Embed Size (px)
Citation preview

Towards a bioinformatics analysis ofanti-Alzheimer’s herbalmedicines froma target network perspectiveYi Sun, Ruixin Zhu, HaoYe, KailinTang, Jing Zhao,Yujia Chen, Qi Liu and Zhiwei CaoSubmitted: 16th January 2012; Received (in revised form): 22nd April 2012
AbstractWith the growth of aging population all over the world, a rising incidence of Alzheimer’s disease (AD) has been re-cently observed. In contrast to FDA-approved western drugs, herbal medicines, featured as abundant ingredientsand multi-targeting, have been acknowledged with notable anti-AD effects although the mechanism of action(MOA) is unknown. Investigating the possible MOA for these herbs can not only refresh but also extend the currentknowledge of AD pathogenesis. In this study, clinically tested anti-AD herbs, their ingredients as well as their cor-responding target proteins were systematically reviewed together with applicable bioinformatics resources andmethodologies. Based on above information and resources, we present a systematically target network analysisframework to explore the mechanism of anti-AD herb ingredients. Our results indicated that, in addition to thebinding of those symptom-relieving targets as the FDA-approved drugs usually do, ingredients of anti-AD herbsalso interact closely with a variety of successful therapeutic targets related to other diseases, such as inflammation,cancer and diabetes, suggesting the possible cross-talks between these complicated diseases. Furthermore, path-ways of Ca2þ equilibrium maintaining upstream of cell proliferation and inflammation were densely targeted by theanti-AD herbal ingredients with rigorous statistic evaluation. In addition to the holistic understanding of the patho-genesis of AD, the integrated network analysis on the MOA of herbal ingredients may also suggest new clues forthe future disease modifying strategies.
Keywords: Alzheimer’s disease (AD); network pharmacology; herbal medicine; therapeutic target
INTRODUCTIONMost complex diseases, such as cancer, inflammation
and neurodegenerative disorders, are usually caused
by multiple genes or their products. The efficacy of
single targeting therapies has often been found lim-
ited due to insufficient understanding of the complex
Yi Sun is a PhD student at Department of School of Life Sciences and Technology, Tongji University. Her research interests include
network pharmacology and TCM pharmacology.
Ruixin Zhu is a lecturer at Department of School of Life Sciences and Technology, Tongji University. His research interests include
TCM pharmacology and drug design.
HaoYe is a PhD student at Shanghai Center for Bioinformation and Technology. His research interests include TCM pharmacology
and network pharmacology.
KailinTang is a researcher at Shanghai Center for Bioinformation and Technology. Her research interests include TCM pharmacol-
ogy and machine learning.
JingZhao is a researcher at Shanghai Center for Bioinformation and Technology. Her research interests include TCM pharmacology
and network biology.
Yujia Chen is a master student at Department of School of Life Sciences and Technology, Tongji University. Her research interests
include network pharmacology and TCM pharmacology.
Qi Liu is an associate professor at Department of School of Life Sciences and Technology, Tongji University. His research interests
include TCM pharmacology and small RNA.
ZhiweiCao is a professor at Department of School of Life Sciences and Technology, Tongji University. She is also a principal investigator
at Shanghai Center for Bioinformation and Technology as well as the Key Laboratory of Liver and Kidney Diseases, Shanghai University
of Traditional Chinese Medicine, Ministry of Education. Her research interests include TCM pharmacology and system biology.
Corresponding authors. Qi Liu and Zhiwei Cao, School of Life Sciences and Technology, Tongji University, 1239 Siping Road,
Shanghai 200092, China. Tel: 86-21-54065003; Fax: 86-21-54065057; E-mail: [email protected] and [email protected]
BRIEFINGS IN BIOINFORMATICS. page 1 of 17 doi:10.1093/bib/bbs025
� The Author 2012. Published by Oxford University Press. For Permissions, please email: [email protected]
Briefings in Bioinformatics Advance Access published August 10, 2012 Briefings in Bioinformatics Advance Access published August 11, 2012 by guest on January 11, 2016
http://bib.oxfordjournals.org/D
ownloaded from

network essence of these diseases [1]. Alzheimer’s
disease (AD) is one of such which is clinically char-
acterized by an age-dependent memory dysfunction
together with cognitive deterioration [2]. Although
the etiology of AD is still waiting to be revealed,
multiple pathogenetic factors have been identified
to be involved in this disease. Animal model studies
have shown that brain accumulation of amyloid beta
(Ab) and neurofibrillary tangles (NFTs) are essential
for the development of AD [3]. In addition, prom-
inent activation of inflammatory processes, the innate
immune response, mitochondrial dysfunction, oxi-
dative stress and neuron apoptosis have been
observed in AD progression as well [4].
Currently, there are mainly two types of
FDA-approved drugs. One is cholinesterase inhibi-
tors (ChEIs) designed based on therapeutic target of
cholinesterase. There are four approved cholinester-
ase inhibitors [5]: Tacrine, Donepezil, Rivastigmine
and Galantamine. They are used for the treatment of
mild to moderate AD, and postulated to exert thera-
peutic effect by enhancing cholinergic function [6].
The other one is N-methyl-D-aspartate antagonists
[7] specifically targeted to NMDA receptors. The
only approved NMDA receptor antagonist is
Memantine [5], which is applied in the treatment
of moderate to severe AD. As it is reported that
these approved drugs only help to relieve the symp-
toms of AD patients rather than producing efficient
disease-modifying effects due to their monotonous
therapeutic function [4], new AD therapies are in
urgent need. In the past few years, many small mol-
ecules or bioproducts are under development for the
treatment of AD, including chemical drugs and anti-
body therapeutics.
Among these drugs, herbal medicines, derived
from thousands of years of application, are especially
promising in the development of AD therapy. As
being supported by cellular and animal model stu-
dies, herbal medicines were reported to be effective
on AD from multiple pathways. Several herbal ex-
tracts, such as the Ginkgo biloba extract EGb761 and
Salvia officinalis extracts have been found with a com-
bination of anti-oxidative, anti-apoptosis, neuropro-
tective and neuromodulatory effects [8–11]. The use
of herbal medicines in the treatment of AD is attract-
ing more and more attention [12, 13], and some of
which have even advanced to clinical trials.
However, their anti-AD mechanism is not yet well
understood. Several questions are still remained to be
solved: what are the ingredients of these herbal
medicines and their target proteins? Are they over-
lapping with therapeutic targets of FDA-approved
western drugs? What pathways are herbal medicines
involving in disease treatment? What is the mechan-
istic difference between herbal medicines and west-
ern drugs? Studying these questions may not only
reveal the MOA of anti-AD herbs but also extend
the domain knowledge of AD pathogenesis.
In this paper, we extensively reviewed current
available in silico methods for anti-AD drug research
and development. Based on the survey of these bio-
informatics methodologies, we described a frame-
work to construct an easily-interpretable map that
could facilitate elucidating (MoA) for anti-AD
herbal medicines. First, the clinically supported
anti-AD herbs, their ingredients, as well as the
target proteins were collected. Then, they were stu-
died as compared to FDA-approved anti-AD drugs
in the context of target network. Finally, a holistic
understanding of the molecular mechanism respon-
sible for the anti-AD effects of the herbal medicines
was presented, and the molecular mechanism
involved in the AD was also refreshed and extended
from the observed action of those herb medicines.
COMPUTATIONAL STRATEGIESFOR ANTI-ADDRUGRESEARCHDuring the past decades, computational methods
have facilitated the exploration of anti-AD drugs
with the abundant bioactivity information. They
could mainly be classified into two categories, i.e.:
‘single-target’-directed and ‘multi-target’-directed
strategy.
‘Single-target’ strategy of anti-AD drugsSeveral in silico methods have been frequently em-
ployed into ‘single-target’ anti-AD drug research
based on the conception of ‘therapeutic target’. For
example, docking approaches, molecular dynamics
studies, quantum mechanical studies, and other
methods that could exhibit quantitative structure–
activity relationships (QSAR) have been applied
to facilitate the understanding of cholinesterase,
and to design new cholinesterase inhibitors
[14–18]. Furthermore, ligand-based computational
approaches have also been used to identify inhibitors
for other attractive targets for AD, such as
b-Secretase [19–21] and g-Secretase [22].
page 2 of 17 Sun et al. by guest on January 11, 2016
http://bib.oxfordjournals.org/D
ownloaded from

‘Multi-target’ strategy of anti-AD drugsIn the resent years, the system-oriented design of
‘multi-target’ anti-AD drugs is an attractive approach
with increasing interests, as AD is a complex disease
involving multiple pathogenetic factors. Besides
the computational methods used in ‘single-target’
anti-AD drug design, several new approaches could
facilitate the development of ‘multi-target’ anti-AD
drugs with integration of various sources of informa-
tion, such as microarrays, literature mining-data, pro-
tein–protein interactions (PPIs), and so on. These
methods were summarized in Table 1.
There are various AD-related microarray gene-ex-
pression profiles, and many of them have been
well-collected in the Connectivity Map (cMAP)
[23], as well as the newly published searchable platformindependent expression database (SPIED) [24]. Different
methods have been applied to explore the micro-
array gene-expression dataset of AD, including un-
supervised machine learning approaches [25], integer
linear programming model [26] and network analysis
[27, 28]. Potential pathways and therapeutic targets
for AD were also identified in these studies.
Nevertheless, the gene-expression experiments are
expensive and time-consuming, and often reported
in disagreement with low-throughput experiments.
Hence, alternative methods without requiring
high-throughput microarray data are attractive as
well. For example, two newly published methods
were proposed based on the interacting profiles of
AD drugs and could help to uncover their thera-
peutic mechanisms by incorporating the ‘off-targets’.
Among them, one is the AD-specific drug–protein
connectivity map [29] built with protein interaction
networks and literature mining. The other one is the
AD drug-oriented chemical–protein interactome
(CPI) [30], which was constructed on the basis of
the relations between 10 drug molecules and 401
human protein pockets derived from the application
of DOCK program. Furthermore, a network was
integrated with published PPI data to study the func-
tions of AD proteins and the relationships among
them [31, 32]. This network analysis provides a sys-
tematic view of AD pathology, as it could help to
find not only important AD-related proteins, but also
important pathways involving in AD.
FRAMEWORK FORTHE ANTI-ADMECHANISM ANALYSIS OFHERBALMEDICINESAccording to the review of current in silico methods
for anti-AD drug discovery, there seems no pub-
lished work for the holistic understanding of the mo-
lecular mechanism for anti-AD drugs. In this section,
we considered to provide a low-cost and effective
way to explore the anti-AD mechanism at a system
level. Specifically, we focused on anti-AD herbs and
the network pharmacology analysis technologies. It
should be noted that network analysis is an increas-
ingly important approach in uncovering the mode of
drug action, which has been well-illustrated in sev-
eral articles [33–35]. Especially, this system-based
network technology is useful in revealing the
Table 1: Current bioinformatics methodologies for AD pharmacology
Data Methods Findings Reference[PMID]
Microarray Unsupervised machine learning approaches Identifying potential pathways and thera-peutic targets of AD
21989140
Microarray and PPI Integer linear programming model Identifying protein signal pathways of AD 21442495Microarray K-shortest paths and k-cycles network
analysisIdentifying network features and importantpathways in AD
19543432
Microarray Weighted gene coexpression networkanalysis
Identifying 12 distinct modules related toAD
18256261
PPI and literature mining data Disease-specific drug^protein connectivitymap
Finding molecular signature differencesbetween different classes of drugs in AD
19649302
DOCK data Drug-oriented chemical^protein interac-tome analysis
Finding interacting profiles of AD drugs andtheir potential therapeutic mechanism
20221449
Published work characterizingboth APP and Ab
Gene ontology and network analysis Identify potentially novel functional rela-tionships among AD-related proteins
20391539
AD-related genes and humanprotein interactions
An algorithm to rank AD-related proteins Functionally relevant AD proteins wereconsistently ranked at the top
17094253
Bioinformatics analysis of anti-Alzheimer’s herbal medicines page 3 of 17 by guest on January 11, 2016
http://bib.oxfordjournals.org/D
ownloaded from

complex modulation essence of herbal medicines as
concluded in the review of Jing Zhao et al. [36]. As a
result, we attempt to (i) systematically collect and
review anti-AD herbs, their ingredients, and the
target proteins from public databases and literatures,
and (ii) study the anti-AD mechanism with the ap-
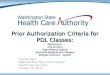
plication of network analysis. This two-part frame-
work was shown in Figure 1.
Mining of anti-AD herbs, theiringredients and the correspondingtarget proteinsThe main purpose of this part is to answer the fol-
lowing questions: what are the ingredients of herbal
medicines and their target proteins? Are they over-
lapping with therapeutic targets of FDA-approved
western drugs?
Anti-AD herbsWe have performed a large-scale text mining of
PubMed and the clinical trial database (www
.Clinicaltrials.gov, currently contains 119 213 trials
from 178 countries), and for the first time manually
extracted the available promising anti-AD herbs from
the English literatures (from 1995 to 2011) with the
keywords ‘herbal medicine’ and ‘Alzheimer’s’.
Among them, Ginkgo biloba, Huperzia serrata, Melissaofficinalis and Salvia officinalis are found to be the top
well studied ones in the large volume of AD-related
articles as shown in Table 2. It can be seen from
literatures that different herbs have been studied to
different extent. Articles relating Ginkgo biloba to AD
are the most abundant (233), probably because
Ginkgo biloba has been studied for a long time and
extensive papers have been accumulated (2357 art-
icles). This herb could significantly improve atten-
tion and memory performance of patients in a phase
III clinical trial [37]. The efficacy of Ginkgobiloba was
even comparable to the results of patients treated
with donepezil, a FDA-approved drug for mild to
moderate AD [37].
As these herbs have been studied to different
extent, a parameter is introduced to balance this
bias and further assess the association between them
and AD. The parameter is calculated as the
(AD-herb-related papers)/(herb-related papers)
ratio. P-value was applied to measure how improb-
able by chance it is to observe a certain level of
co-occurrences of each herb and AD in at least karticles [38]:
P ¼ 1�Xk�1
i¼0
f ðiÞ ¼1�Xk�1
i¼0
Ki
� �N � Kn� i
� �
Nn
� � ,
where N is the total number of papers in PubMed
(19 432 858 articles, as given by GoPubMed), K is
the number of papers associate with AD (52 535 art-
icles, as given by GoPubMed), n is the volume about
one single herb, k is the number of papers about the
effects of corresponding herb on AD. GoPubMed
was used to get the value of N, K, n and k.P-value indicates the significance of relevance be-
tween each herb and AD [39] (significant when
P-value < 0.01).
As a result, Huperzia serrata obtained the highest
ratio (35.71%; with P<< 0.01), indicating that
anti-AD may be one of the major therapeutic effects
found so far for this herb. Ginkgo biloba (9.89%; with
P<< 0.01) is second to Huperzia serrata, and then fol-
lowed by Salvia officinalis (3.99%; with P<< 0.01)
and Melissa officinalis (2.29%; with P<< 0.01).
Furthermore, different stages of clinical trials for
these four herbs were summarized from either clin-
ical trial databases or PubMed, as shown in Table 3.
This suggested that these herbal medicines are pro-
mising in the field of anti-AD drug discovery, as
random and double-blinded clinical studies gave
positive results. Among the four herbs, Ginkgo biloba
Figure 1: Workflow for target network analysis ofanti-AD herbal mechanism.
page 4 of 17 Sun et al. by guest on January 11, 2016
http://bib.oxfordjournals.org/D
ownloaded from

was the most frequently studied one as 12 related
clinical trials can be found. Only 4 of the 12 trials
showed no significant differences from the placebo
groups, and all the other 8 studies have provided
supportive evidence for anti-AD effects of Ginkgobiloba. For Huperzia serrata, most of its clinical trials
were focused on the component named Huperzine
A and significant improvement has been observed in
four trials. As to Melissa officinalis and Salvia officinalis,there was only one trial for each.
Anti-AD herb ingredientsIn this study, the compounds contained in each
herb were collected from Traditional Chinese
Medicine Information Database (TCM-ID) [45],
‘Pharmacopoeia of People’s Republic of China’
and PubMed. It is noted that not all compounds
were extensively studied, and only those with litera-
ture support of target proteins are remained. Finally,
10 compounds were collected from the four herbs.
The significance of their correlations with AD were
also measured with the P-value introduced in the
‘Anti-AD herbs’ part, and were summarized in
Table 2. It is not surprising to observe that P-valuesfor the majority of the ingredients are not significant,
as herbal medicines are usually used in the form of
multiple components. Among these ingredients,
Huperzine A from Huperzia serrata has the highest
correlation with AD (25.81% and 80 articles),
and this correlation is significant as measured by
P-value. Actually, results of the most recent Phase
II clinical trial have indicated the significant cognitive
enhancement of Huperzine A for mild to moderate
AD patients [12]. The activity of this ingredient was
reported to be stronger than another ChEI galata-
mine [46]. Phase III and Phase IV trials of Huperzine
A are also anticipated, as indicated by the clinical trial
database.
Target proteins of anti-AD herb ingredientsInformation of target proteins for herbal ingredi-
ents was identified from HIT [47], a well-known
herb ingredient target database (http://lifecenter.
sgst.cn/hit/). A total of 221 direct targets of
586 herbal compounds have been collected in this
database. Totally 34 target proteins were retrieved
for the 10 anti-AD herbal ingredients (Table 4).
The interactions between the compounds and targets
have been classified into three categories, i.e. activa-
tion, inhibition and neutral binding of the target
proteins.
Then, to assess the relationship between these
target proteins and AD:
First, the 34 target proteins were regarded as a
whole to evaluate the distance between them and
known ‘AD-related proteins’ in the background of
a genome-wide human PPI network. If the distances
between the herbal targets and ‘AD-related proteins’
are significantly shorter than those of the random
counterparts in the context of human PPI, a close
Table 2: Correlations between herbs or compounds with AD
Herb Compound
Herb name Volume of articles Compoundname
Volume of articles BBBpermeability
Total Relevant to AD(Ratio; P-value)
Total Relevant to AD(Ratio; P-value)
Ginkgo biloba 2357 233 [74 are reviews](9.89%; P<< 0.01)
(i) Quercetin 6720 14 (0.21%; P¼ 0.8031) Y(ii) Kaempferol 1904 4 (0.21%; P¼ 0.5852) Y(iii) Ginkgolide a 77 2 [1 is review] (2.60%;
P¼ 0.0012)NK
(iv) Ginkgolide b 726 3 [1 is review] (0.41%;P¼ 0.1360)
Y
Huperzia serrata 56 20 [10 are reviews](35.71%; P<< 0.01)
(i) Huperzine A 310 80 [29 are reviews](25.81%; P<< 0.01)
Y
(ii) Huperzine B 27 6 (22.22%; P<< 0.01) NKMelissa officinalis 612 14 [2 are reviews]
(2.29%; P<< 0.01)(i) Quercetin 6720 14 (0.21%; P¼ 0.8031) Y(ii) Gallic acid 4304 3 (0.07%; P¼ 0.9970) Y
Salvia officinalis 276 11 [2 are reviews](3.99%; P< < 0.01)
(i) Apigenin 1553 2 (0.13%; P¼ 0.7900) Y(ii) b-Sitosterol 2591 3 [1 is review] (0.12%;
P¼ 0.9188)Y
(iii) Ursolic acid 682 3 (0.44%; P¼ 0.1156) NK
Note: Ratio¼ (AD-herb-related papers)/(herb-relatedpapers);Y, yes; NK, not known.
Bioinformatics analysis of anti-Alzheimer’s herbal medicines page 5 of 17 by guest on January 11, 2016
http://bib.oxfordjournals.org/D
ownloaded from

Table
3:Inform
ationforclinicaltrialsof
anti-AD
herbs
Herbal
name
Stud
ySam
ple
Exp
erim
ental
design
Interv
ention
Outco
memea
sure
Con
clusion
(positiveor
nega
tive
eviden
ceforthehe
rbal
med
icinein
AD
trea
tmen
t)
Inform
ation
sour
ce
1Ginkgobiloba
PhaseIIIclinicaltrial
Area:US
Tim
e:20
00.10�2010.07
Age:�
75Num
ber:
3069
Status:no
rmal
cognition
(n¼25
87)
orMCI
(n¼48
2)
preventio
n;rand
o-mized;d
ouble
blind;
placebocon-
trol;p
arallela
ssign-
ment;safety/
Efficacystud
y
120mg/2days
G.biloba;
placebo
ADAS-cog;
CDR
Negative
Clinicaltriald
atabase
(NCT00
0108
03)
PubM
ed(PMID:19
017911;
19321833)
2Ginkgobiloba
Area:
Germany
Tim
e:24
weeks
Num
ber:
216
Status:
prim
ary
degen-
erative
AD
ormild
tomod
eratedementia
doubleblind;
placebo
control;rand
o-mized;m
ulticenter
240mg/dayG.
biloba
;placebo
ADAS-cog;
SKT
Positiv
ePu
bMed
(PMID:14
663654
;8741021)
3Ginkgobiloba
Area:US
Tim
e:26
weeks
Num
ber:
309
Status:m
ildto
severe
AD
ordementia
rand
omized;d
ouble
blind;
placebocon-
trol;p
arallelgroup;
multicenter
120mg/dayG.
biloba;
placebo
ADAS-Cog
Positiv
ePu
bMed
(PMID:10
867450
)
4Ginkgobiloba
Area:
Germany
Tim
e:3mon
ths
Age
:50
^80
Num
ber:
20Status:mild
tomod
erate
AD.
rand
omized;d
ouble
blind;
placebo
control
240mg/dayG.
biloba
;placebo
SKT;
ADAS
Positiv
ePu
bMed
(PMID:944
7569)
5Ginkgobiloba
Area:The
Netherlands
Tim
e:24
weeks
Num
ber:
214
Status:
Dem
entia
orage-associated
mem
ory
impairment
doubleblind;
rand
o-mized;p
lacebo
controll;
parallel
grou
p;multicenter
240mg/dayG.
biloba
;160mg/dayG.
biloba
;placebo
NAI-W
L;NAI-Z
N-G
Negative
PubM
ed(PMID:11037003)
6Ginkgobiloba
Area:US
Tim
e:26
weeks
Num
ber:
513
Status:d
ementia
rand
omized;p
lacebo
control;do
uble
blind;
parallel
grou
p;multicenter
240mg/dayG.
biloba
;120mg/dayG.
biloba
;placebo
ADAS-cog;
ADCS-CGIC
Negative
PubM
ed(PMID:16375657
)
7Ginkgobiloba
Tim
e:22
weeks
Age:�
50Num
ber:
96Status:AD
rand
omized;d
ouble
blind
240mg/dayG.
biloba
;do
nepe
zil
SKT
Positiv
ePu
bMed
(PMID:19347685)
8Ginkgobiloba
Area:Ukraine
Tim
e:22
weeks
Age:�
50Num
ber:
400
Status:AD
orvascular
dementia
rand
omized;d
ouble
blind
240mg/dayG.
biloba;
placebo
SKT
Positiv
ePu
bMed
(PMID:17341003)
9Ginkgobiloba
Area:UK
Tim
e:6mon
ths
Num
ber:176
Status:
early
stage
dementia
rand
omized;p
rag-
matic;d
oubleblind;
commun
itybased;
parallelgroup
120mg/dayG.
biloba;
placebo
ADAS-Cog
Negative
PubM
ed(PMID:18
5372
21)
(con
tinue
d)
page 6 of 17 Sun et al. by guest on January 11, 2016
http://bib.oxfordjournals.org/D
ownloaded from

Table3Continued
Herbal
name
Stud
ySam
ple
Exp
erim
ental
design
Interv
ention
Outco
memea
sure
Con
clusion
(positiveor
nega
tive
eviden
ceforthehe
rbal
med
icinein
AD
trea
tmen
t)
Inform
ation
sour
ce
10Ginkgobiloba
Area:Italy
Tim
e:24
weeks
Age:50
^80
Status:mild
tomod
erate
dementia
rand
omized;p
lacebo
control;do
uble
blind
160mg/dayG.
biloba;
5mg/daydo
nepe
zil;
placebo
MMSE
Positiv
ePu
bMed
(PMID:16930364
)
11Ginkgobiloba
Area:US
Tim
e:52
weeks
Num
ber:168
Status:p
rimarily
visual-
construc
tional
impair-
ment
orpred
ominant
verbaldeficitsor
impaired
inbo
thcognitivedo
mains.
rand
omized;d
ouble
blind;
placebo
control
120mg/dayG.
biloba;
placebo
ADAS-Cog
Positiv
ePu
bMed
(PMID:13130389
)
12Ginkgobiloba
Area:US
Tim
e:52
weeks
Num
ber:
309
Status:AD
ormulti-infarctdementia
multicenter;rand
o-mized;d
ouble
blind;
parallelpla-
cebo
control;
120mg/dayG.
biloba;
placebo
ADAS-cog;
ADCS-CGIC
Positiv
ePu
bMed
(PMID:93434
63)
13Hup
APh
aseIIclinicaltrial
Area:US
Tim
e:24
weeks
Num
ber:150
rand
omized;m
ulti-
center;d
ouble
blind;
placebo
control
200mg/2
days
Hup
A40
0mg/2
days
Hup
A;
placebo
ADAS-cog
Positiv
eClinicaltriald
atabase
(NCT00
083590
)
14Hup
AArea:
China
Tim
e:8weeks
Num
ber:
50rand
omized;d
ouble
blind;
prospe
ctive;
parallel;placebo
control;
multicenter
200mg/day
Hup
A;
placebo
MMSE
Positiv
ePu
bMed
(PMID:8701750
)
15Hup
AArea:
China
Tim
e:60
days
Num
ber:
60Status:AD
rand
omized;d
ouble
blind;
parallel;pro-
spectiv
e;do
uble
mim
ic;m
ulticen-
ter;po
sitiv
econtrol
200mg/dayHup
A;
placebo
psycho
logicalevaluations
Positiv
ePu
bMed
(PMID:10
678137)
16Hup
AArea:
China
Tim
e:12
weeks
Num
ber:
202
Status:AD
rand
omized;d
ouble
blind;
multicenter;
placebocontrol;
parallela
ssignm
ent
400mg/dayHup
A;
placebo
ADAS-Cog;M
MSE
Positiv
ePu
bMed
(PMID:12181083)
17Melissa
officinalis
Area:Tehran,Iran
Tim
e:4mon
ths
Age:65
^80
Status:mild
tomod
erate
AD
rand
omized;d
ouble
blind;
parallel
grou
p;placebo
control
Melissa
officinalis;p
lacebo
ADAS-cog;
CDR
Positiv
ePu
bMed
(PMID:12
810768
)
18Salviaofficinalis
Area:Tehran,Iran
Tim
e:4mon
ths
Age:65
^80
Status:mild
tomod
erate
AD
rand
omized;d
ouble
blind;
parallel
grou
p;placebo
control
Salviaofficinalis;p
lacebo
ADAS-cog;
CDR
Positiv
ePu
bMed
(PMID:12
605619)
Note:ADAS-cog,
Alzheim
er’sdiseaseassessmentscale,Cognitiv
esubscale
[1];CDR,cognitiv
edrug
research
[2];SK
T,shor
tcognitiveperformance
test
[3];ADCS-CGIC,A
DCS-clinicians’globalimpressio
nof
change
scales
[4];MMSE,m
ini-m
entalstate
exam
ination[5];NAI-W
L,verballearning;N
AI-Z
N-G
,digitmem
oryspan.
Bioinformatics analysis of anti-Alzheimer’s herbal medicines page 7 of 17 by guest on January 11, 2016
http://bib.oxfordjournals.org/D
ownloaded from

Table
4:Target
proteins
ofanti-AD
herbs
Target
name
Target
name
(abb
reviation)
Unipr
ot_ID
Gen
e_ID
Com
pou
ndInteracting
type
Stateof
therap
eutic
target
Herb
Pub
Med
_ID
1.Acetylcho
linesterase
AChE
P22303
43Hup
erzine
A;
Hup
erzine
Bi;i
Successful
target
(AD)
Huperziaserrata
1636
4207;16364
207
2.Glutamate[NMDA]receptor
NMDAR
Q0558
629
02Hup
erzine
Ai
Successful
target
(AD)
Huperziaserrata
119209
203.Cho
linesterase
BCHE
P06276
590
Hup
erzine
A;
Hup
erzine
Bi;i
Successful
target
(AD)
Huperziaserrata
1636
4207;16364
207
4.Ep
idermalgrow
thfactor
receptor
EGFR
P00533
1956
Quercetin
bSuccessful
target
(Cancer
andinflammation)
Ginkgobiloba;M
elissa
officinalis
186184
85
5.Receptortyrosin
e-protein
kinase
erbB
-2ErbB
2P0
4626
2064
Quercetin
bSuccessful
target
(Cancer
andinflammation)
Ginkgobiloba;M
elissa
officinalis
186184
85
6.5-lipo
xygenase
ALO
X5
P09917
240
Quercetin
iSuccessful
target
(Cancer
andinflammation)
Ginkgobiloba;M
elissa
officinalis
1586
4785
7.Estrogen
receptor
aESR1
P03372
2099
Kaempferol
aSuccessful
target
(Cancer
andinflammation)
Ginkgobiloba
15182386
8.Estrogen
receptor
bESR2
Q92731
2100
Quercetin;
Kaempferol
a;i
Successful
target
(Cancer
andinflammation)
Ginkgobiloba;M
elissa
officinalis
15182386
;1518238
6
9.Tumor
necrosisfactor
TNFA
P01375
7124
Kaempferol
iSuccessful
target
(Cancer
andinflammation)
Ginkgobiloba
17278014
10.Poly[ADP-ribo
se]po
lyper-
ase1
PARP-1
P098
74142
Quercetin
iSuccessful
target
(Cancer
andinflammation)
Ginkgobiloba;M
elissa
officinalis
1788
4996
11.P
eroxisom
eproliferator
activ
ated
receptor
gamma
PPARG
P37231
5468
Quercetin;
Kaempferol
a;a
Successful
target
(Diabe
te,C
ancerand
inflammation)
Ginkgobiloba;M
elissa
officinalis
18262572
;18262572
12.A
ldosereductase
AR
P15121
231
Quercetin
iSuccessful
target
(Diabe
te)
Ginkgobiloba;M
elissa
officinalis
1680
6328
13.C
almod
ulin-dependent
cal-
cineurin
Asubu
nita
isoform
CNA
Q08
209
5530
Kaempferol
iSuccessful
target
(Parkinson’sdisease)
Ginkgobiloba
1850
6853
14.N
itricoxidesynthase,
inducible
iNOS
P35228
4843
Kaempferol
iSuccessful
target
(ische-
miareperfusion
injuries)
Ginkgobiloba
17278014
15.D
NAtopo
isom
erase2-a
TOP2
AP11388
7153
Quercetin
iClinicaltrialtarget
(cancerand
inflammation)
Ginkgobiloba;M
elissa
officinalis
169508
06
16.A
poptosisregulatorBcl-2
Bcl2
P10415
596
Kaempferol
aClinicaltrialtarget
(cancerand
inflammation)
Ginkgobiloba
15182386
17.A
poptosisregulatorBAX
Bax
Q07812
581
Kaempferol
iClinicaltrialtarget
(cancerand
inflammation)
Ginkgobiloba
15857606
(con
tinue
d)
page 8 of 17 Sun et al. by guest on January 11, 2016
http://bib.oxfordjournals.org/D
ownloaded from

Table4Continued
Target
name
Target
name
(abb
reviation)
Unipr
ot_ID
Gen
e_ID
Com
pou
ndInteracting
type
Stateof
therap
eutic
target
Herb
Pub
Med
_ID
18.Transcriptio
nfactor
AP-1
AP1
P05412
3725
b-Sitosterol
iClinicaltrialtarget
(cancerand
inflammation)
Salviaofficinalis
14612938
19.C
ycloox
ygenase-2
COX2
P35354
5743
Ursolicacid
iResearchtarget
(cancer
andinflammation)
Salviaofficinalis
1290
7607
20.C
aspase-9
Casp9
P55211
842
Gallic
acid
iResearchtarget
(cancer
andinflammation)
Melissa
officinalis
1768
5632
21.Interleuk
in-4
IL4
P05112
3565
Apigenin
iResearchtarget
(cancer
andinflammation)
Salviaofficinalis
1738
4531
22.S
teroid
andxeno
biotic
receptor
SXR
O75469
8856
Ginkg
olidea;
Ginkg
olideb
a;a
Researchtarget
(cancer
andinflammation)
Ginkgobiloba
19034627;19034
627
23.C
aspase-3
Casp3
P42574
836
Gallic
acid
iResearchtarget
(neuro-
degenerativ
edisease)
Melissa
officinalis
1768
5632
24.M
itogen-activated
proteins
kinase
MAPK
P284
825594
Quercetin;G
allic
acid
b;b
Researchtarget
(neuro-
degenerativ
edisease)
Ginkgobiloba;M
elissa
officinalis
1699
6034
;16308
312
25.S
arcoplasmic/end
oplasm
icreticulum
calcium
ATPa
se1/2
ATP2A1/2
O14983;
P16615
487;48
8Quercetin
iResearchtarget
(Diabe
te)
Ginkgobiloba;M
elissa
officinalis
18785622
26.C
ytochrom
eP450
1A2
CYP1A2
P05177
1544
Quercetin;
Kaempferol
i;i
Non
eGinkgobiloba;M
elissa
officinalis
16762476;16226778
27.C
ytochrom
eP450
1A1
CYP1A1
P04798
1543
Quercetin;
Kaempferol
i;i
Non
eGinkgobiloba;M
elissa
officinalis
1622
6778;16226778
28.P
rotein
kinase
CPK
C-B
P05771
5579
Quercetin
bNon
eGinkgobiloba;M
elissa
officinalis
14593496
29.G
lutathione
S-transferaseP
GST
P1P0
9211
2950
Quercetin
iNon
eGinkgobiloba;M
elissa
officinalis
1268
6490
30.N
uclear
factor
NF-k-Bp6
5subu
nit
REL
AQ04
206
5970
Kaempferol
iNon
eGinkgobiloba
17278014
31.M
atrixmetalloproteinase-1
MMP1
P03956
4312
Kaempferol
iNon
eGinkgobiloba
1788
6198
32.C
ollagena-1(III)chain
COL3
A1
P02461
1281
Ginkg
olideb
b;b
Non
eGinkgobiloba
18221374;182
21374
33.P
lateletbasic
protein
PBP
P027
7554
73Ginkg
olideb
iNon
eGinkgobiloba
17934819
34.S
teroid17-a-hydroxy
lase/
17,20lyase
CYP17
P050
931586
Gallic
acid
iNon
eMelissa
officinalis
1184
8291
Note:Interactingtype
:a-Active;i-Inhibit;b-Bind
Bioinformatics analysis of anti-Alzheimer’s herbal medicines page 9 of 17 by guest on January 11, 2016
http://bib.oxfordjournals.org/D
ownloaded from

association between the targets and AD might be
implicated [48].
To perform the association analysis, a group of
AD-related proteins were collected. These proteins
include two parts, i.e. the successful therapeutic tar-
gets for FDA approved drugs, and the disease proteins
of AD. By searching the TTD database, five successful
therapeutic targets were collected with the key word
‘Alzheimer’s disease’: acetylcholinesterase (AChE),
5-hydroxytryptamine receptor 2A (5-HT2A), cho-
linesterase (BChE), 5-hydroxytryptamine receptor
1A (5-HT1A) and Glutamate [NMDA] receptor
(NMDAR). In addition, four AD disease genes
were further retrieved from the Online Mendelian
Inheritance in Man (OMIM) database [49]: amyloid
precursor protein (APP), presenilin 1 (PSEN1), pre-
senilin 2 (PSEN2) and Apolipoprotein E (APOE).
Their corresponding proteins were obtained accord-
ing to Uniprot database. Totally, nine AD-related
proteins were curated.
Our association analysis was performed in the fol-
lowing procedures:
Firstly, PPI data from the HPRD [50], Mint [51],
Intact [52], BioGRID [53], DIP [54] and MIPS [55]
Database was downloaded to construct a compre-
hensive background network. Secondly, the nine
‘AD-related proteins’ were mapped onto the back-
ground network as well as the 34 target proteins.
Then, to explore whether the herbal targets might
relate to the ‘AD-related proteins’ at a higher level of
organization, the shortest path length between both
sets of proteins in the network was measured [48].
The final averaged shortest path length between the
two groups of proteins was 3.118. To test whether
the result is statistically significant, with ‘AD-related
proteins’ fixed to the background network, 34 pro-
teins were randomly taken from the background PPI
network (10 523 proteins) as a control rather than the
34 herbal targets and nine ‘AD-related proteins’.
After 10 000 times of randomization, the distance
of each was obtained similarly. The statistical signifi-
cance between the actual distance and those of
random counterparts was estimated with the com-
monly used Z-score [56]. If the absolute value of
Z-score is >3, the deviation between the actual
value and the random ones is considered to be of
significance. Despite of the difference of
less-than-one on average, the 34 herbal targets ex-
hibit highly significantly close network distance
(3.118) to the nine ‘AD-related proteins’ (Z-score
�5.803), comparing to the randomly-selected 34
nodes from the background PPI network (3.677).
We believe that with more knowledge accumulated,
closer functional linkage of the herbal targets and AD
might be inferred in future.
Second, the relationship between individual target
protein and AD was further investigated by database
and literature searching.
Overlapping between herbal targets and known
therapeutic targets were identified with the informa-
tion from TTD database and DrugBank database
[57]. Among the 34 herbal targets, 3 are successful
anti-AD targets, 11 are successful targets of five dis-
eases, and another 11 are clinical trial targets or re-
search targets of the same five diseases.
The three anti-AD targets covered 60% of the five
known successful anti-AD targets as mentioned
above. They are Acetylcholinesterase (AChE),Cholinesterase (BChE), and Glutamate [NMDA] re-
ceptor (NMDAR). Through inhibiting AChE and
BChE, FDA-approved drugs [58], such as donepezil,
galantamine and rivastigmine have been considered
to be the first line pharmacotherapy for mild to mod-
erate AD. Meanwhile, memantine has been the only
approved drug for the treatment of moderate to
severe AD by repressing NMDAR [59]. From this
point of view, the anti-AD effect of the collected
herbal ingredients, Huperzine A and Huperzine B,
is probably contributed by inhibition of these suc-
cessful therapeutic targets of AD.
In addition to the successful anti-AD targets,
11 targets have been recorded in TTD as successful
targets of other diseases, such as various neurodegen-
erative diseases (e.g. Parkinson), ischemia reperfusion
injuries, cancer, inflammation and diabetes.
Specifically, serine/threonine–protein phosphatase
2B catalytic subunit a isoform (CNA) has been a
successful target for Parkinson’s disease, which is
shown among the 11 targets. Selective inhibition
of inducible NO synthase (iNOS) was shown to be
able to reduce ischemia reperfusion injuries [60],
while iNOS was suggested to play an important
role in Ab-mediated damage [61]. It is reasonable
to detect the relation between the anti-AD herbal
targets and other neurodegenerative diseases as well
as ischemia reperfusion injuries, because these are
related to brain diseases and their therapeutic
approaches are generally aiming at neuroprotection.
Such kind of association has also been reported in
previous studies [60, 62].
Interestingly, targets of other diseases: inflamma-
tion, cancer, and diabetes were retrieved as well in
page 10 of 17 Sun et al. by guest on January 11, 2016
http://bib.oxfordjournals.org/D
ownloaded from

our study. First, eight of the remaining nine targets
have been reported as successful therapeutic tar-
gets for cancer and inflammation. Among
them, Estrogen receptor 2 (ESR2) and Peroxisome
proliferator-activated receptor gamma (PPARG) can
both be hit by two herbal ingredients, while the
other six are all hit by one individual ingredient,
respectively, as indicated in Table 2. Literature
search indicated their potential association with the
process of AD. For example, ALOX5 was observed
to be upregulated with aging [63, 64], while aging is
one import factor for AD. Meanwhile, ESR1,
TNFA and PARP-1 were suspected to be associated
with AD in several studies [65–67]. Second, aldose
reductase (AR) and PPARG are successful targets for
Diabetes.
Although close correlation between the herbal
targets and AD was not inferred by the statistical
tests, there were many evidences suggesting their
inner relationship. In summary, the herbal ingredi-
ents of collected anti-AD herbs can interact with a
wide range of protein targets, where the majority of
them (74%) are either successful or research targets
for AD-related diseases, including the three success-
ful therapeutic targets against AD. Inflammation is
secondary to protein accumulation in ADs, while
all the 16 therapeutic targets (including research
and clinical) for inflammation in our list are also
overlapping cancer targets. Three targets for diabetes,
three targets for Parkinson and one for ischemia
reperfusion injuries were also found within our
anti-AD target list. These results imply that
anti-AD herbs are primarily interacting with tens of
important proteins critical to disease treatment.
Although the relationship between these diseases is
not fully understood, these targets are serving as the
material basis for the therapeutic effects of the
anti-AD herbs, as well as suggesting important
cross-talks between AD and the other complex
diseases.
Part-two: target network analysis ofmolecular mechanism for anti-AD herbsThe main purpose of this part is to answer the fol-
lowing questions: What pathways are herbal medi-
cines involving in disease treatment? What is the
mechanistic difference between herbal medicines
and western drugs?
To better elaborate the holistic modulation of the
anti-AD herbal medicines, an integrated ‘AD-related
pathway’ was compiled based on the ‘Alzheimer’s
disease pathway’ from KEGG Pathway database
[68, 69] and human PPI data from online databases
[50–55]. First, proteins involved in the ‘Alzheimer’s
disease pathway’ were used as the seeds to obtain
their partner proteins in the context of PPIs.
Second, the direct interacting partners were used as
a new query to fish out the secondary partners. The
pathway was expanded step by step as more herbal
targets could be included. Third, closely connected
proteins were grouped together, and they were orga-
nized according to current knowledge of AD path-
ology. Fourth, in order to clearly display the
underlying mechanism of the herbal medicines, the
intermediate interacting partners were removed.
Finally, the pathway was synthesized by ‘Pathway
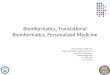
Diagrammer’ [70]. Of 34 target proteins, 28 can be
mapped or connected to the pathway. As shown in
Figure 2, several AD-related processes were
involved, including proliferation, Ab degradation
and cell death. The targets can be organized into
the following pathways: AD symptoms-associated
pathways, inflammation-associated pathways,
cancer-associated pathways, diabetes mellitus-
associated pathways, Ca2þ-associated pathways and
cell proliferation pathways:
Inhibiting theAD symptoms-associated pathwaysAs being mentioned above, three successful thera-
peutic targets for AD can be regulated by anti-AD
herbal ingredients, including Two GPCR family
members (acetylcholinesterase and cholinesterase),
and Glutamate [NMDA] receptor (NMDAR).
These three receptors are all located at cell mem-
brane, as being shown in Figure 2. The acetyl-
cholinesterase and the cholinesterase are involved
in the cholinergic system which has been thought
to have direct influence on cognitive processes
[71]. NMDAR is a glutamate-gated ion channel
which is linked to the induction of excitotoxic
neuron death [72]. It is pleased to see that the
ingredients of Huperzia serrata, could inhibit acetyl-
cholinesterase and cholinesterase [73], as well as
block NMDA ion channels [74]. As the FDA
approved anti-AD drugs usually improve symptoms
of AD patients through inhibiting these targets,
similarly, the anti-AD effects of herbs could prob-
ably be contributed by cognition enhancement
or glutamatergic excitotoxicity reduction to pre-
vent patients from memory and recognition
deterioration.
Bioinformatics analysis of anti-Alzheimer’s herbal medicines page 11 of 17 by guest on January 11, 2016
http://bib.oxfordjournals.org/D
ownloaded from

Suppressing the inflammation-associated pathwaysAs described in Figure 2, a series of inflammatory
factors could be inhibited by herbal ingredients.
Specifically, kaempferol contained in Ginkgo bilobawas shown with a reduction of TNF, NF-kB and
iNOS protein levels in the aged gingival tissues [75],
while another component of Ginkgo biloba,Quercetin could inhibit LOX5 [76]. Moreover,
two ingredients of Salvia officinalli, Ursolic acid and
Apigenin, are correlated with the suppression of
COX-2 expression and the inhibition of IL4 synthe-
sis [77, 78], respectively. Actually, evidence for the
involvement of inflammatory process in AD patho-
genesis has been documented for a long time [79],
and higher peripheral concentrations of several cyto-
kines, chemokines and nitrogen species have been
observed in AD [80]. The downregulation of the
inflammatory cytokines by herbal ingredients will
probably help slowing down of AD progress.
Interfering with the cancer-associated pathwaysCancer-associated pathways could be modulated by
the herbal ingredients, as displayed in Figure 2.
Kaempferol was observed to decrease Bax level
[81] and increase Bcl-2 activity [82] in human
tumor cells, as well as inhibit MMP1 induction
in 12-O-tetradecanoylphorbol 13-acetate-treated
human dermal fibroblasts [83]. Quercetin was
found to reduce PARP1 level in pulmonary epithe-
lial cells [84], and inhibit GSTP1 in malignancies
[85]. A component of Melissa officinalis named Gallic
acid, was shown with decreased activity on Casp3
and Casp9 in 3T3-L1 pre-adipocytes [86], while
b-Sitosterol contained in Salvia officinali inhibited
the expression of AP1 in HT116 human colon
cancer cells [87]. As cancer has been found to be
closely related to AD in a prospective longitudinal
study [88], influencing the cancer-related machinery
may constitute an important part of anti-AD effects
of these herbal ingredients.
Regulating the Diabetes mellitus-associated pathwaysAs shown in Figure 2, Quercetin and Kaempferol
served as agonists of peroxisome proliferator receptor
gamma (PPARg) as validated in the PPARg reporter
gene assay [89], while Quercetin could also inhibit
AR activity by 54% as being measured in an enzyme
assay [90]. In fact, PPARg has been found to induce
insulin signaling as was recently reported to contrib-
ute to modulating Ab accumulation which has been
recognized as a major causative factor in AD patho-
genesis [91]. AR catalyzes the rate limiting step of the
polyol pathway of glucose metabolism, and is
thought to be involved in the pathogenesis of
Figure 2: Distribution of target proteins of herbs on compressed ‘AD pathway’.
page 12 of 17 Sun et al. by guest on January 11, 2016
http://bib.oxfordjournals.org/D
ownloaded from

secondary diabetic complications [92]. Besides the
well-known involvement in glucose metabolism,
AR has recently been suggested by various groups
to play a pivotal role in inflammatory pathologies
which is tightly related to AD as mentioned above
[93]. These results show that PPARg activation and
AR inhibition of the herbs might contribute to the
anti-AD efficacy other than preventing diabetes role.
Downregulating the intracellular Ca2þ homeostasispathwaysFour Ca2þ-related proteins were targeted by
anti-AD herbal ingredients, such as Kaempferol and
Quercetin, being represented as blue squares in
Figure 2. Changes of intracellular Ca2þ are believed
to accompany with almost the whole-brain path-
ology process that has been observed in AD. These
processes include Ab production, tau phosphoryl-
ation, mitrochondrial dysfunction and presenilins
mutation [94]. This indicates that affecting Ca2þ
modulation effects may play an important role in
the anti-AD effects of the herbal ingredients.
Participating in cell proliferation processSome proteins involved in cell proliferaction were
also modulated by the herbal ingredients, as
marked in Figure 2. Ginkgolide a and Ginkgolide
b have been reported to activate SXR in human
primary hepatocytes [95], while Quercetin and
Kaempferol could activate ESR2 and ESR1 respect-
ively in primary rat neuronal cells [96]. Although the
exact mechanism is not very clear, the regulation of
cell proliferation might also be important for the
herbal ingredients in the treatment of AD.
Overall, the above analysis on the ‘AD-related
pathway’ suggests several possible anti-AD mechan-
isms for the herbal ingredients. The herbal ingredi-
ents could produce their anti-AD effect not only by
improving the symptom of AD patients, but also by
targeting the fundamental of the disease pathophysi-
ology such as the inflammation-associated pathways,
cancer-associated pathways, diabetes-associated path-
ways and so on.
As a complex network disease [97], accumulating
evidences have keep indicating the association be-
tween AD and other pathological diseases in the
past few years [79, 98, 99], although the underlying
genetic and molecular connections still need further
investigation.
In summary, from the target network perspective
of these herbal ingredients, it is suggested that
Huperzia serrata might produce anti-AD effects
mainly through a symptom-improving way, while
targets of Salvia officinalis are mainly involved in in-
flammation and cancer-associated pathways. As for
Ginkgo biloba and Melissa officinalis, their targets are
more diversely distributed in these fundamental
pathways of AD indicating their more extensive
anti-AD effects.
CONCLUSIONANDPERSPECTIVETarget proteins of anti-AD herbal ingredients were
systematically collected and analyzed from a network
perspective. Although the anti-AD herbs might
relate to other therapeutic effects or diseases, their
target proteins were found to be closely linked to
AD. Some of the target proteins are successful thera-
peutic targets for AD or cross-talk diseases to AD
(41.18%), while some others are clinical or research
targets for these diseases (32.35%). Furthermore, the
herbal targets were mapped to the ‘AD-related path-
way’ to explore the underlying mechanism of the
anti-AD herbs from the perspective of network
pharmacology. As been observed, the herbs might
treat AD symptomatically as FDA-approved
anti-AD drugs do, or modify the disease through
inflammation-associated pathways, cancer-associated
pathways, diabetes-associated pathways, etc., which
are closely related to AD.
In summary, our work may be beneficial to the
anti-AD field in two aspects:
The first aspectThe underlying mechanism derived from
‘multiple-ingredients multiple-targets’ strategy of
the anti-AD herbs might facilitate the development
of new anti-AD therapy as a complementary to the
current FDA-approved drugs. Besides the ‘multiple-
ingredients multiple-targets’, other properties may
also contribute to the therapeutic effects of
anti-AD herbal medicines. Our comprehensive lit-
erature searching found that 7 of the 10 collected
compounds could pass through the blood–brain bar-
rier (BBB) to produce anti-AD effects. For example,
quercetin and kaempferol have been shown to trans-
port across the BBB in rats [100]. This information
was also shown in Table 2.
On the other hand, although being viewed as low
toxicity, the safety of the herbal medicines should
also be noticed as adverse effects may lead to their
failure in anti-AD drug discovery, development and
marketing. Since few clinical and toxicological
Bioinformatics analysis of anti-Alzheimer’s herbal medicines page 13 of 17 by guest on January 11, 2016
http://bib.oxfordjournals.org/D
ownloaded from

studies have been performed to study the side effects
of herbal medicines, databases and computational
tools designed for studying drug side effects would
be extremely useful. The recent developed side effect
resource (SIDER) database [101] and Drug Adverse
Reaction Database (DART) [102] has documented
the relationship between drugs, ADR targets and
known side effects. Additionally, several computa-
tional methods may also be helpful in the field of
safety evaluation [103–106]. Of course, adverse ef-
fects would be closely related to dosage of the medi-
cine while no bioinformatics report has been seen to
incorporate the information. It is anticipated that
above bioinformatics resources and computational
techniques would be useful to future adverse effects
calculation.
The second aspectRecent studies on disease–disease association have
indicated the cross-talks between different diseases.
As shown by the human disease network (HDN)
[107] and the expanded human disease network
(eHDN) [108], the genetic origins for the majority
of diseases are shared with other diseases, and most of
them are linked to only a few diseases, while a small
part of them are related to many different diseases. In
our paper, the AD-related target network has pro-
vided a more systematic and clear decipher of AD
pathogenesis, including the potential cross-talks with
inflammation, cancer, and diabetes. There are some
reports that people with AD, Parkinson’s and
Huntington’s diseases have a significantly low risk
of most cancers [88] and the reverse correlations
also hold true. The observation in this paper that
the cancer-associated pathways are modulated by
the anti-AD herbal ingredients gives reasonable ex-
planation to that. Secondly, it is known that brain
studies on AD have indicated clear evidence for an
activation of inflammatory pathways and long-term
use of anti-inflammatory drugs is linked with
reduced risk to develop the disease [109]. Since the
cause and effect relationships between them are still
under investigation, the widely repression of inflam-
mation pathway by anti-AD herbal medicine may
provide hints to the future fine tuning of inflamma-
tion to delay, prevent, or treat AD.
Lots of molecules have been studied at different
stages for their potential anti-AD effects. Among
them, herbal medicines are one promising source
with typical ‘multiple-ingredients multiple-targets’
property. Our work has focused on the holistic
understanding of this ‘multiple-ingredients
multiple-targets’ mechanism for anti-AD herbal
medicines at a molecular level. Suggested from
MOA of herbs, future anti-AD therapy might be
considered from multi-intervening several pathways
by systematic evaluation the different roles of com-
binational components.
Key Points
� Since the mechanism of herbal medicines is featured asmultiple-ingredients and multiple-targets network properties,integrated bioinformatics application can provide valuable sup-port to decode theMOAof herbmedicines intervening complexdiseases such as AD.
� Holistic target network analysis of the anti-AD herbs indicatednot only part of the commonmechanism shared between herbsand known FDA-approved drugs, but also the interestingcross-talks between AD and other diseases.
� The proposed bioinformatics method could have a great poten-tial if applied systematically to the inference of new therapeuticuses for natural compounds.
FUNDINGThis work was supported in part by grants from
Ministry of Health (2012ZX10005001), Ministry of
Science and Technology China (2010CB833601),
National Natural Science Foundation of China
(31100956, 61173117, 30900832, and Shanghai
Pujiang Talents Funding (11PJ1407400).
References1. Kitano H. A robustness-based approach to systems-oriented
drug design. Nat RevDrug Discov 2007;6:202–10.
2. Reddy PH, McWeeney S, Park BS, et al. Gene expressionprofiles of transcripts in amyloid precursor protein trans-genic mice: up-regulation of mitochondrial metabolismand apoptotic genes is an early cellular change inAlzheimer’s disease. HumMol Genet 2004;13:1225–40.
3. LaFerla FM. Pathways linking Abeta and tau pathologies.Biochem SocTrans;38:993–5.
4. Citron M. Alzheimer’s disease: strategies for disease modi-fication. Nat Rev Drug Discov 2010;9:387–98.
5. Bajda M, Guzior N, Ignasik M, et al. Multi-target-directedligands in Alzheimer’s disease treatment. Curr Med Chem2011;18:4949–75.
6. Salawu FK, Umar JT, Olokoba AB. Alzheimer’s disease: areview of recent developments. AnnAfrMed 2011;10:73–9.
7. Melnikova I. Therapies for Alzheimer’s disease. Nat RevDrug Discov 2007;6:341–2.
8. Luo Y, Smith JV, Paramasivam V, et al. Inhibition ofamyloid-beta aggregation and caspase-3 activation by theGinkgo biloba extract EGb761. Proc Natl Acad Sci USA2002;99:12197–202.
page 14 of 17 Sun et al. by guest on January 11, 2016
http://bib.oxfordjournals.org/D
ownloaded from

9. Watanabe CM, Wolffram S, Ader P, et al. The in vivoneuromodulatory effects of the herbal medicine ginkgobiloba. Proc Natl Acad Sci USA 2001;98:6577–580.
10. Wu Y, Wu Z, Butko P, etal. Amyloid-beta-induced patho-logical behaviors are suppressed by Ginkgo biloba extractEGb 761 and ginkgolides in transgenic Caenorhabditis ele-gans. J Neurosci 2006;26:13102–13.
11. Perry NS, Bollen C, Perry EK, et al. Salvia for dementiatherapy: review of pharmacological activity and pilot toler-ability clinical trial. Pharmacol Biochem Behav 2003;75:651–9.
12. Little JT, Walsh S, Aisen PS. An update on huperzine A as atreatment for Alzheimer’s disease. Expert Opin Investig Drugs2008;17:209–15.
13. Anekonda TS, Reddy PH. Can herbs provide a new gen-eration of drugs for treating Alzheimer’s disease? Brain ResBrain Res Rev 2005;50:361–76.
14. Bermudez-Lugo JA, Rosales-Hernandez MC, Deeb O,et al. In silico methods to assist drug developers in acetyl-cholinesterase inhibitor design. Curr Med Chem 2011;18:1122–36.
15. Chekmarev D, Kholodovych V, Kortagere S, et al.Predicting inhibitors of acetylcholinesterase by regressionand classification machine learning approaches with com-binations of molecular descriptors. Pharm Res 2009;26:2216–24.
16. Al-Rashid ZF, Hsung RP. (þ)-Arisugacin A—computa-tional evidence of a dual binding site covalent inhibitor ofacetylcholinesterase. BioorgMedChemLett 2011;21:2687–91.
17. da Silva VB, de Andrade P, Kawano DF, et al. In silicodesign and search for acetylcholinesterase inhibitors inAlzheimer’s disease with a suitable pharmacokinetic profileand low toxicity. FutureMed Chem 2011;3:947–60.
18. Adhami HR, Linder T, Kaehlig H, et al. Catechol alkenylsfrom Semecarpus anacardium: acetylcholinesterase inhib-ition and binding mode predictions. J Ethnopharmacol2012;139:142–8.
19. John S, Thangapandian S, Sakkiah S, et al. Potent BACE-1inhibitor design using pharmacophore modeling, in silicoscreening and molecular docking studies. BMCBioinformatics 2011;12(Suppl. 1):S28.
20. Vijayan RS, Prabu M, Mascarenhas NM, et al. Hybridstructure-based virtual screening protocol for the identifica-tion of novel BACE1 inhibitors. J Chem Inf Model 2009;49:647–57.
21. Monceaux CJ, Hirata-Fukae C, Lam PC, et al.Triazole-linked reduced amide isosteres: an approach forthe fragment-based drug discovery of anti-Alzheimer’sBACE1 inhibitors. BioorgMed Chem Lett 2011;21:3992–6.
22. Yang XG, Lv W, Chen YZ, et al. In silico prediction andscreening of gamma-secretase inhibitors by molecular de-scriptors and machine learning methods. J Comput Chem2010;31:1249–58.
23. Lamb J, Crawford ED, Peck D, etal. The connectivity map:using gene-expression signatures to connect small mol-ecules, genes, and disease. Science 2006;313:1929–35.
24. Williams G. A searchable cross-platform gene expressiondatabase reveals connections between drug treatments anddisease. BMCGenomics 2012;13:12.
25. Kong W, Mou X, Hu X. Exploring matrix factorizationtechniques for significant genes identification ofAlzheimer’s disease microarray gene expression data. BMCBioinformatics 2011;12(Suppl 5):S7.
26. Huang Y, Sun X, Hu G. An integrated genetics approachfor identifying protein signal pathways of Alzheimer’s dis-ease. ComputMethods Biomech Biomed Eng 2011;14:371–8.
27. Yanashima R, Kitagawa N, Matsubara Y, et al. Networkfeatures and pathway analyses of a signal transduction cas-cade. Front Neuroinform 2009;3:13.
28. Miller JA, Oldham MC, Geschwind DH. A systems levelanalysis of transcriptional changes in Alzheimer’s disease andnormal aging. J Neurosci 2008;28:1410–20.
29. Li J, Zhu X, Chen JY. Building disease-specificdrug-protein connectivity maps from molecular interactionnetworks and PubMed abstracts. PLoSComput Biol 2009;5:e1000450.
30. Yang L, Chen J, Shi L, et al. Identifying unexpected thera-peutic targets via chemical-protein interactome. PLoS One2010;5:e9568.
31. Perreau VM, Orchard S, Adlard PA, et al. A domain levelinteraction network of amyloid precursor protein and Abetaof Alzheimer’s disease. Proteomics 2010;10:2377–95.
32. Chen JY, Shen C, Sivachenko AY. Mining Alzheimer dis-ease relevant proteins from integrated protein interactomedata. Pac Symp Biocomput 2006;367–78.
33. Mathur S, Dinakarpandian D. Drug repositioning using dis-ease associated biological processes and network analysis ofdrug targets. AMIAAnnu Symp Proc 2011;2011:305–11.
34. Zhao S, Iyengar R. Systems pharmacology: network ana-lysis to identify multiscale mechanisms of drug action. AnnuRev PharmacolToxicol 2012;52:505–21.
35. Berger SI, Iyengar R. Network analyses in systems pharma-cology. Bioinformatics 2009;25:2466–72.
36. Zhao J, Jiang P, Zhang W. Molecular networks for thestudy of TCM pharmacology. Brief Bioinform 2010;11:417–30.
37. Mazza M, Capuano A, Bria P, et al. Ginkgo biloba anddonepezil: a comparison in the treatment of Alzheimer’sdementia in a randomized placebo-controlled double-blindstudy. EurJ Neurol 2006;13:981–5.
38. Tavazoie S, Hughes JD, Campbell MJ, et al. Systematic de-termination of genetic network architecture. Nat Genet1999;22:281–5.
39. Erhardt RA, Schneider R, Blaschke C. Status oftext-mining techniques applied to biomedical text. DrugDiscovToday 2006;11:315–25.
40. Truffinet P, Bordet R, Menard J. Relevance of the evalu-ation criteria used in clinical trials for Alzheimer’s disease.Therapie 2009;64:139–8.
41. Wesnes KA. Assessing change in cognitive function in de-mentia: the relative utilities of the Alzheimer’s disease as-sessment scale-cognitive subscale and the cognitive drugresearch system. Neurodegener Dis 2008;5:261–3.
42. Flaks MK, Forlenza OV, Pereira FS, et al. Short cognitiveperformance test: diagnostic accuracy and educationbias in older Brazilian adults. Arch Clin Neuropsychol 2009;24:301–6.
43. Schneider LS, Clark CM, Doody R, etal. ADCS PreventionInstrument Project: ADCS-clinicians’ global impression ofchange scales (ADCS-CGIC), self-rated and studypartner-rated versions. Alzheimer Dis Assoc Disord 2006;20:S124–38.
44. Lancu I, Olmer A. [The minimental state examination—anup-to-date review]. Harefuah 2006;145:687–90, 701.
Bioinformatics analysis of anti-Alzheimer’s herbal medicines page 15 of 17 by guest on January 11, 2016
http://bib.oxfordjournals.org/D
ownloaded from

45. Ji ZL, Zhou H, Wang JF, et al. Traditional Chinese medi-cine information database. J Ethnopharmacol 2006;103:501.
46. Zhang Z, Wang X, Chen Q, et al. [Clinical efficacy andsafety of huperzine Alpha in treatment of mild to moderateAlzheimer disease, a placebo-controlled, double-blind, ran-domized trial]. ZhonghuaYi Xue ZaZhi 2002;82:941–4.
47. Ye H, Ye L, Kang H, et al. HIT: linking herbal active in-gredients to targets. Nucleic Acids Res 2011;39:D1055–9.
48. Yildirim MA, Goh KI, Cusick ME, et al. Drug-target net-work. Nat Biotechnol 2007;25:1119–26.
49. Hamosh A, Scott AF, Amberger JS, et al. Online MendelianInheritance in Man (OMIM), a knowledgebase of humangenes and genetic disorders. Nucleic Acids Res 2005;33:D514–7.
50. Keshava Prasad TS, Goel R, Kandasamy K, et al. HumanProtein Reference Database–2009 update. Nucleic Acids Res2009;37:D767–72.
51. Ceol A, Chatr Aryamontri A, Licata L, et al. MINT, themolecular interaction database: 2009 update. Nucleic AcidsRes 2009;38:D532–9.
52. Kerrien S, Alam-Faruque Y, Aranda B, et al. IntAct—opensource resource for molecular interaction data. Nucleic AcidsRes 2007;35:D561–5.
53. Stark C, Breitkreutz BJ, Chatr-Aryamontri A, et al. TheBioGRID Interaction Database: 2011 update. Nucleic AcidsRes 2011;39:D698–704.
54. Xenarios I, Salwinski L, Duan XJ, etal. DIP, the Database ofInteracting Proteins: a research tool for studying cellularnetworks of protein interactions. Nucleic Acids Res 2002;30:303–5.
55. Mewes HW, Frishman D, Guldener U, et al. MIPS: a data-base for genomes and protein sequences. Nucleic Acids Res2002;30:31–4.
56. Maslova S, Sneppen K, Zaliznyaka A. Detection of topo-logical patterns in complex networks: correlation profile ofthe internet. Phys AStatTheor Phys 2003;333:529–40.
57. Wishart DS, Knox C, Guo AC, et al. DrugBank: a compre-hensive resource for in silico drug discovery and explor-ation. Nucleic Acids Res 2006;34:D668–72.
58. Birks J. Cholinesterase inhibitors for Alzheimer’s disease.Cochrane Database Syst Rev 2006;1:CD005593.
59. Robinson DM, Keating GM. Memantine: a review of itsuse in Alzheimer’s disease. Drugs 2006;66:1515–34.
60. Qi WN, Chen LE, Zhang L, et al. Reperfusion injury inskeletal muscle is reduced in inducible nitric oxide synthaseknockout mice. JAppl Physiol 2004;97:1323–8.
61. Colton CA, Wilcock DM, Wink DA, et al. The effects ofNOS2 gene deletion on mice expressing mutated humanAbetaPP. JAlzheimers Dis 2008;15:571–87.
62. Lashuel HA, Hartley D, Petre BM, etal. Neurodegenerativedisease: amyloid pores from pathogenic mutations. Nature2002;418:291.
63. Firuzi O, Zhuo J, Chinnici CM, et al. 5-Lipoxygenase genedisruption reduces amyloid-beta pathology in a mousemodel of Alzheimer’s disease. FASEB J 2008;22:1169–78.
64. Manev H, Chen H, Dzitoyeva S, etal. Cyclooxygenases and5-lipoxygenase in Alzheimer’s disease. ProgNeuropsychophar-macol Biol Psychiatry 2011;35:315–9.
65. Gnjec A, D’Costa KJ, Laws SM, et al. Association of allelescarried at TNFA-850 and BAT1-22 with Alzheimer’s dis-ease. J Neuroinflammation 2008;5:36.
66. Luckhaus C, Sand PG. Estrogen Receptor 1 gene (ESR1)variants in Alzheimer’s disease. Results of a meta-analysis.Aging Clin Exp Res 2007;19:165–8.
67. Liu HP, Lin WY, Wu BT, et al. Evaluation of thepoly(ADP-ribose) polymerase-1 gene variants inAlzheimer’s disease. J Clin Lab Anal;24:182–6.
68. Ogata H, Goto S, Sato K, et al. KEGG: KyotoEncyclopedia of Genes and Genomes. Nucleic Acids Res1999;27:29–34.
69. Kanehisa M, Goto S. KEGG: kyoto encyclopedia of genesand genomes. Nucleic Acids Res 2000;28:27–30.
70. Drakkar Soft. Pathway Diagrammer. http://download.cnet.com/Pathway-Diagrammer/3000-2054_4-10844649.html(Oct 24th, 2009–9th Jan, 2012).
71. Furey ML. The prominent role of stimulus processing: cho-linergic function and dysfunction in cognition. Curr OpinNeurol 2011;24:364–70.
72. Goussakov I, Miller MB, Stutzmann GE. NMDA-mediatedCa(2þ) influx drives aberrant ryanodine receptor activationin dendrites of young Alzheimer’s disease mice. J Neurosci2010;30:12128–37.
73. Wang R, Yan H, Tang XC. Progress in studies of huperzineA, a natural cholinesterase inhibitor from Chinese herbalmedicine. Acta Pharmacol Sin 2006;27:1–26.
74. Gordon RK, Nigam SV, Weitz JA, et al. The NMDA re-ceptor ion channel: a site for binding of Huperzine A. JApplToxicol 2001;21(Suppl. 1):S47–51.
75. Kim HK, Park HR, Lee JS, etal. Down-regulation of iNOSand TNF-alpha expression by kaempferol via NF-kappaBinactivation in aged rat gingival tissues. Biogerontology 2007;8:399–408.
76. Brathe A, Gundersen LL, Malterud KE, et al. 6-substitutedpurines as inhibitors of 15-lipoxygenase; a structure-activitystudy. Arch Pharm 2005;338:159–66.
77. Kawai M, Hirano T, Higa S, et al. Flavonoids and relatedcompounds as anti-allergic substances. Allergol Int 2007;56:113–23.
78. Shishodia S, Majumdar S, Banerjee S, et al. Ursolic acidinhibits nuclear factor-kappaB activation induced by car-cinogenic agents through suppression of IkappaBalphakinase and p65 phosphorylation: correlation withdown-regulation of cyclooxygenase 2, matrix metallopro-teinase 9, and cyclin D1. Cancer Res 2003;63:4375–83.
79. Akiyama H, Barger S, Barnum S, et al. Inflammation andAlzheimer’s disease. Neurobiol Aging 2000;21:383–421.
80. Swardfager W, Lanctot K, Rothenburg L, et al. Ameta-analysis of cytokines in Alzheimer’s disease. BiolPsychiatry 2010;68:930–41.
81. Chen D, Daniel KG, Chen MS, et al. Dietary flavonoids asproteasome inhibitors and apoptosis inducers in human leu-kemia cells. Biochem Pharmacol 2005;69:1421–32.
82. Leung LK, Po LS, Lau TY, et al. Effect of dietary flavonolson oestrogen receptor transactivation and cell death induc-tion. BrJ Nutr 2004;91:831–9.
83. Lim H, Kim HP. Inhibition of mammalian collagenase,matrix metalloproteinase-1, by naturally-occurring flavon-oids. PlantaMed 2007;73:1267–74.
84. Geraets L, Moonen HJ, Brauers K, et al. Dietary flavonesand flavonoles are inhibitors of poly(ADP-ribose)-polymerase-1 in pulmonary epithelial cells. J Nutr 2007;137:2190–5.
page 16 of 17 Sun et al. by guest on January 11, 2016
http://bib.oxfordjournals.org/D
ownloaded from

85. Hayeshi R, Mutingwende I, Mavengere W, et al. The in-hibition of human glutathione S-transferases activity byplant polyphenolic compounds ellagic acid and curcumin.Food ChemToxicol 2007;45:286–95.
86. Hsu CL, Lo WH, Yen GC. Gallic acid induces apoptosis in3T3-L1 pre-adipocytes via a Fas- and mitochondrial-mediated pathway. JAgric Food Chem 2007;55:7359–65.
87. Choi YH, Kong KR, Kim YA, et al. Induction of Bax andactivation of caspases during beta-sitosterol-mediated apop-tosis in human colon cancer cells. Int J Oncol 2003;23:1657–62.
88. Behrens MI, Lendon C, Roe CM. A common biologicalmechanism in cancer and Alzheimer’s disease? CurrAlzheimer Res 2009;6:196–204.
89. Fang XK, Gao J, Zhu DN. Kaempferol and quercetin iso-lated from Euonymus alatus improve glucose uptake of3T3-L1 cells without adipogenesis activity. Life Sci 2008;82:615–22.
90. Logendra S, Ribnicky DM, Yang H, et al. Bioassay-guidedisolation of aldose reductase inhibitors from Artemisia dra-cunculus. Phytochemistry 2006;67:1539–46.
91. Jones A, Kulozik P, Ostertag A, etal. Common pathologicalprocesses and transcriptional pathways in Alzheimer’s diseaseand type 2 diabetes. JAlzheimers Dis 2009;16:787–808.
92. Ramana KV. Aldose reductase: new insights for an oldenzyme. Biomol Concepts 2011;2:103–14.
93. Ramana KV, Srivastava SK. Aldose reductase: a novel thera-peutic target for inflammatory pathologies. IntJ BiochemCellBiol 2010;42:17–20.
94. Yu JT, Chang RC, Tan L. Calcium dysregulation inAlzheimer’s disease: from mechanisms to therapeutic oppor-tunities. Prog Neurobiol 2009;89:240–55.
95. Li L, Stanton JD, Tolson AH, etal. Bioactive terpenoids andflavonoids from Ginkgo biloba extract induce the expres-sion of hepatic drug-metabolizing enzymes through preg-nane X receptor, constitutive androstane receptor, and arylhydrocarbon receptor-mediated pathways. PharmRes 2009;26:872–82.
96. Ansari MA, Abdul HM, Joshi G, et al. Protective effect ofquercetin in primary neurons against Abeta(1-42): relevanceto Alzheimer’s disease. J Nutr Biochem 2009;20:269–75.
97. Babiloni C, Babiloni F, Carducci F, etal. Movement-relatedelectroencephalographic reactivity in Alzheimer disease.Neuroimage 2000;12:139–46.
98. Roe CM, Behrens MI, Xiong C, et al. Alzheimer diseaseand cancer. Neurology 2005;64:895–8.
99. Arvanitakis Z, Wilson RS, Bienias JL, etal. Diabetes mellitusand risk of Alzheimer disease and decline in cognitive func-tion. Arch Neurol 2004;61:661–6.
100.Rangel-Ordonez L, Noldner M, Schubert-Zsilavecz M,et al. Plasma levels and distribution of flavonoids in ratbrain after single and repeated doses of standardizedGinkgo biloba extract EGb 761(R). Planta Med 2010;76:1683–90.
101.Kuhn M, Campillos M, Letunic I, et al. A side effect re-source to capture phenotypic effects of drugs. Mol Syst Biol2010;6:343.
102. Ji ZL, Han LY, Yap CW, et al. Drug adverse reaction targetdatabase (DART): proteins related to adverse drug reactions.Drug Saf 2003;26:685–90.
103.Atias N, Sharan R. An algorithmic framework for predict-ing side effects of drugs. J Comput Biol 2011;18:207–18.
104.Lee S, Lee KH, Song M, et al. Building the process-drug-side effect network to discover the relationship betweenbiological processes and side effects. BMC Bioinformatics2011;12(Suppl. 2):S2.
105.Ma C, Kang H, Liu Q, et al. Insight into potential toxicitymechanisms of melamine: an in silico study. Toxicology2011;283:96–100.
106.Brouwers L, Iskar M, Zeller G, et al. Network neighbors ofdrug targets contribute to drug side-effect similarity. PLoSOne 2011;6:e22187.
107.Goh KI, Cusick ME, Valle D, et al. The human diseasenetwork. Proc Natl Acad Sci USA 2007;104:8685–90.
108.Zhang X, Zhang R, Jiang Y, et al. The expanded humandisease network combining protein-protein interaction in-formation. EurJ HumGenet 2011;19:783–8.
109.Wyss-Coray T, Rogers J. Inflammation in Alzheimerdisease-a brief review of the basic science and clinical litera-ture. Cold Spring Harb PerspectMed 2012;2:a006346.
Bioinformatics analysis of anti-Alzheimer’s herbal medicines page 17 of 17 by guest on January 11, 2016
http://bib.oxfordjournals.org/D
ownloaded from