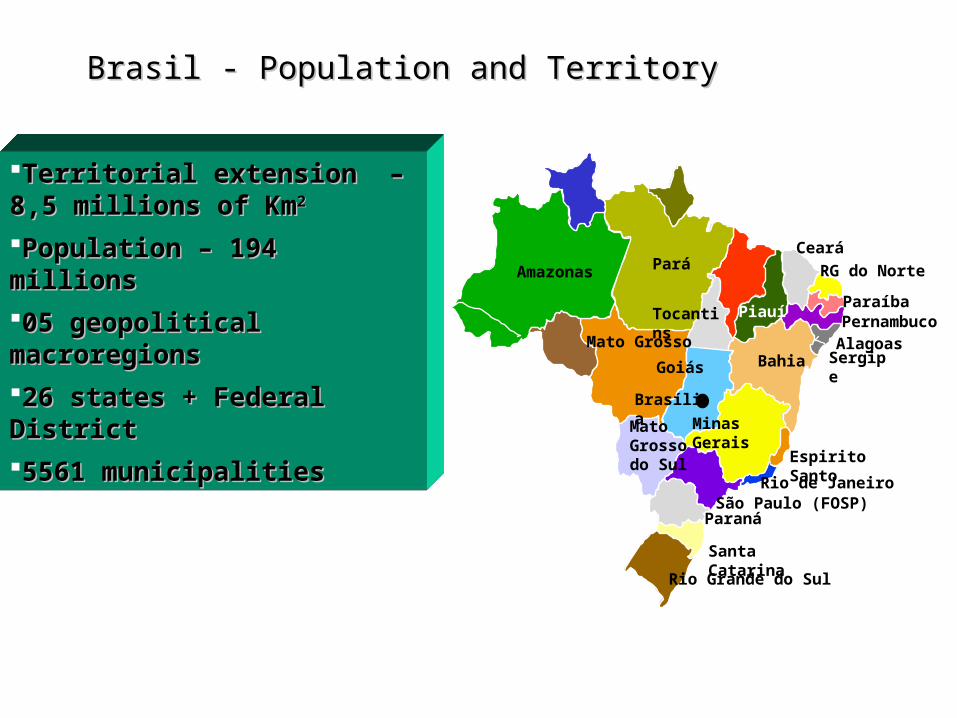
Territorial extension Territorial extension – 8,5 – 8,5 millmillionsions ofof Km Km22
PoPopulation pulation – – 194194 mill millionsions
05 05 geopolitical geopolitical macroregions macroregions
26 26 statesstates + Federal + Federal District District
5561 munic5561 municipalitiesipalities
Rio Grande do Sul
ParanáSão Paulo (FOSP)
Rio de Janeiro
Goiás Bahia
Pernambuco
RG do Norte
CearáPará
Santa Catarina
Tocantins
Espirito Santo
Alagoas
Brasília
Minas Gerais
PiauíParaíba
Amazonas
Mato Grosso
Mato Grosso do Sul
Sergipe
Brasil - Brasil - PoPopulation and Territorypulation and Territory

The Brazilian Experience in the conquest of the Human Right to Health
• The formulation of a concept and its political intention – the brazilian social health reform as the expression of the struggle for health as a right of every woman and man in the country
• The conquest of a new concept to order the health system – trough a political mobilization motivated by the insatisfied needs of the population regards their fundamental rights
• Political achievements at the VIII National Health Conference in 1986 and the New National Constitution adopted in 1988

The SUS (Unique Health System)
• 1988 National Constitution: “Health is a right of everyone and the duty of the State”
• The SUS: ensemble of policies, services and actions that are developed by state institutions of the three levels of government – national, regional and local, with complementary participation of the private sector – composing a public organization oriented to fulfill the universal right to health with comprehensiveness and equity.
Public Dimension composed by:
1 - State owned structures
2- Non profit private and private for profit
Ordered by public contracts
The principles of the SUS
• Universal access;• Comprehensive care;• Equality on access and quality of care;• Social and community participation with
decision power;• Descentralization of the system
management with exclusive direction at each level of government.

Our experience in this process:
• The Federal Constitution of 1988 and the Organic Laws of 1990:
• Law 8080 of 1990, establish the definitions of an unique national health system in order to warranty the organization of an unique national public health system to make real the universality, the comprehensiveness and the equity in terms of health for all population, establishing the public orders that will discipline the private activities – building the public esphere composed by the state owned services and the private services, oriented by the constitutional public relevance that health has achieved nationally and internationally
Our experience in this process:
• The organic law 8142/90, establish the creation and the implementation of the health councils, and the conferences,
• The councils are health decision making bodies at each level of the republic: national, regional / states and local / municipalities.
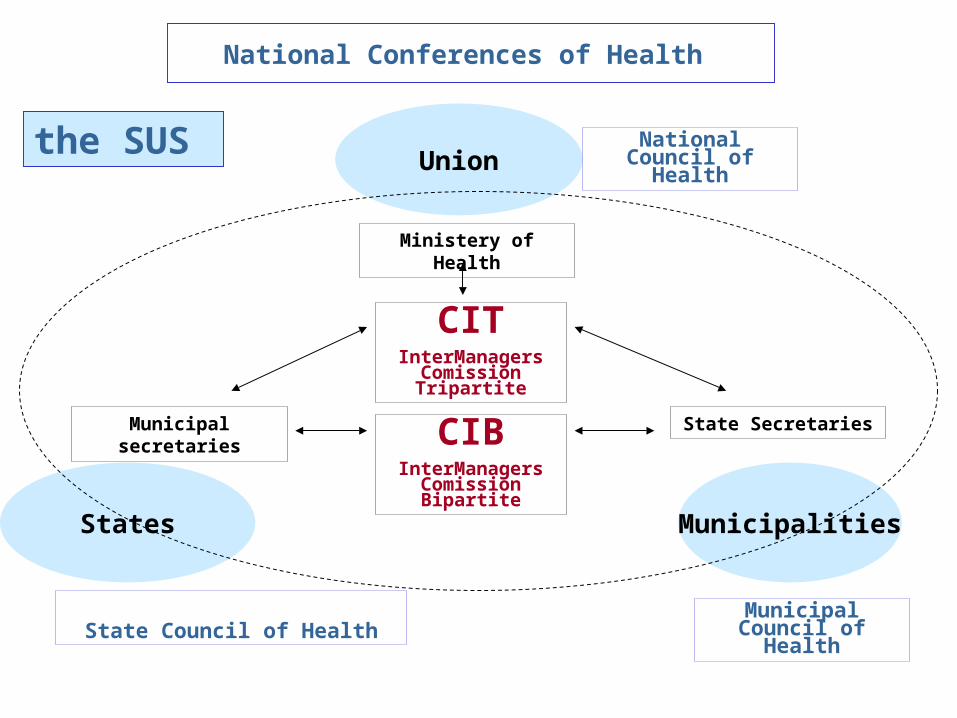
Union
States Municipalities
Ministery of Health
State SecretariesMunicipal secretaries
CITInterManagers
Comission Tripartite
National Council of Health
State Council of HealthMunicipal Council of
Health
National Conferences of Health
CIBInterManagers
Comission Bipartite
the SUS
Our experience in this process:• The radical descentralization – as radical
democratization - towards the municipalities – NOB 93
• The creation of the intergovernment agreement bodies – Primary Health Care minimun value transfer - NOB 96
• In search of the financing estability – CPMF and constitutional amendement 29 (2000), towards its regulamentation (2008)
• The struggle for enough financing support and the human resources on health.
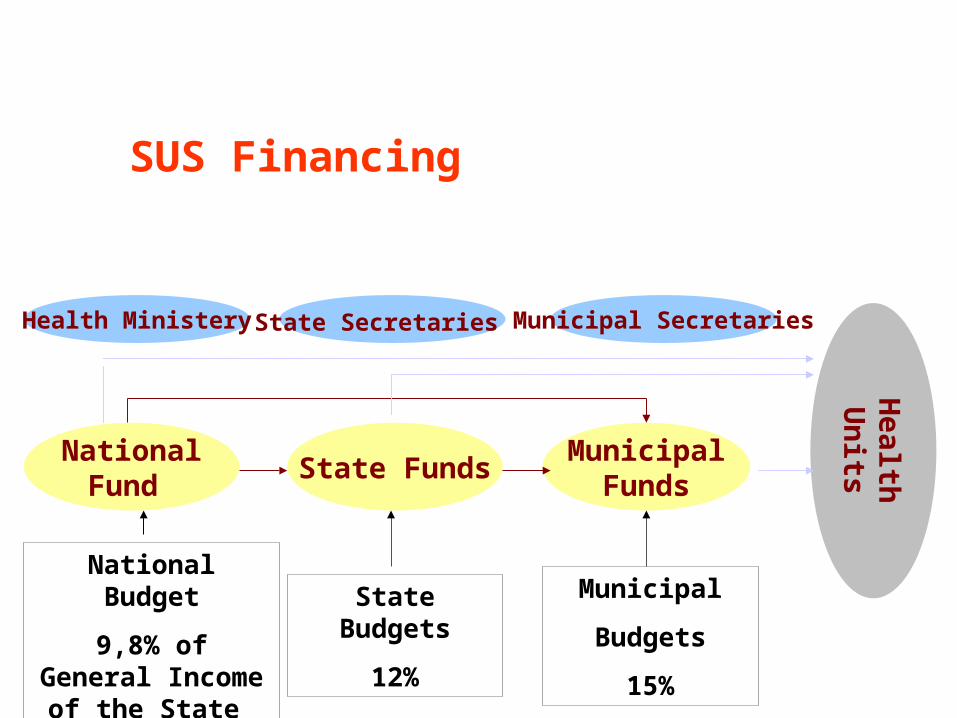
SUS Financing
NationalFund
State FundsMunicipal
Funds
Health Ministery State Secretaries Municipal Secretaries
National Budget
9,8% of General Income
of the State
State Budgets
12%
Municipal
Budgets
15%
Health
U
nits

• The State is the rector, financer, regulator and
provider.
• Regular and automatic transference of financial
resources among the health funds.
• Totally free care, financed by the global tax
income of the State.
• **Public Expenditure is 50% of the total health
expenditure, around 160 dollars per capita / per
year`. 3,7 % of the GNP.
Our experience in this process:• Today the system is already installed in all the
5561 municipalities, where there are health local authorities and health councils, as well as health plans established.
• There are health goals established and compromises of accomplishment, public accountability exercises each three months and transparency trough a web system - SIOPS.
• There is a daily struggle to keep and perfeccionate the System as an integral health care system.
Per year / year base 2006
1 bill1 billioion n of procedures of primary health careof procedures of primary health care
251 mill251 milliions ons of clinical lab testsof clinical lab tests
8,1 mill8,1 milliions ons of ultrasound examinations of ultrasound examinations
132,5 mill132,5 milliions ons of high complexity careof high complexity care
140 millions of vaccines applied140 millions of vaccines applied
150 mil persons receiving ARTV150 mil persons receiving ARTV
Sistema Único de SaludSistema Único de Salud
GENERALGENERAL DATA ABOUT THE OUPATIENTS CARE IN THE DATA ABOUT THE OUPATIENTS CARE IN THE SUSSUS
63.650 Ambulatory Units that produced in average of 153 millions of medical care per year
Per year / year base 2006
2,6 millions of child deliveries
83.000 cardiac surgeries
60.000 oncological surgeries
GENERALES GENERALES DATA ABOUT INPATIENT CARE IN THE SUSDATA ABOUT INPATIENT CARE IN THE SUS
5.794 Hospitals / 441.045 hospital beds/ 900 thousand patients are admitted per month/ 11,7 millions of admissions per year
92.900 varices surgeries
23.400 organ transplantations
Sistema Único de Sistema Único de Saude Saude SUSSUS
FONTE: SIAB - Sistema de Informação da Atenção Básica
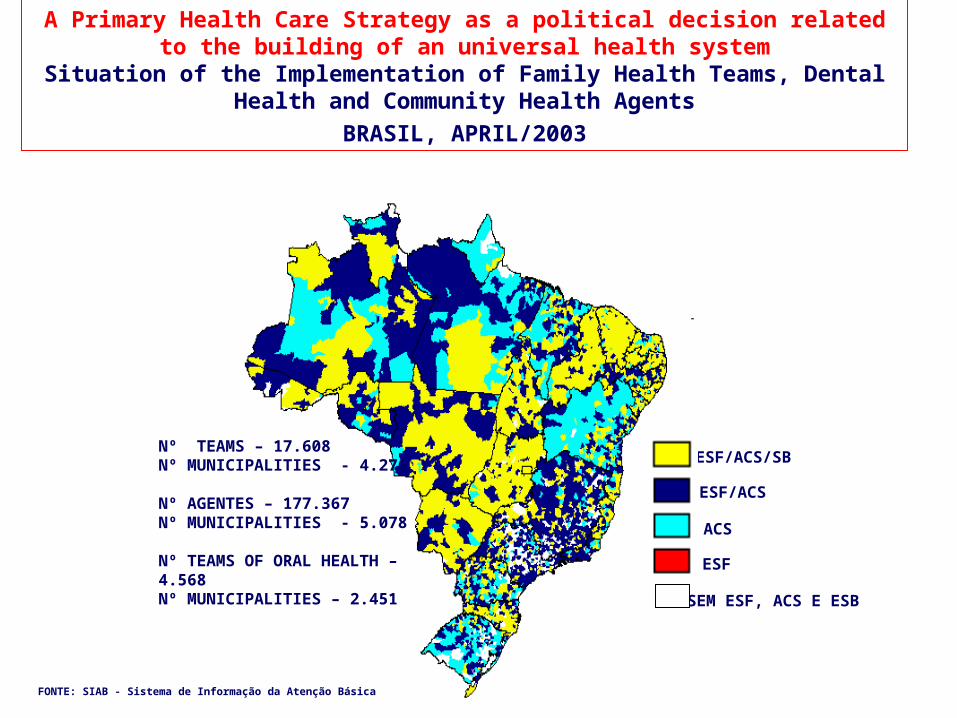
A Primary Health Care Strategy as a political decision related to the building of an universal health system
Situation of the Implementation of Family Health Teams, Dental Health and Community Health Agents
BRASIL, APRIL/2003
Nº TEAMS – 17.608Nº MUNICIPALITIES - 4.276
Nº AGENTES – 177.367Nº MUNICIPALITIES - 5.078
Nº TEAMS OF ORAL HEALTH – 4.568Nº MUNICIPALITIES – 2.451
ESF/ACS/SB
ACS
SEM ESF, ACS E ESB
ESF
ESF/ACS

Evolution of the Number Family Teams ImplementedBRASIL - 1994 – ApRIL/2003
0
5.000
10.000
15.000
20.000
25.000
META REALIZADO
META 328 724 847 1.623 4.000 5.000 10.500 17.000 20.000 21.000
REALIZADO 328 724 847 1.623 3.083 4.254 8.604 13.168 16.698 17.608
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
FONTE: SIAB - Sistema de Informação da Atenção Básica
ESF

“Family Health” a Comprehensive Primary Health Care Strategy
Figures of 2007• 28.000 teams with a full time team: medical
doctor, nurse, 1-2 auxiliary nurses , 4 to 6 community health agents for each 800 to 1200 families.
• 235.000 community health agents• 14 thousand teams of dental care (dentistry
professional, dental technician and a dentistry consultant assistant) at more than 5000 municipalities with 476 specialized centers

National Network for Emergencies Health Care
• At march 2007:– Pre Hospital Care began 2003 – Now there are 113 emergency medical regulatory
centers that make medical coordination 24 hours a day– 1358 ambulances ( 360 for Advanced Life Support with
MD)– 92.539.000 inhabitants covered – 925 Municipalities covered
– Humanization of 120 hospital emergency services
Pharmaceutical Assistance
• List of Essential Drugs for free provision for a patients doing follow up at the PHC and beyond
• Popular Drugstore / commercial establishments convened / prices control
SUS – next steps and its challenges
• Financial stability and sufficiency• Human resources profiles and economical
sustainability • New health care mode – promotional
strategy – a possible pathway – universal, comprehensive and equitable answer to the social (health) needs of the people / needs derived from the human and social rights
Structuring Project on Equity in the Quality of Life and Health of the Childhood
Structuring Project on Equity in the Quality of Life and Health of the Teenagers and Youth
Structuring Project on Equity in the Quality of Life and Health of the Adults
Structuring Project on Equity in the Quality of Life and Health of the Elderly
**By Social Classes and its Social Territories **By Genders
**By Ethnics
Four Structuring Projects
**with three transversal perspectives
SOCIAL LIFE ITINERARY OR VITAL CYCLE
Territories or social classes Sex or genders
Ethnics and Races

SPEQLH - CH
SPEQLH TEEN/YOUTH
SPEQLH - ELDERLY
ADP-CDD
ADP-IPD
ADP-SRH
ADP-INJURIES
ADP-MH
ADP - ORAL
Transversal Project on Autonomy Development
Physical Activity Nutrition/Food Security
Adictions
Discapacities
Ocupation
Environments
ZeroVision
SPEQLH - ADULTS

ZERO VISION AS INTERNATIONAL STANDARD
NATIONAL STANDARD
BEST GROUP STANDARD
BEST INTERNAL OR LOCAL STANDARD
DYNAMICS OF ZERO VISION
Progressive answer to the deficits and gaps
Government and social movements agendas
SOCIAL NETWORKS

Especific exposures
Disease, injury or damage
Social and EconomicalConsequences of the health –disease process
Social Estratification (I)
Influences over the estratification (A) Social
Position
Reducing the social exposures (B)Acces to public systems and services
Reducing the frailty (C) damage and illness prevention / health protection
INDIVIDUALS SOCIETY
Social Context
Political Context
Preventing inequities on the social consequences of the damages or diseases / injuries (D) Disease Treatment / Social Protection
Impacts on Social Estratification(I)
Differential frailty III
Differentials
on
consecuences IV
Adapted by Armando De Negri Filho from the original of Diderichsen and Hallqvist - 1998
Differential
Exposition II
Mechanisms that act in the stratification of the health achievements
Entrance points of the state or public policies
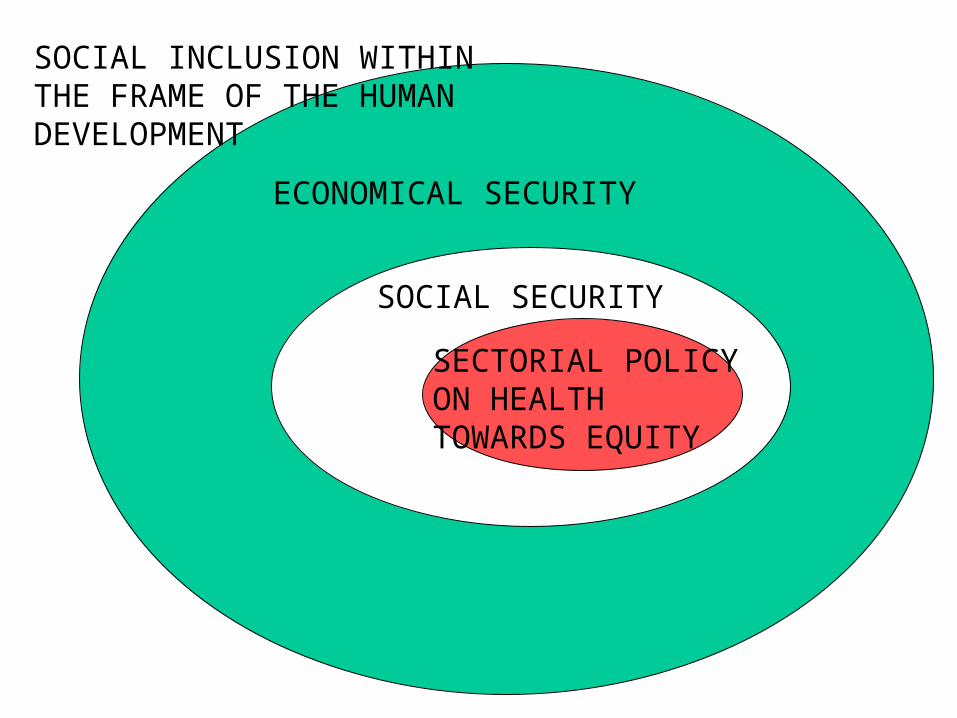
SECTORIAL POLICY ON HEALTH TOWARDS EQUITY
SOCIAL SECURITY
ECONOMICAL SECURITY
SOCIAL INCLUSION WITHIN THE FRAME OF THE HUMAN DEVELOPMENT
Necessary impact at 5 fronts of social inclusion:• -with universalistic public policies as in the case of health,
education and social security as a protection against inequities and against the loss of opportunities.
• -at the taxes policies in order to be progressive - fair• -at the transference of richness and universal income• -at the strenghtening of the participative democracy and
the democratic institucionality• -at the promotion of job quality, safety and income level,
social security inclusion
Comprehensive answers to the radical needs of people as expression of their radical social needs at defined social territories.

World Conference on the Development of the Universal Health and Social Security Systems
• An initiative of the II World Social Forum on Health, as decided in the Thematic Final Plenary of the VII World Social Forum / Nairobi in January 2007
• Host Organization – the National Health Council of Brasil
• Place and date: Brasilia – last week of November 2008

Objectives• 1.To permit a equitable dialogue among governments, parliaments, academic
institutions, intergovernmental agencies and social, popular and labor movements about the development of universal systems as an alternative for countries and regions
• 2.To strength the existing universal health systems through the share of its historical experiences, achievements and challenges
• 3.To stimulate other countries, governments and societies to adopt the universal, comprehensive and equitable systems as a valid and feasible option on the process of the national reforms and the regional integration process
• 4.To develop the necessary approach of the role of universal systems in its relationships with the economical and social development of the countries towards poverty eradication and social justice as equity
• 5.To establish a network of governments, movements and academic institutions motivated to develop the policies, systems and services / actions, technologies and human capacities towards universal, comprehensive and pro-equity in health and social security.
Program Subjects 1/3
• 1. The political/ ethical basis for the assumption and development of universal, comprehensive and pro-equity systems of health and social security – historical background and present rationality – national, regional and international perspectives
• 2. The economical feasibility and the political sustainability of the universal approach – analysis of conceptual frameworks, tax systems and universal and comprehensive insurances with case studies from the various Continents
Program Subjects 2/3• 3. The dynamics of the technological incorporation and
dependency, intellectual property, research patents policy and the sovereignty around the universal systems
• 4. The challenge of the human resources for the development of universal systems – professional profiles, careers and salaries, brain drain, public investment and the educational policies
• 5. The state / private relationship and the building of national and international public goods around the universal systems
• 6. Health and welfare social accountability of the universal systems, relationship with poverty erradication efforts and multidimensional development - achievements and challenges
Program Subjects 3/3• 7. The roles of international aid and cooperation and
humanitarian aid ( north-south, south-south and multilateral, private) and its potentials and compromises regards the development of universal systems
• 8. An international network of governments, social and popular movements and academic centers to support the development of universal systems
• 9. Management challenges and new capacities needed in the development of universal systems
• 10. Democracy strenghtening and protagonic social participation in the development and dynamics of universal systems

GoalsParticipation:• Around 750 participants • From 75 countriesPreparatory meetings already considered:• In Senegal for western Africa • In Angola for southern Africa• In the WHA of WHO • In Spain, Belgium or Italy for Occidental Europe (?)• In Argentina for Southern America• In Venezuela for the Andean and Caribbean Region• In Sweden for Scandinavian Countries• New ideas: north african countries in Tunisia ? , Middle East
in Lebanon ?,