Embed Size (px)
Citation preview

Minimally Invasive Therapy. 2012;21:150–160
REVIEW ARTICLE
Totally laparoscopic gastrectomy for gastric cancer: Meta-analysis ofshort-term outcomes
UMBERTO BRACALE1,2,3, MARCELLA ROVANI2, MARCELLO BRACALE2,GIUSTO PIGNATA3, FRANCESCO CORCIONE4, LEANDRO PECCHIA2
1Department of General, Vascular and Thoracic Surgery. University Federico II of Naples, Italy, 2Department ofBiomedical, Electronic and Telecommunication Engineering, University Federico II of Naples, Italy, 3General andMini-invasive Surgical Unit. “San Camillo” Hospital,Trento, Italy, and 4General and Mini-invasive Surgical Unit.“Monaldi” Hospital, Naples, Italy
AbstractIntroduction: We present a review of the literature, together with a meta-analysis of short-term outcomes of totally laparoscopicgastrectomy (TLG) compared with open gastrectomy (OG). Material & methods: We carried out a search in the Pubmed andCochrane databases from September 2003 toMay 2009. Controlled studies on early outcomes were included, both prospectiveand retrospective, randomized and non-randomized. Results: We found nine eligible studies, one of which was a randomizedcontrolled trial (RCT), while eight were series of patients (three consecutive). The study group consisted of 1,492 patients,828 of whom had been treated with TLG and 664 treated with OG. TLG for gastric cancer shows a 32.5% (p < 0.001) longeroperative time than OG, whereas TLG demonstrated a 44% (p < 0.001) reduction in blood loss, a 34% (p < 0.001) reductiontime to first flatus and a 33.7% reduced (p < 0.001) hospital stay. No notable differences were registered regarding morbidityand mortality rates, and no significant difference was observed between the two groups regarding the extent of thelymphadenectomy. Conclusions: Despite a longer operative time for TLG, with a gastrointestinal recovery rate faster thanthe OG one for gastric cancer results, no notable differences were recorded between the two techniques for the morbidity andmortality rates and in the spread of the lymphadenectomy.
Key words: Laparoscopy, gastric malignancy, totally laparoscopic gastrectomy
Introduction
Laparoscopic surgery for benign diseases is rapidlyemerging as the new standard for surgery, as there isnow a wide scientific literature supporting its effec-tiveness and efficiency. Nevertheless, laparoscopicsurgery for gastric tumors has not fully entered intodaily clinical practice, especially for malignancies.Scientific literature has shown that the laparo-
scopic procedure surpasses traditional surgery byimproving on primary outcomes such as post-operative pain, hospital stay, and an earlier returnto work. This is also the case, for instance, forfundoplicatio or cholecystectomy (1). More recentlyother studies have reported an improvement inintra-operative blood loss, reduced post-operative
pain and accelerated recovery, an earlier return tonormal bowel functioning with an earlier resump-tion of oral intake and earlier discharge from hos-pital. This is also the case for minimally invasivetechniques applied to colorectal surgery for bothbenign and malignant conditions (2).The first laparoscopic gastric resection for a malig-
nant disease was performed in 1993 by Azagra et al.and was described later on, together with their seriesof laparoscopically assisted gastrectomies for malig-nant diseases (3). Furthermore, in Japan, a total of5,271 laparoscopic gastrectomies were performedbetween 1991 and 2003, and more than 1,500 gas-trectomies were carried out laparoscopically in2003 (4). Kitano et al. (5) first reported laparoscopicgastrectomy with Billorth I anastomosis for early
Correspondence: U. Bracale, General and Mini-invasive Surgical Unit. “San Camillo” Hospital, Via Giovanelli 19, I-38100 Trento, Italy. E-mail: [email protected]
ISSN 1364-5706 print/ISSN 1365-2931 online � 2012 Informa HealthcareDOI: 10.3109/13645706.2011.588712
Min
im I
nvas
ive
The
r A
llied
Tec
hnol
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Ant
onio
Sci
uto
on 0
4/27
/14
For
pers
onal
use
onl
y.

gastric cancer (EGC) in 1994. They used the term“laparoscopy-assisted distal gastrectomy” (LADG),as a mini-laparotomy was required for gastric sectionand anastomosis. Most of the Korean and Japanesesurgeons preferred the “laparoscopy-assisted”-typegastrectomy.Nevertheless, several studies have focused on
the feasibility and safety of “totally laparoscopicgastrectomy”, which we consider as a laparoscopicapproach with intra-corporeal anastomosis (ICA)(6). Compared with the laparoscopy-assisted proce-dure, the totally laparoscopic procedure might prove tobe less invasive, especially in patients with a high bodymass index.The success of both assisted and totally laparo-
scopic surgery in gastric resections for malignantdisease has been evidenced (7–9).More especially, several meta-analyses have shown
the feasibility and advantages of laparoscopy-asisted gstrectomy (LAG) compared with open gas-trectomy (OG) (10–14).Nevertheless, the anastomosis procedure, which dis-
tinguishes assisted from totally laparoscopic surgerycould affect the short-term outcomes of this type ofsurgery. Thus, it might prove interesting to comparetheoutcomesof totally laparoscopicgastrectomy(TLG)with laparoscopic-assisted gastrectomy (LAG). Unfor-tunately, only a few published studies havemade a clearcomparison between LAG and TLG.For these reasons, although LAG has proved to be
feasible, effective and widely used, we performed thismeta-analysis by focusing exclusively on TLG, andexcluded studies involving assisted laparoscopy.Finally, we meta-analyzed short-term outcomes ofTLG compared with open gastrectomy (OG), asOG is still considered to be the benchmark (15,16).
Material and methods
In planning this systematic review, we consideredJadad’s score and Cochrane statements. (17) Unfor-tunately, we also had to include non-randomizedstudies on account of the small number of studiesfocusing exclusively on the totally laparoscopicapproach.
Study designs
Controlled studies on outcomes of totally laparo-scopic gastrectomy (TLG) versus open gastrectomy(OG) were included, whether prospective or retro-spective, randomized or non-randomized. As statedabove, we excluded studies on assisted laparoscopicgastrectomy. In the beginning our focus concentratedon both short- and long-term outcomes; however, we
did not find enough studies to meta-analyze long-term outcomes.
Study group
The stage of tumors ranged from I to IV, according tothe Japanese Research Society for Gastric Cancer(JSGC) (18), with no significant difference foundbetween the treated and the control groups. Finally,there was no significant difference between the twotreatment groups in terms of age and sex distribution.
Search strategy
A search into the Pubmed andCochrane databases wascarried out until May 2009, and the following textualterms andMeSHheadings were used: “laparoscopic orlaparoscopy, cancer or malignant, gastrectomy”; lan-guage restrictions were not applied during the research,but articles written in languages other than Englishwere eventually excluded. Duplicates were removed.We did not find any reviews published in Cochrane.From the titles of all the articles, we excluded the onesthat were of no relevance. After this the abstracts of theremaining studies were reviewed to exclude heteroge-neity in population, control groups, and surgical tech-nique. Finally, other relevant articles were retrievedfrom reference lists of selected publications.
Inclusion and exclusion criteria
Relevant studies published in English by the end of2003 and presenting the short-term outcomes of theoperation were included in the study. Inclusion cri-teria were as follows:
. Study type-RCTs and non-randomized prospec-tive and retrospective studies,
. studies that analyzed both TLG and OG for thetreatment of gastric cancer,
. studies with any sample size, and
. when we found several studies reporting the samepatients, we included only the most recent study.Two authors, using a prefixed criteria-scoringsystem, selected the full papers independently.
Data extraction
The results of the selected studies were extracted andtabulated by two investigators. Disagreements wereresolved by discussion and consensus.
Statistical methods
Relative risk (RR), confidence intervals (CI)and P-values were calculated by using fixed or
Meta-analysis on laparoscopic gastrectomy for cancer 151
Min
im I
nvas
ive
The
r A
llied
Tec
hnol
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Ant
onio
Sci
uto
on 0
4/27
/14
For
pers
onal
use
onl
y.

random-effect models when appropriate, and by usingthe Cochran Q-test to assess heterogeneity. Cumula-tive weighted ratios (CWR) and differences (CWD)were used to assess continuous outcomes. Publicationbias or systematic heterogeneity were excluded byusing funnel plots.
Results
Studies included and excluded
In performing this research, we identified 594 studies inPubmed. We did not find any similar review publishedinCochrane.After reading the titles,475wereexcluded,as they were of no interest.We classified the abstracts ofthe 119 remaining papers by using a prefixed criteria-scoring system. Of these 108 were excluded at this stepbecause of the non-conformity with the focus. Finally,the complete texts of the remaining 11 articles wereretrieved and reviewed. Of these, nine (19–27), fulfilledthe inclusion criteria. One of the excluded studies was afirst publication about the same study (28) and pre-sented a partial duplication of the data; moreover, thegroups of patients were far too heterogeneous since theywere affected by different kinds of cancers. The secondanalyzed the results of different kinds of tumors such asthe oesaphago-gastric one (29). Hence, this reviewincluded a total of nine studies published between2003 and 2009. Also, although no language restrictionshad been introduced, all the selected studies were pub-lished in English. The entire procedure is representedin Figure 1.For the data pooling we selected nine studies, one
of which was a randomized controlled trial (RCT),while eight were series of patients, three of themconsecutive, as reported in Table I.
Study group
The study group consisted of 1,492 patients, 99.0%with gastric adenocarcinoma and the remaining 1.0%with other types of tumors, which were not possible toisolate from the results. Of the 1,492 patients, 828 weretreated with totally laparoscopic gastrectomy, and664 were treated with open gastrectomy (Table II).The study group included 1,482 patients with gastricadenocarcinoma and ten patients with other types oftumor; as represented in Table III, the stage of tumorranged between I and IV, according to the JapaneseResearch Society for Gastric Cancer (JSGC).
Outcome
Meta-analysed outcomes were continuous, such asoperative time, blood loss, hospital stay, retrieval of
lymph nodes and time to flatus, and binaries, suchas post-operative complications and post-operativemortality. The former have been expressed by usingweighted mean differences (WMD), whereas the lat-ter by using relative risk (Table IV).Another parameter which might be considered
is the conversion rate. Nonetheless, we did not findenough homogenous data since the convertedpatients were excluded by certain authors.
Operative time
All nine studies considered suitable for the meta-analysis reported a longer operative time for TLGthan for OG without exception, as shown in Table V.The mean duration of the laparoscopic surgeries wassignificantly longer than that of the open proce-dures (246.2 minutes for the laparoscopic group vs186.0 minutes for the open group). The meta-anal-ysis, therefore, revealed a significant increase in oper-ating time of 60.4 minutes ([35.4, 85.4], p < 0.001)for TLG compared with OG.
Blood loss
Eight of the nine papers considered suitable fordata extraction reported this outcome, as shownin Table VI; seven of them showed a reduced bloodloss for TLG compared with OG.
1. Computerized research
594 Studies
2. Selection by titles
119 Studies
3. Selection by abstracts
4. Full text analyisis
9 Studies
11 Studies
Figure 1. Flowchart describing study selection and excludedstudies.
152 U. Bracale et al.
Min
im I
nvas
ive
The
r A
llied
Tec
hnol
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Ant
onio
Sci
uto
on 0
4/27
/14
For
pers
onal
use
onl
y.
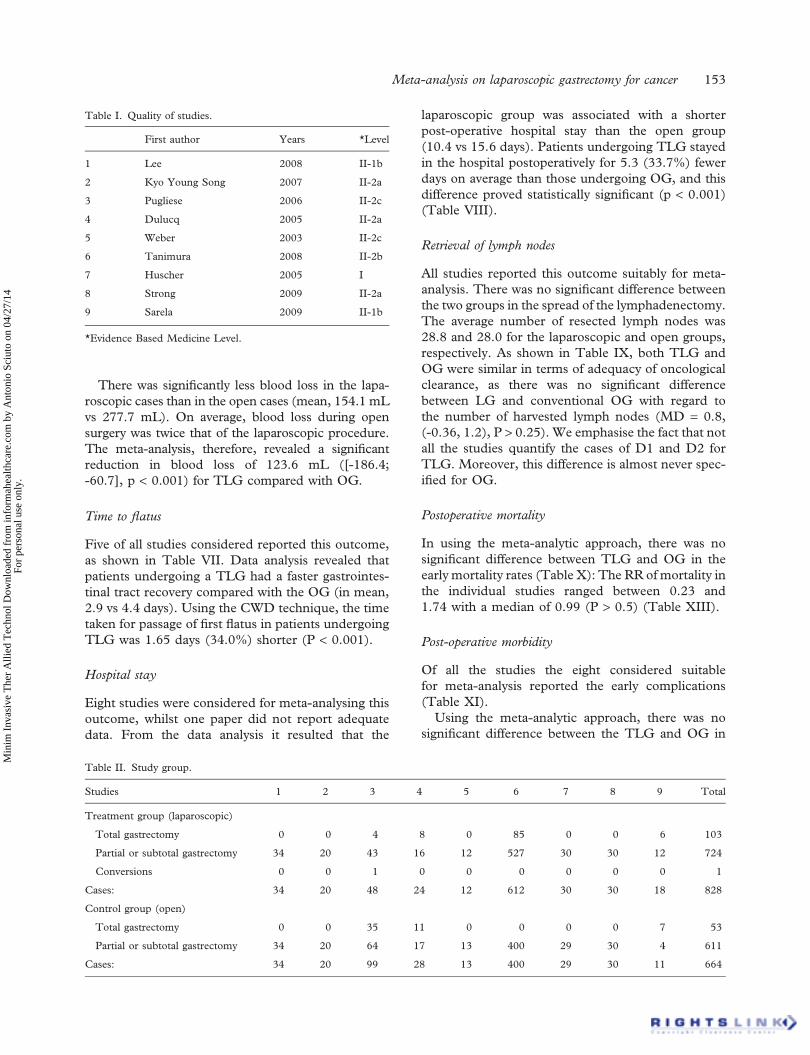
There was significantly less blood loss in the lapa-roscopic cases than in the open cases (mean, 154.1 mLvs 277.7 mL). On average, blood loss during opensurgery was twice that of the laparoscopic procedure.The meta-analysis, therefore, revealed a significantreduction in blood loss of 123.6 mL ([-186.4;-60.7], p < 0.001) for TLG compared with OG.
Time to flatus
Five of all studies considered reported this outcome,as shown in Table VII. Data analysis revealed thatpatients undergoing a TLG had a faster gastrointes-tinal tract recovery compared with the OG (in mean,2.9 vs 4.4 days). Using the CWD technique, the timetaken for passage of first flatus in patients undergoingTLG was 1.65 days (34.0%) shorter (P < 0.001).
Hospital stay
Eight studies were considered for meta-analysing thisoutcome, whilst one paper did not report adequatedata. From the data analysis it resulted that the
laparoscopic group was associated with a shorterpost-operative hospital stay than the open group(10.4 vs 15.6 days). Patients undergoing TLG stayedin the hospital postoperatively for 5.3 (33.7%) fewerdays on average than those undergoing OG, and thisdifference proved statistically significant (p < 0.001)(Table VIII).
Retrieval of lymph nodes
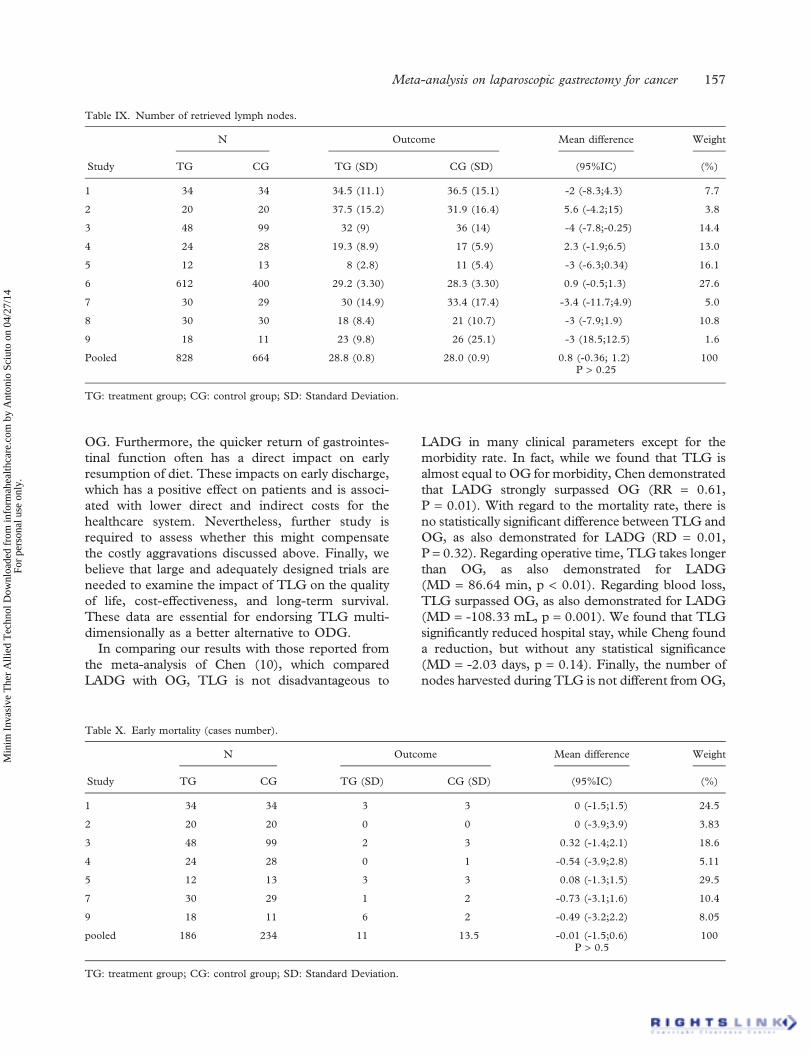
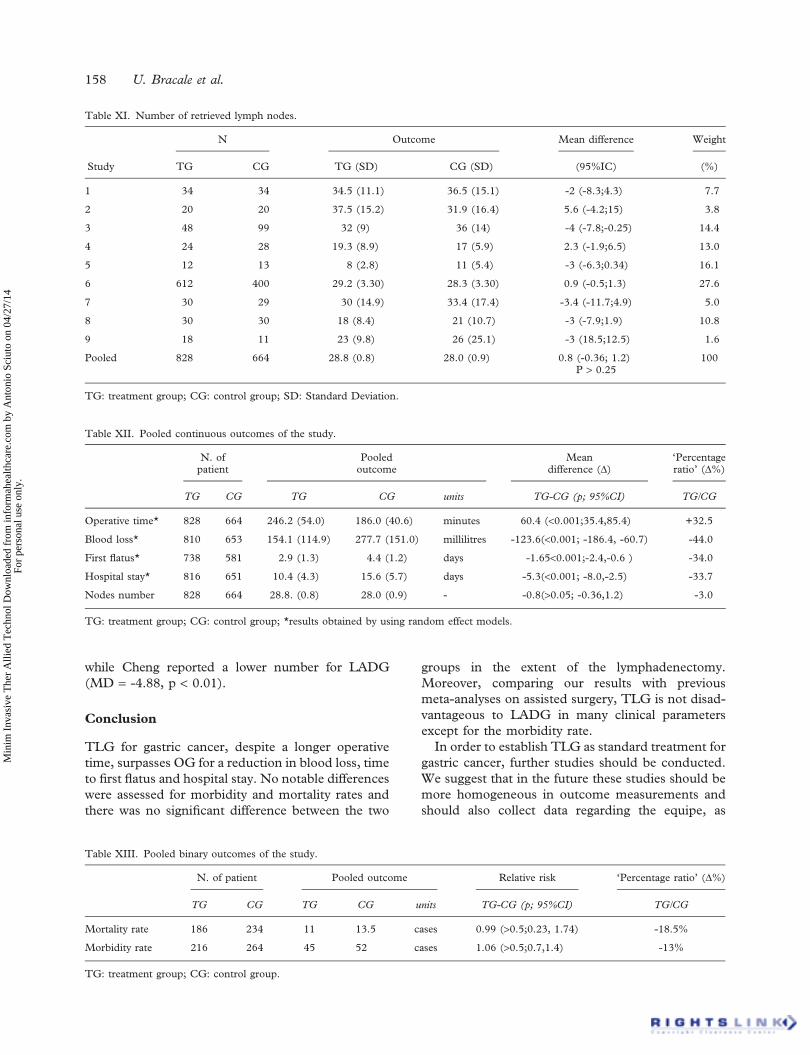
All studies reported this outcome suitably for meta-analysis. There was no significant difference betweenthe two groups in the spread of the lymphadenectomy.The average number of resected lymph nodes was28.8 and 28.0 for the laparoscopic and open groups,respectively. As shown in Table IX, both TLG andOG were similar in terms of adequacy of oncologicalclearance, as there was no significant differencebetween LG and conventional OG with regard tothe number of harvested lymph nodes (MD = 0.8,(-0.36, 1.2), P > 0.25). We emphasise the fact that notall the studies quantify the cases of D1 and D2 forTLG. Moreover, this difference is almost never spec-ified for OG.
Postoperative mortality
In using the meta-analytic approach, there was nosignificant difference between TLG and OG in theearly mortality rates (Table X): The RR of mortality inthe individual studies ranged between 0.23 and1.74 with a median of 0.99 (P > 0.5) (Table XIII).
Post-operative morbidity
Of all the studies the eight considered suitablefor meta-analysis reported the early complications(Table XI).Using the meta-analytic approach, there was no
significant difference between the TLG and OG in
Table I. Quality of studies.
First author Years *Level
1 Lee 2008 II-1b
2 Kyo Young Song 2007 II-2a
3 Pugliese 2006 II-2c
4 Dulucq 2005 II-2a
5 Weber 2003 II-2c
6 Tanimura 2008 II-2b
7 Huscher 2005 I
8 Strong 2009 II-2a
9 Sarela 2009 II-1b
*Evidence Based Medicine Level.
Table II. Study group.
Studies 1 2 3 4 5 6 7 8 9 Total
Treatment group (laparoscopic)
Total gastrectomy 0 0 4 8 0 85 0 0 6 103
Partial or subtotal gastrectomy 34 20 43 16 12 527 30 30 12 724
Conversions 0 0 1 0 0 0 0 0 0 1
Cases: 34 20 48 24 12 612 30 30 18 828
Control group (open)
Total gastrectomy 0 0 35 11 0 0 0 0 7 53
Partial or subtotal gastrectomy 34 20 64 17 13 400 29 30 4 611
Cases: 34 20 99 28 13 400 29 30 11 664
Meta-analysis on laparoscopic gastrectomy for cancer 153
Min
im I
nvas
ive
The
r A
llied
Tec
hnol
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Ant
onio
Sci
uto
on 0
4/27
/14
For
pers
onal
use
onl
y.
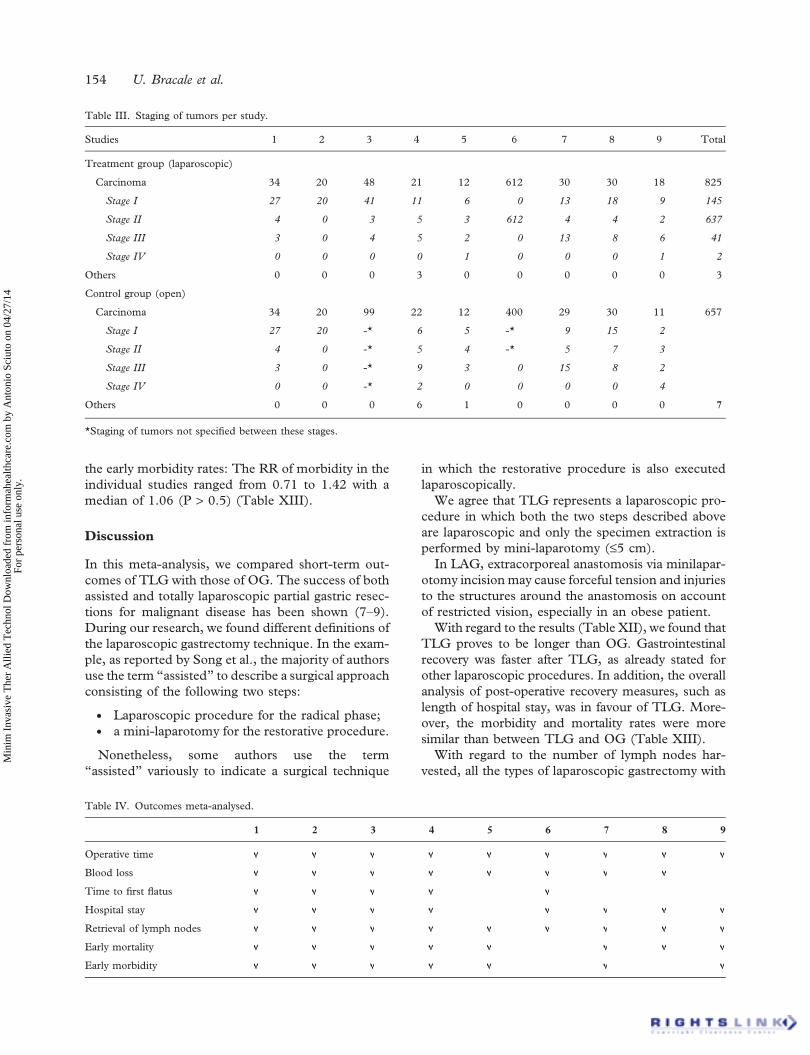
the early morbidity rates: The RR of morbidity in theindividual studies ranged from 0.71 to 1.42 with amedian of 1.06 (P > 0.5) (Table XIII).
Discussion
In this meta-analysis, we compared short-term out-comes of TLG with those of OG. The success of bothassisted and totally laparoscopic partial gastric resec-tions for malignant disease has been shown (7–9).During our research, we found different definitions ofthe laparoscopic gastrectomy technique. In the exam-ple, as reported by Song et al., the majority of authorsuse the term “assisted” to describe a surgical approachconsisting of the following two steps:
. Laparoscopic procedure for the radical phase;
. a mini-laparotomy for the restorative procedure.
Nonetheless, some authors use the term“assisted” variously to indicate a surgical technique
in which the restorative procedure is also executedlaparoscopically.We agree that TLG represents a laparoscopic pro-
cedure in which both the two steps described aboveare laparoscopic and only the specimen extraction isperformed by mini-laparotomy (£5 cm).In LAG, extracorporeal anastomosis via minilapar-
otomy incisionmay cause forceful tension and injuriesto the structures around the anastomosis on accountof restricted vision, especially in an obese patient.With regard to the results (Table XII), we found that
TLG proves to be longer than OG. Gastrointestinalrecovery was faster after TLG, as already stated forother laparoscopic procedures. In addition, the overallanalysis of post-operative recovery measures, such aslength of hospital stay, was in favour of TLG. More-over, the morbidity and mortality rates were moresimilar than between TLG and OG (Table XIII).With regard to the number of lymph nodes har-
vested, all the types of laparoscopic gastrectomy with
Table III. Staging of tumors per study.
Studies 1 2 3 4 5 6 7 8 9 Total
Treatment group (laparoscopic)
Carcinoma 34 20 48 21 12 612 30 30 18 825
Stage I 27 20 41 11 6 0 13 18 9 145
Stage II 4 0 3 5 3 612 4 4 2 637
Stage III 3 0 4 5 2 0 13 8 6 41
Stage IV 0 0 0 0 1 0 0 0 1 2
Others 0 0 0 3 0 0 0 0 0 3
Control group (open)
Carcinoma 34 20 99 22 12 400 29 30 11 657
Stage I 27 20 -* 6 5 -* 9 15 2
Stage II 4 0 -* 5 4 -* 5 7 3
Stage III 3 0 -* 9 3 0 15 8 2
Stage IV 0 0 -* 2 0 0 0 0 4
Others 0 0 0 6 1 0 0 0 0 7
*Staging of tumors not specified between these stages.
Table IV. Outcomes meta-analysed.
1 2 3 4 5 6 7 8 9
Operative time
Blood loss
Time to first flatus
Hospital stay
Retrieval of lymph nodes
Early mortality
Early morbidity
154 U. Bracale et al.
Min
im I
nvas
ive
The
r A
llied
Tec
hnol
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Ant
onio
Sci
uto
on 0
4/27
/14
For
pers
onal
use
onl
y.
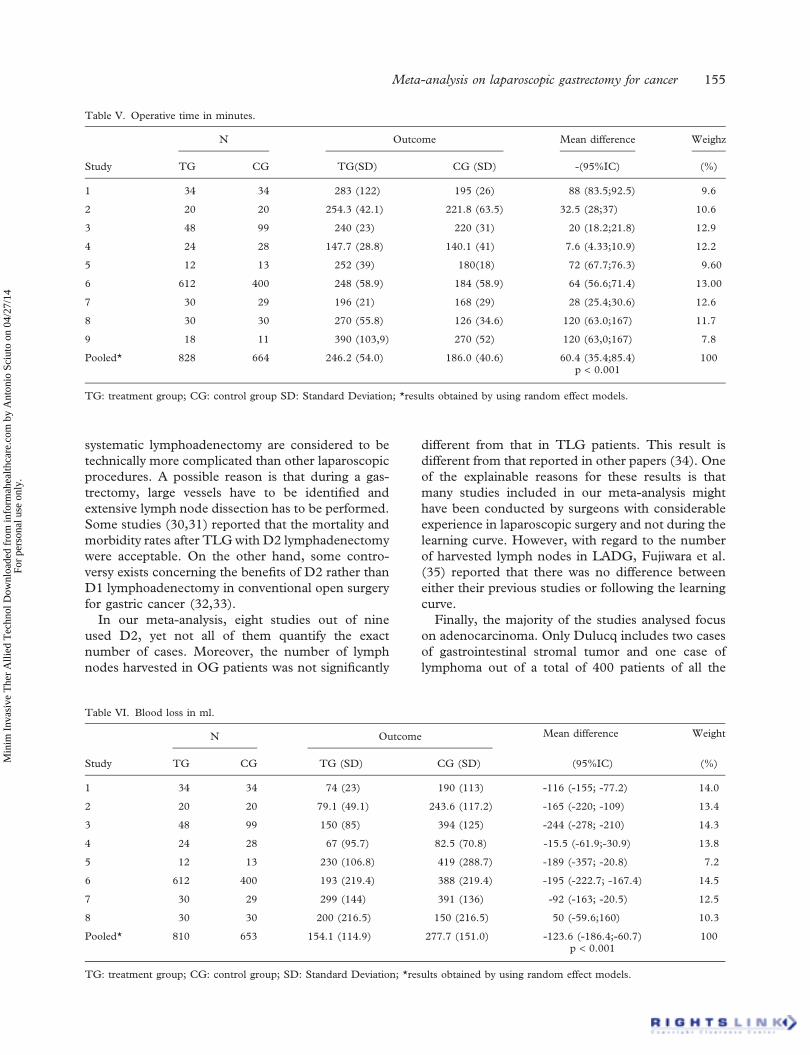
systematic lymphoadenectomy are considered to betechnically more complicated than other laparoscopicprocedures. A possible reason is that during a gas-trectomy, large vessels have to be identified andextensive lymph node dissection has to be performed.Some studies (30,31) reported that the mortality andmorbidity rates after TLG with D2 lymphadenectomywere acceptable. On the other hand, some contro-versy exists concerning the benefits of D2 rather thanD1 lymphoadenectomy in conventional open surgeryfor gastric cancer (32,33).In our meta-analysis, eight studies out of nine
used D2, yet not all of them quantify the exactnumber of cases. Moreover, the number of lymphnodes harvested in OG patients was not significantly
different from that in TLG patients. This result isdifferent from that reported in other papers (34). Oneof the explainable reasons for these results is thatmany studies included in our meta-analysis mighthave been conducted by surgeons with considerableexperience in laparoscopic surgery and not during thelearning curve. However, with regard to the numberof harvested lymph nodes in LADG, Fujiwara et al.(35) reported that there was no difference betweeneither their previous studies or following the learningcurve.Finally, the majority of the studies analysed focus
on adenocarcinoma. Only Dulucq includes two casesof gastrointestinal stromal tumor and one case oflymphoma out of a total of 400 patients of all the
Table V. Operative time in minutes.
N Outcome Mean difference Weighz
Study TG CG TG(SD) CG (SD) -(95%IC) (%)
1 34 34 283 (122) 195 (26) 88 (83.5;92.5) 9.6
2 20 20 254.3 (42.1) 221.8 (63.5) 32.5 (28;37) 10.6
3 48 99 240 (23) 220 (31) 20 (18.2;21.8) 12.9
4 24 28 147.7 (28.8) 140.1 (41) 7.6 (4.33;10.9) 12.2
5 12 13 252 (39) 180(18) 72 (67.7;76.3) 9.60
6 612 400 248 (58.9) 184 (58.9) 64 (56.6;71.4) 13.00
7 30 29 196 (21) 168 (29) 28 (25.4;30.6) 12.6
8 30 30 270 (55.8) 126 (34.6) 120 (63.0;167) 11.7
9 18 11 390 (103,9) 270 (52) 120 (63,0;167) 7.8
Pooled* 828 664 246.2 (54.0) 186.0 (40.6) 60.4 (35.4;85.4)p < 0.001
100
TG: treatment group; CG: control group SD: Standard Deviation; *results obtained by using random effect models.
Table VI. Blood loss in ml.
N Outcome Mean difference Weight
Study TG CG TG (SD) CG (SD) (95%IC) (%)
1 34 34 74 (23) 190 (113) -116 (-155; -77.2) 14.0
2 20 20 79.1 (49.1) 243.6 (117.2) -165 (-220; -109) 13.4
3 48 99 150 (85) 394 (125) -244 (-278; -210) 14.3
4 24 28 67 (95.7) 82.5 (70.8) -15.5 (-61.9;-30.9) 13.8
5 12 13 230 (106.8) 419 (288.7) -189 (-357; -20.8) 7.2
6 612 400 193 (219.4) 388 (219.4) -195 (-222.7; -167.4) 14.5
7 30 29 299 (144) 391 (136) -92 (-163; -20.5) 12.5
8 30 30 200 (216.5) 150 (216.5) 50 (-59.6;160) 10.3
Pooled* 810 653 154.1 (114.9) 277.7 (151.0) -123.6 (-186.4;-60.7)p < 0.001
100
TG: treatment group; CG: control group; SD: Standard Deviation; *results obtained by using random effect models.
Meta-analysis on laparoscopic gastrectomy for cancer 155
Min
im I
nvas
ive
The
r A
llied
Tec
hnol
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Ant
onio
Sci
uto
on 0
4/27
/14
For
pers
onal
use
onl
y.
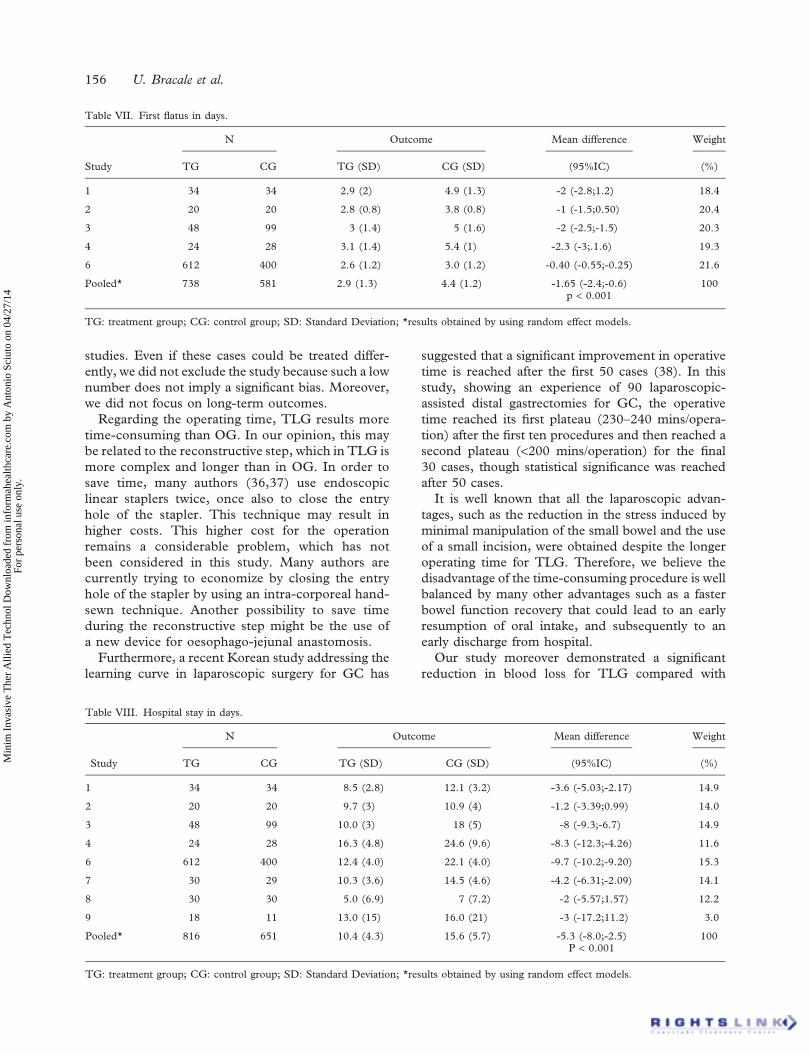
studies. Even if these cases could be treated differ-ently, we did not exclude the study because such a lownumber does not imply a significant bias. Moreover,we did not focus on long-term outcomes.Regarding the operating time, TLG results more
time-consuming than OG. In our opinion, this maybe related to the reconstructive step, which in TLG ismore complex and longer than in OG. In order tosave time, many authors (36,37) use endoscopiclinear staplers twice, once also to close the entryhole of the stapler. This technique may result inhigher costs. This higher cost for the operationremains a considerable problem, which has notbeen considered in this study. Many authors arecurrently trying to economize by closing the entryhole of the stapler by using an intra-corporeal hand-sewn technique. Another possibility to save timeduring the reconstructive step might be the use ofa new device for oesophago-jejunal anastomosis.Furthermore, a recent Korean study addressing the
learning curve in laparoscopic surgery for GC has
suggested that a significant improvement in operativetime is reached after the first 50 cases (38). In thisstudy, showing an experience of 90 laparoscopic-assisted distal gastrectomies for GC, the operativetime reached its first plateau (230–240 mins/opera-tion) after the first ten procedures and then reached asecond plateau (<200 mins/operation) for the final30 cases, though statistical significance was reachedafter 50 cases.It is well known that all the laparoscopic advan-
tages, such as the reduction in the stress induced byminimal manipulation of the small bowel and the useof a small incision, were obtained despite the longeroperating time for TLG. Therefore, we believe thedisadvantage of the time-consuming procedure is wellbalanced by many other advantages such as a fasterbowel function recovery that could lead to an earlyresumption of oral intake, and subsequently to anearly discharge from hospital.Our study moreover demonstrated a significant
reduction in blood loss for TLG compared with
Table VII. First flatus in days.
N Outcome Mean difference Weight
Study TG CG TG (SD) CG (SD) (95%IC) (%)
1 34 34 2.9 (2) 4.9 (1.3) -2 (-2.8;1.2) 18.4
2 20 20 2.8 (0.8) 3.8 (0.8) -1 (-1.5;0.50) 20.4
3 48 99 3 (1.4) 5 (1.6) -2 (-2.5;-1.5) 20.3
4 24 28 3.1 (1.4) 5.4 (1) -2.3 (-3;.1.6) 19.3
6 612 400 2.6 (1.2) 3.0 (1.2) -0.40 (-0.55;-0.25) 21.6
Pooled* 738 581 2.9 (1.3) 4.4 (1.2) -1.65 (-2.4;-0.6)p < 0.001
100
TG: treatment group; CG: control group; SD: Standard Deviation; *results obtained by using random effect models.
Table VIII. Hospital stay in days.
N Outcome Mean difference Weight
Study TG CG TG (SD) CG (SD) (95%IC) (%)
1 34 34 8.5 (2.8) 12.1 (3.2) -3.6 (-5.03;-2.17) 14.9
2 20 20 9.7 (3) 10.9 (4) -1.2 (-3.39;0.99) 14.0
3 48 99 10.0 (3) 18 (5) -8 (-9.3;-6.7) 14.9
4 24 28 16.3 (4.8) 24.6 (9.6) -8.3 (-12.3;-4.26) 11.6
6 612 400 12.4 (4.0) 22.1 (4.0) -9.7 (-10.2;-9.20) 15.3
7 30 29 10.3 (3.6) 14.5 (4.6) -4.2 (-6.31;-2.09) 14.1
8 30 30 5.0 (6.9) 7 (7.2) -2 (-5.57;1.57) 12.2
9 18 11 13.0 (15) 16.0 (21) -3 (-17.2;11.2) 3.0
Pooled* 816 651 10.4 (4.3) 15.6 (5.7) -5.3 (-8.0;-2.5)P < 0.001
100
TG: treatment group; CG: control group; SD: Standard Deviation; *results obtained by using random effect models.
156 U. Bracale et al.
Min
im I
nvas
ive
The
r A
llied
Tec
hnol
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Ant
onio
Sci
uto
on 0
4/27
/14
For
pers
onal
use
onl
y.
OG. Furthermore, the quicker return of gastrointes-tinal function often has a direct impact on earlyresumption of diet. These impacts on early discharge,which has a positive effect on patients and is associ-ated with lower direct and indirect costs for thehealthcare system. Nevertheless, further study isrequired to assess whether this might compensatethe costly aggravations discussed above. Finally, webelieve that large and adequately designed trials areneeded to examine the impact of TLG on the qualityof life, cost-effectiveness, and long-term survival.These data are essential for endorsing TLG multi-dimensionally as a better alternative to ODG.In comparing our results with those reported from
the meta-analysis of Chen (10), which comparedLADG with OG, TLG is not disadvantageous to
LADG in many clinical parameters except for themorbidity rate. In fact, while we found that TLG isalmost equal to OG for morbidity, Chen demonstratedthat LADG strongly surpassed OG (RR = 0.61,P = 0.01). With regard to the mortality rate, there isno statistically significant difference between TLG andOG, as also demonstrated for LADG (RD = 0.01,P = 0.32). Regarding operative time, TLG takes longerthan OG, as also demonstrated for LADG(MD = 86.64 min, p < 0.01). Regarding blood loss,TLG surpassed OG, as also demonstrated for LADG(MD = -108.33 mL, p = 0.001). We found that TLGsignificantly reduced hospital stay, while Cheng founda reduction, but without any statistical significance(MD = -2.03 days, p = 0.14). Finally, the number ofnodes harvested during TLG is not different from OG,
Table IX. Number of retrieved lymph nodes.
N Outcome Mean difference Weight
Study TG CG TG (SD) CG (SD) (95%IC) (%)
1 34 34 34.5 (11.1) 36.5 (15.1) -2 (-8.3;4.3) 7.7
2 20 20 37.5 (15.2) 31.9 (16.4) 5.6 (-4.2;15) 3.8
3 48 99 32 (9) 36 (14) -4 (-7.8;-0.25) 14.4
4 24 28 19.3 (8.9) 17 (5.9) 2.3 (-1.9;6.5) 13.0
5 12 13 8 (2.8) 11 (5.4) -3 (-6.3;0.34) 16.1
6 612 400 29.2 (3.30) 28.3 (3.30) 0.9 (-0.5;1.3) 27.6
7 30 29 30 (14.9) 33.4 (17.4) -3.4 (-11.7;4.9) 5.0
8 30 30 18 (8.4) 21 (10.7) -3 (-7.9;1.9) 10.8
9 18 11 23 (9.8) 26 (25.1) -3 (18.5;12.5) 1.6
Pooled 828 664 28.8 (0.8) 28.0 (0.9) 0.8 (-0.36; 1.2)P > 0.25
100
TG: treatment group; CG: control group; SD: Standard Deviation.
Table X. Early mortality (cases number).
N Outcome Mean difference Weight
Study TG CG TG (SD) CG (SD) (95%IC) (%)
1 34 34 3 3 0 (-1.5;1.5) 24.5
2 20 20 0 0 0 (-3.9;3.9) 3.83
3 48 99 2 3 0.32 (-1.4;2.1) 18.6
4 24 28 0 1 -0.54 (-3.9;2.8) 5.11
5 12 13 3 3 0.08 (-1.3;1.5) 29.5
7 30 29 1 2 -0.73 (-3.1;1.6) 10.4
9 18 11 6 2 -0.49 (-3.2;2.2) 8.05
pooled 186 234 11 13.5 -0.01 (-1.5;0.6)P > 0.5
100
TG: treatment group; CG: control group; SD: Standard Deviation.
Meta-analysis on laparoscopic gastrectomy for cancer 157
Min
im I
nvas
ive
The
r A
llied
Tec
hnol
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Ant
onio
Sci
uto
on 0
4/27
/14
For
pers
onal
use
onl
y.
while Cheng reported a lower number for LADG(MD = -4.88, p < 0.01).
Conclusion
TLG for gastric cancer, despite a longer operativetime, surpasses OG for a reduction in blood loss, timeto first flatus and hospital stay. No notable differenceswere assessed for morbidity and mortality rates andthere was no significant difference between the two
groups in the extent of the lymphadenectomy.Moreover, comparing our results with previousmeta-analyses on assisted surgery, TLG is not disad-vantageous to LADG in many clinical parametersexcept for the morbidity rate.In order to establish TLG as standard treatment for
gastric cancer, further studies should be conducted.We suggest that in the future these studies should bemore homogeneous in outcome measurements andshould also collect data regarding the equipe, as
Table XI. Number of retrieved lymph nodes.
N Outcome Mean difference Weight
Study TG CG TG (SD) CG (SD) (95%IC) (%)
1 34 34 34.5 (11.1) 36.5 (15.1) -2 (-8.3;4.3) 7.7
2 20 20 37.5 (15.2) 31.9 (16.4) 5.6 (-4.2;15) 3.8
3 48 99 32 (9) 36 (14) -4 (-7.8;-0.25) 14.4
4 24 28 19.3 (8.9) 17 (5.9) 2.3 (-1.9;6.5) 13.0
5 12 13 8 (2.8) 11 (5.4) -3 (-6.3;0.34) 16.1
6 612 400 29.2 (3.30) 28.3 (3.30) 0.9 (-0.5;1.3) 27.6
7 30 29 30 (14.9) 33.4 (17.4) -3.4 (-11.7;4.9) 5.0
8 30 30 18 (8.4) 21 (10.7) -3 (-7.9;1.9) 10.8
9 18 11 23 (9.8) 26 (25.1) -3 (18.5;12.5) 1.6
Pooled 828 664 28.8 (0.8) 28.0 (0.9) 0.8 (-0.36; 1.2)P > 0.25
100
TG: treatment group; CG: control group; SD: Standard Deviation.
Table XII. Pooled continuous outcomes of the study.
N. ofpatient
Pooledoutcome
Meandifference (D)
‘Percentageratio’ (D%)
TG CG TG CG units TG-CG (p; 95%CI) TG/CG
Operative time* 828 664 246.2 (54.0) 186.0 (40.6) minutes 60.4 (<0.001;35.4,85.4) +32.5
Blood loss* 810 653 154.1 (114.9) 277.7 (151.0) millilitres -123.6(<0.001; -186.4, -60.7) -44.0
First flatus* 738 581 2.9 (1.3) 4.4 (1.2) days -1.65<0.001;-2.4,-0.6 ) -34.0
Hospital stay* 816 651 10.4 (4.3) 15.6 (5.7) days -5.3(<0.001; -8.0,-2.5) -33.7
Nodes number 828 664 28.8. (0.8) 28.0 (0.9) - -0.8(>0.05; -0.36,1.2) -3.0
TG: treatment group; CG: control group; *results obtained by using random effect models.
Table XIII. Pooled binary outcomes of the study.
N. of patient Pooled outcome Relative risk ‘Percentage ratio’ (D%)
TG CG TG CG units TG-CG (p; 95%CI) TG/CG
Mortality rate 186 234 11 13.5 cases 0.99 (>0.5;0.23, 1.74) -18.5%
Morbidity rate 216 264 45 52 cases 1.06 (>0.5;0.7,1.4) -13%
TG: treatment group; CG: control group.
158 U. Bracale et al.
Min
im I
nvas
ive
The
r A
llied
Tec
hnol
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Ant
onio
Sci
uto
on 0
4/27
/14
For
pers
onal
use
onl
y.

learning curve. In the studies analyzed, we found alack of certain important results, such as the conver-sion rate. However, whereas laparoscopic approachesfor benign gastric disease are already in wider use,TLG is not yet the gold standard procedure formalignancies.
Acknowledgment
The authors thank Albert Coward for his preciouscontribution in reviewing the article English language.The authors acknowledge the IHTSC for the editorialsupport.
Declaration of interest:Umberto Bracale, MarcellaRovani, Marcello Bracale, Giusto Pignata, FrancescoCorcione and Leandro Pecchia have no conflicts ofinterest or financial ties to disclose.
References
1. Scott TR, Zucker KA, Bailey RW. Laparoscopic cholecystec-tomy: a review of 12,397 patients. Surg Laparosc Endosc.1992;2:191–8.
2. Abraham NS, Byrne CM, Young JM and SolomonMJ. Meta-analysis of non-randomized comparative studies of the short-term outcomes of laparoscopic resection for colorectal cancerANZ J. Surg. 2007;77:508–16.
3. Azagra JS, Georgen M, De Simone P, Ibanez-Aguire JL.Minimally invasive surgery for gastric cancer. Surg Endosc.1999;13:351–7.
4. Shiraishi N, Yasuda K, Kitano S. Laparoscopic gastrectomywith lymph node dissection for gastric cancer. Gastric Cancer2006;9:167–76.
5. Kitano S, Iso Y, Moriyama M, Sugimachi K. Laparoscopyassisted Billroth I gastrectomy. Surg Laparosc Endosc. 1994;4:146–8.
6. Kim JJ, Song KY, Chin HM, Kim W, Jeon HM, Park CH,et al. The early experience with a totally laparoscopic distalgastrectomy. J Korean Gastric Cancer Assoc. 2005;5:16–22.
7. Kitano S, Adachi Y, Shiraishi N, Suematsu T,Bando T. Laparoscopic-assisted proximal gastrectomy forearly gastric carcinomas. Surg Today 1999; 29:389–91.
8. Kitano S, Shiraishi N, Fujii K, Yasuda K, Inomata M,Adachi Y. A randomized controlled trial comparing open vslaparoscopy- assisted distal gastrectomy for the treatment ofearly gastric cancer: An interim report. Surgery 2002;131:S306–11.
9. Shiraishi N, Adachi Y, Kitano S, Bandoh T, Katsuta T,Morimoto A. Indication for and outcome of laparoscopy-assisted Billrot I gastrectomy. Br J Surg. 1999;86:541–4.
10. Chen XZ, Hu JK, Yang K, Wang L, Lu QC. Short-termevaluation of laparoscopy-assisted distal gastrectomy for pre-dictive early gastric cancer: a meta-analysis of randomizedcontrolled trials. Surg Laparosc Endosc Percutan Tech. 2009;19:277-84.
11. Ohtani H, Tamamori Y, Noguchi K, Azuma T, Fujimoto S,Oba H, et al. A Meta-Analysis of Randomized ControlledTrials that Compared Laparoscopy-Assisted and Open DistalGastrectomy for Early Gastric Cancer. J Gastrointest Surg.2010;14:958–64.
12. Yakoub D, Athanasiou T, Tekkis P, Hanna GB. Laparoscopicassisted distal gastrectomy for early gastric cancer: Is it analternative to the open approach? Surgical Oncology 2008;doi:10.1016/j.suronc.2008.08.006.
13. Memon MA, Khan S, Yunus RM, Barr R, Memon B. Meta-analysis of laparoscopic and open distal gastrectomy for gastriccarcinoma. Surg Endosc. 2008;22:1781-9.
14. Hosono S, Arimoto Y, Ohtani H, Kanamiya Y. Meta-analysisof short-term outcomes after laparoscopy-assisted distalgastrectomy. World J Gastroenterol. 2006;12:76-83.
15. Management of oesophageal and gastric cancer. A nationalclinical guideline. S.I.G.N. June 2006 ISBN 1 899893598.
16. Laparoscopic Gastrectomy for cancer. National Institute forHealth and Clinical Excellence. July 2008 ISBN 1-84629-753-2.
17. Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D,Stroup DF, . for the QUOROMGroup*Improving the qualityof reports of meta-analyses of randomised controlled trials: theQUOROM statement THE LANCET 1999;354.
18. Japanese Gastric Cancer Association. Japanese Classificationof Gastric Carcinoma - 2nd English Edition. Gastric Cancer1998;11:10–24.
19. Lee WJ, Wang W, Chen TC, Chen JC, Ser KH. TotallyLaparoscopic Radical BII Gastrectomy for the Treatment ofGastric Cancer A Comparison With Open Surgery. SurgLaparosc Endosc Percutan Tech. 2008;18:369–74.
20. Song KY, Park CH, Kang HC, Kim JJ, Park SM, Jun KH,et al. Is Totally Laparoscopic Gastrectomy Less Invasive ThanLaparoscopy-assisted Gastrectomy? Prospective, MulticenterStudy. J Gastrointest Surg. 2008;12:1015–21.
21. Pugliese R, Maggioni D, Sansonna F, Scandroglio I,Ferrari GC, Di Lernia S, et al. Total and subtotal laparoscopicgastrectomy for adenocarcinoma, Surg Endosc. 2007;21:21–7.
22. Dulucq JL, Wintringer P, Stabilini C, Solinas L, Perissat J,Mahajna A. Laparoscopic and open gastric resections formalignant lesions A prospective, comparative study, SurgEndosc. 2005;19:933–8.
23. Weber KJ, Reyes CD, Gagner M, Divino CM. Comparison oflaparoscopic and open gastrectomy for malignant disease.Surg Endosc. 2003;17:968–71.
24. Tanimura S, Higashino M, Fukunaga Y, Kishida S,Nishikawa M, Ogata A et Al. Laparoscopic gastrectomy forgastric cancer: experience with more than 600 cases. SurgEndosc 2008; 22:1161–64.
25. Huscher CGS, Mingoli A, Sgarzini G, Sansonetti A,Di Paola M, Recher A, et al. Laparoscopic Versus OpenSubtotal Gastrectomy for Distal Gastric Cancer: Five-YearResults of a Randomized Prospective Trial. Annals of Surgery2005;241:232–7.
26. Strong VE, Devaud N, Allen PJ, Gonen M, Brennan MF,Coit D. Laparoscopic Versus Open Subtotal Gastrectomy forAdenocarcinoma: A Case–Control Study. Annals of SurgicalOncology 2009;16:1507-13.
27. Sarela AI. Entirely laparoscopic radical gastrectomy for ade-nocarcinoma: lymph node yield and resection margins. SurgEndosc. 2009;23:153-60.
28. Reyes CD, Weber KJ, Gagner M, Divino CM. Laparoscopicvs open gastrectomy: A retrospective review. Surg Endosc.2001;15:928–31.
29. Varela JE, Hiyashi M, Nguyen T, Sabio A, Wilson SE,Nguyen NT. Comparison of laparoscopic and open gastrec-tomy for gastric cancer. Am J Surg. 2006;192:837–42.
30. Noshiro H, Nagai E, Shimizu S, Uchiyama A,Tanaka M. Laparoscopically assisted distal gastrectomy
Meta-analysis on laparoscopic gastrectomy for cancer 159
Min
im I
nvas
ive
The
r A
llied
Tec
hnol
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Ant
onio
Sci
uto
on 0
4/27
/14
For
pers
onal
use
onl
y.

with standard radical lymph node dissection for gastric cancer.Surg Endosc. 2005;19:1592–6.
31. Miura S, Kodera Y, Fujiwara M, Ito S, Mochizuki Y,Yamamura Y, et al. Laparoscopy-assisted distal gastrectomywith systemic lymph node dissection: a critical reappraisalfrom the viewpoint of lymph node retrieval. J Am Coll Surg.2004;198:933–8.
32. Bonenkamp JJ, Songun I, Hermans J, Sasako M, Welvaart K,Plukker JT, et al. Randomised comparison of morbidity afterD1 andD2 dissection for gastric cancer in 996Dutch patients.Lancet 1995;345:745–8.
33. Cuschieri A, Fayers P, Fielding J, Craven J, Bancewicz J,Joypaul V, et al. Postoperative morbidity and mortality afterD1 and D2 resections for gastric cancer: preliminary results ofthe MRC randomised controlled surgical trial. The SurgicalCooperative Group. Lancet 1996;347:995–9.
34. Yakoub D, Athanasiou T, Tekkis P, Hanna GB. Laparoscopicassisted distal gastrectomy for early gastric cancer: Is it an
alternative to the open approach? Surg Oncol. 2009;18:322–33.
35. Fujiwara M, Kodera Y, Miura S, Kanyama Y, Yokoyama H,Ohashi N, et al. Laparoscopy assisted distal gastrectomy withsystemic lymph node dissection: a phase II study following thelearning curve. J Surg Oncol. 2005;91:26–32.
36. Kim JJ, Song KY, Chin HM, Kim W, Jeon HM,Park CH, et al. Totally laparoscopic gastrectomy with varioustypes of intracorporeal anastomosis using laparoscopic linearstaplers: preliminary experience. Surg Endosc. 2008;22:436–42.
37. Matsui H, Uyama I, Sugioka A, Fujita J, Komori Y,Ochiai M, et al. Linear stapling forms improved anastomosesduring esophagojejunostomy after a total gastrectomy. Am JSurg. 2002;184:58–60.
38. Kim MC. Learning curve of laparoscopy-assisted distal gas-trectomy with systemic lymphadenectomy for early gastriccancer. World J Gastroenterol. 2005;11:7508.
160 U. Bracale et al.
Min
im I
nvas
ive
The
r A
llied
Tec
hnol
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Ant
onio
Sci
uto
on 0
4/27
/14
For
pers
onal
use
onl
y.





























