Embed Size (px)
Citation preview

Toward a Science of ConsciousnessTucson2002
April 8-12, 2002Center for Consciousness Studies
University of Arizona
Metacognition in Children with ADHD: Comparison with Controls
Prof. Hélène Poissant, Ph.DUniversité du Québec à Montréal

Statistics on ADHD
- 1% - 3% American school-aged population
- 5% - 10 % other problems/ psychiatric disorder :comorbidity
- Boys are about 3X more likely than girls to develop ADHD
- 30% - 50% still manifest symptoms in adulthood
- 25 % fathers and 17 -25% mothers of ADHD children have this condition

Psychiatric observations: DSM-IV(APA, 1994)9 symptoms of Inattention (ADD)9 symptoms of Hyperactivity/Impulsivity (ADHD)
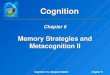
Neurobiological observationsFrontal dysfunction: dorsolateral prefrontal cortex (fig.1)
Reduction in size/activity:prefrontal lobe, basal ganglia & striatum
PET scan: brain areas that control attention used less glucose (fig.2)
ERP: ADHD make more errors and react more slowly than controls in tests of sustained attention
QuickTime™ et un décompresseurPhoto - JPEG sont requis pour visualiser
cette image.

QuickTime™ et un décompresseurPhoto - JPEG sont requis pour visualiser
cette image.
Concurrent explanations of ADHD
- DSM-IV definition of ADHD : insufficient
- deficiency in Attention filtering of ADHD : insufficient
- “control” of impulsivity is a main component of ADHD
- child with ADHD is “hyper-respondent” rather than hyperactive
Barkley,1997,1998

Neuropsychological Evidences
B. I. Tests distinguish ADHD and Control:
ADHD:
•More CPT- Omissions errors;
•More Stroop- Interference and - Word errors;
•Other tests: WCSR; Trail Test; Porteus Mazes; Rey-Osterrieth;
Verbal Fluency; Tower of Hanoi; Time Estimation
Barkley,Grodzinsky & DuPaul,1992; Grodzinsky & Diamond 1992

ADHD children have a deficit in B.I.
- Desinhibited prepotent responses
- Perseveration of ongoing responses
- Poor interference control
Cognitive implication:
•Reduced reflection
•Poor self-questioning
•Deficient rule-governed behavior (instruction)
•Etc.Barkley (1997, 1998)
Behavioral Inhibition (B.I) Hypothesis

Behavioral Inhibition:
•inhibit prepotent response
•interrupt an ongoing response
•interference (intern or extern)
Barkley (1997, 1998)

Behavioral Inhibition
Working memory (Nonverbal)
Internalization of speech(verbal working memory)
Self-regulation of affect/Self-regulation of affect/Motivation/ArousalMotivation/Arousal
Reconstitution
Motor Control/fluency/syntax
Executive Functions

Behavioral Inhibition
N-V. working memory
Holding events in mind
Retrospective function
Prospective function
Self-awareness..
Internalization of speech/V. working memory
Description and reflection
Self-questioning...
Self-regulation affect/motivation/arousal
Self-regulation in the service of goal-directed action...
ReconstitutionAnalysis & Synthesis of B.
Synax of behavior...
Motor control/Fluency/Syntax
Executive Functions

Motor control/ fluency/ syntax
• inhibition of task irrelevant responses• execution of goal-directed responses• goal-directed persistence• sensitivity to response feedback• behavioral flexibility• task re-engagement following disruption
Executive function & Metacognition
Both:•Higher order functioning
•Under governance of prefrontal regions
•Late to mature
Different settings:
Executive function: neuropsychological setting
Metacognition: cognitive developmental setting

Metacognitive Hypothesis
Since:Evidence of neurobiological dysfunctioning in ADHDimplying region of the prefrontal cortex related with B.I.
Evidence of neuropsychological dysfunctioning in ADHDimplying executive functions related with B.I.
Conceptual link between B.I & metacognition theories
We infer that:
ADHD children may experience difficulty in metacognition
Poissant, 2001; 2002

Self-awareness
Metacognitive level Reality level(conform to the fact)
E.g.:«I know that I know» (Brown, 1978; 1987)
«I know that I don ’t know»
E.g.:
«I truly know»
«I truly don ’t know»
Expansion of Brown ’s self-awareness concept ( Poissant, H., 2001)

Secondary ignorance
Metacognitive level Reality level(not conform to the fact)
E.g.:«I don’t know that I know»(Shimamura, 1994)
«I don’t know that I don’t know»(Brown, 1978; 1987)
E.g.:«I truly know»«I truly don ’t know»
Expansion of Brown ’s self-awareness concept ( Poissant, H., 2001)

Knowing what we know
Level of confidence (in our own’s responses) (Brown, 1978; 1987)
Prediction (Brown, 1978; 1987)
E.g.:«I know that I was able to remember an amount x of information»
E.g.:«I know that I am ready to remember an amount x of information»
Poissant, H. (2001)

Knowing what we need to know
Perception of lack of information(Markman, 1978)
Perception of inconsistencies of information (Markman, 1978)
E.g.:«I know that I need a certain kind of information to succeed in task A
E.g.:«I know that information x is in contradiction with information y»
Poissant, H. (2001)

ParticipantsControl (n = 30, mean age = 8): Public SchoolADHD (n=17, mean age = 9): Clinic & Special Education Class
Age group 1= 6-7; Age group 2= 8-9; Age group 3= 10-11.5
1st- 6th grades
Montreal suburban; same SE background
ADHD have a higher score on the Hyperactivity Index of the CPRS-48 (t18.8 = 3.68, p= 0.0016) & on the CTRS-28 (t9.2 = 6.3591, p= 0.0001) compared to Control
Method
Perception of Lack of Information TASK (“Knowing-What-we-Need-to-Nnow”)
Experimenter (E) gives verbally &individually to each child (C) the instructions regarding the performance of a Magic Trick and a Game of Cards
The instructions were designed to be incomplete.E performs, while he describes it, a magic trick in front of C. First, E shows an empty cup, a plate, a penny and a sheet of paper. E makes sure that C sees that the cup is empty. Then, E puts the plate on the empty cup. Then, E wraps the penny in the paper sheet and puts it on the plate. Finally, E makes the wrapped penny slips from the plate into the cup.
(In reality, E pretends to wrap the penny, and let it fall on his own lap. Then E puts the unwrapped penny into the cup, without letting the child know about it).
C must discover what E had “forgotten ” : To mention how the penny could be find unwrapped into the cup, since it was wrapped in the first place.
During the attempt of C to do the Magic Trick, E asks a series of ten questions (10) to help the child discover the missing information (same kind of instruction for the Game of Cards)
TASK

Comparison of means for ADHD and control groups a on perception of lack of information task (metacognitive knowledge)
8,67
6,75
2,67
5,565,39
4,67
0
1
2
3
4
5
6
7
8
9
10
group 1 (6-7) group 2 (8-9) group 3 (10-12)
age groups
num
ber
of q
uest
ions
ADHD
Control
RESULTS
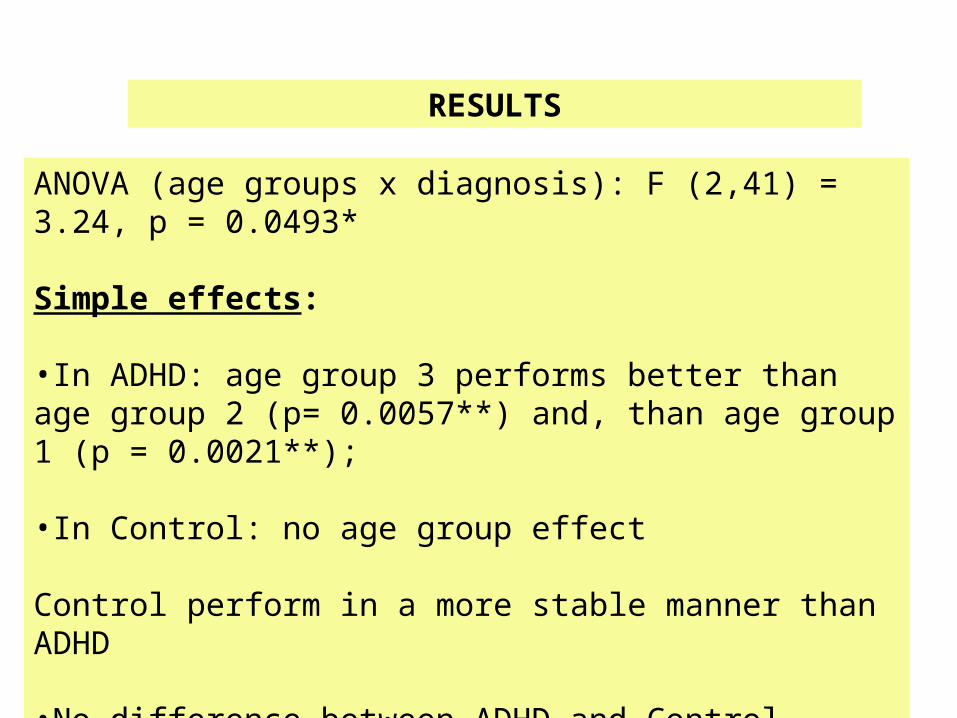
ANOVA (age groups x diagnosis): F (2,41) = 3.24, p = 0.0493*
Simple effects:
•In ADHD: age group 3 performs better than age group 2 (p= 0.0057**) and, than age group 1 (p = 0.0021**);
•In Control: no age group effect
Control perform in a more stable manner than ADHD
•No difference between ADHD and Control(see fig. 4)

DISCUSSION
“Knowing-What-We-Need-to-Know” is an aspect of metacognitiveKnowledge
ADHD and Control did not perform in the same manner across ages on K-W-N-K:
In younger ADHD subjects, the delay in performance of K-W-N-K is progressively fulfilled as ADHD subjects become older
Controls perform in a stable manner across ages
ADHD subjects act as if they take a longer time to reach the Control performance

FUTURE RESEARCH
A comprehension of the link between Executive Functions &Metacognition is beneficial in mutual ways:
1) contributes external validity to standard measurement of E.F
2) gives opportunity for metacognition to be part of assessment ofdysfunctions related to prefrontal symptomatology (e.g. ADHD)
3) helps install metacognitively oriented approaches in treatment ofexecutive disorders (Marlowe, 2001)
Correlation between E.F. & Metacognition among Control and ADHDSubjects should be further explored

SELECTED REFERENCEAmerican Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington,
DC: Author.Barkley, R. A. (1997). ADHD and the nature of self-control. New York, NY: Guilford.Barkley, R.A.(1998). Attention-Deficit Hyperactivity Disorder. Scientific American, 9, 66-71.Benson, D. F. (1991). The role of frontal dysfunction in attention deficit hyperactivity disorder. Journal of Child
Neurology, 6(Suppl.), S9-S12. Biederman, J., Faraone, S. V., Keenan, K., Benjamin, J., Krifcher, B., Moore, C., Sprich-Buckminster, S., Ugaglia, K., Jellinek, M. S., Steingard, R., et al. (1992). Further evidence for family-genetic risk factors in attention deficit
hyperactivity disorder. Patterns of comorbidity in probands and relatives psychiatrically and pediatrically referred samples. Archives of General Psychiatry, 49, 728-38.
Brown, A. L. (1978). Knowing when, where and how to remember: A problem of metacognition. In R. Glaser (Ed.), Advances in instructional psychology. Vol. 1. (pp. 76-115). Hillsdale, NJ: Erlbaum.
Brown, A. L. (1987). Metacognition , executive control, self-regulation, and other more mysterious mechanisms. In F. E. Weinert & R. H. Kluwe (Eds.), Metacognition, motivation, and understanding (pp. 65-116). Hillsdale, NJ: Lawrence Erlbaum.
Conners, K.C. (1990). Conner’s Rating Scale. Toronto: Multihealth System.Faraone, S. V., Biederman, J., & Milberger, S. (1994). An exploratory study of ADHD among second-degree relatives of
ADHD children. Biological Psychiatry, 35, 398-402.Faraone, S. V., Biederman, J., Keenan, K., & Tsuang, M. T. (1991). Separation of DSM-III attention deficit disorder and
conduct disorder: Evidence from a family-genetic study of American child psychiatric patients. Psychological Medicine, 21, 109-121.
Flavell, J. H. (1979). Metacognition and cognitive monitoring: A new area of cognitive-developmental inquiry. American Psychologist, 34, 906-911

Frank, Y., Seiden, J. A., & Napolitano, B. (1994). Event-related potentials to an “oddball” auditory paradigm in children with learning disabilities with or without attention deficit hyperactivity disorder. Clinical Electroencephalography, 25, 136-141.
Gross-Tsur, V., Shalev, R. S., & Amir, N. (1991). Attention deficit disorder: Association with familial-genetic factors. Pediatric Neurology, 7, 258-261.
Hynd, G. W., Hern, K. L., Novey, E. S., Eliopulos, D., Marshall, R., Gonzalez, J. J., & Voeller, K. K. (1993). Attention deficit-hyperactivity disorder and asymmetry of the caudate nucleus. Journal of Child Neurology, 8, 339-
347.Jacoby , L.L. , Witherspoon D. (1982). Remembering without awareness. Canadian Journal of Psychology, 36(2), 300- 324.Janowsky, J.S. , Shimamura, A.P. , Squire, L.R. (1989). Source memory impairement in patients with frontal lobe
lesions. Neuropsychologia, 27, 1043-1056.Klorman, R. (1991). Cognitive event-related potentials in attention deficit disorder. Journal of Learning Disabilities,
24, 130-140. Markman, E. M. (1977). Realizing that you don’t understand: A preliminary investigation. Child Development, 48,
986-992.Semrud-Clikeman, M., Filipek, P. A., Biederman, J., Steingard, R., Kennedy, D., Renshaw, P., & Bekken K. (1994).
Attention-deficit hyperactivity disorder: magnetic resonance imaging morphometric analysis of the corpus callosum. Journal of the American Academy of Child and Adolescent Psychiatry, 33, 875-81.Shimamura, A.P. (1994). Metacognition: Neuropsychological evidence. In J. Metcalfe & A.P. Shimamura (Eds.),
Metacognition: Knowing about knowing (pp. 301-328). Cambridge, MA: MIT Press.Shue, K. L., & Douglas, V. I. (1992). Attention deficit hyperactivity disorder and the frontal lobe syndrome. Brain and
Cognition, 20, 104-24. Trommer, B. L., Hoeppner, J.-A. B., & Zecker, S. G. (1991). The go-no go test in attention deficit disorder is sensitive
to methylphenidate. Journal of Child Neurology, 6(Suppl.), S128-S131.Zametkin, A. J., Nordahl, T. E., Gross, M., King, A. C., Semple, W. E., Rumsey, J., Hamburger, S., & Cohen, R. M.
(1990). Cerebral glucose metabolism in adults with hyperactivity of childhood onset. New England Journal of Medicine, 323, 1361-1366.

Thanks
•Dr. Antonio Trottier, M.D.: Clinique Neuro Rive-Sud (ADHD)
•École Le Déclic & C. Mercier (ADHD)
•École Paul-de-Maricourt (Control)
Graduate students:Linda St-Onge, Claudia ÉcrementAnnick Léveillé, Christiane ChalfounJosée Delisle, Sarah LecomteMarie-Odile Dade
Funds:Conseil de Recherches en Sciences Humaines du Canada