Embed Size (px)
Citation preview

1
Towards an ElderCare Living Lab for Sensor-BasedHealth Assessment and Physical Therapy
Prasad Calyam, Isa Jahnke, Anup Mishra, Ronny Bazan Antequera, Dmitrii Chemodanov, Marjorie SkubicUniversity of Missouri-Columbia
Email: {calyamp, jahnkei, skubicm}@missouri.edu; {akmm94, rcb553, dycbt4}@mail.missouri.edu
Abstract—There is an increasing demand to develop innova-tions in eldercare technologies that can be delivered as ‘Apps’ ata cloud-scale to facilitate proactive monitoring and targeted carecoordination. This article presents the design for an ‘ElderCare-as-a-SmartService’ (ECaaS) system that integrates Apps for in-home health monitoring, and remote physical therapy coaching,respectively. The focus is on the transformation of the Appsinto a cloud-based living lab, which then enables on-going Appdevelopment/refinement to realize a real-world enhanced livingenvironment for eldercare that is secure, privacy-preserving andsocially embedded. We detail the system and network require-ments for cloud-based delivery of ECaaS Apps featuring sensordata analysis and interactive interfaces across urban, suburbanand rural areas. We conclude with a proposal for sociotechnicalinvestigations that can be lead to a human-centered design thatengages older adults and care coordinators as co-developers ofECaaS, while also simultaneously improving their quality of life.
Index Terms—ElderCare Smart Service, Remote HealthcareApps, Living Lab Design
I. INTRODUCTION
As they age, many older adults have significant challenges inmanaging chronic health conditions and maintaining physicalfunctions. Early detection of health problems can help eldersmaintain good health and function by allowing timely healthinterventions. Traditional approaches of healthcare take placein medical centers or clinics, which require availability oftransportation from the home. This is, however, a disadvantagefor rural and sometimes suburban areas where travel distancescan be very long. With emerging digital technology and multi-sensor techniques, new approaches for on-going health assess-ment are emerging to realize enhanced living environments(ELEs) for eldercare. While older adults stay in the home oftheir choice, in-home sensors can be used to monitor olderadults’ activity patterns; smart algorithms recognize changesin the patterns and send health alerts to care coordinators toflag potential health changes and administer targeted coaching.
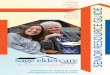
Our previous studies [1] have shown that in-home sensordata from bed, motion, and gait sensors, gathered using webservices in an “App” form, can automatically provide on-goinghealth assessments without being obtrusive. Although they caneven alert care givers when the system detects health changes,alert notifications capability as provided in our App-1 are notenough. In our App-2 work [2], we have also shown howcare coordinators can provide active corrective health coachingby real-time analysis of large amount of data from patient’shomes using a cloud platform. An example use case of App-2 is illustrated in Figure 1, where an interface is shown thatwe developed for a Physical Therapist (PT) at a clinic. TheApp helps the PT interact with an older adult in a home toassess his/her mental and physical health status through guidedphysical exercises designed to overcome fall risk.
Fig. 1. Screenshot of the Physical Therapist view of the Interactive Interface(left side shows the patient, right side shows the PT, right side top alignmentparameters are informed by depth sensor data and exercise activities areadministered using voice commands).
In order to deliver such cloud-based Apps within ELEs foreldercare, the challenges that arise include: (a) ensuring stablenetwork performance and performance-tuned cloud platformsfor large-scale sensor information analysis; (b) interactive in-terface and intuitive displays suitable for effective interactionsbetween older adults and PTs, and (c) the integration of Appsin their social context of use as secure, privacy-preserving andsocially-embedded technologies.
Our pilot studies and conceptual work address these chal-lenges in order to satisfy the needs of independent living,where older adults have the choice to remain in their privatehomes supported through a combination of on-going healthmonitoring and alerts along with access to on-demand re-mote physical therapy. In this paper, we describe the designof ElderCare-as-a-SmartService (ECaaS) along with relatedtechnical and sociotechnical challenges [3] when movingfrom sandbox settings in our prior works into a living labenvironment, and its ultimate transformation into a real-worldELE for eldercare. Towards realizing this vision, we seek toanswer bold research questions such as:
• What new kinds of web services and cloud platformissues, particularly in networking need to be investigatedto deliver an effective, efficient, secure and privacy-preserving smart service system such as the ECaaS?
• How can technology play a role in the future to improveremote accessibility of ECaaS Apps? How to assesswhether new ECaaS App delivery would be the sameor different from either of the urban, suburban and ruraluser perspectives?

2
• What are affordances of the smart service system in anECaaS implementation? How should the implementationbe planned with regard to usability, sociotechnical andhuman-centered integration?
• What new kinds of clinical studies can be enabled by theECaaS Apps to see: (a) how much longer older adultslive, (b) does it enable the family to be more aware ofhealth status of older adults while allowing autonomyduring aging in place, and (c) to what extent does ECaaSsave money and improve care as well as quality of life?
The goal of our design of ECaaS and associated Apps isto ultimately develop and install on-going health assessmentmaking it accessible for a broader group of older adults andphysical therapy clinics. Towards this goal, we integrate LivingLab approaches and User Experience principles. This helpsus to prepare data-driven reflections for revisiting old andnew design decisions and fosters future development of cloud-based services that can be delivered in ELEs for eldercare.
II. RELATED WORK
Monitoring patients in the home for ongoing health assess-ment has typically been done using telehealth methods [4].Particularly for monitoring known chronic health conditions,prior works use network-connected devices placed in thehome, such as a weighing scale and a blood pressure cuff.The patient is expected to use these devices on a regularschedule such as once or twice a day. The data from thenetworked devices can be automatically transferred to a remoteserver for storage in the patient’s health record. Several studieshave shown that adherence with telehealth programs decreasesover time [4]. Moreover, such approaches collect only a smallnumber of data points per day, and do not have the capabilityof monitoring and detecting changes in walking gait, sleeppatterns, or daily activity patterns.
Our App-1 [1] overcomes the above limitation by monitor-ing walking gait that is particularly useful for tracking healthchanges. This is because, gait decline can be correlated with avariety of changes in physical, mental, or cognitive health [5].Existing methods for measuring gait are typically infrequentand provide coarse measurements, e.g., observation by a clin-ician who might use a stop watch for assessment during clinicvisits that occur once every 6 or 12 months. Those methodsoften lead to few or no objective assessments, which limitresults, and therefore do not catch a person’s functional declinein a timely manner [5]. Our App-1 also builds upon newmethods that use sensor technology to measure gait parameterson a continuous basis during normal daily activities. Using in-home sensor technology mounted in the patient environment,tangible information can be obtained for a variety of purposesincluding automated fall risk assessments, early detection ofillness or change in health status, and better assessment ofprogress during rehabilitation or change in medication.
Vision sensors have also been proposed for home use inworks such as [6]. Video cameras offer the potential to trackmore detailed gait information as well as other activities.However, they require calibration and more computationalresources and are sensitive to lighting variations. In addition,many consumers consider video cameras in the home tobe a privacy invasion, although privacy protection methodscan be applied to address this problem, such as the use of
silhouettes [7]. Our App-1 uses the approach of depth sensingusing a depth camera in a Microsoft Kinect that captures adistance measure for each pixel. The potential of the sensoris that it offers a single, low cost sensor device and capturesa three dimensional (3D) representation of the environment asshown in Figure 2. Because it captures a depth image withonly shape data instead of more recognizable video images, itis deemed to be privacy-preserving. The Kinect depth sensorimages are also used in our App-2 in cases where much lesscomputational resources are necessary compared to processinglong-periods of video camera streams.
Fig. 2. A walk captured in a private home using a depth sensor.
Our adoption context for Kinect depth sensors in monitoringof gait in App-1 and other physical activities in App-2 isnovel. There is prior work in [8], where the authors proposea method for extracting joint locations from a side view,which the Microsoft SDK (software-development kit) doesnot support. However, this has not been adapted for use ina naturalistic, unstructured home setting. In addition, there isprior work on tracking gait in the home using the MicrosoftSDK [9]. However, this is restricted to a limited viewingarea, corresponding to the constrained gaming region. Ourwork addresses many of these limitations [10]. We track gaitparameters of walking speed, stride length, and stride timeover observation time windows in multiple residential homes.Gait change and fall risk is automatically detected, whichresult in health alerts being sent to clinical staff. We havealso validated the gait measurements in the lab using goldstandard marker-based motion capture to ensure that the gaitparameters extracted in the home are accurate.
The added novelty of our work is in our design to leveragethe existing Apps 1 and 2 over broadband networks and a cloudplatform via new interactive interfaces for both cliniciansand older adults as shown previously in an example usecase in Figure 1. The work closest to ours is the workin [11], where a cloud-based solution is proposed for a contextmanagement system in ambient assisted living cases. Thesolution features a decision support middleware to processand visualize large amounts of medical and other ambiencemonitoring data in real-time from a multitude of sensors andembedded devices. Two other works [12] and [13] adoptedsimilar cloud-based approaches for eldercare, but focused onsystems that support smart mobile companion robots that canbe accessed via teleoperation. The authors in [12] implementeda system that uses WebRTC, Google App Engine and a fuzzylogic based software for reactive navigation capabilities duringteleoperation with safety considerations such as e.g., avoidingobstacles. Similarly, authors in [13] developed a system thatuses cloud computing for data computation tasks in supportof robotic localization and monitoring services to empower acare giver to simultaneously manage multiple elderly patients.

3
Fig. 3. Remote Physical Therapy; Immersive interactions between the PT and the Patient (older adult) using a network overlay setup.
III. ECAAS DESIGN AND DEVELOPMENT REQUIREMENTS
We envision the ECaaS design to mimic a smart service sys-tem that integrates the two primary Apps we have previouslydeveloped using isolated sandbox approaches. In this section,we first provide our App details. Next, we outline requirementsfor their transformation into a secure, privacy-preserving andembedded form within a real-world ELE for eldercare.
A. ECaaS AppsApp-1 is an in-home health alert system with remote care
coordination capabilities that is based on on-going analysis ofsensor data obtained unobtrusively from older adult homes [1].This App (voted ‘Best App in Health’ at the 2013 US IgniteSummit, Chicago) was developed for generation of healthalerts based on hydraulic bed sensors, motion sensors, Kinectdepth sensing for in-home gait analysis, and data analysisalgorithms from the University of Missouri. The project in-volved installation of sensor networks (each generates 23GB/person/week, even with compressed images) in 15 seniorapartments in Iowa, having motion, bed and gait sensing forone year. Health alerts that are based on e.g., changes in sleeppatterns were sent to clinical staff in Missouri and Iowa. Amajor outcome was the development of bed sensor hardwareand algorithms that capture pulse, respiration, and restlessnessof elders, while positioned under a mattress.
App-2 is an in-home remote physical therapy applicationthat is hosted within a GENI testbed (i.e., Global Environmentfor Network Innovation cloud infrastructure supported bythe National Science Foundation in the United States) andutilizes high-speed last-mile network connections [2]. ThisApp involved an interactive interface (see example screenshotshown previously in Figure 1) that connects a PT located at aclinic to an older adult at home as illustrated in Figure 3. App-2 has been developed using Kinect sensing technologies andhas been tested with five participants in Kansas City connectedthrough Google Fiber last-mile network connections. Majoroutcomes include the effectiveness of the PT interface throughquantitative and qualitative assessments on gait and balanceusing depth images and results of network performance tests.
Figure 4 shows an example set of measurements we col-lected during the laboratory testing and baseline performancecharacterization of our App-2. Specifically, the figure showsthe empirical CDF (cumulative distribution function) plots ofthe bandwidth consumption of various stream types (audio,skeletal, color, depth) individually and in an aggregate asobtained from the Kinect API calls. We can see that a single
PTaaS App session requires a peak of ≈ 200 Mbps end-to-end available bandwidth between therapist and patient sidesto exchange the various data streams.
Moreover, given that the performance of the PTaaS Appcan be affected due to network health factors (e.g., delay,jitter, packet loss), we have tested the controlled network pathbetween the patient and therapist sides. Thereby, we haveconfirmed expected and degraded behavior under good and badnetwork scenarios, respectively. We also identified the needfor integration of cloud-based services on GENI infrastructurefor the large data handling/analysis from the homes. Further,we have identified the need to deal with a lack of public IPaddress support in private homes with Google Fiber. Thesehave consequently led to our on-going investigations on Layer2 tunneling and related time synchronization for correlationanalysis of Kinect sensor data, therapist/senior user experience,RGB video, depth as well as skeletal data [2].
B. Smart Service System Challenges
Several open challenges need to be solved to go beyondour isolated sandbox approaches for the Apps in order to scalethem in a cloud-based smart service system of ECaaS that canbe widely deployed to urban, suburban and rural areas. OurECaaS vision is to make it suitable for embedded health as-sessment for: on-going assessment of health changes based onan individual’s behavior, activity patterns and baseline healthconditions. We also seek to foster remote access at older adulthomes involving frequent health assessments, physical therapysessions, and health interventions, especially for those withtransportation challenges, e.g., frail older adults who do notdrive, or those living in rural communities with long distancesto a PT clinic. In the following, we list the two salient designchallenges that we believe should be critically overcome totransform the ECaaS Apps to a living lab environment for on-going development that will ultimately result in a real-worldELE for eldercare.
1) Technical Architecture Design: The first challenge refersto provisioning of a technical networking capacity that cansupport the ECaaS, both with and without network pathsinvolving last-mile Gigabit fiber connections such as e.g.,Google Fiber. Given that the general assumption that all enduser sites will have very high-speed last-mile links is notpractical, we need to ensure that the Apps delivery worksproperly in cases where the end-to-end network performanceis unstable or not adequately tuned for satisfactory user

4
(a) (b) (c) (d) (e)
Fig. 4. Bandwidth consumption of different PTaaS data streams shown as empirical CDF plots: (a) audio stream; (b) skeletal stream that has the lowestbandwidth consumption; (c) video stream with medium bandwidth consumption; (d) depth data stream that shows the highest bandwidth consumption; (e) allstreams together nearly require ≈ 200 Mbps end-to-end available bandwidth between provider and home sides
experience. For instance, the App configurations should handlebottleneck cases such as e.g., where a PT might want to knowif the data from an older adult home is based on the actualgait measurements of balance or if the lags in the patientresponsiveness data is inaccurate because of network latencyor end-to-end available bandwidth problems.
2) Usability design of Apps: The second challenge pertainsto the delivery of the Apps for older adults and PTs throughuser-friendly and interactive/immersive interface displays. Thedisplays would need to be designed differently for the olderadults and PTs in terms of the feature sets and access controlsto sensor data and eldercare technology functions. Usabilityand user experience studies are required to provide the userinterface layout and system components design for deliverybest QoE to the care coordinators. This will involve iterativedevelopment with end users as co-designers right from thebeginning till regular use of the Apps in practice i.e., they willneed to help with the integration of the ‘Technical’ and the‘Social’ dimensions to make the Apps be ultimately deliveredas socially-embedded technologies within ELEs for eldercare.
IV. CLOUD-BASED ECAAS ARCHITECTURE
In this section, we present our vision of the cloud-basedECaaS architecture in terms of the network and computationinfrastructure components and cloud services. We also de-scribe our solutions that we obtained through experimentation,and prescribe web service development guidelines that canhelp realize the cloud-based ECaaS architecture in practice.
A. Network Infrastructure SolutionThe cloud-based ECaaS architecture relies on high-speed
broadband connections between the older adult’s home, theApp provider (i.e., the clinic) site, as well as the ECaaS Appshosted within a cloud infrastructure. In order to develop a ref-erence implementation of our proposed ECaaS architecture, wehave setup a novel peer-to-peer App deployment infrastructurethat integrates related technology components as illustrated inFigure 5. Our solution approach facilitates App services inter-communication, as well as is suitable for security purposesif sensitive information is being exchanged between the Appprovider and older adult sites. Further, to meet the large datamovement tasks in cloud service interactions, and to satisfythe real-time requirements in the sensor data analysis, wehave experimented with a variety of network configurationsfor network overlay setup between the various sites basedon virtual link (Layer 2) technologies. For the out-of-bandcommunications to support data processing with App-relateddata logs, we utilize regular Internet (Layer 3) protocols.
Fig. 5. Peer-to-peer cloud-hosted Gigabit App deployment infrastructurecomponents between provider (PT/clinic) and home user (patient).
Through extensive performance troubleshooting of softwareand hardware virtualization alternatives provided by the Bro-cade Vyatta vRouter, we have engineered the overlay paths tosatisfy the fast data movement requirements of video, audio,RGB, depth and skeletal data for real-time display of gait andother movement parameters at both ends. Given that privatehome access network connections in Google Fiberhoods aswell as in other home network settings do not have public IPaddresses, our overlay network solution was also helpful incases where our PT interactive interface (example screenshotshown previously in Figure 1) needed binding of ports betweenthe App provider and older adult home ends to allow customprotocol communications.
B. Computation Infrastructure Solution
MU’s hydraulic bed sensors as well sensors for motionand gait data collection are installed as part of the App-1 deployment. In the case of the App-2 deployment, theinteractive interfaces on both the PT and older adult ends usea Kinect device along with a local computer (specifications:Windows 7 64 bits, RAM 4 GB, Storage 500 GB, GigabitNIC) that is mounted on a mobile cart that has a largedisplay (specification: 1920x1080 px). The application, systemand network performance data across the ECaaS supportinginfrastructure are processed locally for tasks such as prelim-inary sanitization and meta data annotation (e.g., data foldernaming), and are immediately sent to a cloud-hosted databasefor detailed data processing that help with later activity reportdiscussions between the care coordinators and the older adults.

5
We utilize a GENI Rack i.e., a community cloud infras-tructure for the database hosting to handle data managementtasks. We also use the GENI Rack to host the peer-to-peerapplication orchestration signaling co-ordination module thatis part of the overlay network setup described previously. Forthese purposes, the GENI Rack is configured with three virtualmachines provisioned using the VMware ESXi hypervisor.The entire application, system and network performance datacollection, aggregation and visualization are performed withour Narada Metrics software [15], which was developed pre-viously as an end-to-end network and application performancemeasurement framework [2].
C. Cloud Services SolutionFor high-scale delivery of the ECaaS Apps within a cloud-
based infrastructure, we prescribe two layers of services withREST (REpresentational State Transfer) web services abstrac-tions that are commonly used in cloud platforms viz., (i)Secure Compute and Network Services, and (ii) Data Services.In Figure 6, we show our App-2 i.e., PhysicalTherapy-as-a-Service (PTaaS) within the cloud-based ECaaS architecture. Achallenge in the infrastructure configuration for secure servicesrefers to compliance issues (i.e., pertaining to FISMA (FederalInformation Security Management Act) Moderate or HIPAA(Heath Insurance Portability and Accountability Act)) that areparamount in the health care related technology infrastructures.
Fig. 6. ECaaS cloud-based services architecture for PTaaS App delivery.
In the first layer, different processing pipelines should bedeveloped that handle the workflow, security issues for thelarge amount of data-in-motion (e.g., SSL (Secure SocketsLayer)), and the access control as well as encryption forthe high volume data-at-rest. The access control for securitymanagement need to be implemented using Federated Identityand Access Management frameworks such as Shibboleth. Wesuggest that custom web interfaces be developed for theowners of the PTaaS system to be able to add, delete or modifypermissions of the different data query, analysis and visual-ization tasks. In the second layer, components are related todata services that operate in virtualized storage environmentsand need to be federated across multiple private cloud (e.g.,hospital data center) and public cloud (e.g., Amazon WebServices) platforms.
While making these decisions in the beginning and as-sessing their impact, our approach is to use the co-designand continuous monitoring approach with frameworks such asNarada Metrics. This approach allows us to query data frommultiple sources, and feed the results to tools that performdata analysis and visualization to indicate salient trends orbottleneck anomaly events. This procedure helps to reflect ondecisions while using ECaaS with the goal to confirm, renewor to revise them based on given data by App-1 and App-2performance evaluations in a controlled environment.
D. Network Quality EstimatorWe tested the health alert system of App-1 in senior
housing with face-to-face clinical care coordination. How-ever, as implemented currently, the approach does not scalewell. Sensor data that was collected in the home is over 23GB per week per elder. To transfer that data in a timelymanner to support health alerts has been hard to achieveconsistently. Moreover, the relational database methods thathave been applied, have not allowed fast interactive access forhuge databases. These technical issues involving local dataprocessing at the network-edge i.e., at the elder homes can beaddressed through the emerging paradigm of ‘fog computing’to meet latency bottlenecks for interactive data analysis. Forinstance, the GENI Rack compute services can be intelligentlycoordinated with a local compute service that can intelligentlyperform pre-processing at the patient side, and post-processingat the clinical care coordinator side based on the estimationof network quality constraints at the end sites. However,such a fog computing architecture in ECaaS will introducesecurity/privacy issues that need to be considered carefully inthe data storage and data access configurations [14].
In the case of App-2, ECaaS relies heavily on videoconferencing for remote care coordination, and thus requireshigh performance (≈ 200 Mbps) for accurately recognizingfacial expressions, skin color, eye clarity, and speech patterns,as well as inspection of depth data in real-time at the PTside. A robust network architecture with predictable end-to-end performance is essential for the interactive monitoring andhealth interventions. We approach this design challenge byinstrumenting the App-2 to obtain measurements for networkquality estimation. Both active measurements (i.e., end-to-end TCP throughput, round-trip time (RTT) delay, jitter andpacket loss) and passive measurements (i.e., transfer rate onuplink of the local interface, download rate at remote interface)are being collected using the Narada Metrics measurementframework [15].
The technical challenges for integrating the ECaaS App-1and App-2 point to several design options. We argue that agood start for ECaaS is the integration with remote deploy-ment of sensing, Big Data analysis methods for storing andaccessing consumer data, high-definition video-based commu-nication, HIPAA-compliant security, and interactive interfaces,leveraging cloud computing and overlay network channels. Forthis integration, we are starting efforts to use and test thenewly deployed fiber networking infrastructures within urban,suburban and rural communities in the state of Missouri.We have established on-going partnerships with healthcareproviders and Gigabit fiber connection providers (e.g., GoogleFiber, Co-Mo Connect, MOREnet) in these efforts in order totranslate our research into real-world ELEs for eldercare.

6
V. A LIVING LAB ENVIRONMENT FOR ECAASWe conceptualize the living lab for ECaaS as combination of
technology, network optimization and cloud-based integrationof our two Apps that is also extensible for other future Apps.We are working towards building a living lab environmentthat involves eight private homes of senior adults in urban,suburban and rural areas, as well as several local PT clinicsin the Missouri region. We have access to a few of thesehomes and PT clinics from previous projects and through ourproject partners of Google Fiber and Co-Mo Connect. Ournext step of development of ECaaS as “design-in-use” withina living lab environment is guided by data-driven design-basedresearch approaches such as usability testing, data analyticsand iterative design testing with end-users.
We address three research approaches that we plan to pursueto deliver ECaaS to users in a manner that is performanceoptimized for satisfactory user experience. The three researchapproaches and the corresponding research questions are de-scribed in the following:A. Cloud service management studies
Huge amounts of data in real time can cause irritations forthe users due to technical network problems (e.g., delays inproviding data). The care coordinator or PT needs to be ableto confidently assess whether non-ideal performance in theexercise forms of an older adult is being impacted due to lag innetwork communications in data-intensive interactive sessions,or in fact is impacted due to the physical and cognitive limita-tions of the older adult. The research questions to be answeredinclude: How to optimize networks and cloud systems forECaaS using health assessment data in remote settings? Howto perform troubleshooting in bottleneck cases? [2]B. Data Analytics Studies
Gait information needs to be presented back to older adultsin-home and in a clear, understandable formats. Further,the Apps need to provide pertinent information that fostersfeedback to patients, PTs or care providers to take suitableactions in cases where proactive care is essential. An importantresearch question here is: What sensor information for auto-mated health alerts needs to be fused for real-time analysisand optimization when in remote use?C. Usability and Human-centered Development Studies
There needs to be an integration of the Apps into theircontext of use through sociotechnical design configurationssuch that patients, care coordinators and PTs will actually usethe Apps in a sustained manner, instead of avoiding them.Important research questions include: How to integrate thesensors and Apps into private homes, and PT clinics such thatthey will become part of a sociotechnical system that supportsco-evolutionary growth? Which interface layouts work best forthe older adults, care coordinators and PTs in the context ofbeing user friendly, effective and efficient? [16].
The above sociotechnical studies and system developmentinvolves agile iterative design testing, usability studies withend-users as co-designers, as well as data collection by adopt-ing the SocioTechnical WalkThrough (STWT) method [17].The STWT is a qualitative co-design workshop method basedon Focus Group interviews in which the PTs and patientsbecome co-designers of ECaaS and ‘model’ the ECaaS inpractice. STWT is moderated by an experienced research team
member in a series of workshops (typically up to 6 workshopsper year) to explore the users’ perspectives and measure thebenefits of ECaaS. Each workshop lasts 2 to 3 hours, andthe obtained results are organized as “case vignettes” [18].The case vignettes inform the iterative and agile softwaredevelopment of ECaaS to produce user-friendly solutions.
Data collection in urban and rural homes through usabil-ity methods can include Tasks Analysis with Think Aloudtechniques and user surveys with 10-point Standard UsabilityScore (SUS) rankings administered during the ECaaS Appsuse. The data collection also encompasses quantitative datasuch as cloud system and network performance measurements.Collected datasets can allow us to measure whether the ECaaSsolution is usable for the users, and how fast the users achievethe tasks when they use ECaaS. User surveys also help us toevaluate interactive interfaces in the context of both remote PTand clinical care coordination, studying the technical qualityof the video and audio streams as well as usability, usersatisfaction, and effectiveness. Further, they can help us assesswhether/how ECaaS increased the patient quality of life (e.g.,avoiding many hours travel to have access to a PT).
VI. CONCLUSION AND OUTLOOK
In this article, we presented the design of an ‘ElderCare-as-a-SmartService’ (ECaaS) system that can facilitate proactivehealth monitoring and targeted care coordination of olderadults within their in-home settings. We detailed the challengesin the cloud transformation of sandbox approaches of ECaaSApps into a living lab environment with actual users. Theliving lab purpose is to facilitate on-going App development toultimately create real-world ELEs for eldercare. We not onlyfocused on the technical design of the infrastructures and Appsdevelopment, but argued how the social and organizationaldesign needs to be considered within the context of ECaaSuse in practice i.e., within the organization of clinics, PTsand their workflows as well as the environments and dailyprocesses of patients’ in-home settings.
We outlined how a “co-development” strategy that involvesthe stakeholders to assume relevant roles (i.e., health careproviders serving as App owners, as well as older adultend-users serving as App consumers) in order to work to-gether to make ECaaS into a highly secure, privacy-preservingand socially embedded smart service system. Our suggestedapproach was to apply different methods of usability andhuman-centered design concepts such as the SocioTechnicalWalkthrough to help stakeholders to adopt the ECaaS andrefine it during ‘design-in-use’ within a living lab environment.
Further research of ECaaS activities based on our designpresented in this paper can enhance understanding at the levelof sociotechnical configurations for ELEs targeted for elder-care. In particular, our proposed efforts to obtain user surveysand conduct behavior modeling with end users will lead touseful interactive interfaces for the ECaaS Apps that improveclinical care coordination. In addition, they enable studiesof cloud-based services to effectively handle the video andaudio streams through metrics of usability, user satisfaction,and App effectiveness for eldercare that can be seamlesslydelivered across urban, suburban and rural areas. Thus, ourECaaS design has the potential to improve quality of lifefor older adults and their care coordinators through pertinentsocial embedding of Apps within ELEs for eldercare.

7
REFERENCES
[1] M. Skubic, R. Guevara, M. Rantz, “Automated Health Alerts using In-home Sensor Data for Embedded Health Assessment”, IEEE Journalof Translational Engineering in Health and Medicine, Vol. 3, pp. 1-11,2015.
[2] P. Calyam, A. Mishra, R. Antequera, D. Chemodanov, A. Berryman,K. Zhu, C. Abbott, M. Skubic, “Synchronous Big Data Analyticsfor Personalized and Remote Physical Therapy”, Elsevier Journal onPervasive and Mobile Computing, Vol. 28, Issue C, pp. 3-20, 2016.
[3] G. Fischer, T. Herrmann, “Socio-technical Systems: A Meta-designPerspective”, IGI Global, pp. 1-33, 2011.
[4] G. Pare, M. Jaana, C. Sicotte, “Systematic Review of Home Telemonitor-ing for Chronic Diseases: the Evidence Base”, Journal of the AmericanMedical Informatics Association, Vol. 14, No. 3, pp. 269-277, 2007.
[5] J. Kaye, N. Mattek, H. Dodge, T. Buracchio, D. Austin, S. Hagler, M.Pavel, T. Hayes, “One Walk a Year to 1000 within a Year: ContinuousIn-home Unobtrusive Gait Assessment of older adults”, Gait & Posture,Vol. 35, No. 2, pp. 197-202, 2012.
[6] G. Baldewijns, V. Claes, G. Debard, M. Mertens, E. Devriendt, K.Milisen, J. Tournoy, T. Croonenborghs, B. Vanrumste, “Automated In-Home Gait Transfer Time Analysis Using Video Cameras”, Journal ofAmbient Intelligence and Smart Environments, Vol. 8, No. 3, pp. 273-286, 2016.
[7] J. Padilla-Lopez, A. Chaaraoui, F. Florez-Revuelta, “Visual PrivacyProtection Methods: A Survey”, Expert Systems with Applications, Vol.42, No. 9, pp. 4177-4195, 2015.
[8] E. Cippitelli, S. Gasparrini, S. Spinsante, E. Gambi, “Kinect as a Toolfor Gait Analysis: Validation of a Real-Time Joint Extraction AlgorithmWorking in Side View”, Sensors, Vol. 15, pp. 1417-1434, 2015.
[9] M. Gabel, E. Renshaw, A. Schuster, R. Gilad-Bachrach, “Full Body GaitAnalysis with Kinect”, Proc. of IEEE EMBC, 2012.
[10] E. Stone, M. Skubic, “Unobtrusive, Continuous, In-home Gait Measure-ment using the Microsoft Kinect”, IEEE Transactions on BiomedicalEngineering, Vol. 60, No. 10, pp. 2925-2932, 2013.
[11] A. Forkan, I. Khalil, Z. Tari, “CoCaMAAL: A Cloud-oriented Context-aware Middleware in Ambient Assisted Living”, Future GenerationComputer Systems, Vol. 35, pp. 114-127, 2014.
[12] N. Pavon-Pulido, J. Lopez-Riquelme, J. Pinuaga-Cascales, J. Ferruz-Melero, R. Santos, “Cybi: A Smart Companion Robot for ElderlyPeople: Improving Teleoperation and Telepresence Skills by CombiningCloud Computing Technologies and Fuzzy Logic”, Proc. of IEEEICARSC, pp. 198-203, 2015.
[13] M. Bonaccorsi, L. Fiorini, S. Sathyakeerthy, A. Saffiotti, F. Cavallo, P.Dario, “Design of Cloud Robotic Services for Senior Citizens to ImproveIndependent Living in Multiple Environments”, Artificial Intelligence,Vol. 9, No. 1, pp. 63-72, 2015.
[14] I. Stojmenovic, W. Sheng, “The Fog Computing Paradigm: Scenariosand Security Issues”, FedCSIS, pp. 1-8, 2014.
[15] P. Calyam, L. Kumarasamy, C. Lee, F. Ozguner, “Ontology-basedSemantic Priority Scheduling for Multi-domain Active Measurements”,Springer Journal of Network and Systems Management, Vol. 22, No. 3,pp. 331-365, 2014.
[16] B. Sheehan, R. Lucero, “Initial Usability and Feasibility Evaluationof a Personal Health Record-based Self-management System for OlderAdults”, eGEMs, Vol. 3, No. 2, 2015.
[17] T. Herrmann, K. Loser, I. Jahnke, “SocioTechnical Walkthrough: AMeans for Knowledge Integration”, The Learning Organization, Vol.14, No. 5, pp. 450-464, 2007.
[18] J. Wherton, P. Sugarhood, R. Procter, S. Hinder, T. Greenhalgh, “Co-production in Practice: How people with assisted living needs can helpdesign and evolve technologies and services”, Implementation Science,Vol. 10, No. 1, 2015.