Embed Size (px)
Citation preview

Towards Non-thrombogenic Performance of Blood Recirculating Devices
D. BLUESTEIN,1 K. B. CHANDRAN,2 and K. B. MANNING3
1Department of Biomedical Engineering, Stony Brook University, Stony Brook, NY 11794, USA; 2Department of BiomedicalEngineering, University of Iowa, Iowa City, IA 52242, USA; and 3Department of Bioengineering, Pennsylvania State University,
University Park, PA 16802, USA
(Received 27 October 2009; accepted 2 January 2010; published online 4 February 2010)
Associate Editor Larry V. McIntire oversaw the review of this article.
Abstract—Implantable blood recirculating devices have pro-vided life saving solutions to patients with severe cardiovas-cular diseases. However, common problems of hemolysis andthromboembolism remain an impediment to these devices. Inthis article, we present a brief review of the work by severalgroups in the field that has led to the development of newmethodologies that may facilitate achieving the dauntinggoal of optimizing the thrombogenic performance of bloodrecirculating devices. The aim is to describe work whichpertains to the interaction between flow-induced stresses andthe blood constituents, and that supports the hypothesis thatthromboembolism in prosthetic blood recirculating devices isinitiated and maintained primarily by the non-physiologicalflow patterns and stresses that activate and enhance theaggregation of blood platelets, increasing the risk of throm-boembolism and cardioembolic stroke. Such work includesstate-of-the-art numerical and experimental tools used toelucidate flow-induced mechanisms leading to thromboem-bolism in prosthetic devices. Following the review, the paperdescribes several efforts conducted by some of the groupsactive in the field, and points to several directions that shouldbe pursued in the future in order to achieve the goal for bloodrecirculating prosthetic devices becoming more effective asdestination therapy in the future.
Keywords—Cardiovascular devices, MHV, VAD, Blood
flow, Numerical simulations, Thromboembolism, Platelets.
INTRODUCTION
The advent of implantable blood recirculatingdevices has provided life saving solutions to patientswith severe cardiovascular diseases. The REMATCHstudy indicated that left ventricular assist devices(LVAD) are superior to drug therapy, paving the way
for their use as long-term heart replacement therapyfor patients not eligible for heart transplants. However,as destination therapy VAD patients still suffer fromunacceptable survival rates, and high complicationrates of thromboembolism and strokes. ProstheticHeart Valves (PHV) are routinely used for replacingdiseased native valves, but Mechanical Heart Valves(MHV) patients, for example, still develop thrombo-embolic complications at a rate that is suboptimal.There are more than a few examples of devices thatwere voluntarily withdrawn during clinical trials due tounacceptable incidence of thromboembolism. All thesedevices, as well as devices that are rapidly appearing onthe market, share common problems of hemolysis andchronic platelet activation that lead to thromboem-bolism. The attendant risk for cardioembolic strokethus remains an impediment to these devices. Themandatory life-long anticoagulant drug regimen mostof the devices require, which induces vulnerability tohemorrhage and is not a viable therapy for somepatients, does not eliminate this risk.
The formation of thromboemboli in flow fields ofblood contacting cardiovascular (CVS) devices ispotentiated by contact with foreign surfaces andregional flow phenomena. The non-physiologic flowpatterns generated in the device is considered as one ofthe major culprits in enhancing the hemostaticresponse by chronically activating platelets, yet in thelack of appropriate methodology it is almost fore-boding for device manufacturers to optimize the devicethrombogenic performance during the research anddevelopment (R&D) stage. This means that they arelikely to follow designs that are proven to performbetter in long-term clinical trials and animal experi-ments as required by regulatory agencies—both arepost the R&D design optimization stage.
In the NHLBI 2004 Working Group for NextGeneration Ventricular Assist Devices for Destination
Address correspondence to D. Bluestein, Department of Bio-
medical Engineering, Stony Brook University, Stony Brook,
NY 11794, USA. Electronic mail: [email protected],
Annals of Biomedical Engineering, Vol. 38, No. 3, March 2010 (� 2010) pp. 1236–1256
DOI: 10.1007/s10439-010-9905-9
0090-6964/10/0300-1236/0 � 2010 Biomedical Engineering Society
1236

Therapy,76 a major recommendation was to developimproved anti-thrombotic therapies and device tech-nologies to reduce thromboembolic events, based onsuccessful computational and experimental fluiddynamic studies within prosthetic heart valves thatshould be further developed and applied to ventricularassist devices. Highlighting the importance of devel-oping a methodology to deal with this daunting chal-lenge, a yearly workshop entitled ‘‘Computer Methodsfor Cardiovascular Device Design and Evaluation’’was recently organized, co-sponsored by the U.S. Foodand Drug Administration, the National Heart, Lungand Blood Institute in the National Institutes ofHealth and the National Science Foundation.Recently, The U.S. Food and Drug Administrationalso initiated a unique project, ‘‘Standardization ofComputational Fluid Dynamic (CFD) TechniquesUsed to Evaluate Performance and Blood DamageSafety in Medical Devices.’’ The purpose of this pro-ject is to determine how CFD can be effectively used tocharacterize fluid flow and to predict blood damage inmedical devices.
The Promise and Challenge of BloodRecirculating Devices
Over 5.3 million patients suffered from heart failurein 2000 and this is expected to grow by 50% over thenext 15 years.43 Of those, a significant proportion willbecome candidates for longer-term VAD destinationtherapy and many other CVS devices, dictating theneed to drastically reduce their complication rates.MHV for example correspond to over 170,000implants worldwide each year,96 with more than100,000 implantations in the US alone. The advent ofimplantable blood recirculating devices has providedlife saving solutions to patients with severe cardiovas-cular diseases. The REMATCH study indicated thatleft ventricular assist devices (LVAD) are superior todrug therapy, paving the way for their use as long-termheart replacement therapy for patients not eligible forheart transplants. However, as destination therapyVAD patients still suffer from unacceptable survivalrates, and high complication rates of thromboembo-lism and strokes. Prosthetic Heart Valves (PHV) areroutinely used for replacing diseased native valves, butMechanical Heart Valves (MHV) patients, for exam-ple, still develop thromboembolic complications at arate that is suboptimal. There are more than a fewexamples of devices that were voluntarily withdrawnduring clinical trials due to unacceptable incidence ofthromboembolism. All these devices, as well as devicesthat are rapidly appearing on the market, share com-mon problems of hemolysis and chronic platelet acti-vation that lead to thromboembolism. The attendant
risk for cardioembolic stroke thus remains an impedi-ment to these devices. The mandatory life-long anti-coagulant drug regimen most of the devices require,which induces vulnerability to hemorrhage and is not aviable therapy for some patients, does not eliminatethis risk.
Thromboembolic Complications in BloodRecirculating Devices
The REMATCH study82,89 indicated that left ven-tricular assist devices (LVAD) are superior to drugtherapy (48% decrease in mortality). However, it hasonly a 30% 2 year survival, and still an unacceptablecomplication rate: thromboembolism in 3–35% ofbridge-to-transplant patients, and strokes in 16% ofdestination therapy VAD patients.68 The implantabletotal artificial heart may eventually offer a solution tothe chronic shortage in heart for transplantation.Prosthetic Heart Valves (PHV) are routinely usedtoday for replacing diseased heart valves, but inMechanical Heart Valves (MHV) patients platelets arechronically activated. All these devices, as well asdevices that are rapidly appearing on the market, sharecommon problems of hemolysis, platelet destruction,and thromboembolism. Combined with the attendantrisk for cardioembolic stroke, it remains an impedi-ment to these devices. The mandatory life-long anti-coagulant drug regimen most of them required, whichinduces vulnerability to hemorrhage and is not a viabletherapy for some patients, does not eliminate this risk.
Contact and Flow Activation of Platelets
The well-known ‘‘Virchow’s triad’’ of blood, sur-face, and flow, establishes the blood–artificial surfaceinteraction problem as a multifactorial one. The flowcomponent, perhaps the most complex part of thetriad, combines the three: local flow patterns play asubstantial role in coagulation reactions, plateletaggregation, and deposition. It determines where athrombus will form, its size and composition, andwhether or not it will remain at its nidus or embol-ize.87,88 Thrombus and thromboemboli generated incardiovascular devices is composed primarily ofplatelets, with less fibrin involvement than one wouldencounter in low-shear thrombosis.44 Flow-inducedshear platelet activation causes both aggregation andthrombin generation, showing consistent ‘dose’ andtime response characteristics of equivalent chemicalagonists.78,79 The cumulative effect of varying flowstresses and exposure times along platelet trajectoriesin stenoses and past MHV further indicates thatplatelet activation criteria should be established undermore realistic flow conditions.
Non-Thrombogenic Performance of Blood Recirculating Devices 1237

Flow-Induced Device Thromboembolism
One of the major culprits in blood recirculatingdevices is the emergence of non-physiologic (patho-logic) flow patterns that enhance the hemostaticresponse. In PHV and similar devices portions of theflow cycle may become turbulent, with elevated tur-bulent stresses within MHV hinges.45,97 VAD inducechanges to coagulation by activating platelets despiteaggressive anticoagulant therapy, with flow patternsimplicated in the underlying risk for their thrombo-embolism,54 especially cerebral embolism (rates rang-ing from 7.4% for the Heartmate VAD to approx.50% for the Novacor VAD system).31 Platelet aggre-gates are the source of microembolic signals (MES)measured in patients with PHV.42,71 A significant effectof valve hemodynamics for two valve designs (bileafletvs. monoleaflet) was found in patients.65,66 Thesehigher number of MES for bileaflet vs. monoleafletMHVs correlated to platelet activity measurements byour group in an LVAD with the same type of valves.94
The Significance of Studying Platelet ActivationOver Hemolysis
Flow-induced blood trauma was almost exclusivelystudied in respect to red blood cells (RBC) damage(hemolysis), and has become a standardized develop-ment tool.80,84,85 However, in recent years it was shownthat platelet activation and thrombogenicity is thesalient aspect of this blood trauma.86 RBCs are muchmore resistant to mechanical damage, and experienceless shear forces than platelets. The relative rigidity ofplatelets membrane causes a higher strain to dissipateacross their membranes. Hemolysis may occur at shearlevels one order of magnitude larger than thoserequired to activate platelets.61 Because their smallersize, turbulent stresses present during MHV flowdeceleration phase and leakage flow poses a directthreat to the platelets. Recent studies contrastinghemolysis by leakage flow with platelet activation inMHV,67 demonstrated that while hemolysis barelyincreased, platelet activation increased significantly.These new findings are closely followed by the FDA,and are likely to set more stringent limits than hemo-lysis for testing devices.
Measuring the Thrombogenic Potential of Devices
The growing recognition that thrombosis, ratherthan hemolysis, is the primary clinical problem asso-ciated with CVS devices, is further accentuated by thepioneering AbioCor Implantable Replacement HeartSystem that was implanted in several patients in recentyears. While no evidence of significant hemolysis was
observed in animal or human patients studies,28 severalof the patients died of stroke related complications.Regretfully, very few data on flow-induced thrombo-genic aspects are currently available. Severalapproaches for studying device-induced thromboge-nicity are in progress by few groups.51,53,56 Jesty andBluestein51 have developed an innovative PlateletActivity State (PAS) assay, facilitating near real timemeasurements of the thrombogenic potential inducedby flow in devices. This technique was applied toin vitro measurements of flow-induced platelet activa-tion in MHV mounted in a LVAD,16,94 and wasrecently utilized to measure the thrombogenicity ofbioprosthetic and new generation polymer valves95
which are targeted for the minimally invasive percu-taneous valve delivery—the breakthrough techniquewith a huge promise for patients who cannot toleratecardiothoracic surgery. The goal is for polymer valves,which are better suited for stented delivery, to havethrombogenic potential comparable to the latter as notto require mandatory anticoagulation therapy.
Flow Mechanisms Overlooked in Thromboembolism
Vortex shedding was observed experimentally andcomputed numerically in the wake of MHV leafletsand in various blood recirculating devices. Shed vor-tices are postulated as a major mechanism for formingthe microemboli associated with prosthetic devices.They provide the necessary conditions for the hemo-static reaction by providing optimal mixing for plateletaggregation, increasing the procoagulant surfacesneeded for the coagulation reactions to proceed, anddispersing the clotting factors in the process. Prioractivation and the extrusion of platelets pseudopodia,potentially induced by the elevated shear stressesglobally preceding vortex shedding, increases theireffective hydrodynamic volume by several folds,resulting in an increased collision rate.92
Numerical Simulations of Flow in PHV
Numerical simulation in the wake of a MHVdepicted the complex behavior of vortex shedding.49
Laminar simulations57,58,62 depicted the effects oftransient flow past MHV and the wake dynamics.However, they may have limited utility as turbulentstresses may easily overwhelm their laminar counter-parts, and are critical in activating the hemostaticsystem.13 Limitations of many turbulence models inhandling valvular flows (pulsatility entails transitionalturbulence, which violates the isotropic turbulenceassumption most turbulence models use), restricts thesuccess of their application. First attempts to solvesteady Reynolds-averaged Navier–Stokes (RANS)
BLUESTEIN et al.1238

equations in MHV used simplistic mixing-length tur-bulence models.60 Bluestein et al.12,15 were the first toperform unsteady turbulent simulations (URANS)using the transient turbulence Wilcox k–x model. Thesimulations depicted the intricate dynamics of the shedvortices in the wake and quantified stress histories ofplatelets along pertinent trajectories. Recently, ad-vanced approaches to turbulence modeling in PHVwere applied, e.g., Large Eddy Simulations.35,36 Ourgroup has conducted such complex transient/turbulentsimulations, including a damage accumulation modelthat takes into account the effects of repeated passagespast the valve,3 and FSI simulation comparing thethrombogenic potential of ATS and St. Jude MedicalMHVs.29
Blood Damage, Platelet Activation, and BloodClotting Models
Few models for hemolysis have been developed overthe years, e.g., as a function of mechanical energydissipation,17 or relating it to shear stress.5,6,8,9,19,20 Inthese predictive phenomenological models, the nor-malized internal damage accumulates until a criticalvalue of damage is reached, either as a function of theinstantaneous stress level and the previous damagehistory, or as weight average damage accumulationover a number of cycles. Recently, in vitro hemolysisindices were investigated numerically over 3D devicesdomains for the purpose of design optimization,33 andby integrating hemolysis and platelet lysis indices alongtrajectories in the flow field of MHV.2,39 Several worksexamined directly the interaction of activated plateletswith blood field,2,32,64,87,88 or platelet depositionmodels.26,81,91 However, these innovative approacheshave not been applied yet to device relevant flowconditions. Multi-phase fluid modes combining effectsof pulsatile flow, indicated that platelet-size particlesare preferentially segregated to the near wall region inwhich the maximum shear stress is found.18 An algo-rithm that takes into account the effect of initialdamage was recently applied for simulating thecumulative damage during repeated passages ofplatelets flowing through a St. Jude Medical MHV.3
Predictions of a similar model were experimentallyvalidated in a hemodynamic shearing device (HSD).77
Such recent modeling efforts provide insight into theareas where platelets have a high probability for acti-vation, leading to clot formation and thromboembo-lism.
Contribution of MHV Closing Dynamicsto Thromboembolism
During the development of MHVs in the period of1960–1980, hemodynamic evaluation of the various
models concentrated on the velocity profiles, wall shearstresses (WSS), regions of flow separation and relativestasis as well as turbulent stresses in the flow fielddownstream from the fully open valve in order todetermine the relationship between fluid-inducedstresses and platelet activation resulting in thrombusdeposition with implanted valves. Numerical simula-tions, including more recent FSI analyses, have con-centrated on the fluid dynamics predominantly duringthe opening phase of the cardiac cycle. However, withthe failure of a new model of a bi-leaflet mechanicalvalve attributed to cavitation type of damage afterimplantation,55 and with a design change resulting inincidences of structural failure with a tilting discvalve,21 more attention has also been devoted to theclosing dynamics with MHV and potential for thevalves to cavitate resulting in structural failure. As theoccluder moves towards the closing position withleaflet tip velocities of the order of 5 m/s and suddenlycomes to a stop in the fully closed position, a largenegative pressure transient develops in the upstreamside of the leaflet with a corresponding positive pres-sure transient on the downstream side of the leaflet.The resulting relatively large pressure gradient acrossthe leaflet in the gap width between the leaflet and thevalve housing as well as in the small gaps in the hingeregion of the bileaflet valves can result in relativelyhigh velocity of blood flow and abnormal WSS nearthe valve structures that the red blood cells andplatelets are subjected to.21,69,72
Closing dynamics of MHV employing FSI analy-sis22,23,63 and experimental studies59 have beenreported in the literature to calculate the local fluiddynamics in the gap width at the instant of valve clo-sure. Highly resolved description of the flow dynamicsin the small gap widths have been reported with localmesh refinement in the analysis.63 These studies dem-onstrate relatively large flow velocities and shearstresses that the formed elements are being subjectedto, during the flow through the gaps at the instant ofvalve closure and the presence of large vortical flow inthe upstream side of the occluder. Platelets that passthrough such gaps at the instant of valve closure can besubjected to relatively high shear stresses can bepotentially activated and subsequently be trapped inthe vortical flow in the vicinity of the leaflets for arelatively large residence time. Particle dynamic anal-ysis with point particles representing platelets seeded inthe flow and the computation of the fluid shear stress-time integral that the particles are subjected to (as aparameter for platelet activation potential13) haveshown that the flow through the gap width at theinstant of valve closure and subsequent rebound of theoccluder presents another potential site for the acti-vation and aggregation of platelets and the aggregated
Non-Thrombogenic Performance of Blood Recirculating Devices 1239

platelets attaching to the surface of the occluder andthe valve housing resulting in the initiation ofthrombi.63
THE DEVICE THROMBOGENICITY
EMULATOR (DTE)—INTERFACING
NUMERICAL AND EXPERIMENTAL
APPROACHES FOR IMPROVING DEVICES
PERFORMANCE
(Bluestein, D., Yin, W., Dumont, K., Alemu, Y.,Xenos, M., Einav, S., Jesty, J.)
The concept of the Device Thrombogenicity Emu-lator (DTE) that is presented below is motivated by thefollowing: A reliable methodology capable of providingquantitatively accurate predictions of flow-inducedblood hemostatic activation is essential for reducingthromboembolism in cardiovascular devices. Suchmethodology would facilitate identifying relevantdesign parameters, and elucidate how various designconfigurations and modifications affect thromboem-bolism in devices. Currently, the device flow dynamicsare mainly investigated using experimental techniques,with a limited ability to resolve the intricate small-scaleflow phenomena involved in thromboembolism. CFDis unfortunately incorporated only at a late stage ofdevice design process, having limited utility for effectivedesign alterations. Additionally, flows in devices exhibita host of unique modeling challenges and difficulties.This is further limited by inadequate characterizationof the complex flow fields and their interaction with theblood borne particulates. Given these enormous com-plexities, sophisticated fluid dynamics testing of car-diovascular device flows requires a close synergybetween advanced experimental and computationaltechniques.96 An integrated methodology which com-bines numerical models with experimental techniquesto measure device thrombogenicity has the potential totransform current devices design and testing practices,leading to substantial time and cost savings during theresearch and development phase.
Some of the work that led to the development of theDTE is described below:
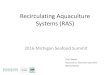
The blood flow dynamics through an aortic bileafletMHV (St. Jude Medical) during the flow decelerationphase following peak systole, that contribute to plateletactivation and thromboemboli formation, are depictedin Fig. 1. The MHV is shown after aortic valvereplacement (AVR).12 The Reynolds-averaged Navier–Stokes (URANS) equations were solved with non-Newtonian blood properties using the Wilcox k–xturbulence model which is primarily intended for sim-ulating globally low-Re internal flows (intermittentturbulent flows in the transitional range). The simulation
depicts the intricate dynamics of the shed vortices thatappear in the wake of the valve leaflets during thedeceleration phase after peak systole, and are postu-lated to be a major source of free emboli formation,enhancing the risk of cardioembolic stroke. The com-plex flow patterns generated in the wake of the valveprovide conditions that promote the formation of largeplatelet aggregates. Previous numerical results werevalidated with Digital Particle Image Velocimetry.15
Turbulent particle paths were computed using aLagrangian approach of particulate two-phase flowand a stochastic model simulating the interactionbetween turbulence and platelets.37,38 A large portionof the platelets flowing around the leaflets whileexposed to elevated shear stresses were entrappedwithin the wake of the shed vortices. Shear stress loadhistories of the platelets along these trajectories werecomputed by a summation of the product of the total(laminar plus turbulent) shear stress (s) by the instan-taneous exposure time to this stress along the trajec-tory,
P(s 9 Dt)—‘Level of Activation’ parameter.13
Two characteristic platelet paths computed during flowdeceleration and their cumulative level of activation areshown for bileaflet and monoleaflet); one in the regionof highest shear stresses near the leaflet, the other in thecore flow region used as a reference lower activationlevel. Platelets flowing near the leaflets showed a muchhigher level of activation, with the bileaflet valve pro-ducing steep and rapid increase in the activation level.The level of activation was further correlated to in vitroplatelet activity measurements performed in LVAD.94
FSI Simulations
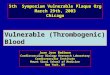
Platelet damage models were incorporated into aFluid Structure Interaction (FSI) simulation, where thethrombogenic potential of two MHV: ATS and theSJM Regent were compared. The detailed geometricfeatures of the valves superstructures (including thehinges) were incorporated.29 The flow fields at peaksystole (T = 0.120 s) and during regurgitation (closedleaflets) are depicted in Fig. 2, with wall shear stressdistributions superimposed on the leaflets, indicatinghigher values for the SJM valve during both the for-ward flow and regurgitation phases. The thrombogenicpotential of each valve was then calculated by com-puting the platelet stress accumulation over trajectoriesof 15,000 particles. Platelets dispersion patterns duringpeak systole and regurgitant flow through the hinges(valve closed) are depicted in Fig. 3. Their corre-sponding activation accumulation intervals (as barcharts of low and high ranges), clearly indicate that theSJM MHV is activating more platelets. This servesto demonstrate the robustness of the numerical meth-odology in showing how small design changes
BLUESTEIN et al.1240

(open pivot hinge ATS valve design as compared to theSJM ‘ear’ hinge design) translates into differentthrombogenic potential for the valve.
DNS Simulations
Recently we have been conducting DNS (DirectNumerical Simulations) of blood flow past St. JudeMHV. While requiring significant computationalresources, DNS liberate from the need to use complexand approximate turbulence models by resolving thegrid below the smallest Kolmogorov turbulent scales(in the range of 20–70 lm in MHV flows, 47 lm in arecent publication34). The highly resolved grid con-sisted of 17 9 106 finite volumes (40 lm). Results ofthese breakthrough simulations depicted an intricatepattern of counter rotating helical vortices in the gapclearance (between the leaflet pivot and the valvehousing recess) of the MHV (Fig. 2). The intricatedynamics of the shed vortices in the wake of the valveduring the deceleration phase after peak systole aredepicted by 3D turbulent trajectories (Fig. 4). 3Dhelical vortices are formed entrain fluid span-wise fromthe leaflet leading edge into the wake of shed vortices.Those trap potentially activated platelets, enhancingthromboemboli formation.
Platelet Activity State (PAS) Assay for MeasuringThrombogenic Potential in Devices
The thrombogenic potential of various PHV wastested in LVAD using the Platelet Activity State (PAS)
assay,51 and was successfully applied to study plateletactivity in pathological cardiovascular flow fields andPHV.10,11,13,14,16,94 The PAS assay is an innovativetechnique, based on a modified prothrombinaseassay.51 The prothrombinase complex that activatesprothrombin to thrombin in coagulation assembles onthe activated platelet surface. It consists of factor Xabound to the two essential cofactors provided by theactivated platelet: Va, and anionic phospholipids.52
Acetylated prothrombin reacts with the prothrombin-ase complex to produce a thrombin species that doesnot activate platelets or clot fibrinogen. The removal ofthe positive feedback activation by thrombin (Fig. 5) isessential for measuring low-level flow-induced plateletactivation. It results in easily measurable linearthrombin generation that accurately reflect the plate-lets procoagulant activity, while segregating flow-induced contributions to the hemostatic response. Inthis way a one-to-one correspondence is establishedbetween the agonist (flow-induced platelet activation)and the resulting platelets procoagulant activity, i.e.,thrombin generation.
Effects of Different MHV Designs
Platelets were recirculated in LVAD40 (Fig. 6),mounted with Carbomedics bileaflet and Bjork–Shileymonoleaflet MHV. Their activity was measured usingan innovative Platelet Activity State (PAS) assay. Themeasurements indicated that the Carbomedics bileafletMHV activated platelets at a rate of more than 2-foldthan the Bjork–Shiley monoleaflet MHV (Fig. 6),indicating that the latter is less prone to thromboem-bolic complications.94 These measurements were incomplete agreement with the numerical predictions ofdifferences in platelet activation between the samevalves, as described above.
The Device Thrombogenicity Emulator (DTE)Methodology Using a Hemodynamic Shearing
Device (HSD)
An effective methodology for testing and optimizingdevice thrombogenic performance is presented, inwhich a thrombogenicity predictive technology isdeveloped to facilitate a reduction of the device flow-induced thrombogenicity. This methodology involves aDevice Thrombogenicity Emulator (DTE) depicted inFig. 7 that replicates device hemodynamics with greataccuracy according to advanced numerical simulationsof blood flow in the device, and measures its thromb-ogenicity using a platelet activity state (PAS) assaycapable of near real time and highly sensitive mea-surements of flow-induced platelet hemostatic activityin devices. Specifically, it combines stress loading
Aortic RootSinusesVortices
Sewingring
Vortexroll-up
Shed Vortices
Recirculationzones
Sutureknot
Pledgetwith scartissue
Velocity colocode
1.0 m/s 0.8 m/s 0.6 m/s 0.4 m/s 0.2 m/s
FIGURE 1. Flow field through St. Jude bileaflet MHV (196 msafter peak systole).
Non-Thrombogenic Performance of Blood Recirculating Devices 1241

waveforms extracted from detailed numerical flowsimulations that are programmed into a computer-controlled, hemodynamics-emulating device (Hemo-dynamic Shearing Device—HSD), and the plateletactivity state measurements. It will be capable of pre-dicting the effect of design modifications aimed spe-cifically at reducing device thrombogenicity. Ratherthan refabricating and testing the entire device, theDTE emulates the hemodynamics in ‘hot spots’ regionsof a CVS device and then test whether specific designmodifications (conducted in the virtual numericaldomain, then replicated in the HSD where their effectsare tested in vitro) achieve a desired level of thromb-ogenicity reduction. The universal nature of the systemgives the technology an unparalleled degree of freedomfor testing and redesigning almost any type of device.
Several DTE prototypes are currently tested forpredicting the thrombogenic potential of various sub-groups of CVS devices: Prosthetic Heart Valves (PHV)
and Ventricular Assist Device (VAD). PHV offer someof the most complex flow fields in CVS devices andthus a real challenge for optimizing their thrombogenicperformance. They serve accordingly as an excellenttest bed for assessing the proposed methodology. Inthe first stage of the DTE methodology, a detailednumerical modeling of the flow field through devices isperformed. Specifically, several PHV designs:Mechanical Heart Valves (MHV), polymeric valves,and bioprosthetic valves are studied, as well as a pul-satile VAD. The models include highly resolved devicegeometries for studying small-scale flow phenomena inregions leading to thromboembolism. Sophisticatedturbulence and fluid/structure interaction (FSI) modelsand damage accumulation models are employed.
In the first stage, the ‘hot spot’ regions that may leadto device thrombogenicity during distinct flow phasesare identified, and flow trajectories within these regionsthat expose platelets to elevated stresses and potentially
FIGURE 2. FSI simulation comparing SJM and ATS valves. Vector flow fields and wall shear stresses on the leaflets are shownduring peak systole (top) and regurgitation (bottom).
BLUESTEIN et al.1242

lead them towards activation are computed. The spa-tial–temporal stress distribution along the pertainingtrajectories are extracted, and applied as stress loadingwaveforms that are programmed into the HSD. Thisbench top system combines the features of cone andplate and Couette viscometers, and is designed with aspecial consideration to ensure that the shear stress is
uniform throughout the device. The HSD is pro-grammed by translating the load waveforms computedalong the pertinent trajectories in the device flow field toa dynamically changing cone spinning input waveform,accurately replicating the shear stress history along theplatelet trajectory and uniformly exposing an entireplatelet population in the HSD to this stress history.
FIGURE 3. Platelet dispersion patterns during peak systole (top) and hinges regurgitation (bottom). Different hinge mechanismdesign translate into higher thrombogenic potential for the SJM valve during regurgitation.
FIGURE 4. DNS simulations of blood flow through St. Jude MHV, showing complex platelet trajectories following helical patternof counter rotating vortices in the hinges region (zoom in, bottom right).
Non-Thrombogenic Performance of Blood Recirculating Devices 1243

TheHSD loaded with a platelet buffer is operated insidean incubator. Access ports are used to introducereagents and easy removal of multiple samples. Plateletactivity measurements are performed on timed aliquotsremoved from the system using the platelet activity state(PAS) assay.
In a blood recirculating device there is no a prioriknowledge of the individual stress histories thatplatelets are subjected to during the ensuing passagesin the device. In the HSD on the other hand, the entireplatelet population is uniformly exposed to a knownprescribed dynamic shear stress waveforms obtainedfrom the simulations. In this way the HSD serves toaccentuate minute effects of design modifications onplatelet activity. The design optimization for a specificdevice type follows an iterative process, where geo-metric optimization is re-iterated in the modelingphase, and the new design tested in the HSD. The HSDreplicates the flow conditions within the optimized
FIGURE 5. PAS assay: platelets prothrombinase activity,and the effect of prothrombin acetylation-eliminating thefeedback loop elimination.
Time (min)0 10 20 30
PA
S (
Nor
mal
ized
)
-0.01
0.00
0.01
0.02
0.03
0.04
0.05
BileafletMonoleaflet
Slope: monoleaflet = 3.14E-4bileaflet = 8.11E-4
Slopes Difference: p < 0.05
Carbomedics Bjork-Shiley
FIGURE 6. In vitro platelet activity measurements in LVAD: the bileaflet MHV generated higher platelet activity than the mono-leaflet MHV (p < 0.05).
FIGURE 7. The DTE methodology: platelet trajectories and their loading history in MHV flow serve to generate input waveforms tothe Hemodynamic Shearing Device (HSD).
BLUESTEIN et al.1244

design, and the new thrombogenic potential is mea-sured. The optimized design will then be manufacturedand tested in the LVAD system to show whether itachieved a reduction in its thrombogenic potential.This optimization methodology may become anessential tool for manufacturers that seek to create,redesign, and test blood recirculating cardiovasculardevices. Besides reducing R&D costs, it may preventunfortunate situations where devices need to berecalled or clinical trials stopped, because of unaccept-able thrombogenicity levels—situations that could becatastrophic to patients and with devastating financialcosts to society and device manufacturers alike. It isenvisioned that it will also facilitate the use of thesedevices for long-term therapy by reducing the need fordifficult pharmacological management with anticoag-ulants, which is mandated for most existing devices.
NUMERICAL SIMULATIONS OF MHV
CLOSING DYNAMICS AND PLATELET
ACTIVATION
(Chandran, K. B., Udaykumar, H. S., Lu, J.,Vigmostad, S.)
MHV Closing Dynamics
As described before, the closing dynamics of MHVillustrate the high velocities and elevated shear stressesthat the formed elements are being subjected to, duringthe flow through the gaps at the instant of valve clo-sure that has the potential to activate the platelets. The
flow through the gap clearance at the instant of valveclosure and subsequent rebound of the occluder mayalso promote initiation of thrombi. Typical plots of theflow stream lines, the shear stress distribution and theplatelet activation parameter computed for flowthrough the gap width of a typical bi-leaflet valve atthe instant of valve closure is shown in Fig. 8. Localmesh refinement in the computational algorithm hasresulted in highly resolved flow through the gap regionat the instant of valve closure exhibiting relatively highshear flows through the gap in which the platelets canbe potentially activated and the activated platelets canget trapped in the vortical flow near the leaflet that canencourage aggregation and adhesion of the platelets tothe surface of the leaflets. The platelet activationparameter (the fluid shear stress–time integral that theparticles are subjected to, Fig. 8c) indicates a region ofincreased potential for platelet activation behind theoccluder, where a jet-like flow passing through the gapforms a recirculation zone (Fig. 8a). Similar dynamicanalysis of flow through a 2D hinge geometry of abi-leaflet valve has also demonstrated that the hingeregion presents another potential region where theplatelets can get activated and subsequently remain inthis region to be deposited on the valve structures.41
Red Blood Cell (RBC)/Platelet Interaction Analysis
Both the simulations of the MHV forward flow andclosing phase dynamic analysis described above arebased on organ-level scale simulation with theassumption of the fluid as a continuum. The analysisfor the potential for the platelets to be activated is
FIGURE 8. Plots of (a) stream lines; (b) shear stress contours; and (c) simulated platelet activation parameter for the flowdynamics in the gap width between the leaflet edge and the valve housing for a bi-leaflet mechanical valve at the instant of valveclosure.
Non-Thrombogenic Performance of Blood Recirculating Devices 1245

based on the assumption that the bulk fluid viscous orturbulent shear stresses are directly transmitted to theplatelets in this region. Such an assumption ignores theinteraction between the relatively large number ofRBCs (95% of formed elements) and platelets (4.9% offormed elements) in the region of such stresses. Inaddition, the analysis of flow dynamics during theclosing phase of MHV dynamics involves analysis offlow in gap widths of 100 lm and the gap width is ofthe same order of that of the diameter of the RBC(~8 lm). Hence the continuum assumption breaksdown in this region as well.
The platelet dynamic analysis employed in thesecalculations assumes that the point particles repre-senting the platelets move with the same velocity ofthat of the fluid and particle–particle and particle–surface interactions are neglected. In the one-waycoupling assumption employed, the effect of theformed elements on the fluid is also neglected. Thus,the organ level simulations are able to predict regionsof relatively high fluid-induced stresses and predictedregions of thrombus deposition that correlates wellwith the regions observed with thrombus formationwith implanted MHVs. Several experimental studieshave demonstrated that, at the micro-scale level,increase in the number of RBCs in flow results in themargination of the platelets to the boundary region ofthe flow regime with the RBCs cluttering towards thecore region of flow.1,30,90 In order to determine themechanical basis for platelet activation in such flowfields, a micro-scale simulation with a detailed analysisof particulate interaction is essential. Towards this end,a first generation micro-scale analysis simulating theRBC/platelet interaction in a flow field has beenrecently reported.4 In this model, 2D flow dynamics ofRBCs simulated as 8 lm ellipsoid semi-rigid elasticsolid and platelets simulated as rigid 2 lm discoids wasanalyzed. Collision and translation of the particleswithin the steady flow field of Newtonian fluid (plas-ma) was computed with the location of the solidsidentified at every instant using the level-set algorithm.The analysis was restricted to low Reynolds numberflows with the hematocrit limited to below 15% in theinitial attempt on the development of the micro-scaleanalysis for RBC/platelet interaction.
The analysis showed that the platelets were mar-ginated to the boundaries where as the RBCs tend tomove towards the core flow region, agreeing with theprevious experimental studies. Furthermore, the com-putations also showed that the platelets in the flowfield experienced significantly higher shear forces thanthe bulk fluid shear, and this effect was due to the fluidstreaming between particles when they move close toeach other immediately before or after collision. It wasalso further determined that the shear forces experienced
by the platelets increased with increase in the numberof RBCs (hematocrit) within the range of hematocritsstudied in the model. Furthermore, this analysisshowed that the relative size of the RBCs was moreimportant in the interaction among the particles ratherthan the ellipsoid shape. Figure 9 depicts the margin-ation of the platelets in the flow field with the ellipsoid(Fig. 9a) or cylindrical (Fig. 9b) shaped RBCs of 8 lmin diameter. During the initial efforts on the micro-scale simulation, the analysis was restricted to lowReynolds number flows and with the hematocrit mag-nitudes restricted to less than 15%. The RBCs were alsoassumed to be semi-rigid solids and more realisticsimulation requires the analysis with a fluid-filled flex-ible membranous cells interacting with relatively rigidplatelets. Efforts are continuing on the parallelizationof the code and improved computational algorithms inorder to analyze the micro-scale dynamics to physio-logically realistic flow and hematocrit ranges.
Need for Multi-Scale Simulation
Although the flow in narrow gap widths can beresolved accurately with local mesh refinement in thesimulation of flow dynamics past MHVs in the organlevel simulation, it is impractical to perform micro-scale computations for the entire flow field at theorgan-level dimensions. Micro-scale analysis of thedetailed interaction between RBCs and platelets dem-onstrates that the forces transmitted to the platelets aresignificantly higher than the bulk shear stress com-puted in the flow fields. Hence the application of par-ticle dynamic analysis with one-way coupling and thecomputation of the integral of the bulk shear stressthat the particles are subjected to and the duration as ameasure of platelet activation may not provide anaccurate depiction of the behavior of the platelets insuch flow fields. For example, in the high shear flowfield in the gap between the leaflet edge and valvehousing with MHVs (and similarly in the hinge regionsof bi-leaflet valves), detailed computation of the inter-action between the RBCs and platelets is necessary to
FIGURE 9. Micro-scale analysis of RBC/platelet interactionin a channel with a width of 42 lm.
BLUESTEIN et al.1246

understand the mechanics related to the activation ofplatelets. One alternative to resolve the behavior ofplatelets in flow past cardiovascular implants is todevelop multi-scale simulation strategies. One possibleapproach to the problem is to develop the detailed flowdynamic analysis for the valve dynamics at the organlevel that includes highly resolved flow dynamicssolution with FSI analysis in the three-dimensionalgeometry. Regions of interest such as with high shearflow fields can be identified with such an analysis andthe micro-scale analysis is then performed in the‘zoomed in’ region of interest for the detailed dynamicsof RBCs and platelets.
Strategies and appropriate algorithms are in need ofdevelopment for concurrent analysis at the organ leveland micro-scale flow fields and appropriate transfer ofinformation among the multi-scale analyses. Devel-opment of such multi-scale simulations will be veryimportant in the understanding of the precise mecha-nism for platelet activation and such understandingcan form the basis for design modifications to mini-mize the problem encountered with cardiovascularimplants. Development of multi-scale simulations is anactive area of algorithm development in theunderstanding of the biological transport phenomenaranging in spatial scale varying from organ level tosub-micron dimensions and temporal scale varyingfrom years to nano-seconds. The reader may want torefer to the position paper ‘‘Particle-Based Methodsfor Multiscale Modeling of Blood Flow in the Circu-lation and in Devices: Challenges and Future Direc-tions’’ appearing in this special issue that describessome of the particle-based methods recently adapted totackle this challenging problem.
THE PENN STATE ARTIFICIAL HEART
(Manning, K. B., Deutsch, S., Paterson, E. G.,Rosenberg, G., Weiss, W. J.)
Although ventricular assist devices (VADs) aremore widely accepted as bridge-to-transplant, bridge-to-recovery and destination therapy, thromboembolicevents still remain a significant problem. At the PennState Artificial Heart Lab we have been focusing ourefforts to more accurately predict when thrombusdeposition would develop using experimental fluidmechanics, computational fluid dynamics, and animalstudies. As part of this effort, we are developing twoVADs, a 12 cc pediatric pneumatically driven VADand a 50 cc electrically driven VAD. A review of theexperimental fluid mechanics of pulsatile blood pumps,written by our group, has recently appeared.27 Thefluid mechanics of the pumps has been studied sincethe early 1970s in an attempt to reduce hemolysis and
thrombus formation by the device. The mechanicalheart valves employed in the devices are the most likelycause for blood damage and platelet activation. Forexample, turbulent stresses in the regurgitant flowthrough the closed valves can easily be as large as10,000 dyn/cm2. A major feature of all pulsatile pumpsis a rotational ‘‘washing’’ flow in mid- to late-diastole,which is set up by a penetrating inlet jet. While flow inthe pump chamber seems largely benign, and the largerpumps show little or no deposition in the chamber, lowwall shear stresses throughout the pump cycle can leadto thrombus formation in the smaller pumps. Under-standing of the local fluid dynamics is critical.
After analyzing a number of dimensionless param-eters such as the Strouhal number, Reynolds number,and Prandtl velocity ratio that potentially could indi-cate the antithrombotic properties of our pulsatileVADs, we are now convinced that the most importantfactor for a given material and texture is wall shearstress of a given magnitude and duration. Althoughmaintaining a non-dimensional shear stress might seemdesirable, we have evidence from in vivo experiments,experimental fluid dynamics (EFD) and CFD, that aspecific magnitude wall shear for a given time are theparameters that are critical in pump design. Previouswork has clearly shown that simply applying fluidmechanic scaling laws has not translated well withthese types of blood pumps.7 Our data also indicatethat areas of low wall shear are areas prone tothrombus formation. For example it is possible to havetwo different size tubes that have different flow ratesand the same Reynolds number but greatly differentwall shear stresses. Maintaining similitude will notensure a given magnitude wall shear stress. Ratherthan a similitude approach our results indicate that anapproach using CFD and EFD to design a pump thathas a shear stress above a value we are determiningfrom in vivo testing is the correct approach. FromHochareon et al.,47 data show the wall strain rate as afunction of time for various locations in the pumps.Comparing the strain rate history of an area wheredeposition occurs to an area where little or none isencountered provides valuable design data. Unlikeprevious studies,50 these data are taken under pulsatileconditions and compared to in vivo deposition. Thisapproach led to pump design modifications intended tostudy regional flow features rather than global scalingeffects. The three desirable features of the flow field inblood pumps may be summarized as: (1) no regions ofstasis or prolonged residence time; (2) turbulent stres-ses not high enough to activate platelets; and (3) wallshear stresses that are high enough to prevent throm-bus deposition on the artificial material surfaces.
The counter example to this is an early designpneumatic 15 cc pump which displayed consistent
Non-Thrombogenic Performance of Blood Recirculating Devices 1247

thrombus deposition on the fixed surface opposite themoving blood sac.7 Our preliminary fluid dynamicstudies of this chamber showed a single wall washingvortex with no obvious signs of stasis, yet peak wallshear stresses away from the valves were less than10 dyn/cm2, (~290 s�1) much lower than in our 70 ccchamber. In addition, the turbulence levels were lowerin the 15 cc chamber (turbulent shear stresses awayfrom the valves did not exceed 200 dyn/cm2). Ittherefore appears that a reduction in wall shear stressesincreased thrombus adherence to the artificial surface.
50 cc Penn State Ventricular Assist Device
Particle image velocimetry (PIV) was used toquantify the local wall shear rates for correlation tothrombus deposition. Hochareon et al.47 were the firstto note that the whole flow field data, provided by PIV,at any time during the cycle could be acquired rapidlyenough to impact the design process, and further48
used a novel post-processing technique to provide wall
shear rate data, critical to the prediction of thrombusdeposition, from high magnification PIV results on thesurface of the 50 cc blood sac. Using 500 s�1 as aminimum wall shear rate to prevent thrombosis on theblood sac50 enabled to predict areas of potentialthrombus deposition from wall shear maps.47 Theregion predicted as potential locations for thrombusformation were shown to contain thrombi in the in vivoimplant study using the same device.93 We also dem-onstrated a relationship between extremely low wallshears (~300 s�1) and visual thrombosis after bovineexplant of our initial 50 cc VAD design.46
Recently, we have been developing a CFD model topredict areas prone to thrombosis within our 50 ccVAD. We have developed an unsteady three-dimen-sional CFD model based upon simplifying assump-tions and validated it through comparisons with ourPIV data.70,75 We have successfully used this model toevaluate port and chamber design (Fig. 10), valveorientation and type (Fig. 11), scale effects (50 cc vs.70 cc vs. 15 cc), and operational parameters. The value
FIGURE 10. Experimental fluid dynamics (EFD) and computational fluid dynamics (CFD) at 350 ms into diastole-port and chambereffects for V0 (a) EFD velocity, (b) CFD velocity, (c) CFD wall strain rate and V1 (d) EFD velocity, (e) CFD velocity, and (f) CFD wallstrain rate.
BLUESTEIN et al.1248

of a combined EFD/CFD/in vivo program, as amethod toward rational VAD design, is best illustratedby comparing the performance of VAD with diffrentMHV designs. The features of the inlet jet during earlydiastole (Fig. 11) clearly depend on the choice of valve.The inlet jet for the BSM valve penetrates further intothe interior of the pump, than does the jet from theCarboMedics (CM) valve (Fig. 11). The computa-tional shear rate maps (Figs. 11c and 11f) confirm thatthe BSM valve jet is stronger. Our experience tells usthen, that the BSM valve will set up a stronger rota-tional washing flow than will the CM valve. We furtherplan to incorporate blood rheology in stress–strainclosure models for prediction of fluid stress and asso-ciated hemolysis.
12 cc Penn State Pediatric Ventricular Assist Device
As mentioned before, scaling laws are inadequate todesign our smaller blood pumps. We modified our
mock circulatory loop to ensure pediatric physiolog-ical flows and pressures for PIV measurements, andcalculated the wall shear rate in any measurementplane over the beat cycle. Viscoelastic blood analogsprovide a better representation of the flow field inpulsatile pumps than the traditionally used Newto-nian ones,73 as was demonstrated in a 15 cc pediatricdevice,7 where larger regions of lower shear rates,more prone to clotting, were observed for the non-Newtonian fluid.
Long et al.70 developed a series of viscoelastic fluids,as a function of blood hematocrit, that are suitable forour optical measurement techniques. In Manninget al.,74 planar PIV was used to explore the flowbehavior of the Penn State 12 cc pneumatic pediatricassist pump with Bjork–Shiley Monostrut 17 mmMHV, operated at 86 bpm using 40% hematocrit vis-coelastic analog fluid. Wall shear maps complementedthe velocity data collected. In contrast with resultsfrom the larger pumps, the flow field was highly
FIGURE 11. A comparison between EFD and CFD at 150 ms into diastole focusing on the influence of valve type for (a) V2 EFDwith the BSM MHV, (b) V1 CFD with the BSM MHV, (c) V1 CFD with the BSM MHV wall strain rate, (d) V2 EFD with the CM MHV, (e) V1CFD with the CM MHV, and (f) V1 CFD with the CM MHV wall strain rate.
Non-Thrombogenic Performance of Blood Recirculating Devices 1249

three-dimensional during early diastole with poorerpenetration by the valve inlet jet. This led to a laterstart of a ‘‘wall washing’’ rotational pattern. A signif-icant separation region was created upstream of theoutlet valve leaflet during late diastole, effectivelyreducing the area and increasing the pressure dropacross the valve. Wall shear maps indicated regions oflow shear persisting throughout the duty cycle.
Comparative measurements were performed todetermine which MHV provides the best overall flow,in the sense of ensuring an adequate wall shear toprevent large scale thrombosis. We compared theBjork–Shiley Monostrut (BSM) tilting disc valve(17 mm) and the CarboMedics (CM) bi-leaflet valve(16 mm). Adequate wall washing was considered whenwall shear rate exceeded 500 s�1 at each spatial loca-tion for a part of the cardiac cycle. The BSM valveconfiguration exhibits a strong major orifice jet(Fig. 12) that develops with enough momentum toprovide sufficient penetration into the body of thedevice leading to a fully developed rotational flowpattern by 250 ms; 100 ms before the CM valve con-figuration (Fig. 13).24 There was also no valvularleakage associated with the BSM valves, in contrastto the heavy regurgitation seen in the CM valve
configuration that can lead to blood damage. Usingour wall shear calculations, we divided the walls of thedevice into seven sections (Fig. 14). A flood contourmap was generated for each Surface for both valveconfigurations. The color corresponds to wall shearrate, is placed spatially (according to wall location) andtemporally (according to time in the cardiac cycle) inthe x and y axes, respectively, and presented normal-ized (by dividing by 500 s�1). Focusing in the PVADbody (11 mm plane), Surface 1 of the BSM configu-ration (Fig. 15a) experienced wall shear rates over500 s�1 from 250 to 450 ms for the entire wall whereasthe CM valve (Fig. 15b) showed a low shear regionacross most of Surface 1 during early diastole. AlongSurface 2 a more significant difference in wall shearpatterns between the two valve configurations isapparent (Figs. 15c and 7d). The BSM configurationshows adequate shear from 250 to 450 ms over theentire surface, while the CM valve configuration onlyshows wall shear rates above 500 s�1 from 400 to500 ms. This low shear rate for most of diastole couldincrease the propensity of thrombus formation. Sur-face 3 highlights the importance of setting up an earlyrotational flow pattern. The BSM valve configuration(Fig. 15e) shows adequate shear rates from 250 to
FIGURE 12. Mean PIV flow maps in the 11 mm plane at (a) 250, (b) 400, (c) 550, and (d) 650 ms for the BSM valve showing the timehistory of the rotational flow pattern. (From Cooper et al.24 with permission).
BLUESTEIN et al.1250

550 ms, while the CM valve configuration (Fig. 15f)shows low shear until 400 ms. The strong diastolic inletjet near the wall of the device is present from the onsetof diastole in the BSM configuration, while this con-centrated inlet jet does not appear until later in thecardiac cycle for the CM valve configuration. Becauseof this, the BSM rotational flow develops earlier andcreates significant velocity near the wall of the deviceand results in adequate shear rates. Regurgitationthrough the CM valve served as a significant hindranceto the development of the rotational flow. As a result,we have selected and are using the BSM valve for theclinical device.
We further explored how during myocardial recov-ery, the PVAD must be weaned from the patient toprepare for explant.83 For pulsatile devices, this oftenincludes a reduction in flow rate, which can change thefluid dynamics of the device. These changes in flowneed to be monitored because strong diastolic rota-tional flow, no areas of blood stasis, low blood resi-dence time and wall shear rates above 500 s�1, can helpprevent thrombus deposition. Using PIV, we observedthe planar flow patterns and wall shear rates at both anormal operating condition and a reduced beat rate.
FIGURE 13. Mean PIV flow maps in the 11 mm plane at (a) 300, (b) 400, (c) 550, and (d) 700 ms for the CM valve configurationillustrating the time history of the rotational flow pattern. (From Cooper et al.24 with permission).
FIGURE 14. Surface locations (S1–S7) used in wall shearcalculations for both valve configurations. (From Cooperet al.24 with permission).
Non-Thrombogenic Performance of Blood Recirculating Devices 1251

FIGURE 15. Non-dimensionalized wall shear maps for the BSM (left column) and CM (right column) valve configurations in the11 mm plane for Surface 1 (a, b), Surface 2 (c, d), and Surface 3 (e, f). Areas of interest are highlighted with ovals. Note that the walllocations are defined in a counter-clockwise fashion. (From Cooper et al.24 with permission).
BLUESTEIN et al.1252

At the reduced beat rate, the PVAD showed an earlierloss of rotational pattern, increased blood residencetime, and an overall reduction in wall shear rate at theouter walls. Because this reduction in flow rate couldlead to a possible increase in thrombus deposition, itmay be necessary to look into other options forweaning a patient from the PVAD. We furtherexplored altering operation of the PVAD during timesof weaning.25 In an effort to develop a strong inlet jetand rotational flow pattern at a lower beat (50 bpm)and flow rate; we compressed diastole by altering theend-diastolic delay time (EDD). Particle image veloc-imetry was used to compare the flow fields and wallshear rates in the chamber of the 12 cc PVAD usingEDDs of 10, 50, and 100 ms. While we expected the100 ms end-diastolic delay to have the best wall shearprofiles, however, we found that the 50 ms EDDcondition was superior to both the 10 and 100 EDDconditions, due to a longer sustained inlet jet.
These experimental and computational studiesprovide the foundation for a methodology to improveventricular assist devices (including pulsatile bloodpumps) that still suffer from thromboembolic events.By integrating EFD and CFD during the design phase,we will help facilitate improved device performanceclinically by correlating the results to in vivo animalstudies. However, in vitro blood studies still need to beperformed to fundamentally understand how wallshear rate and exposure time are related to thrombusdeposition in pulsatile flows.
SUMMARY
The work presented in this article represents onlyfew efforts by several groups working in the field whotackle the daunting goal of developing methodologiesthat may facilitate optimizing the thrombogenic per-formance of blood recirculating devices. This workincludes state-of-the-art numerical and experimentaltools used to elucidate flow-induced mechanismsleading to thromboembolism in prosthetic devices.Design of MHV and VADs is traditionally concernedwith hemocompatibility, durability, and thrombore-sistance, with hemodynamic characteristics somewhattaking a backseat. Hemodynamic optimization isaimed at avoiding the formation of stagnant zones andregions of elevated stresses, while achieving goodwashout characteristics. Traditional design matrixapproaches for optimizing devices are only of limitedutility, as the optimization process is very specific tothe device design characteristics and its inherent geo-metric constraints. Accordingly, in the cardiovasculardevice industry, designing and manufacturing device
prototypes and testing them ad hoc represents a com-mon practice.
Elucidating the hemodynamics of devices viasophisticated fluid dynamics and thrombogenic testingis far from trivial, and the identification and/or inter-pretation of pertinent design parameters is subtle. Withthe inherent design constraints of blood recirculatingdevices this is clearly a formidable challenge. Whilethere are no established set of parameters for achievingdesign optimization, the ultimate goal is to minimizethe thrombogenicity of the device—preferably to alevel that will not require anticoagulation (as is the casefor bioprosthetic valves for example). Clearly, a mod-eling approach represents an efficient way to econom-ically test design modifications to realize whether theyindeed achieve this design goal. However, it requires anumerical approach that goes beyond the commonquantitative flow mapping within the device—a non-trivial undertaking to begin with, given the complexityof the geometries in devices and the complex nature ofblood as a fluid. It should incorporate an accountablemodel that is able to provide quantitatively accuratepredictions of flow-induced blood hemoastatic activa-tion, resulting from accurately resolved flow fieldswithin the device and the stresses they induce on theblood borne particulates. It should also be noted that amodeling approach should be coupled with an exper-imental approach, to validate the models predictionsand ultimately to test whether the methodologydeveloped indeed led to optimizing the thrombogenicperformance of the device. The work presented heredemonstrate that experimental fluid mechanics, com-putational fluid dynamics and in vivo studies can belinked and together, contribute towards the develop-ment of ventricular assist devices in which thrombusdeposition and thromboemboli formation could beminimized. This methodology can be extrapolated toother cardiovascular prosthetic devices. It points toseveral directions that should be pursued in the futurein order to achieve the goal for blood recirculatingprosthetic devices becoming more effective as destina-tion therapy in the future.
REFERENCES
1Aarts, P. A., S. A. van den Broek, G. W. Prins, G. D.Kuiken, J. J. Sixma, and R. M. Heethaar. Blood plateletsare concentrated near the wall and red blood cells, in thecenter in flowing blood. Arteriosclerosis 8(6):819–824,1988.2Affeld, K., L. Goubergrits, U. Kertzscher, J. Gadischke,and A. Reininger. Mathematical model of platelet deposi-tion under flow conditions. Int. J. Artif. Organs 27(8):699–708, 2004.
Non-Thrombogenic Performance of Blood Recirculating Devices 1253

3Alemu, Y., and D. Bluestein. Flow-induced platelet acti-vation and damage accumulation in a mechanical heartvalve: numerical studies. Artif. Organs 31(9):677–688,2007.4AlMomani, T., H. S. Udaykumar, J. S. Marshall, andK. B. Chandran. Micro-scale dynamic simulation oferythrocyte-platelet interaction in blood flow. Ann. Bio-med. Eng. 36(6):905–920, 2008.5Apel, J., F. Neudel, and H. Reul. Computational fluiddynamics and experimental validation of a microaxialblood pump. ASAIO J. 47(5):552–558, 2001.6Apel, J., R. Paul, S. Klaus, T. Siess, and H. Reul.Assessment of hemolysis related quantities in a microaxialblood pump by computational fluid dynamics. Artif.Organs 25(5):341–347, 2001.7Bachmann, C. H. G., G. Rosenberg, S. Deutsch,A. Fontaine, and J. M. Tarbell. Fluid dynamics of a pediatricventricular assist device. Artif. Organs 24:362–372, 2000.8Bludszuweit, C. Model for a general mechanical blooddamage prediction. Artif. Organs 19(7):583–589, 1995.9Bludszuweit, C. Three-dimensional numerical prediction ofstress loading of blood particles in a centrifugal pump.Artif. Organs 19(7):590–596, 1995.
10Bluestein, D. Stent-induced thromboembolism. Ann. Bio-med. Eng. 28(3):346–350, 2000.
11Bluestein, D., C. Gutierrez, M. Londono, and R. T.Schoephoerster. Vortex shedding in steady flow through amodel of an arterial stenosis and its relevance to muralplatelet deposition. Ann. Biomed. Eng. 27(6):763–773, 1999.
12Bluestein, D., Y. M. Li, and I. B. Krukenkamp. Freeemboli formation in the wake of bi-leaflet mechanical heartvalves and the effects of implantation techniques. J. Bio-mech. 35(12):1533–1540, 2002.
13Bluestein, D., L. Niu, R. T. Schoephoerster, and M. K.Dewanjee. Fluid mechanics of arterial stenosis: relationshipto the development of mural thrombus. Ann. Biomed. Eng.25(2):344–356, 1997.
14Bluestein, D., L. Niu, R. T. Schoephoerster, and M. K.Dewanjee. Steady flow in an aneurysm model: correlationbetween fluid dynamics and blood platelet deposition.J. Biomech. Eng. 118(3):280–286, 1996.
15Bluestein, D., E. Rambod, and M. Gharib. Vortex shed-ding as a mechanism for free emboli formation inmechanical heart valves. J. Biomech. Eng. 122(2):125–134,2000.
16Bluestein, D., W. Yin, K. Affeld, and J. Jesty. Flow-induced platelet activation in a mechanical heart valve.J. Heart Valve Dis. 13(3):501–508, 2004.
17Bluestein, M., and L. F. Mockros. Hemolytic effects ofenergy dissipation in flowing blood. Med. Biol. Eng. 7(1):1–16, 1969.
18Buchanan, Jr., J. R., C. Kleinstreuer, and J. K. Comer.Rheological effects on pulsatile hemodynamics in a ste-nosed tube. Comput. Fluids 29(6):695–724, 2000.
19Burgreen, G. W., J. F. Antaki, and B. P. Griffith. A designimprovement strategy for axial blood pumps using com-putational fluid dynamics. ASAIO J. 42(5):M354–M360,1996.
20Burgreen, G. W., J. F. Antaki, Z. J. Wu, and A. J. Holmes.Computational fluid dynamics as a development tool forrotary blood pumps. Artif. Organs 25(5):336–340, 2001.
21Chandran, K. B., C. S. Lee, S. Aluri, K. C. Dellsperger,S. Schreck, and D. W. Wieting. Pressure distribution nearthe occluders and impact forces on the outlet struts of
Bjork-Shiley convexo-concave valves during closing.J. Heart Valve Dis. 5(2):199–206, 1996.
22Cheng, R., Y. G. Lai, and K. B. Chandran. Three-dimen-sional fluid-structure interaction simulation of bileafletmechanical heart valve flow dynamics. Ann. Biomed. Eng.32(11):1471–1483, 2004.
23Cheng, R., Y. G. Lai, and K. B. Chandran. Two-dimen-sional fluid-structure interaction simulation of bileafletmechanical heart valve flow dynamics. J. Heart Valve Dis.12(6):772–780, 2003.
24Cooper, B. T., B. N. Roszelle, T. C. Long, S. Deutsch, andK. B. Manning. The 12 cc Penn State pulsatile pediatricventricular assist device: fluid dynamics associated withvalve selection. J. Biomech. Eng. 130:041019, 2008.
25Cooper, B. T., B. N. Roszelle, T. C. Long, S. Deutsch, andK. B. Manning. The influence of operational protocol onthe fluid dynamics in the 12 cc Penn State pulsatile pedi-atric ventricular assist device: the effect of end-diastolicdelay. Artif. Organs, 2010 (in press).
26David, T., S. Thomas, and P. G. Walker. Platelet deposi-tion in stagnation point flow: an analytical and computa-tional simulation. Med. Eng. Phys. 23(5):299–312, 2001.
27Deutsch, S., J. M. Tarbell, K. B. Manning, G. Rosenberg,and A. A. Fontaine. Experimental fluid mechanics of pul-satile artificial blood pumps. Annu. Rev. Fluid Mech. 38:65–86, 2006.
28Dowling, R. D., S. W. Etoch, K. A. Stevens, A. C.Johnson, and L. A., Gray, Jr. Current status of the Abio-Cor implantable replacement heart. Ann. Thorac. Surg.71(3 Suppl):S147–S149, 2001; discussion S183–S144.
29Dumont, K., J. Vierendeels, G. van Nooten, P. Verdonck,and D. Bluestein. Comparison of ATS open pivot valveand St Jude Regent Valve using a CFD model based onfluid-structure interaction. J. Biomech. Eng. 129(4), 2007.
30Eckstein, E. C., D. L. Bilsker, C. M. Waters,J. S. Kippenhan, and A. W. Tilles. Transport of plateletsin flowing blood. Ann. N. Y. Acad. Sci. 516:442–452,1987.
31El-Banayosy, A., R. Korfer, L. Arusoglu, L. Kizner,M. Morshuis, H. Milting, G. Tenderich, O. Fey, andK. Minami. Device and patient management in a bridge-to-transplant setting. Ann. Thorac. Surg. 71(3 Suppl):S98–S102, 2001; discussion S114–S105.
32Fogelson, A. L., and N. T. Wang. Platelet dense-granulecentralization and the persistence of ADP secretion. Am. J.Physiol. 270(3 Pt 2):H1131–H1140, 1996.
33Garon, A., and M.-I. Farinas. Fast three-dimensionalnumerical hemolysis approximation. Artif. Organs28(11):1016–1025, 2004.
34Ge, L., L. P. Dasi, F. Sotiropoulos, and A. P. Yoganathan.Characterization of hemodynamic forces induced bymechanical heart valves: Reynolds vs. viscous stresses. Ann.Biomed. Eng. 36(2):276–297, 2008.
35Ge, L., S. C. Jones, F. Sotiropoulos, T. M. Healy, and A. P.Yoganathan. Numerical simulation of flow in mechanicalheart valves: grid resolution and the assumption of flowsymmetry. J. Biomech. Eng. 125(5):709–718, 2003.
36Ge, L., H. L. Leo, F. Sotiropoulos, and A. P. Yoganathan.Flow in a mechanical bileaflet heart valve at laminar andnear-peak systole flow rates: CFD simulations and experi-ments. J. Biomech. Eng. 127(5):782–797, 2005.
37Gosman, A., and L. Ioannides. Aspects of compuer simu-lation of liquid-fueled cumbustors. In: AIAA 19th Aero-space Science Meeting, 81-0323, 1981.
BLUESTEIN et al.1254

38Gosman, A., and L. Ioannides. Aspects of computer sim-ulation of liquid-fuelled combustors. AIAA J. Energy7(6):482–490, 1983.
39Goubergrits, L., and K. Affeld. Numerical estimation ofblood damage in artificial organs. Artif. Organs 28(5):499–507, 2004.
40Goubergrits, L., K. Affeld, and U. Kertzscher. Innovativedevelopments of the heart valves designed for use in ven-tricular assist devices. Expert Rev. Med. Devices 2(1):61–71,2005.
41Govindarajan, V., H. S. Udaykumar, and K. B. Chandran.Two-dimensional simulation of flow and platelet dynamicsin the hinge region of a mechanical heart valve. J. Biomech.Eng. 131:031002-1–031002-12, 2009.
42Grosset, D. G., D. Georgiadis, A. W. Kelman, P. Cowburn,S. Stirling, K. R. Lees, A. Faichney, A. Mallinson, R. Quin,I. Bone, L. Pettigrew, E. Brodie, T. MacKay, and D. J.Wheatley. Detection of microemboli by transcranialDoppler ultrasound.Tex.Heart Inst. J. 23(4):289–292, 1996.
43Guezuraga, R. M., and D. Y. Steinbring. View fromindustry. Eur. J. Cardiothorac. Surg. 26(Suppl 1):S19–S23,2004; discussion S23–S26.
44Harker, L. A., and S. J. Slichter. Studies of platelet andfibrinogen kinetics in patients with prosthetic heart valves.N. Engl. J. Med. 283(24):1302–1305, 1970.
45Healy, T. M., J. T. Ellis, A. A. Fontaine, C. A. Jarrett, andA. P. Yoganathan. An automated method for analysis andvisualization of laser Doppler velocimetry data. Ann. Bio-med. Eng. 25(2):335–343, 1997.
46Hochareon, P. M. K., A. A. Fontaine, J. M. Tarbell, andS. Deutsch. Correlation of in vivo clot deposition with theflow characteristics in the 50 cc Penn state artificial heart: apreliminary study. ASAIO J. 50:537–542, 2004.
47Hochareon, P. M. K., A. A. Fontaine, J. M. Tarbell, andS. Deutsch. Fluid dynamic analysis of the 50 cc Penn Stateartificial heart under physiological operating conditionsusing particle image velocimetry. J. Biomech. Eng. 126:585–593, 2004.
48Hochareon, P. M. K., A. A. Fontaine, J. M. Tarbell, andS. Deutsch. Wall shear-rate estimation within the 50 ccPenn State artificial heart using particle image velocimetry.J. Biomech. Eng. 126:430–437, 2004.
49Huang, Z. J., C. L. Merkle, S. Abdallah, and J. M. Tarbell.Numerical simulation of unsteady laminar flow through atilting disk heart valve: prediction of vortex shedding.J. Biomech. 27(4):391–402, 1994.
50Hubbell, J. A. M. L. Visualization and analysis of muralthrombogenesis on collagen, polyurethane and nylon.Biomaterials 7:354–363, 1986.
51Jesty, J., and D. Bluestein. Acetylated prothrombin as asubstrate in the measurement of the procoagulant activityof platelets: elimination of the feedback activation ofplatelets by thrombin. Anal. Biochem. 272(1):64–70, 1999.
52Jesty, J., and Y. Nemerson. The pathways of blood coag-ulation, Chap. 122. In: Williams Hematology, edited byE. Beutler, M. A. Lichtman, B. S. Coller, and T. J. Kipps.New York: McGraw-Hill, 1995, pp. 1227–1238.
53Jesty, J., W. Yin, P. Perrotta, and D. Bluestein. Platelet acti-vation in a circulating flow loop: combined effects of shearstress and exposure time. Platelets 14(3):143–149, 2003.
54Jin, W., and C. Clark. Experimental investigation of un-steady flow behaviour within a sac-type ventricular assistdevice (VAD). J. Biomech. 26(6):697–707, 1993.
55Kafesjian, R., M. Howanec, G. D. Ward, L. Diep, L. S.Wagstaff, and R. Rhee. Cavitation damage of pyrolytic
carbon in mechanical heart valves. J. Heart Valve Dis.3(Suppl 1):S2–S7, 1994.
56Kawahito, K., H. Adachi, and T. Ino. Platelet activationin the gyro C1E3 centrifugal pump: comparison with theterumo capiox and the Nikkiso HPM-15. Artif. Organs24(11):889–892, 2000.
57Kelly, S. G., P. R. Verdonck, J. A. Vierendeels,K. Riemslagh, E. Dick, and G. G. Van Nooten. A three-dimensional analysis of flow in the pivot regions of an ATSbileaflet valve. Int. J. Artif. Organs 22(11):754–763, 1999.
58King, M. J., T. David, and J. Fisher. Three-dimensionalstudy of the effect of two leaflet opening angles on the time-dependent flow through a bileaflet mechanical heart valve.Med. Eng. Phys. 19(3):235–241, 1997.
59Kini, V., C. Bachmann, A. Fontaine, S. Deutsch, and J. M.Tarbell. Integrating particle image velocimetry and laserDoppler velocimetry measurements of the regurgitant flowfield past mechanical heart valves. Artif. Organs 25(2):136–145, 2001.
60Kiris, C., D. Kwak, S. Rogers, and I. D. Chang. Compu-tational approach for probing the flow through artificialheart devices. J. Biomech. Eng. 119(4):452–460, 1997.
61Klaus, S., S. Korfer, K. Mottaghy, H. Reul, andB. Glasmacher. In vitro blood damage by high shear flow:human versus porcine blood. Int. J. Artif. Organs25(4):306–312, 2002.
62Krafczyk, M., M. Cerrolaza, M. Schulz, and E. Rank.Analysis of 3D transient blood flow passing through anartificial aortic valve by Lattice-Boltzmann methods.J. Biomech. 31(5):453–462, 1998.
63Krishnan, S., H. S. Udaykumar, J. S. Marshall, and K. B.Chandran. Two-dimensional dynamic simulation of plate-let activation during mechanical heart valve closure. Ann.Biomed. Eng. 34(10):1519–1534, 2006.
64Kuharsky, A. L., and A. L. Fogelson. Surface-mediatedcontrol of blood coagulation: the role of binding site den-sities and platelet deposition. Biophys. J. 80(3):1050–1074,2001.
65Laas, J., P. Kleine, M. J. Hasenkam, and H. Nygaard.Orientation of tilting disc and bileaflet aortic valve substi-tutes for optimal hemodynamics. Ann. Thorac. Surg.68(3):1096–1099, 1999.
66Laas, J., S. Kseibi, M. Perthel, A. Klingbeil, L. El-Ayoubi,and A. Alken. Impact of high intensity transient signals onthe choice of mechanical aortic valve substitutes. Eur. J.Cardiothorac. Surg. 23(1):93–96, 2003.
67Lamson, T. C., G. Rosenberg, D. B. Geselowitz,S. Deutsch, D. R. Stinebring, J. A. Frangos, and J. M.Tarbell. Relative blood damage in the three phases of aprosthetic heart valve flow cycle. ASAIO J. 39(3):M626–M633, 1993.
68Lazar, R. M., P. A. Shapiro, B. E. Jaski, M. K. Parides,R. C. Bourge, J. T. Watson, L. Damme, W. Dembitsky,J. D. Hosenpud, L. Gupta, A. Tierney, T. Kraus, andY. Naka. Neurological events during long-term mechanicalcirculatory support for heart failure: the RandomizedEvaluation of Mechanical Assistance for the Treatmentof Congestive Heart Failure (REMATCH) experience.Circulation 109(20):2423–2427, 2004.
69Lee, C. S., K. B. Chandran, and L. D. Chen. Cavitationdynamics of medtronic hall mechanical heart valve pros-thesis: fluid squeezing effect. J. Biomech. Eng. 118(1):97–105, 1996.
70Long, J. A. U. A., K. B. Manning, and S. Deutsch. Vis-coelasticity of pediatric blood and its implications for the
Non-Thrombogenic Performance of Blood Recirculating Devices 1255

testing of a pulsatile pediatric blood pump. ASAIO J.51:563–566, 2005.
71Mackay, T. G., D. Georgiadis, D. G. Grosset, K. R. Lees,and D. J. Wheatley. On the origin of cerebrovascularmicroemboli associated with prosthetic heart valves. Neu-rol. Res. 17(5):349–352, 1995.
72Makhijani, V. B., H. Q. Yang, A. K. Singhal, and N. H.Hwang. An experimental-computational analysis of MHVcavitation: effects of leaflet squeezing and rebound.J. Heart Valve Dis. 3(Suppl 1):S35–S44, 1994; discussionS44–S38.
73Mann, K. A. D. S., J. M. Tarbell, D. B. Geselowitz,G. Rosenberg, and W. S. Pierce. An experimental study ofNewtonian and non-Newtonian flow dynamics in a ven-tricular assist device. J. Biomech. Eng. 109:139–147, 1987.
74Manning, K. B. W. B., N. Yang, A. Fontaine, andS. Deutsch. Flow behavior within the 12 cc Penn Statepulsatile pediatric ventricular assist device: an experimentalstudy of the initial design. Artif. Organs 32:442–452, 2008.
75Medvitz, R. B., J. W. Kreider, K. B. Manning, A. A.Fontaine, S. Deutsch, and E. G. Paterson. Developmentand validation of a computational fluid dynamics meth-odology for simulation of pulsatile left ventricular assistdevices. ASAIO J. 53:122–131, 2007.
76NHLBI Working Group R.R.c., T. Baldwin (NHLBI),et al. Next Generation Ventricular Assist Devices forDestination Therapy, Working Group Executive Summary.National Heart Lungs and Blood Institute, 2004.
77Nobili, M., J. Sheriff, U. Morbiducci, A. Redaelli, andD. Bluestein. Platelet activation due to hemodynamic shearstresses: damage accumulation model and comparison toin vitro measurements. ASAIO J. 54(1):64–72, 2008.
78O’Brien, J. R. Shear-induced platelet aggregation. Lancet335(8691):711–713, 1990.
79O’Brien, J. R., and G. P. Salmon. An independent hae-mostatic mechanism: shear induced platelet aggregation.Adv. Exp. Med. Biol. 281:287–296, 1990.
80Paul, R., O. Marseille, E. Hintze, L. Huber, H. Schima,H. Reul, and G. Rau. In vitro thrombogenicity testing ofartificial organs. Int. J. Artif. Organs 21(9):548–552, 1998.
81Reininger, C. B., R. Lasser, M. Rumitz, C. Boger, andL. Schweiberer. Computational analysis of platelet adhe-sion and aggregation under stagnation point flow condi-tions. Comput. Biol. Med. 29(1):1–18, 1999.
82Rose, E. A., A. J. Moskowitz, M. Packer, J. A. Sollano,D. L. Williams, A. R. Tierney, D. F. Heitjan, P. Meier,D. D. Ascheim, R. G. Levitan, A. D. Weinberg, L. W.Stevenson, P. A. Shapiro, R. M. Lazar, J. T. Watson, D. J.Goldstein, and A. C. Gelijns. The REMATCH trial:rationale, design, and end points. Randomized Evaluationof Mechanical Assistance for the Treatment of CongestiveHeart Failure. Ann. Thorac. Surg. 67(3):723–730, 1999.
83Roszelle, B. N. C. B., T. C. Long, S. Deutsch, and K. B.Manning. The 12 cc Penn State pulsatile pediatric ventricu-lar assist device: flow field observations at a reduced beat ratewith application to weaning. ASAIO J. 54:325–331, 2008.
84Schima, H., M. R. Muller, D. Papantonis, C. Schlusche,L. Huber, C. Schmidt, W. Trubel, H. Thoma, U. Losert,and E. Wolner. Minimization of hemolysis in centrifugalblood pumps: influence of different geometries. Int. J. Artif.Organs 16(7):521–529, 1993.
85Schima, H., H. Siegl, S. F. Mohammad, L. Huber, M. R.Muller, U. Losert, H. Thoma, and E. Wolner. In vitroinvestigation of thrombogenesis in rotary blood pumps.Artif. Organs 17(7):605–608, 1993.
86Schima, H., and G. Wieselthaler. Mechanically inducedblood trauma: are the relevant questions already solved, oris it still an important field to be investigated? Artif. Organs19(7):563–564, 1995.
87Sorensen, E. N., G. W. Burgreen, W. R. Wagner, and J. F.Antaki. Computational simulation of platelet depositionand activation: I. Model development and properties. Ann.Biomed. Eng. 27(4):436–448, 1999.
88Sorensen, E. N., G. W. Burgreen, W. R. Wagner, and J. F.Antaki. Computational simulation of platelet depositionand activation: II. Results for Poiseuille flow over collagen.Ann. Biomed. Eng. 27(4):449–458, 1999.
89Stevenson, L. W., L. W. Miller, P. Desvigne-Nickens, et al.Left ventricular assist device as destination for patientsundergoing intravenous inotropic therapy: a subset analysisfrom REMATCH (Randomized Evaluation of MechanicalAssistance in Treatment of Chronic Heart Failure). Circu-lation 110:975–981, 2004.
90Turitto, V. T., and H. J. Weiss. Red blood cells: their dualrole in thrombus formation. Science 207(4430):541–543,1980.
91Worth Longest, P., and C. Kleinstreuer. Comparisonof blood particle deposition models for non-parallel flowdomains. J. Biomech. 36(3):421–430, 2003.
92Wurzinger, L. J., P. Blasberg, and H. Schmid-Schonbein.Towards a concept of thrombosis in accelerated flow:rheology, fluid dynamics, and biochemistry. Biorheology22(5):437–450, 1985.
93Yamanaka, H. R. G., W. J. Weiss, A. J. Snyder, C. M.Zapanta, and C. A. Siedlecki. Short-term in vivo studies ofsurface thrombosis in a left ventricular assist system.ASAIO J. 52:257–265, 2006.
94Yin, W., Y. Alemu, K. Affeld, J. Jesty, and D. Bluestein.Flow-induced platelet activation in bileaflet and mono-leaflet mechanical heart valves. Ann. Biomed. Eng.32(8):1058–1066, 2004.
95Yin, W., S. Gallocher, L. Pinchuk, R. T. Schoephoerster,J. Jesty, and D. Bluestein. Flow induced platelet activationin a St. Jude MHV, a trileaflet polymeric heart valve anda St. Jude tissue valve. Artif. Organs 29(10):826–831,2005.
96Yoganathan, A. P., K. B. Chandran, and F. Sotiropoulos.Flow in prosthetic heart valves: state-of-the-art and futuredirections. Ann. Biomed. Eng. 33(12):1689–1694, 2005.
97Yoganathan, A. P., J. T. Ellis, T. M. Healy, and G. P.Chatzimavroudis. Fluid dynamic studies for the year 2000.J. Heart Valve Dis. 7(2):130–139, 1998.
BLUESTEIN et al.1256